
2D Gait Skeleton Data Normalization for Quantitative Assessment of Movement Disorders from Freehand Single Camera Video Recordings



Abstract
:1. Introduction
2. Materials and Methods
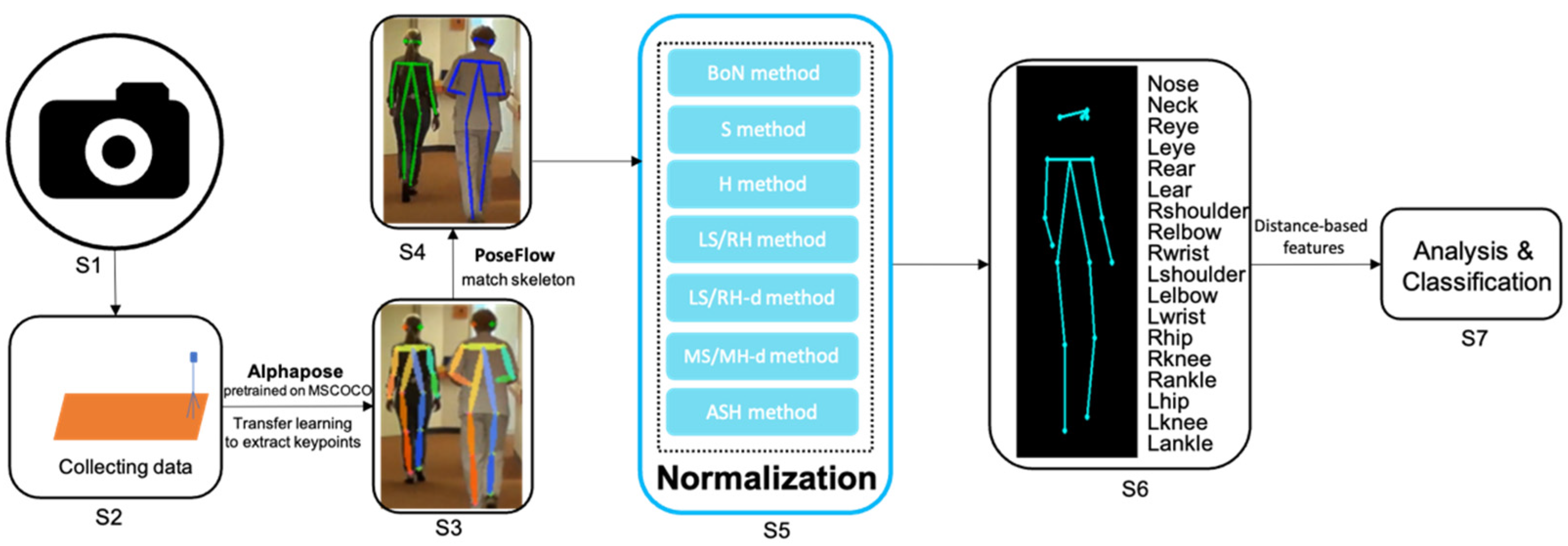
2.1. Pipeline
2.2. Data Preparation
2.3. Pose Estimation
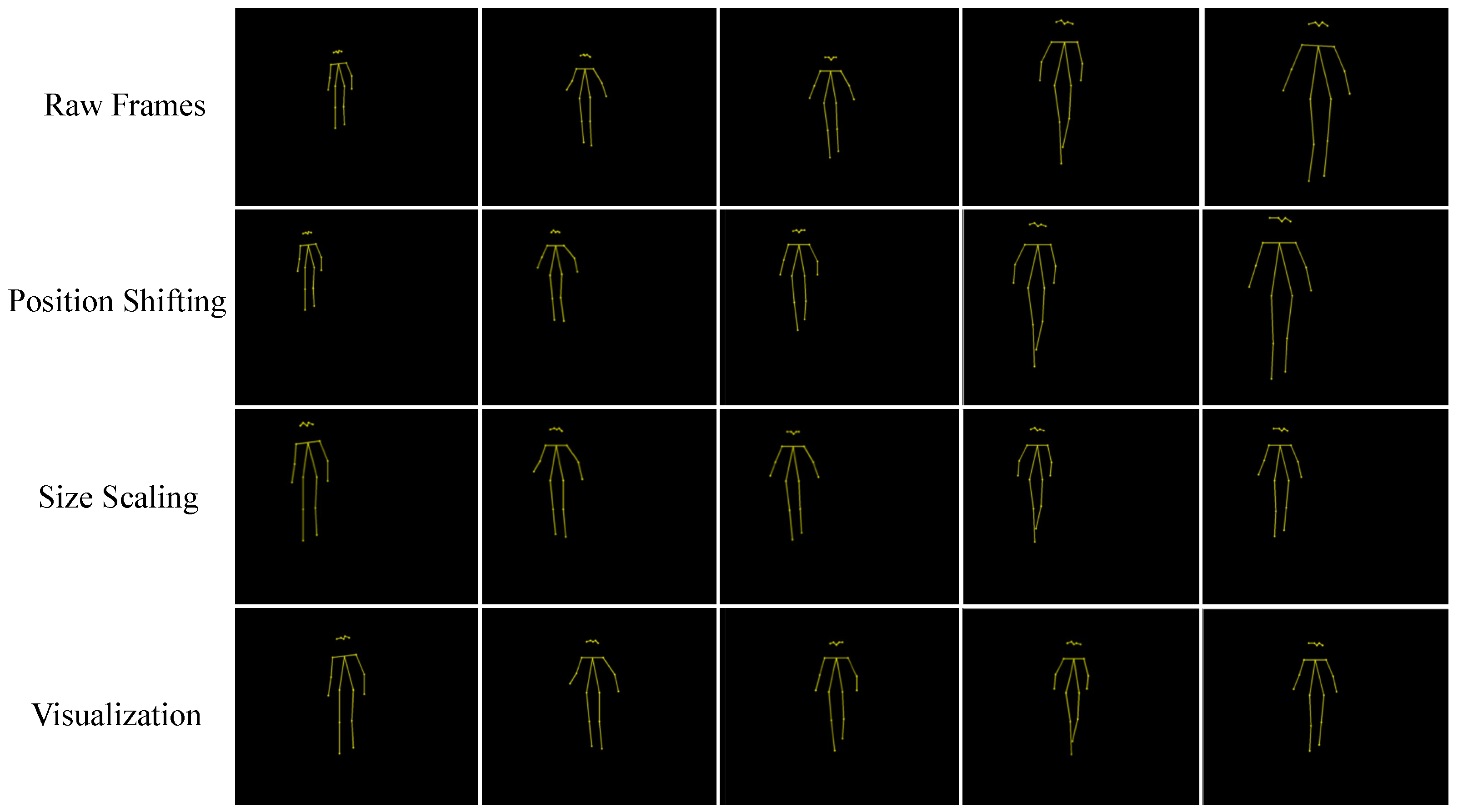
2.4. Normalization
2.5. Evaluation
3. Results
3.1. Likelihood from Pose Estimation
3.2. Mean Absolute Angle Error
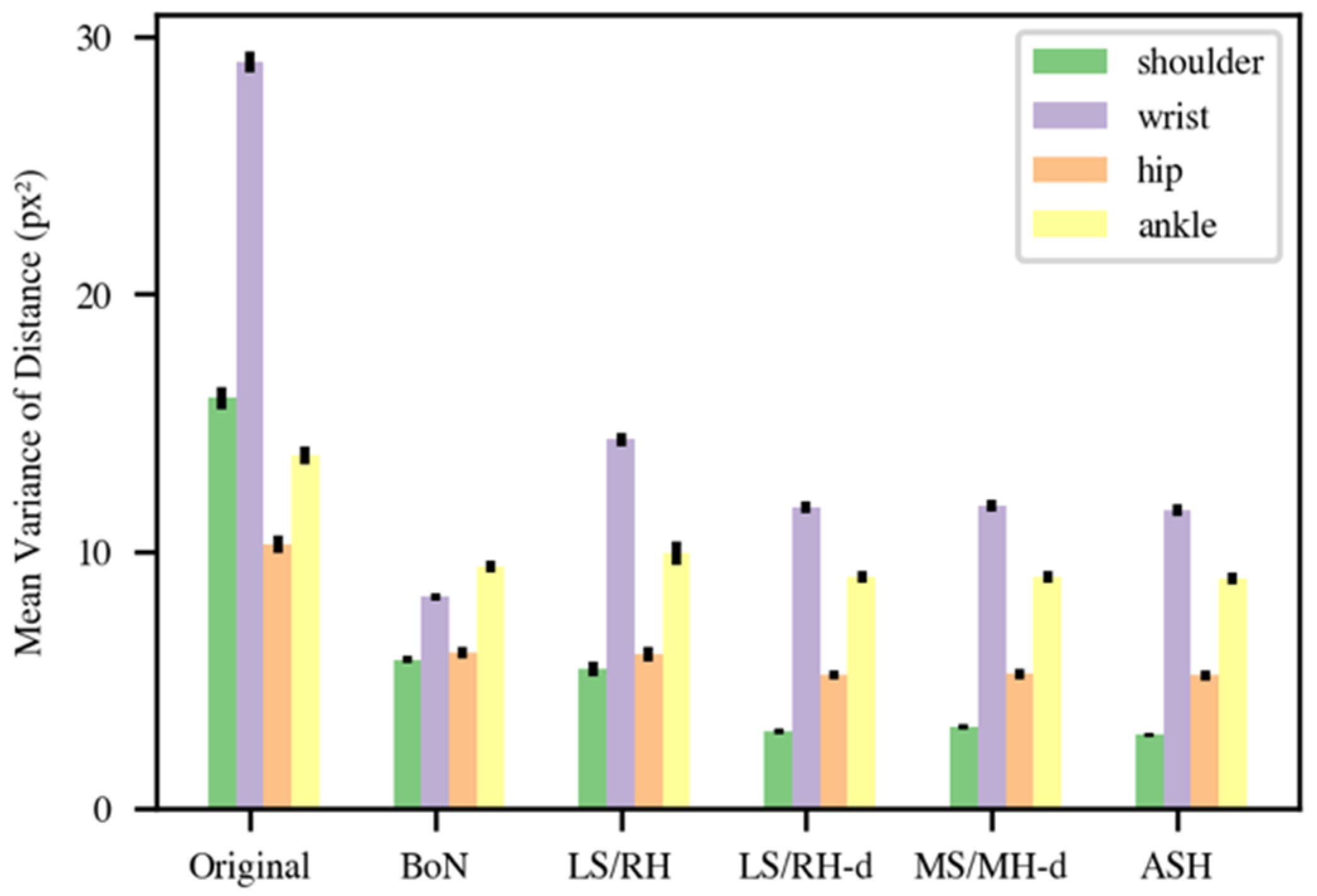
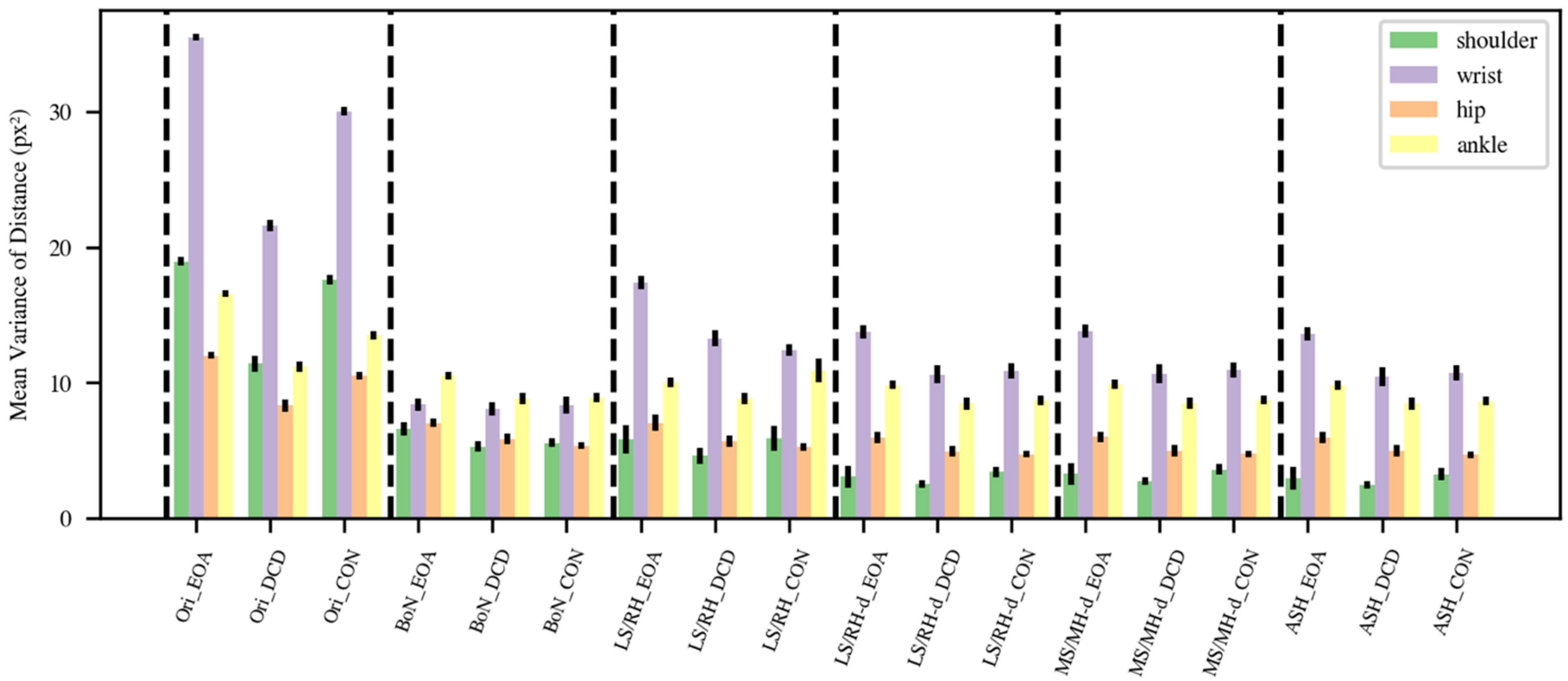
3.3. Mean Variance of Distance
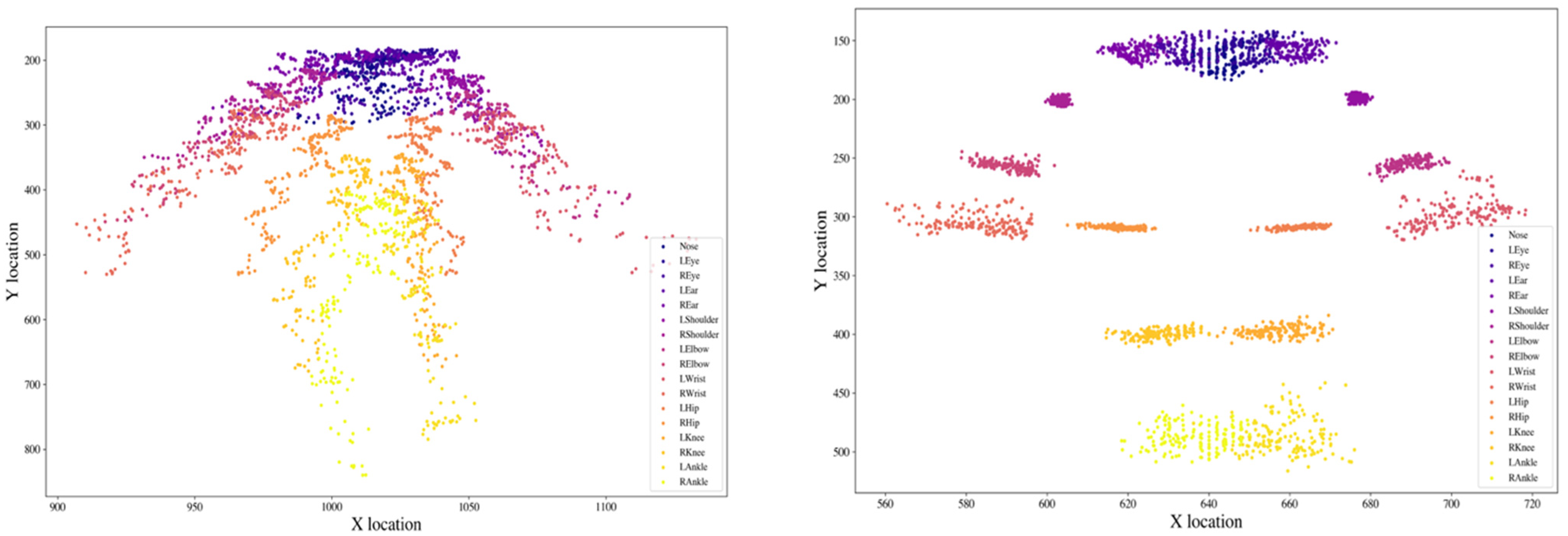
3.4. Location Distribution Comparison
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lawerman, T.F.; Brandsma, R.; Maurits, N.M.; Martinez-Manzanera, O.; Verschuuren-Bemelmans, C.C.; Lunsing, R.J.; Brouwer, O.F.; Kremer, H.P.; Sival, D.A. Paediatric motor phenotypes in early-onset ataxia, developmental coordination disorder, and central hypotonia. Dev. Med. Child Neurol. 2020, 62, 75–82. [Google Scholar] [CrossRef] [Green Version]
- Ilg, W.; Timmann, D. Gait ataxia-specific cerebellar influences and their rehabilitation. Mov. Disord. 2013, 28, 1566–1575. [Google Scholar] [CrossRef]
- Schmitz-Hübsch, T.; Du Montcel, S.T.; Baliko, L.; Berciano, J.; Boesch, S.; Depondt, C.; Giunti, P.; Globas, C.; Infante, J.; Kang, J.-S. Scale for the assessment and rating of ataxia: Development of a new clinical scale. Neurology 2006, 66, 1717–1720. [Google Scholar] [CrossRef]
