
Efficacy of Electromyographic Biofeedback in Muscle Recovery after Meniscectomy in Soccer Players




Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Measurements and Instruments
2.4. Procedure
2.5. Data Analysis
3. Results
3.1. Variance Component Analysis
3.2. Generalizability Analysis
3.3. Trials with BF vs. Trials without BF and Trials before BF vs. Trials after BF
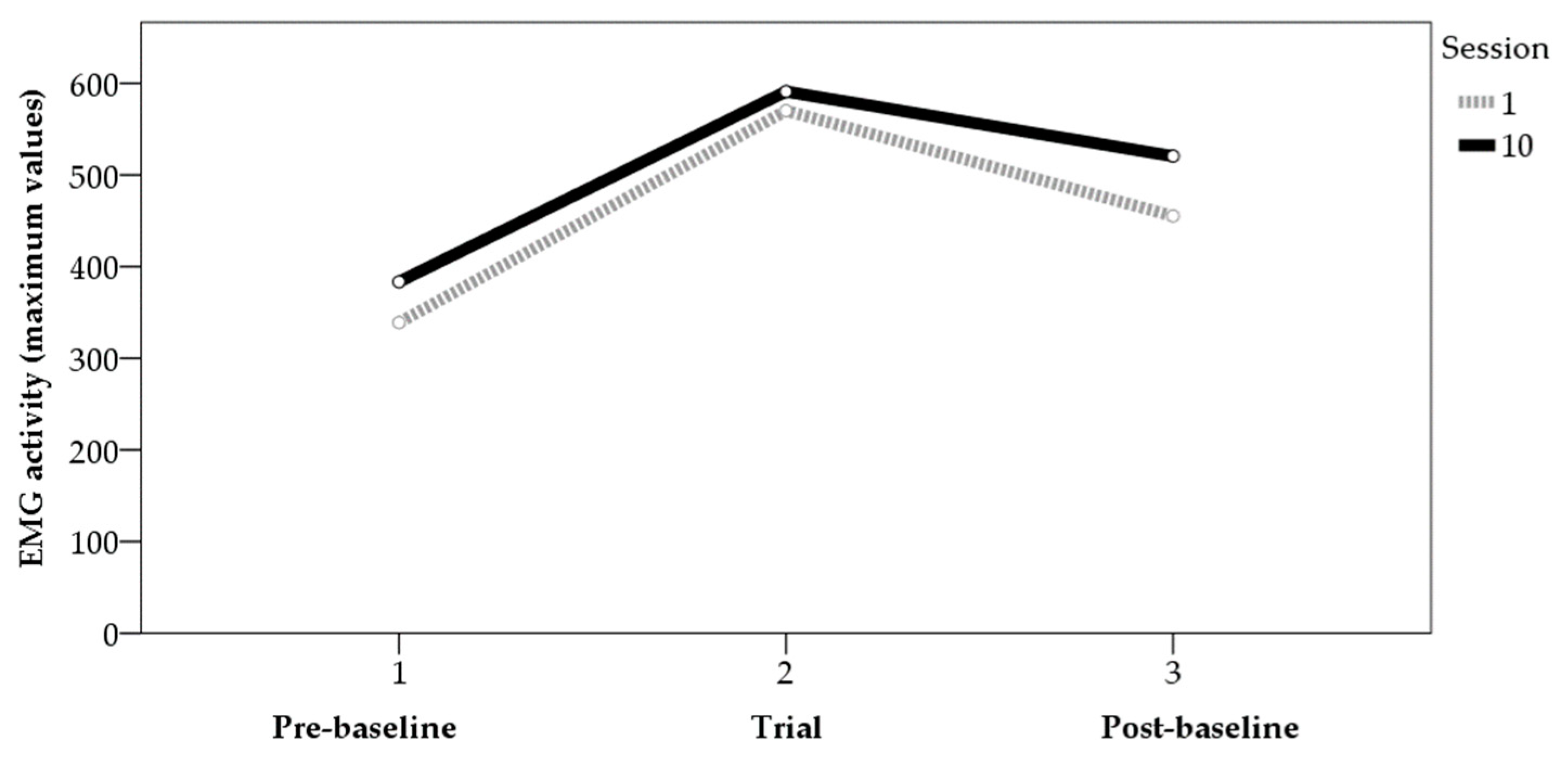
3.4. Session 1 vs. Session 10
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Abril-Rodríguez, S.; Herrero, R. Biofeedback electromiográfico y electroglotográfico aplicado a la terapia vocal: Una revisión sistemática. Rev. Investig. Logop. 2022, 12, e75581. [Google Scholar] [CrossRef]
- Ardizone, I.; Sánchez, T.; Celemín, A.; Rivero, A. Biofeedback electromiográfico. Una alternativa terapéutica útil para la relajación muscular en pacientes con disfunción craneomandibular. Rev. Int. Prótesis Estomatol. 2009, 11, 85–88. [Google Scholar]
- Lehrer, P.; Kaur, K.; Sharma, A.; Shah, K.; Huseby, R.; Bhavsar, J.; Sgobba, P.; Zhang, Y. Heart rate variability biofeedback improves emotional and physical health and performance: A systematic review and meta analysis. Appl. Psychophys. Biof. 2020, 45, 109–129. [Google Scholar] [CrossRef] [PubMed]
- Pizzoli, S.F.; Marzorati, C.; Gatti, D.; Monzani, D.; Mazzocco, K.; Pravettoni, G. A meta-analysis on heart rate variability biofeedback and depressive symptoms. Sci. Rep. 2021, 11, 6650. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, R.H.; Reaz, M.B.I.; Ali, M.A.M. Surface Electromyography Signal Processing and Classification Techniques. Sensors 2013, 13, 12431–12466. [Google Scholar] [CrossRef]
- De Luca, C.J. Electromyography. In Encyclopaedia of Medical Devices and Instrumentation; Webster, J.G., Ed.; Wiley: New York, NY, USA, 1988; pp. 1111–1120. [Google Scholar]
- Phinyomark, A.; Campbell, E.; Scheme, E. Surface Electromyography (EMG) Signal Processing, Classification, and Practical Considerations. In Biomedical Signal Processing: Advances in Theory, Algorithms and Applications; Naik, G., Ed.; Springer: Singapore, 2020; pp. 3–29. [Google Scholar] [CrossRef]
- Simon, M.A. Biofeedback y Rehabilitación; Promolibro: Valencia, Spain, 1989. [Google Scholar]
- Armagan, O.; Tascioglu, F.; Oner, C. Electromyographic biofeedback in the treatment of the hemiplegic hand: A placebo-controlled study. Am. J. Phys. Med. Rehab. 2003, 82, 856–861. [Google Scholar] [CrossRef]
- Schleenbaker, R.E.; Mainous, A.G. Electromyographic biofeedback for neuromuscular reeducation in the hemiplegic stroke patient: A meta-analysis. Arch. Phys. Med. Rehab. 1993, 74, 1301–1304. [Google Scholar] [CrossRef]
