
Skin Lesion Detection Algorithms in Whole Body Images

 ,
,  , ,
, ,
Abstract
:1. Introduction
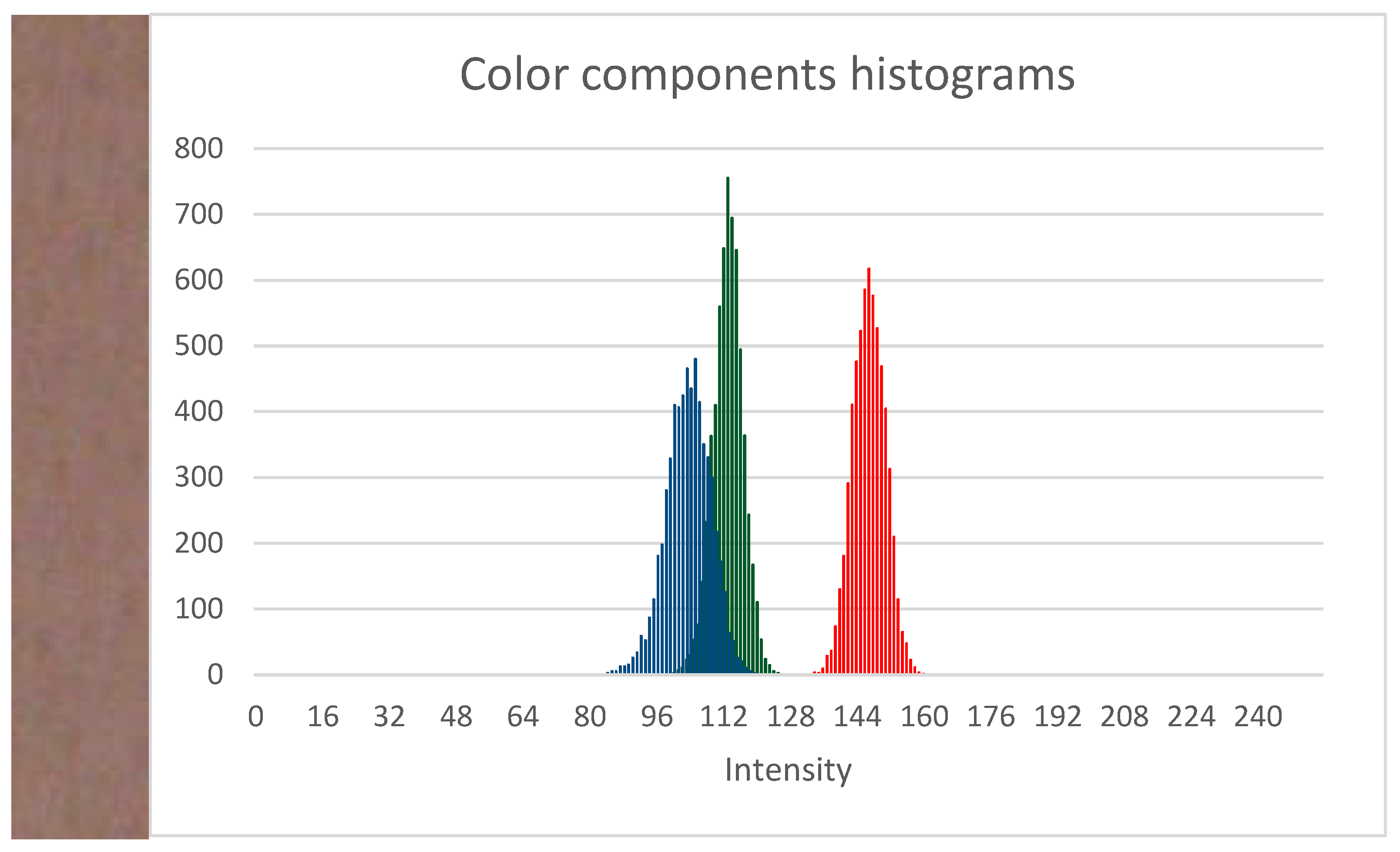
