
Inertia Sensors for Measuring Spasticity of the Ankle Plantarflexors Using the Modified Tardieu Scale—A Proof of Concept Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study 1: Relationship between Muscle Onset (i.e., AOR) and Segment Angular Velocity
2.1.1. Participants
- Diagnosis of an adult onset acquired neurological condition affecting the CNS;
- Identified by their treating physiotherapist as having spasticity in their gastrocnemius and soleus, as rated by an X value of ≥ 2;
- Able to provide informed consent to assessment and cooperate with the testing procedure;
- Were ≥ 18 years of age;
- No contraindications to fast passive movement of the affected limb (for example, if non-weight-bearing).
- Severe dystonic movement patterns limiting the completion of the MTS.
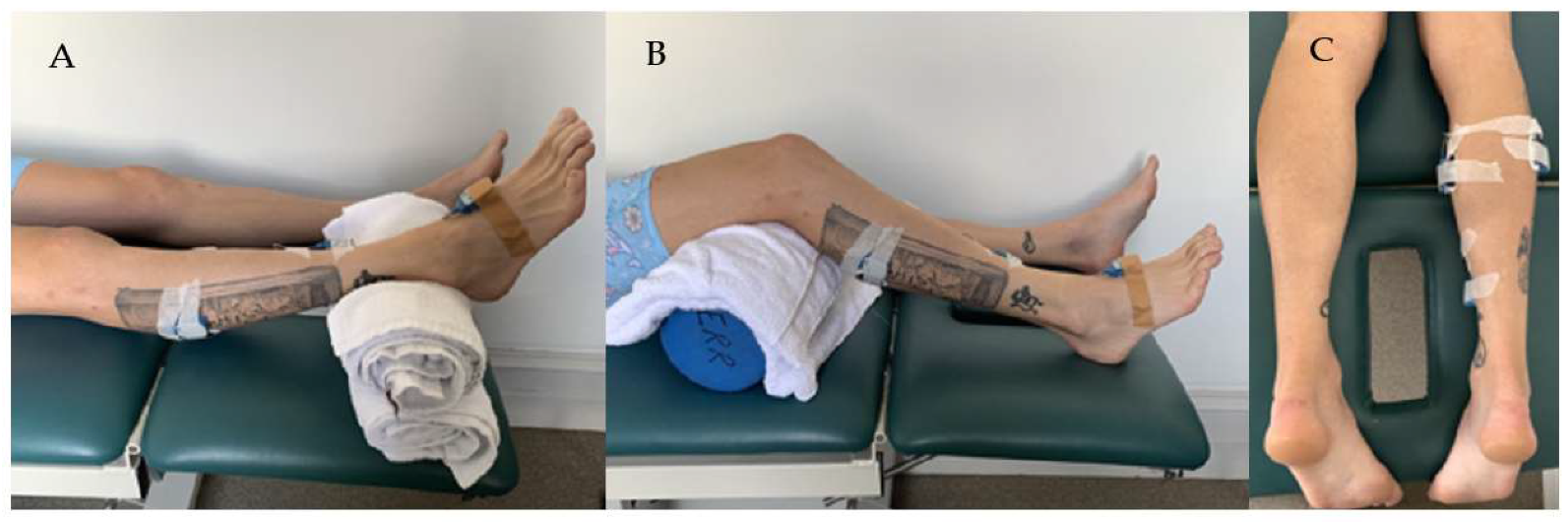
2.1.2. Experimental Setup
2.1.3. Data Collection
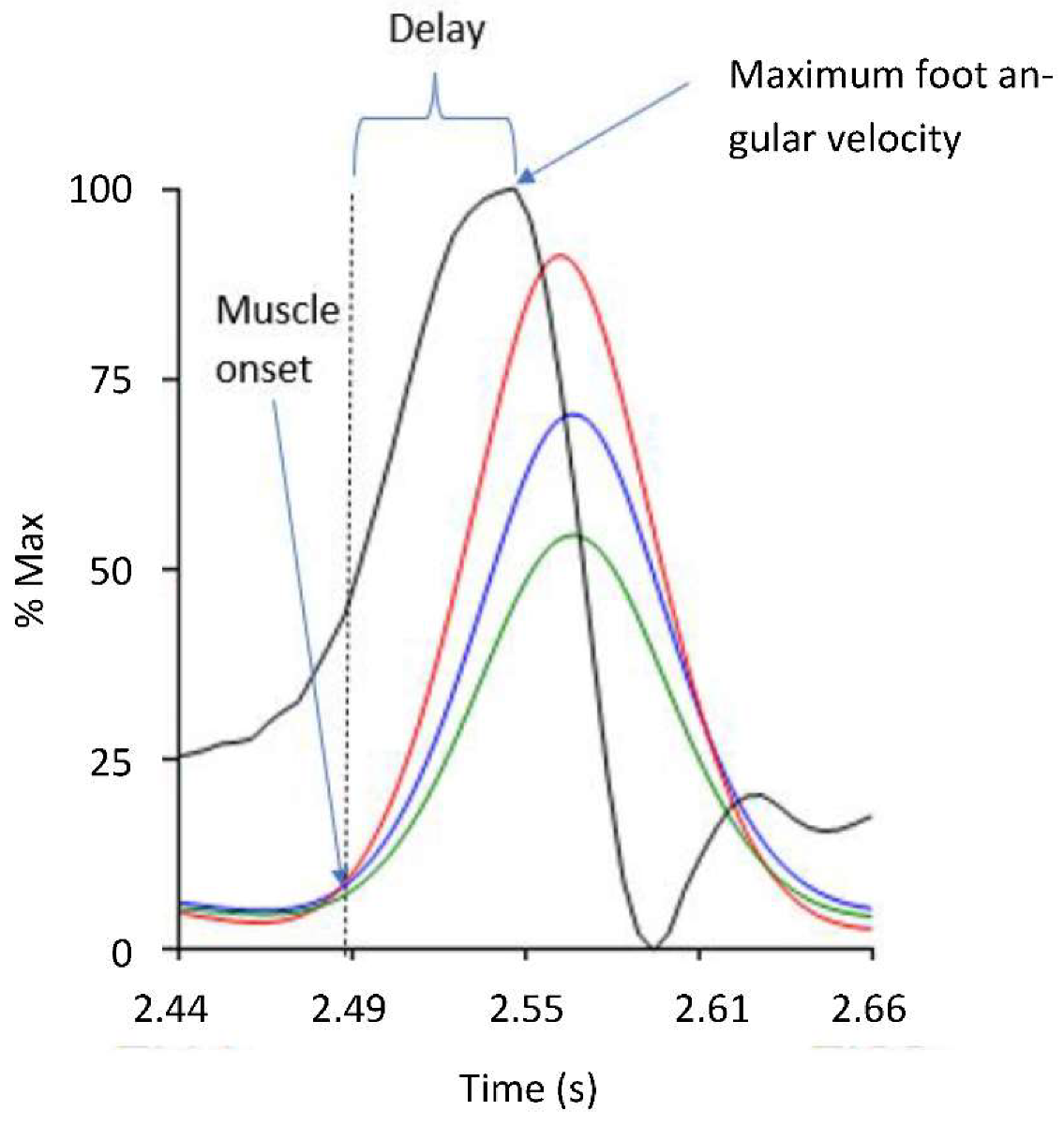
2.1.4. Signal Processing and Outcome Measures
2.2. Study 2: The Use of IMUs to Measure the Angle of Muscle Reaction during the V3 MTS Assessment
2.2.1. Participants
2.2.2. Experimental Setup
2.2.3. Data Collection
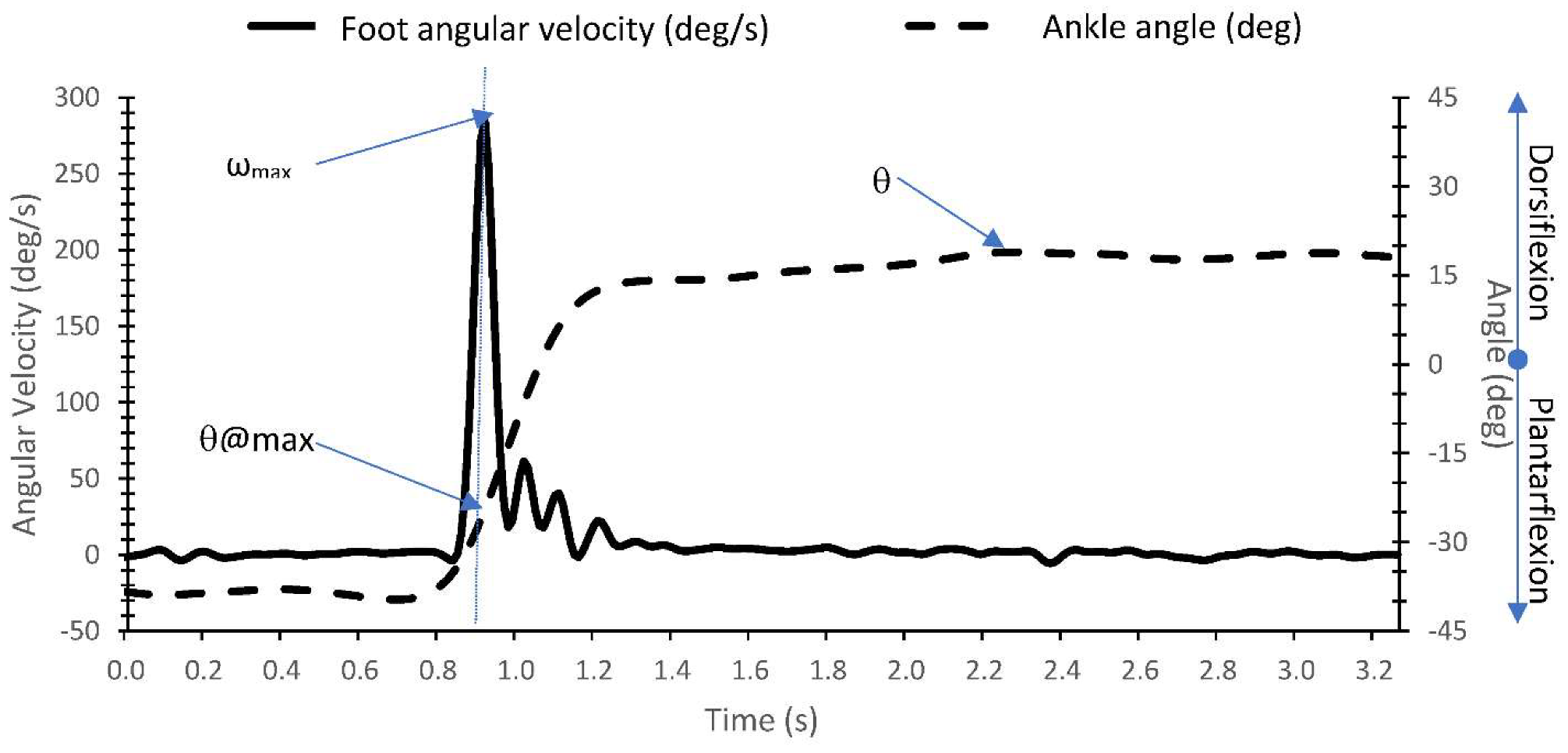
2.2.4. Signal Processing and Outcome Measures
3. Results
3.1. Study 1
3.2. Study 2
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| Abbreviation | Meaning |
| AOR | Angle of muscle reaction (i.e., spastic muscle activation onset) |
| BoNT-A | Botulinum toxin A |
| CI | Confidence interval |
| EMG | Electromyogram |
| ICC | Intraclass correlation |
| IMU | Inertia measuring unit |
| MTS | Modified Tardieu Scale |
| V1 | Slow passive movement during the MTS |
| V3 | Fast passive movement during the MTS |
| Δt | Time delay between spastic muscle activation onset (AOR) and maximum foot angular velocity (s) |
| ωmax | Maximum foot angular velocity (°/s) |
