
A Survey of Methods and Technologies Used for Diagnosis of Scoliosis



Abstract
:1. Introduction
2. Historical Background—Traditional Methods of Measuring the Degree of Spinal Curvature
3. Surface Topography Imaging and Spinal Deformity Assessment
3.1. Moiré Method
3.2. Raster Topography with Automatic Image Analysis
3.3. Diers Formetic II 4D Optoelectronic Method
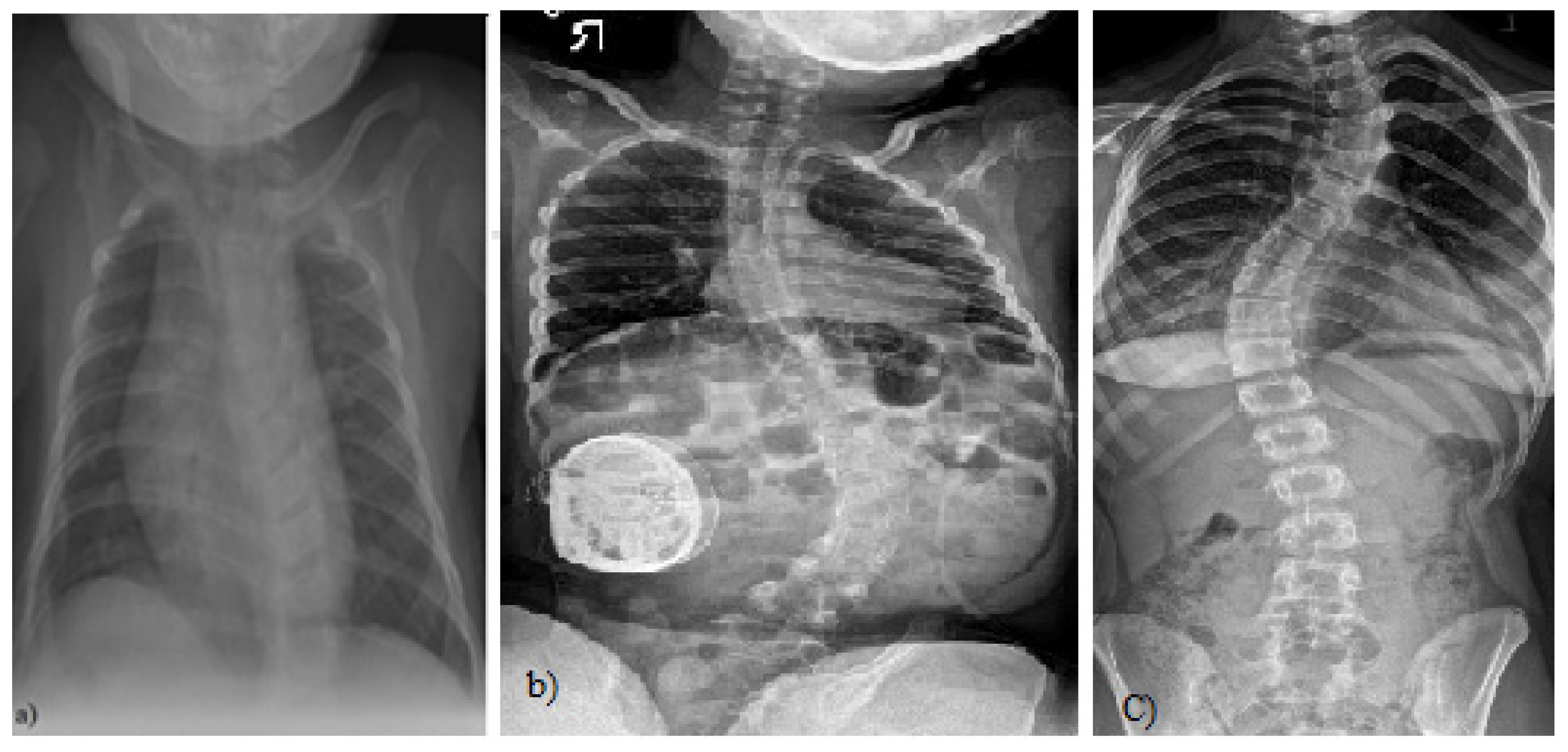
4. Methods for Imaging and Evaluation of Scoliosis Using Radiography
5. Method for Imaging and Evaluation of Scoliosis Using Magnetic Resonance Imaging (MRI)
6. Computed Tomography (CT)
7. Artificial Intelligence (AI) As a Method for Detection of Scoliosis
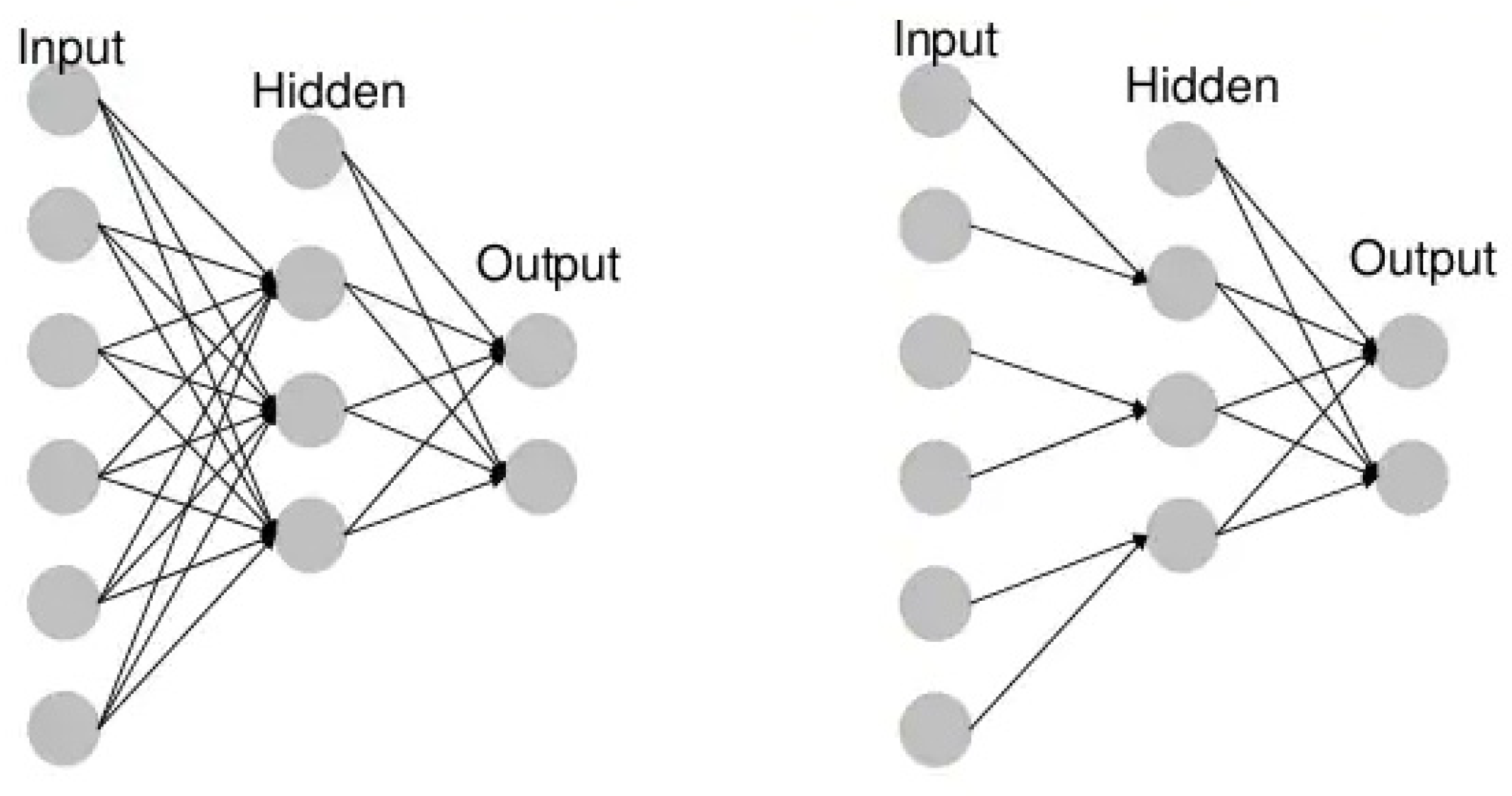
- Unidirectional neural networks, i.e., multilayer perceptrons (MLP) (Figure 3), consist of an input layer, a hidden layer(s) and an output layer. While these neural networks are also commonly referred to as MLPs, keep in mind that they are actually sigmoidal neurons, not perceptrons, as most real-world problems are non-linear. Data are used to train these models. They form the basis of computer vision, natural language processing and other neural networks.
- Convolutional neural networks (CNNs) are similar to unidirectional networks but are typically used for image recognition, pattern recognition and/or computer vision. These networks use the principles of linear algebra, in particular, matrix multiplication, to identify patterns in an image.
- Recursive neural networks (RNNs) are distinguished based on feedback loops.
7.1. Neural Networks and Deep Learning
7.2. Automatic Measurement Algorithm of Scoliosis Cobb Angle Based on Deep Learning
8. Open Databases—Spine/Scoliosis Images
- PhysioNet (accessed on 1 December 2021)
- National Institutes of Health (NIH), e.g., https://clinicaltrials.gov/ct2/home, https://www.clinicaltrials.gov/ct2/show/NCT00448448?term=NCT00448448&rank=1 and https://www.niams.nih.gov/health-topics/scoliosis (accessed on 1 December 2021)
- Radiopaedia.org (accessed on 1 December 2021)
- ieee-dataport.org (accessed on 1 December 2021)
- sethu.ac.in (accessed on 1 December 2021)
- boxdicom.com/samples.html (accessed on 1 December 2021)
- Biomedia (accessed on 1 December 2021)
9. Discussion
