
Wearable Sensors and Machine Learning for Hypovolemia Problems in Occupational, Military and Sports Medicine: Physiological Basis, Hardware and Algorithms

 , ,
, ,  ,
,
Abstract
1. Introduction
2. Hypovolemia and Cardiovascular Adjustments
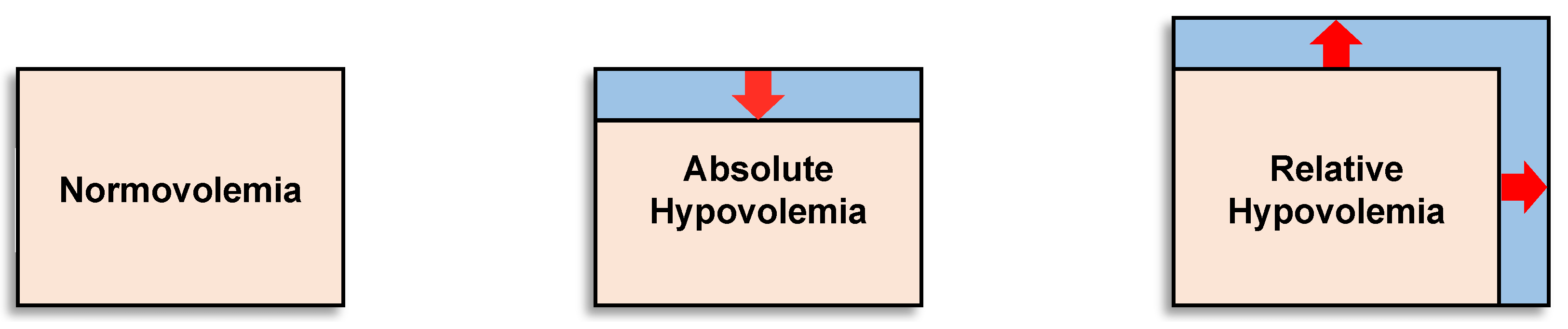
2.1. Relative and Absolute Hypovolemia
2.2. Hypovolemia from Dehydration
2.3. Hypovolemia from Environmental Stress
2.4. Hypovolemia from Physical Work
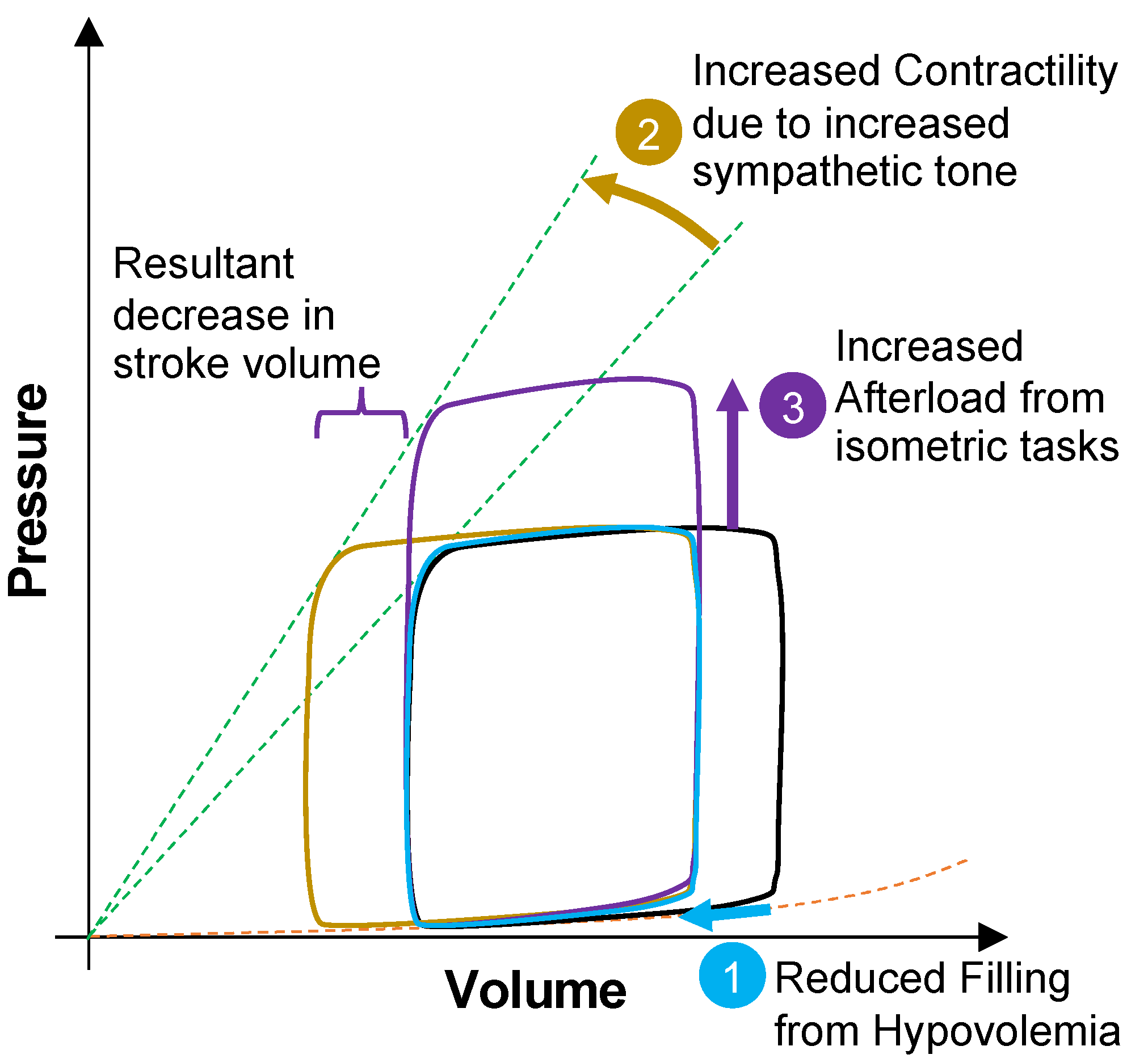
2.5. Cardiovascular Adjustments to Hypovolemia
3. Identifying Integrated Physiological Signals of Compensatory Reserve or Decompensation
3.1. Compensatory Reserve
3.2. Validation of Compensatory Reserve for Heat Stress, Dehydration and Physical Exercise
3.3. Future Capabilities Required to Further Advance the CRM
3.4. Blood Volume Decompensation Status: Multi-Sensor Fusion with Explainable AI
3.5. Validation of Decompensation Status
3.6. Advancements and Next Steps
4. Future Technology Advancement Opportunities
4.1. Contextual Measures
4.2. Integration
4.3. Applications and Opportunities
5. Summary
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sawka, M.N.; Cheuvront, S.N.; Kenefick, R.W. Hypohydration and Human Performance: Impact of Environment and Physiological Mechanisms. Sports Med. 2015, 45, S51–S60. [Google Scholar] [CrossRef]
- Wittbrodt, M.T.; Sawka, M.N.; Mizelle, J.C.; Wheaton, L.A.; Millard-Stafford, M.L. Exercise-heat stress with and without water replacement alters brain structures and impairs visuomotor performance. Physiol. Rep. 2018, 6, e13805. [Google Scholar] [CrossRef] [PubMed]
- Castellani, J.W.; Muza, S.R.; Cheuvront, S.N.; Sils, I.V.; Fulco, C.S.; Kenefick, R.W.; Beidleman, B.A.; Sawka, M.N. Effect of hypohydration and altitude exposure on aerobic exercise performance and acute mountain sickness. J. Appl. Physiol. 2010, 109, 1792–1800. [Google Scholar] [CrossRef] [PubMed]
- Sawka, M.N.; Young, A.J.; Latzka, W.A.; Neufer, P.D.; Quigley, M.D.; Pandolf, K.B. Human Tolerance to Heat Strain During Exercise—Influence of Hydration. J. Appl. Physiol. 1992, 73, 368–375. [Google Scholar] [CrossRef]
- Carter, R.; Cheuvront, S.N.; Vernieuw, C.R.; Sawka, M.N. Hypohydration and prior heat stress exacerbates decreases in cerebral blood flow velocity during standing. J. Appl. Physiol. 2006, 101, 1744–1750. [Google Scholar] [CrossRef] [PubMed]
- Kenefick, R.W.; Sawka, M.N. Hydration at the work site. J. Am. Coll. Nutr. 2007, 26, 597S–603S. [Google Scholar] [CrossRef]
- Convertino, V.A.; Koons, N.J.; Suresh, M.R. Physiology of Human Hemorrhage and Compensation. Compr. Physiol. 2021, 11, 1531–1574. [Google Scholar] [CrossRef]
- Cheuvront, S.N.; Kenefick, R.W.; Montain, S.J.; Sawka, M.N. Water. In Present Knowledge in Nutrition: Basic Nutrition and Metabolism; Marriott, B.P., Birt, D.F., Stallings, V.A., Yates, A.A., Eds.; Academic Press: London, UK, 2020; Volume 1, pp. 503–514. [Google Scholar]
- Buller, M.J.; Welles, A.P.; Friedl, K.E. Wearable physiological monitoring for human thermal-work strain optimization. J. Appl. Physiol. 2018, 124, 432–441. [Google Scholar] [CrossRef]
- Davey, S.L.; Downie, V.; Griggs, K.; Havenith, G. The physiological strain index does not reliably identify individuals at risk of reaching a thermal tolerance limit. Eur. J. Appl. Physiol. 2021, 121, 1701–1713. [Google Scholar] [CrossRef]
