
Does Cup-Grip Type Affect Tremor among People with Essential Tremor?


Abstract
1. Introduction
2. Methods
2.1. Participants
2.2. Research Instruments
2.2.1. Questionnaires
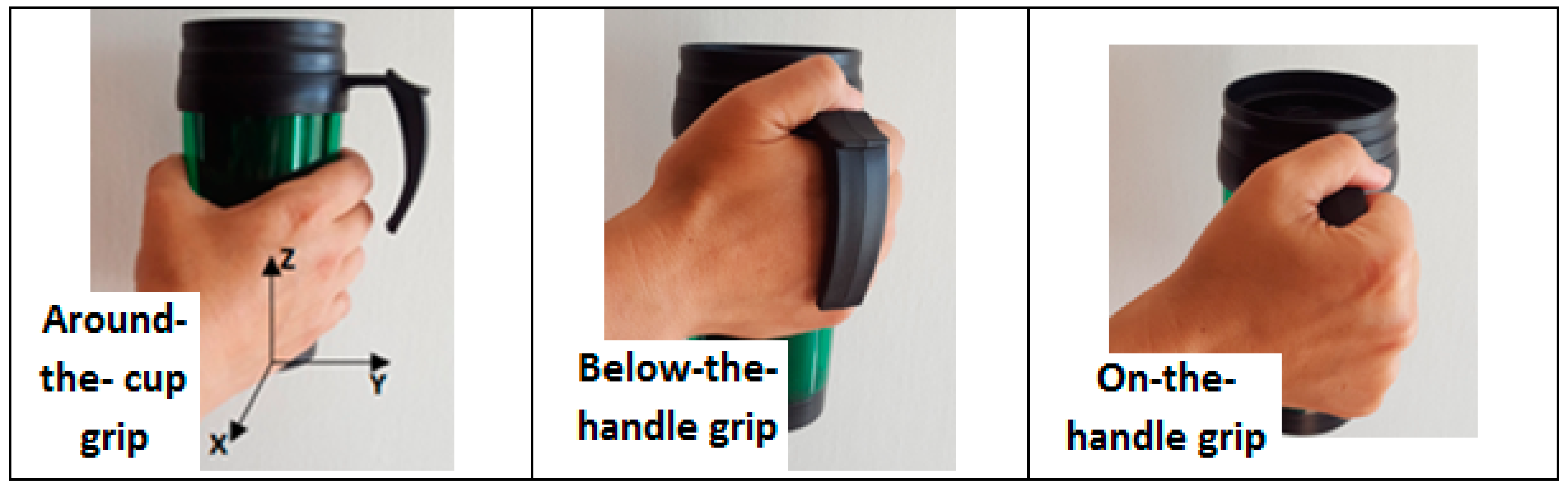
2.2.2. Performance-Based Tasks
2.3. Data Processing
2.4. Statistical Analysis
3. Results
3.1. Demographic and General Information
3.2. Comparing the ET and Control Groups
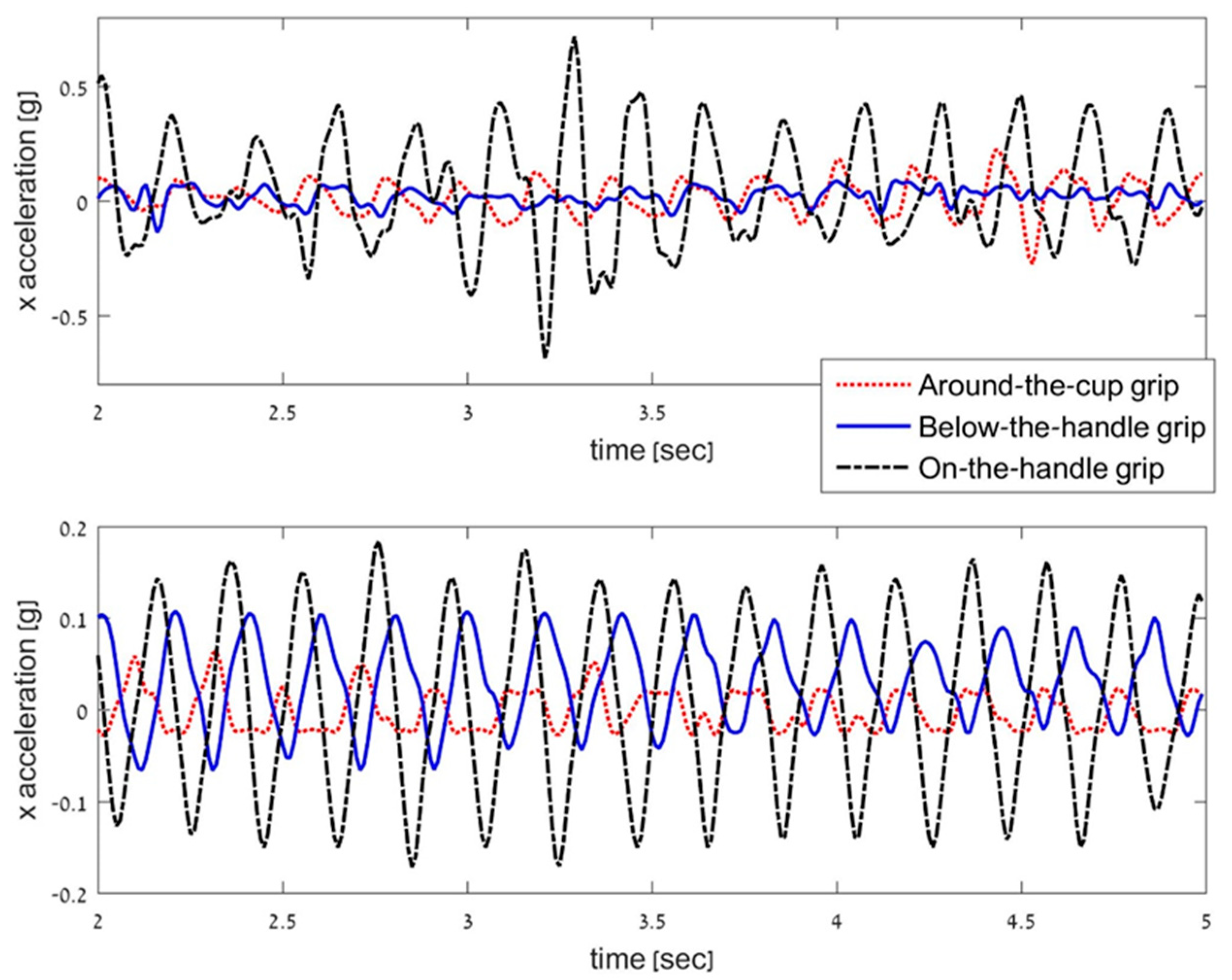
3.3. Comparing Axes Acceleration
3.4. Comparing Grip Types
3.5. Correlation Analysis of Cup-Task and Drawing-Task Outcome Measures
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brennan, K.C.; Jurewicz, E.C.; Ford, B.; Pullman, S.L.; Louis, E.D. Is essential tremor predominantly a kinetic or a postural tremor? A clinical and electrophysiological study. Mov. Disord. 2002, 17, 313–316. [Google Scholar] [CrossRef] [PubMed]
- Louis, E.D.; McCreary, M. How Common is Essential Tremor? Update on the Worldwide Prevalence of Essential Tremor. Tremor Other Hyperkinetic Mov. 2021, 11, 28. [Google Scholar] [CrossRef]
- Elble, R.J. What is Essential Tremor? Curr. Neurol. Neurosci. Rep. 2013, 13, 353. [Google Scholar] [CrossRef] [PubMed]
- Bain, P.G.; Findley, L.J.; Thompson, P.D.; Gresty, M.A.; Rothwell, J.; Harding, A.E.; Marsden, C.D. A study of hereditary essential tremor. Brain 1994, 117, 805–824. [Google Scholar] [CrossRef] [PubMed]
- Louis, E.D.; Barnes, L.; Albert, S.M.; Cote, L.; Schneier, F.R.; Pullman, S.L.; Yu, Q. Correlates of functional disability in essential tremor. Mov. Disord. 2001, 16, 914–920. [Google Scholar] [CrossRef]
- Wendt, K.J.; Albert, S.M.; Pullman, S.L.; Schneier, F.R.; Louis, E.D. Columbia University Assessment of Disability in Essential Tremor (CADET): Methodological issues in essential tremor research. Parkinsonism Relat. Disord. 2000, 6, 17–23. [Google Scholar] [CrossRef]
- Louis, E.D.; Wendt, K.J.; Albert, S.M.; Pullman, S.L.; Yu, Q.; Andrews, H. Validity of a performance-based test of function in essential tremor. Arch. Neurol. 1999, 56, 841–846. [Google Scholar] [CrossRef]
- Louis, E.D.; Barnes, L.F.; Wendt, K.J.; Albert, S.M.; Pullman, S.L.; Yu, Q.; Schneier, F.R. Validity and test-retest reliability of a disability questionnaire for essential tremor. Mov. Disord. 2000, 15, 516–523. [Google Scholar] [CrossRef]