- Jing, G. Clinical effect evaluation and experience of motomed virtual scene training combined with electromyographic biofeedback therapy in the treatment of spastic cerebral palsy. Ann. Phys. Rehab. Med. 2018, 61, e322. [Google Scholar] [CrossRef]
- Kamonseki, D.H.; Calixtre, L.B.; Barreto, R.P.G.; Camargo, P.R. Effects of electromyographic biofeedback interventions for shoulder pain and function: Systematic review and meta-analysis. Clin. Rehab. 2021, 35, 952–963. [Google Scholar] [CrossRef]
- Raeissadat, S.A.; Rayegani, S.M.; Sedighipour, L.; Bossaghzade, Z.; Abdollahzadeh, M.H.; Nikray, R.; Mollayi, F. The efficacy of electromyographic biofeedback on pain, function, and maximal thickness of vastus medialis oblique muscle in patients with knee osteoarthritis: A randomized clinical trial. J. Pain Res. 2018, 11, 2781–2789. [Google Scholar] [CrossRef] [Green Version]
- Inglis, J.; Campbell, D.; Donald, M.W. Electromyographic biofeedback and neuromuscular rehabilitation. Can. J. Behav. Sci. 1976, 8, 299–323. [Google Scholar] [CrossRef]
- Florjanski, W.; Malysa, A.; Orzeszek, S.; Smardz, J.; Olchowy, A.; Paradowska-Stolarz, A.; Wieckiewicz, M. Evaluation of biofeedback usefulness in masticatory muscle activity management—A systematic review. J. Clin. Med. 2019, 8, 766. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hernández-Mendo, A. Biofeedback electromiográfico en la rehabilitación de lesiones de rodilla. Estudio de dos casos en futbolistas profesionales. Cuad. Psicol. Deporte 2011, 11, 71–80. [Google Scholar]
- Hernández-Mendo, A.; Morales-Sánchez, V. Efectividad del biofeedback electromiográfico en la rehabilitación de lesiones deportivas. Rev. Psicol. Deporte 2014, 23, 489–500. [Google Scholar]
- Draper, V.; Ballard, L. Electrical stimulation versus electromyographic biofeedback in the recovery of quadriceps femoris muscle function following anterior cruciate ligament surgery. Phys. Ther. 1991, 71, 455–461. [Google Scholar] [CrossRef]
- Karaborklu-Argut, S.; Celik, D.; Yasacı, Z. Effectiveness of therapeutic electromyographic biofeedback after orthopedic knee surgeries: A systematic review. Disabil. Rehabil. 2021, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Christanell, F.; Hoser, C.; Huber, R.; Fink, C.; Luomajoki, H. The influence of electromyographic biofeedback therapy on knee extension following anterior cruciate ligament reconstruction: A randomized controlled trial. Sports Med. Arthrosc. Rehabil. Ther. Technol. 2012, 4, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xie, Y.J.; Wang, S.; Gong, Q.J.; Wang, J.X.; Sun, F.H.; Miyamoto, A.; Ou, X.; Wang, S.Q.; Zhang, C. Effects of electromyography biofeedback for patients after knee surgery: A systematic review and meta-analysis. J. Biomech. 2021, 120, 110386. [Google Scholar] [CrossRef]
