
Active Game-Based Solutions for the Treatment of Childhood Obesity

 ,
,  and
and 
Abstract
1. Introduction
2. Related Works
3. Active Game-Based Solutions Based on Kinect and Biometric Sensors
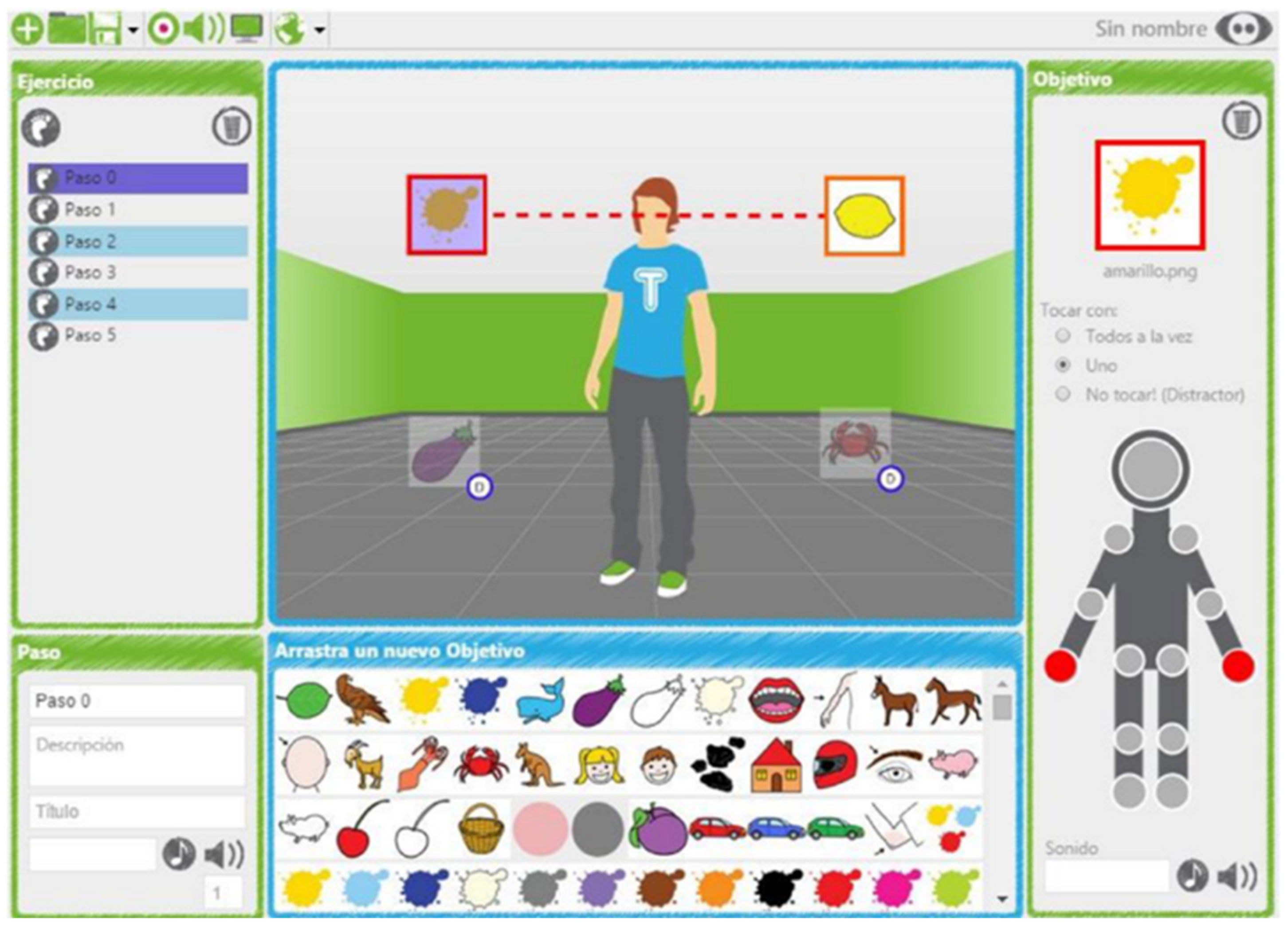
3.1. TANGO:H Web Designer
- (a)
- Menu bar: Executes the actions on the exercise file and the editor configuration.
- (b)
- Exercise panel: Visualizes the outline of an exercise, allowing navigation through its components and performing actions on each of its elements.
- (c)
- Target panel: View and edit the properties of the selected target.
- (d)
- Available objectives panel: Contains objectives that can be used in creating an exercise.
- (e)
- Design panel: Component where the exercise is designed, allowing the dragging of objectives to this panel.

- New. Create a new exercise. It directs the user to the selection window.
- Open. Opens an exercise from a file and loads it into the application. Only the exercises that belong to the user will be displayed.
- Save. It saves the current exercise.
- Objectives manager. Accesses the objective image management window.
- Sound manager. A sound management window is accessed.
- Background manager. The window for managing backgrounds is accessed.
- Languages. Selects the language preferences for the application.
- Information on the exercise. On the right side of the menu bar, information about the exercise being edited is displayed. Clicking on this information will open a window where the exercise’s name and description can be modified.
- Add new components. A set of controls located at the top of the panel. These enable the addition of a new step or phase. For cognitive exercises, the concept phase will not be used; each step will contain a set of objectives to be achieved.
- Step properties. In the lower part of the panel, there is a formula in which the selected Step properties are shown and edited. Here, the name, description, title, and audio file for the step can be edited.
- Target and color. The upper part of the panel shows the target’s image, surrounded by a frame of the associated color.
- Contact points. The assignment of contact points to the lens is made on the character image shown at the bottom of the panel. The selected contact points are shaded with the color associated with the target. It is possible to update the behavior of the target using the controls located on the image.
- Sound of the target. At the bottom of the panel, there is a set of controls that facilitate sound to the target.
- Delete a lens. The control in the upper right corner of the panel allows the target to be removed from the exercise.
- Insert target. To add a lens to the exercise, the desired image is dragged from the panel of available lenses to the day panel.
- Select a target (or several). A target is selected by clicking on it with the mouse. To select several targets at once, the “Ctrl” key is held while each of the desired targets are selected.
- Move one target. To move a target, it must be double-clicked and moved with the cursor around the Design Panel.
- New step. It will add a new step to the structure of the exercise.
- Delete step. It will remove the current step from the exercise.
- Phase properties. It will access the properties of the selected phase.
- Matching (only for cognitive matching exercises). Allows pairing two selected objectives.