| θ | Maximum dorsiflexion angle (°) |
| θ@max | Angle at maximum angular velocity (°) |
| Δθ | Difference between θ and θ@max (°) |
References
- Lance, J.W. The control of muscle tone, reflexes, and movement: Robert Wartenberg Lecture. Neurology 1980, 30, 1303–1313. [Google Scholar] [CrossRef] [PubMed]
- Singh, P.; Joshua, A.M.; Ganeshan, S.; Suresh, S. Intra-rater reliability of the modified Tardieu scale to quantify spasticity in elbow flexors and ankle plantar flexors in adult stroke subjects. Ann. Indian Acad. Neurol. 2011, 14, 23–26. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.Y.; Lee, A.J.; Shin, K.H. Inter-rater and intra-rater reliability of the Modified Ashworth Scale and the Modified Tardieu Scale: A comparison study. J. Korean Phys. Ther. 2010, 22, 29–33. [Google Scholar]
- Akpinar, P.; Atici, A.; Ozkan, F.U.; Aktas, I.; Kulcu, D.G.; Sari, A.; Durmus, B. Reliability of the Modified Ashworth Scale and Modified Tardieu Scale in patients with spinal cord injuries. Spinal Cord 2017, 55, 944–949. [Google Scholar] [CrossRef] [PubMed]
- Mehrholz, J.; Wagner, K.; Meissner, D.; Grundmann, K.; Zange, C.; Koch, R.; Pohl, M. Reliability of the Modified Tardieu Scale and the Modified Ashworth Scale in adult patients with severe brain injury: A comparison study. Clin. Rehabil. 2005, 19, 751–759. [Google Scholar] [CrossRef]
- Ben-Shabat, E.; Palit, M.; Fini, N.A.; Brooks, C.T.; Winter, A.; Holland, A.E. Intra- and interrater reliability of the Modified Tardieu Scale for the assessment of lower limb spasticity in adults with neurologic injuries. Arch. Phys. Med. Rehabil. 2013, 94, 2494–2501. [Google Scholar] [CrossRef]
- Patrick, E.; Ada, L. The Tardieu Scale differentiates contracture from spasticity whereas the Ashworth Scale is confounded by it. Clin. Rehabil. 2006, 20, 173–182. [Google Scholar] [CrossRef]