- Hernández-Mendo, A. Efectividad del Biofeedback Electromiográfico en la rehabilitación de lesiones deportivas. Un caso de fractura radio. Rev. Psicol. Gen. Apl. 2009, 62, 83–89. [Google Scholar]
- Junge, A.; Dvorak, J. Soccer injuries. Sports Med. 2004, 34, 929–938. [Google Scholar] [CrossRef]
- López-Valenciano, A.; Ruiz-Pérez, I.; Garcia-Gómez, A.; Vera-Garcia, F.J.; Croix, M.D.S.; Myer, G.D.; Ayala, F. Epidemiology of injuries in professional football: A systematic review and meta-analysis. Brit. J. Sport Med. 2020, 54, 711–718. [Google Scholar] [CrossRef] [PubMed]
- Dvorak, J.; Junge, A. Football injuries and physical symptoms. Am. J. Sport Med. 2000, 28, 3–9. [Google Scholar] [CrossRef]
- Moreno-Pascual, C.; Rodríguez-Pérez, V.; Seco-Calvo, J. Epidemiología de las lesiones deportivas. Fisioterapia 2008, 30, 40–48. [Google Scholar] [CrossRef]
- Read, P.J.; Oliver, J.L.; De Ste Croix, M.; Myer, G.D.; Lloyd, R.S. Neuromuscular risk factors for knee and ankle ligament injuries in male youth soccer players. Sports Med. 2016, 46, 1059–1066. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nilstad, A.; Andersen, T.E.; Bahr, R.; Holme, I.; Steffen, K. Risk factors for lower extremity injuries in elite female soccer players. Am. J. Sport Med. 2014, 42, 940–948. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Uhm, Y.H. Effect of ankle stabilization training using biofeedback on balance ability and lower limb muscle activity in football players with functional ankle instability. J. Kor. Phys. Ther. 2016, 28, 189–194. [Google Scholar] [CrossRef] [Green Version]
- Grimm, N.L.; Jacobs, J.C., Jr.; Kim, J.; Denney, B.S.; Shea, K.G. Anterior cruciate ligament and knee injury prevention programs for soccer players: A systematic review and meta-analysis. Am. J. Sport Med. 2015, 43, 2049–2056. [Google Scholar] [CrossRef]
- Kellis, E.; Katis, A.; Gissis, I. Knee biomechanics of the support leg in soccer kicks from three angles of approach. Med. Sci. Sport Exerc. 2004, 36, 1017–1028. [Google Scholar] [CrossRef]
- Arundale, A.J.; Silvers-Granelli, H.J.; Marmon, A.; Zarzycki, R.; Dix, C.; Snyder-Mackler, L. Changes in biomechanical knee injury risk factors across two collegiate soccer seasons using the 11+ prevention program. Scand. J. Med. Sci. Spor. 2018, 28, 2592–2603. [Google Scholar] [CrossRef]
- Steinbacher, G.; Alentorn-Geli, E.; Alvarado-Calderón, M.; Barastegui, D.; Álvarez-Díaz, P.; Cugat, R. Meniscal fixation is a successful treatment for hypermobile lateral meniscus in soccer players. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 354–360. [Google Scholar] [CrossRef]
