
Diagnostics of Articular Cartilage Damage Based on Generated Acoustic Signals Using ANN—Part II: Patellofemoral Joint

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Physical Examination
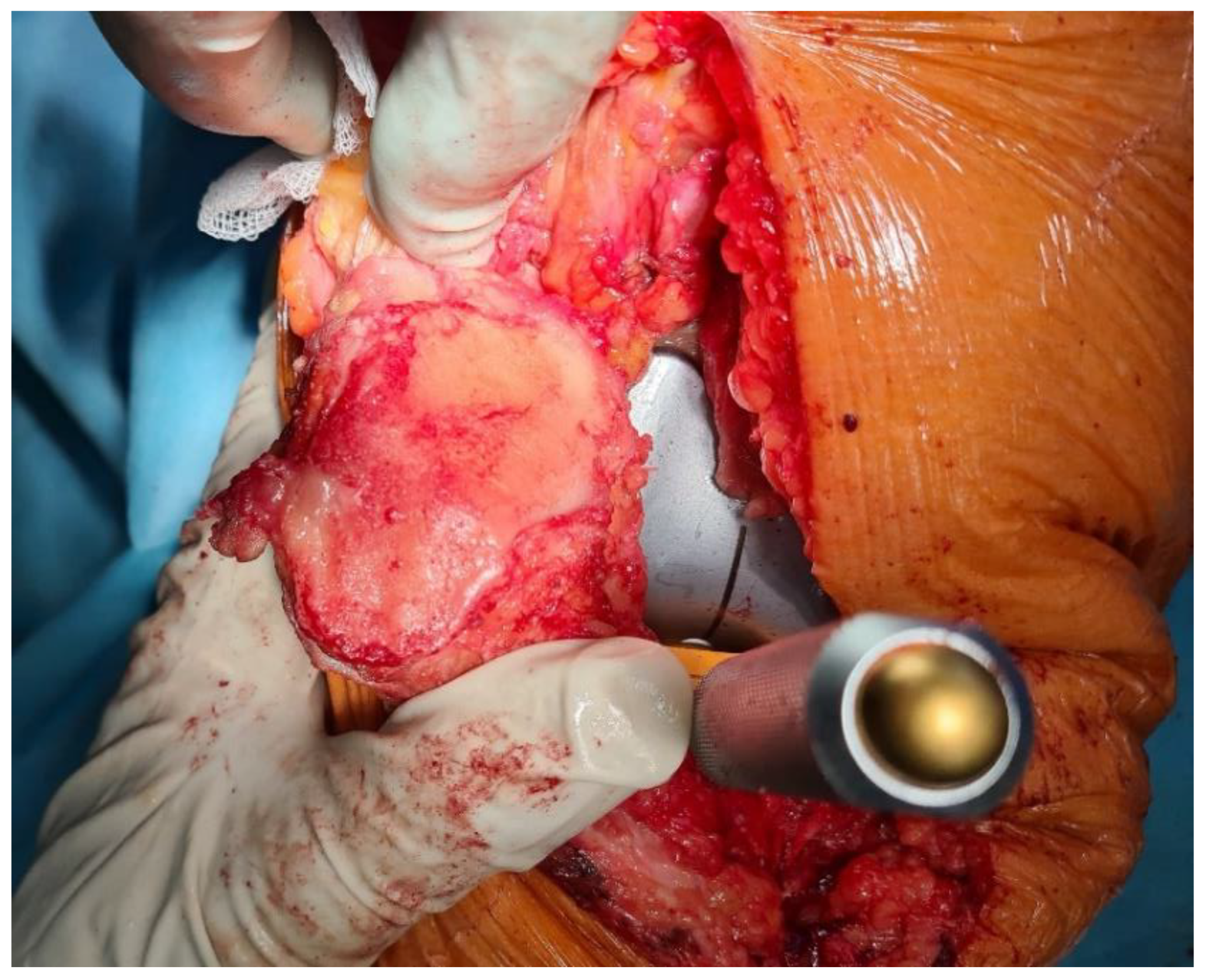
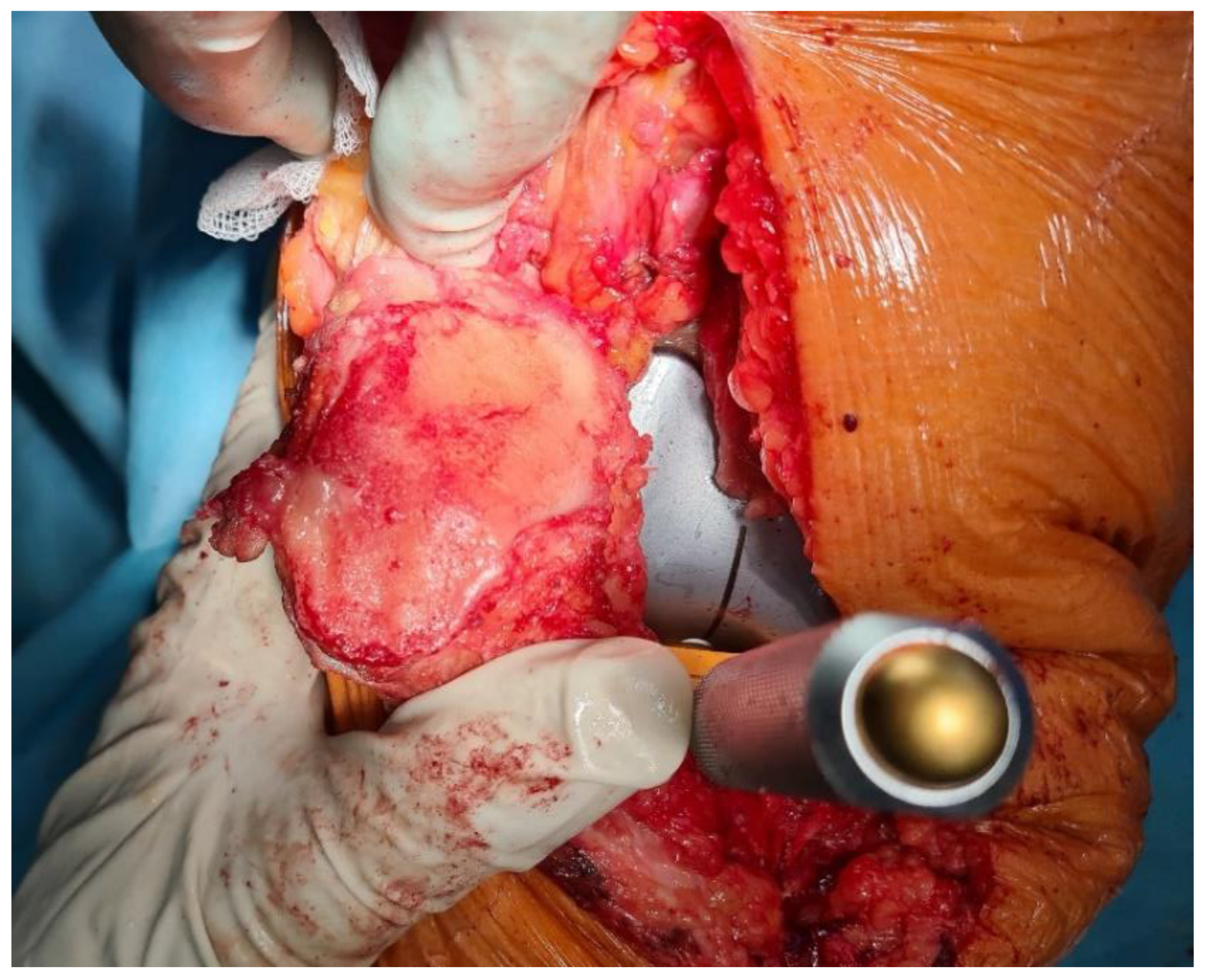
2.3. Surgical Treatment
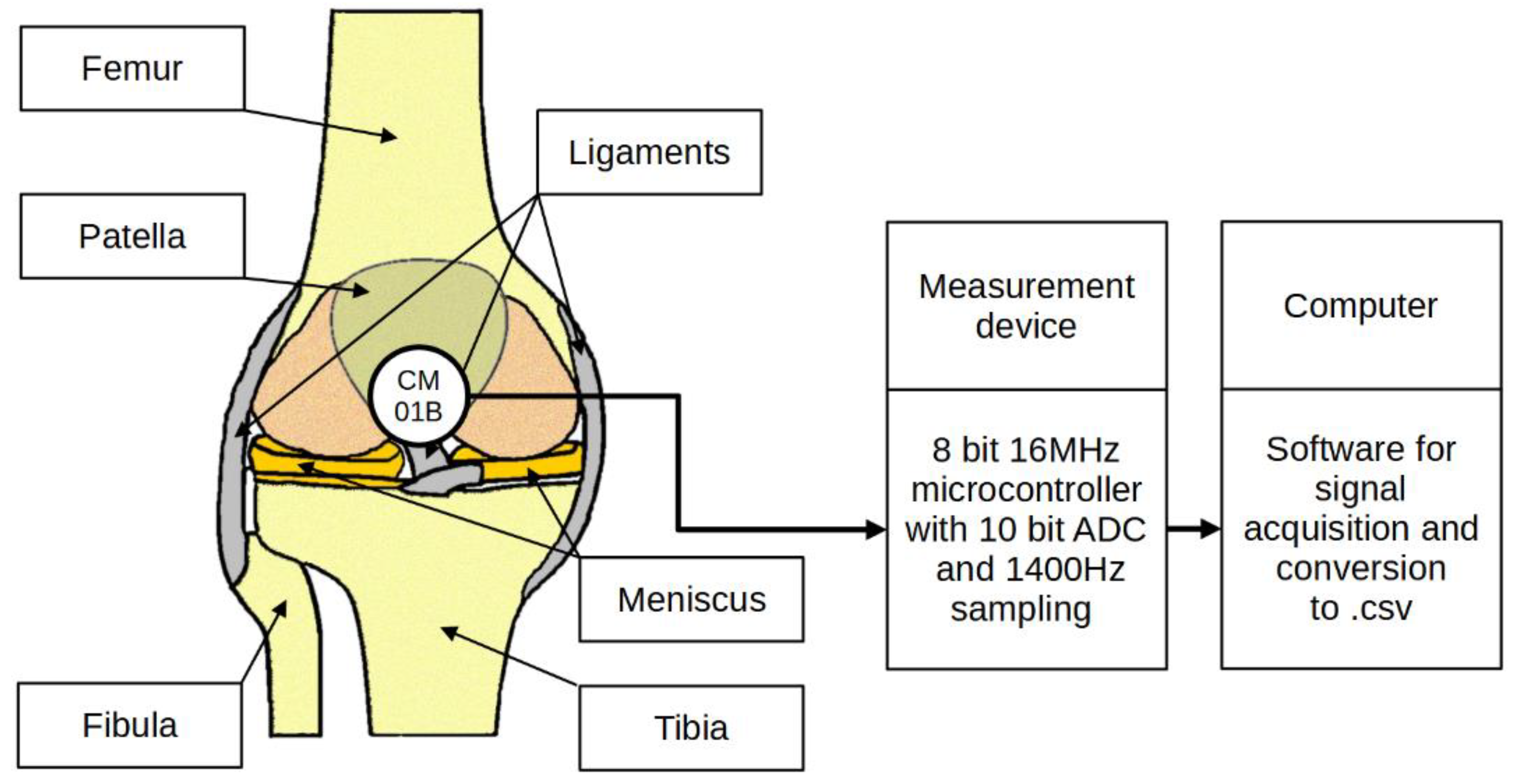
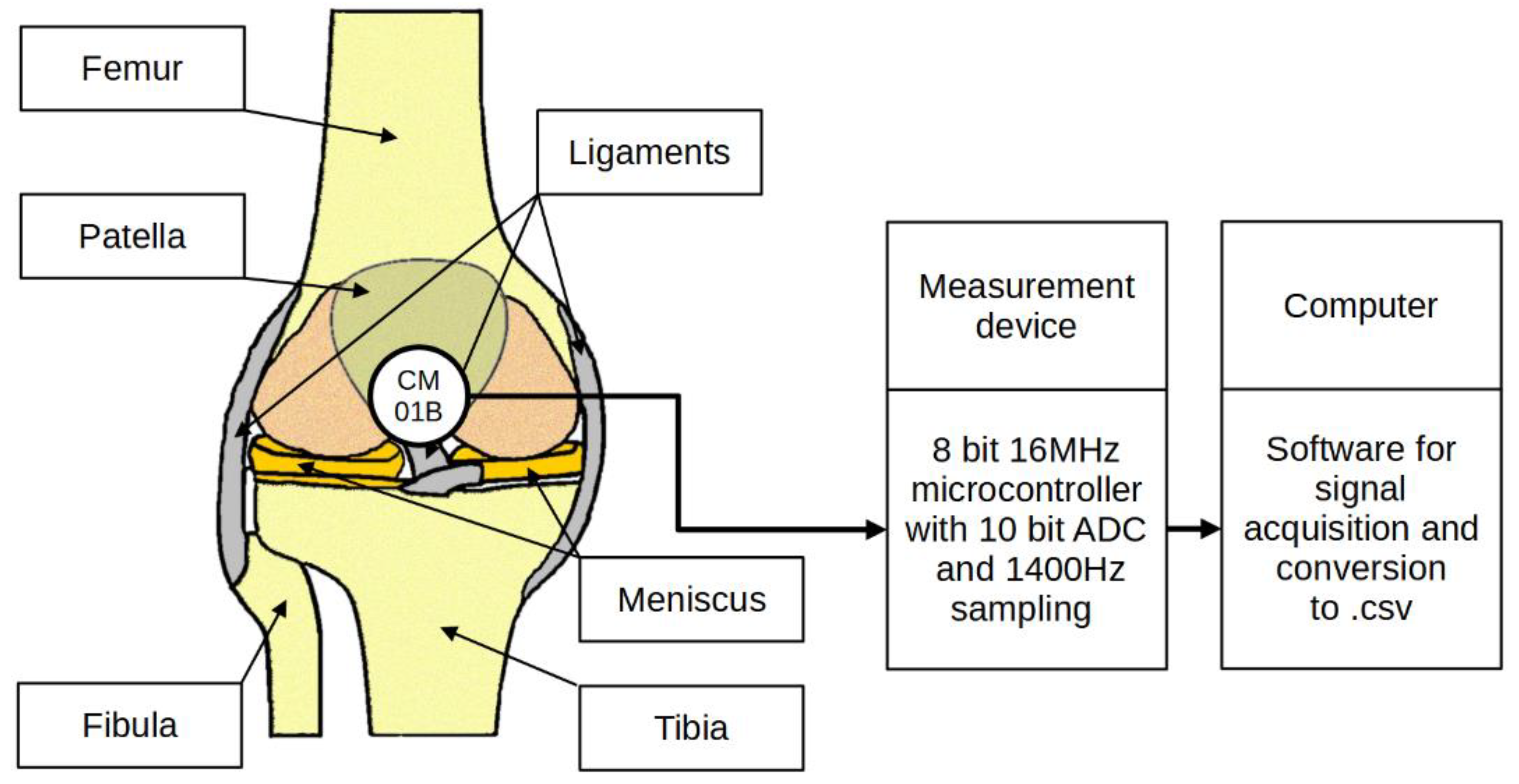
2.4. Signal Acquisition
- Orthesis with a rotary encoder and vibration transducer;
- Microcontroller with peripherals for signal acquisition;
