
Wristbands in Home-Based Rehabilitation—Validation of Heart Rate Measurement



Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Study Protocol
2.3. Participants
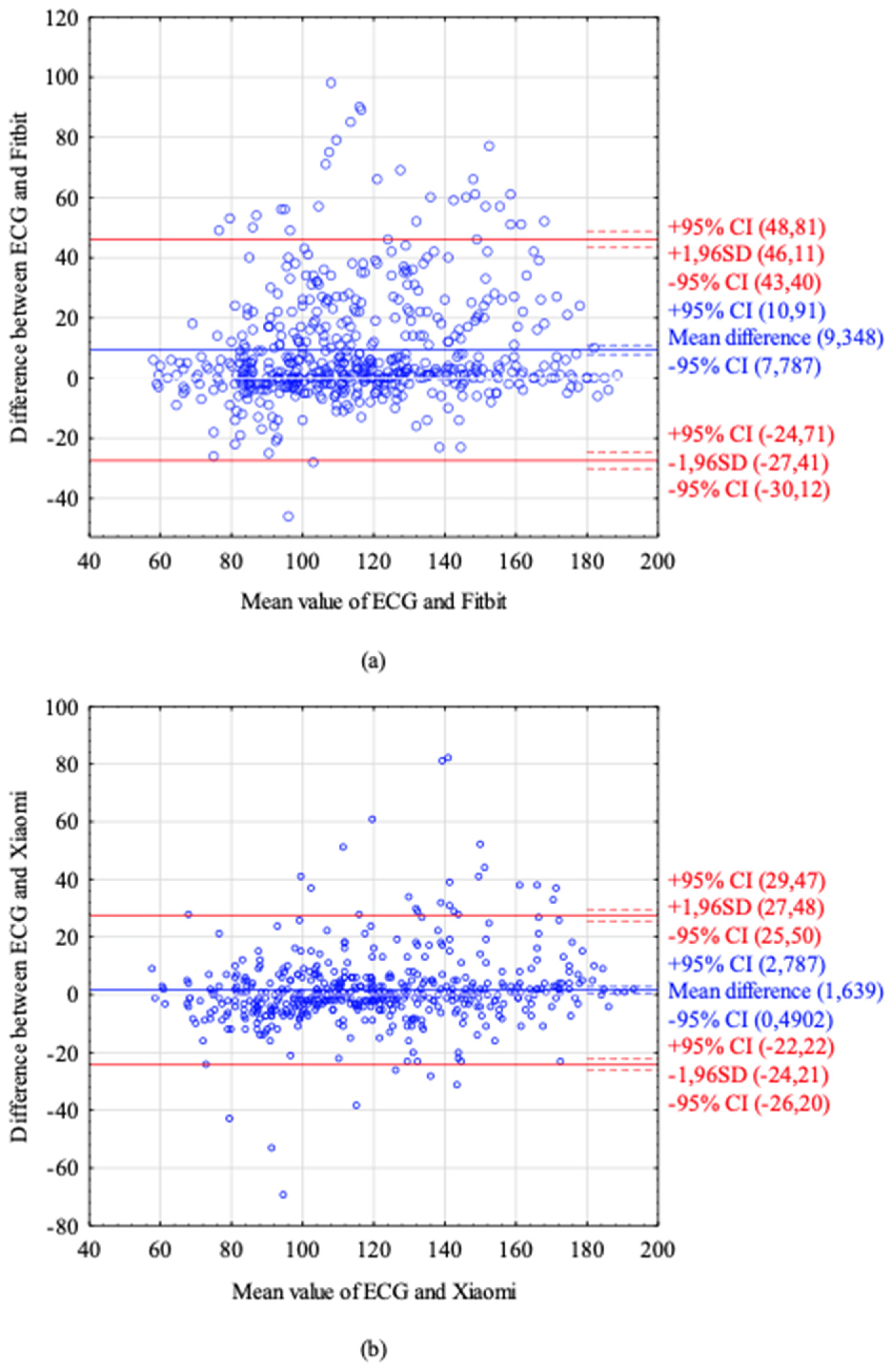
2.4. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Witt, D.R.; Kellogg, R.A.; Snyder, M.P.; Dunn, J. Windows into human health through wearables data analytics. Curr. Opin. Biomed. Eng. 2019, 9, 28–46. [Google Scholar] [CrossRef]
- Henriksen, A.; Mikalsen, M.H.; Woldaregay, A.Z.; Muzny, M.; Hartvigsen, G.; Hopstock, L.A.; Grimsgaard, S. Using Fitness Trackers and Smartwatches to Measure Physical Activity in Research: Analysis of Consumer Wrist-Worn Wearables. J. Med. Internet Res. 2018, 20, e110. [Google Scholar] [CrossRef] [PubMed]
- Batalik, L.; Dosbaba, F.; Hartman, M.; Batalikova, K.; Spinar, J. Benefits and effectiveness of using a wrist heart rate monitor as a telerehabilitation device in cardiac patients. Medicine 2020, 99, e19556. [Google Scholar] [CrossRef] [PubMed]
- Allen, J. Photoplethysmography and its application in clinical physiological measurement. Physiol. Meas. 2007, 28, R1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thiebaud, R.S.; Funk, M.D.; Patton, J.C.; Massey, B.L.; Shay, T.E.; Schmidt, M.G.; Giovannitti, N. Validity of wrist-worn consumer products to measure heart rate and energy expenditure. Digit. Health 2018, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jo, E.; Lewis, K.; Directo, D.; Kim, M.J.; Dolezal, B.A. Validation of Biofeedback Wearables for Photoplethysmographic Heart Rate Tracking. J. Sports Sci. Med. 2016, 15, 540. [Google Scholar] [PubMed]
- Dooley, E.E.; Golaszewski, N.M.; Bartholomew, J.B. Estimating Accuracy at Exercise Intensities: A Comparative Study of Self-Monitoring Heart Rate and Physical Activity Wearable Devices. JMIR mHealth uHealth 2017, 5, e34. [Google Scholar] [CrossRef] [PubMed]
