
Development of an Exoskeleton Platform of the Finger for Objective Patient Monitoring in Rehabilitation

 ,
,  , ,
, ,
Abstract
:1. Introduction
- We extended the exoskeleton by Dickmann et al. [18] to incorporate a Bluetooth remote control and connection to a newly developed mobile application.
- The application enables adaptive, individual control and is enhanced by two games to motivate patients for longer therapy sessions and record objective data.
- We performed a small patient study with three patients and tracked their longitudinal progress over six weeks; we present the results.
- We compare the results of the patient to the subject study from Dickmann et al. [18].
2. Materials and Methods
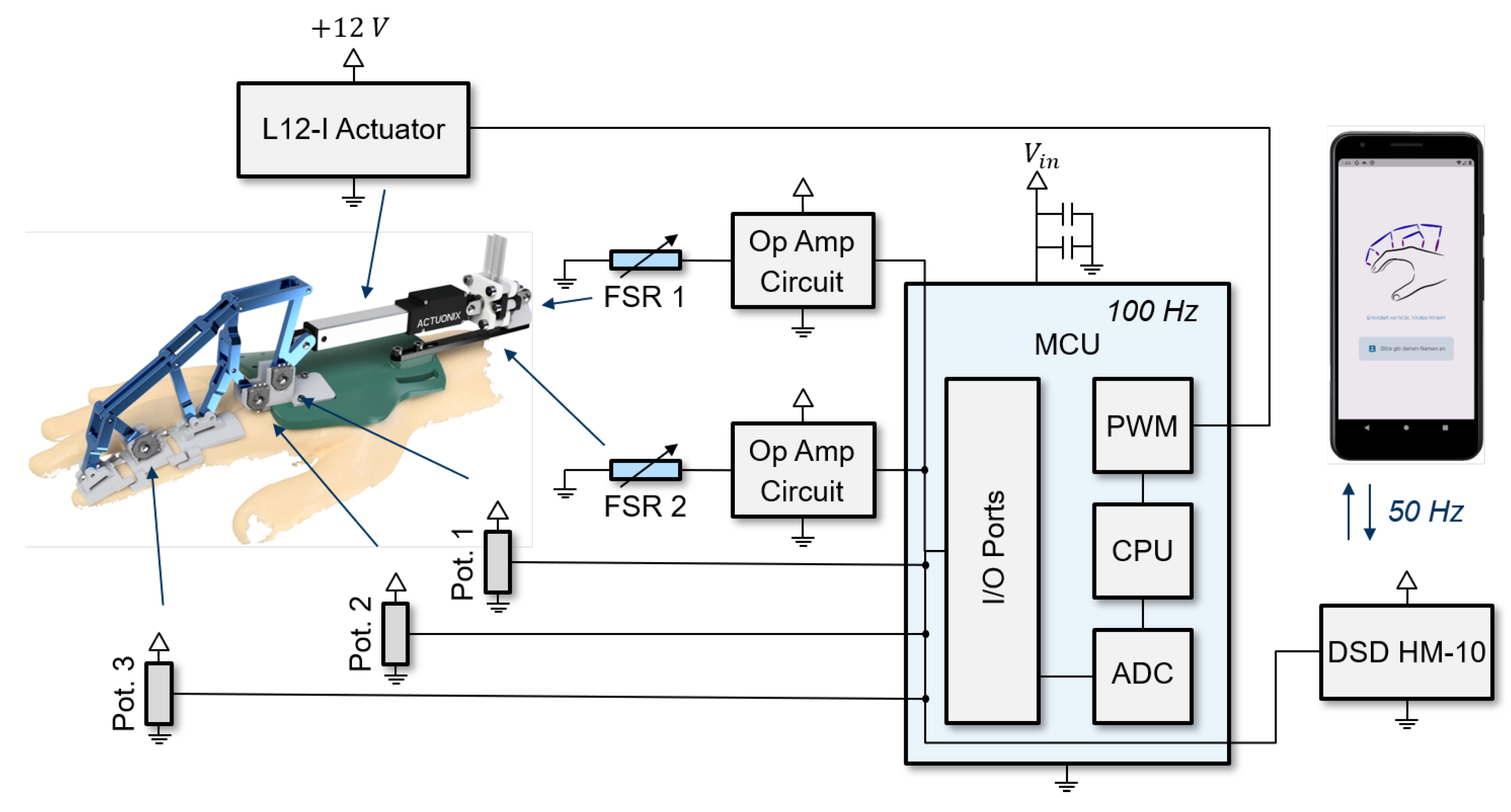
2.1. Mechatronic System
2.2. Exoskeleton Framework
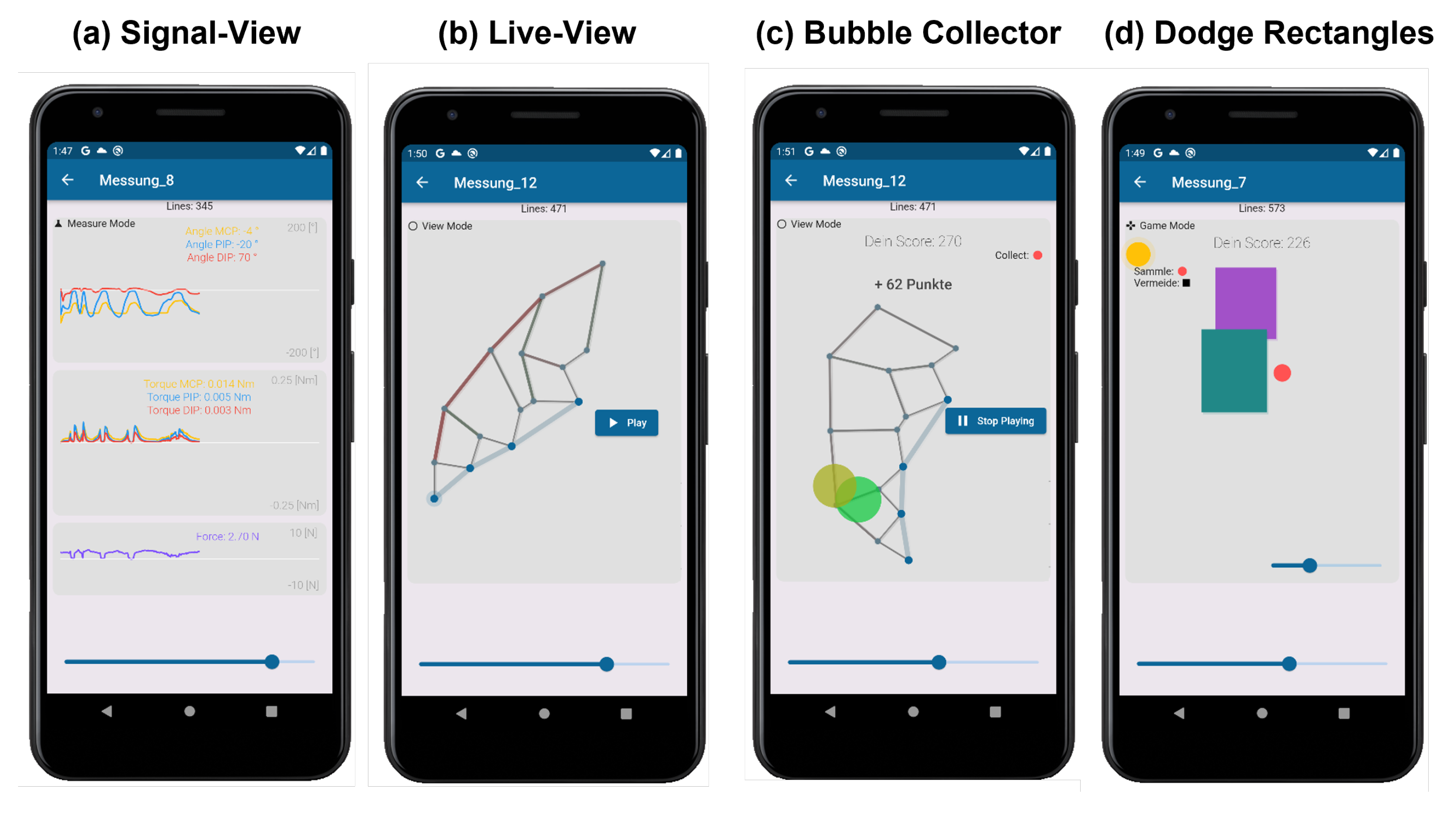
2.3. Application Details
2.4. Application Games in the Context of Hand Rehabilitation
2.5. Implementation of Clinical Studies
3. Results
3.1. Demographics
3.2. Accompanying Measurements
3.3. Patient-Reported Outcome Measures (PROMS)
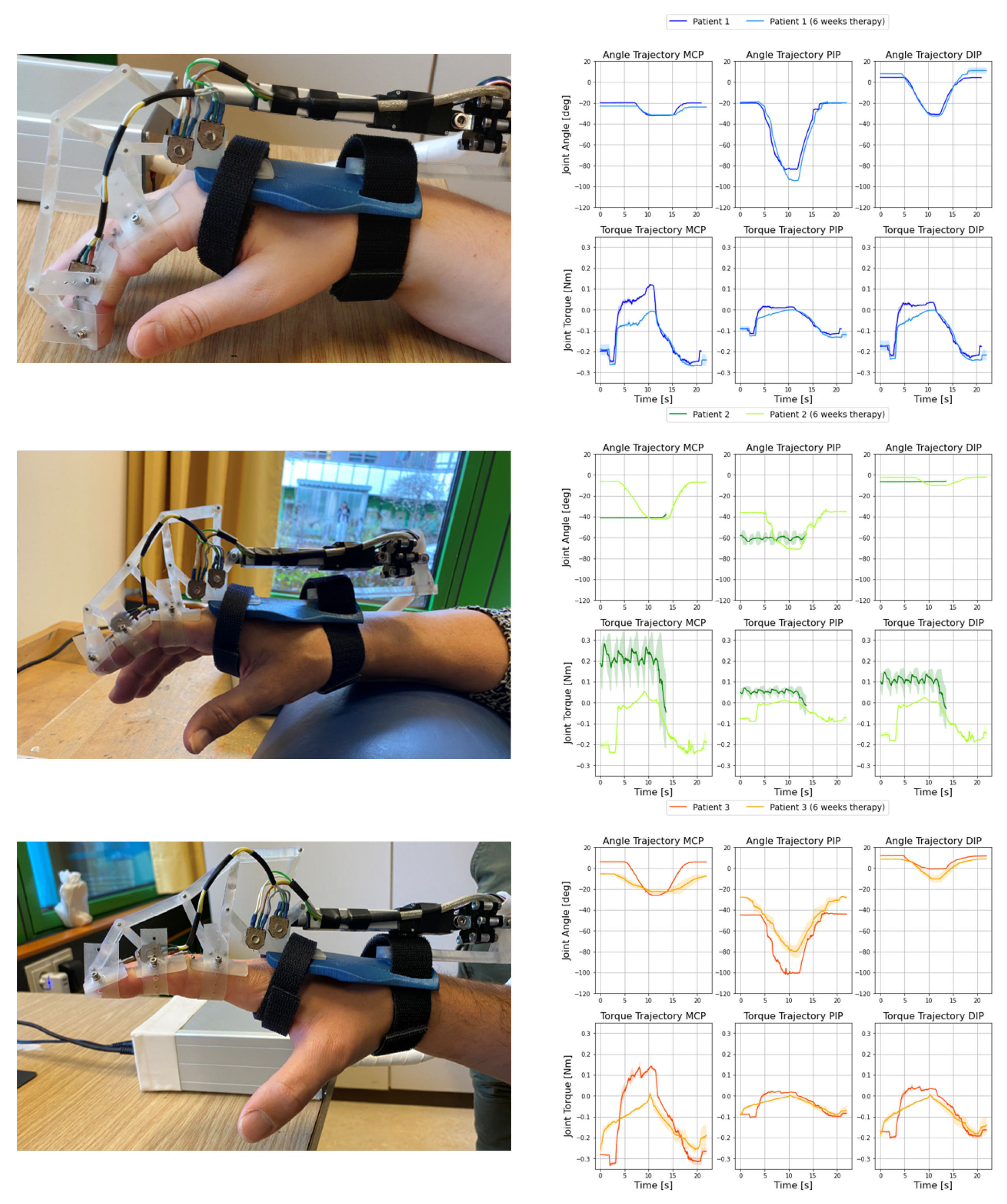
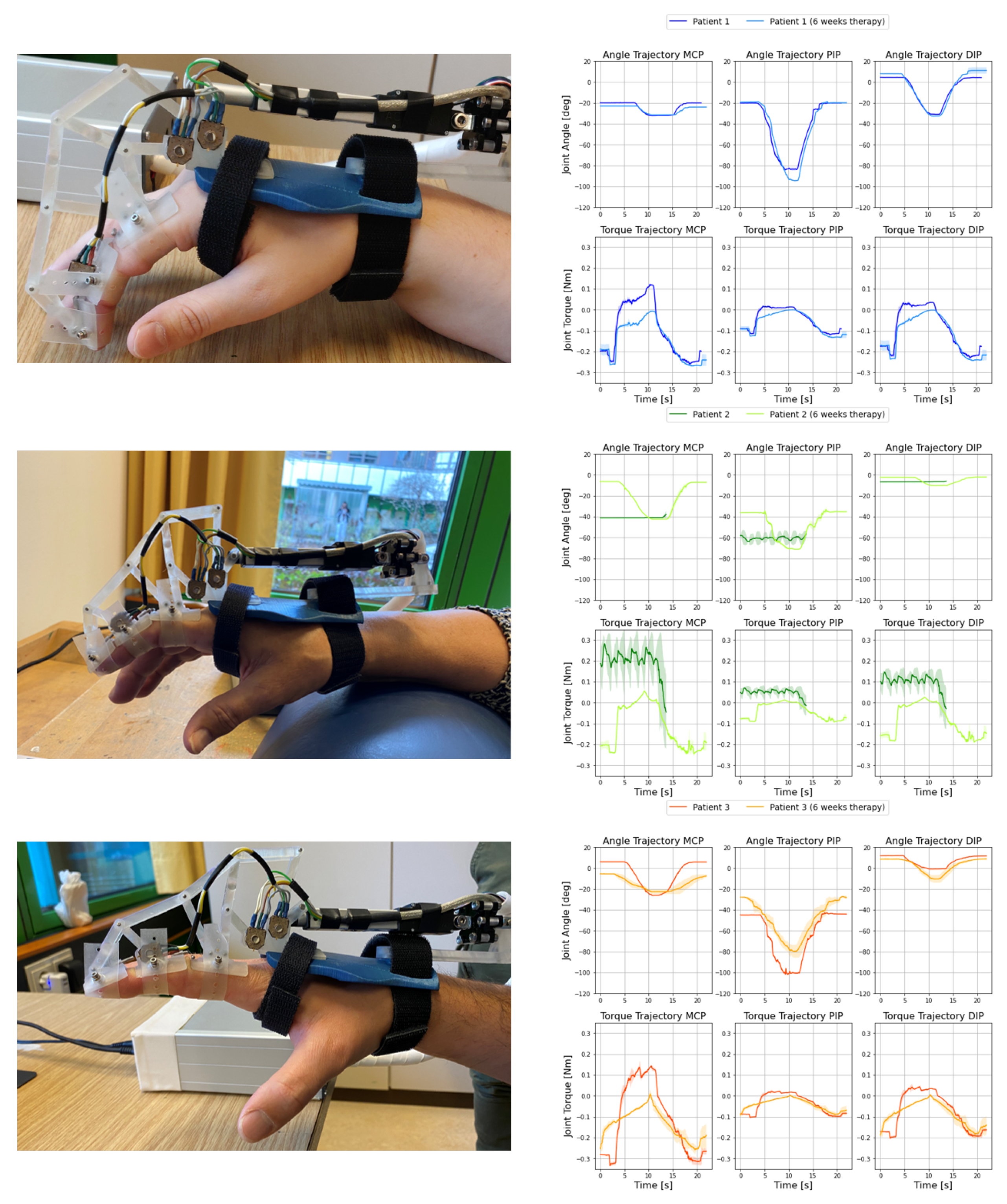
3.4. Exoskeleton Measurements
4. Discussion
4.1. Applicability of the Exoskeleton System
4.2. Applicability of Gamification in Rehabilitation
4.3. Evaluation of Exoskeleton Measurements
4.4. Comparison to Healthy Subjects
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CRPS | Complex regional pain syndrome |
| MCP | metacarpophalangeal joint |
| PIP | proximal interphalangeal joint |
| DIP | distal interphalangeal joint |
| MCU | microcontroller unit |
