
Smart Homes as Enablers for Depression Pre-Diagnosis Using PHQ-9 on HMI through Fuzzy Logic Decision System

 , ,
, ,  ,
,  ,
, 
Abstract
:1. Introduction
2. Literature Review
2.1. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5)
2.2. Patient Health Questionnaire 9 (PHQ-9)
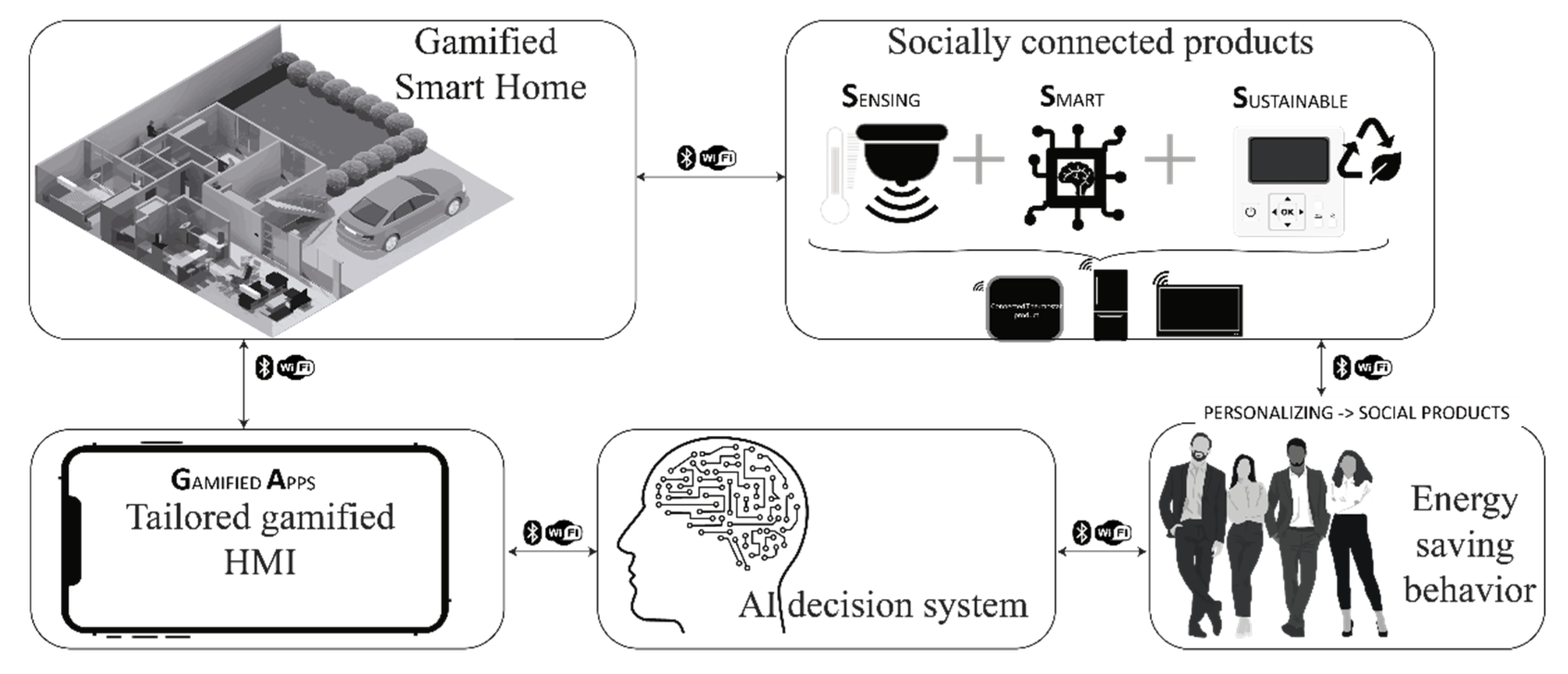
2.3. Smart Homes
- Surveillance home: Householders receive alerts about possible natural disasters or security interventions. Besides, the SH gathers data from the environment to detect burglary threats.
- Assistive home: This home type promotes the householders’ well-being through action recognition. Hence, three types of services are offered:
- Senior oriented
- Child oriented
- Overall health-oriented
- Detection and multimedia home: This home type detects and collects information from videos and photos of householders’ daily lives.
- Ecological awareness home: Householders monitor and control their energy supply against demand through special sensors and automatic monitoring systems. Thus, this home type promotes environmental sustainability.
- Smart Home Energy Management Systems have advanced IoT devices to convert a traditional home into an energy-aware home to reduce energy consumption and promote money savings [36].
Fuzzy Logic and Smart Homes for Detection of Depressive Disorders
2.4. Gamification for Treatment Depression
- What characteristics should an HMI framework consider helping the healthcare workers pre-diagnose depression using SHs as enablers?
3. Material and Methods
- The statistical analysis and data cleaning considered the SPSS v. 25 and R-studio v. 1.4.1106.
- The fuzzy logic decision systems used LabVIEW v. 20.0.1.
- Demographic characteristics of the sample (mean age, male and female proportion, and median PHQ9 scores), for normally distributed data, the mean and standard deviation were reported. The median and interquartile range were reported for non-normally distributed data.
- Setting the normal, expected, and abnormal depression thresholds for each age group, by obtaining the 3, 25, 50, 75, and 97 percentiles.
- The associations between age group and depression severity and sex and depression severity were determined. These associations were achieved with a frequency table and a chi-squared analysis; if the chi-squared analysis was found significant, a Crammer’s V was performed to obtain the strength of the association. Furthermore, a Spearman’s correlation test was performed between age and PHQ9 score.
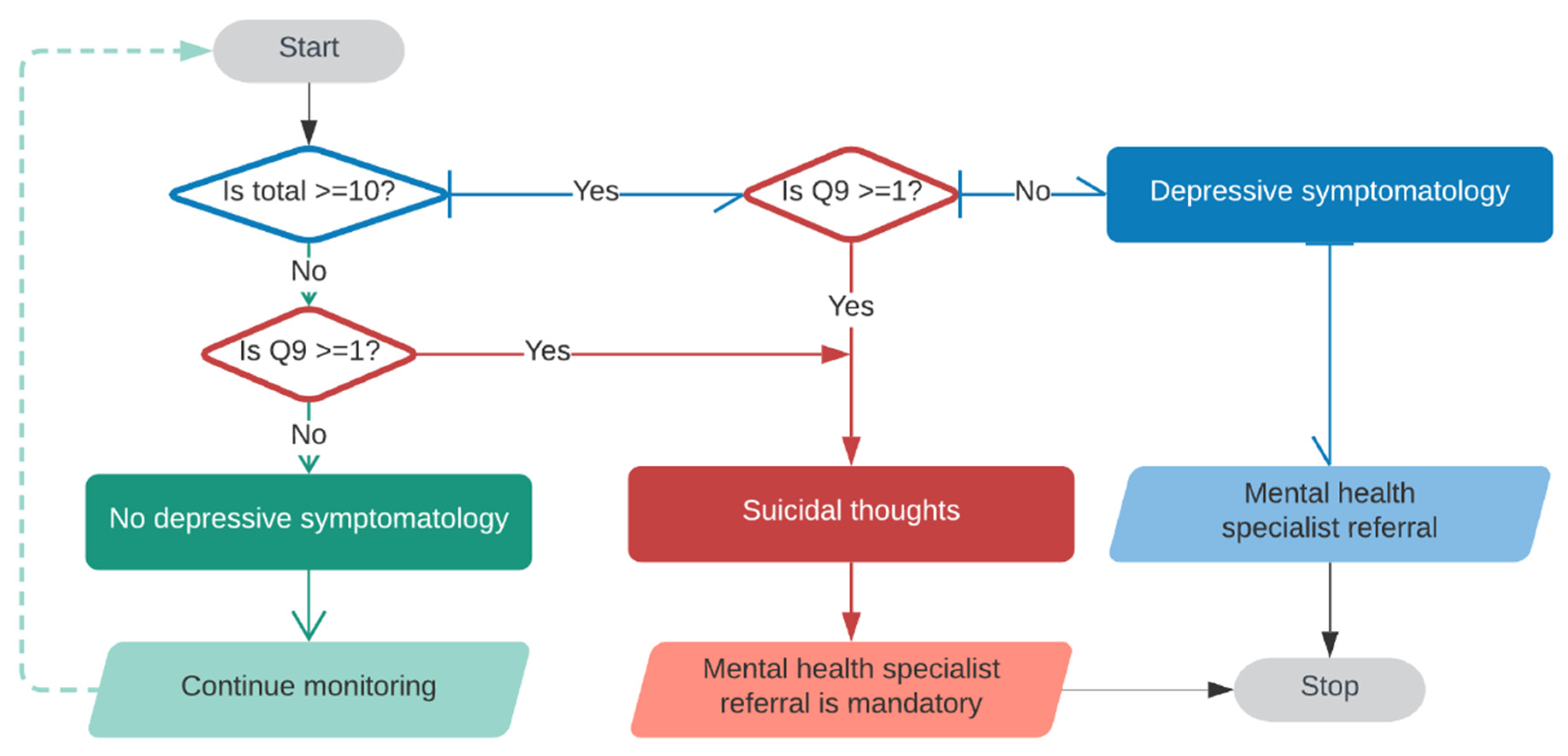
- Items 1, 2, and 9 are crucial, because according to DSM, to make a depression diagnosis, 4 of the nine questions have to be positive, and at least one of the five must be items 1 or 2 [25,28]. Moreover, if item 9 is positive, the psychological referral is mandatory. In order to assess the distribution and association of these items in the different age groups and sex, frequency tables and chi-squared tests were performed with Crammer’s V test whenever it applied.