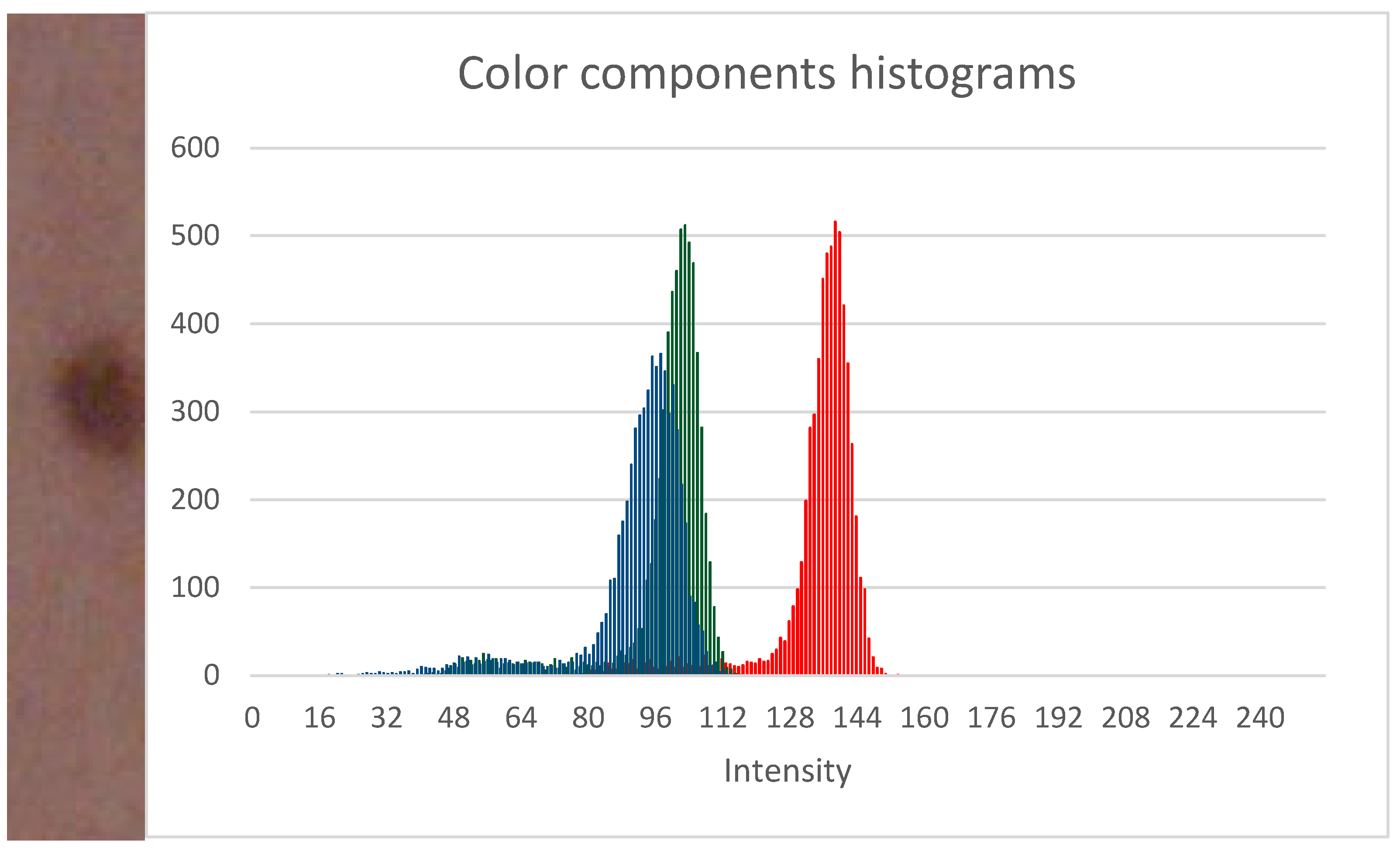
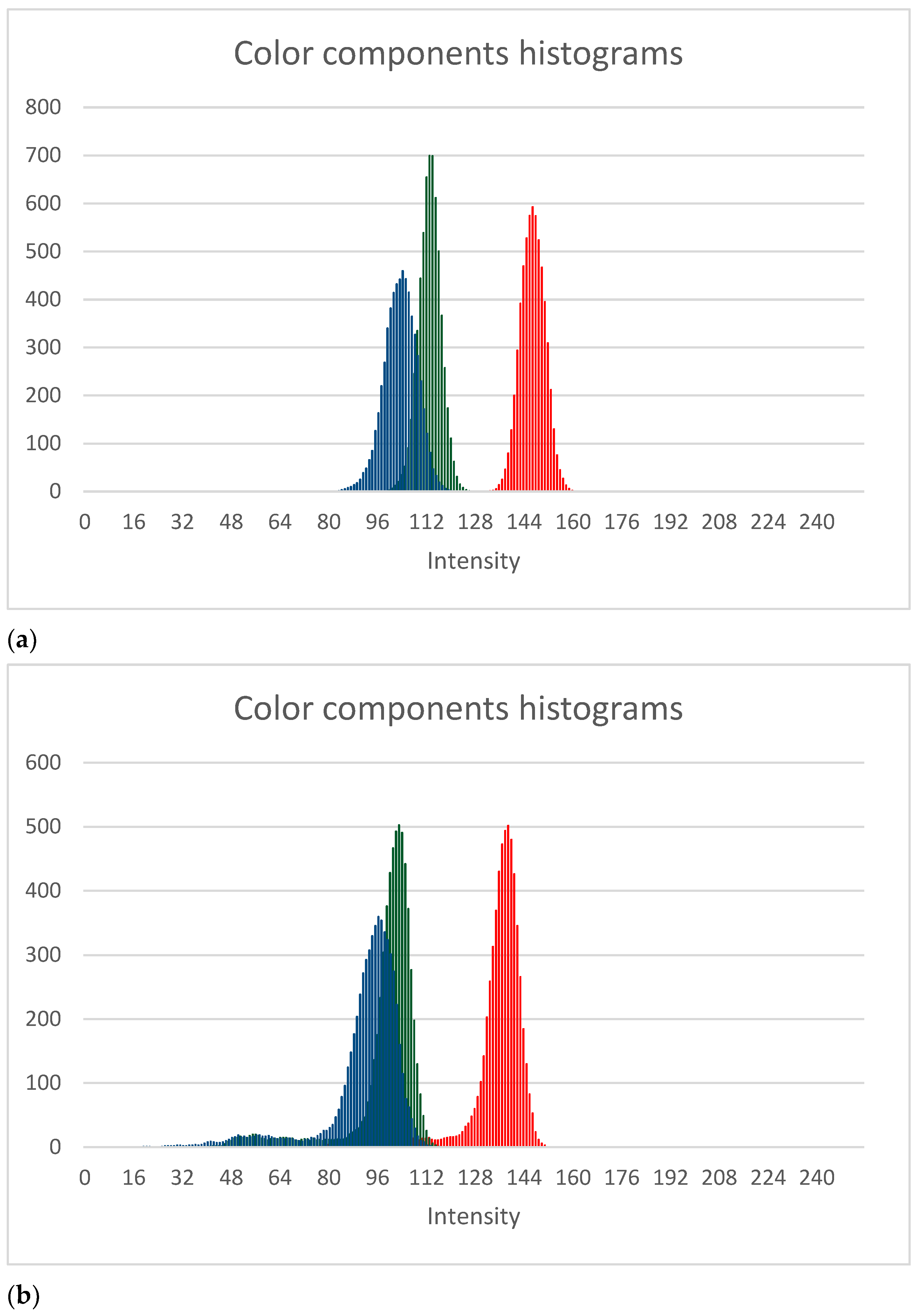
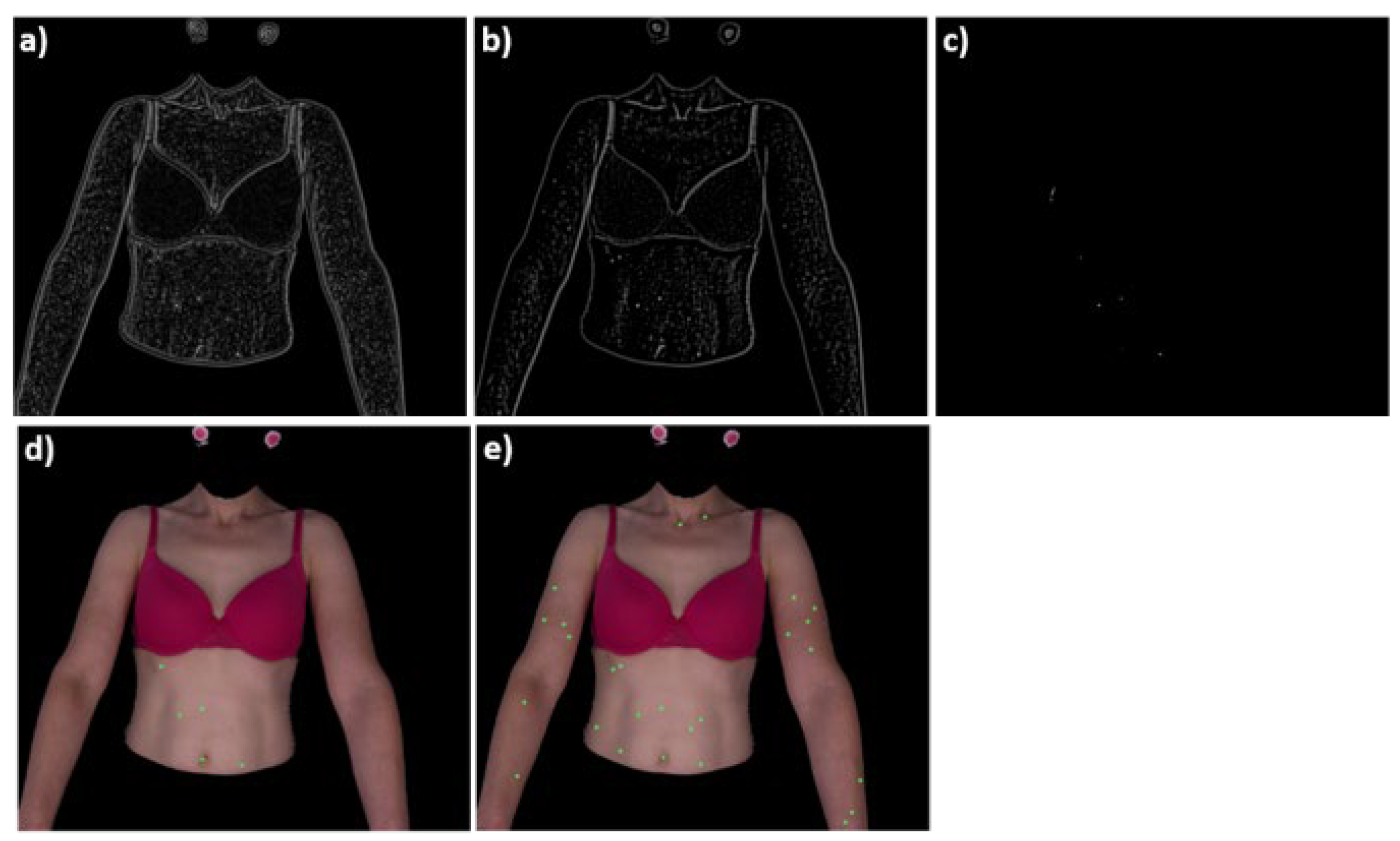
- The first approach is based on local skin modelling and analysis of histograms of selected color components. When an analyzed image fragment contains a lesion, it is reflected in its histogram. Analysis of histogram shapes enable efficient lesion segmentation (Section 2.2.1).