| PWM | pulse-width modulation |
| CPU | central processing unit |
| ADC | analog-to-digital converter |
| FSR | force-sensing resistor |
| PROMS | patient-reported outcome measures |
| MDR | medical device regulation |
References
- Birch, B.; Haslam, E.; Heerah, I.; Dechev, N.; Park, E.J. Design of a Continuous Passive and Active Motion Device for Hand Rehabilitation. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Vancouver, BC, Canada, 20–24 August 2008; Volume 2008, pp. 4306–4309. [Google Scholar] [CrossRef]
- Wang, J.; Li, J.; Zhang, Y.; Wang, S. Design of an exoskeleton for index finger rehabilitation. In Proceedings of the 31st Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Minneapolis, MN, USA, 3–6 September 2009; pp. 5957–5960. [Google Scholar] [CrossRef]
- Heo, P.; Gu, G.M.; Lee, S.J.; Rhee, K.; Kim, J. Current hand exoskeleton technologies for rehabilitation and assistive engineering. Int. J. Precis. Eng. Manuf. 2012, 13, 807–824. [Google Scholar] [CrossRef]
- Cempini, M.; Cortese, M.; Vitiello, N. A Powered Finger–Thumb Wearable Hand Exoskeleton With Self-Aligning Joint Axes. IEEE/ASME Trans. Mechatron. 2015, 20, 705–716. [Google Scholar] [CrossRef]
- Yue, Z.; Zhang, X.; Wang, J. Hand Rehabilitation Robotics on Poststroke Motor Recovery. Behav. Neurol. 2017, 2017, 3908135. [Google Scholar] [CrossRef] [PubMed]
- Conti, R.; Meli, E.; Ridolfi, A.; Bianchi, M.; Governi, L.; Volpe, Y.; Allotta, B. Kinematic synthesis and testing of a new portable hand exoskeleton. Meccanica 2017, 52, 2873–2897. [Google Scholar] [CrossRef]