- p-values below 0.05 were considered statistically significant.
- Cramer’s V results were interpreted as follows: 0.0–0.1 negligible; 0.1–0.2 weak; 0.2–0.4 moderate; 0.4–0.6 relatively strong; 0.6–0.8 strong; 0.8–1.0 very strong [63].
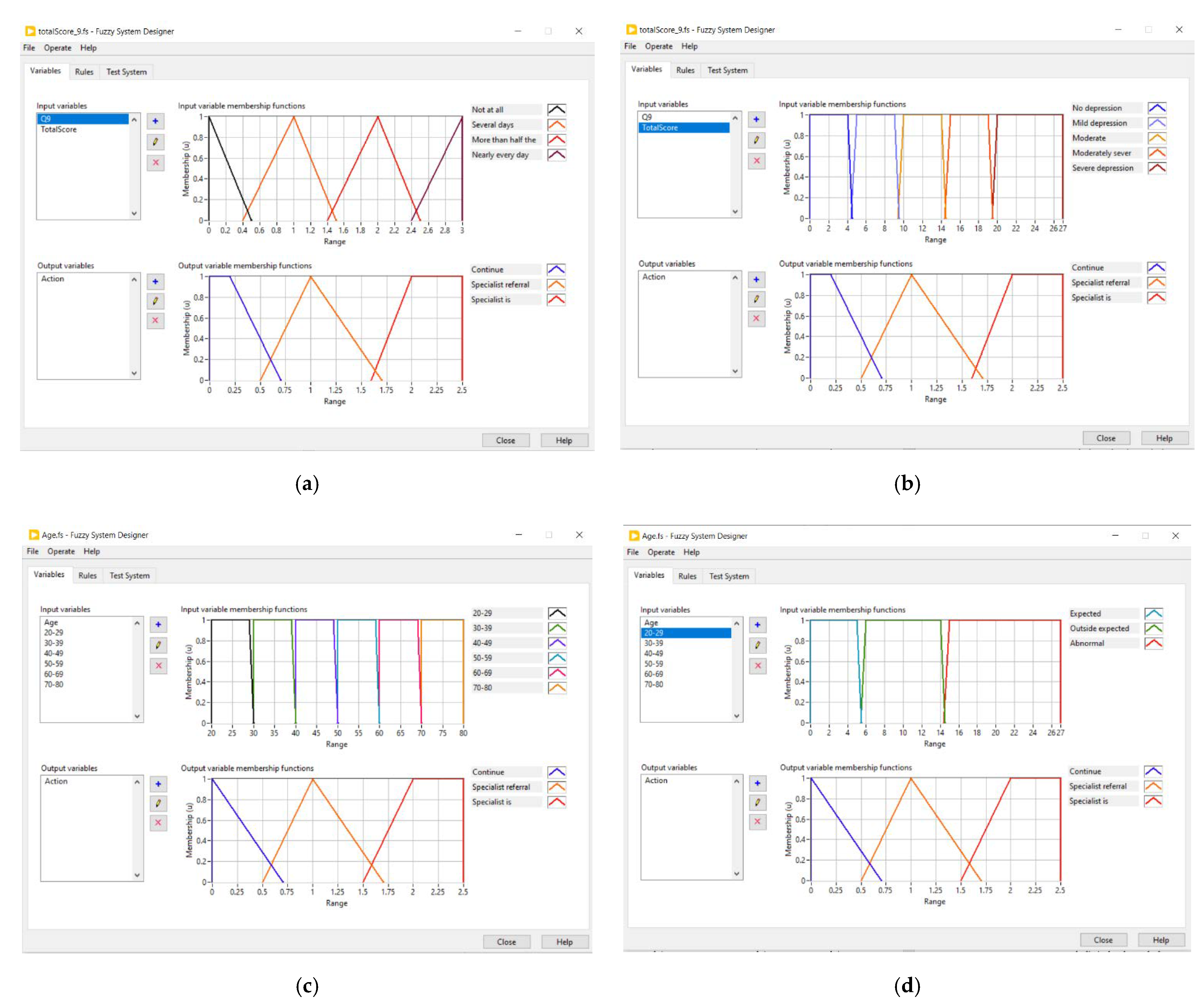
3.1. Fuzzy Logic Decision System
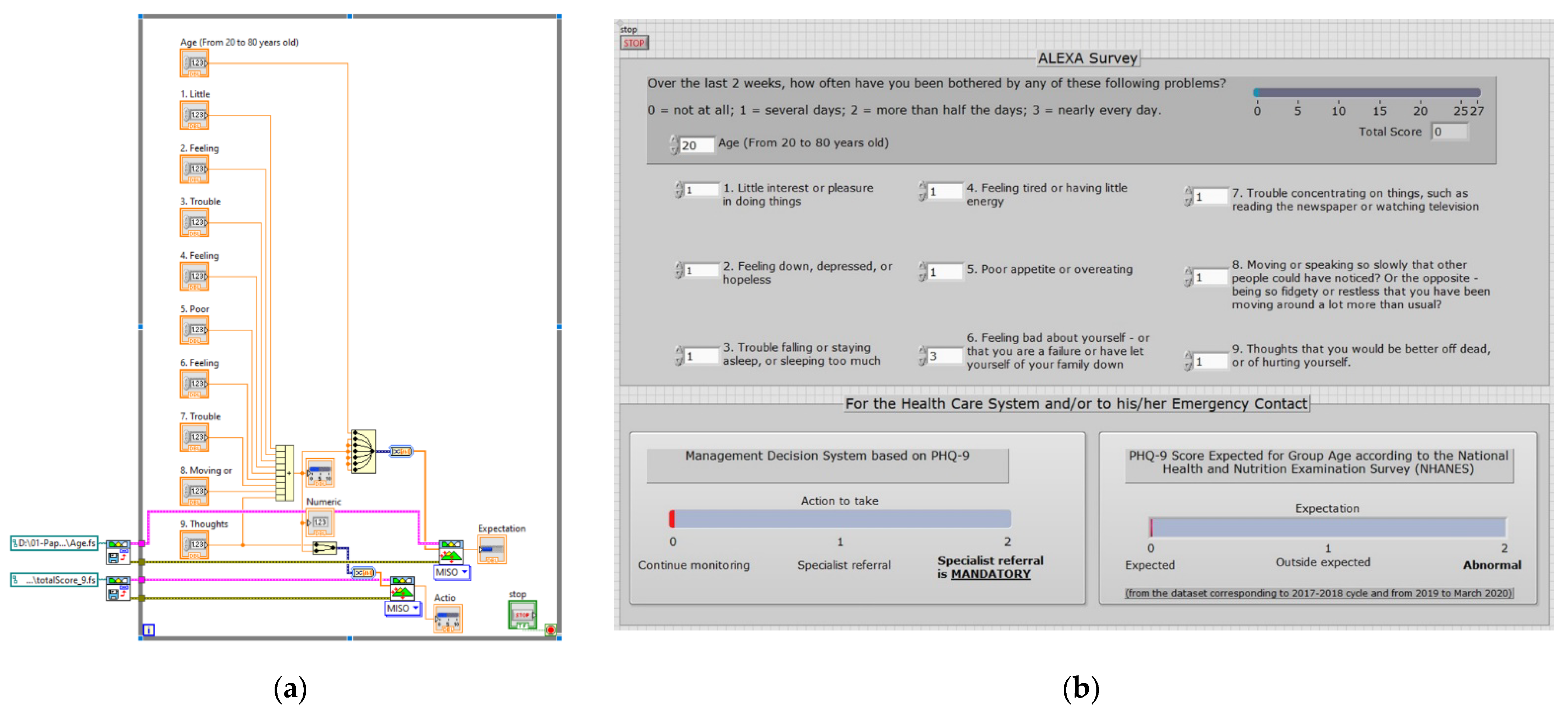
