
Converging Robotic Technologies in Targeted Neural Rehabilitation: A Review of Emerging Solutions and Challenges

 ,
,  ,
,  ,
, 

Abstract
1. Introduction
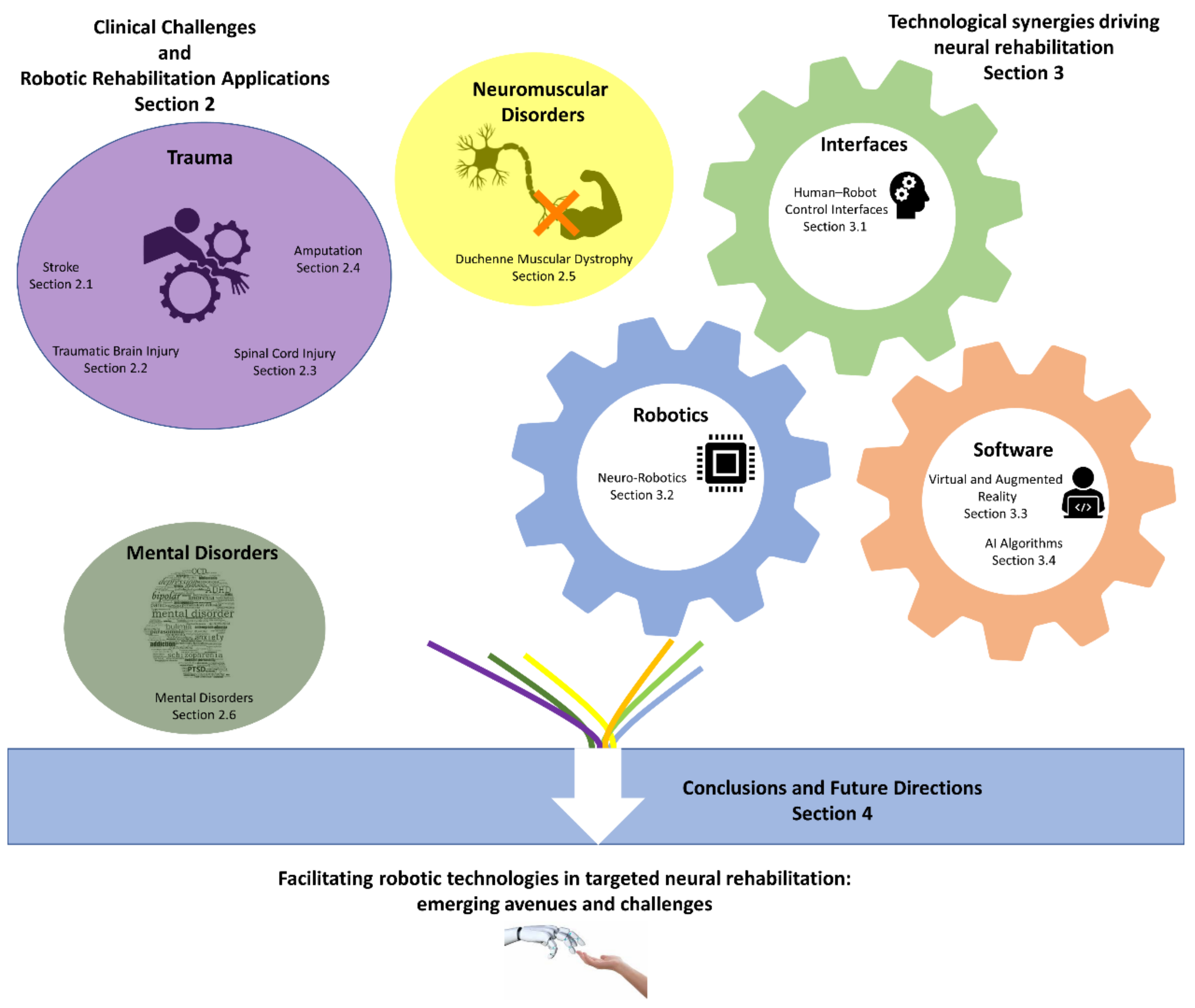
2. Clinical Challenges and Robotic Rehabilitation Applications
2.1. Stroke
2.2. Traumatic Brain Injury
2.3. Spinal Cord Injury
2.4. Amputation
2.5. Duchenne Muscular Dystrophy (DMD)
2.6. Mental Disorders
3. Technological Synergies Driving Neural Rehabilitation
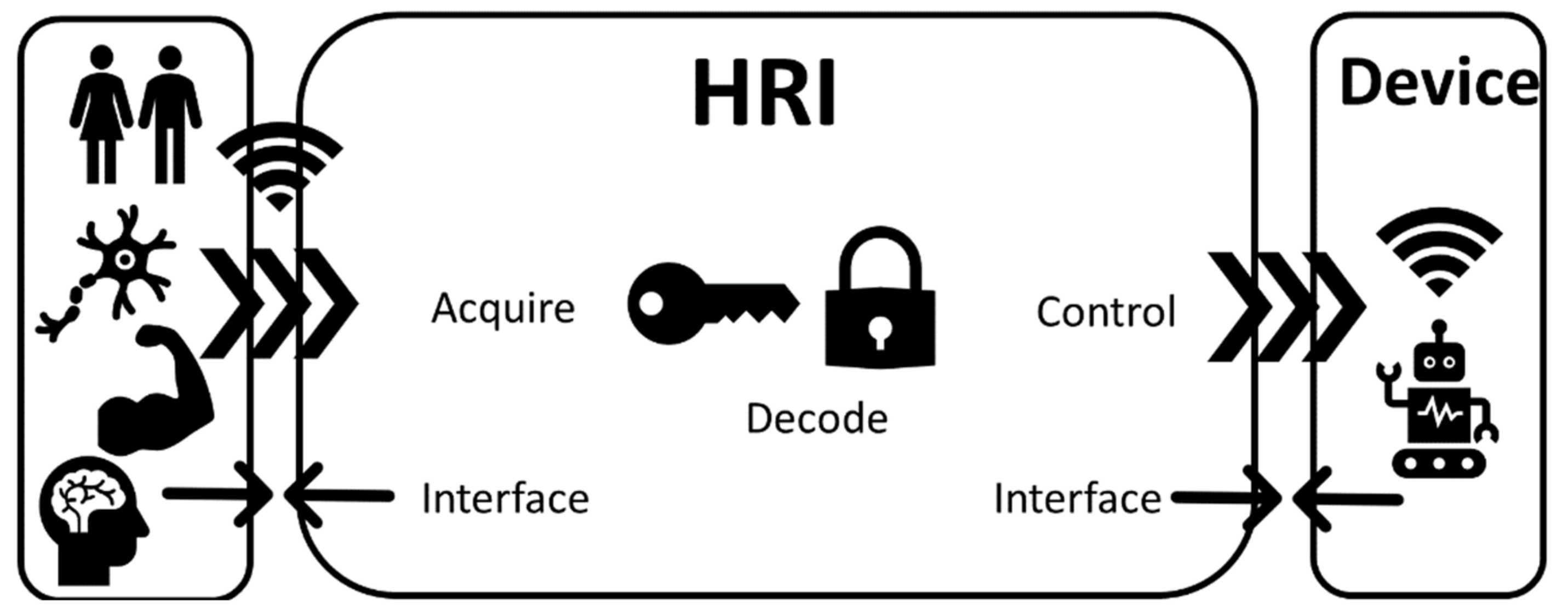
3.1. Human–Robot Control Interfaces
3.1.1. Digital–Neural Interfaces
3.1.2. Electromyography
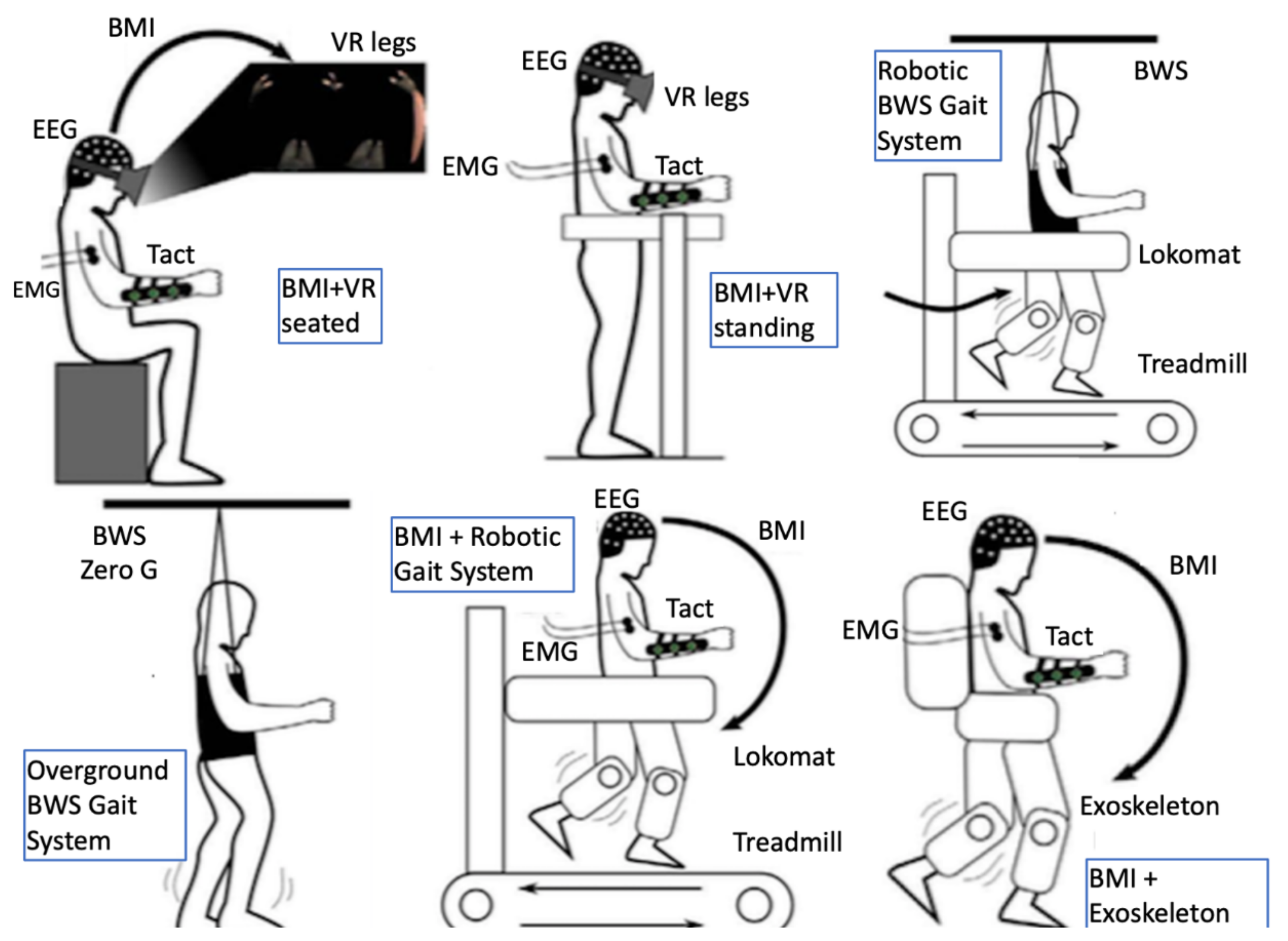
3.1.3. Brain–Computer Interfaces
3.2. Neuro-Robotics
3.2.1. Exoskeletons
Technological Challenges of Exoskeletons
Examples of Exoskeletons
3.2.2. Neuroprosthetics
Technological Challenges of Neuroprosthetics
Examples of Neuroprosthetics
3.3. Virtual and Augmented Reality
3.4. AI Algorithms
3.4.1. AI Algorithms for Human–Robot Interaction
3.4.2. AI Algorithms for Neural Signal Processing
4. Conclusions and Future Directions
5. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ADL | Activities of Daily Living |
| AI | Artificial Intelligence |
| ANN | Artificial Neural Network |
| AR | Augmented Reality |
| BCI | Brain–Computer Interface |
| CNN | Convolutional Neural Networks |
| CNS | Central Nervous System |
| DBS | Deep Brain Stimulation |
| DC | Direct Current |
| DL | Deep Learning |
| DMD | Duchenne Muscular Dystrophy |
| DOF | Degrees of Freedom |
| DQN | Deep Q-Networks |
| ECoG | Electrocorticography |
| EC-PC | Exponential-Component–Power-Component |
| EEG | Electroencephalography |
| EM | Expectation Maximization |
| EMG | Electromyography |
| FDA | Food and Drug Administration |
| FES | Functional Electrical Stimulation |
| GPU | Graphical Processing Units |
| HCI | Human–Computer Interaction |
| HMI | Human–Machine Interface |
| HRI | Human–Robot Interface |
| LL | Lower Limb |
| LSTM | Long Short-Term Memory |
| MEG | Magnetoencephalography |
| MEMS | Microelectromechanical Systems |
| ML | Machine Learning |
| MRI | Magnetic Resonance Imaging |
| MUs | Motor Units |
| NEMS | Nanoelectromechanical Systems |
| NLU | Natural Language Understanding |
| OC | Object Classification |
| PC | Personal Computer |
| PNS | Peripheral Nervous System |
| PCA | Principal Component Analysis |
| RF | Radio Frequency |
| RL | Reinforcement Learning |
| RNN | Recurrent Neural Networks |
| SCI | Spinal Cord Injury |
| TBI | Traumatic Brain Injury |
| TDCS | Transcranial Direct Current Stimulation |
| TMS | Transcranial Magnetic Stimulation |
| TMSR | Targeted Muscle and Sensory Reinnervation |
| UL | Upper Limb |
| VLSI | Very Large-Scale Integration |
| VR | Virtual Reality |
| VRE | Virtual Reality Environment |
| WT | Wavelet Transform |
| YOLO | You Only Look Once |
References
- Gassert, R.; Dietz, V. Rehabilitation robots for the treatment of sensorimotor deficits: A neurophysiological perspective. J. Neuroeng. Rehabil. 2018, 15, 1–15. [Google Scholar] [CrossRef]
- Hobbs, B.; Artemiadis, P. A Review of Robot-Assisted Lower-Limb Stroke Therapy: Unexplored Paths and Future Directions in Gait Rehabilitation. Front. Neurorobotics 2020, 14, 19. [Google Scholar] [CrossRef] [PubMed]
- Kleim, J.A.; Jones, T.A. Principles of Experience-Dependent Neural Plasticity: Implications for Rehabilitation After Brain Damage. J. Speech Lang. Hear. Res. 2008, 51, S225–S239. [Google Scholar] [CrossRef]
- Belda-Lois, J.M.; Horno, S.M.-D.; Bermejo-Bosch, I.; Moreno, J.C.; Pons, J.L.; Farina, D.; Iosa, M.; Molinari, M.; Tamburella, F.; Ramos-Murguialday, A.; et al. Rehabilitation of gait after stroke: A review towards a top-down approach. J. Neuroeng. Rehabil. 2011, 8, 66. [Google Scholar] [CrossRef]
- Fasoli, S.E.; Adans-Dester, C.P. A Paradigm Shift: Rehabilitation Robotics, Cognitive Skills Training, and Function After Stroke. Front. Neurol. 2019, 10, 1088. [Google Scholar] [CrossRef]
- Reinkensmeyer., D.J.; Dietz, V. (Eds.) Neurorehabilitation Technology; Springer International Publishing: Cham, Switzerland, 2016. [Google Scholar]
- Nizamis, K.; Stienen, A.H.; Kamper, D.G.; Keller, T.; Plettenburg, D.H.; Rouse, E.J.; Farina, D.; Koopman, B.F.J.M.; Sartori, M. Transferrable Expertise From Bionic Arms to Robotic Exoskeletons: Perspectives for Stroke and Duchenne Muscular Dystrophy. IEEE Trans. Med. Robot. Bionics 2019, 1, 88–96. [Google Scholar] [CrossRef]
- Eapen, B.C.; Murphy, D.P.; Cifu, D.X. Neuroprosthetics in amputee and brain injury rehabilitation. Exp. Neurol. 2017, 287, 479–485. [Google Scholar] [CrossRef] [PubMed]
- Graimann, B.; Dietl, H. Introduction to Upper Limb Prosthetics. In Introduction to Neural Engineering for Motor Rehabilitation; IEEE Press: Piscataway, NJ, USA, 2013; pp. 267–290. [Google Scholar]
- Basteris, A.; Nijenhuis, S.M.; Stienen, A.H.A.; Buurke, J.H.; Prange, G.B.; Amirabdollahian, F. Training modalities in robot-mediated upper limb rehabilitation in stroke: A framework for classification based on a systematic review. J. Neuroeng. Rehabil. 2014, 11, 111. [Google Scholar] [CrossRef]
- Morone, G.; Masiero, S.; Werner, C.; Paolucci, S. Advances in Neuromotor Stroke Rehabilitation. BioMed Res. Int. 2014, 2014, 1–2. [Google Scholar] [CrossRef]
- Mubin, O.; Alnajjar, F.; Jishtu, N.; Alsinglawi, B.; Al Mahmud, A. Exoskeletons with Virtual Reality, Augmented Reality, and Gamification for Stroke Patients’ Rehabilitation: Systematic Review. JMIR Rehabil. Assist. Technol. 2019, 6, e12010. [Google Scholar] [CrossRef] [PubMed]
- Fong, J.; Ocampo, R.; Tavakoli, M. Intelligent Robotics and Immersive Displays for Enhancing Haptic Interaction in Physical Rehabilitation Environments. In Haptic Interfaces for Accessibility, Health, and Enhanced Quality of Life; Springer: Cham, Switzerland, 2020; pp. 265–297. [Google Scholar]
- Jayaraman, A.; Marinov, B.; Singh, Y.; Burt, S.; Rymer, W.Z. Current Evidence for Use of Robotic Exoskeletons in Rehabilitation. In Wearable Robotics; Elsevier BV: Amsterdam, The Netherlands, 2020; pp. 301–310. [Google Scholar]
- Weber, L.M.; Stein, J. The use of robots in stroke rehabilitation: A narrative review. Neurorehabilitation 2018, 43, 99–110. [Google Scholar] [CrossRef]
- Hidler, J.; Sainburg, R. Role of Robotics in Neurorehabilitation. Top. Spinal Cord Inj. Rehabil. 2011, 17, 42–49. [Google Scholar] [CrossRef][Green Version]
- Major, Z.Z.; Vaida, C.; Major, K.A.; Tucan, P.; Simori, G.; Banica, A.; Brusturean, E.; Burz, A.; Craciunas, R.; Ulinici, I.; et al. The Impact of Robotic Rehabilitation on the Motor System in Neurological Diseases. A Multimodal Neurophysiological Approach. Int. J. Environ. Res. Public Health 2020, 17, 6557. [Google Scholar] [CrossRef]
- Iandolo, R.; Marini, F.; Semprini, M.; Laffranchi, M.; Mugnosso, M.; Cherif, A.; De Michieli, L.; Chiappalone, M.; Zenzeri, J. Perspectives and Challenges in Robotic Neurorehabilitation. Appl. Sci. 2019, 9, 3183. [Google Scholar] [CrossRef]