- Bain, P.G.; Findley, L.J.; Atchison, P.; Behari, M.; Vidailhet, M.; Gresty, M.; Rothwell, J.C.; Thompson, P.D.; Marsden, C.D. Assessing tremor severity. J. Neurol. Neurosurg. Psychiatry 1993, 56, 868–873. [Google Scholar] [CrossRef] [PubMed]
- Hess, C.W.; Pullman, S.L. Tremor: Clinical phenomenology and assessment techniques. Tremor Other Hyperkinetic Mov. 2012, 2. [Google Scholar] [CrossRef]
- Heldman, D.A.; Jankovic, J.; Vaillancourt, D.E.; Prodoehl, J.; Elble, R.J.; Giuffrida, J.P. Essential tremor quantification during activities of daily living. Parkinsonism Relat. Disord. 2011, 17, 537–542. [Google Scholar] [CrossRef]
- Golan, D.; Giladi, N.; Thorne, R.; Korczyn, A.D.; Simon, E.S. Subdivision of essential tremor patients according to physiologic characteristics. Acta Neurol. Scand. 2004, 109, 393–397. [Google Scholar] [CrossRef]
- Elble, R.J.; Brilliant, M.; Leffler, K.; Higgins, C. Quantification of essential tremor in writing and drawing. Mov. Disord. 1996, 11, 70–78. [Google Scholar] [CrossRef] [PubMed]
- Schuhmayer, N.; Weber, C.; Kieler, M.; Voller, B.; Pirker, W.; Auff, E.; Haubenberger, D. Task-dependent variability of Essential Tremor. Parkinsonism Relat. Disord. 2017, 41, 79–85. [Google Scholar] [CrossRef]
- Roth, N.; Braun-Benyamin, O.; Rosenblum, S. Drawing Direction Effect on a Task’s Performance Characteristics among People with Essential Tremor. Sensors 2021, 21, 5814. [Google Scholar] [CrossRef] [PubMed]
- Jeon, H.; Lee, W.-W.; Park, H.; Lee, H.J.; Kim, S.K.; Kim, H.B.; Jeon, B.; Park, K.S. Automatic Classification of Tremor Severity in Parkinson’s Disease Using a Wearable Device. Sensors 2017, 17, 2067. [Google Scholar] [CrossRef] [PubMed]
- Grimaldi, G.; Manto, M. Neurological Tremor: Sensors, Signal Processing and Emerging Applications. Sensors 2010, 10, 1399–1422. [Google Scholar] [CrossRef] [PubMed]
- Elble, R.J.; McNames, J. Using Portable Transducers to Measure Tremor Severity. Tremor Other Hyperkinetic Mov. 2016, 6, 375. [Google Scholar] [CrossRef]
- Roth, N.; Rosenblum, S. What are the functional daily characteristics of people with essential tremor? Submitted.
- Gironell, A.; Martínez-Corral, M.; Pagonabarraga, J.; Kulisevsky, J. The Glass scale: A simple tool to determine severity in essential tremor. Parkinsonism Relat. Disord. 2010, 16, 412–414. [Google Scholar] [CrossRef]
- Bain, P.G.; Mally, J.; Gresty, M.; Findley, L.J. Assessing the impact of essential tremor on upper limb function. J. Neurol. 1993, 241, 54–61. [Google Scholar] [CrossRef]