- Alentorn-Geli, E.; Vázquez, R.S.; Díaz, P.Á.; Cuscó, X.; Cugat, R. Arthroscopic meniscal transplants in soccer players: Outcomes at 2-to 5-year follow-up. Clin. J. Sport Med. 2010, 20, 340–343. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Diaz, P.; Alentorn-Geli, E.; Llobet, F.; Granados, N.; Steinbacher, G.; Cugat, R. Return to play after all-inside meniscal repair in competitive football players: A minimum 5-year follow-up. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 1997–2001. [Google Scholar] [CrossRef] [PubMed]
- Villarreal, J.M.B.; González, I.L.; Sánchez, G.V. Lesiones meniscales. Orthotips AMOT 2009, 5, 39–48. [Google Scholar]
- Adams, B.G.; Houston, M.N.; Cameron, K.L. The epidemiology of meniscus injury. Sports Med. Arthrosc. 2021, 29, e24–e33. [Google Scholar] [CrossRef] [PubMed]
- Marcacci, M.; Marcheggiani-Muccioli, G.M.; Grassi, A.; Ricci, M.; Tsapralis, K.; Nanni, G.; Bonanzinga, T.; Zaffagnini, S. Arthroscopic meniscus allograft transplantation in male professional soccer players: A 36-month follow-up study. Am. J. Sport Med. 2014, 42, 382–388. [Google Scholar] [CrossRef] [PubMed]
- Jeong, H.J.; Lee, S.H.; Ko, C.S. Meniscectomy. Knee Surg. Relat. Res. 2012, 24, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.H.; D’Lima, D.D.; Lee, S.H. Clinical and radiographic results of partial versus total meniscectomy in patients with symptomatic discoid lateral meniscus: A systematic review and meta-analysis. Orthop. Traumatol. Surg. Res. 2019, 105, 669–675. [Google Scholar] [CrossRef] [PubMed]
- Reito, A.; Harris, I.A.; Karjalainen, T. Arthroscopic partial meniscectomy: Did it ever work? A narrative review from basic research to proposed disease framework and science of clinical practice. Acta Orthop. 2021, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Campos-Vázquez, M.A. Propuesta de readaptación tras meniscectomía parcial en futbolistas. Apunts 2012, 47, 105–112. [Google Scholar] [CrossRef]
- Lavoie-Gagne, O.Z.; Korrapati, A.; Retzky, J.; Bernstein, D.N.; Diaz, C.C.; Berlinberg, E.J.; Forlenza, E.M.; Fury, M.S.; Mehta, N.; O’Donnell, E.A.; et al. Return to Play and Player Performance After Meniscal Tear Among Elite-Level European Soccer Players: A Matched Cohort Analysis of Injuries From 2006 to 2016. Orthop. J. Sport Med. 2022, 10, 23259671211059541. [Google Scholar] [CrossRef]
- Núñez-Sánchez, F.J.; Cabrera, F.I.M.; Abad, F.H.; Suárez-Arrones, L. Progressive Rehabilitation of a Professional Soccer Player After an Anterior Cruciate Ligament Reconstruction in Phase 1: Clinical Perspective with Video Demonstration. J. Athl. Train. 2021, 56, 1132–1136. [Google Scholar] [CrossRef] [PubMed]