- Computer with data recording software.
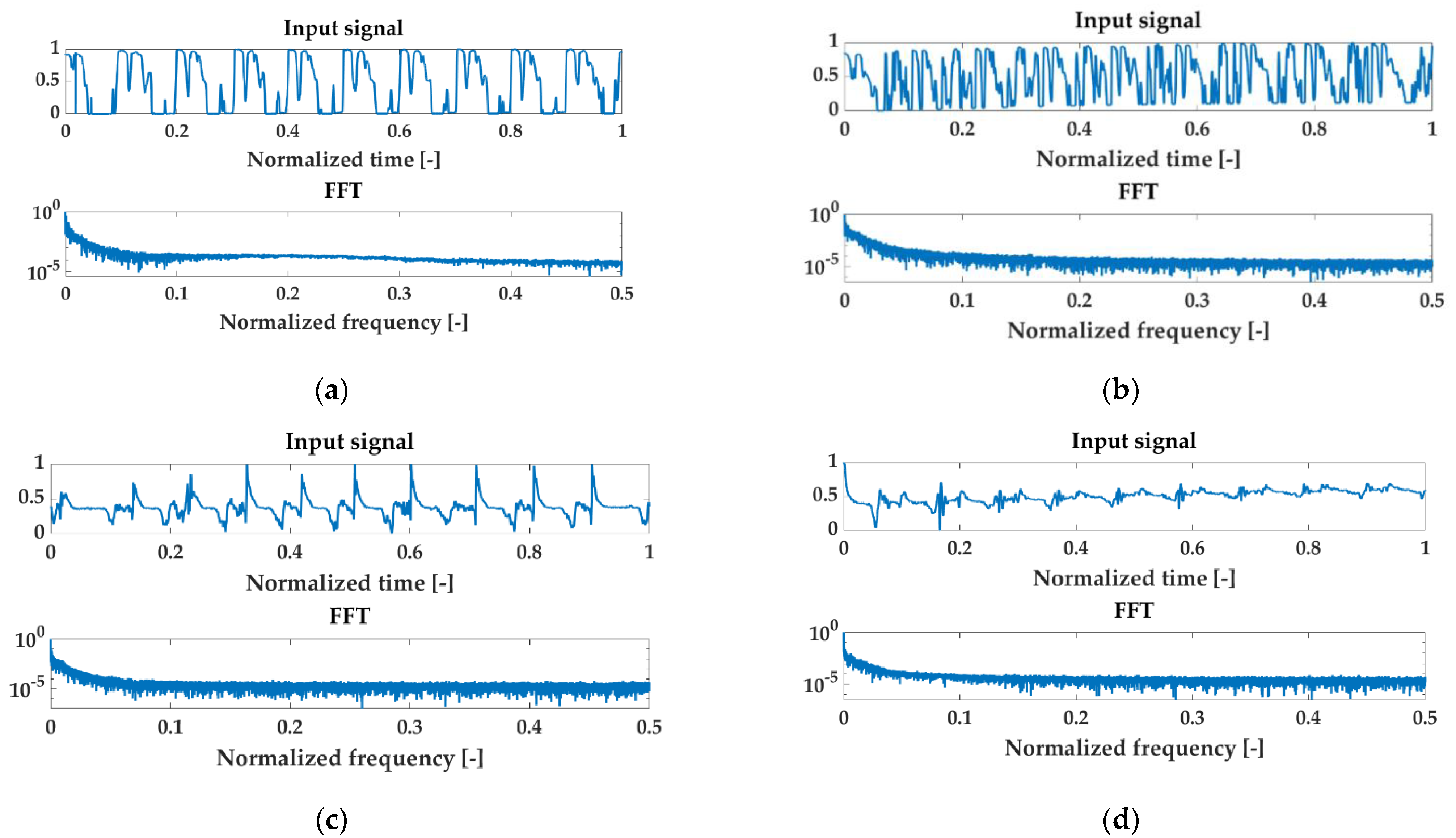
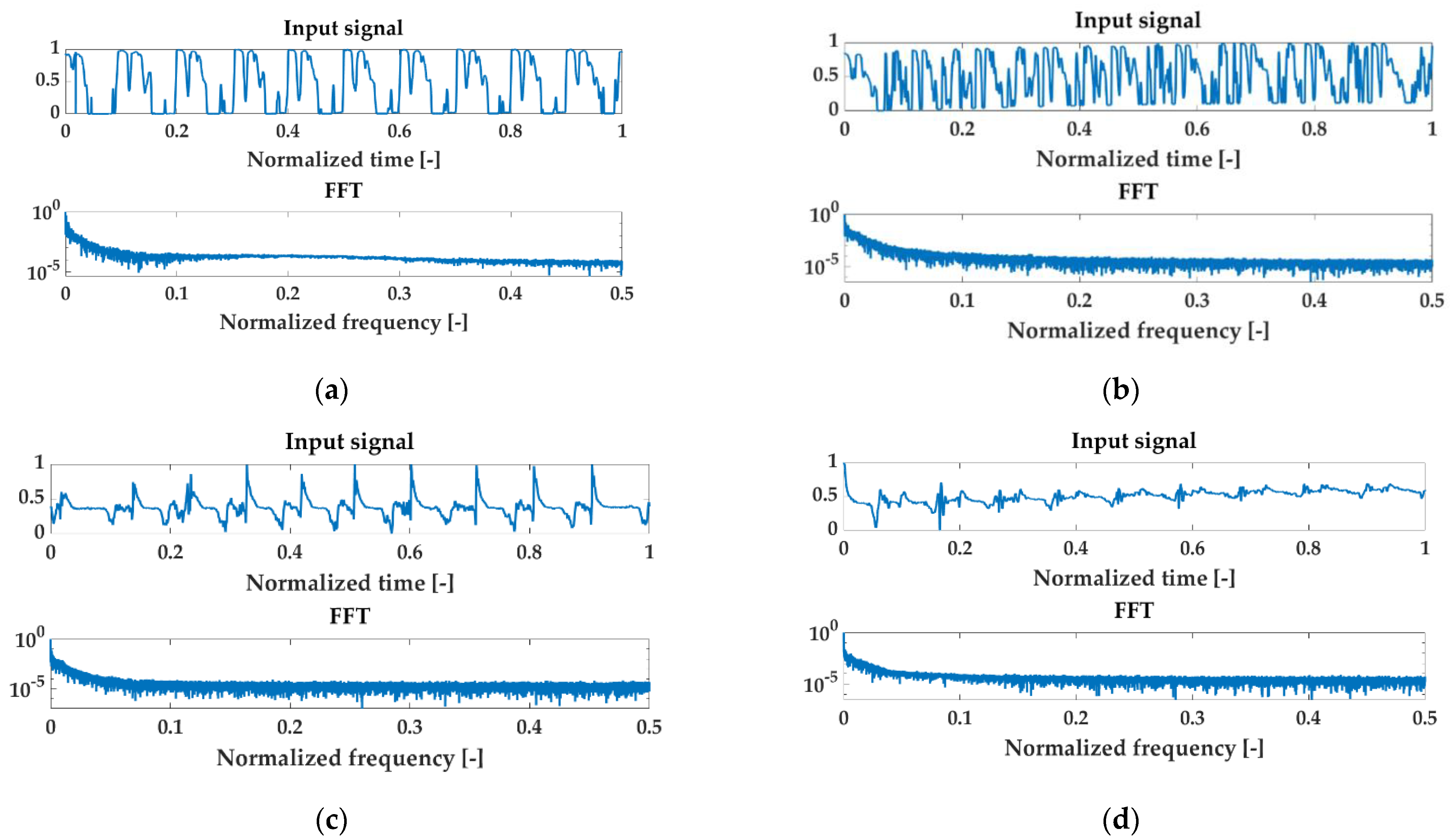
2.5. Signal Preprocessing
2.6. Feature Extraction
- The mean value (MV) is one of the most popular intuitive descriptive statistics. It is the sum of the values of a measurable characteristic divided by the number of units of a finite statistical population.where:is the value of the discrete signal at the nth point, n = 1, …, N;is the number of samples in the signal.