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rogala, E.J.; Drummond, D.S.; Gurr, J. Scoliosis: Incidence and Natural History. A Prospective Epidemiological Study. J. Bone Jt. Surg. 1978, 60, 173–176. [Google Scholar] [CrossRef]
- Altaf, F.; Gibson, A.; Dannawi, Z.; Noordeen, H. Adolescent Idiopathic Scoliosis. BMJ 2013, 346, 1527–1537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bunnell, W.P. The Natural History of Idiopathic Scoliosis. Clin. Orthop. Relat. Res. 1988, 229, 20–25. [Google Scholar] [CrossRef]
- Kaufman, B.A. Congenital Intraspinal Anomalies: Spinal Dysraphism-Embryology, Pathology and Treatment. Textb. Spinal Surg. 1997, 1, 365–400. [Google Scholar]
- Desai, S. Infantile Vertebral Scoliosis. Case Study. Available online: https://radiopaedia.org/cases/63310 (accessed on 1 December 2021).
- Jones, J. Neurodevelopmental Scoliosis. Case Study. Available online: https://doi.org/10.53347/rID-89566 (accessed on 1 December 2021).
- Jones, J. Idiopathic Scoliosis with Spondylolisthesis. Case Study. Available online: https://doi.org/10.53347/rID-89456 (accessed on 1 December 2021).
- Stokes, I.A. Axial Rotation Component of Thoracic Scoliosis. J. Orthop. Res. Off. Publ. Orthop. Res. Soc. 1989, 7, 702–708. [Google Scholar] [CrossRef] [PubMed]
- Asher, M.A.; Burton, D.C. Adolescent Idiopathic Scoliosis: Natural History and Long Term Treatment Effects. Scoliosis 2006, 1, 2. [Google Scholar] [CrossRef] [Green Version]
- Dubousset, J. Three-Dimensional Analysis of the Scoliotic Deformity (Chapter 22). Pediatr. Spine Princ. Pract. 1994, 1, 479–496. [Google Scholar]
- Ferguson, A.B. The study and treatment of scoliosis. South. Med. J. 1930, 23, 116–120. [Google Scholar] [CrossRef]
- Cobb, R.J. Outline for Study of Scoliosis. Instructional Course Lectures. Am. Acad. Orthop. Surg. 1948, 261–275. [Google Scholar]
- Zhou, G.-Q.; Jiang, W.-W.; Lai, K.-L.; Zheng, Y.-P. Automatic Measurement of Spine Curvature on 3-D Ultrasound Volume Projection Image with Phase Features. IEEE Trans. Med. Imaging 2017, 36, 1250–1262. [Google Scholar] [CrossRef] [PubMed]
- Cobb Angle Measurment. Case Study. Available online: https://radiopaedia.org/cases/cobb-angle-measurment (accessed on 1 December 2021).