- Lawerman, T.F.; Brandsma, R.; Verbeek, R.J.; Van Der Hoeven, J.H.; Lunsing, R.J.; Kremer, H.P.H.; Sival, D.A. Construct Validity and Reliability of the SARA Gait and Posture Sub-scale in Early Onset Ataxia. Front. Hum. Neurosci. 2017, 11, 605. [Google Scholar] [CrossRef] [Green Version]
- Bürk, K.; Sival, D.A. Scales for the clinical evaluation of cerebellar disorders. Handb. Clin. Neurol. 2018, 154, 329–339. [Google Scholar]
- Brandsma, R.; Lawerman, T.F.; Kuiper, M.J.; Lunsing, R.J.; Burger, H.; Sival, D.A. Reliability and discriminant validity of ataxia rating scales in early onset ataxia. Dev. Med. Child. Neurol. 2017, 59, 427–432. [Google Scholar] [CrossRef]
- Aguilar, V.S.; Manzanera, O.M.; Sival, D.A.; Maurits, N.M.; Roerdink, J.B.T.M. Distinguishing Patients with a Coordination Disorder from Healthy Controls Using Local Features of Movement Trajectories during the Finger-to-Nose Test. IEEE Trans. Biomed. Eng. 2018, 66, 1714–1722. [Google Scholar] [CrossRef]
- Dominguez-Vega, Z.T.; Dubber, D.; Elting, J.W.J.; Sival, D.; Maurits, N.M. Instrumented classification of patients with early onset ataxia or developmental coordination disorder and healthy control children combining information from three upper limb SARA tests. Eur. J. Paediatr. Neurol. 2021, 34, 74–83. [Google Scholar] [CrossRef]
- Mannini, A.; Martinez-Manzanera, O.; Lawerman, T.F.; Trojaniello, D.; Della Croce, U.; Sival, D.A.; Maurits, N.M.; Sabatini, A.M. Automatic classification of gait in children with early-onset ataxia or developmental coordination disorder and controls using inertial sensors. Gait Posture 2017, 52, 287–292. [Google Scholar] [CrossRef] [Green Version]