- The straightened average value (SA) is the average value from the absolute value; the use of this parameter allows eliminating the phenomenon of the average value approaching zero, especially visible for oscillatory signals.
- The root mean square (RMS) is defined as the square root of the mean square. This parameter is not sensitive to sudden changes manifested by single peaks in the signal.
- The peak value (PV), also called the maximum value of the signal, as opposed to RMS, is an indicator that is highly sensitive to rapid changes in the state of the test objects.
- The peak to peak value (PPV) is the amplitude measured from the largest top to the largest bottom of the wave, unlike PV, the two extremes, smallest and largest, are considered.
- The crest factor (CF) is a measure that gives the ratio of the peak value (PV) to the RMS value of the signal.
- The impact factor (IF) is defined similarly to the CF, except that the denominator in this case is the mean value (MV). Its diagnostic properties are also similar to those of CF, but it is more sensitive.
- The shape factor (SF) is a measure giving the ratio of the RMS value to the mean of the absolute value (SA).
- The variance (VAR) is a measure of the dispersion of the sample results around the distribution center; it is the expected value of the square of the variance of a random variable minus its population mean.
- Kurtosis (KUR) is a measure that describes the degree of concentration of outcomes in a distribution. It is a fourth-order central moment. It provides information about the degree of similarity of the data scattered around the mean with respect to a normal distribution.
- The M6A parameter is the sixth central moment normalized by the variance raised to the third power. This coefficient is more sensitive to the presence of pulses in the signal. It is defined as:
- The M8A parameter is known as the eighth central moment, normalized by the variance to the fourth power. It is defined as:
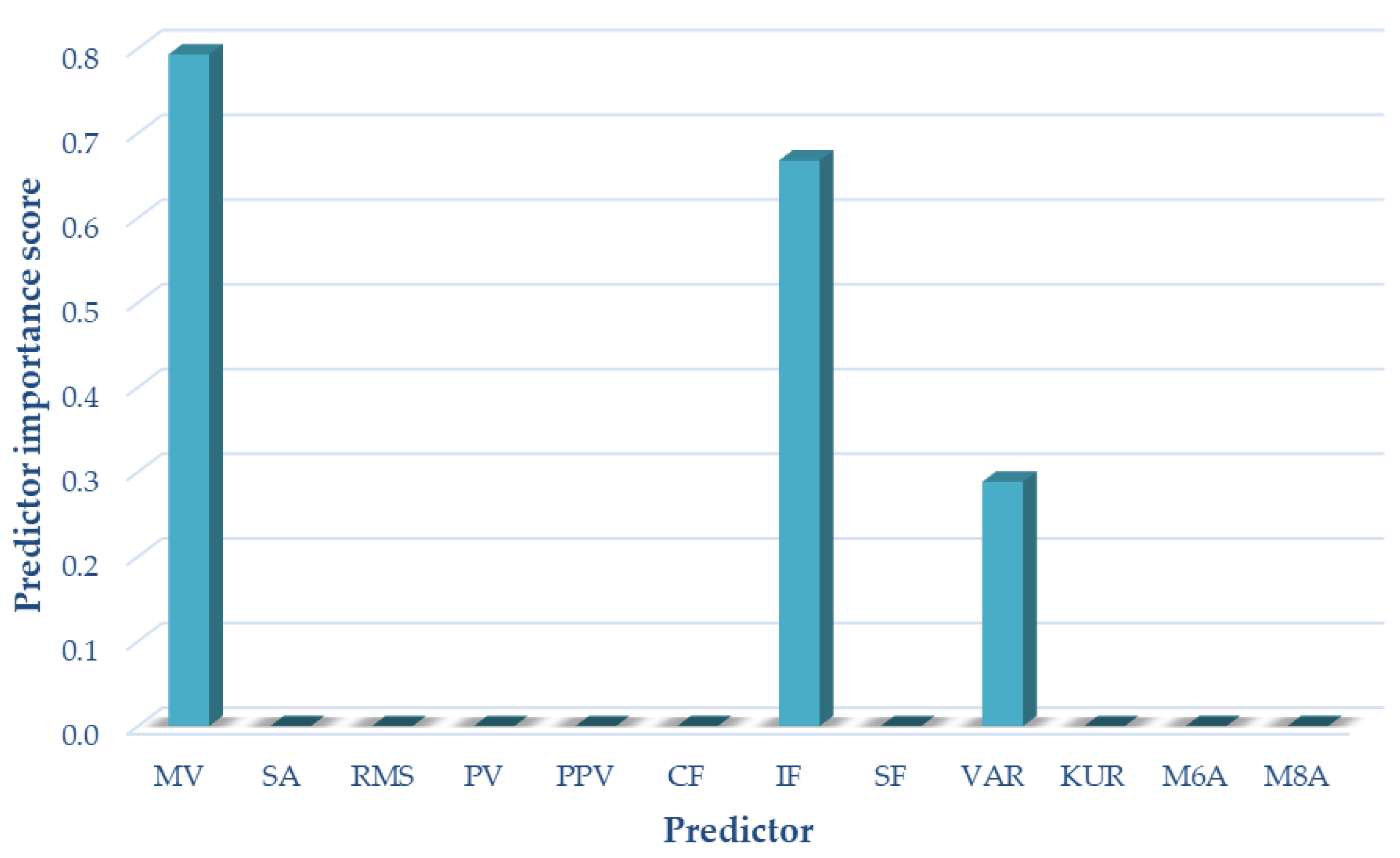
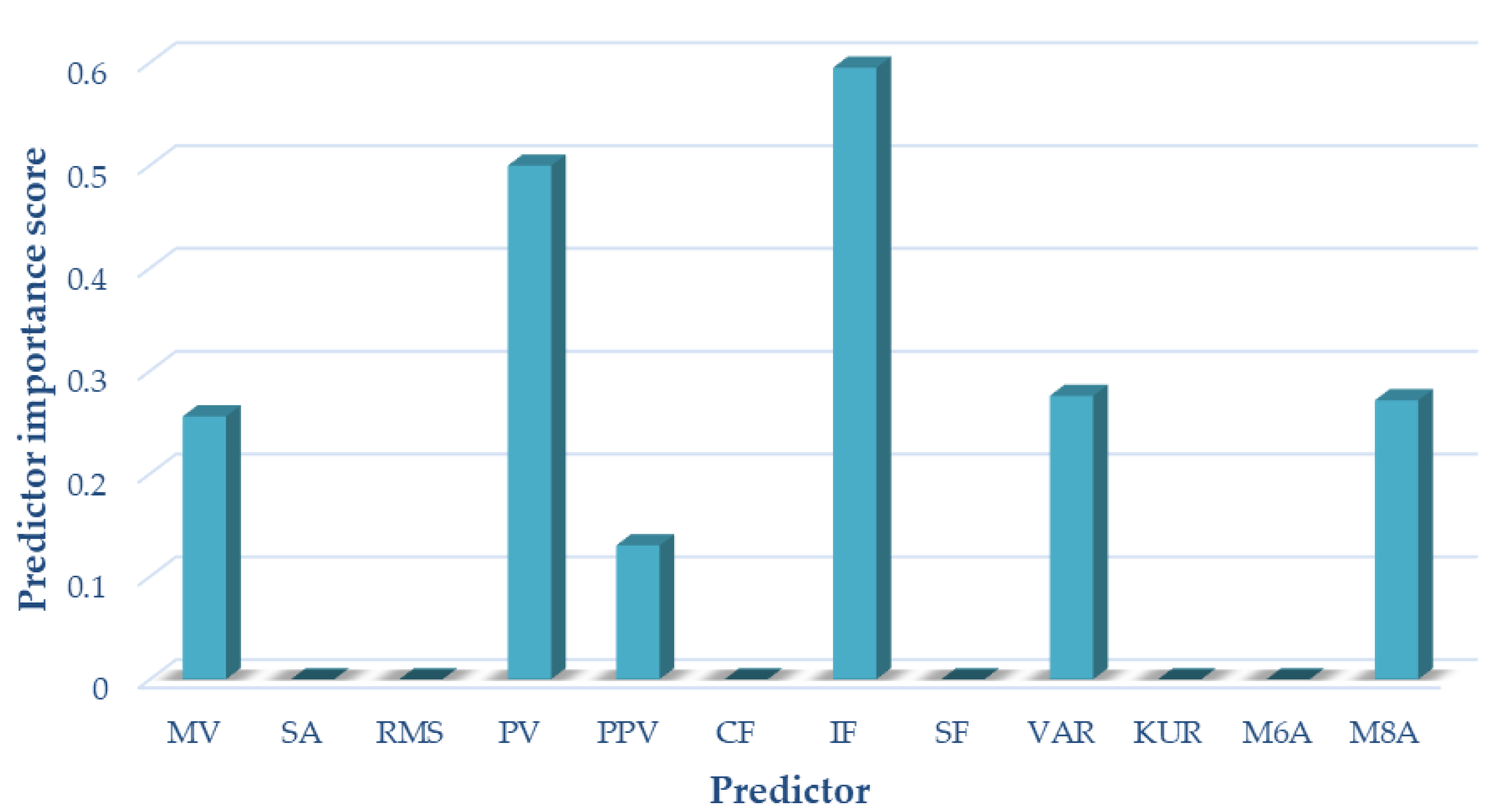
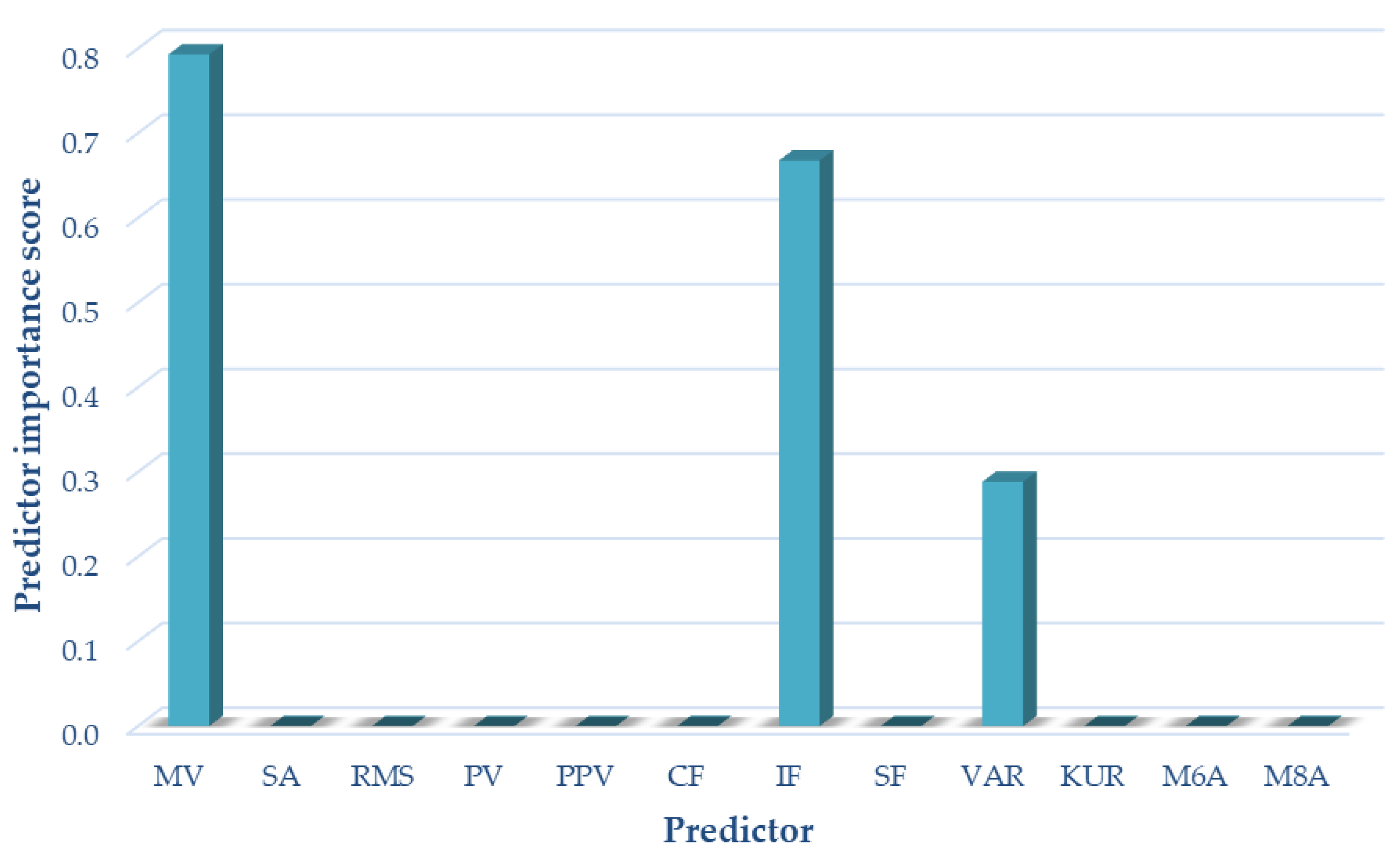
2.7. Selection of Optimal Signal Features
2.8. Artificial Neural Networks
3. Results and Discussion
3.1. Selection of Optimal Signal Features
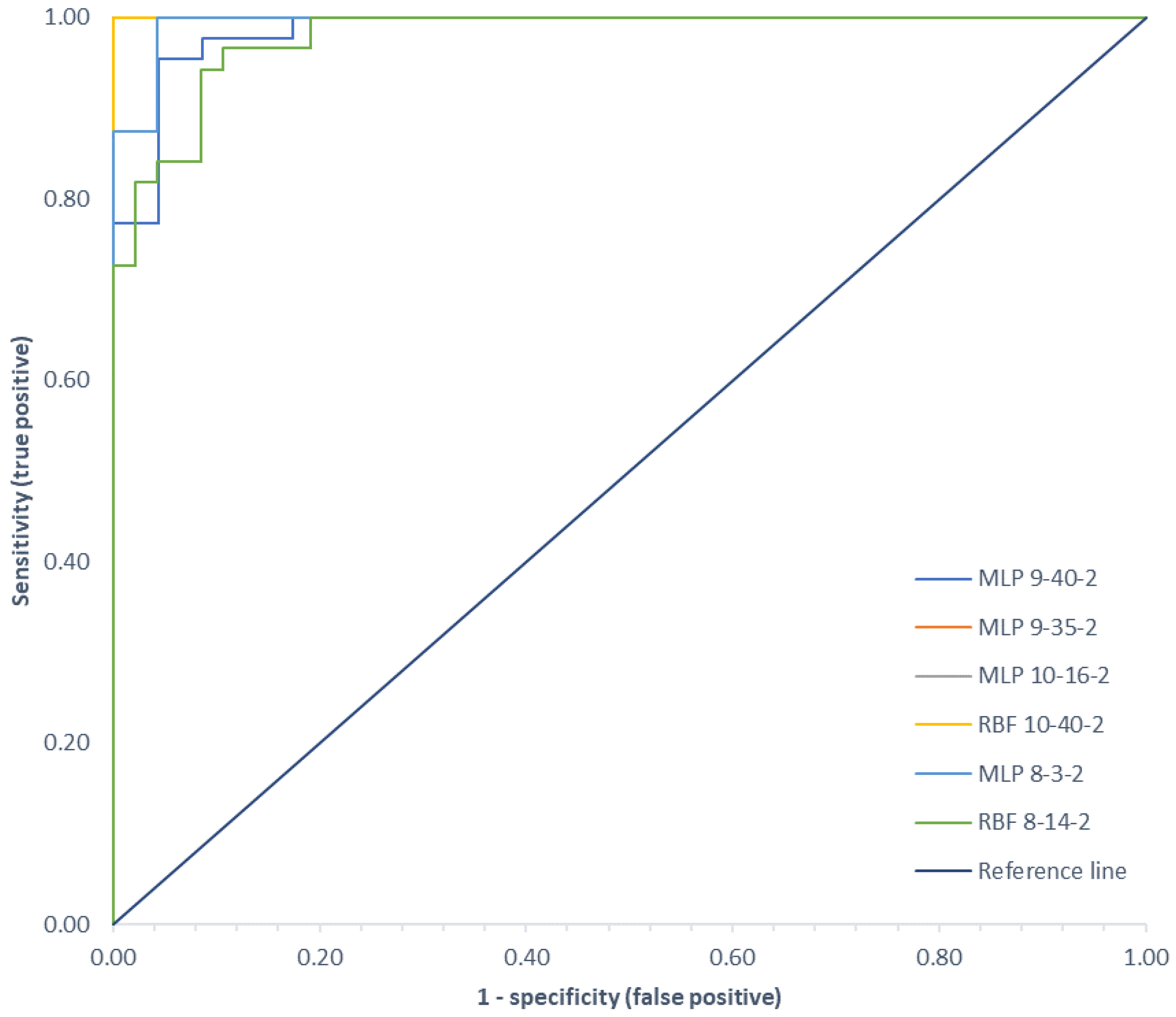
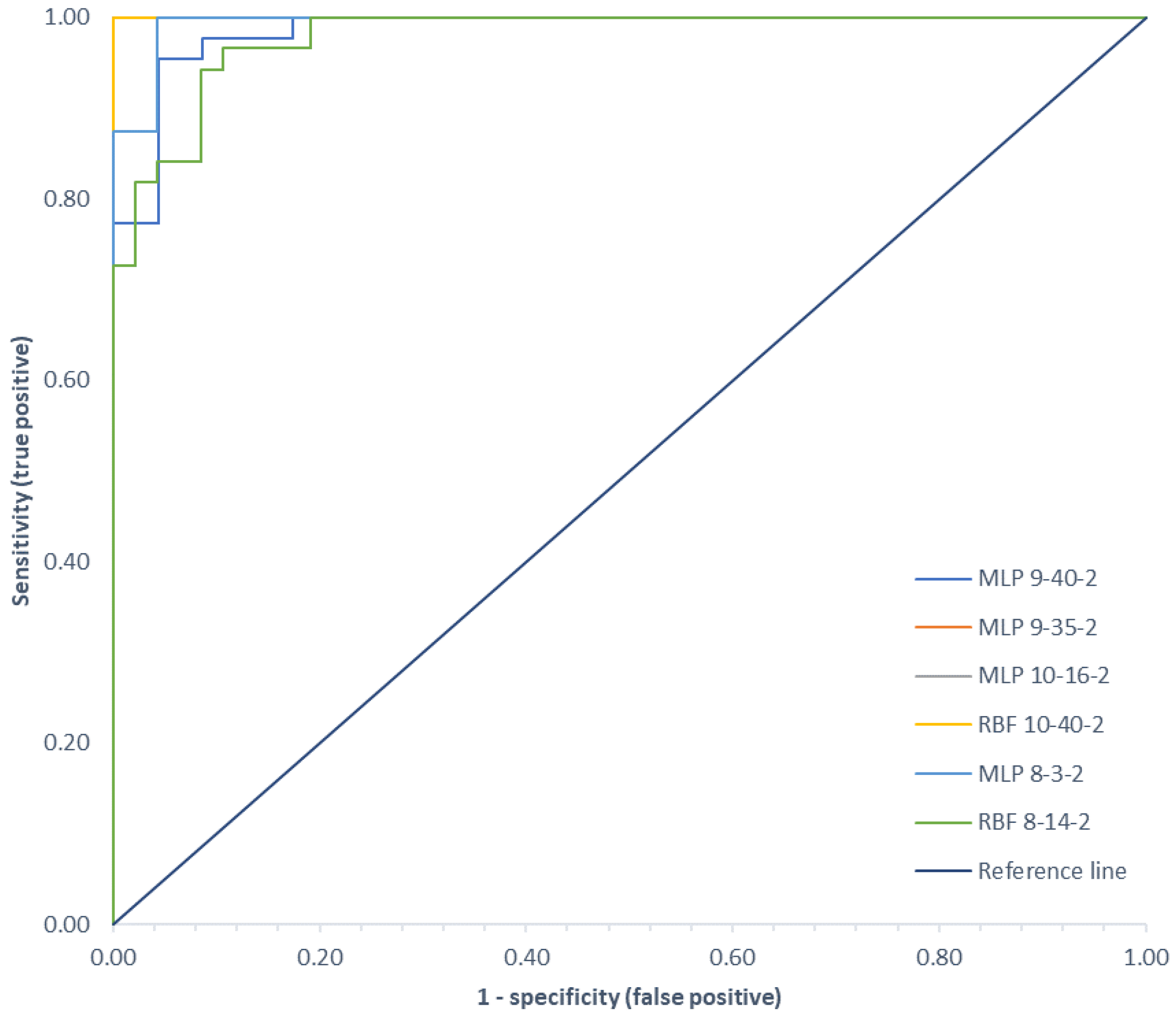
3.2. Classification
3.3. Limitations of the Study and Future Plans
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Crossley, K.M.; Stefanik, J.J.; Selfe, J.; Collins, N.J.; Davis, I.S.; Powers, C.M.; McConnell, J.; Vicenzino, B.; Bazett-Jones, D.M.; Esculier, J.-F.; et al. 2016 Patellofemoral Pain Consensus Statement from the 4th International Patellofemoral Pain Research Retreat, Manchester. Part 1: Terminology, Definitions, Clinical Examination, Natural History, Patellofemoral Osteoarthritis and Patient-Reported Outcome Measures. Br. J. Sports Med. 2016, 50, 839–843. [Google Scholar] [CrossRef] [PubMed]
- Loudon, J.K. Biomechanics and Pathomechanics of the Patellofemoral Joint. Int. J. Sports Phys. Ther. 2016, 11, 820–830. [Google Scholar] [PubMed]
- Goldring, M.B. Update on the Biology of the Chondrocyte and New Approaches to Treating Cartilage Diseases. Best Pract. Res. Clin. Rheumatol. 2006, 20, 1003–1025. [Google Scholar] [CrossRef] [PubMed]
- Cibere, J.; Sayre, E.C.; Guermazi, A.; Nicolaou, S.; Kopec, J.A.; Esdaile, J.M.; Thorne, A.; Singer, J.; Wong, H. Natural History of Cartilage Damage and Osteoarthritis Progression on Magnetic Resonance Imaging in a Population-Based Cohort with Knee Pain. Osteoarthr. Cartil. 2011, 19, 683–688. [Google Scholar] [CrossRef] [Green Version]
- Brody, L. Knee Osteoarthritis: Clinical Connections to Articular Cartilage Structure and Function. Phys. Ther. Sport 2015, 16, 301–316. [Google Scholar] [CrossRef]
- Grelsamer, R.P. Patellar Malalignment. J. Bone Jt. Surg. Am. 2000, 82, 1639–1650. [Google Scholar] [CrossRef]
- Grelsamer, R.P.; Weinstein, C.H. Applied Biomechanics of the Patella. Clin. Orthop. Relat. Res. 2001, 389, 9–14. [Google Scholar] [CrossRef]
- Cohen, Z.A.; Roglic, H.; Grelsamer, R.P.; Henry, J.H.; Levine, W.N.; Van Mow, C.; Ateshian, G.A. Patellofemoral Stresses during Open and Closed Kinetic Chain Exercises: An Analysis Using Computer Simulation. Am. J. Sports Med. 2001, 29, 480–487. [Google Scholar] [CrossRef]
- Krakowski, P.; Nogalski, A.; Jurkiewicz, A.; Karpiński, R.; Maciejewski, R.; Jonak, J. Comparison of Diagnostic Accuracy of Physical Examination and MRI in the Most Common Knee Injuries. Appl. Sci. 2019, 9, 4102. [Google Scholar] [CrossRef] [Green Version]
- Davies, A.P.; Vince, A.S.; Shepstone, L.; Donell, S.T.; Glasgow, M.M. The Radiologic Prevalence of Patellofemoral Osteoarthritis. Clin. Orthop. Relat. Res. 2002, 402, 206–212. [Google Scholar] [CrossRef]
- McAlindon, T.E.; Bannuru, R.R.; Sullivan, M.C.; Arden, N.K.; Berenbaum, F.; Bierma-Zeinstra, S.M.; Hawker, G.A.; Henrotin, Y.; Hunter, D.J.; Kawaguchi, H.; et al. OARSI Guidelines for the Non-Surgical Management of Knee Osteoarthritis. Osteoarthr. Cartil. 2014, 22, 363–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jevsevar, D.S. Treatment of Osteoarthritis of the Knee: Evidence-Based Guideline, 2nd Edition. J. Am. Acad. Orthop. Surg. 2013, 21, 571–576. [Google Scholar] [CrossRef] [PubMed]