- Komeili, A.; Westover, L.M.; Parent, E.C.; Moreau, M.; El-Rich, M.; Adeeb, S. Surface Topography Asymmetry Maps Categorizing External Deformity in Scoliosis. Spine J. Off. J. N. Am. Spine Soc. 2014, 14, 973–983.e2. [Google Scholar] [CrossRef]
- Pruijs, J.E.; Hageman, M.A.; Keessen, W.; van der Meer, R.; van Wieringen, J.C. Variation in Cobb Angle Measurements in Scoliosis. Skelet. Radiol. 1994, 23, 517–520. [Google Scholar] [CrossRef]
- Watanabe, K.; Aoki, Y.; Matsumoto, M. An Application of Artificial Intelligence to Diagnostic Imaging of Spine Disease: Estimating Spinal Alignment from Moiré Images. Neurospine 2019, 16, 697–702. [Google Scholar] [CrossRef] [PubMed]
- Beekman, C.E.; Hall, V. Variability of Scoliosis Measurement from Spinal Roentgenograms. Phys. Ther. 1979, 59, 764–765. [Google Scholar] [CrossRef] [PubMed]
- Carman, D.L.; Browne, R.H.; Birch, J.G. Measurement of Scoliosis and Kyphosis Radiographs. Intraobserver and Interobserver Variation. J. Bone Jt. Surg. 1990, 72, 328–333. [Google Scholar] [CrossRef]
- Facanha-Filho, F.A.; Winter, R.B.; Lonstein, J.E.; Koop, S.; Novacheck, T.; L’Heureux, E.A.; Noren, C.A. Measurement Accuracy in Congenital Scoliosis. J. Bone Jt. Surg. 2001, 83, 42–45. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, M.S.; Poitras, B.; Mayo, N.E.; Labelle, H.; Bourassa, R.; Cloutier, R. Observer Variation in Assessing Spinal Curvature and Skeletal Development in Adolescent Idiopathic Scoliosis. Spine 1988, 13, 1371–1377. [Google Scholar] [CrossRef] [PubMed]
- Gross, C.; Gross, M.; Kuschner, S. Error Analysis of Scoliosis Curvature Measurement. Bull. Hosp. Jt. Dis. Orthop. Inst. 1983, 43, 171–177. [Google Scholar] [PubMed]
- Loder, R.T.; Urquhart, A.; Steen, H.; Graziano, G.; Hensinger, R.N.; Schlesinger, A.; Schork, M.A.; Shyr, Y. Variability in Cobb Angle Measurements in Children with Congenital Scoliosis. J. Bone Jt. Surg. Br. Vol. 1995, 77, 768–770. [Google Scholar] [CrossRef] [Green Version]
- Mok, J.M.; Berven, S.H.; Diab, M.; Hackbarth, M.; Hu, S.S.; Deviren, V. Comparison of Observer Variation in Conventional and Three Digital Radiographic Methods Used in the Evaluation of Patients with Adolescent Idiopathic Scoliosis. Spine 2008, 33, 681–686. [Google Scholar] [CrossRef] [PubMed]
- Morrissy, R.T.; Goldsmith, G.S.; Hall, E.C.; Kehl, D.; Cowie, G.H. Measurement of the Cobb Angle on Radiographs of Patients Who Have Scoliosis. Evaluation of Intrinsic Error. J. Bone Jt. Surg. 1990, 72, 320–327. [Google Scholar] [CrossRef] [Green Version]
- Oda, M.; Rauh, S.; Gregory, P.B.; Silverman, F.N.; Bleck, E.E. The Significance of Roentgenographic Measurement in Scoliosis. J. Pediatr. Orthop. 1982, 2, 378–382. [Google Scholar] [CrossRef] [PubMed]
- Bunnell, W.P. An Objective Criterion for Scoliosis Screening. J. Bone Jt. Surg. 1984, 66, 1381–1387. [Google Scholar] [CrossRef]
- Chowanska, J.; Kotwicki, T.; Rosadzinski, K.; Sliwinski, Z. School Screening for Scoliosis: Can Surface Topography Replace Examination with Scoliometer? Scoliosis 2012, 7, 9. [Google Scholar] [CrossRef] [Green Version]
- Bunnell, W.P. Selective Screening for Scoliosis. Clin. Orthop. Relat. Res. 2005, 40–45. [Google Scholar] [CrossRef]
- Będziński, R. Biomechanika Inżynierska: Zagadnienia Wybrane; Oficyna Wydawnicza Politechniki Wrocławskiej: Wrocław, Poland, 1997; ISBN 83-7085-240-8. [Google Scholar]
- Mrozkowiak, M. Uwarunkowania Wybranych Parametrów Postawy Ciała Dzieci i Młodzieży oraz ich Zmienność w Świetle Mory Projekcyjnej; Oficyna Wydawnicza Uniwersytetu Zielonogórskiego: Zielona Góra, Poland, 2010; ISBN 978-83-7481-350-1. [Google Scholar]
- Schulte, T.L.; Hierholzer, E.; Boerke, A.; Lerner, T.; Liljenqvist, U.; Bullmann, V.; Hackenberg, L. Raster Stereography versus Radiography in the Long-Term Follow-up of Idiopathic Scoliosis. J. Spinal Disord. Tech. 2008, 21, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Harzmann, H.C. Optischer Gipsabdruck Hilft Bei Der Rückenanalyse. Süddeutscher Orthopädenkongress Kongressausgabe 1999, 2, 15. [Google Scholar]
- Harzmann, H.C. Stellenwert Der Videorasterstereographie Als Schulärztliche Screeningmethode von Skoliotischen Fehlhaltungen Und Strukturellen Skoliosen. PhD Thesis, Ludwig-Maximilians-Universität, Medizinischen Fakultät, München, Germany, 2000. [Google Scholar]
- Frerich, J.M.; Hertzler, K.; Knott, P.; Mardjetko, S. Comparison of Radiographic and Surface Topography Measurements in Adolescents with Idiopathic Scoliosis. TOORTHJ 2012, 6, 261–265. [Google Scholar] [CrossRef] [Green Version]
- Kalender, W.A. X-ray Computed Tomography. Phys. Med. Biol. 2006, 51, R29–R43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffman, D.A.; Lonstein, J.E.; Morin, M.M.; Visscher, W.; Harris, B.S.; Boice, J.D. Breast Cancer in Women with Scoliosis Exposed to Multiple Diagnostic x Rays. J. Natl. Cancer Inst. 1989, 81, 1307–1312. [Google Scholar] [CrossRef]
- Kutanzi, K.; Lumen, A.; Koturbash, I.; Miousse, I. Pediatric Exposures to Ionizing Radiation: Carcinogenic Considerations. Int. J. Environ. Res. Public Health 2016, 13, 1057. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- IARC Monographs on the Evaluation of Carcionogenic Risks to Humans. Available online: https://monographs.iarc.who.int/wp-content/uploads/2018/08/14-002.pdf (accessed on 1 December 2021).
- UNSCEAR 2013 Report to the General Assembly with Scientific Annexes Volume II: Scientific Annex B. 283. Available online: https://reliefweb.int/sites/reliefweb.int/files/resources/UNSCEAR_2013_Report_Annex_B_Children.pdf (accessed on 1 December 2021).