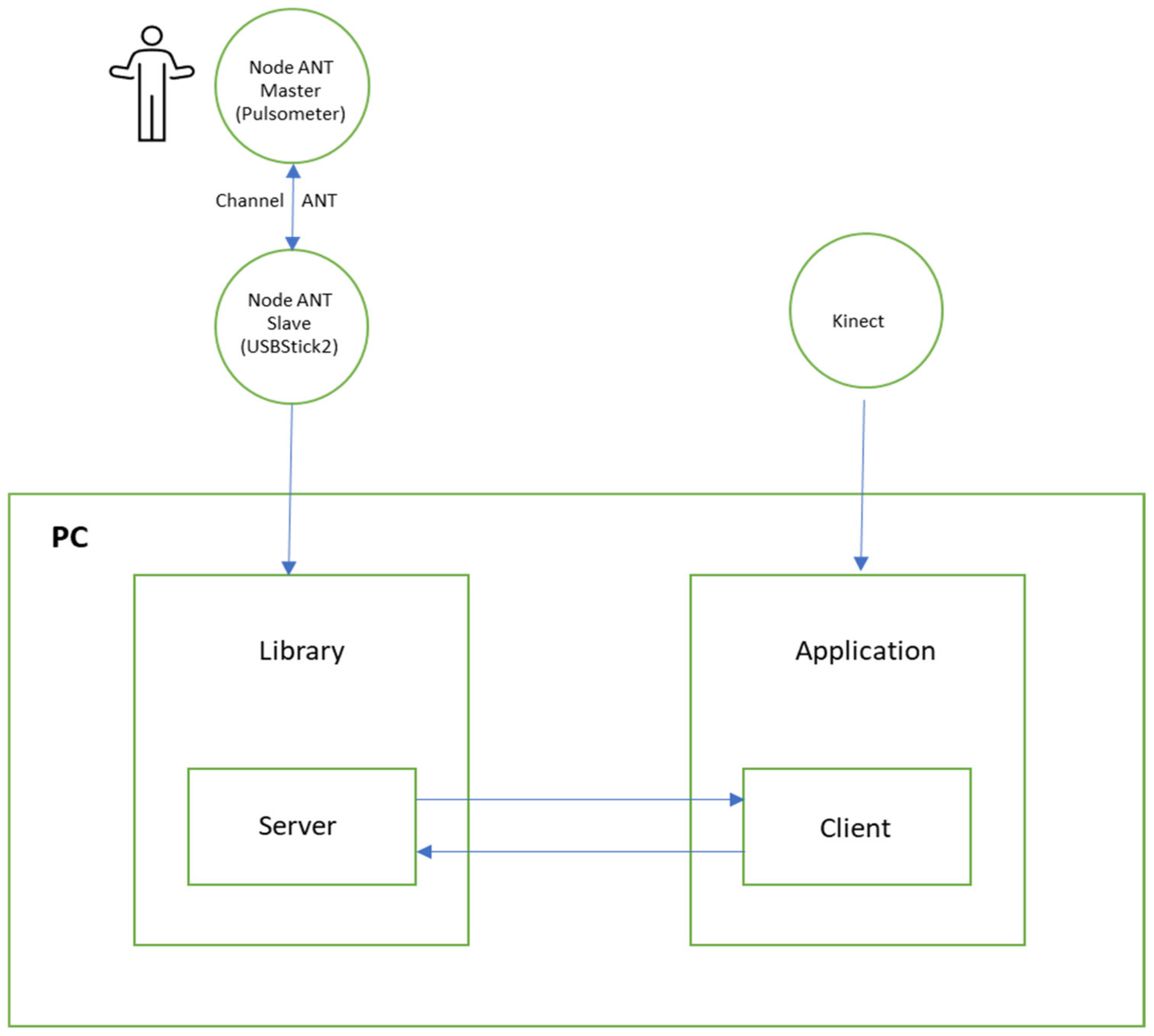
3.2. Exergame with Sensory Integration of Biometric Signals
(1 − sex) * (−20.402 + 0.4472 * HR−0.1263 * weight + 0.074 * age) kJ/min
- Jump. The central hip joint is raised above 12 cm from its previous position within 1.5 s.
- Squat. The center hip joint is lowered by six inches from its previous position in a 1.5 s interval.
- Lateral jumps. Starting from a position with the feet together (distance between the joints of the feet less than 30 cm) and finishing in this same position but having moved 25 cm to the right or left, depending on the response.
- Punch. The left or right hands advance in an interval of 1.5 s.
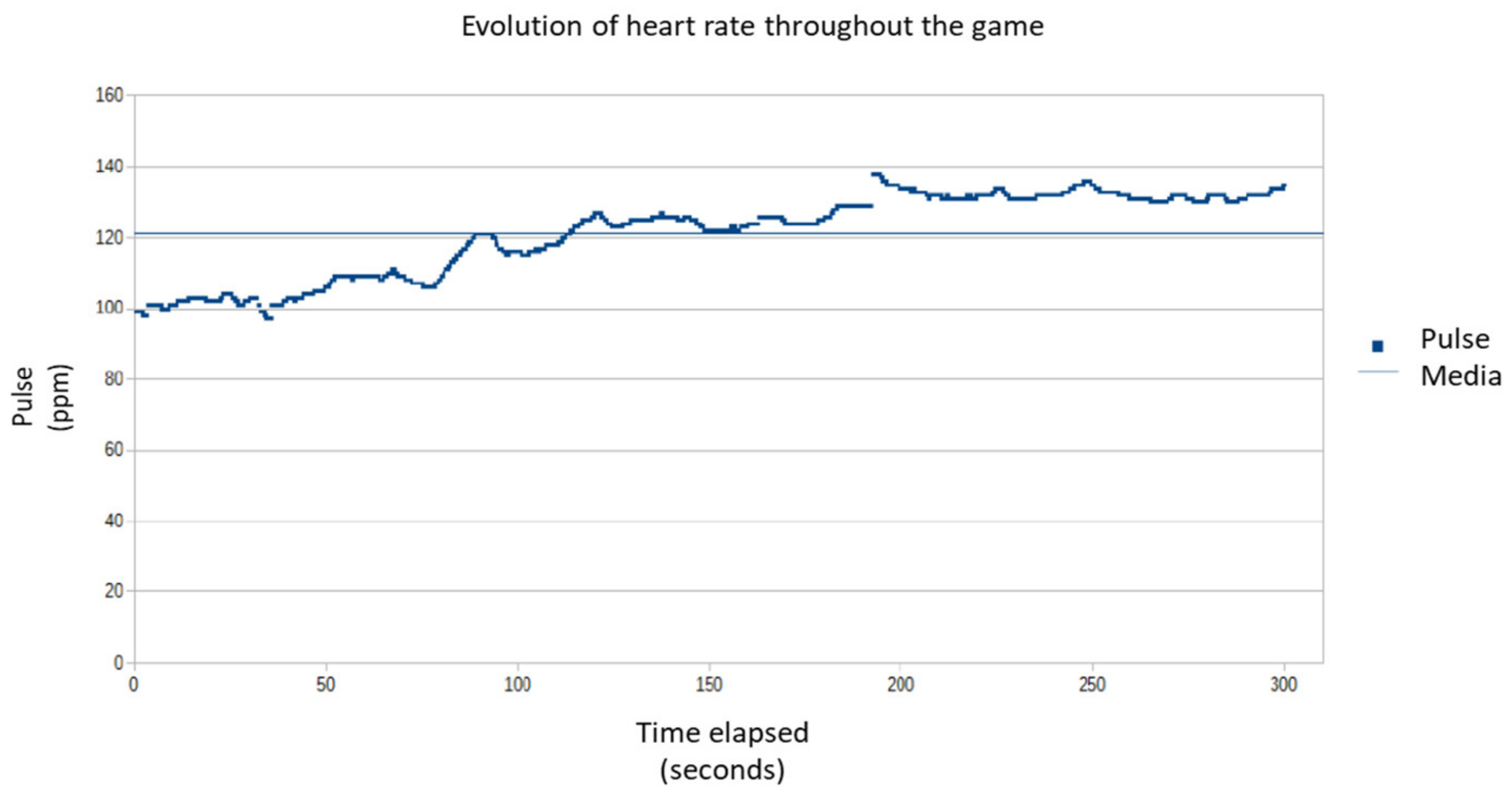
- Heart Rate: Located in the upper right corner, it indicates the user’s heart rate, which changes color from blue to red depending on the range of heartbeats.
- Calories: Indicates the accumulated energy consumption since the beginning of the game and are based in the energy expenditure estimation explained above.
- Score: Fraction that indicates the number of objects drawn or destroyed satisfactorily concerning the total number of objects that have appeared.