- Pirker, W.; Katzenschlager, R. Gait disorders in aults and the elderly: A clinical guide. Wien. Klin. Wochenschr. 2016, 129, 81–95. [Google Scholar] [CrossRef] [Green Version]
- He, K.; Gkioxari, G.; Dollár, P.; Girshick, R. Mask r-cnn. In Proceedings of the IEEE International Conference on Computer Vision, Venice, Italy, 22–29 October 2017; pp. 2961–2969. [Google Scholar]
- Insafutdinov, E.; Pishchulin, L.; Andres, B.; Andriluka, M.; Schiele, B. Deepercut: A deeper, stronger, and faster multi-person pose estimation model. In Proceedings of the European Conference on Computer Vision, Amsterdam, The Netherlands, 11–14 October 2016; pp. 34–50. [Google Scholar]
- Mathis, A.; Mamidanna, P.; Cury, K.M.; Abe, T.; Murthy, V.N.; Mathis, M.W.; Bethge, M. DeepLabCut: Markerless pose estimation of user-defined body parts with deep learning. Nat. Neurosci. 2018, 21, 1281–1289. [Google Scholar] [CrossRef]
- Chen, Y.; Wang, Z.; Peng, Y.; Zhang, Z.; Yu, G.; Sun, J. Cascaded pyramid network for multi-person pose estimation. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Salt Lake City, UT, USA, 18–22 June 2018; pp. 7103–7112. [Google Scholar]
- Cao, Z.; Simon, T.; Wei, S.-E.; Sheikh, Y. Realtime multi-person 2d pose estimation using part affinity fields. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Hawaii, HI, USA, 21–26 July 2017; pp. 7291–7299. [Google Scholar]
- Fang, H.-S.; Xie, S.; Tai, Y.-W.; Lu, C. Rmpe: Regional multi-person pose estimation. In Proceedings of the IEEE International Conference on Computer Vision, Venice, Italy, 22–29 October 2017; pp. 2334–2343. [Google Scholar]