- Sonna, L.A.; Kain, J.E.; Hoyt, R.W.; Muza, S.R.; Sawka, M.N. Ambulatory physiological status monitoring during a mountaineering expedition. Mil. Med. 2000, 165, 860–866. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Kimball, J.P.; Zia, J.S.; An, S.T.; Rolfes, C.; Hahn, J.O.; Sawka, M.N.; Inan, O.T. Unifying the Estimation of Blood Volume Decompensation Status in a Porcine Mode of Relative and Absolute Hypovolemia Via Wearable Sensing. IEEE J. Biomed. Health Inform. 2021, 25, 3351–3360. [Google Scholar] [CrossRef] [PubMed]
- Convertino, V.A.; Sawka, M.N. Wearable technology for compensatory reserve to sense hypovolemia. J. Appl. Physiol. 2018, 124, 442–451. [Google Scholar] [CrossRef]
- Convertino, V.A.; Schauer, S.G.; Weitzel, E.K.; Cardin, S.; Stackle, M.E.; Talley, M.J.; Sawka, M.N.; Inan, O.T. Wearable Sensors Incorporating Compensatory Reserve Measurement for Advancing Physiological Monitoring in Critically Injured Trauma Patients. Sensors 2020, 20, 6413. [Google Scholar] [CrossRef] [PubMed]
- Convertino, V.A.; Lye, K.R.; Koons, N.J.; Joyner, M.J. Physiological comparison of hemorrhagic shock and VO(2)max: A conceptual framework for defining the limitation of oxygen delivery. Exp. Biol. Med. 2019, 244, 690–701. [Google Scholar] [CrossRef]
- Cheuvront, S.N.; Kenefick, R.W.; Charkoudian, N.; Sawka, M.N. Physiologic basis for understanding quantitative dehydration assessment. Am. J. Clin. Nutr. 2013, 97, 455–462. [Google Scholar] [CrossRef]
- Young, A.J.; Muza, S.R.; Sawka, M.N.; Pandolf, K.B. Human vascular fluid responses to cold stress are not altered by cold acclimation. Undersea Biomed. Res. 1987, 14, 215–228. [Google Scholar] [PubMed]
- Beidleman, B.A.; Staab, J.E.; Muza, S.R.; Sawka, M.N. Quantitative model of hematologic and plasma volume responses after ascent and acclimation to moderate to high altitudes. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2017, 312, R265–R272. [Google Scholar] [CrossRef] [PubMed]
- Pendergast, D.R.; Moon, R.E.; Krasney, J.J.; Held, H.E.; Zamparo, P. Human Physiology in an Aquatic Environment. Compr. Physiol. 2015, 5, 1705–1750. [Google Scholar] [CrossRef]
- Sawka, M.N.; Leon, L.R.; Montain, S.J.; Sonna, L.A. Integrated Physiological Mechanisms of Exercise Performance, Adaptation, and Maladaptation to Heat Stress. Compr. Physiol. 2011, 1, 1883–1928. [Google Scholar] [CrossRef]
- Crandall, C.G.; Gonzalez-Alonso, J. Cardiovascular function in the heat-stressed human. Acta Physiol. 2010, 199, 407–423. [Google Scholar] [CrossRef]
- Kenefick, R.W.; Sollanek, K.J.; Charkoudian, N.; Sawka, M.N. Impact of skin temperature and hydration on plasma volume responses during exercise. J. Appl. Physiol. 2014, 117, 413–420. [Google Scholar] [CrossRef] [PubMed]
- Montain, S.J.; Sawka, M.N.; Latzka, W.A.; Valeri, C.R. Thermal and cardiovascular strain from hypohydration: Influence of exercise intensity. Int. J. Sports Med. 1998, 19, 87–91. [Google Scholar] [CrossRef]
- Nybo, L.; Rasmussen, P.; Sawka, M.N. Performance in the Heat-Physiological Factors of Importance for Hyperthermia-Induced Fatigue. Compr. Physiol. 2014, 4, 657–689. [Google Scholar] [CrossRef] [PubMed]
- Periard, J.D.; Travers, G.J.S.; Racinais, S.; Sawka, M.N. Cardiovascular adaptations supporting human exercise-heat acclimation. Auton. Neurosci. Basic Clin. 2016, 196, 52–62. [Google Scholar] [CrossRef] [PubMed]
- Bass, D.E.; Henschel, A. Responses of Body Fluid Compartments to Heat and Cold. Physiol. Rev. 1956, 36, 128–144. [Google Scholar] [CrossRef]