- Gillinov, S.; Etiwy, M.; Wang, R.; Blackburn, G.; Phelan, D.; Gillinov, A.M.; Houghtaling, P.; Javadikasgari, H.; Desai, M.Y. Variable Accuracy of Wearable Heart Rate Monitors during Aerobic Exercise. Med. Sci. Sports Exerc. 2017, 49, 1697–1703. [Google Scholar] [CrossRef] [PubMed]
- Stahl, S.E.; An, H.-S.; Dinkel, D.M.; Noble, J.M.; Lee, J.-M. How accurate are the wrist-based heart rate monitors during walking and running activities? Are they accurate enough? BMJ Open Sport Exerc. Med. 2016, 2, e000106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boudreaux, B.; Hebert, E.P.; Hollander, D.B.; Williams, B.M.; Cormier, C.L.; Naquin, M.R.; Gillan, W.W.; Gusew, E.E.; Kraemer, R.R. Validity of Wearable Activity Monitors during Cycling and Resistance Exercise. Med. Sci. Sports Exerc. 2018, 50, 624–633. [Google Scholar] [CrossRef] [PubMed]
- Kendall, B.; Bellovary, B.; Gothe, N.P. Validity of wearable activity monitors for tracking steps and estimating energy expenditure during a graded maximal treadmill test. J. Sports Sci. 2019, 37, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Chow, H.-W.; Yang, C.-C. Accuracy of Optical Heart Rate Sensing Technology in Wearable Fitness Trackers for Young and Older Adults: Validation and Comparison Study. JMIR mHealth uHealth 2020, 8, e14707. [Google Scholar] [CrossRef] [PubMed]
- Shcherbina, A.; Mattsson, C.M.; Waggott, D.; Salisbury, H.; Christle, J.W.; Hastie, T.; Wheeler, M.T.; Ashley, E.A. Accuracy in Wrist-Worn, Sensor-Based Measurements of Heart Rate and Energy Expenditure in a Diverse Cohort. J. Pers. Med. 2017, 7, 3. [Google Scholar] [CrossRef] [PubMed]
- De Novo Classification Request for ECG App. Food and Drug Administration, 2018. Available online: https://www.accessdata.fda.gov/cdrh_docs/reviews/DEN180044.pdf (accessed on 17 December 2021).