- Time Left: Time to analyze the game.
- Cylinders (“logs” or “barrels”): dodge by jumping.
- Blocks: destroy by frontal hit (punch).
- Shurikens: dodging by squats.
- Spheres: destroy by lateral jumps. They are presented in series and always appear in front of the user.
4. Method
4.1. Participants
4.2. Instruments
- Biomedical area (pediatrics, nutrition, nursing)
- ➢
- Variables: age, weight, height, BMI, skin folds, body perimeters, percentiles, blood pressure, and analytical parameters
- ➢
- Instruments: weight, height meter, BMI formula, lipo calibre, inextensible tape measure, growth curve, sphygmomanometer, and blood analysis.
- Psychological and psycho-pedagogical area:
- ➢
- Variables to be measured in children: evaluation of emotions resulting from human–computer interaction-observational measures; interpersonal relationships, relationships with parents, self-esteem, and self-confidence; knowledge and attitudes about healthy living habits and active video games.
- ➢
- Instruments:
- -
- EMODIANA [34]. An instrument which allows measuring 10 basic emotions, represented with different expressions of a character associated with their corresponding labels, adjusted to children’s language. It is used during group intervention sessions.
- -
- BASC (Behavior Assessment System for Children and Adolescents) [35]. This is a multidimensional questionnaire which measures numerous aspects of behavior and personality.
- -
- Adaptation of the questionnaire on Physical-Sports Activity and Health-Wellness [36].
- -
- Player profile test. Adaptation of the questionnaire on use and attitudes towards video games [37].
- -
- Mediterranean Diet Quality Index—KIDMED Questionnaire (Mediterranean Diet Quality Index for children and teenagers) [38].