- Maihöfner, C.; Seifert, F.; Markovic, K. Complex regional pain syndromes: New pathophysiological concepts and therapies. Eur. J. Neurol. 2010, 17, 649–660. [Google Scholar] [CrossRef]
- Barnhoorn, K.J.; van de Meent, H.; van Dongen, R.T.M.; Klomp, F.P.; Groenewoud, H.; Samwel, H.; Nijhuis-van der Sanden, M.W.G.; Frölke, J.P.M.; Staal, J.B. Pain exposure physical therapy (PEPT) compared to conventional treatment in complex regional pain syndrome type 1: A randomised controlled trial. BMJ Open 2015, 5, e008283. [Google Scholar] [CrossRef]
- Oerlemans, H.M.; Oostendorp, R.A.; de Boo, T.; Goris, R.J. Pain and reduced mobility in complex regional pain syndrome I: Outcome of a prospective randomised controlled clinical trial of adjuvant physical therapy versus occupational therapy. Pain 1999, 83, 77–83. [Google Scholar] [CrossRef]
- Oerlemans, H.M.; Oostendorp, R.A.; de Boo, T.; van der Laan, L.; Severens, J.L.; Goris, J.A. Adjuvant physical therapy versus occupational therapy in patients with reflex sympathetic dystrophy/complex regional pain syndrome type I. Arch. Phys. Med. Rehabil. 2000, 81, 49–56. [Google Scholar] [CrossRef]
- Epstein, D.; Mason, A.; Manca, A. The hospital costs of care for stroke in nine European countries. Health Econ. 2008, 17, S21–S31. [Google Scholar] [CrossRef]
- Elsamadicy, A.A.; Yang, S.; Sergesketter, A.R.; Ashraf, B.; Charalambous, L.; Kemeny, H.; Ejikeme, T.; Ren, X.; Pagadala, P.; Parente, B.; et al. Prevalence and Cost Analysis of Complex Regional Pain Syndrome (CRPS): A Role for Neuromodulation. Neuromodul. Technol. Neural Interface 2017, 21, 423–430. [Google Scholar] [CrossRef]