- Betsch, M.; Wild, M.; Jungbluth, P.; Thelen, S.; Hakimi, M.; Windolf, J.; Horstmann, T.; Rapp, W. The Rasterstereographic-Dynamic Analysis of Posture in Adolescents Using a Modified Matthiass Test. Eur. Spine J. 2010, 19, 1735–1739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coblentz, A.M.; Herron, R.E. (Eds.) NATO Symposium on Applications of Human Biostereoietrics; Proceedings Volume; Society of Photo-Optical Instrumentation Engineers: Paris, France, 1980; Volume 166. [Google Scholar]
- Frobin, W. Rasterstereography: A Photogrammetric Method for Measurement of Body Surfaces. Photogramm. Eng. Remote. Sens. 1981, 47, 1717–1724. [Google Scholar]
- Hackenberg, L.; Hierholzer, E.; Pötzl, W.; Götze, C.; Liljenqvist, U. Rasterstereographic Back Shape Analysis in Idiopathic Scoliosis after Posterior Correction and Fusion. Clin. Biomech. 2003, 18, 883–889. [Google Scholar] [CrossRef]
- Mangone, M.; Raimondi, P.; Paoloni, M.; Pellanera, S.; Di Michele, A.; Di Renzo, S.; Vanadia, M.; Dimaggio, M.; Murgia, M.; Santilli, V. Vertebral Rotation in Adolescent Idiopathic Scoliosis Calculated by Radiograph and Back Surface Analysis-Based Methods: Correlation between the Raimondi Method and Rasterstereography. Eur. Spine J. 2013, 22, 367–371. [Google Scholar] [CrossRef]
- Schröder, J.; Schaar, H.; Korn, M.; Färber, I.; Ziegler, M.; Braumann, K.M.; Reer, R.; Mattes, K. Zur Sensitivität Und Reproduzierbarkeit Der Pedobarographie Mit Dem System PedoScan. Deutsche Zeitschrift Sportmedizin 2007, 58, 207. [Google Scholar]
- Seiberlich, N.; Gulani, V.; Campbell, A.; Sourbron, S.; Doneva, M.I.; Calamante, F.; Hu, H.H. Quantitative Magnetic Resonance Imaging; Academic Press: Cambridge, MA, USA, 2020; ISBN 978-0-12-817058-8. [Google Scholar]
- Yetişir, F. Local and Global SAR Constrained Large Tip Angle 3D KT-Points Parallel Transmit Pulse Design at 7 T, Massachusetts Institute of Technology: Massachusetts, 2014. Available online: https://dspace.mit.edu/handle/1721.1/87790 (accessed on 1 December 2021).
- Davids, J.R.; Chamberlin, E.; Blackhurst, D.W. Indications for Magnetic Resonance Imaging in Presumed Adolescent Idiopathic Scoliosis. J. Bone Jt. Surg. 2004, 86, 2187–2195. [Google Scholar] [CrossRef] [Green Version]
- Maiocco, B.; Deeney, V.F.; Coulon, R.; Parks, P.F. Adolescent Idiopathic Scoliosis and the Presence of Spinal Cord Abnormalities. Spine 1997, 22, 2537–2541. [Google Scholar] [CrossRef] [PubMed]
- Do, T.M.D.; Fras, C.M.D.; Burke, S.M.D.; Widmann, R.F.M.D.; Rawlins, B.M.D.; Boachie-Adjei, O.M.D. Clinical Value of Routine Preoperative Magnetic Resonance Imaging in Adolescent Idiopathic Scoliosis. J. Bone Jt. Surg. 2001, 83, 577–579. [Google Scholar] [CrossRef] [PubMed]
- Wright, N. Imaging in Scoliosis. Arch. Dis. Child. 2000, 82, 38–40. [Google Scholar] [CrossRef]
- Zhu, C.; Huang, S.; Song, Y.; Liu, H.; Liu, L.; Yang, X.; Zhou, C.; Hu, B.; Chen, H. Surgical Treatment of Scoliosis-Associated with Syringomyelia: The Role of Syrinx Size. Neurol. India 2020, 68, 299. [Google Scholar] [CrossRef]
- Shih, R.Y.; Koeller, K.K. Intramedullary Masses of the Spinal Cord: Radiologic-Pathologic Correlation. RadioGraphics 2020, 40, 1125–1145. [Google Scholar] [CrossRef] [PubMed]
- Bolognese, P.A.; Brodbelt, A.; Bloom, A.B.; Kula, R.W. Chiari I Malformation: Opinions on Diagnostic Trends and Controversies from a Panel of 63 International Experts. World Neurosurg. 2019, 130, e9–e16. [Google Scholar] [CrossRef] [PubMed]
- Rogers, B.P.; Haughton, V.M.; Arfanakis, K.; Meyerand, M.E. Application of Image Registration to Measurement of Intervertebral Rotation in the Lumbar Spine. Magn. Reson. Med. 2002, 48, 1072–1075. [Google Scholar] [CrossRef] [PubMed]
- Rogers, B.; Wiese, S.; Blankenbaker, D.; Meyerand, E.; Haughton, V. Accuracy of an Automated Method to Measure Rotations of Vertebrae from Computerized Tomography Data. Spine 2005, 30, 694–696. [Google Scholar] [CrossRef] [PubMed]
- Carro, P.A. Magnetic Resonance Imaging in Children with Scoliosis. Semin. Musculoskelet. Radiol. 1999, 3, 257–266. [Google Scholar] [CrossRef] [PubMed]
- Heinrich, A.; Reinhold, M.; Güttler, F.V.; Matziolis, G.; Teichgräber, U.K.-M.; Zippelius, T.; Strube, P. MRI Following Scoliosis Surgery? An Analysis of Implant Heating, Displacement, Torque, and Susceptibility Artifacts. Eur. Radiol. 2021, 31, 4298–4307. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, F.U.; Sidani, C.; Fourzali, R.; Wang, M.Y. Postoperative Magnetic Resonance Imaging Artifact with Cobalt-Chromium versus Titanium Spinal Instrumentation. J. Neurosurg. Spine 2013, 19, 629–636. [Google Scholar] [CrossRef] [Green Version]
- Etemadifar, M.R.; Andalib, A.; Rahimian, A.; Nodushan, S.M.H.T. Cobalt Chromium-Titanium Rods versus Titanium-Titanium Rods for Treatment of Adolescent Idiopathic Scoliosis; Which Type of Rod Has Better Postoperative Outcomes? Rev. Assoc. Med. Bras. 2018, 64, 1085–1090. [Google Scholar] [CrossRef] [PubMed]
- Buzug, T.M. Computed Tomography. In Springer Handbook of Medical Technology; Krame, R., Hoffmann, K.P., Pozos, R.S., Eds.; Springer Handbooks; Springer: Berlin/Heidelberg, Germany, 2011. [Google Scholar]
- Brenner, D.J.; Hall, E.J. Computed Tomography--an Increasing Source of Radiation Exposure. N. Engl. J. Med. 2007, 357, 2277–2284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yawn, B.P.; Yawn, R.A.; Hodge, D.; Kurland, M.; Shaughnessy, W.J.; Ilstrup, D.; Jacobsen, S.J. A Population-Based Study of School Scoliosis Screening. JAMA 1999, 282, 1427–1432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, K.; Zhai, X.; Sun, K.; Wang, H.; Yang, C.; Li, M. A Narrative Review of Machine Learning as Promising Revolution in Clinical Practice of Scoliosis. Ann. Transl. Med. 2021, 9, 67. [Google Scholar] [CrossRef]