- Reinkensmeyer, D.J.; Blackstone, S.; Bodine, C.; Brabyn, J.; Brienza, D.; Caves, K.; DeRuyter, F.; Durfee, E.; Fatone, S.; Fernie, G.; et al. How a diverse research ecosystem has generated new rehabilitation technologies: Review of NIDILRR’s Rehabilitation Engineering Research Centers. J. Neuroeng. Rehabil. 2017, 14, 109. [Google Scholar] [CrossRef]
- Poli, P.; Morone, G.; Rosati, G.; Masiero, S. Robotic Technologies and Rehabilitation: New Tools for Stroke Patients’ Therapy. BioMed Res. Int. 2013, 2013, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Virani, S.S.; Alonso, A.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics—2020 Update: A Report from the American Heart Association. Circulation 2020, 141, e139–e596. [Google Scholar] [CrossRef]
- Thrift, A.G.; Thayabaranathan, T.; Howard, G.; Howard, V.J.; Rothwell, P.M.; Feigin, V.L.; Norrving, B.; Donnan, G.A.; Cadilhac, D.A. Global stroke statistics. Int. J. Stroke 2017, 12, 13–32. [Google Scholar] [CrossRef] [PubMed]
- Coleman, E.R.; Moudgal, R.; Lang, K.; Hyacinth, H.I.; Awosika, O.O.; Kissela, B.M.; Feng, W. Early Rehabilitation After Stroke: A Narrative Review. Curr. Atheroscler. Rep. 2017, 19, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Mazzoleni, S.; Duret, C.; Grosmaire, A.G.; Battini, E. Combining Upper Limb Robotic Rehabilitation with Other Therapeutic Approaches after Stroke: Current Status, Rationale, and Challenges. BioMed Res. Int. 2017, 2017, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Veerbeek, J.M.; Langbroek-Amersfoort, A.C.; Van Wegen, E.E.H.; Meskers, C.G.M.; Kwakkel, G. Effects of Robot-Assisted Therapy for the Upper Limb After Stroke. Neurorehabilit. Neural Repair 2016, 31, 107–121. [Google Scholar] [CrossRef] [PubMed]
- Whitfield, P.C.; Thomas, E.O.; Summers, F.; Whyte, M.; Hutchinson, P.J. (Eds.) Head Injury: A Multidisciplinary Approach; Cambridge University Press: Cambridge, UK, 2009. [Google Scholar]
- Dewan, M.C.; Rattani, A.; Gupta, S.; Baticulon, R.E.; Hung, Y.-C.; Punchak, M.; Agrawal, A.; Adeleye, A.O.; Shrime, M.G.; Rubiano, A.M.; et al. Estimating the global incidence of traumatic brain injury. J. Neurosurg. 2019, 130, 1080–1097. [Google Scholar] [CrossRef] [PubMed]
- Bigler, E.D. Anterior and middle cranial fossa in traumatic brain injury: Relevant neuroanatomy and neuropathology in the study of neuropsychological outcome. Neuropsychology 2007, 21, 515–531. [Google Scholar] [CrossRef] [PubMed]
- Miotto, E.C.; Cinalli, F.Z.; Serrao, V.T.; Benute, G.G.; Lucia, M.C.S.; Scaff, M. Cognitive deficits in patients with mild to moderate traumatic brain injury. Arq. Neuro-Psiquiatria 2010, 68, 862–868. [Google Scholar] [CrossRef]
- Zelek, V. QEEG Brainwave Amplitude and Coherence Values as Predictors of Cognitive Improvement to Neurofeedback After Moderate-to-Severe Acquired Brain Injury. J. Head Trauma Rehabil. 2008, 23, 343. [Google Scholar] [CrossRef]
- Mathias, J.L.; Wheaton, P. Changes in attention and information-processing speed following severe traumatic brain injury: A meta-analytic review. Neuropsychology 2007, 21, 212–223. [Google Scholar] [CrossRef] [PubMed]
- Haneef, Z.; Levin, H.S.; Frost, J.D.; Mizrahi, E.M. Electroencephalography and Quantitative Electroencephalography in Mild Traumatic Brain Injury. J. Neurotrauma 2013, 30, 653–656. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, D.; Stockdale, S.; Van Egren, L. EEG neurofeedback in the treatment of mild traumatic brain injury. Clin. Electroencephalogr. 1996, 24, 6. [Google Scholar]
- Walker, J.E.; Norman, C.A.; Weber, R.K. Impact of qEEG-Guided Coherence Training for Patients with a Mild Closed Head Injury. J. Neurother. 2002, 6, 31–43. [Google Scholar] [CrossRef]
- Zorcec, T.; Demerdzieva, A.; Jordanova, P.; Qeeg, N. Brain Rate, Executive Functions and Neurofeedback Training in Patients with Traumatic Brain Injury. Acta Inform. Medica 2011, 19, 23–28. [Google Scholar]
- Barco, A.; Albo-Canals, J.; Ng, M.K.; Garriga, C.; Callejón, L.; Turon, M.; Gomez, C.; López-Sala, A. A robotic therapy for children with TBI. In Proceedings of the 2013 8th ACM/IEEE International Conference on Human-Robot Interaction (HRI), Tokyo, Japan, 3–6 March 2013; pp. 75–76. [Google Scholar]
- Matarić, M.; Tapus, A.; Winstein, C.; Eriksson, J. Socially assistive robotics for stroke and mild TBI rehabilitation. Stud. Health Technol. Inform. 2009, 145, 249–262. [Google Scholar]
- Sacco, K.; Cauda, F.; D’Agata, F.; Duca, S.; Zettin, M.; Virgilio, R.; Nascimbeni, A.; Belforte, G.; Eula, G.; Gastaldi, L.; et al. A combined robotic and cognitive training for locomotor rehabilitation: Evidences of cerebral functional reorganization in two chronic traumatic brain injured patients. Front. Hum. Neurosci. 2011, 5, 146. [Google Scholar] [CrossRef] [PubMed]
- Debert, C.T.; Herter, T.M.; Scott, S.H.; Dukelow, S. Robotic Assessment of Sensorimotor Deficits After Traumatic Brain Injury. J. Neurol. Phys. Ther. 2012, 36, 58–67. [Google Scholar] [CrossRef]
- Nolan, K.J.; Karunakaran, K.K.; Ehrenberg, N.; Kesten, A.G. Robotic Exoskeleton Gait Training for Inpatient Rehabilitation in a Young Adult with Traumatic Brain Injury. In Proceedings of the 2018 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 17–21 July 2018; Volume 2018, pp. 2809–2812. [Google Scholar]
- Resquín, F.; Gonzalez-Vargas, J.; Ibáñez, J.; Brunetti, F.; Dimbwadyo, I.; Carrasco, L.; Alves, S.; Gonzalez-Alted, C.; Gomez-Blanco, A.; Pons, J.L. Adaptive hybrid robotic system for rehabilitation of reaching movement after a brain injury: A usability study. J. Neuroeng. Rehabil. 2017, 14, 104. [Google Scholar] [CrossRef]
- Antoniou, P.E.; Athanasiou, A.; Bamidis, P.D. Virtual and augmented reality in neuroscience. In Neurotechnology: Methods, Advances and Applications; The Institution of Engineering and Technology (The IET): Stevenage, UK, 2020; pp. 69–96. [Google Scholar]
- Sessoms, P.H.; Gottshall, K.R.; Collins, J.-D.; Markham, A.E.; Service, K.A.; Reini, S.A. Improvements in Gait Speed and Weight Shift of Persons with Traumatic Brain Injury and Vestibular Dysfunction Using a Virtual Reality Computer-Assisted Rehabilitation Environment. Mil. Med. 2015, 180, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Zanier, E.R.; Zoerle, T.; Di Lernia, D.; Riva, G. Virtual Reality for Traumatic Brain Injury. Front. Neurol. 2018, 9, 345. [Google Scholar] [CrossRef] [PubMed]
- Maggio, M.G.; Torrisi, M.; Buda, A.; De Luca, R.; Piazzitta, D.; Cannavò, A.; Leo, A.; Milardi, D.; Manuli, A.; Calabro, R.S. Effects of robotic neurorehabilitation through lokomat plus virtual reality on cognitive function in patients with traumatic brain injury: A retrospective case-control study. Int. J. Neurosci. 2019, 130, 117–123. [Google Scholar] [CrossRef]
- 2016 Annual Report - Complete Public Version.pdf. Available online: https://www.nscisc.uab.edu/Public/2016%20Annual%20Report%20-%20Complete%20Public%20Version.pdf (accessed on 29 April 2020).