- Joshi, D.; Merler, M.; Nguyen, Q.-B.; Hammer, S.; Kent, J.; Smith, J.R.; Feris, R.S. IBM High-Five: Highlights from Intelligent Video Engine. In Proceedings of the ACM Multimedia, Mountain View, CA, USA, 23–27 October 2017; pp. 1249–1250. [Google Scholar]
- Tian, L.; Cheng, X.; Honda, M.; Ikenaga, T. Multi-technology Correction Based 3D Human Pose Estimation for Jump Analysis in Figure Skating. In Proceedings of the Multidisciplinary Digital Publishing Institute Proceedings, West Lafayette, IN, USA, 22–26 June 2020; p. 95. [Google Scholar]
- Chen, W.; Jiang, Z.; Guo, H.; Ni, X. Fall detection based on key points of human-skeleton using openpose. Symmetry 2020, 12, 744. [Google Scholar] [CrossRef]
- Lin, T.-Y.; Maire, M.; Belongie, S.; Hays, J.; Perona, P.; Ramanan, D.; Dollár, P.; Zitnick, C.L. Microsoft coco: Common objects in context. In Proceedings of the European Conference on Computer Vision, Zurich, Switzerland, 6–12 September 2014; pp. 740–755. [Google Scholar]
- Tian, Y.; Li, N.; Mao, B. Video Behavior Detection based on Optimized Alphapose in Electricity Facility Management. In Proceedings of the IEEE/WIC/ACM International Conference on Web Intelligence and Intelligent Agent Technology, Maebashi, Japan, 14–17 December 2021; pp. 364–367. [Google Scholar]
- Zhang, C.; Yang, X. Bed-Leaving Action Recognition Based on YOLOv3 and AlphaPose. In Proceedings of the 2022 the 5th International Conference on Image and Graphics Processing (ICIGP), Beijing, China, 7–9 January 2022; pp. 117–123. [Google Scholar]
- Lv, X.; Ta, N.; Chen, T.; Zhao, J.; Wei, H. Analysis of Gait Characteristics of Patients with Knee Arthritis Based on Human Posture Estimation. BioMed Res. Int. 2022, 2022, 7020804. [Google Scholar] [CrossRef]