- Yang, J.; Zhang, K.; Fan, H.; Huang, Z.; Xiang, Y.; Yang, J.; He, L.; Zhang, L.; Yang, Y.; Li, R.; et al. Development and Validation of Deep Learning Algorithms for Scoliosis Screening Using Back Images. Commun. Biol. 2019, 2, 390. [Google Scholar] [CrossRef] [PubMed]
- Pazos, V.; Cheriet, F.; Song, L.; Labelle, H.; Dansereau, J. Accuracy Assessment of Human Trunk Surface 3D Reconstructions from an Optical Digitising System. Med. Biol. Eng. Comput. 2005, 43, 11–15. [Google Scholar] [CrossRef]
- Jaremko, J.L.; Poncet, P.; Ronsky, J.; Harder, J.; Dansereau, J.; Labelle, H.; Zernicke, R.F. Estimation of Spinal Deformity in Scoliosis From Torso Surface Cross Sections. Spine 2001, 26, 1583–1591. [Google Scholar] [CrossRef] [PubMed]
- Komeili, A.; Westover, L.; Parent, E.C.; El-Rich, M.; Adeeb, S. Correlation Between a Novel Surface Topography Asymmetry Analysis and Radiographic Data in Scoliosis. Spine Deform. 2015, 3, 303–311. [Google Scholar] [CrossRef]
- Ramirez, L.; Durdle, N.G.; Raso, V.J.; Hill, D.L. A Support Vector Machines Classifier to Assess the Severity of Idiopathic Scoliosis From Surface Topography. IEEE Trans. Inf. Technol. Biomed. 2006, 10, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Bergeron, C.; Cheriet, F.; Ronsky, J.; Zernicke, R.; Labelle, H. Prediction of Anterior Scoliotic Spinal Curve from Trunk Surface Using Support Vector Regression. Eng. Appl. Artif. Intell. 2005, 18, 973–983. [Google Scholar] [CrossRef]
- Liu, X.C.; Thometz, J.G.; Lyon, R.M.; Klein, J. Functional Classification of Patients with Idiopathic Scoliosis Assessed by the Quantec System. Spine 2001, 26, 1274–1279. [Google Scholar] [CrossRef]
- Zhang, J.; Lou, E.; Hill, D.L.; Raso, J.V.; Wang, Y.; Le, L.H.; Shi, X. Computer-Aided Assessment of Scoliosis on Posteroanterior Radiographs. Med. Biol. Eng. Comput. 2010, 48, 185–195. [Google Scholar] [CrossRef]
- Samuvel, B.; Thomas, V.; Mini, M.G.; Kumar, J.R. A Mask Based Segmentation Algorithm for Automatic Measurement of Cobb Angle from Scoliosis X-ray Image. In Proceedings of the 2012 International Conference on Advances in Computing and Communications, Cochin, India, 9–11 August 2012; IEEE: Piscataway, NJ, USA, 2012; pp. 110–113. [Google Scholar]
- Zhang, J.; Li, H.; Lv, L.; Zhang, Y. Computer-Aided Cobb Measurement Based on Automatic Detection of Vertebral Slopes Using Deep Neural Network. Int. J. Biomed. Imaging 2017, 2017, 9083916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, W.; Liang, J.; Du, Y.; Tan, X.; Xiang, X.; Wang, W.; Ru, N.; Le, J. Reliability and Reproducibility Analysis of the Cobb Angle and Assessing Sagittal Plane by Computer-Assisted and Manual Measurement Tools. BMC Musculoskelet. Disord. 2014, 15, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaw, M.; Adam, C.J.; Izatt, M.T.; Licina, P.; Askin, G.N. Use of the IPhone for Cobb Angle Measurement in Scoliosis. Eur. Spine J. 2012, 21, 1062–1068. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dollár, P.; Appel, R.; Belongie, S.; Perona, P. Fast Feature Pyramids for Object Detection. IEEE Trans. Pattern Anal. Mach. Intell. 2014, 36, 1532–1545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ronneberger, O.; Fischer, P.; Brox, T. U-Net: Convolutional Networks for Biomedical Image Segmentation; Springer: Berlin/Heidelberg, Germany, 2015. [Google Scholar]
- Yongcheng, T.; Nian, W.; Fei, T.; Hemu, C. Automatic Measurement Algorithm of Scoliosis Cobb Angle Based on Deep Learning. J. Phys. Conf. Ser. 2019, 1187, 042100. [Google Scholar] [CrossRef]
- Forsberg, D.; Lundström, C.; Andersson, M.; Vavruch, L.; Tropp, H.; Knutsson, H. Fully Automatic Measurements of Axial Vertebral Rotation for Assessment of Spinal Deformity in Idiopathic Scoliosis. Phys. Med. Biol. 2013, 58, 1775–1787. [Google Scholar] [CrossRef] [Green Version]
- Anitha, H.; Prabhu, G.; Karunakar, A.K. Reliable and Reproducible Classification System for Scoliotic Radiograph Using Image Processing Techniques. J. Med. Syst. 2014, 38, 124. [Google Scholar] [CrossRef]
- Anitha, H.; Prabhu, G.K. Automatic Quantification of Spinal Curvature in Scoliotic Radiograph Using Image Processing. J. Med. Syst. 2012, 36, 1943–1951. [Google Scholar] [CrossRef]
- Sardjono, T.A.; Wilkinson, M.H.F.; Veldhuizen, A.G.; van Ooijen, P.M.A.; Purnama, K.E.; Verkerke, G.J. Automatic Cobb Angle Determination from Radiographic Images. Spine 2013, 38, E1256–E1262. [Google Scholar] [CrossRef] [Green Version]
- Sun, H.; Zhen, X.; Bailey, C.; Rasoulinejad, P.; Yin, Y.; Li, S. Direct Estimation of Spinal Cobb Angles by Structured Multi-Output Regression. In Proceedings of the International Conference on Information Processing in Medical Imaging, Boone, IA, USA, 25–30 June 2017. [Google Scholar]
- Xue, W.; Islam, A.; Bhaduri, M.; Li, S. Direct Multitype Cardiac Indices Estimation via Joint Representation and Regression Learning. IEEE Trans. Med. Imaging 2017, 36, 2057–2067. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, H.; Bailey, C.; Rasoulinejad, P.; Li, S. Automated Comprehensive Adolescent Idiopathic Scoliosis Assessment Using MVC-Net. Med. Image Anal. 2018, 48, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Xu, Q.; Leung, S.; Chung, J.; Chen, B.; Li, S. Accurate Automated Cobb Angles Estimation Using Multi-View Extrapolation Net.Medical Image Analysis. Med. Image Anal. 2019, 58, 101542. [Google Scholar] [CrossRef] [PubMed]