- Wege, A.; Kondak, K.; Hommel, G. Mechanical design and motion control of a hand exoskeleton for rehabilitation. In Proceedings of the IEEE International Conference Mechatronics and Automation, Niagara Falls, ON, Canada, 20 July–1 August 2005; Volume 1, pp. 155–159. [Google Scholar]
- Chiri, A.; Giovacchini, F.; Vitiello, N.; Cattin, E.; Roccella, S.; Vecchi, F.; Carrozza, M.C. HANDEXOS: Towards an exoskeleton device for the rehabilitation of the hand. In Proceedings of the 2009 IEEE/RSJ International Conference on Intelligent Robots and Systems, St. Louis, MO, USA, 10–15 October 2009; IEEE: Piscataway, NJ, USA, 2009; pp. 1106–1111. [Google Scholar] [CrossRef]
- Lee, J.; Lee, M.; Bae, J. Development of a Hand Exoskeleton System for Quantitative Analysis of Hand Functions. J. Bionic. Eng. 2018, 15, 783–794. [Google Scholar] [CrossRef]
- Iqbal, J.; Khan, H.; Tsagarakis, N.G.; Caldwell, D.G. A novel exoskeleton robotic system for hand rehabilitation – Conceptualization to prototyping. Biocybern. Biomed. Eng. 2014, 34, 79–89. [Google Scholar] [CrossRef]
- Sarac, M.; Solazzi, M.; Sotgiu, E.; Bergamasco, M.; Frisoli, A. Design and kinematic optimization of a novel underactuated robotic hand exoskeleton. Meccanica 2016, 52, 749–761. [Google Scholar] [CrossRef]
- Dickmann, T.; Wilhelm, N.J.; Glowalla, C.; Haddadin, S.; van der Smagt, P.; Burgkart, R. An Adaptive Mechatronic Exoskeleton for Force-Controlled Finger Rehabilitation. Front. Robot. 2021, 8, 314. [Google Scholar] [CrossRef] [PubMed]