- Convertino, V.A.; Greenleaf, J.E.; Bernauer, E.M. Role of Thermal and Exercise Factors in the Mechanism of Hypervolemia. J. Appl. Physiol. 1980, 48, 657–664. [Google Scholar] [CrossRef] [PubMed]
- Sawka, M.N.; Coyle, E.F. Influence of body water and blood volume on thermoregulation and exercise performance in the heat. Exerc. Sport Sci. Rev. 1999, 27, 167–218. [Google Scholar] [PubMed]
- Oberholzer, L.; Siebenmann, C.; Mikkelsen, C.J.; Junge, N.; Piil, J.F.; Morris, N.B.; Goetze, J.P.; Lundby, A.K.M.; Nybo, L.; Lundby, C. Hematological Adaptations to Prolonged Heat Acclimation in Endurance-Trained Males. Front. Physiol. 2019, 10, 1379. [Google Scholar] [CrossRef]
- Sawka, M.N.; Young, A.J. Acute Polycythemia and Human-Performance during Exercise and Exposure to Extreme Environments. Exerc. Sport Sci. Rev. Ser. 1989, 17, 265–293. [Google Scholar] [CrossRef]
- Hoyt, R.W.; Honig, A. Environmental Influences on Body Fluid Balance During Exercise: Altitude. In Body Fluid Balance: Exercise and Sport; Buskirk, E.R., Puhl, S.M., Eds.; CRC Press: Boca Raton, FL, USA, 1996; pp. 183–196. [Google Scholar]
- Sawka, M.N.; Young, A.J.; Rock, P.B.; Lyons, T.P.; Boushel, R.; Freund, B.J.; Muza, S.R.; Cymerman, A.; Dennis, R.C.; Pandolf, K.B.; et al. Altitude acclimatization and blood volume: Effects of exogenous erythrocyte volume expansion. J. Appl. Physiol. 1996, 81, 636–642. [Google Scholar] [CrossRef]
- Young, A.J.; Karl, J.P.; Berryman, C.E.; Montain, S.J.; Beidleman, B.A.; Pasiakos, S.M. Variability in human plasma volume responses during high-altitude sojourn. Physiol. Rep. 2019, 7, e14051. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, R.R.; Kenefick, R.W.; Muza, S.R.; Hamilton, S.W.; Sawka, M.N. Sweat rate and prediction validation during high-altitude treks on Mount Kilimanjaro. J. Appl. Physiol. 2013, 114, 436–443. [Google Scholar] [CrossRef]
- Simmons, G.H.; Minson, C.T.; Cracowski, J.L.; Halliwill, J.R. Systemic hypoxia causes cutaneous vasodilation in healthy humans. J. Appl. Physiol. 2007, 103, 608–615. [Google Scholar] [CrossRef] [PubMed]
- Freund, B.J.; Young, A.J. Environmental Influences on Body Fluid Balance during Exercise: Cold Exposure. In Body Fluid Balance: Exercise and Sport; Buskirk, E.R., Puhl, S.M., Eds.; CRC Press: Boca Raton, FL, USA, 1996; pp. 159–181. [Google Scholar]
- Alba, B.K.; Castellani, J.W.; Charkoudian, N. Cold-induced cutaneous vasoconstriction in humans: Function, dysfunction and the distinctly counterproductive. Exp. Physiol. 2019, 104, 1202–1214. [Google Scholar] [CrossRef] [PubMed]
- Hellsten, Y.; Nyberg, M. Cardiovascular Adaptations to Exercise Training. Compr. Physiol. 2016, 6, 1–32. [Google Scholar] [CrossRef]
- Convertino, V.A. Blood volume response to physical activity and inactivity. Am. J. Med. Sci. 2007, 334, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Sawka, M.N.; Convertino, V.A.; Eichner, E.R.; Schnieder, S.M.; Young, A.J. Blood volume: Importance and adaptations to exercise training, environmental stresses, and trauma/sickness. Med. Sci. Sports Exerc. 2000, 32, 332–348. [Google Scholar] [CrossRef]
- Neufer, P.D. The Effect of Detraining and Reduced Training on the Physiological Adaptations to Aerobic ExerciseTraining. Sports Med. 1989, 8, 302–320. [Google Scholar] [CrossRef]