- Sweis, R.; Biller, J. Systemic Complications of Spinal Cord Injury. Curr. Neurol. Neurosci. Rep. 2017, 17, 8. [Google Scholar] [CrossRef] [PubMed]
- Gowinnage, S.S.; Arambepola, C. Quality of life and its determinants among community re-integrated soldiers with permanent disabilities following traumatic limb injuries. Qual. Life Res. 2020, 29, 2119–2127. [Google Scholar] [CrossRef]
- Chang, F.-H.; Liu, C.-H.; Hung, H.-P. An in-depth understanding of the impact of the environment on participation among people with spinal cord injury. Disabil. Rehabil. 2017, 40, 2192–2199. [Google Scholar] [CrossRef]
- McDaid, D.; Park, A.-L.; Gall, A.; Purcell, M.; Bacon, M. Understanding and modelling the economic impact of spinal cord injuries in the United Kingdom. Spinal Cord 2019, 57, 778–788. [Google Scholar] [CrossRef]
- Scivoletto, G. The Rehabilitation of Spinal Cord Injury Patients in Europe. Trends Reconstr. Neurosurg. 2017, 124, 203–210. [Google Scholar]
- Mekki, M.; Delgado, A.D.; Fry, A.; Putrino, D.; Huang, V. Robotic Rehabilitation and Spinal Cord Injury: A Narrative Review. Neurother 2018, 15, 604–617. [Google Scholar] [CrossRef] [PubMed]
- Esquenazi, A.; Talaty, M.; Packel, A.; Saulino, M. The ReWalk Powered Exoskeleton to Restore Ambulatory Function to Individuals with Thoracic-Level Motor-Complete Spinal Cord Injury. Am. J. Phys. Med. Rehabil. 2012, 91, 911–921. [Google Scholar] [CrossRef]
- Mehrholz, J.; A Harvey, L.; Thomas, S.; Elsner, B. Is body-weight-supported treadmill training or robotic-assisted gait training superior to overground gait training and other forms of physiotherapy in people with spinal cord injury? A systematic review. Spinal Cord 2017, 55, 722–729. [Google Scholar] [CrossRef]
- Swinnen, E.; Duerinck, S.; Baeyens, J.-P.; Meeusen, R.; Kerckhofs, E. Effectiveness of robot-assisted gait training in persons with spinal cord injury: A systematic review. J. Rehabil. Med. 2010, 42, 520–526. [Google Scholar] [CrossRef] [PubMed]
- Athanasiou, A.; Arfaras, G.; Pandria, N.; Xygonakis, I.; Foroglou, N.; Astaras, A.; Bamidis, P.D. Wireless Brain-Robot Interface: User Perception and Performance Assessment of Spinal Cord Injury Patients. Wirel. Commun. Mob. Comput. 2017, 2017, 1–16. [Google Scholar] [CrossRef]
- Fakhoury, M. Spinal cord injury: Overview of experimental approaches used to restore locomotor activity. Rev. Neurosci. 2015, 26, 397–405. [Google Scholar] [CrossRef]
- Donati, A.R.C.; Shokur, S.; Morya, E.; Campos, D.S.F.; Moioli, R.C.; Gitti, C.M.; Augusto, P.B.; Tripodi, S.; Pires, C.G.; Pereira, G.A.; et al. Long-Term Training with a Brain-Machine Interface-Based Gait Protocol Induces Partial Neurological Recovery in Paraplegic Patients. Sci. Rep. 2016, 6, 30383. [Google Scholar] [CrossRef]
- Athanasiou, A.; Klados, M.A.; Pandria, N.; Foroglou, N.; Kavazidi, K.R.; Polyzoidis, K.; Bamidis, P.D. A Systematic Review of Investigations into Functional Brain Connectivity Following Spinal Cord Injury. Front. Hum. Neurosci. 2017, 11, 517. [Google Scholar] [CrossRef]
- Ahuja, C.S.; Nori, S.; Tetreault, L.; Wilson, J.; Kwon, B.; Harrop, J.; Choi, D.; Fehlings, M.G. Traumatic Spinal Cord Injury—Repair and Regeneration. Neurosurgery 2017, 80, S9–S22. [Google Scholar] [CrossRef] [PubMed]
- Koffler, J.; Zhu, W.; Qu, X.; Platoshyn, O.; Dulin, J.N.; Brock, J.; Graham, L.; Lu, P.; Sakamoto, J.; Marsala, M.; et al. Biomimetic 3D-printed scaffolds for spinal cord injury repair. Nat. Med. 2019, 25, 263–269. [Google Scholar] [CrossRef]
- Bunday, K.L.; Urbin, M.; Perez, M.A. Potentiating paired corticospinal-motoneuronal plasticity after spinal cord injury. Brain Stimul. 2018, 11, 1083–1092. [Google Scholar] [CrossRef]
- Formento, E.; Minassian, K.; Wagner, F.; Mignardot, J.B.; Le Goff-Mignardot, C.G.; Rowald, A.; Bloch, J.; Micera, S.; Capogrosso, M.; Courtine, G. Electrical spinal cord stimulation must preserve proprioception to enable locomotion in humans with spinal cord injury. Nat. Neurosci. 2018, 21, 1728–1741. [Google Scholar] [CrossRef]
- Wagner, F.B.; Mignardot, J.-B.; Le Goff-Mignardot, C.G.; Demesmaeker, R.; Komi, S.; Capogrosso, M.; Rowald, A.; Seáñez, I.; Caban, M.; Pirondini, E.; et al. Targeted neurotechnology restores walking in humans with spinal cord injury. Nat. Cell Biol. 2018, 563, 65–71. [Google Scholar] [CrossRef]
- Shokur, S.; Donati, A.R.C.; Campos, D.S.F.; Gitti, C.; Bao, G.; Fischer, D.; Almeida, S.; Braga, V.A.S.; Augusto, P.; Petty, C.; et al. Training with brain-machine interfaces, visuo-tactile feedback and assisted locomotion improves sensorimotor, visceral, and psychological signs in chronic paraplegic patients. PLoS ONE 2018, 13, e0206464. [Google Scholar] [CrossRef] [PubMed]
- Selfslagh, A.; Shokur, S.; Campos, D.S.F.; Donati, A.R.C.; Almeida, S.; Yamauti, S.Y.; Coelho, D.B.; Bouri, M.; Nicolelis, M.A.L. Non-invasive, Brain-controlled Functional Electrical Stimulation for Locomotion Rehabilitation in Individuals with Paraplegia. Sci. Rep. 2019, 9, 1–17. [Google Scholar] [CrossRef]
- Cappello, L.; Meyer, J.T.; Galloway, K.C.; Peisner, J.D.; Granberry, R.; Wagner, D.A.; Engelhardt, S.; Paganoni, S.; Walsh, C.J. Assisting hand function after spinal cord injury with a fabric-based soft robotic glove. J. Neuroeng. Rehabil. 2018, 15, 1–10. [Google Scholar] [CrossRef]
- Mitsopoulos, K. Design of a Prehensile Rehabilitation Assistant for Directed Actuation,” Aristotle University of Thessaloniki, Thessaloniki. 2020. Available online: http://ikee.lib.auth.gr/record/318391?ln=en (accessed on 14 March 2021).