- Choi, R.; Watanabe, K.; Jinguji, H.; Fujita, N.; Ogura, Y.; Demura, S.; Kotani, T.; Wada, K.; Miyazaki, M.; Shigematsu, H.; et al. CNN-Based Spine and Cobb Angle Estimator Using Moire Images. J. Med. Syst. 2017, 5, 135–144. [Google Scholar]
- Choi, R.; Watanabe, K.; Fujita, N.; Ogura, Y.; Matsumoto, M.; Demura, S.; Kotani, T.; Wada, K.; Miyazaki, M.; Shigematsu, H.; et al. Measurement of Vertebral Rotation from Moire Image for Screening of Adolescent Idiopathic Scoliosis. IEEE Trans. Image Electron. Vis. Comput. 2018, 6, 55–64. [Google Scholar]
- Kokabu, T.; Kanai, S.; Kawakami, N.; Uno, K.; Kotani, T.; Suzuki, T.; Tachi, H.; Abe, Y.; Iwasaki, N.; Sudo, H. An Algorithm for Using Deep Learning Convolutional Neural Networks with Three Dimensional Depth Sensor Imaging in Scoliosis Detection. Spine J. 2021, 21, 980–987. [Google Scholar] [CrossRef] [PubMed]
- Sudo, H.; Kokabu, T.; Abe, Y.; Iwata, A.; Yamada, K.; Ito, Y.M.; Iwasaki, N.; Kanai, S. Automated Noninvasive Detection of Idiopathic Scoliosis in Children and Adolescents: A Principle Validation Study. Sci. Rep. 2018, 8, 17714. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Xie, C.; Lin, Y.; Zhou, H.-Y.; Chen, K.; Cheng, D.; Dubost, F.; Collery, B.; Khanal, B.; Khanal, B.; et al. Evaluation and Comparison of Accurate Automated Spinal Curvature Estimation Algorithms with Spinal Anterior-Posterior X-ray Images: The AASCE2019Challenge.Medical Image Analysis (MedIA). Med. Image Anal. 2021, 72, 102115. [Google Scholar] [CrossRef] [PubMed]
- Ayed, I.B.; Punithakumar, K.; Garvin, G.; Romano, W.; Li, S. Graph Cuts with Invariant Object-Interaction Priors: Application to Intervertebral Disc Segmentation. Inf. Process. Med. Imaging 2011, 22, 221–232. [Google Scholar] [PubMed]
- Law, M.W.K.; Garvin, G.; Tummala, S.; Tay, K.; Leung, E.; Li, S. Gradient Competition Anisotropy for Centerline Extraction and Segmentation of Spinal Cords. In Proceedings of the Information Processing in Medical Imaging (IPMI), Asilomar, CA, USA, 28 June–3 July 2013; pp. 49–61. [Google Scholar]
- Law, M.; Tay, K.; Leung, A.; Garvin, G.; Li, S. Intervertebral Disc Segmentation in MR Images using Anisotropic Oriented Flux. Med. Image Anal. 2013, 17, 43–61. [Google Scholar] [CrossRef] [PubMed]
- Miles, B.; Ayed, I.B.; Law, M.; Garvin, G.; Fenster, A.; Li, S. Spine Image Fusion via Graph Cuts. IEEE Trans. Biomed. Eng. (TBME) 2013, 60, 1841–1850. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Zhen, X.; Tay, K.Y.; Osman, S.; Romano, W.; Li, S. Regression Segmentation for M3 Spine Segmentation. IEEE Trans. Med. Imaging 2015, 34, 1640–1648. [Google Scholar] [CrossRef]
- Zheng, G.; Li, S. Medical Image Computing in Diagnosis and Intervention of Spinal Diseases. Comput. Med. Imaging Graph. (CMIG) 2015, 45, 99–101. [Google Scholar] [CrossRef] [PubMed]
- He, X.; Chong, J.; Osman, S.; Sharma, M.; Landis, M.; Li, S. Automated Delineation of Neural Foramina from Spine Images. In Proceedings of the Annual Meeting of Radiological Society of North America (RSNA), Chicago, IL, USA, 29 November–4 December 2015. [Google Scholar]
- Yao, J.; Burns, J.E.; Forsberg, D.; Seitel, A.; Rasoulian, A.; Abolmaesumi, P.; Hammernik, K.; Urschler, M.; Ibragimov, B.; RobertKorez, T.V.; et al. A Multi-center Milestone Study of ClinicalVertebral CT Segmentation. Comput. Med. Imaging Graph. 2016, 49, 16–28. [Google Scholar] [CrossRef] [Green Version]
- Cai, Y.; Laidley, D.; Kornecki, A.; Shmuilovich, O.; Lum, A.; Li, S. Multi-Modal Vertebrae Recognition Using Transformed Deep Convolution Net-Work. Comput. Med. Imaging Graph. 2016, 51, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Miles, B.; Ayed, I.B.; Hojjat, P.; Wang, M.; Fenster, A.; Li, S.; Garvin, G. Spine Labeling in Axial Magnetic Resonance Imaging ViaIntegral Kernels. Comput. Med. Imaging Graph. 2017, 54, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Tam, C.; He, X.; Sharma, M.; Mercado, A.; Landis, M.; Li, S. Automated Multi-Vertebrae and Disc Delineation for MR and CT Spinal Images. In Proceedings of the Annual Meeting of Radiological Society of North America (RSNA), Chicago, IL, USA, 26 November–1 December 2017. [Google Scholar]
- Zheng, G.; Chu, C.; Ibragimov, B.; Korez, R.; Vrtovec, T.; Hugo-Hutt, R.E.; Meakin, J.; Andrade, I.L.; Glocker, B.; HaoChen, Q.D.; et al. Evaluation and Comparison of 3D Intervertebral Disc Localization and SegmentationMethods for 3D T2 MR Data: A Grand Challenge. Med. Image Anal. 2017, 35, 327–344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, H.; Bailey, C.; Rasoulinejad, P.; Li, S. Automatic Landmark Estimation for Adolescent Idiopathic Scoliosis Assessment Using BoostNet. In International Conference on Medical Image Computing and Computer-Assisted Intervention; Springer: Cham, Switzerland, 2017. [Google Scholar] [CrossRef]
- Cai, Y.; Leung, S.; Warrington, J.; Pandey, S.; Shmuilovich, O.; Li, S. Direct Spondylolysis Identification and Spondylolisthesis Measurement in MR/CT Using Detectors Trained by Articulated Parameterized Spine Model. In Proceedings of the SPIE Conference on Medical Imaging, Orlando, FL, USA, 11–16 February 2017. [Google Scholar]
- Cai, Y.; Lum, A.; Mercado, A.; Landis, M.; Warrington, J.; Li, S. Unsupervised Shape Discovery Using Synchronized Spectral Networks. Pattern Recognit. 2017, 69, 39–51. [Google Scholar] [CrossRef]
- He, X.; Lum, A.; Sharma, M.; Shmuilovich, O.; Brahm, G.; Li, S. First Computer-Aided Diagnosis of Neural Foramina Stenosis. In Proceedings of the Annual Meeting of Radiological Society of North America (RSNA), Chicago, IL, USA, 26–30 December 2016. [Google Scholar]