- Chou, T.H.; Allen, J.R.; Hahn, D.; Leary, B.K.; Coyle, E.F. Cardiovascular responses to exercise when increasing skin temperature with narrowing of the core-to-skin temperature gradient. J. Appl. Physiol. 2018, 125, 697–705. [Google Scholar] [CrossRef]
- Petrofsky, J.S.; Phillips, C.A. The Physiology of Static Exercise. Exerc. Sport Sci. Rev. Ser. 1986, 14, 1–44. [Google Scholar] [CrossRef]
- Sawka, M.N. Physiology of Upper-Body Exercise. Exerc. Sport Sci. Rev. Ser. 1986, 14, 175–211. [Google Scholar] [CrossRef]
- Rowell, L.B.; Murray, J.A.; Brengelmann, G.L.; Kraning, K.K. Human Cardiovascular Adjustments to Rapid Changes in Skin Temperature During Exercise. Circ. Res. 1969, 24, 711. [Google Scholar] [CrossRef]
- Watanabe, K.; Stohr, E.J.; Akiyama, K.; Watanabe, S.; Gonzalez-Alonso, J. Dehydration reduces stroke volume and cardiac output during exercise because of impaired cardiac filling and venous return, not left ventricular function. Physiol. Rep. 2020, 8, e14433. [Google Scholar] [CrossRef] [PubMed]
- Posch, A.M.; Luippold, A.J.; Mitchell, K.M.; Bradbury, K.E.; Kenefick, R.W.; Cheuvront, S.N.; Charkoudian, N. Sympathetic neural and hemodynamic responses to head-up tilt during isoosmotic and hyperosmotic hypovolemia. J. Neurophysiol. 2017, 118, 2232–2237. [Google Scholar] [CrossRef] [PubMed]
- Schiller, A.M.; Howard, J.T.; Convertino, V.A. The physiology of blood loss and shock: New insights from a human laboratory model of hemorrhage. Exp. Biol. Med. 2017, 242, 874–883. [Google Scholar] [CrossRef] [PubMed]
- Crandall, C.G.; Rickards, C.A.; Johnson, B.D. Impact of environmental stressors on tolerance to hemorrhage in humans. Am. J. Physiol.-Regul. Integr. Comp. Physiol. 2019, 316, R88–R100. [Google Scholar] [CrossRef] [PubMed]
- Convertino, V.A.; Wirt, M.D.; Glenn, J.F.; Lein, B.C. The Compensatory Reserve for Early and Accurate Prediction of Hemodynamic Compromise: A Review of the Underlying Physiology. Shock 2016, 45, 580–590. [Google Scholar] [CrossRef] [PubMed]
- Gagnon, D.; Schlader, Z.J.; Adams, A.; Rivas, E.; Mulligan, J.; Grudic, G.Z.; Convertino, V.A.; Howard, J.T.; Crandall, C.G. The Effect of Passive Heat Stress and Exercise-Induced Dehydration on the Compensatory Reserve During Simulated Hemorrhage. Shock 2016, 46, 74–82. [Google Scholar] [CrossRef] [PubMed]
- Stewart, C.L.; Nawn, C.D.; Mulligan, J.; Grudic, G.Z.; Moulton, S.L.; Convertino, V.A. Compensatory Reserve for Early and Accurate Prediction of Hemodynamic Compromise: Case Studies for Clinical Utility in Acute Care and Physical Performance. J. Spec. Oper. Med. 2016, 16, 6–13. [Google Scholar]
- Mulder, M.B.; Eidelson, S.A.; Buzzelli, M.D.; Gross, K.R.; Batchinsky, A.I.; Convertino, V.A.; Schulman, C.I.; Namias, N.; Proctor, K.G. Exercise-Induced Changes in Compensatory Reserve and Heart Rate Complexity. Aerosp. Med. Hum. Perform. 2019, 90, 1009–1015. [Google Scholar] [CrossRef]
- Tamura, T.; Maeda, Y.; Sekine, M.; Yoshida, M. Wearable Photoplethysmographic Sensors-Past and Present. Electronics 2014, 3, 282–302. [Google Scholar] [CrossRef]
- Jeong, I.C.; Yoon, H.; Kang, H.; Yeom, H. Effects of Skin Surface Temperature on Photoplethysmograph. J. Healthc. Eng. 2014, 5, 429–438. [Google Scholar] [CrossRef]
- Fine, J.; Branan, K.L.; Rodriguez, A.J.; Boonya-ananta, T.; Ajmal; Ramella-Roman, J.C.; McShane, M.J.; Cote, G.L. Sources of Inaccuracy in Photoplethysmography for Continuous Cardiovascular Monitoring. Biosensors 2021, 11, 126. [Google Scholar] [CrossRef]