- Krakowski, P.; Karpiński, R.; Maciejewski, R.; Jonak, J.; Jurkiewicz, A. Short-Term Effects of Arthroscopic Microfracturation of Knee Chondral Defects in Osteoarthritis. Appl. Sci. 2020, 10, 8312. [Google Scholar] [CrossRef]
- Sánchez-Romero, E.A.; González-Zamorano, Y.; Arribas-Romano, A.; Martínez-Pozas, O.; Fernández Espinar, E.; Pedersini, P.; Villafañe, J.H.; Alonso Pérez, J.L.; Fernández-Carnero, J. Efficacy of Manual Therapy on Facilitatory Nociception and Endogenous Pain Modulation in Older Adults with Knee Osteoarthritis: A Case Series. Appl. Sci. 2021, 11, 1895. [Google Scholar] [CrossRef]
- Imhoff, A.B.; Feucht, M.J.; Meidinger, G.; Schöttle, P.B.; Cotic, M. Prospective Evaluation of Anatomic Patellofemoral Inlay Resurfacing: Clinical, Radiographic, and Sports-Related Results after 24 Months. Knee Surg. Sports Traumatol. Arthrosc. 2015, 23, 1299–1307. [Google Scholar] [CrossRef]
- Kellgren, J.H.; Lawrence, J.S. Radiological Assessment of Osteo-Arthrosis. Ann. Rheum. Dis. 1957, 16, 494–502. [Google Scholar] [CrossRef] [Green Version]
- Felson, D.T.; Niu, J.; Guermazi, A.; Sack, B.; Aliabadi, P. Defining Radiographic Incidence and Progression of Knee Osteoarthritis: Suggested Modifications of the Kellgren and Lawrence Scale. Ann. Rheum. Dis. 2011, 70, 1884–1886. [Google Scholar] [CrossRef] [Green Version]
- Riecke, B.F.; Christensen, R.; Torp-Pedersen, S.; Boesen, M.; Gudbergsen, H.; Bliddal, H. An Ultrasound Score for Knee Osteoarthritis: A Cross-Sectional Validation Study. Osteoarthr. Cartil. 2014, 22, 1675–1691. [Google Scholar] [CrossRef] [Green Version]
- Figueroa, D.; Calvo, R.; Vaisman, A.; Carrasco, M.A.; Moraga, C.; Delgado, I. Knee Chondral Lesions: Incidence and Correlation Between Arthroscopic and Magnetic Resonance Findings. Arthrosc. J. Arthrosc. Relat. Surg. 2007, 23, 312–315. [Google Scholar] [CrossRef]
- Bredella, M.A.; Tirman, P.F.; Peterfy, C.G.; Zarlingo, M.; Feller, J.F.; Bost, F.W.; Belzer, J.P.; Wischer, T.K.; Genant, H.K. Accuracy of T2-Weighted Fast Spin-Echo MR Imaging with Fat Saturation in Detecting Cartilage Defects in the Knee: Comparison with Arthroscopy in 130 Patients. Am. J. Roentgenol. 1999, 172, 1073–1080. [Google Scholar] [CrossRef] [Green Version]
- Krakowski, P.; Karpiński, R.; Jojczuk, M.; Nogalska, A.; Jonak, J. Knee MRI Underestimates the Grade of Cartilage Lesions. Appl. Sci. 2021, 11, 1552. [Google Scholar] [CrossRef]
- Krakowski, P.; Karpiński, R.; Maciejewski, R.; Jonak, J. Evaluation of the Diagnostic Accuracy of MRI in Detection of Knee Cartilage Lesions Using Receiver Operating Characteristic Curves. J. Phys. Conf. Ser. 2021, 1736, 012028. [Google Scholar] [CrossRef]
- Solivetti, F.M.; Guerrisi, A.; Salducca, N.; Desiderio, F.; Graceffa, D.; Capodieci, G.; Romeo, P.; Sperduti, I.; Canitano, S. Appropriateness of Knee MRI Prescriptions: Clinical, Economic and Technical Issues. La Radiol. Med. 2016, 121, 315–322. [Google Scholar] [CrossRef] [PubMed]
- Bryan, S.; Bungay, H.P.; Weatherburn, G.; Field, S. Magnetic Resonance Imaging for Investigation of the Knee Joint: A Clinical and Economic Evaluation. Int. J. Technol. Assess. Health Care 2004, 20, 222–229. [Google Scholar] [CrossRef]
- Shoeibi, A.; Ghassemi, N.; Khodatars, M.; Moridian, P.; Alizadehsani, R.; Zare, A.; Khosravi, A.; Subasi, A.; Rajendra Acharya, U.; Gorriz, J.M. Detection of Epileptic Seizures on EEG Signals Using ANFIS Classifier, Autoencoders and Fuzzy Entropies. Biomed. Signal. Processing Control. 2022, 73, 103417. [Google Scholar] [CrossRef]
- Khozeimeh, F.; Sharifrazi, D.; Izadi, N.H.; Joloudari, J.H.; Shoeibi, A.; Alizadehsani, R.; Gorriz, J.M.; Hussain, S.; Sani, Z.A.; Moosaei, H.; et al. Combining a Convolutional Neural Network with Autoencoders to Predict the Survival Chance of COVID-19 Patients. Sci. Rep. 2021, 11, 15343. [Google Scholar] [CrossRef]
- Khodatars, M.; Shoeibi, A.; Sadeghi, D.; Ghaasemi, N.; Jafari, M.; Moridian, P.; Khadem, A.; Alizadehsani, R.; Zare, A.; Kong, Y.; et al. Deep Learning for Neuroimaging-Based Diagnosis and Rehabilitation of Autism Spectrum Disorder: A Review. Comput. Biol. Med. 2021, 139, 104949. [Google Scholar] [CrossRef]
- Shoeibi, A.; Sadeghi, D.; Moridian, P.; Ghassemi, N.; Heras, J.; Alizadehsani, R.; Khadem, A.; Kong, Y.; Nahavandi, S.; Zhang, Y.-D.; et al. Automatic Diagnosis of Schizophrenia in EEG Signals Using CNN-LSTM Models. Front. Neuroinform. 2021, 15, 777977. [Google Scholar] [CrossRef]
- Sharifrazi, D.; Alizadehsani, R.; Roshanzamir, M.; Joloudari, J.H.; Shoeibi, A.; Jafari, M.; Hussain, S.; Sani, Z.A.; Hasanzadeh, F.; Khozeimeh, F.; et al. Fusion of Convolution Neural Network, Support Vector Machine and Sobel Filter for Accurate Detection of COVID-19 Patients Using X-Ray Images. Biomed. Signal. Processing Control. 2021, 68, 102622. [Google Scholar] [CrossRef]
- Currie, G.; Hawk, K.E.; Rohren, E.; Vial, A.; Klein, R. Machine Learning and Deep Learning in Medical Imaging: Intelligent Imaging. J. Med. Imaging Radiat. Sci. 2019, 50, 477–487. [Google Scholar] [CrossRef] [Green Version]