3.2. Human Machine Interface
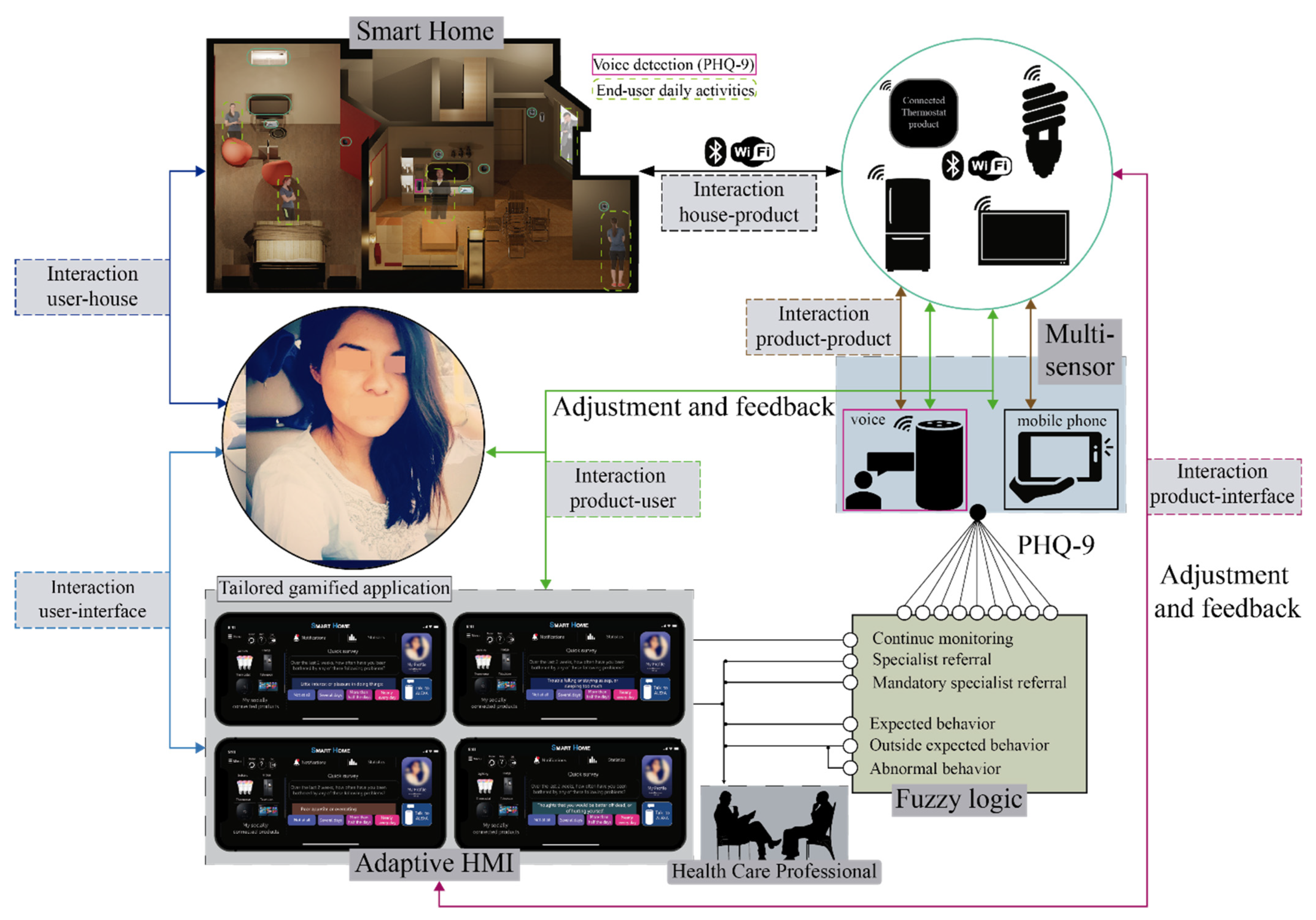
4. Proposed Framework
5. Results
5.1. Knowledge Base Step: Statistical Analysis
5.2. Fuzzy Logic Decision System Step
5.3. Evaluation Step
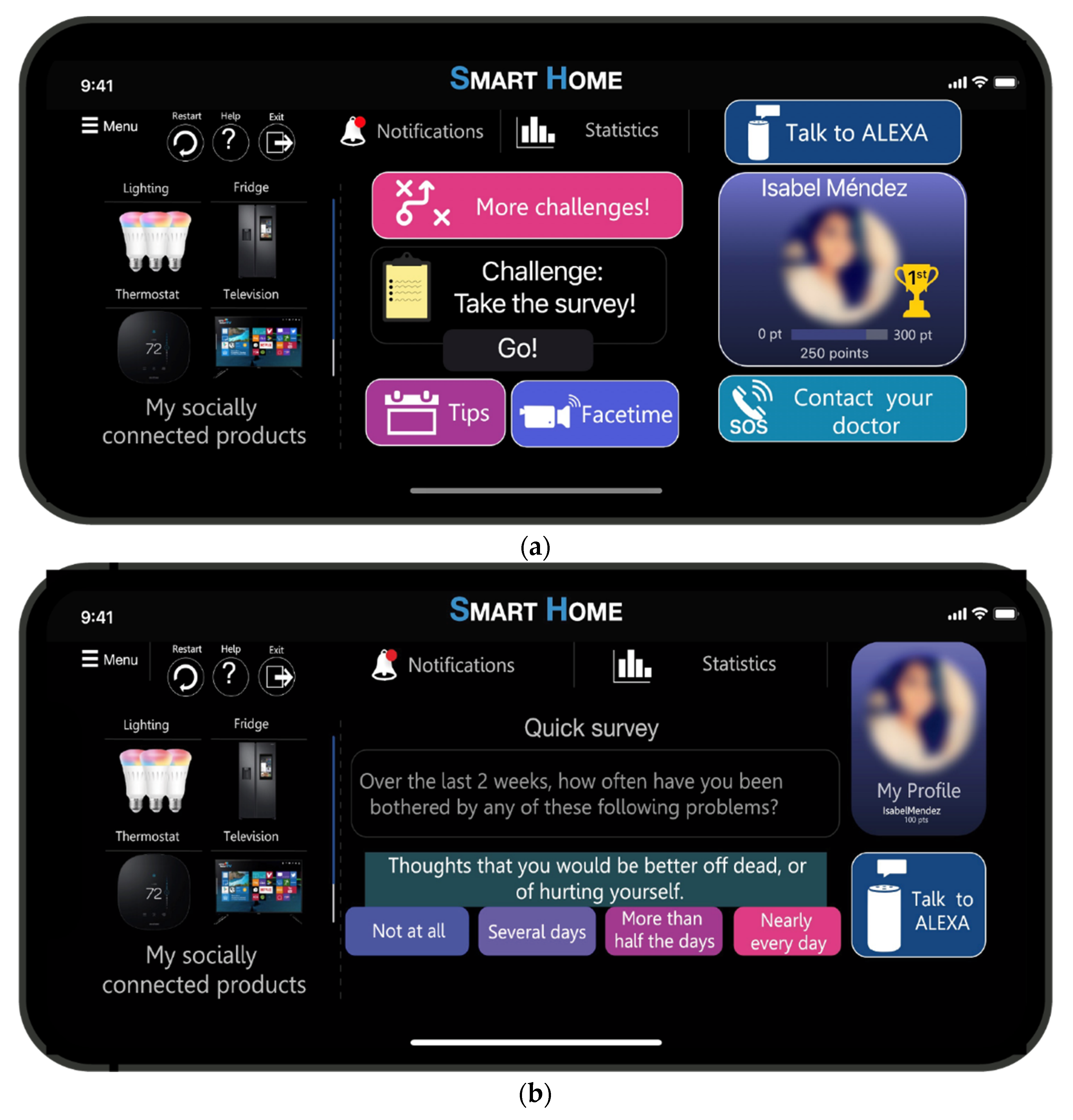
5.4. Human Machine Interface in a Smart Home Context
6. Discussion
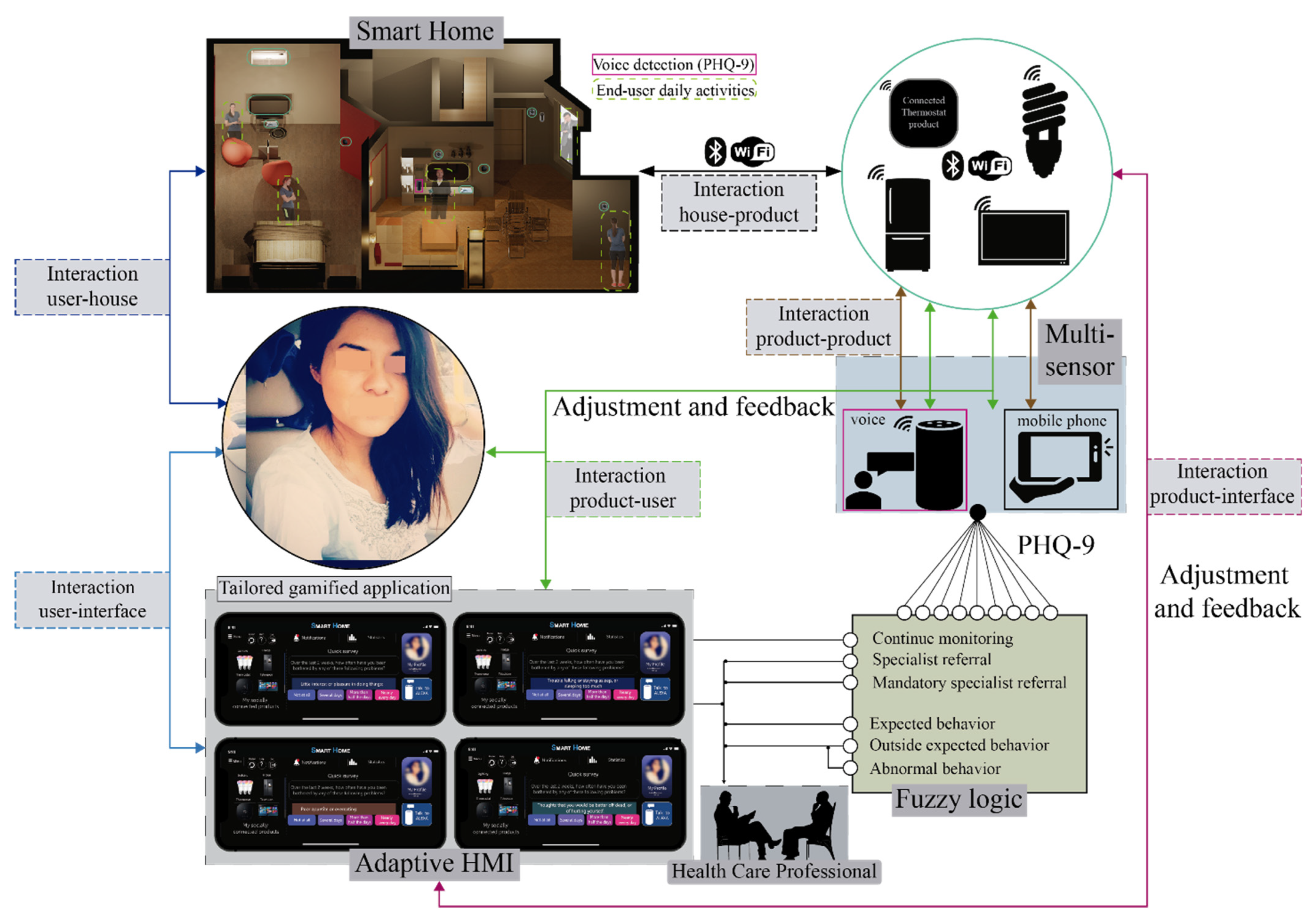