- Muza, S.R. Wearable physiological sensors and real-time algorithms for detection of acute mountain sickness. J. Appl. Physiol. 2018, 124, 557–563. [Google Scholar] [CrossRef]
- Zia, J.; Kimball, J.; Rolfes, C.; Hahn, J.O.; Inan, O.T. Enabling the assessment of trauma-induced hemorrhage via smart wearable systems. Sci. Adv. 2020, 6. [Google Scholar] [CrossRef]
- Etemadi, M.; Inan, O.T.; Heller, J.A.; Hersek, S.; Klein, L.; Roy, S. A Wearable Patch to Enable Long-Term Monitoring of Environmental, Activity and Hemodynamics Variables. IEEE Trans. Biomed. Circuits Syst. 2016, 10, 280–288. [Google Scholar] [CrossRef]
- Ganti, V.G.; Carek, A.M.; Nevius, B.N.; Heller, J.A.; Etemadi, M.; Inan, O.T. Wearable Cuff-Less Blood Pressure Estimation at Home via Pulse Transit Time. IEEE J. Biomed. Health Inform. 2021, 25, 1926–1937. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.S.; Schwartz, C.J.; Levinson, G.E.; Ettinger, P.O. Systolic Time Intervals as Measures of Contractile State of Left Ventricular Myocardium in Man. Circulation 1972, 46, 559. [Google Scholar] [CrossRef] [PubMed]
- Lewis, R.P.; Rittgers, S.E.; Forester, W.F.; Boudoulas, H. Critical-Review of Systolic-Time Intervals. Circulation 1977, 56, 146–158. [Google Scholar] [CrossRef]
- Tavakolian, K.; Dumont, G.A.; Houlton, G.; Blaber, A.P. Precordial Vibrations Provide Noninvasive Detection of Early-Stage Hemorrhage. Shock 2014, 41, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Inan, O.T.; Pouyan, M.B.; Javaid, A.Q.; Dowling, S.; Etemadi, M.; Dorier, A.; Heller, J.A.; Bicen, A.O.; Roy, S.; De Marco, T.; et al. Novel Wearable Seismocardiography and Machine Learning Algorithms Can Assess Clinical Status of Heart Failure Patients. Circ. Heart Fail. 2018, 11, e004313. [Google Scholar] [CrossRef] [PubMed]
- Shandhi, M.M.H.; Hersek, S.; Fan, J.; Sander, E.; De Marco, T.; Heller, J.A.; Etemadi, M.; Klein, L.; Inan, O.T. Wearable Patch-Based Estimation of Oxygen Uptake and Assessment of Clinical Status during Cardiopulmonary Exercise Testing in Patients With Heart Failure. J. Card. Fail. 2020, 26, 948–958. [Google Scholar] [CrossRef] [PubMed]
- Lin, D.J.; Kimball, J.P.; Zia, J.S.; Ganti, V.G.; Inan, O.T. Reducing the Impact of External Vibrations on Fiducial Point Detection in Seismocardiogram Signals. IEEE Trans. Biomed. Eng. 2022, 69, 176–185. [Google Scholar] [CrossRef] [PubMed]
- Javaid, A.Q.; Ashouri, H.; Dorier, A.; Etemadi, M.; Heller, J.A.; Roy, S.; Inan, O.T. Quantifying and Reducing Motion Artifacts in Wearable Seismocardiogram Measurements During Walking to Assess Left Ventricular Health. IEEE Trans. Biomed. Eng. 2017, 64, 1277–1286. [Google Scholar] [CrossRef]
- Vest, A.N.; Poian, G.D.; Li, Q.; Liu, C.; Nemati, S.; Shah, A.; Clifford, G.D. Cliffordlab/PhysioNet-Cardiovascular-Signal-Toolbox: PhysioNet-Cardiovascular-Signal-Toolbox 1.0.2. Zenodo 2019. [Google Scholar] [CrossRef]
- Zia, J.; Kimball, J.; Hersek, S.; Shandhi, M.M.H.; Semiz, B.; Inan, O.T. A Unified Framework for Quality Indexing and Classification of Seismocardiogram Signals. IEEE J. Biomed. Health Inform. 2020, 24, 1080–1092. [Google Scholar] [CrossRef]
- Yang, C.X.; Tavassolian, N. Motion Artifact Cancellation of Seismocardiographic Recording From Moving Subjects. IEEE Sens. J. 2016, 16, 5702–5708. [Google Scholar] [CrossRef]
- Yang, C.X.; Tavassolian, N. Combined Seismo- and Gyro-Cardiography: A More Comprehensive Evaluation of Heart-Induced Chest Vibrations. IEEE J. Biomed. Health Inform. 2018, 22, 1466–1475. [Google Scholar] [CrossRef]