- Ziegler-Graham, K.; MacKenzie, E.J.; Ephraim, P.L.; Travison, T.G.; Brookmeyer, R. Estimating the Prevalence of Limb Loss in the United States: 2005 to 2050. Arch. Phys. Med. Rehabil. 2008, 89, 422–429. [Google Scholar] [CrossRef]
- Wheaton, L.A. Neurorehabilitation in upper limb amputation: Understanding how neurophysiological changes can affect functional rehabilitation. J. Neuroeng. Rehabil. 2017, 14, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Sansam, K.; Neumann, V.; O’Connor, R.; Bhakta, B. Predicting walking ability following lower limb amputation: A systematic review of the literature. J. Rehabil. Med. 2009, 41, 593–603. [Google Scholar] [CrossRef] [PubMed]
- Esquenazi, A. Amputation rehabilitation and prosthetic restoration. From surgery to community reintegration. Disabil. Rehabil. 2004, 26, 831–836. [Google Scholar] [CrossRef] [PubMed]
- Carey, S.L.; Lura, D.J.; Highsmith, M.J. Differences in myoelectric and body-powered upper-limb prostheses: Systematic literature review. J. Rehabil. Res. Dev. 2015, 52, 247–262. [Google Scholar] [CrossRef] [PubMed]
- Nizamis, K.; Rijken, N.H.M.; Van Middelaar, R.; Neto, J.; Koopman, B.F.J.M.; Sartori, M. Characterization of Forearm Muscle Activation in Duchenne Muscular Dystrophy via High-Density Electromyography: A Case Study on the Implications for Myoelectric Control. Front. Neurol. 2020, 11, 231. [Google Scholar] [CrossRef] [PubMed]
- Pangalila, R.F.; Bartels, B.; Bergen, M.P.; Cobben, N.A.M.; Stam, H.J.; Roebroeck, M.E. Upper limb function in adults with Duchenne muscular dystrophy. J. Rehabil. Med. 2011, 43, 770–775. [Google Scholar] [CrossRef]
- Darras, B.T.; Urion, D.K.; Ghosh, P.S. Dystrophinopathies. In GeneReviews®; Adam, M.P., Ardinger, H.H., Pagon, R.A., Wallace, S.E., Bean, L.J., Stephens, K., Amemiya, A., Eds.; University of Washington: Seattle, WA, USA, 1993. [Google Scholar]
- Opstal, S.L.S.H.; Jansen, M.; Van Alfen, N.; De Groot, I.J.M. Health-Related Quality of Life and Its Relation to Disease Severity in Boys with Duchenne Muscular Dystrophy. J. Child Neurol. 2013, 29, 1486–1495. [Google Scholar] [CrossRef] [PubMed]
- Eagle, M.; Baudouin, S.V.; Chandler, C.; Giddings, D.R.; Bullock, R.; Bushby, K. Survival in Duchenne muscular dystrophy: Improvements in life expectancy since 1967 and the impact of home nocturnal ventilation. Neuromuscul. Disord. 2002, 12, 926–929. [Google Scholar] [CrossRef]
- Bergsma, A.; Lobo-Prat, J.; Vroom, E.; Furlong, P.; Herder, J.L.; Corrigan, M.; De Groot, I.; Faisal, A.; Goemans, N.; Han, J.; et al. 1st Workshop on Upper-Extremity Assistive Technology for People with Duchenne: State of the art, emerging avenues, and challenges. Neuromuscul. Disord. 2016, 26, 386–393. [Google Scholar] [CrossRef] [PubMed]
- Wagner, M.B.; Vignos, P.J.; Carlozzi, C. Duchenne muscular dystrophy: A study of wrist and hand function. Muscle Nerve 1989, 12, 236–244. [Google Scholar] [CrossRef]
- Janssen, M.M.H.P.; Bergsma, A.; Geurts, A.C.H.; De Groot, I.J.M. Patterns of decline in upper limb function of boys and men with DMD: An international survey. J. Neurol. 2014, 261, 1269–1288. [Google Scholar] [CrossRef]
- Pratt, J.L. Control Interfaces to Actively Support the Arm Function of Men with Duchenn Muscular Dystrophy. Ph.D. Thesis, University of Twente, Enschede, The Netherlands, 2016. [Google Scholar]
- Mahmood, M.N.; Peeters, L.H.C.; Paalman, M.; Verkerke, G.J.; Kingma, I.; Van Dieën, J.H. Development and evaluation of a passive trunk support system for Duchenne muscular dystrophy patients. J. Neuroeng. Rehabil. 2018, 15, 22. [Google Scholar] [CrossRef]
- Verros, S.; Mahmood, N.; Peeters, L.; Lobo-Prat, J.; Bergsma, A.; Hekman, E.; Verkerke, G.J.; Koopman, B. Evaluation of Control Interfaces for Active Trunk Support. IEEE Trans. Neural Syst. Rehabil. Eng. 2018, 26, 1965–1974. [Google Scholar] [CrossRef] [PubMed]
- Bos, R.A.; Nizamis, K.; Koopman, B.F.J.M.; Herder, J.L.; Sartori, M.; Plettenburg, D.H. A Case Study With Symbihand: An sEMG-Controlled Electrohydraulic Hand Orthosis for Individuals With Duchenne Muscular Dystrophy. IEEE Trans. Neural Syst. Rehabil. Eng. 2019, 28, 258–266. [Google Scholar] [CrossRef]
- Bos, R.A.; Nizamis, K.; Plettenburg, D.H.; Herder, J.L. Design of an Electrohydraulic Hand Orthosis for People with Duchenne Muscular Dystrophy Using Commercially Available Components. In Proceedings of the 2018 7th IEEE International Conference on Biomedical Robotics and Biomechatronics (Biorob), Enschede, The Netherlands, 27–29 August 2018; pp. 305–311. [Google Scholar]
- Nizamis, K. Hand Neuro-Motor Characterization and Motor Intention Decoding in Duchenne Muscular Dystrophy. Ph.D. Thesis, University of Twente, Enschede, The Netherlands, 2019. [Google Scholar]
- Desguerre, I.; Christov, C.; Mayer, M.; Zeller, R.; Becane, H.-M.; Bastuji-Garin, S.; Leturcq, F.; Chiron, C.; Chelly, J.; Gherardi, R.K. Clinical Heterogeneity of Duchenne Muscular Dystrophy (DMD): Definition of Sub-Phenotypes and Predictive Criteria by Long-Term Follow-Up. PLoS ONE 2009, 4, e4347. [Google Scholar] [CrossRef] [PubMed]
- Bushby, K.; Finkel, R.; Birnkrant, D.J.; Case, L.E.; Clemens, P.R.; Cripe, L.; Kaul, A.; Kinnett, K.; McDonald, C.; Pandya, S.; et al. Diagnosis and management of Duchenne muscular dystrophy, part 1: Diagnosis, and pharmacological and psychosocial management. Lancet Neurol. 2010, 9, 77–93. [Google Scholar] [CrossRef]
- Bushby, K.; Finkel, R.; Birnkrant, D.J.; Case, L.E.; Clemens, P.R.; Cripe, L.; Kaul, A.; Kinnett, K.; McDonald, C.; Pandya, S.; et al. Diagnosis and management of Duchenne muscular dystrophy, part 2: Implementation of multidisciplinary care. Lancet Neurol. 2010, 9, 177–189. [Google Scholar] [CrossRef]
- Riek, L.D. Robotics Technology in Mental Health Care. In Artificial Intelligence in Behavioral and Mental Health Care; Elsevier BV: Amsterdam, The Netherlands, 2016; pp. 185–203. [Google Scholar]
- Kleih, S.; Nijboer, F.; Halder, S.; Kübler, A. Motivation modulates the P300 amplitude during brain–computer interface use. Clin. Neurophysiol. 2010, 121, 1023–1031. [Google Scholar] [CrossRef]
- Wood, G.; Kober, S.E.; Witte, M.; Neuper, C. On the need to better specify the concept in brain-computer-interfaces/neurofeedback research. Front. Syst. Neurosci. 2014, 8, 171. [Google Scholar] [CrossRef]
- Ziemke, T.; Lowe, R.; Morse, A. Affective robotics modelling emotion and motivation. Connect. Sci. 2010, 22, 193–195. [Google Scholar] [CrossRef]
- Luneski, A.; Konstantinidis, E.; Bamidis, P.D. Affective Medicine. Methods Inf. Med. 2010, 49, 207–218. [Google Scholar] [CrossRef] [PubMed]
- Rouaix, N.; Retru-Chavastel, L.; Rigaud, A.-S.; Monnet, C.; Lenoir, H.; Pino, M. Affective and Engagement Issues in the Conception and Assessment of a Robot-Assisted Psychomotor Therapy for Persons with Dementia. Front. Psychol. 2017, 8, 950. [Google Scholar] [CrossRef] [PubMed]
- Scoglio, A.A.; Reilly, E.D.; Gorman, J.A.; Drebing, C.E. Use of Social Robots in Mental Health and Well-Being Research: Systematic Review. J. Med. Internet Res. 2019, 21, e13322. [Google Scholar] [CrossRef]
- Jerčić, P.; Hagelbäck, J.; Lindley, C. An affective serious game for collaboration between humans and robots. Entertain. Comput. 2019, 32, 100319. [Google Scholar] [CrossRef]
- Lorenzetti, V.; Melo, B.; Basílio, R.; Suo, C.; Yücel, M.; Tierra-Criollo, C.J.; Moll, J. Emotion Regulation Using Virtual Environments and Real-Time fMRI Neurofeedback. Front. Neurol. 2018, 9, 390. [Google Scholar] [CrossRef]
- Fernández-Caballero, A.; Navarro, E.; Fernández-Sotos, P.; González, P.; Ricarte, J.J.; Latorre, J.M.; Rodriguez-Jimenez, R. Human-Avatar Symbiosis for the Treatment of Auditory Verbal Hallucinations in Schizophrenia through Virtual/Augmented Reality and Brain-Computer Interfaces. Front. Aging Neurosci. 2017, 11, 64. [Google Scholar] [CrossRef]
- Russell, C.; Roche, A.D.; Chakrabarty, S. Peripheral nerve bionic interface: A review of electrodes. Int. J. Intell. Robot. Appl. 2019, 3, 11–18. [Google Scholar] [CrossRef]
- Yildiz, K.A.; Shin, A.Y.; Kaufman, K.R. Interfaces with the peripheral nervous system for the control of a neuroprosthetic limb: A review. J. Neuroeng. Rehabil. 2020, 17, 1–19. [Google Scholar] [CrossRef]
- Cheung, K.C. Implantable microscale neural interfaces. Biomed. Microdevices 2007, 9, 923–938. [Google Scholar] [CrossRef]
- Lazarou, I.; Nikolopoulos, S.; Petrantonakis, P.C.; Kompatsiaris, I.; Tsolaki, M. EEG-Based Brain–Computer Interfaces for Communication and Rehabilitation of People with Motor Impairment: A Novel Approach of the 21st Century. Front. Hum. Neurosci. 2018, 12, 14. [Google Scholar] [CrossRef]
- Segato, A.; Pieri, V.; Favaro, A.; Riva, M.; Falini, A.; De Momi, E.; Castellano, A. Automated Steerable Path Planning for Deep Brain Stimulation Safeguarding Fiber Tracts and Deep Gray Matter Nuclei. Front. Robot. AI 2019, 6, 70. [Google Scholar] [CrossRef] [PubMed]
- Hong, G.; Lieber, C.M. Novel electrode technologies for neural recordings. Nat. Rev. Neurosci. 2019, 20, 330–345. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, A.B. Movement: How the Brain Communicates with the World. Cell 2016, 164, 1122–1135. [Google Scholar] [CrossRef]
- Farina, D.; Negro, F. Accessing the Neural Drive to Muscle and Translation to Neurorehabilitation Technologies. IEEE Rev. Biomed. Eng. 2012, 5, 3–14. [Google Scholar] [CrossRef]
- De Luca, C.J.; Adam, A.; Wotiz, R.; Gilmore, L.D.; Nawab, S.H. Decomposition of Surface EMG Signals. J. Neurophysiol. 2006, 96, 1646–1657. [Google Scholar] [CrossRef] [PubMed]
- Merletti, R.; Parker, P.J. Electromyography: Physiology, Engineering, and Non-Invasive Applications; John Wiley & Sons: Hoboken, NJ, USA, 2004; Volume 11. [Google Scholar]
- Herrel, A.; Schaerlaeken, V.; Ross, C.; Meyers, J.; Nishikawa, K.; Abdala, V.; Manzano, A.; Aerts, P. Electromyography and the evolution of motor control: Limitations and insights. Integr. Comp. Biol. 2008, 48, 261–271. [Google Scholar] [CrossRef] [PubMed]
- MyoPro Elbow-Wrist-Hand Orthosis (EWHO). Available online: https://myomo.com/what-is-a-myopro-orthosis/ (accessed on 14 March 2021).
- SaeboGlove | Finger Extension Rehabilitation Glove for Stroke Survivors. Available online: https://www.saebo.com/saeboglove/ (accessed on 14 March 2021).