- Peng, X.; Zhang, Y.; Song, L. Research on Gait Evaluation Method Based on Machine Vision. In Proceedings of the 2021 International Conference on Intelligent Computing, Automation and Applications (ICAA), Nanjing, China, 25–27 June 2021; pp. 357–362. [Google Scholar]
- Sabo, A.; Mehdizadeh, S.; Iaboni, A.; Taati, B. Prediction of Parkinsonian Gait in Older Adults with Dementia using Joint Trajectories and Gait Features from 2D Video. In Proceedings of the 2021 43rd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Jalisco, Mexico, 26 July 2021; pp. 5700–5703. [Google Scholar]
- Sabo, A.; Mehdizadeh, S.; Iaboni, A.; Taati, B. Estimating parkinsonism severity in natural gait videos of older adults with dementia. IEEE J. Biomed. Health Inform. 2022, 26, 2288–2298. [Google Scholar] [CrossRef]
- Whittle, M.W. Clinical gait analysis: A review. Hum. Mov. Sci. 1996, 15, 369–387. [Google Scholar] [CrossRef]
- Mehdizadeh, S.; Nabavi, H.; Sabo, A.; Arora, T.; Iaboni, A.; Taati, B. Concurrent validity of human pose tracking in video for measuring gait parameters in older adults: A preliminary analysis with multiple trackers, viewing angles, and walking directions. J. Neuro Eng. Rehabil. 2021, 18, 139. [Google Scholar] [CrossRef]
- Xiu, Y.; Li, J.; Wang, H.; Fang, Y.; Lu, C. Pose Flow: Efficient online pose tracking. arXiv 2018, arXiv:1802.00977. [Google Scholar]
- Schöls, L.; Bauer, P.; Schmidt, T.; Schulte, T.; Riess, O. Autosomal dominant cerebellar ataxias: Clinical features, genetics, and pathogenesis. Lancet Neurol. 2004, 3, 291–304. [Google Scholar] [CrossRef]