- Shandhi, M.M.H.; Semiz, B.; Hersek, S.; Goller, N.; Ayazi, F.; Inan, O.T. Performance Analysis of Gyroscope and Accelerometer Sensors for Seismocardiography-Based Wearable Pre-Ejection Period Estimation. IEEE J. Biomed. Health Inform. 2019, 23, 2365–2374. [Google Scholar] [CrossRef]
- Yang, C.X.; Tavassolian, N. An Independent Component Analysis Approach to Motion Noise Cancelation of Cardio-Mechanical Signals. IEEE Trans. Biomed. Eng. 2019, 66, 784–793. [Google Scholar] [CrossRef]
- Kim, B.S.; Yoo, S.K. Motion artifact reduction in photoplethysmography using independent component analysis. IEEE Trans. Biomed. Eng. 2006, 53, 566–568. [Google Scholar] [CrossRef]
- Yousefi, R.; Nourani, M.; Ostadabbas, S.; Panahi, I. A Motion-Tolerant Adaptive Algorithm for Wearable Photoplethysmographic Biosensors. IEEE J. Biomed. Health Inform. 2014, 18, 670–681. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.L.; Pi, Z.Y.; Liu, B.Y. TROIKA: A General Framework for Heart Rate Monitoring Using Wrist-Type Photoplethysmographic Signals During Intensive Physical Exercise. IEEE Trans. Biomed. Eng. 2015, 62, 522–531. [Google Scholar] [CrossRef] [PubMed]
- Di Rienzo, M.; Vaini, E.; Castiglioni, P.; Merati, G.; Meriggi, P.; Parati, G.; Faini, A.; Rizzo, F. Wearable seismocardiography: Towards a beat-by-beat assessment of cardiac mechanics in ambulant subjects. Auton. Neurosci. Basic Clin. 2013, 178, 50–59. [Google Scholar] [CrossRef]
- An, X.; Stylios, G.K. Comparison of Motion Artefact Reduction Methods and the Implementation of Adaptive Motion Artefact Reduction in Wearable Electrocardiogram Monitoring. Sensors 2020, 20, 1468. [Google Scholar] [CrossRef]
- Hesar, H.D.; Mohebbi, M. ECG Denoising Using Marginalized Particle Extended Kalman Filter With an Automatic Particle Weighting Strategy. IEEE J. Biomed. Health Inform. 2017, 21, 635–644. [Google Scholar] [CrossRef]
- Reyes, B.A.; Posada-Quintero, H.F.; Bales, J.R.; Clement, A.L.; Pins, G.D.; Swiston, A.; Riistama, J.; Florian, J.P.; Shykoff, B.; Qin, M.; et al. Novel Electrodes for Underwater ECG Monitoring. IEEE Trans. Biomed. Eng. 2014, 61, 1863–1876. [Google Scholar] [CrossRef]
- Noh, Y.; Bales, J.R.; Reyes, B.A.; Molignano, J.; Clement, A.L.; Pins, G.D.; Florian, J.P.; Chon, K.H. Novel Conductive Carbon Black and Polydimethlysiloxane ECG Electrode: A Comparison with Commercial Electrodes in Fresh, Chlorinated, and Salt Water. Ann. Biomed. Eng. 2016, 44, 2464–2479. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.D.; Chen, Y.Q.; Hao, S.J.; Peng, X.H.; Hu, L.S. Deep learning for sensor-based activity recognition: A survey. Pattern Recognit. Lett. 2019, 119, 3–11. [Google Scholar] [CrossRef]
- An, S.; Medda, A.; Sawka, M.N.; Hutto, C.J.; Millard-Stafford, M.L.; Appling, S.; Richardson, K.L.S.; Inan, O.T. AdaptNet: Human Activity Recognition via Bilateral Domain Adaptation Using Semi-Supervised Deep Translation Networks. IEEE Sens. J. 2021, 21, 20398–20411. [Google Scholar] [CrossRef]
- Karantonis, D.M.; Narayanan, M.R.; Mathie, M.; Lovell, N.H.; Celler, B.G. Implementation of a real-time human movement classifier using a triaxial accelerometer for ambulatory monitoring. IEEE Trans. Inf. Technol. Biomed. 2006, 10, 156–167. [Google Scholar] [CrossRef] [PubMed]