- Roos, E.M.; Östenberg, A.; Roos, H.; Ekdahl, C.; Lohmander, L.S. Long-term outcome of meniscectomy: Symptoms, function, and performance tests in patients with or without radiographic osteoarthritis compared to matched controls. Osteoarthr. Cartil. 2001, 9, 316–324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matthews, P.; St-Pierre, D.M. Recovery of muscle strength following arthroscopic meniscectomy. J. Orthop. Sport Phys. Ther. 1996, 23, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Chambless, D.L.; Hollon, S.D. Defining empirically supported therapies. J. Consult. Clin. Psych. 1998, 66, 7–18. [Google Scholar] [CrossRef]
- Criado, L.; de La Fuente, A.; Heredia, M.; Montero, J.; Albaladejo, A.; Criado, J.-M. Electromyographic biofeedback training for reducing muscle pain and tension on masseter and temporal muscles: A pilot study. J. Clin. Exp. Dent. 2016, 8, e571–e576. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. World medical association declaration of Helsinki: Ethical principles for medical research involving human subjects. J. Am. Med. Assoc. 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [Green Version]
- Solé, V.; Moliner, L. Metodología para el estudio de la fatiga y la contracción muscular. Rehabilitación 1988, 22, 37–50. [Google Scholar]
- Krebs, D.E.; Staples, W.H.; Cuttita, D.; Zickel, R.E. Knee joint angle: Its relationship to quadriceps femoris activity in normal and postarthrotomy limbs. Arch. Phys. Med. Rehab. 1983, 64, 441–447. [Google Scholar]
- SAS Institute. User’s Guide, 8th ed.; SAS/STAT SAS Institute: Cary, NC, USA, 1999. [Google Scholar]
- Schlotzhauer, S.D.; Littell, R. SAS System for Elementary Statistical Analysis; SAS Institute Inc.: Cary, NC, USA, 1997. [Google Scholar]
- Hernández-Mendo, A.; Blanco-Villaseñor, A.; Pastrana, J.L.; Morales-Sánchez, V.; Ramos-Pérez, F.J. SAGT: New software for generalizability analysis. Rev. Iberoam. Psicol. Ejerc. Deporte 2016, 11, 77–89. [Google Scholar]
- Hemmerle, W.; Hartley, H. Computing maximum likelihood estimates for the mixed AOV Model using the w-transformation. Technometrics 1973, 15, 819–831. [Google Scholar] [CrossRef]
- Searle, S.; Casella, G.; McCulloch, C. Variance Components; John Wiley & Sons: New York, NY, USA, 1992. [Google Scholar] [CrossRef]
- Valera-Calero, J.A.; Fernández-de-Las-Peñas, C.; Varol, U.; Ortega-Santiago, R.; Gallego-Sendarrubias, G.M.; Arias-Buría, J.L. Ultrasound imaging as a visual biofeedback tool in rehabilitation: An updated systematic review. Int. J. Environ. Res. Public Health 2021, 18, 7554. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Sources of Variation | Sum of Squares | Degrees of Freedom | Average Square | Random Comp. | Mixed Comp. | Corrected Comp. | % | Standard Error | |