- Homberg, V.; Hefter, H.; Reiners, K.; Freund, H.J. Differential effects of changes in mechanical limb properties on physiological and pathological tremor. J. Neurol. Neurosurg. Psychiatry 1987, 50, 568–579. [Google Scholar] [CrossRef] [PubMed]
- Kavanagh, J.J.; Keogh, J.W. Correlates Between Force and Postural Tremor in Older Individuals with Essential Tremor. Cerebellum 2015, 15, 688–695. [Google Scholar] [CrossRef][Green Version]
- Elble, R.J. Essential tremor frequency decreases with time. Neurology 2000, 55, 1547–1551. [Google Scholar] [CrossRef]
- Kamakura, N.; Matsuo, M.; Ishii, H.; Mitsuboshi, F.; Miura, Y. Patterns of Static Prehension in Normal Hands. Am. J. Occup. Ther. 1980, 34, 437–445. [Google Scholar] [CrossRef] [PubMed]
- Lagacé, S.; Downing-Doucet, F.; Guérard, K. Norms for grip agreement for 296 photographs of objects. Behav. Res. Methods 2012, 45, 772–781. [Google Scholar] [CrossRef] [PubMed]
- Sternberg, E.J.; Alcalay, R.N.; Levy, O.A.; Louis, E.D.M. Postural and Intention Tremors: A Detailed Clinical Study of Essential Tremor vs. Parkinson’s Disease. Front. Neurol. 2013, 4, 51. [Google Scholar] [CrossRef]
- Héroux, M.E.; Pari, G.; Norman, K.E. The effect of inertial loading on wrist postural tremor in essential tremor. Clin. Neurophysiol. 2009, 120, 1020–1029. [Google Scholar] [CrossRef] [PubMed]
- Louis, E.D.; Yu, Q.; Floyd, A.G.; Moskowitz, C.; Pullman, S.L. Axis is a feature of handwritten spirals in essential tremor. Mov. Disord. 2006, 21, 1294–1295. [Google Scholar] [CrossRef]
- Elble, R.J. The Essential Tremor Rating Assessment Scale. J. Neurol. Neuromed. 2016, 1, 34–38. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Lin, P.-C.; Chen, K.-H.; Yang, B.-S.; Chen, Y.-J. A digital assessment system for evaluating kinetic tremor in essential tremor and Parkinson’s disease. BMC Neurol. 2018, 18, 25. [Google Scholar] [CrossRef] [PubMed]
- Feys, P.; Helsen, W.; Prinsmel, A.; Ilsbroukx, S.; Wang, S.; Liu, X. Digitised spirography as an evaluation tool for intention tremor in multiple sclerosis. J. Neurosci. Methods 2007, 160, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.Y.; Luo, L.; Yu, Q.; Mirallave, A.; Saunders-Pullman, R.; Lipton, R.B.; Louis, E.D.; Pullman, S.L. Repeated Spiral Drawings in Essential Tremor: A Possible Limb-Based Measure of Motor Learning. Cerebellum 2019, 18, 178–187. [Google Scholar] [CrossRef]