- McCabe, C.S.; Haigh, R.C.; Ring, E.F.J.; Halligan, P.W.; Wall, P.D.; Blake, D.R. A controlled pilot study of the utility of mirror visual feedback in the treatment of complex regional pain syndrome (type 1). Rheumatology 2003, 42, 97–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cacchio, A.; De Blasis, E.; Necozione, S.; di Orio, F.; Santilli, V. Mirror therapy for chronic complex regional pain syndrome type 1 and stroke. N. Engl. J. Med. 2009, 361, 634–636. [Google Scholar] [CrossRef] [PubMed]
- Moseley, G.L. Graded motor imagery is effective for long-standing complex regional pain syndrome: A randomised controlled trial. Pain 2004, 108, 192–198. [Google Scholar] [CrossRef]
- Moseley, G.L. Graded motor imagery for pathologic pain: A randomized controlled trial. Neurology 2006, 67, 2129–2134. [Google Scholar] [CrossRef]
- den Hollander, M.; Goossens, M.; de Jong, J.; Ruijgrok, J.; Oosterhof, J.; Onghena, P.; Smeets, R.; Vlaeyen, J.W.S. Expose or protect? A randomized controlled trial of exposure in vivo vs pain-contingent treatment as usual in patients with complex regional pain syndrome type 1. Pain 2016, 157, 2318–2329. [Google Scholar] [CrossRef]
- Harden, N.R.; Bruehl, S.; Perez, R.S.G.M.; Birklein, F.; Marinus, J.; Maihofner, C.; Lubenow, T.; Buvanendran, A.; Mackey, S.; Graciosa, J.; et al. Validation of proposed diagnostic criteria (the “Budapest Criteria”) for Complex Regional Pain Syndrome. Pain 2010, 150, 268–274. [Google Scholar] [CrossRef] [Green Version]
- Beaton, D.E.; Wright, J.G.; Katz, J.N.; Upper Extremity Collaborative Group. Development of the QuickDASH: Comparison of three item-reduction approaches. J. Bone Jt. Surg. Am. 2005, 87, 1038–1046. [Google Scholar]