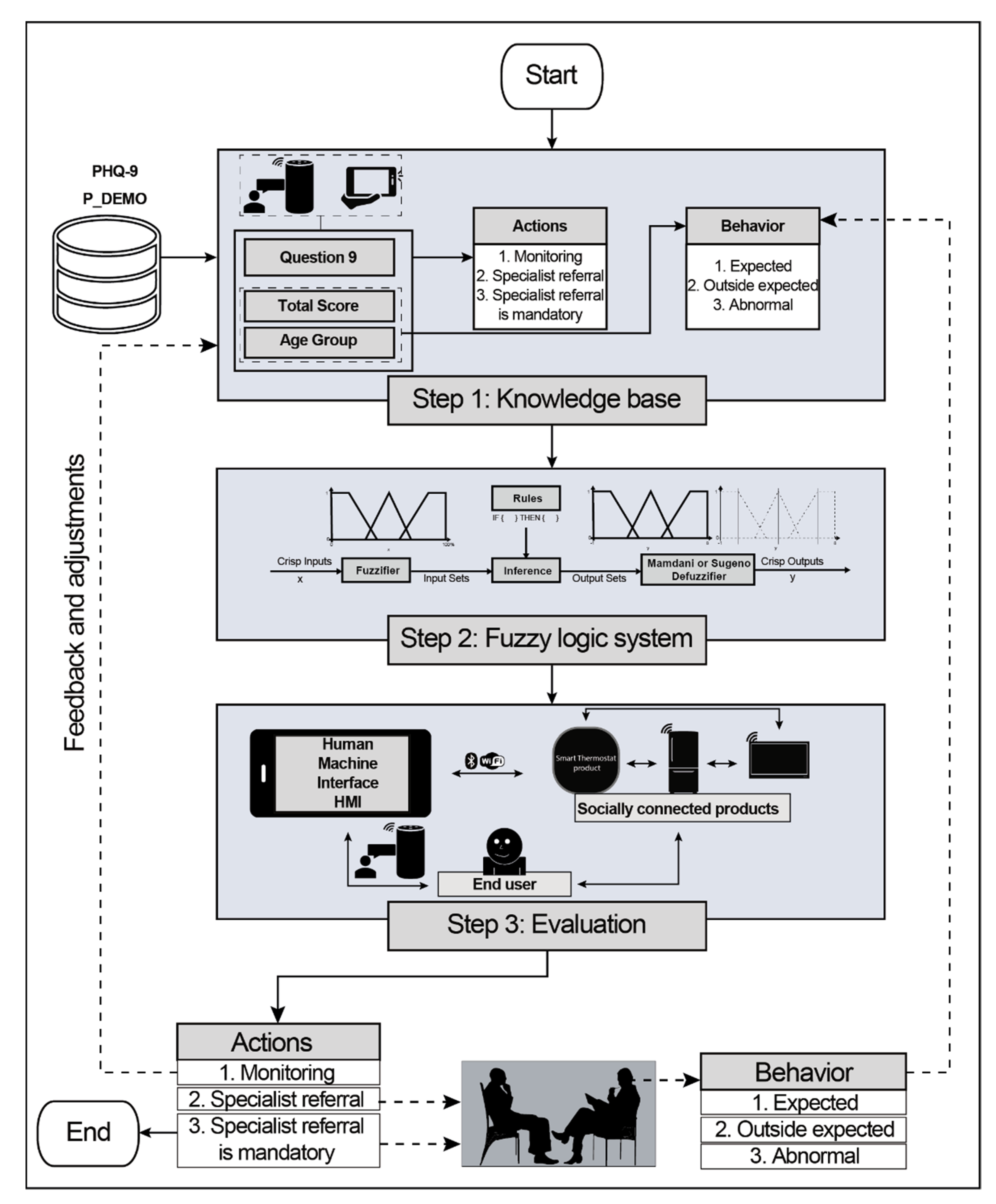
- A knowledge base gathers the population with depression symptomatology through available PHQ-9 answers to relate them with the proposal and identify if the householder is within the range of expected depression or requires more attention. During this step, the most common gamification elements for depression are collected.