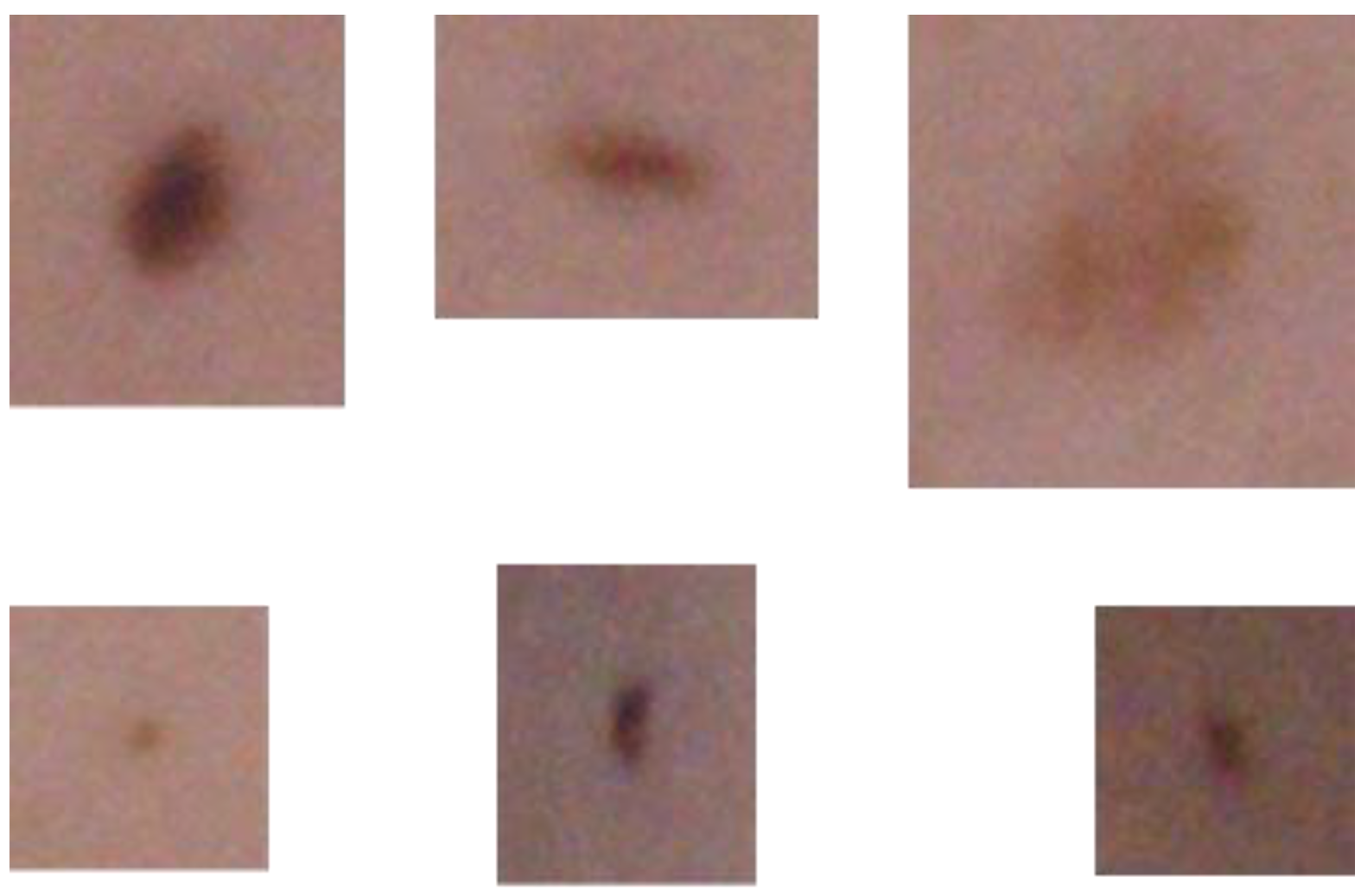
- The second algorithm assumes that the vast majority of lesions present in the whole-body image can be modelled by a finite number of lesion patterns. Two-dimensional cross-correlation functions are calculated for such patterns and the analyzed image. Functions’ maxima indicate the lesion position in the image. Detected lesions’ regions are further segmented by the active contour approach to detect the lesion shape (Section 2.2.2).