- Redmon, J.; Farhadi, A. Yolov3: An incremental improvement. arXiv 2018, arXiv:1804.02767. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Caesars Palace, NV, USA, 26 June–1 July 2016; pp. 770–778. [Google Scholar]
- Buckley, E.; Mazzà, C.; McNeill, A. A systematic review of the gait characteristics associated with Cerebellar Ataxia. Gait Posture 2018, 60, 154–163. [Google Scholar] [CrossRef]
- Baker, J.M. Gait disorders. Am. J. Med. 2018, 131, 602–607. [Google Scholar] [CrossRef]
- Hannink, J.; Kautz, T.; Pasluosta, C.F.; Gaßmann, K.-G.; Klucken, J.; Eskofier, B.M. Sensor-based gait parameter extraction with deep convolutional neural networks. IEEE J. Biomed. Health Inform. 2016, 21, 85–93. [Google Scholar] [CrossRef] [Green Version]
- Li, X.X.R.W.M.; Jia-hua, S.C. Accuracy of the Microsoft KinectTM for measuring gait. Eur. J. Med. 2012, 7, 176–182. [Google Scholar]
- Kidziński, Ł.; Yang, B.; Hicks, J.L.; Rajagopal, A.; Delp, S.L.; Schwartz, M.H. Deep neural networks enable quantitative movement analysis using single-camera videos. Nat. Commun. 2020, 11, 4054. [Google Scholar] [CrossRef]
- Sato, K.; Nagashima, Y.; Mano, T.; Iwata, A.; Toda, T. Quantifying normal and parkinsonian gait features from home movies: Practical application of a deep learning–based 2D pose estimator. PLoS ONE 2019, 14, e0223549. [Google Scholar] [CrossRef] [Green Version]
- Kwolek, B.; Michalczuk, A.; Krzeszowski, T.; Switonski, A.; Josinski, H.; Wojciechowski, K. Calibrated and synchronized multi-view video and motion capture dataset for evaluation of gait recognition. Multimed. Tools Appl. 2019, 78, 32437–32465. [Google Scholar] [CrossRef] [Green Version]