- Park, J.; Bae, S.; Seo, S.; Park, S.; Bang, J.-I.; Han, J.H.; Lee, W.W.; Lee, J.S. Measurement of Glomerular Filtration Rate Using Quantitative SPECT/CT and Deep-Learning-Based Kidney Segmentation. Sci. Rep. 2019, 9, 4223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, H.; Ha, S.; Kang, H.; Lee, H.; Lee, D.S. Deep Learning Only by Normal Brain PET Identify Unheralded Brain Anomalies. EBioMedicine 2019, 43, 447–453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeBaun, M.R.; Chavez, G.; Fithian, A.; Oladeji, K.; Van Rysselberghe, N.; Goodnough, L.H.; Bishop, J.A.; Gardner, M.J. Artificial Neural Networks Predict 30-Day Mortality After Hip Fracture: Insights From Machine Learning. J. Am. Acad. Orthop. Surg. 2021, 29, 977–983. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.M.; Mstafa, R.J. A Comprehensive Survey on Bone Segmentation Techniques in Knee Osteoarthritis Research: From Conventional Methods to Deep Learning. Diagnostics 2022, 12, 611. [Google Scholar] [CrossRef]
- Lundervold, A.S.; Lundervold, A. An Overview of Deep Learning in Medical Imaging Focusing on MRI. Z. Med. Phys. 2019, 29, 102–127. [Google Scholar] [CrossRef]
- Choy, G.; Khalilzadeh, O.; Michalski, M.; Do, S.; Samir, A.E.; Pianykh, O.S.; Geis, J.R.; Pandharipande, P.V.; Brink, J.A.; Dreyer, K.J. Current Applications and Future Impact of Machine Learning in Radiology. Radiology 2018, 288, 318–328. [Google Scholar] [CrossRef]
- Kernohan, W.G.; Beverland, D.E.; McCoy, G.F.; Hamilton, A.; Watson, P.; Mollan, R.A.B. Vibration Arthrometry. Acta Orthop. Scand. 1990, 61, 70–79. [Google Scholar] [CrossRef] [Green Version]
- Wu, Y. Knee Joint Vibroarthrographic Signal. Processing and Analysis; Springer: Berlin/Heidelberg, Germany, 2015; ISBN 3-662-44283-3. [Google Scholar]
- Rangayyan, R.M.; Reddy, N.P. Biomedical Signal Analysis: A Case-Study Approach. Ann. Biomed. Eng. 2002, 30, 983. [Google Scholar]
- Frank, C.B.; Rangayyan, R.M.; Bell, G.D. Analysis of Knee Joint Sound Signals for Non-Invasive Diagnosis of Cartilage Pathology. IEEE Eng. Med. Biol. Mag. 1990, 9, 65–68. [Google Scholar] [CrossRef]
- van den Borne, M.P.J.; Raijmakers, N.J.H.; Vanlauwe, J.; Victor, J.; de Jong, S.N.; Bellemans, J.; Saris, D.B.F. International Cartilage Repair Society (ICRS) and Oswestry Macroscopic Cartilage Evaluation Scores Validated for Use in Autologous Chondrocyte Implantation (ACI) and Microfracture. Osteoarthr. Cartil. 2007, 15, 1397–1402. [Google Scholar] [CrossRef] [Green Version]
- Karpiński, R.; Machrowska, A.; Maciejewski, M. Application of Acoustic Signal Processing Methods in Detecting Differences between Open and Closed Kinematic Chain Movement for the Knee Joint. Appl. Comput. Sci. 2019, 11, 36–48. [Google Scholar] [CrossRef]
- Prior, J.; Mascaro, B.; Shark, L.-K.; Stockdale, J.; Selfe, J.; Bury, R.; Cole, P.; Goodacre, J.A. Analysis of High Frequency Acoustic Emission Signals as a New Approach for Assessing Knee Osteoarthritis. Ann. Rheum. Dis. 2010, 69, 929–930. [Google Scholar] [CrossRef] [PubMed]
- Nevalainen, M.T.; Veikkola, O.; Thevenot, J.; Tiulpin, A.; Hirvasniemi, J.; Niinimäki, J.; Saarakkala, S.S. Acoustic Emissions and Kinematic Instability of the Osteoarthritic Knee Joint: Comparison with Radiographic Findings. Sci. Rep. 2021, 11, 19558. [Google Scholar] [CrossRef] [PubMed]
- Blodgett, W.E. Auscultation of the Knee Joint. Boston Med. Surg. J. 1902, 146, 63–66. [Google Scholar] [CrossRef]
- Feng, G.-H.; Chen, W.-M. Piezoelectric-Film-Based Acoustic Emission Sensor Array with Thermoactuator for Monitoring Knee Joint Conditions. Sens. Actuators A Phys. 2016, 246, 180–191. [Google Scholar] [CrossRef]
- Mascaro, B.; Prior, J.; Shark, L.-K.; Selfe, J.; Cole, P.; Goodacre, J. Exploratory Study of a Non-Invasive Method Based on Acoustic Emission for Assessing the Dynamic Integrity of Knee Joints. Med. Eng. Phys. 2009, 31, 1013–1022. [Google Scholar] [CrossRef]
- Shark, L.-K.; Chen, H.; Goodacre, J. Knee Acoustic Emission: A Potential Biomarker for Quantitative Assessment of Joint Ageing and Degeneration. Med. Eng. Phys. 2011, 33, 534–545. [Google Scholar] [CrossRef]
- Kiselev, J.; Ziegler, B.; Schwalbe, H.J.; Franke, R.P.; Wolf, U. Detection of Osteoarthritis Using Acoustic Emission Analysis. Med. Eng. Phys. 2019, 65, 57–60. [Google Scholar] [CrossRef]
- Jeong, H.K.; Whittingslow, D.; Inan, O.T. B -Value: A Potential Biomarker for Assessing Knee-Joint Health Using Acoustical Emission Sensing. IEEE Sens. Lett. 2018, 2, 1–4. [Google Scholar] [CrossRef]
- Karpiński, R.; Krakowski, P.; Jonak, J.; Machrowska, A.; Maciejewski, M.; Nogalski, A. Estimation of Differences in Selected Indices of Vibroacoustic Signals between Healthy and Osteoarthritic Patellofemoral Joints as a Potential Non-Invasive Diagnostic Tool. J. Phys. Conf. Ser. 2021, 2130, 012009. [Google Scholar] [CrossRef]
- Karpiński, R.; Krakowski, P.; Jonak, J.; Machrowska, A.; Maciejewski, M.; Nogalski, A. Analysis of Differences in Vibroacoustic Signals between Healthy and Osteoarthritic Knees Using EMD Algorithm and Statistical Analysis. J. Phys. Conf. Ser. 2021, 2130, 012010. [Google Scholar] [CrossRef]
- Cai, S.; Yang, S.; Zheng, F.; Lu, M.; Wu, Y.; Krishnan, S. Knee Joint Vibration Signal Analysis with Matching Pursuit Decomposition and Dynamic Weighted Classifier Fusion. Comput. Math. Methods Med. 2013, 2013, 904267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krishnan, S.; Rangayyan, R.M.; Bell, G.D.; Frank, C.B. Auditory Display of Knee-Joint Vibration Signals. J. Acoust. Soc. Am. 2001, 110, 3292–3304. [Google Scholar] [CrossRef] [PubMed]