- Sehgal, S.; Chowdhury, A.; Rabih, F.; Gadre, A.; Park, M.M.; Li, M.; Wang, X.; Highland, K.B. Counting Steps: A New Way to Monitor Patients with Pulmonary Arterial Hypertension. Lung 2019, 197, 501–508. [Google Scholar] [CrossRef] [PubMed]
- Hao, Y.; Ma, X.-K.; Zhu, Z.; Cao, Z.-B. Validity of Wrist-Wearable Activity Devices for Estimating Physical Activity in Adolescents: Comparative Study. JMIR mHealth uHealth 2021, 9, e18320. [Google Scholar] [CrossRef]
- Broekhuizen, K.; De Gelder, J.; Wijsman, C.A.; Wijsman, L.W.; Westendorp, R.G.; Verhagen, E.; Slagboom, P.E.; De Craen, A.J.; Van Mechelen, W.; Van Heemst, D.; et al. An Internet-Based Physical Activity Intervention to Improve Quality of Life of Inactive Older Adults: A Randomized Controlled Trial. J. Med. Internet Res. 2016, 18, e74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alley, S.; Schoeppe, S.; Guertler, D.; Jennings, C.; Duncan, M.J.; Vandelanotte, C. Interest and preferences for using advanced physical activity tracking devices: Results of a national cross-sectional survey. BMJ Open 2016, 6, e011243. [Google Scholar] [CrossRef] [Green Version]
- Pasadyn, S.R.; Soudan, M.; Gillinov, M.; Houghtaling, P.; Phelan, D.; Gillinov, N.; Bittel, B.; Desai, M.Y. Accuracy of commercially available heart rate monitors in athletes: A prospective study. Cardiovasc. Diagn. Ther. 2019, 9, 379–385. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Functions | Fitbit Charge 4 | Xiaomi Mi Band 5 |
|---|---|---|
| Price | EUR 149.95 | ~EUR 40 |
| Battery life | Up to 7 days | Up to 14 days |
| GPS | Yes | No |
| Photoplethysmography (PPG) heart rate (HR) monitor | Yes (measured in 1 s intervals) | Yes |
| Syncing | Bluetooth, near-field communication (NFC) | Bluetooth |
| Operating system | Android, iOS | Android, iOS |
| Sleep Tracking | Yes | Yes |
| All-day activity tracking | Steps, distance, calories, activity time | Steps, calories, activity time |
| Training mode | Yes | Yes |
| Automatic exercise recognition | Yes | No |
| Waterproof | Up to 50 m | Up to 5 atm |
| Application | Yes | Yes |
| Payments | Yes | No |
| Smartphone notifications | Yes | Yes |
| Google FIT App | No | Yes |
| Internet application | Yes | No |
| Total | Female | Male | |
|---|---|---|---|
| n | 31 | 10 | 21 |
| Age (years) | 28 (18–71) | 27.5 (23–54) | 32 (18–71) |
| Height (cm) | 177.7 (±14.62) | 168 (±4.5) | 181.9 (±6.3) |
| BMI (kg/m2) | 23.5 (20.1–37.1) | 22 (20–23) | 24 (21–37.1) |
| Peak HR (BMP) | 164.7 (±19.9) | 161.1 (±13.8) | 166.5 (±22.4) |
| %HR MAX | 88.8 (±8.5) | 85.1 (±6.8) | 90.6 (±8.7) |
| METs | 14.3 (±3) | 12.7 (±1.2) | 15 (±3.2) |
| Subgroup (N Measurements) | Fitbit | Xiaomi | p | |||
|---|---|---|---|---|---|---|
| Absolute Error (BPM) | Absolute Percentage Error (%) | Absolute Error (BPM) | Absolute Percentage Error (%) | |||
| Total n = 557 | Mean | 12.84 ± 16.55 | 10.19 ± 11.79 | 7.99 ± 10.61 | 7.99 ± 10.61 | |
| Median | 6 (0–98) | 5.17 (0–63) | 4 (0–82) | 3.95 (0–115) | <0.0001 | |
| Male n = 391 | Mean | 12.59 ± 16.70 | 9.92 ± 11.67 | 7.74 ± 10.90 | 6.73 ± 10.35 | |
| Median | 5 (0–90) | 4.92 (0–63.01) | 4 (0–82) | 3.85 (0–115) | <0.001 | |
| Female n = 166 | Mean | 13.46 ± 16.21 | 10.83 ± 12.09 | 8.82 ± 9.58 | 7.40 ± 7.46 | |