- Hansen, F.; Sawatzky, J.A.V. Stress in Patients With Lung Cancer: A Human Response to Illness. Oncol. Nurs. Forum 2008, 35, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Appelhans, B.M.; Luecken, L.J. Heart Rate Variability as an Index of Regulated Emotional Responding. Rev. Gen. Psychol. 2006, 10, 229–240. [Google Scholar] [CrossRef] [Green Version]
- Birklein, F.; Dimova, V. Complex regional pain syndrome–up-to-date. Pain Rep. 2017, 2, e624. [Google Scholar] [CrossRef] [PubMed]
- Michalos, A.C. (Ed.) Quick DASH, Questionnaire (13-Item Short Version). In Encyclopedia of Quality of Life and Well-Being Research; Springer: Dordrecht, The Netherlands, 2014; p. 5382. [Google Scholar] [CrossRef]
- Dawson, M.E.; Schell, A.M.; Filion, D.L.; Berntson, G.G. The Electrodermal System. In Handbook of Psychophysiology; Cacioppo, J.T., Tassinary, L.G., Berntson, G., Eds.; Cambridge University Press: Cambridge, UK, 2000; pp. 157–181. [Google Scholar]
- Glowinski, S.; Blazejewski, A. SPIDER as A Rehabilitation Tool for Patients with Neurological Disabilities: The Preliminary Research. J. Pers. Med. 2020, 10, 33. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Age | Sex | BMI | Duration CRPS | Trigger CRPS |
|---|---|---|---|---|---|
| 1 | 26 | female | 32.1 kg/m | 5 years | Hand overload when writing |
| 2 | 68 | female | 28.3 kg/m | 7 months | Elbow fracture |
| 3 | 44 | male | 21.3 kg/m | 8 months | Wrist fracture |
| Patient | Temperature | O2-Saturation | Heart Rate | Skin Conductivity |
|---|---|---|---|---|
| 1 pre | 37 °C | 90% | 91 | 0.78 µS |
| 1 post | 37 °C | 99% | 82 | 0.34 µS |