- Rangayyan, R.M.; Wu, Y. Screening of Knee-Joint Vibroarthrographic Signals Using Probability Density Functions Estimated with Parzen Windows. Biomed. Signal. Processing Control. 2010, 5, 53–58. [Google Scholar] [CrossRef]
- Łysiak, A.; Froń, A.; Bączkowicz, D.; Szmajda, M. Vibroarthrographic Signal Spectral Features in 5-Class Knee Joint Classification. Sensors 2020, 20, 5015. [Google Scholar] [CrossRef]
- Bączkowicz, D.; Majorczyk, E. Joint Motion Quality in Vibroacoustic Signal Analysis for Patients with Patellofemoral Joint Disorders. BMC Musculoskelet Disord 2014, 15, 426. [Google Scholar] [CrossRef] [Green Version]
- Wu, Y.; Chen, P.; Luo, X.; Huang, H.; Liao, L.; Yao, Y.; Wu, M.; Rangayyan, R.M. Quantification of Knee Vibroarthrographic Signal Irregularity Associated with Patellofemoral Joint Cartilage Pathology Based on Entropy and Envelope Amplitude Measures. Comput. Methods Programs Biomed. 2016, 130, 1–12. [Google Scholar] [CrossRef]
- Andersen, R.E.; Arendt-Nielsen, L.; Madeleine, P. A Review of Engineering Aspects of Vibroarthography of the Knee Joint. Crit Rev. Phys. Rehabil Med. 2016, 28, 13–32. [Google Scholar] [CrossRef]
- Krishnan, S.; Rangayyan, R.M.; Bell, G.D.; Frank, C.B. Adaptive Time-Frequency Analysis of Knee Joint Vibroarthrographic Signals for Noninvasive Screening of Articular Cartilage Pathology. IEEE Trans. Biomed. Eng. 2000, 47, 773–783. [Google Scholar] [CrossRef]
- Rangayyan, R.M.; Oloumi, F.; Wu, Y.; Cai, S. Fractal Analysis of Knee-Joint Vibroarthrographic Signals via Power Spectral Analysis. Biomed. Signal. Processing Control. 2013, 8, 23–29. [Google Scholar] [CrossRef]
- Befrui, N.; Elsner, J.; Flesser, A.; Huvanandana, J.; Jarrousse, O.; Le, T.N.; Müller, M.; Schulze, W.H.W.; Taing, S.; Weidert, S. Vibroarthrography for Early Detection of Knee Osteoarthritis Using Normalized Frequency Features. Med. Biol Eng. Comput. 2018, 56, 1499–1514. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, N.; Hoshiyama, M. Vibroarthrography in Patients with Knee Arthropathy. BMR 2012, 25, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Krishnan, S.; Rangayyan, R.M. Computer-Aided Diagnosis of Knee-Joint Disorders via Vibroarthrographic Signal Analysis: A Review. Crit. Rev. Biomed. Eng. 2010, 38, 119. [Google Scholar] [CrossRef] [PubMed]
- Apley, A.G. The Diagnosis of Meniscus Injuries; Some New Clinical Methods. J. Bone Jt. Surg Am. 1947, 29, 78–84. [Google Scholar]
- McMurray, T.P. The Semilunar Cartilages. Br. J. Surg. 1942, 29, 407–414. [Google Scholar] [CrossRef]
- Karachalios, T.; Hantes, M.; Zibis, A.H.; Zachos, V.; Karantanas, A.H.; Malizos, K.N. Diagnostic Accuracy of a New Clinical Test (the Thessaly Test) for Early Detection of Meniscal Tears. J. Bone Jt. Surg. 2005, 87, 955–962. [Google Scholar] [CrossRef] [Green Version]
- Torg, J.S.; Conrad, W.; Kalen, V. Clinical I Diagnosis of Anterior Cruciate Ligament Instability in the Athlete. Am. J. Sports Med. 1976, 4, 84–93. [Google Scholar] [CrossRef]
- Paessler, H.H.; Michel, D. How New Is the Lachman Test? Am. J. Sports Med. 1992, 20, 95–98. [Google Scholar] [CrossRef]
- Galway, H.R.; MacIntosh, D.L. The Lateral Pivot Shift: A Symptom and Sign of Anterior Cruciate Ligament Insufficiency. Clin. Orthop. Relat. Res. 1980, 11, 45–50. [Google Scholar] [CrossRef]
- Lelli, A.; Di Turi, R.P.; Spenciner, D.B.; Dòmini, M. The “Lever Sign”: A New Clinical Test for the Diagnosis of Anterior Cruciate Ligament Rupture. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 2794–2797. [Google Scholar] [CrossRef]
- Nijs, J.; Van Geel, C.; Auwera, C.; Van de Velde, B. Diagnostic Value of Five Clinical Tests in Patellofemoral Pain Syndrome. Man. Ther. 2006, 11, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Malanga, G.A.; Andrus, S.; Nadler, S.F.; McLean, J. Physical Examination of the Knee: A Review of the Original Test Description and Scientific Validity of Common Orthopedic Tests. Arch. Phys. Med. Rehabil. 2003, 84, 592–603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cameron, M.L.; Briggs, K.K.; Steadman, J.R. Reproducibility and Reliability of the Outerbridge Classification for Grading Chondral Lesions of the Knee Arthroscopically. Am. J. Sports Med. 2003, 31, 83–86. [Google Scholar] [CrossRef] [PubMed]
- Brittberg, M.; Winalski, C.S. Evaluation of Cartilage Injuries and Repair. J. Bone Jt. Surg Am. 2003, 85 (Suppl. 2), 58–69. [Google Scholar] [CrossRef]
- Contact Microphone CM-01B, Technical Data Sheet. 2015. Available online: https://www.te.com/commerce/DocumentDelivery/DDEController (accessed on 16 February 2022).
- Bourns® Encoders, Technical Data Sheet 2015. Available online: https://www.bourns.com/docs/technical-documents/technical-library/sensors-controls/publications/Bourns_SC1180_Encoder_SF_Broch.pdf (accessed on 16 February 2022).
- Karandikar, N.; Vargas, O.O.O. Kinetic Chains: A Review of the Concept and Its Clinical Applications. PMR 2011, 3, 739–745. [Google Scholar] [CrossRef]
- ADUM4160 Datasheet and Product Info|Analog Devices. Available online: https://www.analog.com/en/products/adum4160.html (accessed on 5 February 2022).