- Kim, G.J.; Rivera, L.; Stein, J. Combined Clinic-Home Approach for Upper Limb Robotic Therapy After Stroke: A Pilot Study. Arch. Phys. Med. Rehabil. 2015, 96, 2243–2248. [Google Scholar] [CrossRef] [PubMed]
- Merrill, D.R.; Lockhart, J.; Troyk, P.R.; Weir, R.F.; Hankin, D.L. Development of an Implantable Myoelectric Sensor for Advanced Prosthesis Control. Artif. Organs 2011, 35, 249–252. [Google Scholar] [CrossRef] [PubMed]
- Heo, P.; Gu, G.M.; Lee, S.-J.; Rhee, K.; Kim, J. Current hand exoskeleton technologies for rehabilitation and assistive engineering. Int. J. Precis. Eng. Manuf. 2012, 13, 807–824. [Google Scholar] [CrossRef]
- Dick, S.F.; Bert, K.U.; Bernd, L.G.; Johannes, V.D.P. High-density Surface EMG: Techniques and Applications at a Motor Unit Level. Biocybern. Biomed. Eng. 2012, 32(3), 3–27. [Google Scholar] [CrossRef]
- Negro, F.; Orizio, C. Robust estimation of average twitch contraction forces of populations of motor units in humans. J. Electromyogr. Kinesiol. 2017, 37, 132–140. [Google Scholar] [CrossRef][Green Version]
- Farina, D.; Jiang, N.; Rehbaum, H.; Holobar, A.; Graimann, B.; Dietl, H.; Aszmann, O.C. The Extraction of Neural Information from the Surface EMG for the Control of Upper-Limb Prostheses: Emerging Avenues and Challenges. IEEE Trans. Neural Syst. Rehabil. Eng. 2014, 22, 797–809. [Google Scholar] [CrossRef]
- Dupan, S.S.; Krasoulis, A.; Nazarpour, K. Intramuscular EMG For Abstract Myoelectric Control: A Proof Of Concept Study. In Proceedings of the 2020 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Montreal, Canada, 20–24 July 2020; pp. 3277–3280. [Google Scholar]
- Rodrigues, C.; Fernandeez, M.; Megia, A.; Comino, N.; Del-Ama, A.; Gil-Agudo, A.; Jung, M.K.; Muceli, S.; Farina, D.; Moreno, J.; et al. Comparison of Intramuscular and Surface Electromyography Recordings Towards the Control of Wearable Robots for Incomplete Spinal Cord Injury Rehabilitation. In Proceedings of the 2020 8th IEEE RAS/EMBS International Conference for Biomedical Robotics and Biomechatronics (BioRob), New York, NY, USA, 29 Novemeber–1 December 2020; pp. 564–569. [Google Scholar]
- Crouch, D.L.; Pan, L.; Filer, W.; Stallings, J.W.; Huang, H. Comparing Surface and Intramuscular Electromyography for Simultaneous and Proportional Control Based on a Musculoskeletal Model: A Pilot Study. IEEE Trans. Neural Syst. Rehabil. Eng. 2018, 26, 1735–1744. [Google Scholar] [CrossRef]
- Salminger, S.; Sturma, A.; Hofer, C.; Evangelista, M.; Perrin, M.; Bergmeister, K.D.; Roche, A.D.; Hasenoehrl, T.; Dietl, H.; Farina, D.; et al. Long-term implant of intramuscular sensors and nerve transfers for wireless control of robotic arms in above-elbow amputees. Sci. Robot. 2019, 4, eaaw6306. [Google Scholar] [CrossRef]
- Gopura, R.A.R.C.; Bandara, D.S.V.; Gunasekara, J.M.P. Recent Trends in EMG-Based Control Methods for Assistive Robots. In Electrodiagnosis in New Frontiers of Clinical Research; IntechOpen: London, UK, 2013. [Google Scholar]
- Farina, D.; Vujaklija, I.; Sartori, M.; Kapelner, T.; Negro, F.; Jiang, N.; Bergmeister, K.; Andalib, A.; Principe, J.; Aszmann, O.C. Man/machine interface based on the discharge timings of spinal motor neurons after targeted muscle reinnervation. Nat. Biomed. Eng. 2017, 1, 0025. [Google Scholar] [CrossRef]
- Cerone, G.L.; Botter, A.; Gazzoni, M. A Modular, Smart, and Wearable System for High Density sEMG Detection. IEEE Trans. Biomed. Eng. 2019, 66, 3371–3380. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, R.H.; Reaz, M.B.I.; Ali, M.A.B.M.; Bakar, A.A.A.; Chellappan, K.; Chang, T.G. Surface Electromyography Signal Processing and Classification Techniques. Sensors 2013, 13, 12431–12466. [Google Scholar] [CrossRef] [PubMed]
- Hahne, J.M.; Efarina, D.; Ejiang, N.; Eliebetanz, D. A Novel Percutaneous Electrode Implant for Improving Robustness in Advanced Myoelectric Control. Front. Neurosci. 2016, 10, 114. [Google Scholar] [CrossRef]
- Chadwell, A.; Kenney, L.; Thies, S.; Galpin, A.; Head, J. The Reality of Myoelectric Prostheses: Understanding What Makes These Devices Difficult for Some Users to Control. Front. Neurorobotics 2016, 10, 7. [Google Scholar] [CrossRef] [PubMed]
- Pasquina, P.F.; Evangelista, M.; Carvalho, A.; Lockhart, J.; Griffin, S.; Nanos, G.; McKay, P.; Hansen, M.; Ipsen, D.; Vandersea, J.; et al. First-in-man demonstration of a fully implanted myoelectric sensors system to control an advanced electromechanical prosthetic hand. J. Neurosci. Methods 2015, 244, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Farina, D.; Sartori, M. Surface Electromyography for MAN-Machine Interfacing in Rehabilitation Technologies. In Surface Electromyography: Physiology, Engineering, and Applications; Wiley: Hoboken, NJ, USA, 2016; pp. 540–560. [Google Scholar]
- Jiang, N.; Dosen, S.; Muller, K.-R.; Farina, D. Myoelectric Control of Artificial Limbs—Is There a Need to Change Focus? [In the Spotlight]. IEEE Signal Process. Mag. 2012, 29, 152-150. [Google Scholar] [CrossRef]
- Durandau, G.; Farina, D.; Sartori, M. Robust Real-Time Musculoskeletal Modeling Driven by Electromyograms. IEEE Trans. Biomed. Eng. 2017, 65, 556–564. [Google Scholar] [CrossRef] [PubMed]
- Shih, J.J.; Krusienski, D.J.; Wolpaw, J.R. Brain-Computer Interfaces in Medicine. Mayo Clin. Proc. 2012, 87, 268–279. [Google Scholar] [CrossRef] [PubMed]
- Lotte, F.; Bougrain, L.; Cichocki, A.; Clerc, M.; Congedo, M.; Rakotomamonjy, A.; Yger, F. A review of classification algorithms for EEG-based brain–computer interfaces: A 10 year update. J. Neural Eng. 2018, 15, 031005. [Google Scholar] [CrossRef]
- Nicolas-Alonso, L.F.; Gomez-Gil, J. Brain Computer Interfaces, a Review. Sensors 2012, 12, 1211–1279. [Google Scholar] [CrossRef]
- Wang, W.; Collinger, J.L.; Perez, M.A.; Tyler-Kabara, E.C.; Cohen, L.G.; Birbaumer, N.; Brose, S.W.; Schwartz, A.B.; Boninger, M.L.; Weber, D.J. Neural Interface Technology for Rehabilitation: Exploiting and Promoting Neuroplasticity. Phys. Med. Rehabil. Clin. North Am. 2010, 21, 157–178. [Google Scholar] [CrossRef] [PubMed]
- Rupp, R. Challenges in clinical applications of brain computer interfaces in individuals with spinal cord injury. Front. Neuroeng. 2014, 7, 38. [Google Scholar] [CrossRef] [PubMed]
- Athanasiou, A.; Xygonakis, I.; Pandria, N.; Kartsidis, P.; Arfaras, G.; Kavazidi, K.R.; Foroglou, N.; Astaras, A.; Bamidis, P.D. Towards Rehabilitation Robotics: Off-the-Shelf BCI Control of Anthropomorphic Robotic Arms. BioMed Res. Int. 2017, 2017, 1–17. [Google Scholar] [CrossRef]
- Mak, J.N.; Wolpaw, J.R. Clinical Applications of Brain-Computer Interfaces: Current State and Future Prospects. IEEE Rev. Biomed. Eng. 2009, 2, 187–199. [Google Scholar] [CrossRef]
- Al-Quraishi, M.S.; Elamvazuthi, I.; Daud, S.A.; Parasuraman, S.; Borboni, A. EEG-Based Control for Upper and Lower Limb Exoskeletons and Prostheses: A Systematic Review. Sensors 2018, 18, 3342. [Google Scholar] [CrossRef] [PubMed]
- Mattia, D.; Pichiorri, F.; Molinari, M.; Rupp, R. Brain Computer Interface for Hand Motor Function Restoration and Rehabilitation. In Towards Practical Brain-Computer Interfaces; Allison, B.Z., Dunne, S., Leeb, R., Del R. Millán, J., Nijholt, A., Eds.; Springer: Berlin/Heidelberg, Germany, 2012; pp. 131–153. [Google Scholar]
- Mane, R.; Chew, E.; Phua, K.S.; Ang, K.K.; Robinson, N.; Vinod, A.P.; Guan, C. Prognostic and Monitory EEG-Biomarkers for BCI Upper-Limb Stroke Rehabilitation. IEEE Trans. Neural Syst. Rehabil. Eng. 2019, 27, 1654–1664. [Google Scholar] [CrossRef]
- Dobkin, B.H. Confounders in Rehabilitation Trials of Task-Oriented Training: Lessons From the Designs of the EXCITE and SCILT Multicenter Trials. Neurorehabilit. Neural Repair 2007, 21, 3–13. [Google Scholar] [CrossRef]
- Daly, J.J.; Cheng, R.; Hrovat, K.; Rogers, J.M.; Litinas, K.; Dohring, M.E. Development and Testing of Non-Invasive BCI + FES/Robot System For Use in Motor Re-Learning After Stroke. In Proceedings of the 13th Annual Conference of the International Functional Electrical Stimulation Society “From Movement to Mind”, Freiburg, Germany, 21–25 September 2008; pp. 200–202. [Google Scholar]
- Soekadar, S.R.; Birbaumer, N.; Slutzky, M.W.; Cohen, L.G. Brain–machine interfaces in neurorehabilitation of stroke. Neurobiol. Dis. 2015, 83, 172–179. [Google Scholar] [CrossRef] [PubMed]
- Vourvopoulos, A.; Pardo, O.M.; Lefebvre, S.; Neureither, M.; Saldana, D.; Jahng, E.; Liew, S.-L. Effects of a Brain-Computer Interface with Virtual Reality (VR) Neurofeedback: A Pilot Study in Chronic Stroke Patients. Front. Hum. Neurosci. 2019, 13, 210. [Google Scholar] [CrossRef]
- Remsik, A.; Young, B.; Vermilyea, R.; Kiekhoefer, L.; Abrams, J.; Elmore, S.E.; Schultz, P.; Nair, V.; Edwards, D.; Williams, J.; et al. A review of the progression and future implications of brain-computer interface therapies for restoration of distal upper extremity motor function after stroke. Expert Rev. Med. Devices 2016, 13, 445–454. [Google Scholar] [CrossRef]
- Rouillard, J.; Duprès, A.; Cabestaing, F.; Leclercq, S.; Bekaert, M.-H.; Piau, C.; Vannobel, J.-M.; Lecocq, C. Hybrid BCI Coupling EEG and EMG for Severe Motor Disabilities. Procedia Manuf. 2015, 3, 29–36. [Google Scholar] [CrossRef]
- Krusienski, D.J.; Grosse-Wentrup, M.; Galán, F.; Coyle, D.; Miller, K.J.; Forney, E.; Anderson, C.W. Critical issues in state-of-the-art brain–computer interface signal processing. J. Neural Eng. 2011, 8, 025002. [Google Scholar] [CrossRef]
- Sengupta, S.; Basak, S.; Saikia, P.; Paul, S.; Tsalavoutis, V.; Atiah, F.; Ravi, V.; Peters, A. A review of deep learning with special emphasis on architectures, applications and recent trends. Knowl. Based Syst. 2020, 194, 105596. [Google Scholar] [CrossRef]
- Sünderhauf, N.; Brock, O.; Scheirer, W.; Hadsell, R.; Fox, D.; Leitner, J.; Upcroft, B.; Abbeel, P.; Burgard, W.; Milford, M.; et al. The limits and potentials of deep learning for robotics. Int. J. Robot. Res. 2018, 37, 405–420. [Google Scholar] [CrossRef]
- Shen, Y.; Ferguson, P.W.; Rosen, J. Chapter 1 - Upper Limb Exoskeleton Systems—Overview. In Wearable Robotics; Rosen, J., Ferguson, P.W., Eds.; Academic Press: Cambridge, MA, USA, 2020; pp. 1–22. [Google Scholar]
- Mehrholz, J.; Thomas, S.; Kugler, J.; Pohl, M.; Elsner, B. Electromechanical-assisted training for walking after stroke. Cochrane Database Syst. Rev. 2020, 10, CD006185. [Google Scholar] [CrossRef] [PubMed]