2. Materials and Methods
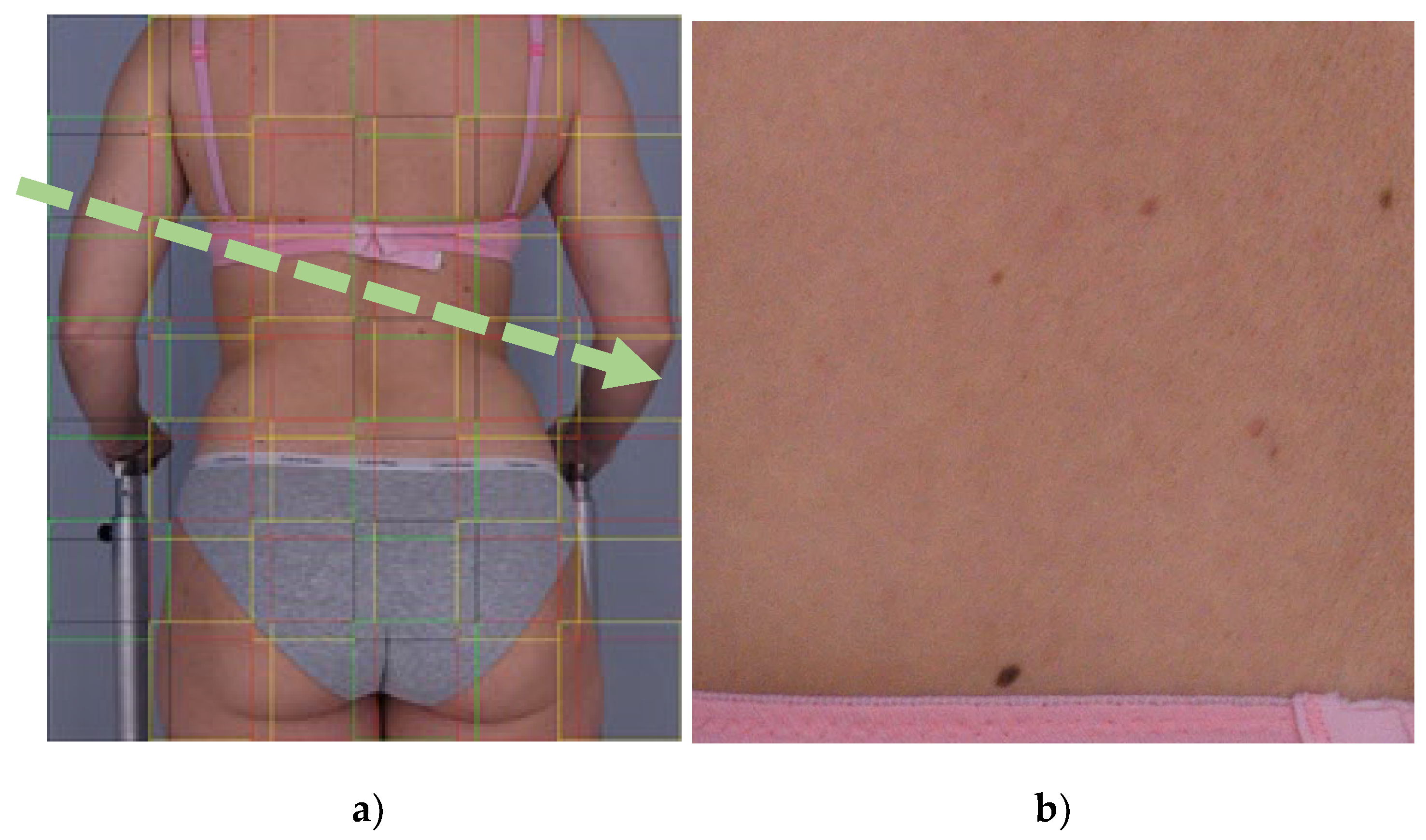
2.1. Image Acquisition System
2.2. Skin Image Analysis
2.2.1. Local Skin Model Based Approach
| Algorithm 1 Segmentation method based on local skin model |
| Function GetLesionMaskSkinModel Data: JSKIN—input RGB image Result: LM—lesion mask Divide input image into overlapping tiles: JTile ← JSKIN Create empty lesion mask LM having the size of JSKIN foreach JTile in JSKIN Extract green and blue channels from tile: G, B ← JTile Determine a histogram for the green and blue color components. Smooth the histograms with the averaging filter. Find mode and maximum value for both histograms. Find the threshold values for the green and blue components Find the lesion mask end Label lesion mask in the way that each separate lesion will have a unique numerical identifier End |
2.2.2. Correlation-Based Approach
- f(x,y)—is the image,
- t(x,y)—is the lesion template,
- is the mean of template,
- —is the mean of f(x,y) in the region under the template.