- A fuzzy logic step that helps as a decision system triggers three actions: continue monitoring, specialist referral, and specialist referral is mandatory. Furthermore, three expected behaviors are analyzed: expected, outside expected, or abnormal behavior.
- The evaluation step assesses the interaction between the householder and depression by taking advantage of household appliances through gamified interfaces. The interface uses gamification elements to help as an enabler for helping in the pre-diagnosis of depression. The elements are divided into extrinsic and intrinsic. Moreover, this pre-diagnosis runs into a feedback and adjustment environment; hence, the householder receives points by answering the survey, contacting the doctor, and interacting with ALEXA or through video call. In [20], it is proposed to use video callings as social connectors to avoid social isolation or depression.
7. Conclusions
- Evaluate and improve the proposed application with different scenarios and target populations. For instance, there are sectors with chronic diseases such as rheumatoid arthritis that commonly have depression. With this proposal, evaluate their performance through their treatment to analyze if this proposal helps in improving their depression symptomatology. Besides, the proposal should be evaluated outside controlled environments and in several countries in which any cultural factor needs to consider the framework.
- Update the framework and HMI by including SWRL technologies as they have more robust rules than FL. However, this research did not propose SWRL or SWRL-F because the objective was to generate a conventional knowledge base. Afterward, future work will explore the use of these rules, and their optimization will be evaluated.
- Submit this proposal into medical protocols to assess the system in a pilot study with real users.
- Include, if possible, the camera tracking to develop facial recognition and compare the answers with the camera feedback.
- Employ ALEXA in combination with cameras or other household appliances to analyze householders’ patterns and compare their behavioral patterns with their survey answers. For example, the perception of depression is important. Thus, if the end-user is feeling depressed, but the actions reflect the opposite, a message could be displayed through the gamified interfaces. Moreover, ALEXA could talk to the householders and explain how they have been acting to cheer them up.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Depression. Available online: https://www.who.int/news-room/fact-sheets/detail/depression (accessed on 14 October 2021).
- Daly, M.; Sutin, A.R.; Robinson, E. Depression Reported by US Adults in 2017–2018 and March and April 2020. J. Affect. Disord. 2021, 278, 131–135. [Google Scholar] [CrossRef] [PubMed]
- NHANES 2017-March 2020 Pre-Pandemic Questionnaire Data. Available online: https://wwwn.cdc.gov/nchs/nhanes/search/datapage.aspx?Component=Questionnaire&Cycle=2017-2020 (accessed on 13 October 2021).
- Spitzer, R.L.; Williams, J.B.W.; Kroenke, K. Test Review: Patient Health Questionnaire–9 (PHQ-9). Rehabil. Couns. Bull. 2014, 57, 246–248. [Google Scholar] [CrossRef]
- Narziev, N.; Goh, H.; Toshnazarov, K.; Lee, S.A.; Chung, K.-M.; Noh, Y. STDD: Short-Term Depression Detection with Passive Sensing. Sensors 2020, 20, 1396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torous, J.; Staples, P.; Shanahan, M.; Lin, C.; Peck, P.; Keshavan, M.; Onnela, J.-P. Utilizing a Personal Smartphone Custom App to Assess the Patient Health Questionnaire-9 (PHQ-9) Depressive Symptoms in Patients with Major Depressive Disorder. JMIR Ment. Health 2015, 2, e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hickey, B.A.; Chalmers, T.; Newton, P.; Lin, C.-T.; Sibbritt, D.; McLachlan, C.S.; Clifton-Bligh, R.; Morley, J.; Lal, S. Smart Devices and Wearable Technologies to Detect and Monitor Mental Health Conditions and Stress: A Systematic Review. Sensors 2021, 21, 3461. [Google Scholar] [CrossRef] [PubMed]
- Malwade, S.; Abdul, S.S.; Uddin, M.; Nursetyo, A.A.; Fernandez-Luque, L.; Zhu, X.; Cilliers, L.; Wong, C.-P.; Bamidis, P.; Li, Y.-C. (Jack) Mobile and Wearable Technologies in Healthcare for the Ageing Population. Comput. Methods Programs Biomed. 2018, 161, 233–237. [Google Scholar] [CrossRef] [PubMed]
- Avila, M.; Méndez, J.I.; Ponce, P.; Peffer, T.; Meier, A.; Molina, A. Energy Management System Based on a Gamified Application for Households. Energies 2021, 14, 3445. [Google Scholar] [CrossRef]
- Marikyan, D.; Papagiannidis, S.; Alamanos, E. A Systematic Review of the Smart Home Literature: A User Perspective. Technol. Forecast. Soc. Chang. 2019, 138, 139–154. [Google Scholar] [CrossRef]
- Harper, R. (Ed.) Inside the Smart Home; Springer: London, UK, 2003; ISBN 978-1-85233-688-2. [Google Scholar]
- Aldrich, F.K. Smart Homes: Past, Present and Future. In Inside the Smart Home; Harper, R., Ed.; Springer: London, UK, 2003; pp. 17–39. ISBN 978-1-85233-688-2. [Google Scholar]
- Fulmer, R.; Joerin, A.; Gentile, B.; Lakerink, L.; Rauws, M. Using Psychological Artificial Intelligence (Tess) to Relieve Symptoms of Depression and Anxiety: Randomized Controlled Trial. JMIR Ment. Health 2018, 5, e64. [Google Scholar] [CrossRef] [PubMed]
- Robinson, A. Can a Chatbot Help My Mental Health? Available online: https://onemindpsyberguide.org/blog/can-a-chatbot-help-my-mental-health/ (accessed on 14 October 2021).
- Quiroz, J.C.; Bongolan, T.; Ijaz, K. Alexa Depression and Anxiety Self-Tests: A Preliminary Analysis of User Experience and Trust. In Proceedings of the Adjunct Proceedings of the 2020 ACM International Joint Conference on Pervasive and Ubiquitous Computing and Proceedings of the 2020 ACM International Symposium on Wearable Computers, ACM: Virtual Event Mexico, 10 September 2020; pp. 494–496. Available online: https://dl.acm.org/doi/abs/10.1145/3410530.3414374 (accessed on 12 November 2021).
- Brenner, M.H.; Bhugra, D. Acceleration of Anxiety, Depression, and Suicide: Secondary Effects of Economic Disruption Related to COVID-19. Front. Psychiatry 2020, 11, 592467. [Google Scholar] [CrossRef] [PubMed]
- Lii Inn, T. Smart City Technologies Take on COVID-19–Penang Institute. Available online: https://penanginstitute.org/publications/issues/smart-city-technologies-take-on-covid-19/ (accessed on 7 July 2020).