- Ang, W.S.; Geyer, H.; Chen, I.M.; Ang, W.T. Objective Assessment of Spasticity With a Method Based on a Human Upper Limb Model. IEEE Trans. Neural. Syst. Rehabil. Eng. 2018, 26, 1414–1423. [Google Scholar] [CrossRef]
- Kim, J.Y.; Park, G.; Lee, S.A.; Nam, Y. Analysis of Machine Learning-Based Assessment for Elbow Spasticity Using Inertial Sensors. Sensors 2020, 20, 1622. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Tang, X.; Zhu, X.; Gao, X.; Chen, X.; Chen, X. A Regression-Based Framework for Quantitative Assessment of Muscle Spasticity Using Combined EMG and Inertial Data From Wearable Sensors. Front. Neurosci. 2019, 13, 398. [Google Scholar] [CrossRef] [Green Version]
- Weizman, Y.; Tirosh, O.; Fuss, F.K.; Tan, A.M.; Rutz, E. Recent State of Wearable IMU Sensors Use in People Living with Spasticity: A Systematic Review. Sensprs 2022, 22, 1791. [Google Scholar] [CrossRef] [PubMed]
- Aleksic, A.; Popovic, D.B. New scale for assessing spasticity based on the pendulum test. Comput. Methods Biomech. Biomed. Engin. 2022, 25, 593–602. [Google Scholar] [CrossRef]
- Jim, R.; David, L.; Michael, W. Whittle’s Gait Analysis, 5th ed.; Churchill Livingstone, Elsevier: Amsterdam, The Netherlands, 2012. [Google Scholar]
- Nalysnyk, L.; Papapetropoulos, S.; Rotella, P.; Simeone, J.C.; Alter, K.E.; Esquenazi, A. OnabotulinumtoxinA muscle injection patterns in adult spasticity: A systematic literature review. BMC Neurol. 2013, 13, 118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van den Noort, J.C.; Scholtes, V.A.; Harlaar, J. Evaluation of clinical spasticity assessment in cerebral palsy using inertial sensors. Gait Posture 2009, 30, 138–143. [Google Scholar] [CrossRef] [PubMed]
- Lynn, B.O.; Erwin, A.; Guy, M.; Herman, B.; Davide, M.; Ellen, J.; Anne, C.; Kaat, D. Comprehensive quantification of the spastic catch in children with cerebral palsy. Res. Dev. Disabil. 2013, 34, 386–396. [Google Scholar] [CrossRef]