- -
- Questionnaires for children and parents ad hoc. Items to collect information about the intervention carried out during the project.
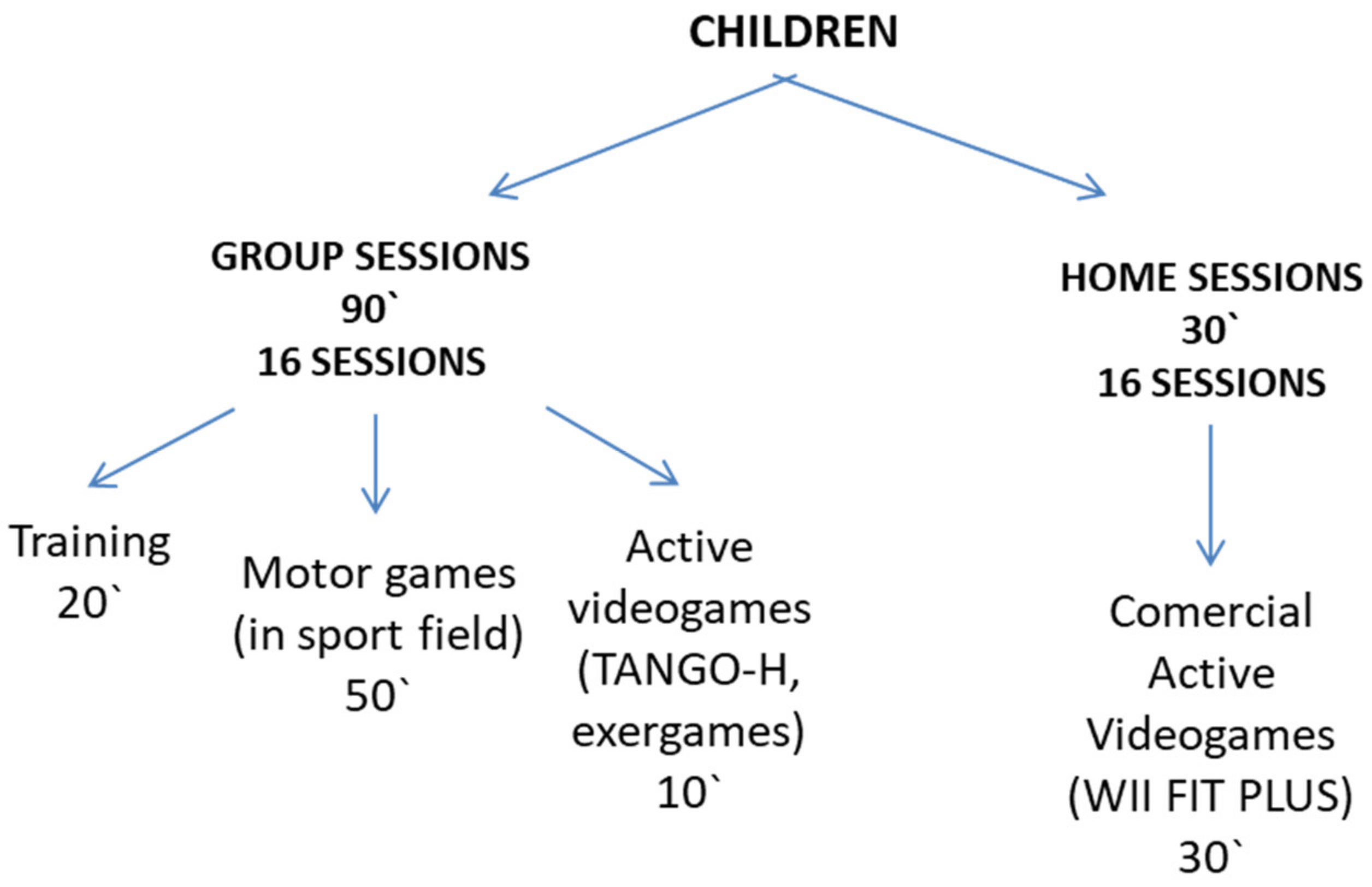
4.3. Procedure
5. Results
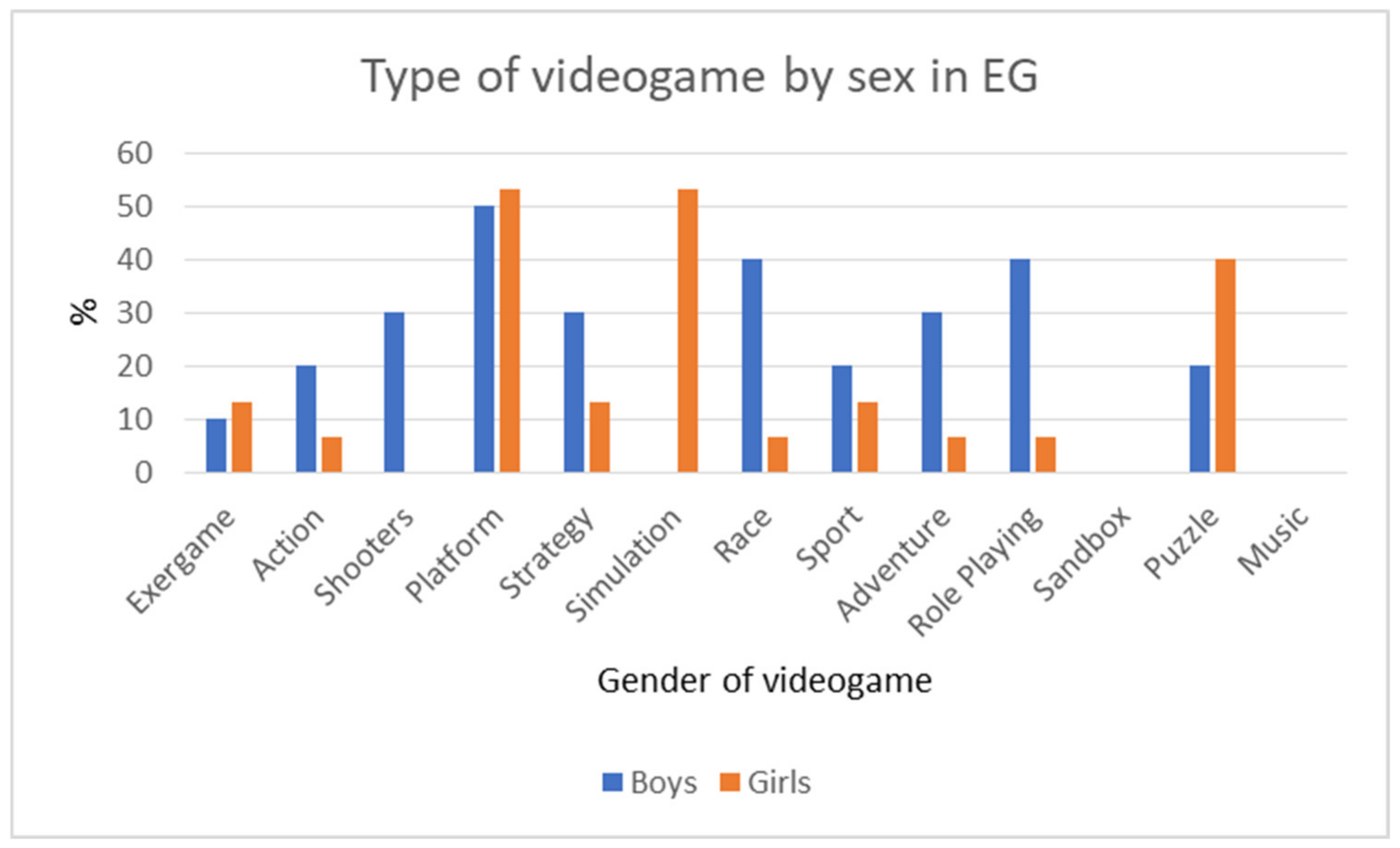
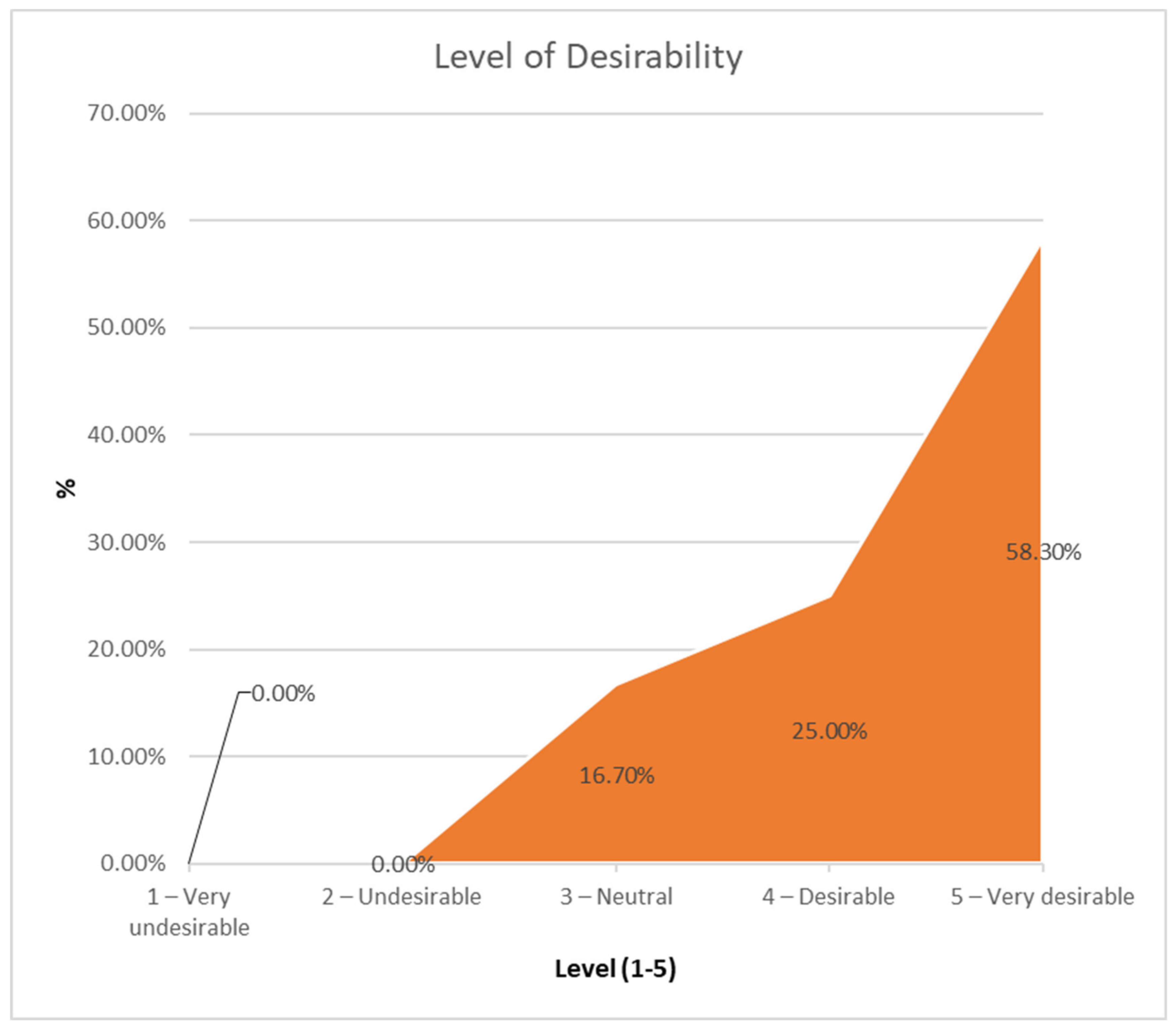
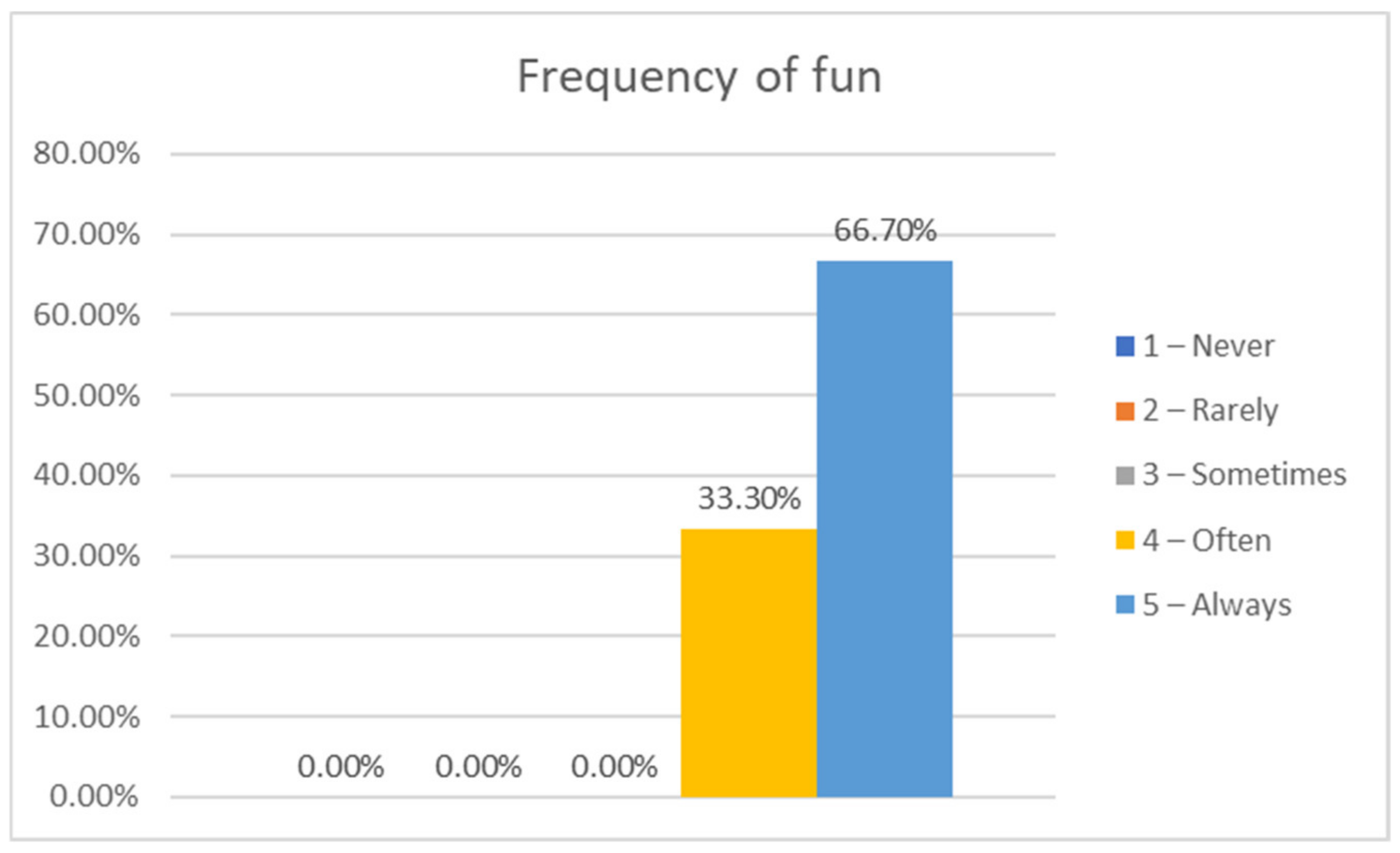
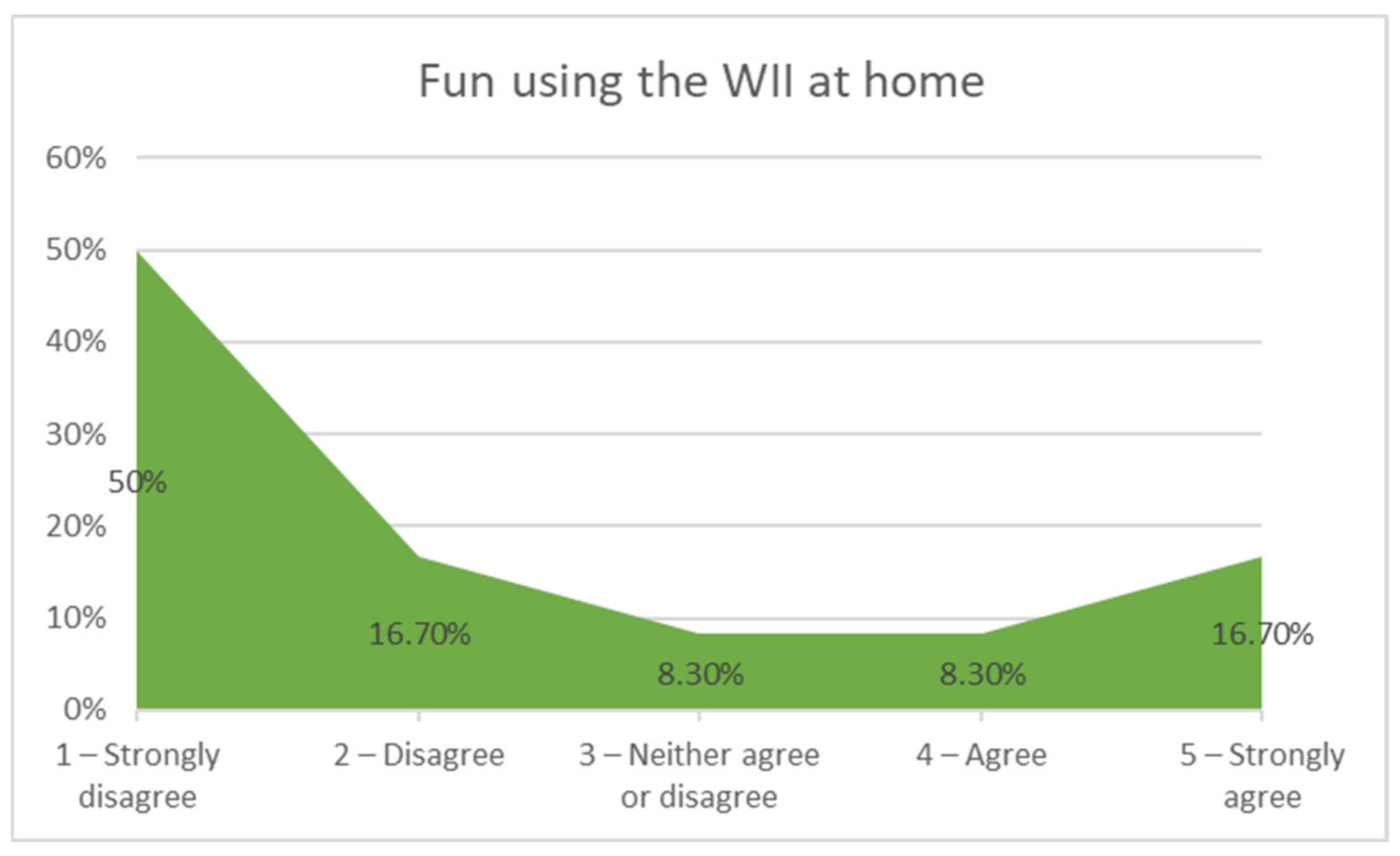
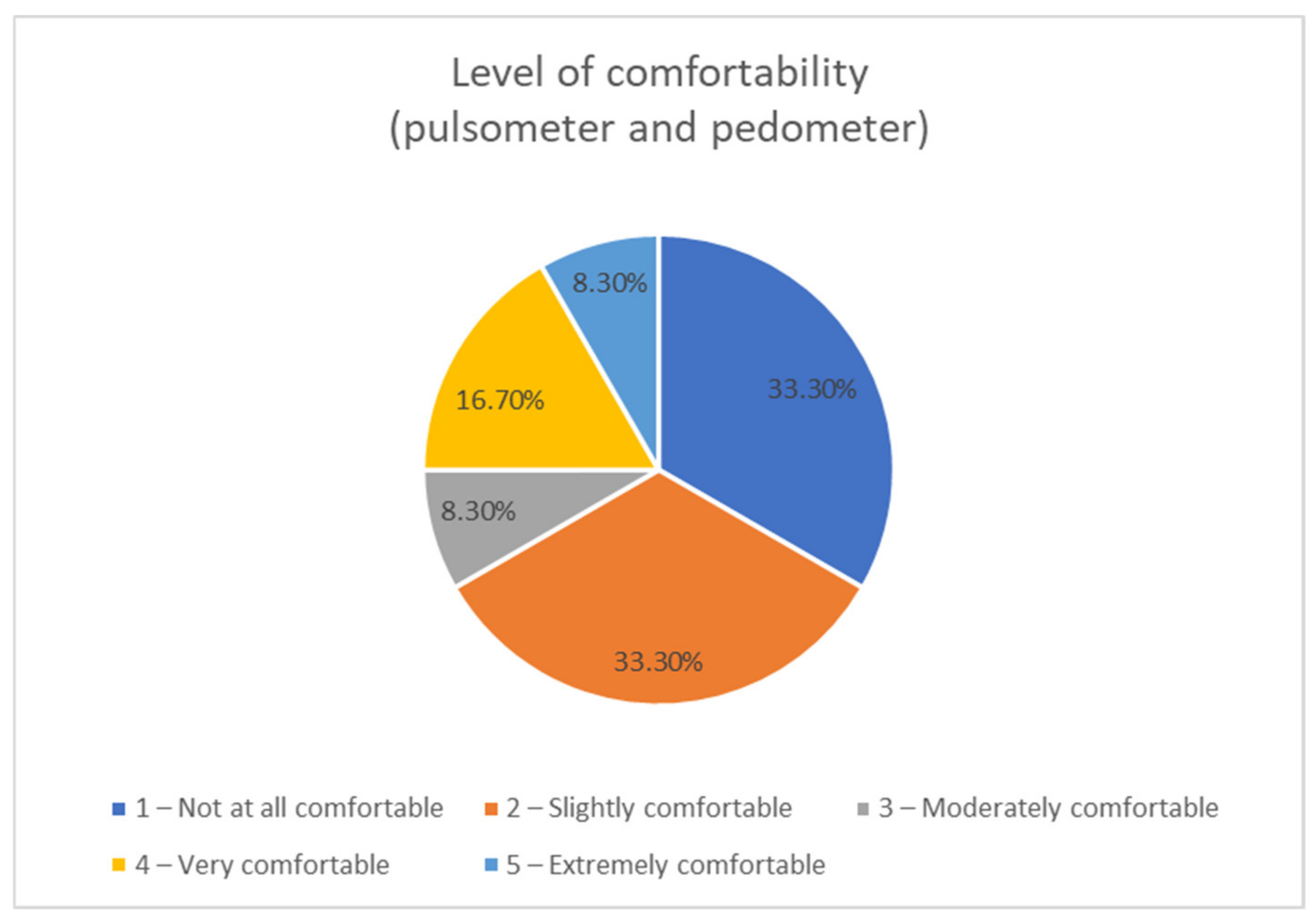
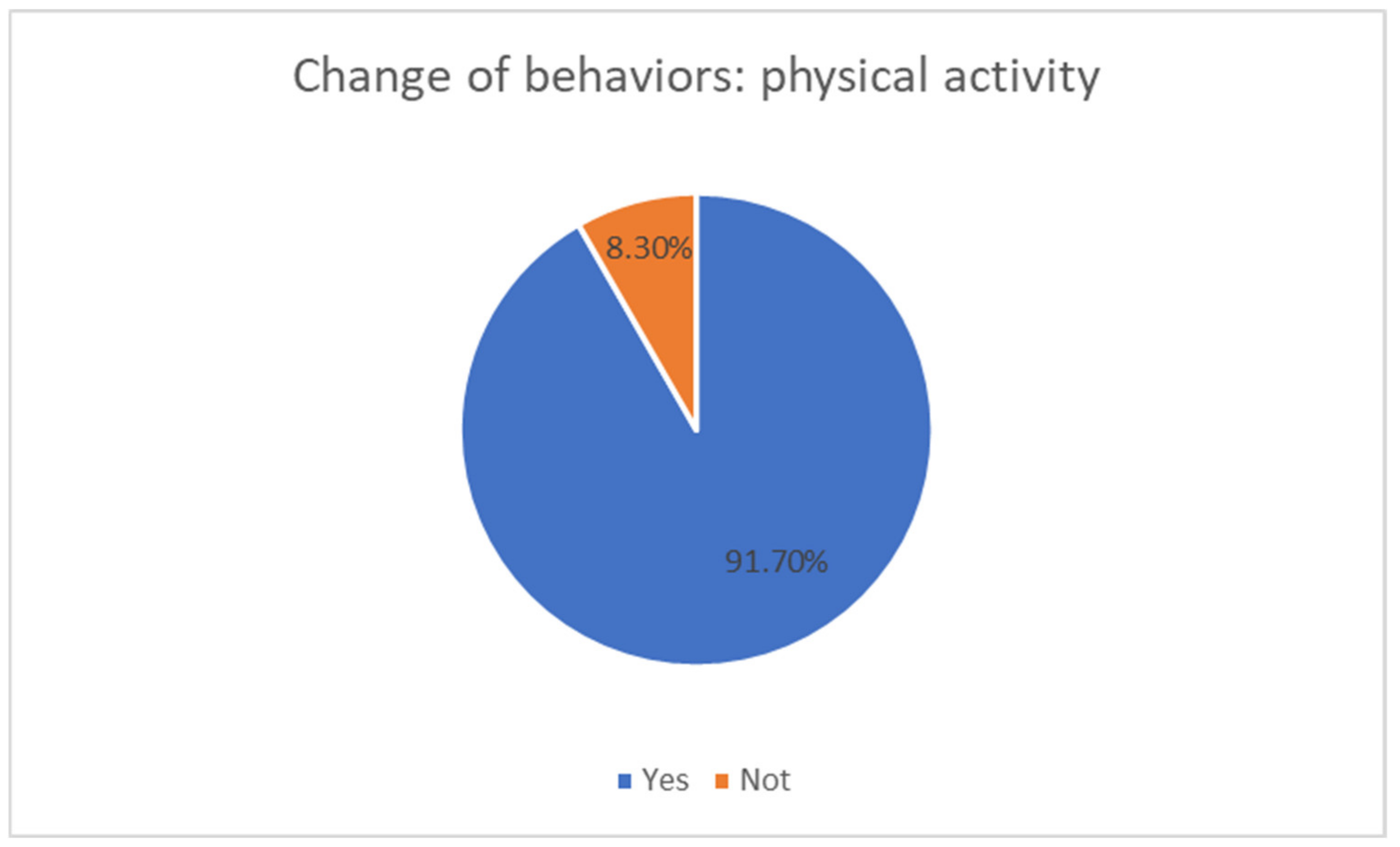
5.1. Perceived Variables Related to Active Video Games
- What I learned (50%);
- Play (58.3%);
- Do physical activity (25%);
- Earn qualifying points (41.7%);
- Being with colleagues (50%);
- Being with the professionals (8.3%);
- Improve my lifestyle (25%).
- It was fun (58.3%);
- Do physical activity (25%);
- That it was mandatory (8.3%);
- Other (8.3%).
- -
- The games and being with the companions;
- -
- Because I had fun games;
- -
- Improve my sessions and have a lot of fun;
- -
- That I learned new things and had fun with all;
- -
- To play;
- -
- That I played and sweated and had a lot of fun;
- -
- We learned;
- -
- The games;
- -
- Everything we did;
- -
- The games were fun;
- -
- That I had fun and had more friends to play;
- -
- TANGO:H;
- -
- The games we made.
5.2. Emotions Related to the Intervention
5.3. Anthropometric Variables Related to Obesity
5.4. Healthy Habits
6. Discussion
7. Conclusions
- -
- The creation of a web-based solution for creating active video games: TANGO:H designer, which allows for designing games in the cloud, and then be downloaded to be used with the Kinect sensor.
- -
- The creation of a heart rate-controlled exergame that uses biometric sensors and the Kinect sensor.