- Arac, A. Machine learning for 3D kinematic analysis of movements in neurorehabilitation. Curr. Neurol. Neurosci. Rep. 2020, 20, 29. [Google Scholar] [CrossRef]
- Zhang, Y.; Funkhouser, T. Deep depth completion of a single rgb-d image. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Salt Lake City, UT, USA, 18–22 June 2018; pp. 175–185. [Google Scholar]
- Elias, P.; Sedmidubsky, J.; Zezula, P. Understanding the limits of 2D skeletons for action recognition. Multimed. Syst. 2021, 27, 547–561. [Google Scholar] [CrossRef]
- Cornwall, M.W.; McPoil, T. Comparison of 2-dimensional and 3-dimensional rearfoot motion during walking. Clin. Biomech. 1995, 10, 36–40. [Google Scholar] [CrossRef]
- Dingenen, B.; Staes, F.F.; Santermans, L.; Steurs, L.; Eerdekens, M.; Geentjens, J.; Peers, K.H.; Thysen, M.; Deschamps, K. Are two-dimensional measured frontal plane angles related to three-dimensional measured kinematic profiles during running? Phys. Ther. Sport 2018, 29, 84–92. [Google Scholar] [CrossRef]
- Daugaard, M.; Brandborg Nielsen, D. Comparison of Angular Measurements by 2D and 3D Gait Analysis. Available online: https://www.diva-portal.org/smash/get/diva2:113552/FULLTEXT01.pdf (accessed on 31 May 2022).
- Saner, R.J.; Washabaugh, E.P.; Krishnan, C. Reliable sagittal plane kinematic gait assessments are feasible using low-cost webcam technology. Gait Posture 2017, 56, 19–23. [Google Scholar] [CrossRef]