- Ferris, D.P. The exoskeletons are here. J. Neuroeng. Rehabil. 2009, 6, 17. [Google Scholar] [CrossRef]
- Lee, H.; Ferguson, P.W.; Rosen, J. Chapter 11 - Lower Limb Exoskeleton Systems—Overview. In Wearable Robotics; Rosen, J., Ferguson, P.W., Eds.; Academic Press: Cambridge, MA, USA, 2020; pp. 207–229. [Google Scholar]
- Farris, R.J.; Quintero, H.A.; Goldfarb, M. Performance evaluation of a lower limb exoskeleton for stair ascent and descent with Paraplegia. In Proceedings of the 2012 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Diego, CA, USA, 28 August–1 September 2012; pp. 1908–1911. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.S.; Wang, L.L.; Meijneke, C.C.; Van Asseldonk, E.E.; Hoellinger, T.; Cheron, G.; Ivanenko, Y.Y.; La Scaleia, V.V.; Sylos-Labini, F.; Molinari, M.M.; et al. Design and Control of the MINDWALKER Exoskeleton. IEEE Trans. Neural Syst. Rehabil. Eng. 2015, 23, 277–286. [Google Scholar] [CrossRef] [PubMed]
- Hogan, N.; Krebs, H.; Charnnarong, J.; Srikrishna, P.; Sharon, A. MIT-MANUS: A workstation for manual therapy and training. I. In Proceedings of the IEEE International Workshop on Robot and Human Communication, Tokyo, Japan, 1–3 September 1992; pp. 161–165. [Google Scholar]
- Maciejasz, P.; Eschweiler, J.; Gerlach-Hahn, K.; Jansen-Troy, A.; Leonhardt, S. A survey on robotic devices for upper limb rehabilitation. J. Neuroeng. Rehabil. 2014, 11, 3. [Google Scholar] [CrossRef] [PubMed]
- Perry, B.E.; Evans, E.K.; Stokic, D.S. Weight compensation characteristics of Armeo®Spring exoskeleton: Implications for clinical practice and research. J. Neuroeng. Rehabil. 2017, 14, 14. [Google Scholar] [CrossRef]
- Frisoli, A.; Bergamasco, M.; Carboncini, M.C.; Rossi, B. Robotic assisted rehabilitation in Virtual Reality with the L-EXOS. Stud. Heal. Technol. Inform. 2009, 145, 40–54. [Google Scholar]
- Kumar, S.; Wöhrle, H.; Trampler, M.; Simnofske, M.; Peters, H.; Mallwitz, M.; Kirchner, E.A.; Kirchner, F. Modular Design and Decentralized Control of the Recupera Exoskeleton for Stroke Rehabilitation. Appl. Sci. 2019, 9, 626. [Google Scholar] [CrossRef]
- Xiloyannis, M.; Chiaradia, D.; Frisoli, A.; Masia, L. Physiological and kinematic effects of a soft exosuit on arm movements. J. Neuroeng. Rehabil. 2019, 16, 29. [Google Scholar] [CrossRef]
- Riener, R.; Lünenburger, L.; Jezernik, S.; Anderschitz, M.; Colombo, G.; Dietz, V. Patient-Cooperative Strategies for Robot-Aided Treadmill Training: First Experimental Results. IEEE Trans. Neural Syst. Rehabil. Eng. 2005, 13, 380–394. [Google Scholar] [CrossRef]
- Dimitrousis, C.; Almpani, S.; Stefaneas, P.; Veneman, J.; Nizamis, K.; Astaras, A. Neurorobotics: Review of underlying technologies, current developments, and future directions. Neurotechnology Methods Adv. Appl. 2020, 14, 181–213. [Google Scholar] [CrossRef]
- Wright, J.; Macefield, V.G.; Van Schaik, A.; Tapson, J.C. A Review of Control Strategies in Closed-Loop Neuroprosthetic Systems. Front. Neurosci. 2016, 10, 312. [Google Scholar] [CrossRef] [PubMed]
- Carmena, J.M. Advances in Neuroprosthetic Learning and Control. PLoS Biol. 2013, 11, e1001561. [Google Scholar] [CrossRef] [PubMed]
- Bumbaširević, M.; Lesic, A.; Palibrk, T.; Milovanovic, D.; Zoka, M.; Kravić-Stevović, T.; Raspopovic, S. The current state of bionic limbs from the surgeon’s viewpoint. EFORT Open Rev. 2020, 5, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Morris, S.; Hirata, M.; Sugata, H.; Goto, T.; Matsushita, K.; Yanagisawa, T.; Saitoh, Y.; Kishima, H.; Yoshimine, T. Patient-Specific Cortical Electrodes for Sulcal and Gyral Implantation. IEEE Trans. Biomed. Eng. 2014, 62, 1034–1041. [Google Scholar] [CrossRef]
- Serino, A.; Akselrod, M.; Salomon, R.; Martuzzi, R.; Blefari, M.L.; Canzoneri, E.; Rognini, G.; Van Der Zwaag, W.; Iakova, M.; Luthi, F.; et al. Upper limb cortical maps in amputees with targeted muscle and sensory reinnervation. Brain 2017, 140, 2993–3011. [Google Scholar] [CrossRef] [PubMed]
- Kuiken, T.A.; Barlow, A.K.; Hargrove, L.J.; Dumanian, G.A. Targeted Muscle Reinnervation for the Upper and Lower Extremity. Tech. Orthop. 2017, 32, 109–116. [Google Scholar] [CrossRef]
- Hargrove, L.J.; Simon, A.M.; Young, A.J.; Lipschutz, R.D.; Finucane, S.B.; Smith, D.G.; Kuiken, T.A. Robotic Leg Control with EMG Decoding in an Amputee with Nerve Transfers. N. Engl. J. Med. 2013, 369, 1237–1242. [Google Scholar] [CrossRef]
- Jönsson, S.; Caine-Winterberger, K.; Brånemark, R. Osseointegration amputation prostheses on the upper limbs: Methods, prosthetics and rehabilitation. Prosthet. Orthot. Int. 2011, 35(2), 190–200. [Google Scholar] [CrossRef] [PubMed]
- Malešević, N.M.; Maneski, L.Z.P.; Ilić, V.; Jorgovanović, N.; Bijelić, G.; Keller, T.; Popović, D.B. A multi-pad electrode based functional electrical stimulation system for restoration of grasp. J. Neuroeng. Rehabil. 2012, 9, 66. [Google Scholar] [CrossRef]
- Popovic-Maneski, L.P.; Kostic, M.D.; Bijelic, G.; Keller, T.; Mitrovic, S.; Konstantinovic, L.; Popovic, D.B. Multi-Pad Electrode for Effective Grasping: Design. IEEE Trans. Neural Syst. Rehabil. Eng. 2013, 21, 648–654. [Google Scholar] [CrossRef] [PubMed]
- Hara, Y. Neurorehabilitation with New Functional Electrical Stimulation for Hemiparetic Upper Extremity in Stroke Patients. J. Nippon. Med. Sch. 2008, 75, 4–14. [Google Scholar] [CrossRef] [PubMed]
- Müller, P.; Del Ama, A.J.; Moreno, J.C.; Schauer, T. Adaptive multichannel FES neuroprosthesis with learning control and automatic gait assessment. J. Neuroeng. Rehabil. 2020, 17, 36. [Google Scholar] [CrossRef] [PubMed]
- Franck, J.A.; Smeets, R.J.E.M.; Seelen, H.A.M. Evaluation of a functional hand orthosis combined with electrical stimulation adjunct to arm-hand rehabilitation in subacute stroke patients with a severely to moderately affected hand function. Disabil. Rehabil. 2018, 41, 1160–1168. [Google Scholar] [CrossRef]
- Peters, T.E.; Bhavaraju, N.C.; Frei, M.G.; Osorio, I. Network System for Automated Seizure Detection and Contingent Delivery of Therapy. J. Clin. Neurophysiol. 2001, 18, 545–549. [Google Scholar] [CrossRef]
- Wilder, A.; Hiatt, S.; Dowden, B.; Brown, N.; Normann, R.; Clark, G. Automated Stimulus-Response Mapping of High-Electrode-Count Neural Implants. IEEE Trans. Neural Syst. Rehabil. Eng. 2009, 17, 504–511. [Google Scholar] [CrossRef]
- Markovic, M.; Dosen, S.; Cipriani, C.; Popovic, D.; Farina, D. Stereovision and augmented reality for closed-loop control of grasping in hand prostheses. J. Neural Eng. 2014, 11, 046001. [Google Scholar] [CrossRef] [PubMed]
- Shpigelman, L.; Lalazar, H.; Vaadia, E. Kernel-ARMA for Hand Tracking and Brain-Machine interfacing During 3D Motor Control. In Advances in Neural Information Processing Systems 21; Koller, D., Schuurmans, D., Bengio, Y., Bottou, L., Eds.; Curran Associates, Inc.: Red Hook, NY, USA, 2009; pp. 1489–1496. [Google Scholar]
- Li, Z.; O’Doherty, J.E.; Hanson, T.L.; Lebedev, M.A.; Henriquez, C.S.; Nicolelis, M.A.L. Unscented Kalman Filter for Brain-Machine Interfaces. PLoS ONE 2009, 4, e6243. [Google Scholar] [CrossRef]
- DiGiovanna, J.; Mahmoudi, B.; Fortes, J.; Principe, J.C.; Sanchez, J.C. Coadaptive Brain–Machine Interface via Reinforcement Learning. IEEE Trans. Biomed. Eng. 2009, 56(1), 54–64. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, V.; Singhal, G.; He, J.; Schieber, M.H.; Thakor, N.V. Towards closed-loop decoding of dexterous hand movements using a virtual integration environment. In Proceedings of the 2008 30th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Vancouver, Canada, 20–24 August 2008; pp. 1703–1706. [Google Scholar]
- Ehrsson, H.H.; Rosén, B.; Stockselius, A.; Ragnö, C.; Köhler, P.; Lundborg, G. Upper limb amputees can be induced to experience a rubber hand as their own. Brain 2008, 131, 3443–3452. [Google Scholar] [CrossRef]
- Manero, A.; Smith, P.; Sparkman, J.; Dombrowski, M.; Courbin, D.; Kester, A.; Womack, I.; Chi, A. Implementation of 3D Printing Technology in the Field of Prosthetics: Past, Present, and Future. Int. J. Environ. Res. Public Health 2019, 16, 1641. [Google Scholar] [CrossRef] [PubMed]
- Kate, J.T.; Smit, G.; Breedveld, P. 3D-printed upper limb prostheses: A review. Disabil. Rehabil. Assist. Technol. 2017, 12, 300–314. [Google Scholar] [CrossRef] [PubMed]
- Windrich, M.; Grimmer, M.; Christ, O.; Rinderknecht, S.; Beckerle, P. Active lower limb prosthetics: A systematic review of design issues and solutions. Biomed. Eng. Online 2016, 15, 5–19. [Google Scholar] [CrossRef]
- Azocar, A.F.; Mooney, L.M.; Duval, J.-F.; Simon, A.M.; Hargrove, L.J.; Rouse, E.J. Design and clinical implementation of an open-source bionic leg. Nat. Biomed. Eng. 2020, 4, 941–953. [Google Scholar] [CrossRef]
- VijayaVenkataRaman, S.; Fuh, J.Y.H.; Lu, W.F. 3D Printing and 3D Bioprinting in Pediatrics. Bioengeniring 2017, 4, 63. [Google Scholar] [CrossRef]
- Burdea, G.C.; Coiffet, P. Virtual Reality Technology. Presence: Teleoperators Virtual Environ. 2003, 12, 663–664. [Google Scholar] [CrossRef]
- Azuma, R.; Baillot, Y.; Behringer, R.; Feiner, S.; Julier, S.; MacIntyre, B. Recent advances in augmented reality. IEEE Eng. Med. Boil Mag. 2001, 21, 34–47. [Google Scholar] [CrossRef]
- Holden, M.K. Virtual Environments for Motor Rehabilitation: Review. CyberPsychology Behav. 2005, 8, 187–211. [Google Scholar] [CrossRef] [PubMed]
- Keshner, E.A. Virtual reality and physical rehabilitation: A new toy or a new research and rehabilitation tool? J. Neuroeng. Rehabil. 2004, 1, 8. [Google Scholar] [CrossRef]
- Bohil, C.J.; Alicea, B.; Biocca, F.A. Virtual reality in neuroscience research and therapy. Nat. Rev. Neurosci. 2011, 12, 752–762. [Google Scholar] [CrossRef] [PubMed]
- Howard, M.C. A meta-analysis and systematic literature review of virtual reality rehabilitation programs. Comput. Hum. Behav. 2017, 70, 317–327. [Google Scholar] [CrossRef]
- Sucar, L.E.; Orihuela-Espina, F.; Velazquez, R.L.; Reinkensmeyer, D.J.; Leder, R.; Hernandez-Franco, J. Gesture Therapy: An Upper Limb Virtual Reality-Based Motor Rehabilitation Platform. IEEE Trans. Neural Syst. Rehabil. Eng. 2014, 22, 634–643. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.; Wolf, S.L.; He, J. Recent developments in biofeedback for neuromotor rehabilitation. J. Neuroeng. Rehabil. 2006, 3, 11. [Google Scholar] [CrossRef] [PubMed]