- -
- An educational intervention program approach to childhood obesity using commercially available active video games created by the research group, both at home and in weekly group sessions.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Baranowski, T.; Buday, R.; Thompson, D.I.; Baranowski, J. Playing for real–video games and stories for health-related behavior change. Am. J. Prev. Med. 2008, 34, 74–82. [Google Scholar] [CrossRef]
- Gonzalez, C.S.; Gómez, N.; Navarro, V.; Cairos, M.; Quirce, C.; Toledo, P.; Marrero-Gordillo, N. Learning healthy lifestyles through active videogames, motor games and the gamification of educational activities. Comput. Hum. Behav. 2016, 55, 529–551. [Google Scholar] [CrossRef]
- Guixeres, J. Terapias en Obesidad Infantil: Estudio de los Videojuegos Activos Como Promotor del Ejercicio Físico. Alto Rendimiento, 2011. Available online: http://altorendimiento.com/terapias-en-obesidad-infantil-estudio-de-los-videojuegos-activos-comopromotor-del-ejercicio-fisico (accessed on 9 February 2021).
- Clark, R.A.; Bryant, A.L.; Pua, Y.; McCrory, P.; Bennell, K.; Hunt, M. Validity and reliability of the Nintendo Wii Balance Board for assessment of standing balance. Gait Posture 2010, 31, 307–310. [Google Scholar] [CrossRef] [PubMed]
- Kato, P.M. Evaluating Efficacy and Validating Games for Health. Games Heal. J. 2012, 1, 74–76. [Google Scholar] [CrossRef] [PubMed]
- Sardi, L.; Idri, A.; Fernández-Alemán, J.L. A systematic review of gamification in e-Health. J. Biomed. Inform. 2017, 71, 31–48. [Google Scholar] [CrossRef] [PubMed]
- Southhall, J.E.; Okely, A.D.; Steele, J. Actual and perceived physical competence in overweight and nonover-weight children. Pediatr. Exerc. Sci. 2004, 16, 15–24. [Google Scholar] [CrossRef]
- Lu, A.S.; Kharrazi, H.; Gharghabi, F.; Thompson, D. A systematic review of health videogames on childhood obe-sity prevention and intervention. Games Health Res. Dev. Clin. Appl. 2013, 2, 131–141. [Google Scholar] [CrossRef]
- Del Rio, N.G.; González, C.S.G.; Gonzalez, R.M.; Adelantado, V.N.; Delgado, P.T.; Fleitas, Y.B. Gamified educational programme for childhood obesity. In Proceedings of the 2018 IEEE Global Engineering Education Conference (EDUCON), Tenerife, Spain, 17–20 April 2018. [Google Scholar] [CrossRef]
- Cuberos, R.C.; Gracés, T.E.; Fernándes, Á.C.; Sánches, M.C.; López Fernándes, J.F.; Ortega, F.Z. Exergames para la Mejora de la Salud en Niños y Niñas en Edad Escolar: Estudio a Partir de Hábi-tos Sedentarios e Índices de Obesidad. 2015. Available online: http://relatec.unex.es/article/view/1471 (accessed on 9 February 2021).
- Gao, Z.; Chen, S. Are field-based exergames useful in preventing childhood obesity? A systematic review. Obes. Rev. 2014, 15, 676–691. [Google Scholar] [CrossRef]
- González, C.S.; Gómez del Río, N.G.; Navarro, V. Exploring the benefits of using gamification and videogames for physical exercise: A review of state of art. IJIMAI 2018, 5, 46–52. [Google Scholar] [CrossRef]
- Papastergiou, M. Exploring the potential of computer and video games for health and physical education: A literature review. Comput. Educ. 2009, 53, 603–622. [Google Scholar] [CrossRef]
- Sánchez López, A.M.; Aguilar Cordero, M.; González Jiménez, E.; Padilla López, C.; Álvarez Ferre, J.; Ocete Hita, E. La Obesidad como factor pronóstico de la falta de motivación en el niño y en el adolescente. X Congreso Nacional de la SEEDO. Revista Española de la Obesidad 2011, 9, 99. [Google Scholar]
- Tan, B.; Aziz, A.; Chua, K.; The, K. Aerobic demands of the dance simulation game. Int. J. Sports Med. 2002, 23, 125–129. [Google Scholar] [CrossRef]
- Lanningham-Foster, L.; Jensen, T.; Foster, R.; Redmond, A.; Walker, B.; Heinz, D. Energy expenditure of sedentary screen time compared with active screen time for children. J. Pediatr. 2006, 118, 1831–1835. [Google Scholar] [CrossRef]
- Lanningham-Foster, L.; Foster, R.C.; McCrady, S.K.; Jensen, T.B.; Mitre, N.; Levine, J.A. Activity-promoting video-games and increased energy expenditure. J. Pediatr. 2009, 154, 819–823. [Google Scholar] [CrossRef] [PubMed]
- Mellecker, R.; McManus, A. Energy expenditure and cardiovascular responses to seated and active gaming in chil-dren. Arch. Pediatr. Adolesc. Med. 2008, 162, 886–891. [Google Scholar] [CrossRef] [PubMed]
- Maddison, R.; Mhurchu, C.; Jull, A.; Jiang, Y.; Prapavessis, H.; Rodgers, A. Energy expended playing video console games: An opportunity to increase children’s physical activity? Pediatr. Exerc. Sci. 2007, 19, 334–343. [Google Scholar] [CrossRef] [PubMed]
- Wetzsleon, R.; Swanson, K.; Pickett, K. Energy expenditure and ground reaction forces of an active video game, Dance Dance Revolution, in healthy weight and overweight children. Med. Sci. Sports Exerc. 2008, 40, S255. [Google Scholar]
- Staiano, A.E.; Beyl, R.A.; Guan, W.; Hendrick, C.A.; Hsia, D.S.; Newton, R.L. Home-based exergaming among children with overweight and obesity: A randomized clinical trial. Pediatr. Obes. 2018, 13, 724–733. [Google Scholar] [CrossRef]
- Brown, T.; Moore, T.H.; Hooper, L.; Gao, Y.; Zayegh, A.; Ijaz, S.; Elwenspoek, M.; Foxen, S.C.; Magee, L.; O’Malley, C.; et al. Interventions for preventing obesity in children. Cochrane Database Syst. Rev. 2019, 7, CD001871. [Google Scholar] [CrossRef]
- Chin, A.; Paw, M.; Jacobs, W.; Vaessen, E.; Titze, S.; van Mechelen, W. The motivation of children to play an active video game. J. Sci. Med. Sport 2008, 11, 163–166. [Google Scholar] [CrossRef]
- Del Río, N.G.; González-González, C.S.; Toledo-Delgado, P.A.; Muñoz-Cruz, V.; García-Peñalvo, F. Health Promotion for Childhood Obesity: An Approach Based on Self-Tracking of Data. Sensors 2020, 20, 3778. [Google Scholar] [CrossRef]
- Nenonen, V.; Lindblad, A.; Häkkinen, V.; Laitinen, T.; Jouhtio, M.; Hämäläinen, P. Using heart rate to control an interactive game. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems; ACM: Hong Kong, China, 2007; pp. 853–856. [Google Scholar]
- Hoffmann, K.; Wiemeyer, J.; Hardy, S.; Göbel, S. Personalized Adaptive Control of Training Load in Exergames from a Sport-Scientific Perspective. In Proceedings of the Constructive Side-Channel Analysis and Secure Design; Springer International Publishing: Berlin/Heidelberg, Germany, 2014; pp. 129–140. [Google Scholar]
- Happitech. Skip a Beat Game. Available online: http://skipabeatgame.com/ (accessed on 9 February 2021).
- Osterwalder, F.; Pollinger, P. Flitz! Adaptative exErgame. Echo Grafik. Available online: http://www.echo-grafik.ch/flitz/index.html (accessed on 9 February 2021).