- Bueno-Notivol, J.; Gracia-García, P.; Olaya, B.; Lasheras, I.; López-Antón, R.; Santabárbara, J. Prevalence of Depression during the COVID-19 Outbreak: A Meta-Analysis of Community-Based Studies. Int. J. Clin. Health Psychol. 2021, 21, 100196. [Google Scholar] [CrossRef]
- Maalsen, S.; Dowling, R. Covid-19 and the Accelerating Smart Home. Big Data Soc. 2020, 7, 205395172093807. [Google Scholar] [CrossRef]
- Méndez, J.I.; Mata, O.; Ponce, P.; Meier, A.; Peffer, T.; Molina, A. Multi-Sensor System, Gamification, and Artificial Intelligence for Benefit Elderly People. In Challenges and Trends in Multimodal Fall Detection for Healthcare; Ponce, H., Martínez-Villaseñor, L., Brieva, J., Moya-Albor, E., Eds.; Springer International Publishing: Cham, Switzerland, 2020; Volume 273, pp. 207–235. ISBN 978-3-030-38747-1. [Google Scholar]
- Méndez, J.I.; Ponce, P.; Medina, A.; Meier, A.; Peffer, T.; McDaniel, T.; Molina, A. Human-Machine Interfaces for Socially Connected Devices: From Smart Households to Smart Cities. In Multimedia for Accessible Human Computer Interfaces; McDaniel, T., Liu, X., Eds.; Springer International Publishing: Cham, Switzerland, 2021; pp. 253–289. ISBN 978-3-030-70715-6. [Google Scholar]
- Maharjan, R.; Bækgaard, P.; Bardram, J.E. “Hear Me out”: Smart Speaker Based Conversational Agent to Monitor Symptoms in Mental Health. In Proceedings of the Adjunct Proceedings of the 2019 ACM International Joint Conference on Pervasive and Ubiquitous Computing and Proceedings of the 2019 ACM International Symposium on Wearable Computers, London, UK, 9–13 September 2019; Association for Computing Machinery: New York, NY, USA, 2019; pp. 929–933. [Google Scholar]
- Holmlund, T.B.; Chandler, C.; Foltz, P.W.; Cohen, A.S.; Cheng, J.; Bernstein, J.C.; Rosenfeld, E.P.; Elvevåg, B. Applying Speech Technologies to Assess Verbal Memory in Patients with Serious Mental Illness. NPJ Digit. Med. 2020, 3, 33. [Google Scholar] [CrossRef] [PubMed]
- Müller, G.; Bombana, M.; Heinzel-Gutenbrenner, M.; Kleindienst, N.; Bohus, M.; Lyssenko, L.; Vonderlin, R. Socio-Economic Consequences of Mental Distress: Quantifying the Impact of Self-Reported Mental Distress on the Days of Incapacity to Work and Medical Costs in a Two-Year Period: A Longitudinal Study in Germany. BMC Public Health 2021, 21, 625. [Google Scholar] [CrossRef] [PubMed]
- Chand, S.P.; Arif, H. Depression. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Del Barrio, V. Raíces y Evolución Del DSM. Rev. Hist. Psicol. 2009, 30, 81–90. [Google Scholar]
- Psychiatry DSM-5 FAQ. Available online: https://www.psychiatry.org/psychiatrists/practice/dsm/feedback-and-questions/frequently-asked-questions (accessed on 21 October 2021).
- Marvin, K. Patient Health Questionnaire (PHQ-9)—Strokengine. Available online: https://strokengine.ca/en/assessments/patient-health-questionnaire-phq-9/ (accessed on 21 October 2021).
- He, C.; Levis, B.; Riehm, K.E.; Saadat, N.; Levis, A.W.; Azar, M.; Rice, D.B.; Krishnan, A.; Wu, Y.; Sun, Y.; et al. The Accuracy of the Patient Health Questionnaire-9 (PHQ-9) Algorithm for Screening to Detect Major Depression: An Individual Participant Data Meta-Analysis. Psychother. Psychosom. 2020, 89, 25–37. [Google Scholar] [CrossRef]
- McCord, D.M.; Provost, R.P. Construct Validity of the PHQ-9 Depression Screen: Correlations with Substantive Scales of the MMPI-2-RF. J. Clin. Psychol. Med. Settings 2020, 27, 150–157. [Google Scholar] [CrossRef] [PubMed]
- National Health and Nutrition Examination Survey 2017—March 2020 Data Documentation, Codebook, and Frequencies–Mental Health–Depression Screener (P_DPQ). Available online: https://wwwn.cdc.gov/Nchs/Nhanes/2017-2018/P_DPQ.htm (accessed on 13 October 2021).
- National Health and Nutrition Examination Survey P_DPQ_Dataset. Available online: https://wwwn.cdc.gov/Nchs/Nhanes/2017-2018/P_DPQ.XPT (accessed on 13 October 2021).
- Holst, A. Smart Home in the United States—Statistics & Facts. Available online: https://www.statista.com/topics/6201/smart-home-in-the-united-states/ (accessed on 13 October 2021).
- Ponce, P.; Meier, A.; Mendez, J.; Peffer, T.; Molina, A.; Mata, O. Tailored Gamification and Serious Game Framework Based on Fuzzy Logic for Saving Energy in Smart Thermostats. J. Clean. Prod. 2020, 262, 121167. [Google Scholar] [CrossRef]
- Mendez, J.I.; Ponce, P.; Mata, O.; Meier, A.; Peffer, T.; Molina, A.; Aguilar, M. Empower Saving Energy into Smart Homes Using a Gamification Structure by Social Products. In Proceedings of the 2020 IEEE International Conference on Consumer Electronics (ICCE), IEEE, Las Vegas, NV, USA, 4–6 January 2020; pp. 1–7. [Google Scholar]
- Aliero, M.S.; Qureshi, K.N.; Pasha, M.F.; Jeon, G. Smart Home Energy Management Systems in Internet of Things Networks for Green Cities Demands and Services. Environ. Technol. Innov. 2021, 22, 101443. [Google Scholar] [CrossRef]
- Méndez, J.I.; Ponce, P.; Meier, A.; Peffer, T.; Mata, O.; Molina, A. S4 Product Design Framework: A Gamification Strategy Based on Type 1 and 2 Fuzzy Logic. In Smart Multimedia; Lecture Notes in Computer Science; McDaniel, T., Berretti, S., Curcio, I.D.D., Basu, A., Eds.; Springer International Publishing: Cham, Switzerland, 2020; Volume 12015, pp. 509–524. ISBN 978-3-030-54406-5. [Google Scholar]
- Méndez, J.I.; Ponce, P.; Miranda, O.; Pérez, C.; Cruz, A.P.; Peffer, T.; Meier, A.; McDaniel, T.; Molina, A. Designing a Consumer Framework for Social Products Within a Gamified Smart Home Context. In Universal Access in Human-Computer Interaction. Design Methods and User Experience; Lecture Notes in Computer Science; Antona, M., Stephanidis, C., Eds.; Springer International Publishing: Cham, Switzerland, 2021; Volume 12768, pp. 429–443. ISBN 978-3-030-78091-3. [Google Scholar]
- Mendez, J.I.; Ponce, P.; Meier, A.; Peffer, T.; Mata, O.; Molina, A. Framework for Promoting Social Interaction and Physical Activity in Elderly People Using Gamification and Fuzzy Logic Strategy. In Proceedings of the 2019 IEEE Global Conference on Signal and Information Processing (GlobalSIP), Ottawa, ON, Canada, 11–14 November 2019; pp. 1–5. [Google Scholar]