- He, X.; Lum, A.; Mercado, A.; Landis, M.; Warrington, J.; Li, S. Automated Grading of Lumbar Disc Degeneration via Supervised-Distance Metric Learning. In Proceedings of the SPIE Medical Imaging, Orlando, FL, USA, 11–16 February 2017. [Google Scholar]
- Pang, S.; Feng, Q.; Leung, S.; Nachum, I.B.; Li, S. Direct Automated Quantitative Measurement of Spine via Cascade Amplifier Regression Network. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Granada, Spain, 16–20 September 2018. [Google Scholar]
- Huang, J.; Shen, H.; Chen, B.; Wang, Y.; Li, S. Segmentation of Paraspinal Muscles at Varied Lumbar Spinal Levels by Explicit Saliency-Aware Learning. In Proceedings of the 23rd International Conference on Medical Image Computing and Computer Assisted Intervention (MICCA)I, Lima, Peru, 4–8 October 2020. [Google Scholar]
- Han, Z.; Wei, B.; Mercado, A.; Leung, S.; Li, S. Spine-GAN: Semantic Segmentation of Multiple Spinal Structures. Med. Image Anal. 2018, 50, 23–35. [Google Scholar] [CrossRef]
- Chang, H.; Zhao, S.; Zheng, H.; Li, S. Multi-Vertebrae Segmentation from Arbitrary Spine MRI Images under Global View. In Proceedings of the 23rd International Conference on Medical Image Computing and Computer Assisted Intervention (MICCAI), Lima, Peru, 4–8 October 2020. [Google Scholar]
- Zhang, R.; Xiao, X.; Liu, Z.; Li, Y.; Li, S. Multi-Task Relational Learning Network for MRI Vertebral Localization, Identification and Segmentation. IEEE J. Biomed. Health Inform. 2020, 24, 2902–2911. [Google Scholar] [CrossRef]
- Lin, L.; Tao, X.; Pang, S.; Su, Z.; Lu, H.; Li, S.; Feng, Q.; Chen, B. Multiple Axial Spine Indices Estimation via Dense Enhancing Network with Cross-Space Distance-Preserving Regularization. IEEE J. Biomed. Health Inform. 2020, 24, 3248–3257. [Google Scholar] [CrossRef] [PubMed]
- Hong, Y.; Wei, B.; Han, Z.; Li, X.; Zheng, Y.; Li, S. MMCL-Net: Spinal Disease Diagnosis in Global Mode Using Progressive Multi-Task Joint Learning. Neurocomputing 2020, 399, 307–316. [Google Scholar] [CrossRef]
- Zhang, D.; Chen, B.; Li, S. Sequential Conditional ReinforcementLearning for Simultaneous Vertebral Body Detection and Segmentation with Modeling the Spine Anatomy. Med. Image Anal. 2020, 67, 101861. [Google Scholar] [CrossRef] [PubMed]
- Han, Z.; Wei, B.; Chen, B.; Yin, Y.; Li, S. Unifying Neural Learning and Symbolic Reasoning for Spinal Medical Report Generation. Med. Image Anal. 2021, 67. [Google Scholar] [CrossRef]
- Lin, L.; Tao, X.; Yang, W.; Pang, S.; Su, Z.; Lu, H.; Li, S.; Qianjin, F.; Chen, B. Quantifying Axial Spine Images Using Object-Specific Bi-Path Network. IEEE J. Biomed. Health Inform. 2021, 25, 2978–2987. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Lin, A.; Tay, K.Y.; Romano, W.; Osman, S. Prognosis of Intervertebral Disc Loss from Diagnosis of Degenerative Disc Disease. In Proceedings of the SPIE Medical Imaging, Orlando, FL, USA, 22 February 2015; Volume 9414. [Google Scholar]
- Han, Z.; Wei, B.; Leung, S.; Chung, J.; Li, S. Towards Automatic Report Generation in Spine Radiology Using Weakly Supervised Framework. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Granada, Spain, 16–20 September 2018. [Google Scholar]
- Zhao, S.; Wu, X.; Chen, B.; Li, S. Automatic Spondylolisthesis Gradingfrom MRIs across Modalities Using Faster Adversarial Recognition Network. Med. Image Anal. 2019, 58, 101533. [Google Scholar] [CrossRef] [PubMed]
- Zhao, S.; Wu, X.; Chen, B.; Li, S. Automatic Vertebrae Recognition from Arbitrary Spine MRI Images by a Category Consistent Self-Calibration Detection Framework. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Shenzhen, China, 13–17 October 2019. [Google Scholar]
- Zhao, S.; Chen, B.; Chang, H.; Wu, X.; Li, S. Discriminative Dictionary-Embedded Network for Comprehensive Vertebrae Tumor Diagnosis. In Proceedings of the 23rd International Conference on Medical Image Computing and Computer Assisted Intervention (MICCAI), Lima, Peru, 4–8 October 2020. [Google Scholar]
- Vrtovec, T.; Pernuš, F.; Likar, B. A Review of Methods for Quantitative Evaluation of Spinal Curvature. Eur. Spine J. 2009, 18, 593–607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patias, P.; Grivas, T.B.; Kaspiris, A.; Aggouris, C.; Drakoutos, E. A Review of the Trunk Surface Metrics Used as Scoliosis and Other Deformities Evaluation Indices. Scoliosis 2010, 5, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| Study/ Number of Data | Algorithms Applied | Objectives | Outcome Presentation |
|---|---|---|---|
| Liansheng W. [93] 707 spinal AP X-ray images | U-net | Top eight methods from twelve teams (including intuition, workflow, and implementation). Experimental results show that, overall, the best performing method achieved an asymmetric mean absolute percentage (SMAPE) of 21.7%. | Quantitative measurement of the spine. |
| Liyan L. [116] 895 axial spine MRI images from 143 patients | OSBP-Net, IPDC, and IICR | Applied to the output of the SFEs, taking into account that the activated regions in the feature maps of two paths should be theoretically different. | The prediction results, comparison with many other CADq models |
| Shen Z. [123] 450 MRI scans | Can-See is a two-step detection framework:
| Category-consistent self-calibration recognition system (Can-See) used to accurately classify the labels and precisely predict the bounding boxes of all vertebrae with improved discriminative capabilities for vertebrae categories and self-awareness of false-positive detections. | Can-See achieves high performance (testing accuracy reaches 0.955) and outperforms other state-of-the-art methods. |