- Verma, R.; Arya, K.N.; Garg, R.; Singh, T. Task-Oriented Circuit Class Training Program with Motor Imagery for Gait Rehabilitation in Poststroke Patients: A Randomized Controlled Trial. Top. Stroke Rehabil. 2011, 18, 620–632. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Huang, H.; Xu, W.; Wallis, R.I.; Sundaram, H.; Rikakis, T.; Ingalls, T.; Olson, L.; He, J. The design of a real-time, multimodal biofeedback system for stroke patient rehabilitation. In Proceedings of the 14th ACM International Conference on Multimedia, Santa Barbara, CA, USA, 23–27 October 2006; p. 763. [Google Scholar]
- Michalski, S.C.; Szpak, A.; Saredakis, D.; Ross, T.J.; Billinghurst, M.; Loetscher, T. Getting your game on: Using virtual reality to improve real table tennis skills. PLoS ONE 2019, 14, e0222351. [Google Scholar] [CrossRef]
- De Araújo, A.V.L.; Neiva, J.F.D.O.; Monteiro, C.B.D.M.; Magalhães, F.H. Efficacy of Virtual Reality Rehabilitation after Spinal Cord Injury: A Systematic Review. BioMed Res. Int. 2019, 2019, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Tageldeen, M.K.; Elamvazuthi, I.; Perumal, N.; Ganesan, T. A virtual reality based serious games for rehabilitation of arm. In Proceedings of the 2017 IEEE 3rd International Symposium in Robotics and Manufacturing Automation (ROMA), Kuala Lumpur, Malaysia, 19–21 September 2017; pp. 1–6. [Google Scholar]
- Comani, S.; Velluto, L.; Schinaia, L.; Cerroni, G.; Serio, A.; Buzzelli, S.; Sorbi, S.; Guarnieri, B. Monitoring Neuro-Motor Recovery from Stroke with High-Resolution EEG, Robotics and Virtual Reality: A Proof of Concept. IEEE Trans. Neural Syst. Rehabil. Eng. 2015, 23, 1106–1116. [Google Scholar] [CrossRef] [PubMed]
- Eng, K.; Siekierka, E.; Pyk, P.; Chevrier, E.; Hauser, Y.; Cameirao, M.; Holper, L.; Hägni, K.; Zimmerli, L.; Duff, A.; et al. Interactive visuo-motor therapy system for stroke rehabilitation. Med. Biol. Eng. Comput. 2007, 45, 901–907. [Google Scholar] [CrossRef]
- Anderson, F.; Grossman, T.; Matejka, J.; Fitzmaurice, G. YouMove. In Proceedings of the 26th Annual ACM Symposium on User interface Software and Technology, St. Andrews, UK, 8–11 October 2013; pp. 311–320. [Google Scholar]
- Hondori, H.M.; Khademi, M.; Dodakian, L.; McKenzie, A.; Lopes, C.V.; Cramer, S.C. Choice of Human–Computer Interaction Mode in Stroke Rehabilitation. Neurorehabilit. Neural Repair 2016, 30, 258–265. [Google Scholar] [CrossRef] [PubMed]
- Garrett, B.; Taverner, T.; Gromala, D.; Tao, G.; Cordingley, E.; Sun, C. Virtual Reality Clinical Research: Promises and Challenges. JMIR Serious Games 2018, 6, e10839. [Google Scholar] [CrossRef] [PubMed]
- Slater, M.; Wilbur, S. A framework for immersive virtual environments (FIVE): Speculations on the role of presence in virtual environments. Presence 1997, 6, 603. [Google Scholar] [CrossRef]
- Slater, M.; Lotto, B.; Arnold, M.M.; Sanchez-Vives, M.V. How we experience immersive virtual environments: The concept of presence and its measurement. Anu. Psicol. 2009, 40, 18. [Google Scholar]
- Steuer, J. Defining Virtual Reality: Dimensions Determining Telepresence. J. Commun. 1992, 42, 73–93. [Google Scholar] [CrossRef]
- Weech, S.; Kenny, S.; Barnett-Cowan, M. Presence and Cybersickness in Virtual Reality Are Negatively Related: A Review. Front. Psychol. 2019, 10, 158. [Google Scholar] [CrossRef] [PubMed]
- Raaen, K.; Kjellmo, I. Measuring Latency in Virtual Reality Systems. In Proceedings of the Entertainment Computing - ICEC 2015, Trondheim, Norway, 29 September–2 October 2015; Chorianopoulos, K., Divitini, M., Baalsrud Hauge, J., Jaccheri, L., Malaka, R., Eds.; Springer International Publishing: Cham, Switzerland, 2015; Volume 9353, pp. 457–462. [Google Scholar]
- Oña, E.D.; Garcia-Haro, J.M.; Jardón, A.; Balaguer, C. Robotics in Health Care: Perspectives of Robot-Aided Interventions in Clinical Practice for Rehabilitation of Upper Limbs. Appl. Sci. 2019, 9, 2586. [Google Scholar] [CrossRef]
- Sim, D.Y.Y.; Loo, C.K. Extensive assessment and evaluation methodologies on assistive social robots for modelling human–robot interaction – A review. Inf. Sci. 2015, 301, 305–344. [Google Scholar] [CrossRef]
- WHO|Neurological Disorders: Public Health Challenges,” WHO. Available online: https://www.who.int/mental_health/neurology/neurodiso/en/ (accessed on 21 March 2020).
- Karikari, T.K.; Charway-Felli, A.; Höglund, K.; Blennow, K.; Zetterberg, H. Commentary: Global, regional, and national burden of neurological disorders during 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Front. Neurol. 2018, 9. [Google Scholar] [CrossRef] [PubMed]
- Cassimatis, N.L.; Trafton, J.G.; Bugajska, M.D.; Schultz, A.C. Integrating cognition, perception and action through mental simulation in robots. Robot. Auton. Syst. 2004, 49, 13–23. [Google Scholar] [CrossRef]
- Laird, J.E.; Lebiere, C.; Rosenbloom, P.S. A Standard Model of the Mind: Toward a Common Computational Framework across Artificial Intelligence, Cognitive Science, Neuroscience, and Robotics. AI Mag. 2017, 38, 13–26. [Google Scholar] [CrossRef]
- Zhao, Z.-Q.; Zheng, P.; Xu, S.-T.; Wu, X. Object Detection with Deep Learning: A Review. IEEE Trans. Neural Netw. Learn. Syst. 2019, 30, 3212–3232. [Google Scholar] [CrossRef]
- Aoki, Y.; Goforth, H.; Srivatsan, R.A.; Lucey, S. PointNetLK: Robust & Efficient Point Cloud Registration Using PointNet. In Proceedings of the 2019 IEEE/CVF Conference on Computer Vision and Pattern Recognition (CVPR), Long Beach, CA, USA, 16–20 June 2019; pp. 7156–7165. [Google Scholar]
- Redmon, J.; Divvala, S.; Girshick, R.; Farhadi, A. You Only Look Once: Unified, Real-Time Object Detection. In Proceedings of the 2016 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 27–30 June 2016; pp. 779–788. [Google Scholar] [CrossRef]
- Kramer, E.R.; Sáinz, A.O.; Mitrevski, A.; Plöger, P.G. Tell Your Robot What to Do: Evaluation of Natural Language Models for Robot Command Processing. In Robot World Cup; Chalup, S., Niemueller, T., Suthakorn, J., Williams, M.-A., Eds.; Springer International Publishing: Cham, Switzerland, 2019; Volume 11531, pp. 255–267. [Google Scholar]
- Mnih, V. Playing Atari with Deep Reinforcement Learning. ArXiv 2013, arXiv:1312.5602. Available online: http://arxiv.org/abs/1312.5602 (accessed on 21 March 2020).
- Lillicrap, T.P. Continuous control with deep reinforcement learning. ArXiv 2019, arXiv:1509.00297. Available online: http://arxiv.org/abs/1509.02971 (accessed on 21 April 2020).
- Schuld, M.; Sinayskiy, I.; Petruccione, F. An introduction to quantum machine learning. Contemp. Phys. 2014, 56, 172–185. [Google Scholar] [CrossRef]
- Biamonte, J.; Wittek, P.; Pancotti, N.; Rebentrost, P.; Wiebe, N.; Lloyd, S. Quantum machine learning. Nat. Cell Biol. 2017, 549, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Haufe, F.L.; Wolf, P.; Riener, R. Human-in-the-loop optimization of a multi-joint wearable robot for movement assistance. Proc. Autom. Med Eng. 2020, 1, 23. [Google Scholar]
- EMERGING FRONTIERS IN RESEARCH AND INNOVATION (EFRI): Distributed Chemical Manufacturing (DCheM) and Engineering the Elimination of End-of-Life Plastics (E3P) | NSF National Science Foundation. Available online: https://www.nsf.gov/funding/pgm_summ.jsp?pims_id=13708 (accessed on 21 March 2020).
- Quiroga, R.Q.; Nadasdy, Z.; Ben-Shaul, Y. Unsupervised Spike Detection and Sorting with Wavelets and Superparamagnetic Clustering. Neural Comput. 2004, 16, 1661–1687. [Google Scholar] [CrossRef]
- Bonnet, S.; Bêche, J.-F.; Gharbi, S.; Abdoun, O.; Bocquelet, F.; Joucla, S.; Agache, V.; Sauter, F.; Pham, P.; Dupont, F.; et al. NeuroPXI: A real-time multi-electrode array system for recording, processing and stimulation of neural networks and the control of high-resolution neural implants for rehabilitation. IRBM 2012, 33, 55–60. [Google Scholar] [CrossRef]
- Wu, T.; Yang, Z. Power-efficient VLSI implementation of a feature extraction engine for spike sorting in neural recording and signal processing. In Proceedings of the 2014 13th International Conference on Control Automation Robotics & Vision (ICARCV), Singapore, 10–12 December 2014; pp. 7–12. [Google Scholar]
- Chen, Z. A Primer on Neural Signal Processing. IEEE Circuits Syst. Mag. 2017, 17, 33–50. [Google Scholar] [CrossRef]
- El-Samie, F.E.A.; Alotaiby, T.N.; Khalid, M.I.; Alshebeili, S.A.; Aldosari, S.A. A Review of EEG and MEG Epileptic Spike Detection Algorithms. IEEE Access 2018, 6, 60673–60688. [Google Scholar] [CrossRef]
- Johansen, A.R.; Jin, J.; Maszczyk, T.; Dauwels, J.; Cash, S.S.; Westover, M.B. Epileptiform spike detection via convolutional neural networks. In Proceedings of the 2016 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), Shanghai, China, 20–25 March 2016; pp. 754–758. [Google Scholar]
- Lewicki, M.S. A review of methods for spike sorting: The detection and classification of neural action potentials. Netw. Comput. Neural Syst. 1998, 9, R53–R78. [Google Scholar] [CrossRef]
- Kilicarslan, A.; Prasad, S.; Grossman, R.G.; Contreras-Vidal, J.L. High accuracy decoding of user intentions using EEG to control a lower-body exoskeleton. In Proceedings of the 2013 35th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Osaka, Japan, 3–7 July 2013; pp. 5606–5609. [Google Scholar] [CrossRef]
- Kwon, K.Y.; Eldawlatly, S.; Oweiss, K. NeuroQuest: A comprehensive analysis tool for extracellular neural ensemble recordings. J. Neurosci. Methods 2012, 204, 189–201. [Google Scholar] [CrossRef]
- Burns, M.K.; Pei, D.; Vinjamuri, R. Myoelectric Control of a Soft Hand Exoskeleton Using Kinematic Synergies. IEEE Trans. Biomed. Circuits Syst. 2019, 13, 1351–1361. [Google Scholar] [CrossRef]
- Tam, W.-K.; Yang, Z. Neural Parallel Engine: A toolbox for massively parallel neural signal processing. J. Neurosci. Methods 2018, 301, 18–33. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.; Wang, L.; Ouyang, G.; Li, X. Massively Parallel Neural Signal Processing on a Many-Core Platform. Comput. Sci. Eng. 2011, 13, 42–51. [Google Scholar] [CrossRef]
- Basic Neuroscience|National Institute of Neurological Disorders and Stroke. Available online: https://www.ninds.nih.gov/Current-Research/Research-Funded-NINDS/Basic-Neuroscience (accessed on 19 October 2020).