| Median | 7 (0–98) | 6.08 (0–62.42) | 5 (0–44) | 4.84 (0–38.58) | 0.0528 | |
| Stage 0 nF = 93, nx = 84 | Mean | 7.56 ± 8.45 | 8.69 ± 9.06 | 8.08 ± 10.65 | 10.58 ± 17.14 | |
| Median | 5 (0–54) | 5.33 (0–47.37) | 5 (0–69) | 5.67 (0–115) | 0.86 | |
| Stage 1 nF = 90, nx = 81 | Mean | 12.81 ± 12.04 | 12.20 ± 11.27 | 4.58 ± 4.73 | 4.80 ± 5.32 | |
| Median | 8 (0–46) | 8.51 (0–63.01) | 3 (0–28) | 3.53 (0–34.15) | 0.001 | |
| Stage 2 nF = 93, nx = 84 | Mean | 11.78 ± 13.96 | 10.17 ± 11.66 | 6.68 ± 7.33 | 5.99 ± 5.77 | |
| Median | 6 (0–57) | 5.38 (0–50) | 4.5 (0–34) | 4.37 (0–23.13) | 0.0012 | |
| Stage 3 nF = 90, nx = 81 | Mean | 14.71 ± 19.60 | 10.61 ± 13.36 | 7.38 ± 8.01 | 5.53 ± 5.91 | |
| Median | 5 (0–98) | 3.88 (0–62.42) | 4 (0–29) | 2.88 (0–23.01) | 0.14 | |
| Stage 4 nF = 70, nx = 67 | Mean | 21.47 ± 21.67 | 13.16 ± 12.31 | 8.73 ±11.38 | 5.52 ± 7.28 | |
| Median | 16 (1–79) | 10.11 (0.57–53.02) | 4 (0–51) | 2.53 (0–37.22) | 0.0012 | |
| Stage 5 n = 25 | Mean | 21.6 ± 26.23 | 11.97 ± 12.88 | 12.72 ±16.19 | 7.41 ± 9.92 | |
| Median | 6 (0–85) | 3.33 (0–54.49) | 5 (0–61) | 2.76 (0–40.67) | 0.4 | |
| Stage 6 n = 6 | Mean | 1.67 ± 4.08 | 0.89 ± 2.18 | 46.5 ± 30.32 | 25.7 ± 16.87 | |
| Median | 0 (0–10) | 0 (0–5.35) | 42.5 (13–82) | 23.6 (7.22–45.05) | 0.017 | |
| Recovery nF = 90, nx = 81 | Mean | 9.2 ± 14.84 | 7.15 ± 10.51 | 8.33 ± 8.81 | 7.03 ± 7.81 | |
| Median | 4 (0–90) | 3.36 (0–55.9) | 6 (0–41) | 4.42 (0–39.58) | 0.38 | |
| Stage of Exercise | Fitbit (LCCC, 95% CI) | Xiaomi (LCCC, 95% CI) |
|---|---|---|
| Total | 0.753 (0.717–0.785) | 0.903 (0.886–0.917) |
| Stage 0 | 0.757 (0.655–0.831) | 0.675 (0.542–0.774) |
| Stage 1 | 0.3 (0.139–0.446) | 0.912 (0.867–0.942) |
| Stage 2 | 0.408 (0.250–0.545) | 0.795 (0.704–0.861) |
| Stage 3 | 0.228 (0.075–0.371) | 0.730 (0.612–0.816) |
| Stage 4 | 0.176 (0.04–0.305) | 0.660 (0.518–0.766) |
| Stage 5 | 0.051 (0.161–0.259) | 0.455 (0.209–0.647) |
| Recovery | 0.651 (0.517–0.753) | 0.851 (0.783–0.899) |
| Female | 0.688 (0.605–0.756) | 0.887 (0.842–0.919) |
| Male | 0.774 (0.743–0.809) | 0.906 (0.887–0.922) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jachymek, M.; Jachymek, M.T.; Kiedrowicz, R.M.; Kaźmierczak, J.; Płońska-Gościniak, E.; Peregud-Pogorzelska, M. Wristbands in Home-Based Rehabilitation—Validation of Heart Rate Measurement. Sensors 2022, 22, 60. https://doi.org/10.3390/s22010060
Jachymek M, Jachymek MT, Kiedrowicz RM, Kaźmierczak J, Płońska-Gościniak E, Peregud-Pogorzelska M. Wristbands in Home-Based Rehabilitation—Validation of Heart Rate Measurement. Sensors. 2022; 22(1):60. https://doi.org/10.3390/s22010060
Chicago/Turabian StyleJachymek, Magdalena, Michał T. Jachymek, Radosław M. Kiedrowicz, Jarosław Kaźmierczak, Edyta Płońska-Gościniak, and Małgorzata Peregud-Pogorzelska. 2022. "Wristbands in Home-Based Rehabilitation—Validation of Heart Rate Measurement" Sensors 22, no. 1: 60. https://doi.org/10.3390/s22010060
APA StyleJachymek, M., Jachymek, M. T., Kiedrowicz, R. M., Kaźmierczak, J., Płońska-Gościniak, E., & Peregud-Pogorzelska, M. (2022). Wristbands in Home-Based Rehabilitation—Validation of Heart Rate Measurement. Sensors, 22(1), 60. https://doi.org/10.3390/s22010060