| 2 pre | 38 °C | 96% | 58 | 0.38 µS |
| 2 post | 38 °C | 96% | 62 | 0.09 µS |
| 3 pre | 39 °C | 97% | 64 | 0.64 µS |
| 3 post | 36 °C | 99% | 60 | 0.33 µS |
| Score | Patient 1 | Patient 2 | Patient 3 |
|---|---|---|---|
| Budapest Pre [28] | 6/11 | 5/11 | 7/11 |
| Budapest Post [28] | 5/11 | 1/11 | 2/11 |
| QuickDASH Pre [29] | 50% | 43% | 40% |
| QuickDASH Post [29] | 45% | 38% | 38% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wilhelm, N.J.; Haddadin, S.; Lang, J.J.; Micheler, C.; Hinterwimmer, F.; Reiners, A.; Burgkart, R.; Glowalla, C. Development of an Exoskeleton Platform of the Finger for Objective Patient Monitoring in Rehabilitation. Sensors 2022, 22, 4804. https://doi.org/10.3390/s22134804
Wilhelm NJ, Haddadin S, Lang JJ, Micheler C, Hinterwimmer F, Reiners A, Burgkart R, Glowalla C. Development of an Exoskeleton Platform of the Finger for Objective Patient Monitoring in Rehabilitation. Sensors. 2022; 22(13):4804. https://doi.org/10.3390/s22134804
Chicago/Turabian StyleWilhelm, Nikolas Jakob, Sami Haddadin, Jan Josef Lang, Carina Micheler, Florian Hinterwimmer, Anselm Reiners, Rainer Burgkart, and Claudio Glowalla. 2022. "Development of an Exoskeleton Platform of the Finger for Objective Patient Monitoring in Rehabilitation" Sensors 22, no. 13: 4804. https://doi.org/10.3390/s22134804
APA StyleWilhelm, N. J., Haddadin, S., Lang, J. J., Micheler, C., Hinterwimmer, F., Reiners, A., Burgkart, R., & Glowalla, C. (2022). Development of an Exoskeleton Platform of the Finger for Objective Patient Monitoring in Rehabilitation. Sensors, 22(13), 4804. https://doi.org/10.3390/s22134804