- Mata, O.; Ponce, P.; McDaniel, T.; Méndez, J.I.; Peffer, T.; Molina, A. Smart City Concept Based on Cyber-Physical Social Systems with Hierarchical Ethical Agents Approach. In Proceedings of the Universal Access in Human-Computer Interaction. Access to Media, Learning and Assistive Environments, Washington, DC, USA, 24–29 July 2021; Antona, M., Stephanidis, C., Eds.; Springer International Publishing: Cham, Switzerland, 2021; pp. 424–437. [Google Scholar]
- Ponce, P.; Mendez, J.I.; Medina, A.; Mata, O.; Meier, A.; Peffer, T.; Molina, A. Smart Cities Using Social Cyber-Physical Systems Driven by Education. In Proceedings of the 2021 IEEE European Technology and Engineering Management Summit (E-TEMS), Dortmund, Germany, 18 March 2021; pp. 155–160. [Google Scholar]
- Mendez, J.I.; Ponce, P.; Medina, A.; Peffer, T.; Meier, A.; Molina, A. A Smooth and Accepted Transition to the Future of Cities Based on the Standard ISO 37120, Artificial Intelligence, and Gamification Constructors. In Proceedings of the 2021 IEEE European Technology and Engineering Management Summit (E-TEMS), Dortmund, Germany, 18 March 2021; pp. 65–71. [Google Scholar]
- Méndez, J.I.; Ponce, P.; Peffer, T.; Meier, A.; Molina, A. A Gamified HMI as a Response for Implementing a Smart-Sustainable University Campus. In Proceedings of the Smart and Sustainable Collaborative Networks 4.0, Saint-Étienne, France, 22–24 November 2021; Camarinha-Matos, L.M., Boucher, X., Afsarmanesh, H., Eds.; Springer International Publishing: Cham, Switzerland, 2021; pp. 683–691. [Google Scholar]
- Méndez, J.I.; Ponce, P.; Pecina, M.; Schroeder, G.; Castellanos, S.; Peffer, T.; Meier, A.; Molina, A. A Rapid HMI Prototyping Based on Personality Traits and AI for Social Connected Thermostats. In Advances in Soft Computing; Batyrshin, I., Gelbukh, A., Sidorov, G., Eds.; Springer International Publishing: Cham, Switzerland, 2021; pp. 216–227. [Google Scholar]
- Mata, O.; Ponce, P.; Méndez, I.; Molina, A.; Meier, A.; Peffer, T. A Model Using Artificial Neural Networks and Fuzzy Logic for Knowing the Consumer on Smart Thermostats as a S3 Product. In Advances in Soft Computing; Martínez-Villaseñor, L., Batyrshin, I., Marín-Hernández, A., Eds.; Springer International Publishing: Cham, Switzerland, 2019; Volume 11835, pp. 430–439. ISBN 978-3-030-33748-3. [Google Scholar]
- Zadeh, L.A. Fuzzy Sets. Inf. Control. 1965, 8, 338–353. [Google Scholar] [CrossRef] [Green Version]
- Ponce, P. Inteligencia Artificial Con Aplicaciones a La Ingeniería, 1st ed.; Alfaomega: Mexico City, Mexico, 2011; ISBN 978-607-7854-83-8. [Google Scholar]
- Ponce-Cruz, P.; Molina, A.; MacCleery, B. Fuzzy Logic Type 1 and Type 2 Based on LabVIEW(TM) FPGA, 1st ed.; Studies in Fuzziness and Soft Computing; Springer: Cham, Switzerland, 2016; Volume 334, ISBN 3-319-26655-1. [Google Scholar]
- Wlodarczyk, T.W.; Rong, C.; O’Connor, M.; Musen, M. SWRL-F: A Fuzzy Logic Extension of the Semantic Web Rule Language. In Proceedings of the International Conference on Web Intelligence, Mining and Semantics—WIMS ’11, Sogndal, Norway, 25–27 May 2011; ACM Press: New York, NY, USA, 2011; pp. 1–9. [Google Scholar]
- Thakur, A.; Alam, M.S.; Abir, R.M.H.; Kushal, M.A.A.; Rahman, R.M. A Fuzzy Approach for the Diagnosis of Depression. In Modern Approaches for Intelligent Information and Database Systems, Studies in Computational Intelligence; Sieminski, A., Kozierkiewicz, A., Nunez, M., Ha, Q.T., Eds.; Springer International Publishing: Cham, Switzerland, 2018; Volume 769, pp. 199–211. ISBN 978-3-319-76080-3. [Google Scholar]
- Leon, E.; Montejo, M.; Dorronsoro, I. Prospect of Smart Home-Based Detection of Subclinical Depressive Disorders. In Proceedings of the 5th International ICST Conference on Pervasive Computing Technologies for Healthcare, Dublin, Ireland, 23–26 May 2011. [Google Scholar]
- Pal, D.; Triyason, T.; Funikul, S. Smart Homes and Quality of Life for the Elderly: A Systematic Review. In Proceedings of the 2017 IEEE International Symposium on Multimedia (ISM), Taichung, Taiwan, 11–13 December 2017; pp. 413–419. [Google Scholar]
- VandeWeerd, C.; Yalcin, A.; Aden-Buie, G.; Wang, Y.; Roberts, M.; Mahser, N.; Fnu, C.; Fabiano, D. HomeSense: Design of an Ambient Home Health and Wellness Monitoring Platform for Older Adults. Health Technol. 2020, 10, 1291–1309. [Google Scholar] [CrossRef]
- Silva, D.C.B.; Cruz, P.P.; Gutiérrez, A.M.; Avendaño, L.A.S. Applications of Human-Computer Interaction and Robotics Based on Artificial Intelligence; Editorial Digital del Tecnológico de Monterrey: Monterrey, Mexico, 2020. [Google Scholar]
- Summers, C.; Wu, P.; Taylor, A.J.G. Supporting Mental Health During the COVID-19 Pandemic Using a Digital Behavior Change Intervention: An Open-Label, Single-Arm, Pre-Post Intervention Study. JMIR Form Res. 2021, 5, e31273. [Google Scholar] [CrossRef]
- Mangrulkar, R.S.; Michalas, A.; Shekokar, N.M.; Narvekar, M.; Chavan, P.V. Design of Intelligent Applications Using Machine Learning and Deep Learning Techniques, 1st ed.; Chapman and Hall/CRC: Boca Raton, FL, USA, 2021; ISBN 978-1-00-313368-1. [Google Scholar]
- Chou, Y. Actionable Gamification Beyond Points, Badges, and Leaderboards; Octalysis Media: Fremont, CA, USA, 2015; ISBN 978-1-5117-4404-1. [Google Scholar]
- Dias, L.P.S.; Barbosa, J.L.V.; Vianna, H.D. Gamification and Serious Games in Depression Care: A Systematic Mapping Study. Telemat. Inform. 2018, 35, 213–224. [Google Scholar] [CrossRef]
- Lukas, C.A.; Eskofier, B.; Berking, M. A Gamified Smartphone-Based Intervention for Depression: Randomized Controlled Pilot Trial. JMIR Ment. Health 2021, 8, e16643. [Google Scholar] [CrossRef] [PubMed]
- Hungerbuehler, I.; Daley, K.; Cavanagh, K.; Garcia Claro, H.; Kapps, M. Chatbot-Based Assessment of Employees’ Mental Health: Design Process and Pilot Implementation. JMIR Form Res. 2021, 5, e21678. [Google Scholar] [CrossRef]
- National Health and Nutrition Examination Survey 2017–March 2020 Data Documentation, Codebook, and Frequencies–Demographic Variables and Sample Weights (P_DEMO). Available online: https://wwwn.cdc.gov/Nchs/Nhanes/2017-2018/P_DEMO.htm#RIAGENDR (accessed on 14 October 2021).
- National Health and Nutrition Examination Survey P_DEMO_Dataset. Available online: https://wwwn.cdc.gov/Nchs/Nhanes/2017-2018/P_DEMO.XPT (accessed on 13 October 2021).