- Solbach, K.; Mumm, M.; Brandauer, B.; Kronenbürger, M.; Hermsdörfer, J.; Timmann, D. Prehension Kinematics, Grasping Forces, and Independent Finger Control in Mildly Affected Patients with Essential Tremor. Cerebellum 2015, 15, 498–508. [Google Scholar] [CrossRef] [PubMed]
- Ulmanová, O.; Homann, C.N.; Ulman, R.; Jech, R.; Čapek, V.; Klempíř, J.; Růžička, E. Tremor magnitude: A single index to assess writing and drawing in essential tremor. Parkinsonism Relat. Disord. 2007, 13, 250–253. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Grip Type | Axis | nSSE from Filtered Signal 10−5 [g2] M (SD) | Mann–Whitney | ||
|---|---|---|---|---|---|
| ET (n = 20) | Control (n = 18) | Z | p | ||
| Around-the-cup grip | X | 184.06 (327.53) | 7.91 (6.25) | −4.36 | <0.001 |
| Y | 535.33 (1664.17) | 4.58 (3.32) | −4.24 | <0.001 | |
| Z | 71.78 (144.0) | 7.42 (3.98) | −3.19 | 0.001 | |
| Below-the-handle grip | X | 201.13 (452.89) | 16.95 (27.37) | −4.24 | <0.001 |
| Y | 957.22 (2598.85) | 16.95 (30.98) | −4.00 | <0.001 | |
| Z | 52.44 (82.59) | 15.63 (31.49) | −3.16 | 0.002 | |
| On-the-handle grip | X | 1048.56 (2762.87) | 24.07 (27.51) | −4.36 | <0.001 |
| Y | 1303.76 (3512.06) | 24.11 (41.66) | −4.06 | <0.001 | |
| Z | 280.49 (552.37) | 19.36 (31.30) | −2.87 | 0.004 | |
| Grip Type | Y Axis | Comparing Z–X Axes | Comparing Z–Y Axes | |
|---|---|---|---|---|
| M (SD) | (Z, p) | |||
| Peak amplitude [g] | Around-the-cup grip | 0.05 (0.09) | −2.50 *, 0.012 | −3.10 **, 0.002 |
| Below-the-handle grip | 0.06 (0.10) | −2.05 *, 0.040 | −2.91 **, 0.004 | |
| On-the-handle grip | 0.08 (0.13) | −2.84 **, 0.005 | −3.92 ***, <0.001 | |
| ±1 integral around main frequency [g·Hz] | Around-the-cup grip | 0.03 (0.05) | −2.50 *, 0.010 | −3.10 **, 0.002 |
| Below-the-handle grip | 0.04 (0.06) | −2.24 *, 0.025 | −3.40 **, 0.001 | |
| On-the-handle grip | 0.05 (0.07) | −3.06 **, 0.002 | −3.83 ***, <0.001 | |
| 4–20 Hz integral [g·Hz] | Around-the-cup grip | 0.06 (0.08) | −3.29 **, 0.001 | −3.14 **, 0.002 |
| Below-the-handle grip | 0.08 (0.10) | −3.85 ***, <0.001 | −3.47 **, 0.001 | |
| On-the-handle grip | 0.09 (0.10) | −3.62 ***, <0.001 | −3.92 ***, <0.001 | |
| nSSE from filtered signal 10−5 [g2] | Around-the-cup grip | a | −2.80 **, 0.005 | −3.20 **, 0.001 |