- Choi, S.; Shin, Y.B.; Kim, S.Y.; Kim, J. A novel sensor-based assessment of lower limb spasticity in children with cerebral palsy. J. Neuroeng. Rehabil. 2018, 15, 45. [Google Scholar] [CrossRef] [Green Version]
- Klausler, M.; Speth, B.M.; Brunner, R.; Tirosh, O.; Camathias, C.; Rutz, E. Long-term follow-up after tibialis anterior tendon shortening in combination with Achilles tendon lengthening in spastic equinus in cerebral palsy. Gait Posture 2017, 58, 457–462. [Google Scholar] [CrossRef]
- Mahmoudzadeh, A.; Nakhostin Ansari, N.; Naghdi, S.; Sadeghi-Demneh, E.; Motamedzadeh, O.; Shaw, B.S.; Shariat, A.; Shaw, I. Effect of Ankle Plantar Flexor Spasticity Level on Balance in Patients with Stroke: Protocol for a Cross-Sectional Study. JMIR Res. Protoc. 2020, 9, e16045. [Google Scholar] [CrossRef]
- Rutz, E.; Baker, R.; Tirosh, O.; Romkes, J.; Haase, C.; Brunner, R. Tibialis anterior tendon shortening in combination with Achilles tendon lengthening in spastic equinus in cerebral palsy. Gait Posture 2011, 33, 152–157. [Google Scholar] [CrossRef]
- Williams, G.; Banky, M.; Olver, J. Ankle Plantarflexor Spasticity Does Not Restrict the Recovery of Ankle Plantarflexor Strength or Ankle Power Generation for Push-Off during Walking Following Traumatic Brain Injury. J. Head Trauma Rehabil. 2016, 31, E52–E58. [Google Scholar] [CrossRef]
- Merletti, R.; Hermens, H. Introduction to the special issue on the SENIAM European Concerted Action. J. Electromyogr. Kinesiol. 2000, 10, 283–286. [Google Scholar] [CrossRef]
- Boyd, R.N.; Graham, K.H. Objective measurement of clinical findings in the use of botulinum toxin type A for the management of children with cerebral palsy. Eur. J. Neurol. 1999, 6, S23–S35. [Google Scholar] [CrossRef]