- Brandsma, R.; Lawerman, T.; Burger, H.; Burgerhof, J.; Sival, D. Age-related Reference Values for the Pediatric Scale for Assessment and Rating of Ataxia-A Multicenter Study. Dev. Med. Child Neurol. 2017, 59, 1077–1082. [Google Scholar]
- Golenia, L.; Bongers, R.M.; van Hoorn, J.F.; Otten, E.; Mouton, L.J.; Schoemaker, M.M. Variability in coordination patterns in children with developmental coordination disorder (DCD). Hum. Mov. Sci. 2018, 60, 202–213. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mean | STD | |
|---|---|---|
| before cleaning | 0.817 | 0.09 |
| after cleaning | 0.889 | 0.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tang, W.; van Ooijen, P.M.A.; Sival, D.A.; Maurits, N.M. 2D Gait Skeleton Data Normalization for Quantitative Assessment of Movement Disorders from Freehand Single Camera Video Recordings. Sensors 2022, 22, 4245. https://doi.org/10.3390/s22114245
Tang W, van Ooijen PMA, Sival DA, Maurits NM. 2D Gait Skeleton Data Normalization for Quantitative Assessment of Movement Disorders from Freehand Single Camera Video Recordings. Sensors. 2022; 22(11):4245. https://doi.org/10.3390/s22114245
Chicago/Turabian StyleTang, Wei, Peter M. A. van Ooijen, Deborah A. Sival, and Natasha M. Maurits. 2022. "2D Gait Skeleton Data Normalization for Quantitative Assessment of Movement Disorders from Freehand Single Camera Video Recordings" Sensors 22, no. 11: 4245. https://doi.org/10.3390/s22114245
APA StyleTang, W., van Ooijen, P. M. A., Sival, D. A., & Maurits, N. M. (2022). 2D Gait Skeleton Data Normalization for Quantitative Assessment of Movement Disorders from Freehand Single Camera Video Recordings. Sensors, 22(11), 4245. https://doi.org/10.3390/s22114245