- Lee, D.K. Alternatives to P Value: Confidence Interval and Effect Size. Korean J. Anesthesiol. 2016, 69, 555. [Google Scholar] [CrossRef] [Green Version]
- Méndez, J.I.; Meza-Sánchez, A.V.; Ponce, P.; McDaniel, T.; Meier, A.; Molina, A. PHQ9-LabVIEW Results. Available online: https://github.com/IsabelMendezG/PHQ9_FuzzyLogicResults (accessed on 14 November 2021).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Over the Last 2 Weeks, How Often Have You Been Bothered by Any of These Following Problems? | Not at All | Several Days | More than Half the Days | Nearly Every Day |
|---|---|---|---|---|
| 1. Little interest or pleasure in doing things | 0 | 1 | 2 | 3 |
| 2. Feeling down, depressed, or hopeless | 0 | 1 | 2 | 3 |
| 3. Trouble falling or staying asleep, or sleeping too much | 0 | 1 | 2 | 3 |
| 4. Feeling tired or having little energy | 0 | 1 | 2 | 3 |
| 5. Poor appetite or overeating | 0 | 1 | 2 | 3 |
| 6. Feeling bad about yourself—or that you are a failure or have let yourself of your family down | 0 | 1 | 2 | 3 |
| 7. Trouble concentrating on things, such as reading the newspaper or watching television | 0 | 1 | 2 | 3 |
| 8. Moving or speaking so slowly that other people could have noticed? Or the opposite—being so fidgety or restless that you have been moving around a lot more than usual? | 0 | 1 | 2 | 3 |
| 9. Thoughts that you would be better off dead, or of hurting yourself. | 0 | 1 | 2 | 3 |
| Extrinsic Motivation | Intrinsic Motivation |
|---|---|
| Challenges | Notifications |
| Levels | Messages |
| Dashboard | Tips |
| Statistics | Community |
| Profile picture or avatar | Collaboration |
| Points, badges, leaderboard | Competition |
| Code | Description |
|---|---|
| SEQN | Respondent sequence number. |
| RIAGENDR | Gender of the participant. |
| RIDAGEYR | Age in years of the participant at the time of screening. Individuals 80 and over were coded at 80 years of age. |
| DPQ010 to DPQ090 | Represent each question described in Table 1. |
| Total | Total score up to 27. |
| Score Percentile | Age Group | |||||
|---|---|---|---|---|---|---|
| 20–29 | 30–39 | 40–49 | 50–59 | 60–69 | 70–80 | |
| P3 (Expected low limit) | 0 | 0 | 0 | 0 | 0 | 0 |
| P25 (Expected) | 0 | 0 | 0 | 0 | 0 | 0 |
| P50 (Median) | 2 | 2 | 2 | 2 | 2 | 2 |
| P75 (Expected) | 5 | 4 | 5 | 5 | 5 | 4 |
| P97 (Expected high limit) | 14 | 15 | 15 | 16 | 16 | 14.67 |
| Depression Severity | Male | Female |
|---|---|---|
| No | 3033 | 2790 |
| Mild | 553 | 780 |
| Moderate | 180 | 296 |
| Moderately severe | 69 | 108 |
| Severe | 30 | 43 |
| Score Percentile | Age Group | |||||
|---|---|---|---|---|---|---|
| 20–29 | 30–39 | 40–49 | 50–59 | 60–69 | 70–80 | |
| No Depression | 861 | 920 | 941 | 964 | 1143 | 994 |
| Total Depression | 336 | 289 | 869 | 397 | 402 | 316 |
| Rule | IF | AND | THEN |
|---|---|---|---|
| 1 | Q9 is “Not at all” | TotalScore is “No depression” | Action is “Continue monitoring” |
| 2 | Q9 is “Not at all” | TotalScore is “Mild depression” | Action is “Continue monitoring” |
| 3 | Q9 is “Not at all” | TotalScore is “Moderate depression” | Action is “Specialist referral” |
| 4 | Q9 is “Not at all” | TotalScore is “Moderately severe depression” | Action is “Specialist referral” |
| 5 | Q9 is “Not at all” | TotalScore is “Severe depression” | Action is “Specialist referral” |
| 6 | Q9 is “Several days” | TotalScore is “No depression” | Action is “Specialist referral is mandatory” |
| 7 | Q9 is “Several days” | TotalScore is “Mild depression” | Action is Specialist referral is mandatory |
| 8 | Q9 is “Several days” | TotalScore is “Moderate depression” | Action is Specialist referral is mandatory |
| 9 | Q9 is “Several days” | TotalScore is “Moderately severe depression” | Action is Specialist referral is mandatory |
| 10 | Q9 is “Several days” | TotalScore is “Severe depression” | Action is Specialist referral is mandatory |
| 11 | Q9 is “More than half the days” | TotalScore is “No depression” | Action is “Specialist referral is mandatory” |
| 12 | Q9 is “More than half the days” | TotalScore is “Mild depression” | Action is Specialist referral is mandatory |
| 13 | Q9 is “More than half the days” | TotalScore is “Moderate depression” | Action is Specialist referral is mandatory |
| 14 | Q9 is “More than half the days” | TotalScore is “Moderately severe depression” | Action is Specialist referral is mandatory |
| 15 | Q9 is “More than half the days” | TotalScore is “Severe depression” | Action is Specialist referral is mandatory |
| 16 | Q9 is “Nearly every day” | TotalScore is “No depression” | Action is “Specialist referral is mandatory” |
| 17 | Q9 is “Nearly every day” | TotalScore is “Mild depression” | Action is Specialist referral is mandatory |
| 18 | Q9 is “Nearly every day” | TotalScore is “Moderate depression” | Action is Specialist referral is mandatory |
| 19 | Q9 is “Nearly every day” | TotalScore is “Moderately severe depression” | Action is Specialist referral is mandatory |
| 20 | Q9 is “Nearly every day” | TotalScore is “Severe depression” | Action is “Specialist referral is mandatory |
| Rule | IF | AND | THEN |
|---|---|---|---|
| 1 | Age is “20–29” | 20–29 is “Expected” | Action is “Continue monitoring” |
| 2 | Age is “20–29” | 20–29 is “Outside expected” | Action is “Specialist referral” |
| 3 | Age is “20–29” | 20–29 is “Abnormal” | Action is “Specialist referral is mandatory” |
| 4 | Age is “30–39” | 30–39 is “Expected” | Action is “Continue monitoring” |
| 5 | Age is “30–39” | 30–39 is “Outside expected” | Action is “Specialist referral” |
| 6 | Age is “30–39” | 30–39 is “Abnormal” | Action is “Specialist referral is mandatory” |
| 7 | Age is “40–49” | 40–49 is “Expected” | Action is “Continue monitoring” |
| 8 | Age is “40–49” | 40–49 is “Outside expected” | Action is “Specialist referral” |
| 9 | Age is “40–49” | 40–49 is “Abnormal” | Action is “Specialist referral is mandatory” |
| 10 | Age is “50–59” | 50–59 is “Expected” | Action is “Continue monitoring” |
| 11 | Age is “50–59” | 50–59 is “Outside expected” | Action is “Specialist referral” |
| 12 | Age is “50–59” | 50–59 is “Abnormal” | Action is “Specialist referral is mandatory” |
| 13 | Age is “60–69” | 60–69 is “Expected” | Action is “Continue monitoring” |
| 14 | Age is “60–69” | 60–69 is “Outside expected” | Action is “Specialist referral” |
| 15 | Age is “60–69” | 60–69 is “Abnormal” | Action is “Specialist referral is mandatory” |
| 16 | Age is “70–80” | 70–80 is “Expected” | Action is “Continue monitoring” |
| 17 | Age is “70–80” | 70–80 is “Outside expected” | Action is “Specialist referral” |
| 18 | Age is “70–80” | 70–80 is “Abnormal” | Action is “Specialist referral is mandatory” |
| SEQN | RIDAGEYR | DPQ010 | DPQ020 | DPQ030 | DPQ040 | DPQ050 | DPQ060 | DPQ070 | DPQ080 | DPQ090 | Total | Action to Take | Expectation |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 109266 | 29 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | Continue monitoring | Expected |
| 119042 | 75 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | Specialist referral is MANDATORY | Expected |
| 109994 | 73 | 3 | 3 | 3 | 3 | 2 | 0 | 0 | 3 | 0 | 17 | Specialist referral | Abnormal |
| 121279 | 28 | 1 | 1 | 2 | 1 | 2 | 1 | 1 | 0 | 0 | 9 | Continue monitoring | Outside expected |
| 124698 | 51 | 2 | 3 | 1 | 1 | 2 | 1 | 1 | 2 | 0 | 13 | Specialist referral | Outside expected |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Méndez, J.I.; Meza-Sánchez, A.V.; Ponce, P.; McDaniel, T.; Peffer, T.; Meier, A.; Molina, A. Smart Homes as Enablers for Depression Pre-Diagnosis Using PHQ-9 on HMI through Fuzzy Logic Decision System. Sensors 2021, 21, 7864. https://doi.org/10.3390/s21237864
Méndez JI, Meza-Sánchez AV, Ponce P, McDaniel T, Peffer T, Meier A, Molina A. Smart Homes as Enablers for Depression Pre-Diagnosis Using PHQ-9 on HMI through Fuzzy Logic Decision System. Sensors. 2021; 21(23):7864. https://doi.org/10.3390/s21237864
Chicago/Turabian StyleMéndez, Juana Isabel, Ana Victoria Meza-Sánchez, Pedro Ponce, Troy McDaniel, Therese Peffer, Alan Meier, and Arturo Molina. 2021. "Smart Homes as Enablers for Depression Pre-Diagnosis Using PHQ-9 on HMI through Fuzzy Logic Decision System" Sensors 21, no. 23: 7864. https://doi.org/10.3390/s21237864
APA StyleMéndez, J. I., Meza-Sánchez, A. V., Ponce, P., McDaniel, T., Peffer, T., Meier, A., & Molina, A. (2021). Smart Homes as Enablers for Depression Pre-Diagnosis Using PHQ-9 on HMI through Fuzzy Logic Decision System. Sensors, 21(23), 7864. https://doi.org/10.3390/s21237864