- Abhayasinghe, N.; Murray, I.; Sharif Bidabadi, S. Validation of Thigh Angle Estimation Using Inertial Measurement Unit Data against Optical Motion Capture Systems. Sensors 2019, 19, 596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bar-On, L.; Aertbelien, E.; Wambacq, H.; Severijns, D.; Lambrecht, K.; Dan, B.; Huenaerts, C.; Bruyninckx, H.; Janssens, L.; Van Gestel, L.; et al. A clinical measurement to quantify spasticity in children with cerebral palsy by integration of multidimensional signals. Gait Posture 2013, 38, 141–147. [Google Scholar] [CrossRef]
- Banky, M.; Clark, R.A.; Mentiplay, B.F.; Olver, J.H.; Kahn, M.B.; Williams, G. Toward Accurate Clinical Spasticity Assessment: Validation of Movement Speed and Joint Angle Assessments Using Smartphones and Camera Tracking. Arch. Phys. Med. Rehabil. 2019, 100, 1482–1491. [Google Scholar] [CrossRef]
- Banky, M.; Clark, R.A.; Pua, Y.H.; Mentiplay, B.F.; Olver, J.H.; Williams, G. Inter- and intra-rater variability of testing velocity when assessing lower limb spasticity. J. Rehabil. Med. 2019, 51, 54–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burridge, J.H.; Wood, D.E.; Hermens, H.J.; Voerman, G.E.; Johnson, G.R.; van Wijck, F.; Platz, T.; Gregoric, M.; Hitchcock, R.; Pandyan, A.D. Theoretical and methodological considerations in the measurement of spasticity. Disabil. Rehabil. 2005, 27, 69–80. [Google Scholar] [CrossRef] [PubMed]
- Platz, T.; Eickhof, C.; Nuyens, G.; Vuadens, P. Clinical scales for the assessment of spasticity, associated phenomena, and function: A systematic review of the literature. Disabil. Rehabil. 2005, 27, 7–18. [Google Scholar] [CrossRef]