- Turner, D.L.; Emurguialday, A.R.; Ebirbaumer, N.; Ehoffmann, U.; Eluft, A. Neurophysiology of Robot-Mediated Training and Therapy: A Perspective for Future Use in Clinical Populations. Front. Neurol. 2013, 4, 184. [Google Scholar] [CrossRef] [PubMed]
- Severini, G.; Koenig, A.; Adans-Dester, C.; Cajigas, I.; Cheung, V.C.K.; Bonato, P. Robot-Driven Locomotor Perturbations Reveal Synergy-Mediated, Context-Dependent Feedforward and Feedback Mechanisms of Adaptation. Sci. Rep. 2020, 10, 1–16. [Google Scholar] [CrossRef]
- Cajigas, I.; Koenig, A.; Severini, G.; Smith, M.; Bonato, P. Robot-induced perturbations of human walking reveal a selective generation of motor adaptation. Sci. Robot. 2017, 2, eaam7749. [Google Scholar] [CrossRef]
- Ebolognini, N.; Erusso, C.; Evallar, G. Crossmodal illusions in neurorehabilitation. Front. Behav. Neurosci. 2015, 9, 212. [Google Scholar] [CrossRef]
- Cumming, D.R.S.; Furber, S.B.; Paul, D.J. Beyond Moore’s law. Philos. Trans. R. Soc. A Math. Phys. Eng. Sci. 2014, 372, 20130376. [Google Scholar] [CrossRef]
- Chen, Z.; Li, Z.; Li, J.; Liu, C.; Lao, C.; Fu, Y.; Liu, C.; Li, Y.; Wang, P.; He, Y. 3D printing of ceramics: A review. J. Eur. Ceram. Soc. 2019, 39, 661–687. [Google Scholar] [CrossRef]
- Frazier, W.E. Metal Additive Manufacturing: A Review. J. Mater. Eng. Perform. 2014, 23, 1917–1928. [Google Scholar] [CrossRef]
- Munaz, A.; Vadivelu, R.K.; John, J.S.; Barton, M.; Kamble, H.; Nguyen, N.-T. Three-dimensional printing of biological matters. J. Sci. Adv. Mater. Devices 2016, 1, 1–17. [Google Scholar] [CrossRef]
- Gao, B.; Yang, Q.; Zhao, X.; Jin, G.; Ma, Y.; Xu, F. 4D Bioprinting for Biomedical Applications. Trends Biotechnol. 2016, 34, 746–756. [Google Scholar] [CrossRef] [PubMed]
- Kaur, K.; Noor, A. Strategies & Methodologies for Low Power VLSI Designs: A Review. Int. J. Adv. Eng. Technol. 2011, 1, 159–165. [Google Scholar]
- Gul, J.Z.; Sajid, M.; Rehman, M.M.; Siddiqui, G.U.; Shah, I.; Kim, K.-H.; Lee, J.-W.; Choi, K.H. 3D printing for soft robotics—A review. Sci. Technol. Adv. Mater. 2018, 19, 243–262. [Google Scholar] [CrossRef] [PubMed]
- Sojan, S.; Kulkarni, R. A Comprehensive Review of Energy Harvesting Techniques and its Potential Applications. Int. J. Comput. Appl. 2016, 139, 14–19. [Google Scholar] [CrossRef]
- Seo, D.; Carmena, J.M.; Rabaey, J.M.; Alon, E.; Maharbiz, M.M. Neural Dust: An Ultrasonic, Low Power Solution for Chronic Brain-Machine Interfaces. ArXiv 2013, arXiv:1307.2196. Available online: http://arxiv.org/abs/1307.2196 (accessed on 28 April 2020).
- Warneke, B.; Last, M.; Liebowitz, B.; Pister, K. Smart Dust: Communicating with a cubic-millimeter computer. Computers 2001, 34, 44–51. [Google Scholar] [CrossRef]
- Zrenner, C.; Ebelardinelli, P.; Emüller-Dahlhaus, F.; Eziemann, U. Closed-Loop Neuroscience and Non-Invasive Brain Stimulation: A Tale of Two Loops. Front. Cell. Neurosci. 2016, 10, 92. [Google Scholar] [CrossRef]
- Broccard, F.D.; Mullen, T.; Chi, Y.M.; Peterson, D.; Iversen, J.R.; Arnold, M.; Kreutz-Delgado, K.; Jung, T.-P.; Makeig, S.; Poizner, H.; et al. Closed-Loop Brain–Machine–Body Interfaces for Noninvasive Rehabilitation of Movement Disorders. Ann. Biomed. Eng. 2014, 42, 1573–1593. [Google Scholar] [CrossRef] [PubMed]
- Stroppa, F.; Loconsole, C.; Frisoli, A. Convex polygon fitting in robot-based neurorehabilitation. Appl. Soft Comput. 2018, 68, 609–625. [Google Scholar] [CrossRef]
- Wutzl, B.; Leibnitz, K.; Rattay, F.; Kronbichler, M.; Murata, M.; Golaszewski, S.M. Genetic algorithms for feature selection when classifying severe chronic disorders of consciousness. PLoS ONE 2019, 14, e0219683. [Google Scholar] [CrossRef] [PubMed]
- Neely, R.M.; Piech, D.K.; Santacruz, S.R.; Maharbiz, M.M.; Carmena, J.M. Recent advances in neural dust: Towards a neural interface platform. Curr. Opin. Neurobiol. 2018, 50, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Seo, D.; Neely, R.M.; Shen, K.; Singhal, U.; Alon, E.; Rabaey, J.M.; Carmena, J.M.; Maharbiz, M.M. Wireless Recording in the Peripheral Nervous System with Ultrasonic Neural Dust. Neuron 2016, 91, 529–539. [Google Scholar] [CrossRef]
- Reinkensmeyer, D.J. JNER at 15 years: Analysis of the state of neuroengineering and rehabilitation. J. Neuroeng. Rehabil. 2019, 16, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Stinear, C.M.; Lang, C.E.; Zeiler, S.; Byblow, W.D. Advances and challenges in stroke rehabilitation. Lancet Neurol. 2020, 19, 348–360. [Google Scholar] [CrossRef]
- Musselman, K.E.; Shah, M.; Zariffa, J. Rehabilitation technologies and interventions for individuals with spinal cord injury: Translational potential of current trends. J. Neuroeng. Rehabil. 2018, 15, 40. [Google Scholar] [CrossRef] [PubMed]
- Song, W.-K. Trends in rehabilitation robots and their translational research in National Rehabilitation Center, Korea. Biomed. Eng. Lett. 2016, 6, 1–9. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Robotic Rehabilitation Technology | Underlying Technologies | Area of Application | Readiness Level | Major Roadblocks | Convergence |
|---|---|---|---|---|---|
| Human–Robot Control Interfaces Section 3.1 Technologies that enable the communication between humans and neuro-robotics | Digital–Neural Interfaces Section 3.1.1 Technologies that interface the human nervous system with robotics. | Implantable devices acquiring data, stimulating nerves, and assisting signal transfer across traumatized parts of the central and peripheral nervous system. | Microelectronic design processes are mature. Microelectromechanical systems (MEMS) design processes are well developed; however, simulation design tools need improvement. | Parts of the CNS are not easily accessible to implantable devices without traumatic and risky surgical procedures (invasiveness). Electrode and implantable device placement require precise navigation inside the human body, with error tolerances that are not always possible to achieve. Selectivity of electrodes, data flow, and long-term consequences are still active challenges. | Existing: Microelectronic very large-scale integration (VLSI), microelectromechanical systems (MEMS) design and micromanufacturing techniques lead to novel electrodes. Low power mixed signal and radio frequency (RF) electronics design leads to increasingly more power-autonomous implantable devices. Potential: MEMS microgenerators lead to complete power autonomy for implantable devices. |
| Electromyography Section 3.1.2 Enables the communication between a user and a robotic device by interfacing with the muscles. | Rehabilitation of stroke, muscular dystrophy, and amputation. | There are existing commercial applications. Ongoing research toward musculoskeletal modelling and safe and reliable implantable devices. | Lack of portability restricts movement and limits convergence with robotics. Unreliable sensors’ result in limited interfacing, which further deteriorates outside of lab conditions. Intention decoding algorithms for electromyography (EMG) are of limited robustness and generalizability. | Existing: Virtual reality, functional electrical stimulation, robotic exoskeletons, prosthetics. Potential: EMG needs the development of reliable sensors and portable amplifiers. Safe and reliable implantable sensors may achieve better signal quality. Additionally, better AI algorithms or biomechanical models for intention decoding may result in improved human–robot interfacing. | |
| Brain-Computer Interfaces Section 3.1.3 Enables the communication between a user and a robotic device by interfacing with the brain. | Rehabilitation of stroke, spinal cord injury, muscular dystrophy, amputation, traumatic brain injury, and mental disorders. | There are existing commercial applications. Research is still underway toward better sensors and intention decoding algorithms. | Unclear therapeutic benefits compared to traditional rehabilitation. Sensors still require long set-up times. Intention decoding algorithms require long calibration and lack generalization. | Existing: Virtual reality, functional electrical stimulation, robotic exoskeletons, and prosthetics. Potential: Brain–computer interfaces (BCIs) can improve dramatically with the use of better digital–neural interfaces and the development of AI algorithms for intention decoding. | |
| Neuro-Robotics Section 3.2 The science and technology of embodied autonomous neural systems. | Exoskeletons Section 3.2.1 Assists with the recovery of function compromised due to sensory and cognitive deficits or daily assistance. | Rehabilitation of stroke, spinal cord injury, muscular dystrophy, traumatic brain injury, and mental disorders. | There are existing commercial applications. Research toward soft exoskeletons is currently attracting interest. | Human–machine interface compliance, optimization of the control algorithms, and the smooth coordination with the physiology of the human body. Restrictions to mimic the gesture of the joints, to measure joint torques, and to drive joint-specific rehabilitation. | Existing: BCI, virtual and augmented reality, AI algorithms. Potential: Sensors for new information on human intent and motor status, big data for the vast number of physiological signals, machine learning for new control approaches, and 3D printing of materials for customization and cost-effectiveness. |
| Neuroprosthetics Section 3.2.2 A device or system that replaces a missing body part to supplement its functionality. | Amputations. | There are existing commercial applications. Ongoing research toward better fitting and human–machine interfacing solutions. | Patient’s reaction to long-lasting implantation of microelectrode as well as the proper part of the body to collect a signal. Limitations in stretchable electronics, electrode–skin interfaces, and personalization. | Existing: BCI, virtual and augmented reality, AI algorithms. Potential: Control methods that include peripheral nerve interfaces and BCIs. Decoding and control using biomechanical musculoskeletal modelling and model-free machine learning. | |
| Virtual Reality and Augmented Reality Section 3.3 Technologies that generate an artificial simulation of an environment (virtual reality, VR) and project computer generated graphics in real world space (augmented reality, AR) | Virtual Reality The combination of algorithms, sensors, and high-definition (HD) display for the reproduction of an environment using virtual objects. Augmented Reality An augmented version of the actual physical world that is accomplished by the use of visual objects, sound, or other sensory stimulation. | Task-oriented biofeedback therapy, rehabilitation of stroke, brain, and spinal cord injury. | There are existing commercial applications. Research toward the “interaction” aspect of VR and AR. | Theoretical ambiguity for presence and immersion. Motion sickness and discomfort is another roadblock. | Existing: Artificial intelligence, human–computer interactions (HCIs). Potential: Improving VR/AR system’s latency may increase interactivity. Additionally, a solid theoretical basis for presence will give clear direction for the fields. |
| AI Algorithms Section 3.4 Algorithms that learn from experience and simulate human-level intelligence. | AI algorithms for Human–Robot Interaction Section 3.4.1 Deep learning algorithms aimed to enable and enhance the interaction between humans and robotic devices. | Object classification, action detection, and action planning. | There are existing commercial applications. Research on quantum machine learning (ML) and safety measures is still underway. | Computational complexity, computing resources, and safety risks. | Existing: HCIs, virtual reality, robotic exoskeletons, and prosthetics. Potential: Quantum ML may overcome the computational challenges of the current ML approach. |
| AI algorithms for Neural Signal Processing Section 3.4.2 Machine Learning and Unsupervised Learning algorithms and techniques that process and analyze neural signals to extract information. | Signal capture, feature extraction, and feature clustering. | There are existing commercial applications. Research on massively parallel signal processing and algorithmic design still underway. | The algorithms work on a limited number of signal inputs. In addition, they suffer from high computational complexity and need high computing resources. | Existing: Brain–machine interfaces (BMIs)/BCIs, robotic exoskeletons, and prosthetics. Potential: Parallel signal processing may dramatically boost the accuracy of the models. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nizamis, K.; Athanasiou, A.; Almpani, S.; Dimitrousis, C.; Astaras, A. Converging Robotic Technologies in Targeted Neural Rehabilitation: A Review of Emerging Solutions and Challenges. Sensors 2021, 21, 2084. https://doi.org/10.3390/s21062084
Nizamis K, Athanasiou A, Almpani S, Dimitrousis C, Astaras A. Converging Robotic Technologies in Targeted Neural Rehabilitation: A Review of Emerging Solutions and Challenges. Sensors. 2021; 21(6):2084. https://doi.org/10.3390/s21062084
Chicago/Turabian StyleNizamis, Kostas, Alkinoos Athanasiou, Sofia Almpani, Christos Dimitrousis, and Alexander Astaras. 2021. "Converging Robotic Technologies in Targeted Neural Rehabilitation: A Review of Emerging Solutions and Challenges" Sensors 21, no. 6: 2084. https://doi.org/10.3390/s21062084
APA StyleNizamis, K., Athanasiou, A., Almpani, S., Dimitrousis, C., & Astaras, A. (2021). Converging Robotic Technologies in Targeted Neural Rehabilitation: A Review of Emerging Solutions and Challenges. Sensors, 21(6), 2084. https://doi.org/10.3390/s21062084