- Gyllensten, I.C.; Bonomi, A.G. Identifying Types of Physical Activity With a Single Accelerometer: Evaluating Laboratory-trained Algorithms in Daily Life. IEEE Trans. Biomed. Eng. 2011, 58, 2656–2663. [Google Scholar] [CrossRef]
- Bonomi, A.G.; Goris, A.H.C.; Yin, B.; Westerterp, K.R. Detection of Type, Duration, and Intensity of Physical Activity Using an Accelerometer. Med. Sci. Sports Exerc. 2009, 41, 1770–1777. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.D.; San-Segundo, R.; Pardo, J.M. Feature extraction for robust physical activity recognition. Hum. Cent. Comput. Inf. Sci. 2017, 7, 16. [Google Scholar] [CrossRef]
- Bao, L.; Intille, S.S. Activity Recognition from User-Annotated Acceleration Data. In Pervasive Computing, Proceedings; Ferscha, A., Mattern, F., Eds.; Lecture Notes in Computer Science; Springer: Berlin/Heidelberg, Germany, 2004; Volume 3001, pp. 1–17. [Google Scholar]
- Bourke, A.K.; O’Brien, J.V.; Lyons, G.M. Evaluation of a threshold-based tri-axial accelerometer fall detection algorithm. Gait Posture 2007, 26, 194–199. [Google Scholar] [CrossRef] [PubMed]
- Bouarfa, L.; Atallah, L.; Kwasnicki, R.M.; Pettitt, C.; Frost, G.; Yang, G.Z. Predicting Free-Living Energy Expenditure Using a Miniaturized Ear-Worn Sensor: An Evaluation Against Doubly Labeled Water. IEEE Trans. Biomed. Eng. 2014, 61, 566–575. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Ohtaki, Y.; Susumago, M.; Suzuki, A.; Sagawa, K.; Nagatomi, R.; Inooka, H. Automatic classification of ambulatory movements and evaluation of energy consumptions utilizing accelerometers and a barometer. Microsyst. Technol.-Micro-Nanosyst. Inf. Storage Processing Syst. 2005, 11, 1034–1040. [Google Scholar] [CrossRef]
- Sazonov, E.; Hegde, N.; Browning, R.C.; Melanson, E.L.; Sazonova, N.A. Posture and Activity Recognition and Energy Expenditure Estimation in a Wearable Platform. IEEE J. Biomed. Health Inform. 2015, 19, 1339–1346. [Google Scholar] [CrossRef]
- Altini, M.; Penders, J.; Vullers, R.; Amft, O. Automatic Heart Rate Normalization for Accurate Energy Expenditure Estimation An Analysis of Activities of Daily Living and Heart Rate Features. Methods Inf. Med. 2014, 53, 382–388. [Google Scholar] [CrossRef][Green Version]
- Murakami, H.; Kawakami, R.; Nakae, S.; Yamada, Y.; Nakata, Y.; Ohkawara, K.; Sasai, H.; Ishikawa-Takata, K.; Tanaka, S.; Miyachi, M. Accuracy of 12 Wearable Devices for Estimating Physical Activity Energy Expenditure Using a Metabolic Chamber and the Doubly Labeled Water Method: Validation Study. JMIR Mhealth Uhealth 2019, 7, e13938. [Google Scholar] [CrossRef]
- Beltrame, T.; Amelard, R.; Wong, A.; Hughson, R.L. Extracting aerobic system dynamics during unsupervised activities of daily living using wearable sensor machine learning models. J. Appl. Physiol. 2018, 124, 473–481. [Google Scholar] [CrossRef]
- Kenefick, R.W.; Cheuvront, S.N.; Palombo, L.J.; Ely, B.R.; Sawka, M.N. Skin temperature modifies the impact of hypohydration on aerobic performance. J. Appl. Physiol. 2010, 109, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Sawka, M.N.; Cheuvront, S.N.; Kenefick, R.W. High skin temperature and hypohydration impair aerobic performance. Exp. Physiol. 2012, 97, 327–332. [Google Scholar] [CrossRef]
- Texas Instruments: Electrocardiogram (ECG). Electrocardiogram (ECG) Integrated Circuits and Reference Designs. Available online: https://www.ti.com/solution/electrocardiogram-ecg (accessed on 2 December 2021).