- Zhang, M.; Wei, G. An Integrated EMD Adaptive Threshold Denoising Method for Reduction of Noise in ECG. PLoS ONE 2020, 15, e0235330. [Google Scholar] [CrossRef]
- Ghofrani, S.; Akbari, H. Comparing Nonlinear Features Extracted in EEMD for Discriminating Focal and Non-Focal EEG Signals. In Proceedings of the Tenth International Conference on Signal Processing Systems, Singapore, 17 April 2019; Mao, K., Jiang, X., Eds.; SPIE: Singapore, 2019; p. 43. [Google Scholar]
- Kumar, S.; Panigrahy, D.; Sahu, P.K. Denoising of Electrocardiogram (ECG) Signal by Using Empirical Mode Decomposition (EMD) with Non-Local Mean (NLM) Technique. Biocybern. Biomed. Eng. 2018, 38, 297–312. [Google Scholar] [CrossRef]
- Carvalho, V.R.; Moraes, M.F.D.; Braga, A.P.; Mendes, E.M.A.M. Evaluating Five Different Adaptive Decomposition Methods for EEG Signal Seizure Detection and Classification. Biomed. Signal. Processing Control. 2020, 62, 102073. [Google Scholar] [CrossRef]
- Huang, N.E.; Shen, Z.; Long, S.R.; Wu, M.C.; Shih, H.H.; Zheng, Q.; Yen, N.-C.; Tung, C.C.; Liu, H.H. The Empirical Mode Decomposition and the Hilbert Spectrum for Nonlinear and Non-Stationary Time Series Analysis. Proc. R. Soc. London. Ser. A Math. Phys. Eng. Sci. 1998, 454, 903–995. [Google Scholar] [CrossRef]
- Chaudhari, H.; Nalbalwar, S.L.; Sheth, R. A Review on Intrensic Mode Function of EMD. In Proceedings of the 2016 International Conference on Electrical, Electronics, and Optimization Techniques (ICEEOT), Chennai, India, 12 March 2016; pp. 2349–2352. [Google Scholar]
- Zhang, J.; Yan, R.; Gao, R.X.; Feng, Z. Performance Enhancement of Ensemble Empirical Mode Decomposition. Mech. Syst. Signal. Processing 2010, 24, 2104–2123. [Google Scholar] [CrossRef]
- Zheng, J.; Cheng, J.; Yang, Y. Partly Ensemble Empirical Mode Decomposition: An Improved Noise-Assisted Method for Eliminating Mode Mixing. Signal. Processing 2014, 96, 362–374. [Google Scholar] [CrossRef]
- Rilling, G.; Flandrin, P. One or Two Frequencies? The Empirical Mode Decomposition Answers. IEEE Trans. Signal Processing 2007, 56, 85–95. [Google Scholar] [CrossRef] [Green Version]
- Wu, Z.; Huang, N.E. Ensemble Empirical Mode Decomposition: A Noise-Assisted Data Analysis Method. Adv. Adapt. Data Anal. 2009, 1, 1–41. [Google Scholar] [CrossRef]
- Jedliński, Ł.; Jonak, J. Early Fault Detection in Gearboxes Based on Support Vector Machines and Multilayer Perceptron with a Continuous Wavelet Transform. Appl. Soft Comput. 2015, 30, 636–641. [Google Scholar] [CrossRef]
- Jedliński, Ł.; Caban, J.; Krzywonos, L.; Wierzbicki, S.; Brumerčík, F. Application of Vibration Signal in the Diagnosis of IC Engine Valve Clearance. J. Vibroengineering 2015, 17, 175–187. [Google Scholar]
- Cempel, C. Diagnostyka Wibroakustyczna Maszyn-Historia, Stan Obecny, Perspektywy Rozwoju. Probl. Eksploat. 2005, 7, 25. [Google Scholar]
- Stanik, Z.; Instytut Technologii Eksploatacji; Wydawnictwo. Diagnozowanie Lozysk Tocznych Pojazdów Samochodowych Metodami Wibroakustycznymi; Wydawnictwo Naukowe Instytutu Technologii Eksploatacji—Panstwowego Instytutu Badawczego: Radom, Poland, 2013; ISBN 978-83-7789-204-6. [Google Scholar]
- Glowacz, A.; Tadeusiewicz, R.; Legutko, S.; Caesarendra, W.; Irfan, M.; Liu, H.; Brumercik, F.; Gutten, M.; Sulowicz, M.; Antonino Daviu, J.A.; et al. Fault Diagnosis of Angle Grinders and Electric Impact Drills Using Acoustic Signals. Appl. Acoust. 2021, 179, 108070. [Google Scholar] [CrossRef]
- Jonak, J.; Karpinski, R.; Machrowska, A.; Krakowski, P.; Maciejewski, M. A Preliminary Study on the Use of EEMD-RQA Algorithms in the Detection of Degenerative Changes in Knee Joints. IOP Conf. Ser. Mater. Sci. Eng. 2019, 710, 012037. [Google Scholar] [CrossRef]
- Karpiński, R.; Krakowski, P.; Jonak, J.; Machrowska, A.; Maciejewski, M.; Nogalski, A. Diagnostics of Articular Cartilage Damage Based on Generated Acoustic Signals Using ANN—Part I: Femoral-Tibial Joint. Sensors 2022, 22, 2176. [Google Scholar] [CrossRef]
- Jin, X.; Xu, A.; Bie, R.; Guo, P. Machine Learning Techniques and Chi-Square Feature Selection for Cancer Classification Using SAGE Gene Expression Profiles. In Data Mining for Biomedical Applications; Lecture Notes in Computer Science; Li, J., Yang, Q., Tan, A.-H., Eds.; Springer: Berlin/Heidelberg, Germany, 2006; Volume 3916, pp. 106–115. ISBN 978-3-540-33104-9. [Google Scholar]
- Shrestha, U.; Alsadoon, A.; Prasad, P.W.C.; Al Aloussi, S.; Alsadoon, O.H. Supervised Machine Learning for Early Predicting the Sepsis Patient: Modified Mean Imputation and Modified Chi-Square Feature Selection. Multimed Tools Appl. 2021, 80, 20477–20500. [Google Scholar] [CrossRef]
- Zhou, H.; Zhang, J.; Zhou, Y.; Guo, X.; Ma, Y. A Feature Selection Algorithm of Decision Tree Based on Feature Weight. Expert Syst. Appl. 2021, 164, 113842. [Google Scholar] [CrossRef]
- Nanda, M.K.; Patra, M.R. Intrusion Detection and Classification Using Decision Tree-Based Feature Selection Classifiers. In Intelligent and Cloud Computing; Smart Innovation, Systems and Technologies; Mishra, D., Buyya, R., Mohapatra, P., Patnaik, S., Eds.; Springer: Singapore, 2021; Volume 153, pp. 157–170. ISBN 9789811562013. [Google Scholar]
- Risqiwati, D.; Wibawa, A.D.; Pane, E.S.; Islamiyah, W.R.; Tyas, A.E.; Purnomo, M.H. Feature Selection for EEG-Based Fatigue Analysis Using Pearson Correlation. In Proceedings of the 2020 International Seminar on Intelligent Technology and Its Applications (ISITIA), Surabaya, Indonesia, 7 July 2020; pp. 164–169. [Google Scholar]
- Nasir, I.M.; Khan, M.A.; Yasmin, M.; Shah, J.H.; Gabryel, M.; Scherer, R.; Damaševičius, R. Pearson Correlation-Based Feature Selection for Document Classification Using Balanced Training. Sensors 2020, 20, 6793. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, P.; Azam, S.; Jonkman, M.; Karim, A.; Shamrat, F.M.J.M.; Ignatious, E.; Shultana, S.; Beeravolu, A.R.; De Boer, F. Efficient Prediction of Cardiovascular Disease Using Machine Learning Algorithms With Relief and LASSO Feature Selection Techniques. IEEE Access 2021, 9, 19304–19326. [Google Scholar] [CrossRef]
- Hamada, M.; Tanimu, J.J.; Hassan, M.; Kakudi, H.A.; Robert, P. Evaluation of Recursive Feature Elimination and LASSO Regularization-Based Optimized Feature Selection Approaches for Cervical Cancer Prediction. In Proceedings of the 2021 IEEE 14th International Symposium on Embedded Multicore/Many-core Systems-on-Chip (MCSoC), Singapore, 12 December 2021; pp. 333–339. [Google Scholar]
- Muthukrishnan, R.; Rohini, R. LASSO: A Feature Selection Technique in Predictive Modeling for Machine Learning. In Proceedings of the 2016 IEEE International Conference on Advances in Computer Applications (ICACA); IEEE: Coimbatore, India, October 2016; pp. 18–20. [Google Scholar]
- Li, J.; Cheng, K.; Wang, S.; Morstatter, F.; Trevino, R.P.; Tang, J.; Liu, H. Feature Selection: A Data Perspective. ACM Comput. Surv. 2018, 50, 1–45. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Jeong, J.C. Enhanced Recursive Feature Elimination. In Proceedings of the Sixth International Conference on Machine Learning and Applications (ICMLA 2007), Cincinnati, OH, USA, 11 December 2007; pp. 429–435. [Google Scholar]
- Yang, W.; Wang, K.; Zuo, W. Neighborhood Component Feature Selection for High-Dimensional Data. JCP 2012, 7, 161–168. [Google Scholar] [CrossRef]
- Raghu, S.; Sriraam, N. Classification of Focal and Non-Focal EEG Signals Using Neighborhood Component Analysis and Machine Learning Algorithms. Expert Syst. Appl. 2018, 113, 18–32. [Google Scholar] [CrossRef]
- Dudek-Dyduch, E.; Tadeusiewicz, R.; Horzyk, A. Neural Network Adaptation Process Effectiveness Dependent of Constant Training Data Availability. Neurocomputing 2009, 72, 3138–3149. [Google Scholar] [CrossRef]
- Rogala, M.; Gajewski, J.; Górecki, M. Study on the Effect of Geometrical Parameters of a Hexagonal Trigger on Energy Absorber Performance Using ANN. Materials 2021, 14, 5981. [Google Scholar] [CrossRef]
- Smoleń, A.; Czekierdowski, A.; Stachowicz, N.; Kotarski, J. Use of multilayer perception artificial neutral networks for the prediction of the probability of malignancy in adnexal tumors. Ginekol. Pol. 2003, 74, 855–862. [Google Scholar]
- Szpurek, D.; Moszynski, R.; Smolen, A.; Sajdak, S. Artificial Neural Network Computer Prediction of Ovarian Malignancy in Women with Adnexal Masses. Int. J. Gynecol. Obstet. 2005, 89, 108–113. [Google Scholar] [CrossRef]
- Rogala, M. Neural Networks in Crashworthiness Analysis of Thin-Walled Profile with Foam Filling. Adv. Sci. Technol. Res. J. 2020, 14, 93–99. [Google Scholar] [CrossRef]
- Gajewski, J.; Vališ, D. Verification of the Technical Equipment Degradation Method Using a Hybrid Reinforcement Learning Trees–Artificial Neural Network System. Tribol. Int. 2021, 153, 106618. [Google Scholar] [CrossRef]
- Kruse, R.; Mostaghim, S.; Borgelt, C.; Braune, C.; Steinbrecher, M. Radial Basis Function Networks. In Computational Intelligence; Texts in Computer Science; Springer International Publishing: Cham, Switzerland, 2022; pp. 125–148. ISBN 978-3-030-42226-4. [Google Scholar]
- Montazer, G.A.; Giveki, D.; Karami, M.; Rastegar, H. Radial Basis Function Neural Networks: A Review. Comput. Rev. J. 2018, 1, 52–74. [Google Scholar]
- Krakowski, P.; Karpiński, R.; Jonak, J.; Maciejewski, R. Evaluation of Diagnostic Accuracy of Physical Examination and MRI for Ligament and Meniscus Injuries. J. Phys. Conf. Ser. 2021, 1736, 012027. [Google Scholar] [CrossRef]