- Machado, F.; Denadai, B. Validity of maximum heart rate prediction equations for children and adolescents. Ar-Quivos Bras. Cardiol. 2011, 97, 136–140. [Google Scholar] [CrossRef] [PubMed]
- Roy, S.J. Validation of Maximal Heart Rate Regression Equations. Ph.D. Thesis, University of Pittsburgh, Pittsburgh, PA, USA, 2009. [Google Scholar]
- Cicone, Z.S.; Holmes, C.J.; Fedewa, M.V.; Macdonald, H.V.; Esco, M.R. Age-Based Prediction of Maximal Heart Rate in Children and Adolescents: A Systematic Review and Meta-Analysis. Res. Q. Exerc. Sport 2019, 90, 417–428. [Google Scholar] [CrossRef]
- Benson, R.; Connolly, D. Heart Rate Training; Human Kinetics: Champaign, IL, USA, 2019. [Google Scholar]
- Keytel, L.R.; Goedecke, J.H.; Noakes, T.D.; Hiiloskorpi, H.; Laukkanen, R.; van der Merwe, L.; Lambert, E.V. Prediction of energy expenditure from heart rate monitor-ing during submaximal exercise. J. Sports Sci. 2005, 23, 289–297. [Google Scholar] [CrossRef] [PubMed]
- González-González, C.S.; Cairós-González, M.; Navarro-Adelantado, V. EMODIANA: Un instrumento para la evaluación subjetiva de emociones en niños y niñas. In Actas del XIV Congreso Internacional de Interacción Persona-Ordenador; Asociación Interacción Persona-Ordenador (AIPO): Madrid, Spain, 2013. [Google Scholar] [CrossRef]
- Reynolds, C.R.; Kamphaus, R.W. BASC-2. Behavior Assessment System for Children, 2nd ed.; Pearson: Blooming-ton, MN, USA, 2004. [Google Scholar]
- Estévez-López, F.; Tercedor, P. Delgado-Fernández, M. Recomendaciones de actividad física para adultos sanos. J. Sport Health Res. 2012, 4, 233–244. [Google Scholar]
- Alfageme González, M.B.; Sánchez Rodríguez, P.A. Un instrumento para evaluar el uso y las actitudes hacia los videojuegos. Pixel-Bit. Rev. Med. Educ. 2003, 20, 17–32. [Google Scholar]
- Del Río, N.G.; González-González, C.S.; Martín-González, R.; Navarro-Adelantado, V.; Toledo-Delgado, P.; García-Peñalvo, F. Effects of a Gamified Educational Program in the Nutrition of Children with Obesity. J. Med Syst. 2019, 43, 198. [Google Scholar] [CrossRef]
- González-González, C.S.; Navarro-Adelantado, V. Methods and techniques for evaluating the emotional expe-riences of children with active videogames. In Proceedings of the XVI International Conference on Human Computer Interaction, Rome, Italy, 2–6 September 2013. [Google Scholar]
- Fleiss, J.L.; Levin, B.; Paik, M.C. The measurement of interrater agreement. Stat. Methods Rates Pro-Portions 1981, 2, 22–23. [Google Scholar]
- Fernández, C.; Lorenzo, H.; Vrotsou, K.; Aresti, U.; Rica, E.; Sánchez, I. Estudio de crecimiento de Bilbao. Cur-vas y tablas de crecimiento. Faustino Orbegozo Foundation, 2011. Available online: https://www.fundacionorbegozo.com/wp-content/uploads/pdf/estudios_2011.pdf (accessed on 9 February 2021).
- Fardoun, H.; González-González, C.S.; Collazos, C.A.; Yousef, M. Estudio exploratorio en Iberoamérica sobre procesos de enseñanza-aprendizaje y propuesta de evaluación en tiempos de pandemia. Educ. Knowl. Soc. 2020, 21. [Google Scholar] [CrossRef]
- García-Peñalvo, F.J.; Corell, A.; Abella-García, V.; Grande-de-Prado, M. Online Assessment in Higher Education in the Time of COVID-19. Educ. Knowl. Soc. 2020, 21. [Google Scholar] [CrossRef]
- García-Peñalvo, F.J.; Corell, A. La COVID-19: ¿enzima de la transformación digital de la docencia o reflejo de una crisis metodológica y competencial en la educación superior? Campus Virtuales 2020, 9, 83–98. [Google Scholar]
- Violant-Holz, V.; Gallego-Jiménez, M.G.; González-González, C.S.; Muñoz-Violant, S.; Rodríguez, M.J.; San-sano-Nadal, O.; Guerra-Balic, M. Psychological Health and Physical Activity Levels during the COVID-19 Pan-demic: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 9419. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Zone | Range | Characteristics |
|---|---|---|
| 1 | 50–60% HRmax | Low intensity. Indicated for heating and recovery after exercise. |
| 2 | 60–70% HRmax | Moderate intensity. Zone indicated for the increased metabolism of adipose tissue. |
| 4 | 80–90% HRmax | Aerobic limit. |
| 5 | 90–100% HRmax | Beginning of the anaerobic training zone (oxygen deficit). |
| Variables | Pre-Test | Post-Test | |||
|---|---|---|---|---|---|
| Median | SD | Median | SD | ||
| Age | Experimental Group | 9.275 | 1.745 | 9.23 | 2.03 |
| Control Group | 9.38 | 1.585 | 9.65 | 1.44 | |
| Weight | Experimental Group | 60.615 | 13.95 | 58.915 | 11.435 |
| Control Group | 55.865 | 10.69 | 56.335 | 7.575 | |
| Height | Experimental Group | 1.425 | 0.115 | 1.435 | 0.115 |
| Control Group | 1.445 | 0.11 | 1.465 | 0.09 | |
| BMI | Experimental Group | 29.62 | 4.73 | 28.3 | 3.51 |
| Control Group | 26.675 | 3.065 | 25.99 | 2.32 | |
| Waist-to-hip ratio | Experimental Group | 0.98 | 0.055 | 0.995 | 0.07 |
| Control Group | 0.91 | 0.15 | 1.55 | 2.28 | |
| Group | Stage | KIDMED Index |
|---|---|---|
| Experimental Group Min = 5.00 Max = 11.00 | Pre-test | 7.67 |
| Control Group Min = 4.00 Max = 11.00 | Pre-test | 7.11 |
| Experimental Group Min = 5.00 Max = 10.00 | Post-test | 7.65 |
| Control Group Min = 5.00 Max = 10.00 | Post-test | 6.78 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
González-González, C.S.; Gómez del Río, N.; Toledo-Delgado, P.A.; García-Peñalvo, F.J. Active Game-Based Solutions for the Treatment of Childhood Obesity. Sensors 2021, 21, 1266. https://doi.org/10.3390/s21041266
González-González CS, Gómez del Río N, Toledo-Delgado PA, García-Peñalvo FJ. Active Game-Based Solutions for the Treatment of Childhood Obesity. Sensors. 2021; 21(4):1266. https://doi.org/10.3390/s21041266
Chicago/Turabian StyleGonzález-González, Carina S., Nazaret Gómez del Río, Pedro A. Toledo-Delgado, and Francisco José García-Peñalvo. 2021. "Active Game-Based Solutions for the Treatment of Childhood Obesity" Sensors 21, no. 4: 1266. https://doi.org/10.3390/s21041266
APA StyleGonzález-González, C. S., Gómez del Río, N., Toledo-Delgado, P. A., & García-Peñalvo, F. J. (2021). Active Game-Based Solutions for the Treatment of Childhood Obesity. Sensors, 21(4), 1266. https://doi.org/10.3390/s21041266