- Rogers, J.A.; Someya, T.; Huang, Y.G. Materials and Mechanics for Stretchable Electronics. Science 2010, 327, 1603–1607. [Google Scholar] [CrossRef]
- van der Ster, B.J.P.; Bennis, F.C.; Delhaas, T.; Westerhof, B.E.; Stok, W.J.; van Lieshout, J.J. Support Vector Machine Based Monitoring of Cardio-Cerebrovascular Reserve during Simulated Hemorrhage. Front. Physiol. 2018, 8, 1057. [Google Scholar] [CrossRef] [PubMed]
- Reljin, N.; Zimmer, G.; Malyuta, Y.; Shelley, K.; Mendelson, Y.; Blehar, D.J.; Darling, C.E.; Chon, K.H. Using support vector machines on photoplethysmographic signals to discriminate between hypovolemia and euvolemia. PLoS ONE 2018, 13, e195087. [Google Scholar] [CrossRef] [PubMed]
- Pinsky, M.R.; Clermont, G.; Hravnak, M. Predicting cardiorespiratory instability. Crit. Care 2016, 20, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Ogundele, O.; Clermont, G.; Hravnak, M.; Pinsky, M.R.; Dubrawski, A.W. Dynamic and Personalized Risk Forecast in Step-Down Units Implications for Monitoring Paradigms. Ann. Am. Thorac. Soc. 2017, 14, 384–391. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Dubrawski, A.; Clermont, G.; Hravnak, M.; Pinsky, M.R. Modelling Risk of Cardio-Respiratory Instability as a Heterogeneous Process. AMIA Annu. Symp. Proc. AMIA Symp. 2015, 2015, 1841–1850. [Google Scholar]
- Yoon, J.H.; Jeanselme, V.; Dubrawski, A.; Hravnak, M.; Pinsky, M.R.; Clermont, G. Prediction of hypotension events with physiologic vital sign signatures in the intensive care unit. Crit. Care 2020, 24, 1–9. [Google Scholar] [CrossRef]
- Pandolf, K.B.; Stroschein, L.A.; Drolet, L.L.; Gonzalez, R.R.; Sawka, M.N. Prediction Modeling of Physiological-Responses and Human-Performance in the Heat. Comput. Biol. Med. 1986, 16, 319–329. [Google Scholar] [CrossRef]
- Montain, S.J.; Latzka, W.A.; Sawka, M.N. Fluid replacement recommendations for training in hot weather. Mil. Med. 1999, 164, 502–508. [Google Scholar] [CrossRef] [PubMed]
- Jacklitsch, B.; Williams, W.J.; Musolin, K.; Coca, A.; Kim, J.-H.; Turner, N. NIOSH Criteria for a Recommended Standard: Occupational Exposure to Heat and Hot Environments; U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health: Cincinnati, OH, USA, 2016. [Google Scholar]
- Heat Stress Control and Heat Casualty Management; Technical Bulletin Medical 507/AFPAM 48-152(I); Headquarters, Department of Army and Air Force, Army Publishing Directorate: Fort Belvoir, VA, USA, 2003.
- Cheuvront, S.N.; Kenefick, R.W.; Montain, S.J.; Sawka, M.N. Mechanisms of aerobic performance impairment with heat stress and dehydration. J. Appl. Physiol. 2010, 109, 1989–1995. [Google Scholar] [CrossRef] [PubMed]
- Sawka, M.N.; Latzka, W.A.; Montain, S.J.; Cadarette, B.S.; Kolka, M.A.; Kraning, K.K.; Gonzalez, R.R. Physiologic tolerance to uncompensable heat: Intermittent exercise, field vs laboratory. Med. Sci. Sports Exerc. 2001, 33, 422–430. [Google Scholar] [CrossRef] [PubMed]
- Periard, J.D.; Racinais, S.; Sawka, M.N. Heat adaptation in humans with controlled heart rate heat acclimation. Eur. J. Appl. Physiol. 2021, 121, 1233–1235. [Google Scholar] [CrossRef]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ruggedization Measure | Purpose | Major Challenges | State of the Art | Opportunities for Advancement |
|---|---|---|---|---|
| Signal Quality Indexing | Assess noisy portions of the signal to determine whether they are salvageable for feature extraction | Determining an appropriate comparator (i.e., template) to recognize “good” signals, particularly in changing physiology | [68,69] | Address specific wearable issues: sensor misplacement; realistic varied noise sources such as clothing interference, speech, body movement, fluids, etc. |
| Motion Artifact Removal | Mitigate the effects of noise due to movement of the subject | Tracking physiology during periods of extended motion | [78] (ECG) [76] (PPG) [73] (SCG) | Multimodal, multi-sensor analysis; realistic varied noise sources; sparse estimation; |
| External Vibration Removal | Mitigate the effects of noise from the environment such as from transport vehicles | Semi-periodic in-band noise sources | [79] (ECG) [66] (SCG) | Methods specific to reflectance-mode PPG; noise data from multiple vehicle types; multimodal, multi-sensor analysis |
| Moisture Resistance | Protect sensors and signals from fluid interference (e.g., sweat, blood, mud) | Fluids can block or short sensors and distort signals | [80,81] | Improved packaging; machine learning or signal processing methods for detecting and adjusting to fluid interference |
| Activity Recognition | Provide context for physiological measurements | Large amounts of data required with consistent labeling | [82,83] | Multi-modal and additional domain transfer techniques |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kimball, J.P.; Inan, O.T.; Convertino, V.A.; Cardin, S.; Sawka, M.N. Wearable Sensors and Machine Learning for Hypovolemia Problems in Occupational, Military and Sports Medicine: Physiological Basis, Hardware and Algorithms. Sensors 2022, 22, 442. https://doi.org/10.3390/s22020442
Kimball JP, Inan OT, Convertino VA, Cardin S, Sawka MN. Wearable Sensors and Machine Learning for Hypovolemia Problems in Occupational, Military and Sports Medicine: Physiological Basis, Hardware and Algorithms. Sensors. 2022; 22(2):442. https://doi.org/10.3390/s22020442
Chicago/Turabian StyleKimball, Jacob P., Omer T. Inan, Victor A. Convertino, Sylvain Cardin, and Michael N. Sawka. 2022. "Wearable Sensors and Machine Learning for Hypovolemia Problems in Occupational, Military and Sports Medicine: Physiological Basis, Hardware and Algorithms" Sensors 22, no. 2: 442. https://doi.org/10.3390/s22020442
APA StyleKimball, J. P., Inan, O. T., Convertino, V. A., Cardin, S., & Sawka, M. N. (2022). Wearable Sensors and Machine Learning for Hypovolemia Problems in Occupational, Military and Sports Medicine: Physiological Basis, Hardware and Algorithms. Sensors, 22(2), 442. https://doi.org/10.3390/s22020442