|---|---|---|---|---|---|---|---|---|---|
| EMG-Means. | [p] | 114,837.542 | 9 | 12,759.727 | −144.637 | −144.637 | −144.637 | 0 | 121.871 |
| [t] | 1,093,841.16 | 1 | 1,093,841.16 | 3614.682 | 3614.682 | 3614.682 | 34.885 | 2977.089 | |
| [p][t] | 85,850.05 | 9 | 9538.894 | 307.165 | 307.165 | 307.165 | 2.964 | 135.59 | |
| [b] | 1,348,437.57 | 2 | 674,218.784 | 3329.438 | 3329.438 | 3329.438 | 32.132 | 2383.76 | |
| [p][b] | 149,522.483 | 18 | 8306.805 | 402.547 | 402.547 | 402.547 | 3.885 | 131.35 | |
| [t][b] | 0 | 2 | 0 | 0 | 0 | 0 | 0 | 0 | |
| [p][t][b] | 0 | 18 | 0 | 0 | 0 | 0 | 0 | 0 | |
| [n] | 1,047,707.54 | 9 | 116,411.949 | 1871.96 | 1871.96 | 1871.96 | 18.066 | 827.377 | |
| [p][n] | 337,938.074 | 81 | 4172.075 | 598.708 | 598.708 | 598.708 | 5.778 | 108.366 | |
| [t][n] | 1995.732 | 9 | 221.748 | −3.407 | −3.407 | −3.407 | 0 | 3.57 | |
| [p][t][n] | 26,240.469 | 81 | 323.956 | 107.985 | 107.985 | 107.985 | 1.042 | 16.763 | |
| [b][n] | 5046.168 | 18 | 280.343 | 1.223 | 1.223 | 1.223 | 0.012 | 4.652 | |
| [p][b][n] | 41,451.469 | 162 | 255.873 | 127.937 | 127.937 | 127.937 | 1.235 | 14.128 | |
| [t][b][n] | 0 | 18 | 0 | 0 | 0 | 0 | 0 | 0 | |
| [p][t][b][n] | 0 | 162 | 0 | 0 | 0 | 0 | 0 | 0 | |
| EMG-Maximum | [p] | 1,676,104.52 | 9 | 186,233.835 | 1367.702 | 1367.702 | 1367.702 | 4.142 | 1443.346 |
| [t] | 5,934,252.8 | 1 | 5,934,252.8 | 19,517.865 | 19,517.865 | 19,517.865 | 59.109 | 16,151.388 | |
| [p][t] | 717,267.103 | 9 | 79,696.345 | 2618.238 | 2618.238 | 2618.238 | 7.929 | 1132.77 | |
| [b] | 1,946,405.58 | 2 | 973,202.79 | 4768.066 | 4768.066 | 4768.066 | 14.44 | 3440.929 | |
| [p][b] | 350,381.772 | 18 | 19,465.654 | 968.568 | 968.568 | 968.568 | 2.933 | 307.779 | |
| [t][b] | 0 | 2 | 0 | 0 | 0 | 0 | 0 | 0 | |
| [p][t][b] | 0 | 18 | 0 | 0 | 0 | 0 | 0 | 0 | |
| [n] | 1,404,654.19 | 9 | 156,072.688 | 2508.311 | 2508.311 | 2508.311 | 7.596 | 1109.286 | |
| [p][n] | 506,508.931 | 81 | 6253.197 | 834.949 | 834.949 | 834.949 | 2.529 | 164.499 | |
| [t][n] | 3115.654 | 9 | 346.184 | −26.768 | −26.768 | −26.768 | 0 | 7.718 | |
| [p][t][n] | 93,086.762 | 81 | 1149.219 | 383.073 | 383.073 | 383.073 | 1.16 | 59.464 | |
| [b][n] | 3926.932 | 18 | 218.163 | 6.194 | 6.194 | 6.194 | 0.019 | 3.489 | |
| [p][b][n] | 15,274.282 | 162 | 94.286 | 47.143 | 47.143 | 47.143 | 0.143 | 5.206 | |
| [t][b][n] | 0 | 18 | 0 | 0 | 0 | 0 | 0 | 0 | |
| [p][t][b][n] | 0 | 162 | 0 | 0 | 0 | 0 | 0 | 0 |
| EMG Means | EMG Maximum | |||
|---|---|---|---|---|
| Relative G ξρ2(δ) | Absolute G ξρ2(Δ) | Relative G ξρ2(δ) | Absolute G ξρ2(Δ) | |