| Below-the-handle grip | a | −2.72 **, 0.006 | −3.29 **, 0.001 | |
| On-the-handle grip | a | −2.80 **, 0.005 | −3.92 ***, <0.001 | |
| Mean amplitude computed from consequential (time domain) peaks [g] | Around-the-cup grip | 0.06 (0.10) | −2.50 *, 0.012 | −2.99 **, 0.003 |
| Below-the-handle grip | 0.08 (0.13) | −2.99 **, 0.003 | −2.99 **, 0.003 | |
| On-the-handle grip | 0.09 (0.14) | −2.65 **, 0.008 | −3.55 ***, <0.001 | |
| Domain | Cup Outcome Measure | Grip Type | Axis | Age | Spiral nSSE |
|---|---|---|---|---|---|
| Frequency | Peak amplitude [g] | Around-the-cup grip | X | ||
| Y | 0.45 * | 0.60 ** | |||
| Below-the-handle grip | X | ||||
| Y | 0.56 * | ||||
| On-the-handle grip | X | 0.48 * | 0.59 ** | ||
| Y | 0.45 * | 0.64 ** | |||
| ±1 integral around main frequency [g·Hz] | Around-the-cup grip | X | 0.45 * | ||
| Y | 0.76 ** | ||||
| Below-the-handle grip | X | ||||
| Y | 0.57 * | ||||
| On-the-handle grip | X | 0.57 * | 0.71 ** | ||
| Y | 0.68 ** | ||||
| 4–20 Hz integral [g·Hz] | Around-the-cup grip | X | 0.64 ** | ||
| Y | 0.49 * | 0.74 ** | |||
| Below-the-handle grip | X | 0.53 * | |||
| Y | 0.69 ** | ||||
| On-the-handle grip | X | 0.49 * | 0.65 ** | ||
| Y | 0.46 * | 0.67 ** | |||
| Time | nSSE from filtered signal [g2] | Around-the-cup grip | X | 0.52 * | |
| Y | 0.73 ** | ||||
| Below-the-handle grip | X | ||||
| Y | 0.61 ** | ||||
| On-the-handle grip | X | 0.50 * | 0.64 ** | ||
| Y | 0.61 ** | ||||
| Mean amplitude computed from consequential peaks [g] | Around-the-cup grip | X | 0.56 * | ||
| Y | 0.58 ** | ||||
| Below-the-handle grip | X | ||||
| Y | 0.59 ** | ||||
| On-the-handle grip | X | 0.59 ** | |||
| Y | 0.45 * | 0.61 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roth, N.; Rosenblum, S. Does Cup-Grip Type Affect Tremor among People with Essential Tremor? Sensors 2021, 21, 7797. https://doi.org/10.3390/s21237797
Roth N, Rosenblum S. Does Cup-Grip Type Affect Tremor among People with Essential Tremor? Sensors. 2021; 21(23):7797. https://doi.org/10.3390/s21237797
Chicago/Turabian StyleRoth, Navit, and Sara Rosenblum. 2021. "Does Cup-Grip Type Affect Tremor among People with Essential Tremor?" Sensors 21, no. 23: 7797. https://doi.org/10.3390/s21237797
APA StyleRoth, N., & Rosenblum, S. (2021). Does Cup-Grip Type Affect Tremor among People with Essential Tremor? Sensors, 21(23), 7797. https://doi.org/10.3390/s21237797