- Banky, M.; Clark, R.A.; Mentiplay, B.F.; Olver, J.H.; Williams, G. Clinical spasticity assessment using the Modified Tardieu Scale does not reflect joint angular velocity or range of motion during walking: Assessment tool implications. J. Rehabil. Med. 2021, 53, jrm00137. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MTS Test | Med Gastroc Δt (s) | Lat Gastroc Δt (s) | Soleus Δt (s) | Angular Velocity ωmax (°/s) |
|---|---|---|---|---|
| Gastrocnemius | 0.049 ± 0.022 (0.020–0.080) | 0.049 ± 0.020 (0.010–0.080) | 0.032 ± 0.075 (0.020–0.120) | 452.5 ± 70.9 (325–608) |
| Soleus | 0.046 ± 0.026 (0.020–0.100) | 558.6 ± 72.8 (440–726) |
| MTS Test | ωmax (deg/sec) | θ@max (deg) | θ (deg) | Δθ (deg) |
|---|---|---|---|---|
| Gastrocnemius | 430.3 ± 90.4 (262.7–612.4) | −16.1 ± 8.7 (−35.0–2.8) | 12.3 ± 8.3 (−1.0–34.7) | 28.4 ± 10.9 (14.7–55.9) |
| Soleus | 439.9 ± 74.5 (260.4–575.6) | −10.9 ± 8.3 (−24.6–2.5) | 17.4 ± 8.6 (1.2–33.9) | 28.2 ± 11.4 (10.6–47.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Banky, M.; Williams, G.; Davey, R.; Tirosh, O. Inertia Sensors for Measuring Spasticity of the Ankle Plantarflexors Using the Modified Tardieu Scale—A Proof of Concept Study. Sensors 2022, 22, 5151. https://doi.org/10.3390/s22145151
Banky M, Williams G, Davey R, Tirosh O. Inertia Sensors for Measuring Spasticity of the Ankle Plantarflexors Using the Modified Tardieu Scale—A Proof of Concept Study. Sensors. 2022; 22(14):5151. https://doi.org/10.3390/s22145151
Chicago/Turabian StyleBanky, Megan, Gavin Williams, Rebecca Davey, and Oren Tirosh. 2022. "Inertia Sensors for Measuring Spasticity of the Ankle Plantarflexors Using the Modified Tardieu Scale—A Proof of Concept Study" Sensors 22, no. 14: 5151. https://doi.org/10.3390/s22145151
APA StyleBanky, M., Williams, G., Davey, R., & Tirosh, O. (2022). Inertia Sensors for Measuring Spasticity of the Ankle Plantarflexors Using the Modified Tardieu Scale—A Proof of Concept Study. Sensors, 22(14), 5151. https://doi.org/10.3390/s22145151