- Chicco, D.; Jurman, G. The Advantages of the Matthews Correlation Coefficient (MCC) over F1 Score and Accuracy in Binary Classification Evaluation. BMC Genom. 2020, 21, 6. [Google Scholar] [CrossRef] [Green Version]
- Matthews, B.W. Comparison of the Predicted and Observed Secondary Structure of T4 Phage Lysozyme. Biochim. Et Biophys. Acta (BBA)-Protein Struct. 1975, 405, 442–451. [Google Scholar] [CrossRef]
- Powers, D.M.W. Evaluation: From Precision, Recall and F-Measure to ROC, Informedness, Markedness and Correlation. arXiv 2020, arXiv:2010.16061. [Google Scholar]
- Umapathy, K.; Krishnan, S. Modified Local Discriminant Bases Algorithm and Its Application in Analysis of Human Knee Joint Vibration Signals. IEEE Trans. Biomed. Eng. 2006, 53, 517–523. [Google Scholar] [CrossRef]
- Mascarenhas, E.; Nalband, S.; Fredo, A.R.J.; Prince, A.A. Analysis and Classification of Vibroarthrographic Signals Using Tuneable ‘Q’ Wavelet Transform. In Proceedings of the 2020 7th International Conference on Signal Processing and Integrated Networks (SPIN), Noida, India, 2 February 2020; pp. 65–70. [Google Scholar]
- Sharma, M.; Acharya, U.R. Analysis of Knee-Joint Vibroarthographic Signals Using Bandwidth-Duration Localized Three-Channel Filter Bank. Comput. Electr. Eng. 2018, 72, 191–202. [Google Scholar] [CrossRef]
- Wu, Y.; Krishnan, S. Combining Least-Squares Support Vector Machines for Classification of Biomedical Signals: A Case Study with Knee-Joint Vibroarthrographic Signals. J. Exp. Theor. Artif. Intell. 2011, 23, 63–77. [Google Scholar] [CrossRef]
- Rangayyan, R.M.; Wu, Y.F. Screening of Knee-Joint Vibroarthrographic Signals Using Statistical Parameters and Radial Basis Functions. Med. Biol Eng. Comput 2008, 46, 223–232. [Google Scholar] [CrossRef] [PubMed]
- Nalband, S.; Valliappan, C.A.; Prince, R.G.A.A.; Agrawal, A. Feature Extraction and Classification of Knee Joint Disorders Using Hilbert Huang Transform. In Proceedings of the 2017 14th International Conference on Electrical Engineering/Electronics, Computer, Telecommunications and Information Technology (ECTI-CON), Phuket, Thailand, 23 June 2017; pp. 266–269. [Google Scholar]
- Shidore, M.M.; Athreya, S.S.; Deshpande, S.; Jalnekar, R. Screening of Knee-Joint Vibroarthrographic Signals Using Time and Spectral Domain Features. Biomed. Signal. Processing Control. 2021, 68, 102808. [Google Scholar] [CrossRef]
- Yang, S.; Cai, S.; Zheng, F.; Wu, Y.; Liu, K.; Wu, M.; Zou, Q.; Chen, J. Representation of Fluctuation Features in Pathological Knee Joint Vibroarthrographic Signals Using Kernel Density Modeling Method. Med. Eng. Phys. 2014, 36, 1305–1311. [Google Scholar] [CrossRef] [PubMed]
- Rangayyan, R.M.; Wu, Y. Analysis of Vibroarthrographic Signals with Features Related to Signal Variability and Radial-Basis Functions. Ann. Biomed. Eng. 2009, 37, 156–163. [Google Scholar] [CrossRef]
- Mu, T.; Nandi, A.K.; Rangayyan, R.M. Screening of Knee-Joint Vibroarthrographic Signals Using the Strict 2-Surface Proximal Classifier and Genetic Algorithm. Comput. Biol. Med. 2008, 38, 1103–1111. [Google Scholar] [CrossRef]
- Kim, K.S.; Seo, J.H.; Kang, J.U.; Song, C.G. An Enhanced Algorithm for Knee Joint Sound Classification Using Feature Extraction Based on Time-Frequency Analysis. Comput. Methods Programs Biomed. 2009, 94, 198–206. [Google Scholar] [CrossRef]
- Daniel, C.; Jeong, H.-K.; Ganti, V.G.; Kirkpatrick, N.J.; Kogler, G.F.; Inan, O.T. Acoustic Emissions as a Non-Invasive Biomarker of the Structural Health of the Knee. Ann. Biomed. Eng. 2020, 48, 225–235. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Group | N | Males/ Females | Age (years ± SD) | Height (m ± SD) | Weight (kg ± SD) | BMI | Tegner-Lyshom Score |
|---|---|---|---|---|---|---|---|
| Healthy control (HC) | 33 | 9/24 | 24.10 ± 5.56 | 1.71 ± 0.09 | 65.16 ± 15.10 | 21.95 ± 3.09 | 100 ± 0.0 |
| Osteoarthritis (OA) | 34 | 15/19 | 56.15 ± 12.99 | 1.69 ± 0.09 | 89.08 ± 14.30 | 31.19 ± 4.83 | 38.59 ± 12.96 |
| Variant | Network Name | Accuracy of Learning (%) | Accuracy of Testing (%) | Accuracy of Validation (%) | Learning Algorithm | Error Function | Activation (Hidden) | Activation (Output) |
|---|---|---|---|---|---|---|---|---|
| I | MLP 9-40-2 | 89.71 | 100.00 | 85.71 | BFGS 25 | SOS | Linear | Exponential |
| RBF 9-35-2 | 98.53 | 85.71 | 100.00 | RBFT | Entropy | Gauss | Softmax | |
| II | MLP 10-16-2 | 98.53 | 100.00 | 100.00 | BFGS 17 | Entropy | Logistic | Softmax |
| RBF 10-40-2 | 97.06 | 92.86 | 100.00 | RBFT | Entropy | Gauss | Softmax | |
| III | MLP 8-3-2 | 97.79 | 100.00 | 96.43 | BFGS 103 | Entropy | Tanh | Softmax |
| RBF 8-14-2 | 91.91 | 96.43 | 96.43 | RBFT | Entropy | Gauss | Softmax |
| Network Name | HC | OA | Total | |
|---|---|---|---|---|
| MLP 9-40-2 | Total | 45.00 | 23.00 | 68.00 |
| Correct | 43.00 | 18.00 | 61.00 | |
| Correct (%) | 95.56 | 78.26 | 89.71 | |
| RBF 9-35-2 | Total | 45.00 | 23.00 | 68.00 |
| Correct | 44.00 | 23.00 | 67.00 | |
| Correct (%) | 97.78 | 100.00 | 98.53 | |
| MLP 10-16-2 | Total | 45.00 | 23.00 | 68.00 |
| Correct | 44.00 | 23.00 | 67.00 | |
| Correct (%) | 97.78 | 100.00 | 98.53 | |
| RBF 10-40-2 | Total | 45.00 | 23.00 | 68.00 |
| Correct | 43.00 | 23.00 | 66.00 | |
| Correct (%) | 95.56 | 100.00 | 97.06 | |
| MLP 8-3-2 | Total | 89.00 | 47.00 | 136.00 |
| Correct | 88.00 | 45.00 | 133.00 | |
| Correct (%) | 98.88 | 95.74 | 97.79 | |
| RBF 8-14-2 | Total | 89.00 | 47.00 | 136.00 |
| Correct | 85.00 | 40.00 | 125.00 | |
| Correct (%) | 95.51 | 85.11 | 91.91 | |
| Variant I | Variant II | Variant III | ||||
|---|---|---|---|---|---|---|
| MPL | RBF | MPL | RBF | MPL | RBF | |
| ROC area | 0.986 | 1.000 | 1.000 | 1.000 | 0.995 | 0.979 |
| ROC Threshold | 0.533 | 0.480 | 0.470 | 0.437 | 0.866 | 0.620 |
| Location | Variant | Network Name | Accuracy (%) | Sensitivity | Specificity | AUC | Precision | Recall | F1 Score | MCC |
|---|---|---|---|---|---|---|---|---|---|---|
| Femoral-Tibial Joint | I | MLP 13-9-2 | 96.32 | 0.957 | 0.967 | 0.996 | 0.936 | 0.957 | 0.946 | 0.918 |
| RBF 13-43-2 | 89.71 | 0.867 | 0.912 | 0.960 | 0.830 | 0.867 | 0.848 | 0.771 | ||
| II | MLP 15-12-2 | 94.85 | 0.935 | 0.956 | 0.989 | 0.915 | 0.935 | 0.925 | 0.886 | |
| RBF 15-6-2 | 91.91 | 0.950 | 0.906 | 0.977 | 0.809 | 0.950 | 0.874 | 0.820 | ||
| III | MLP 15-24-2 | 93.70 | 0.928 | 0.941 | 0.977 | 0.875 | 0.928 | 0.901 | 0.855 | |
| RBF 15-5-2 | 89.63 | 0.806 | 0.948 | 0.974 | 0.898 | 0.806 | 0.849 | 0.773 | ||
| Patellofemoral joint | I | MLP 9-40-2 | 89.71 | 0.900 | 0.896 | 0.986 | 0.783 | 0.900 | 0.837 | 0.766 |
| RBF 9-35-2 | 98.53 | 0.958 | 1.000 | 1.000 | 1.000 | 0.958 | 0.979 | 0.968 | ||
| II | MLP 10-16-2 | 98.53 | 0.958 | 1.000 | 1.000 | 1.000 | 0.958 | 0.979 | 0.968 | |
| RBF 10-40-2 | 97.06 | 0.920 | 1.000 | 1.000 | 1.000 | 0.920 | 0.958 | 0.938 | ||
| III | MLP 8-3-2 | 97.79 | 0.978 | 0.978 | 0.995 | 0.957 | 0.978 | 0.968 | 0.951 | |
| RBF 8-14-2 | 91.91 | 0.909 | 0.924 | 0.979 | 0.851 | 0.909 | 0.879 | 0.819 |
| Authors | Classification Methods | Accuracy (%) | Sensitivity | Specificity | AUC |
|---|---|---|---|---|---|
| Krishnan et al. [60] | Logistic regression analysis | 68.90 | 0.564 | 0.784 | N/A |
| Umpathy and Krishnan [122] | Linear discriminant analysis | 76.40 | 0.789 | 0.745 | N/A |
| Rangayyan and Wu [55] | RBF | 77.53 | 0.711 | 0.824 | 0.832 |
| Mascarenhas et al. [123] | Random forest | 80.89 | 0.868 | 0.765 | 0.817 |
| Sharma and Acharya [124] | LS-SVM | 89.89 | 0.914 | 0.889 | N/A |
| Wu and Krishnan [125] | Multiple classifier Fusion system | 80.9 | 0.895 | 0.922 | 0.948 |
| Rangayyan and Wu [126] | RBF | 82.02 | 0.711 | 0.902 | 0.820 |
| Nalband et al. [127] | LS-SVM | 83.14 | 0.981 | 0.622 | 0.671 |
| Wu et al. 45 | Bayesian decision rule | 86.67 | 0.750 | 0.936 | 0.910 |
| Shidore et al. [128] | SVM | 87.69 | 0.857 | 0.838 | 0.926 |
| Yang et al. [129] | Bayesian decision rule | 88.00 | 0.714 | 0.979 | 0.957 |
| Cai et al. [53] | Dynamic weighted classifier Fusion system | 88.76 | 0.737 | 1.000 | 0.952 |
| Rangayyan and Wu [130] | RBF | 89.89 | 0.921 | 0.882 | 0.917 |
| Mu et al. [131] | Strict 2-surface proximal classifier | 91.01 | 0.947 | 0.882 | 0.950 |
| Kim et al. [132] | Back propagation neural network | 95.4 | 0.920 | 0.987 | N/A |
| Karpiński et al. [96] | MLP, RBF | 96.32 | 0.957 | 0.967 | 0.996 |
| Proposed method | MLP, RBF | 98.53 | 0.958 | 1.000 | 1.000 |
| Rangayyan et al. [61] | RBF | 100 | 1 | 1 | 0.961 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karpiński, R.; Krakowski, P.; Jonak, J.; Machrowska, A.; Maciejewski, M.; Nogalski, A. Diagnostics of Articular Cartilage Damage Based on Generated Acoustic Signals Using ANN—Part II: Patellofemoral Joint. Sensors 2022, 22, 3765. https://doi.org/10.3390/s22103765
Karpiński R, Krakowski P, Jonak J, Machrowska A, Maciejewski M, Nogalski A. Diagnostics of Articular Cartilage Damage Based on Generated Acoustic Signals Using ANN—Part II: Patellofemoral Joint. Sensors. 2022; 22(10):3765. https://doi.org/10.3390/s22103765
Chicago/Turabian StyleKarpiński, Robert, Przemysław Krakowski, Józef Jonak, Anna Machrowska, Marcin Maciejewski, and Adam Nogalski. 2022. "Diagnostics of Articular Cartilage Damage Based on Generated Acoustic Signals Using ANN—Part II: Patellofemoral Joint" Sensors 22, no. 10: 3765. https://doi.org/10.3390/s22103765
APA StyleKarpiński, R., Krakowski, P., Jonak, J., Machrowska, A., Maciejewski, M., & Nogalski, A. (2022). Diagnostics of Articular Cartilage Damage Based on Generated Acoustic Signals Using ANN—Part II: Patellofemoral Joint. Sensors, 22(10), 3765. https://doi.org/10.3390/s22103765