| Zhongyi H. [113] 253 clinical patients | Neural-symbolic learning (NSL) framework | Compares the semantic segmentation ability of a neural symbolic learning framework (NSL) with several state-of-the-art semantic segmentation networks (FCN, SegNet, DeepLabV3+, U-Net, Spine-GAN, GN-SGR, AGN-SGR, and AGN-DN). | NSL can directly generate radiologist-level diagnosis reports (using two steps) in spine radiology. |
| Dong Z. [118] 240 subjects | Sequential conditional reinforcement learning (SCRL). SCRL coordinates three major components (AMRL, Y-Net and FC-ResNet) | Propose a sequential conditional reinforcement learning network (SCRL) to tackle the simultaneous detection and segmentation of VBs from MR spine images. | SCRL achieves accurate detection and segmentation results, where on average, the detection IoU is 92.3%, segmentation dice is 92.6%, and classification mean accuracy is 96.4%. |
| Yanfei H. [117] 200 subjects | MMCL-Net:
| Novel end-to-end multi-task multi-structure correlation learning network (MMCL-Net) for the detection, segmentation and classification (normal, slight, marked and severe) of three types of spine structure: disc, vertebra and neural foramen simultaneously | MMCL-Net achieves high performance with a mAP of 0.9187, a classification accuracy of 90.67%, and a dice coefficient of 90.60%. |
| Liyan L. [116] 895 axial spine MRI images from 143 subjects | Dense enhancing network (DE-Net) | Dense enhancing network (DE-Net), which uses the dense enhancing blocks (DEBs) as its main body. | All deep learning models obtain very small prediction errors, and the proposed DE-Net with CSDPR acquires the smallest error among all methods. |
| Ranran Z. [115] 407 subjects | Multi-task relational learning network (MRLN) | A dilation convolution group is used to expand the receptive field, and LSTM (long short-term memory) to learn the prior knowledge of the order relationship between the vertebral bodies. | The accurate segmentation, localization and identification of vertebrae. |
| Jiawei H. [112] 320 axial lumbar MRIs | BS-ESNet | For the first time:
| Proposal an explicit saliency-aware learning framework for segmentation of paraspinal muscles at varied spine levels. |
| Heyou Ch. [114] 292 MRI scans | A spatial graph convolutional network (GCN) | The proposed method is trained in an end-to-end. | Method achieves high performance (89.28 ± 5.21) of IDR and (85.37 ± 4.09%) of mIoU) from arbitrary input images. |
| Shen Z. [124] none | Adversarial recognition (FAR) network | Network to accurately perform spondylolisthesis grading by excellently detecting critical vertebrae without the need for locating landmarks. | Training accuracy: 0.9883 ± 0.0094, testing accuracy: 0.8933 ± 0.0276 for MRI images of different modalities, which can be attributed to the excellent critical vertebrae detection (detection mAP75 for training: 1 ± 0, for testing: 0.9636 ± 0.0180, and IoU (intersection-over-union) ≥ 0.9/0.8 for most detections with their corresponding ground truth in the training/testing dataset). |
| Liansheng W. [88] 526 X-rays | MVE-Net | Proposed multi-view extrapolation net (MVE-Net) that provides accurate automated scoliosis estimation in multi-view (both AP and LAT) X-rays. | Experimental results on 526 X-rays show 7.81 and 6.26 circular mean absolute error in AP and LAT angle estimation, which shows the MVE-Net provides an accurate Cobb angle estimation in multi-view X-rays |
| Shen Z. [123] none | Faster adversarial recognition (FAR) | Proposed faster adversarial recognition (FAR) network to accurately perform spondylolisthesis grading by excellently detecting critical vertebrae without the need for locating landmarks. | training accuracy: 0.9883 ± 0.0094, testing accuracy: 0.8933 ± 0.0276 for MRI images of different modalities, which can be attributed to the excellent critical vertebrae detection (detection mAP75 for training: 1 ± 0, for testing: 0.9636 ± 0.0180, and IoU (intersection-over-union) ≥ 0.9/0.8 for most detections with their corresponding ground truth in the training/testing dataset). |
| Shumao P. [111] MR images of 215 subjects | Cascade amplifier regression network (CARN) | Proposed novel cascade amplifier regression network (CARN) with manifold regularization including local structure-preserved manifold regularization (LSPMR) and adaptive local shape-constrained manifold regularization (ALSCMR) to achieve accurate direct automated multiple indices estimation. | Proposed approach achieves impressive performance with mean absolute errors of 1.22±1.04 mm and 1.24 ± 1.07 mm for the estimation of 30 lumbar spinal indices of the T1-weighted and T2-weighted spinal MR images, respectively. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karpiel, I.; Ziębiński, A.; Kluszczyński, M.; Feige, D. A Survey of Methods and Technologies Used for Diagnosis of Scoliosis. Sensors 2021, 21, 8410. https://doi.org/10.3390/s21248410
Karpiel I, Ziębiński A, Kluszczyński M, Feige D. A Survey of Methods and Technologies Used for Diagnosis of Scoliosis. Sensors. 2021; 21(24):8410. https://doi.org/10.3390/s21248410
Chicago/Turabian StyleKarpiel, Ilona, Adam Ziębiński, Marek Kluszczyński, and Daniel Feige. 2021. "A Survey of Methods and Technologies Used for Diagnosis of Scoliosis" Sensors 21, no. 24: 8410. https://doi.org/10.3390/s21248410
APA StyleKarpiel, I., Ziębiński, A., Kluszczyński, M., & Feige, D. (2021). A Survey of Methods and Technologies Used for Diagnosis of Scoliosis. Sensors, 21(24), 8410. https://doi.org/10.3390/s21248410