| [t] [b] [n]/[p] | 0.983 | 0.983 | 0.982 | 0.977 |
| [p] [t] [b]/[n] | 0.989 | 0.966 | 0.996 | 0.987 |
| [p] [t] [n]/[b] | 0.973 | 0.835 | 0.988 | 0.934 |
| [p] [b] [n]/[t] | 0.968 | 0.759 | 0.875 | 0.483 |
| [t] [b]/[p] [n] | 0.990 | 0.963 | 0.985 | 0.970 |
| [t] [n]/[p] [b] | 0.981 | 0.817 | 0.983 | 0.911 |
| [b] [n]/[p] [t] | 0.978 | 0.728 | 0.973 | 0.416 |
| Electromyographic Activity (μV) | |||||
|---|---|---|---|---|---|
| Values | M | SD | S | K | |
| Trials without BF (before and after) | Maximum | 422.27 | 88.79 | −0.08 | −1.24 |
| Mean | 256.89 | 72.59 | 0.18 | −1.16 | |
| Pre-BF intervention trials | Maximum | 357.63 | 54.18 | 1.62 | 5.67 |
| Mean | 202.89 | 45.03 | 1.85 | 5.05 | |
| Post-BF intervention trials | Maximum | 486.53 | 67.23 | −2.22 | 5.19 |
| Mean | 310.45 | 51.92 | −0.98 | 2.12 | |
| Trials with BF | Maximum | 578.42 | 122.78 | 0.04 | −0.73 |
| Mean | 322.98 | 74.12 | −0.02 | −0.70 | |
| Electromyographic Activity (μV) | ||||||
|---|---|---|---|---|---|---|
| Values | M | SD | S | K | ||
| Trials before BF | Session 1 | Maximum | 338.98 | 50.22 | −0.89 | 1.89 |
| Mean | 181.70 | 37.41 | −1.04 | 0.24 | ||
| Session 10 | Maximum | 383.52 | 74.81 | 2.39 | 5.09 | |
| Mean | 213.68 | 59.77 | 2.14 | 4.75 | ||
| Trials after BF | Session 1 | Maximum | 570.19 | 165.76 | −0.04 | −1.37 |
| Mean | 277.28 | 92.32 | 0.30 | −1.03 | ||
| Session 10 | Maximum | 591.07 | 101.98 | 0.30 | −0.37 | |
| Mean | 344.85 | 73.31 | 0.20 | −0.52 | ||
| Trials with BF | Session 1 | Maximum | 455.27 | 86.89 | −1.81 | 3.22 |
| Mean | 269.57 | 78.14 | −0.47 | −1.36 | ||
| Session 10 | Maximum | 520.56 | 37.78 | 3.41 | 2.74 | |
| Mean | 336.87 | 47.43 | 1.79 | 5.58 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morales-Sánchez, V.; Falcó, C.; Hernández-Mendo, A.; Reigal, R.E. Efficacy of Electromyographic Biofeedback in Muscle Recovery after Meniscectomy in Soccer Players. Sensors 2022, 22, 4024. https://doi.org/10.3390/s22114024
Morales-Sánchez V, Falcó C, Hernández-Mendo A, Reigal RE. Efficacy of Electromyographic Biofeedback in Muscle Recovery after Meniscectomy in Soccer Players. Sensors. 2022; 22(11):4024. https://doi.org/10.3390/s22114024
Chicago/Turabian StyleMorales-Sánchez, Verónica, Coral Falcó, Antonio Hernández-Mendo, and Rafael E. Reigal. 2022. "Efficacy of Electromyographic Biofeedback in Muscle Recovery after Meniscectomy in Soccer Players" Sensors 22, no. 11: 4024. https://doi.org/10.3390/s22114024
APA StyleMorales-Sánchez, V., Falcó, C., Hernández-Mendo, A., & Reigal, R. E. (2022). Efficacy of Electromyographic Biofeedback in Muscle Recovery after Meniscectomy in Soccer Players. Sensors, 22(11), 4024. https://doi.org/10.3390/s22114024