| Algorithm 2 Spot detection based on cross-correlation between mask and the image. |
| Function spotDetectionCCorrelation Data: JSKIN—input RGB image MS—list of model spots (masks) Result: FDS—detected spots (location, area, MaxFeretDiameter) Selecting green channel from images: JG ← JSKIN, MSG ← MS foreach msi in MSG Cross-correlation calculation: cci = crossCorrelation(JG, msi) Spots detection: dsi = maximaDetection(cci, sensit) Adding detected spots to the list: DS = DS + dsi end Removing duplicated spots: DS = removeDuplications(DS,minDist) Removing spots close to background: DS = removeCloseToBG(DS,JG) Detected spots segmentation: FDS = spotsSegmentation(DS) end |
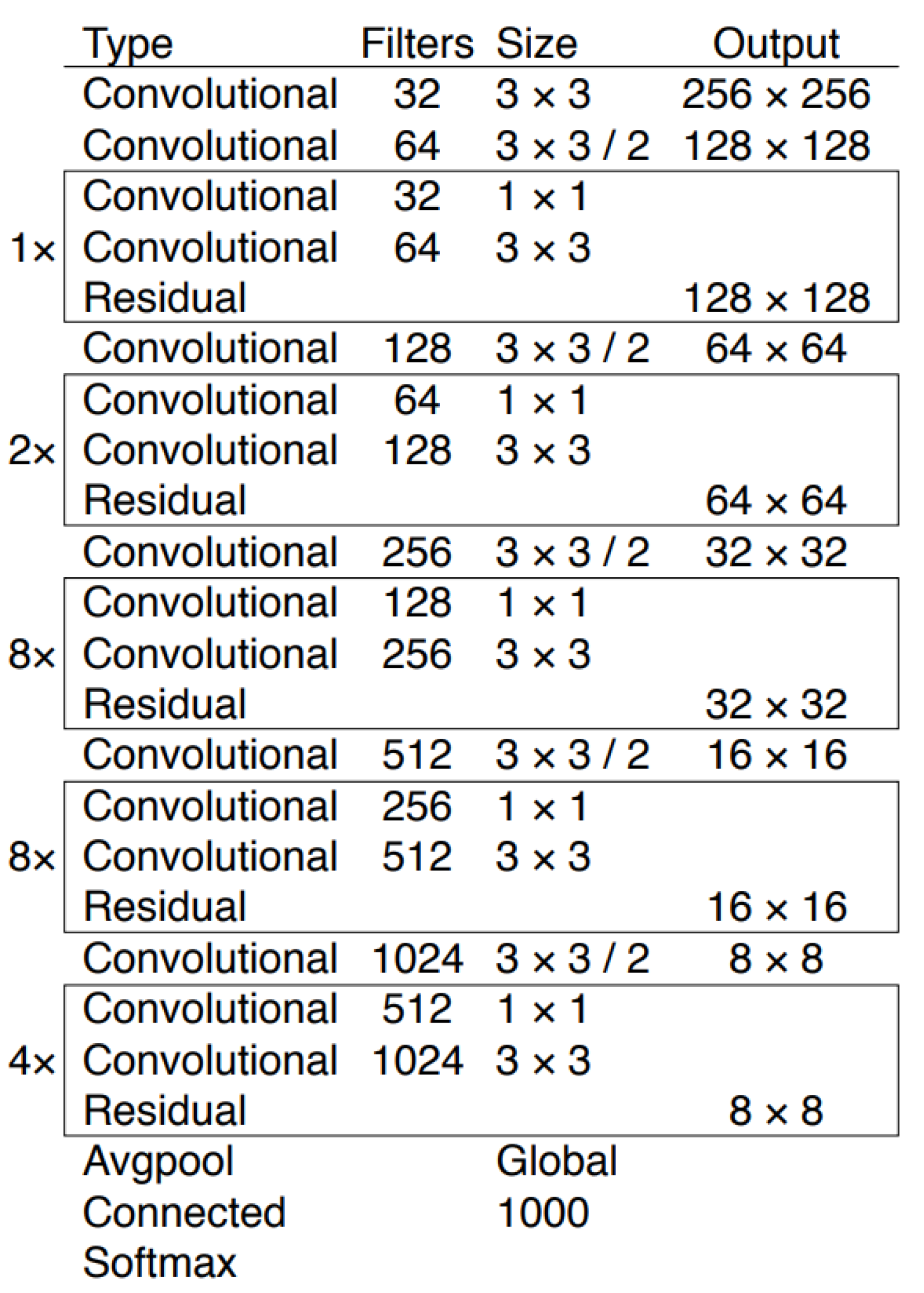
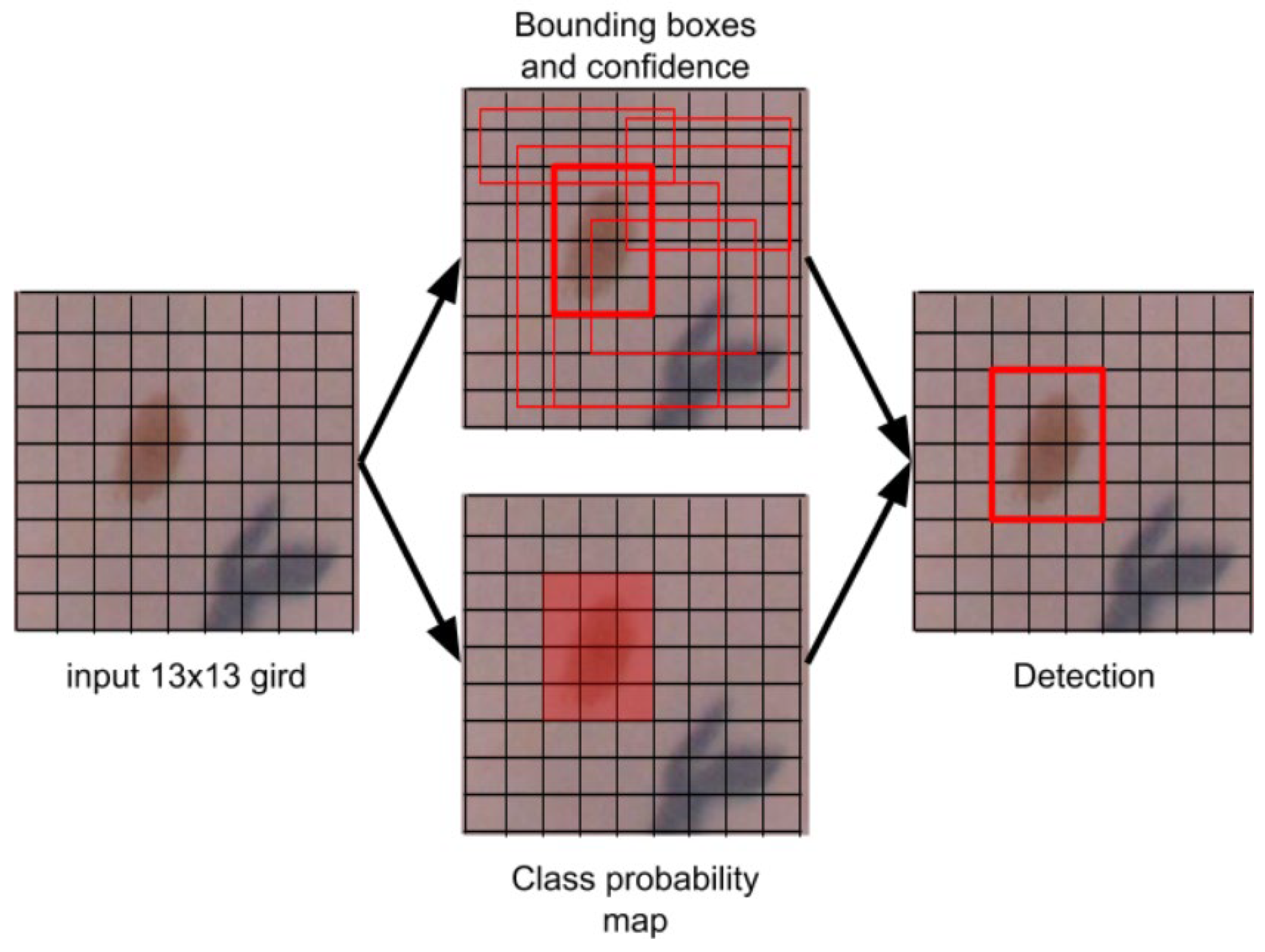
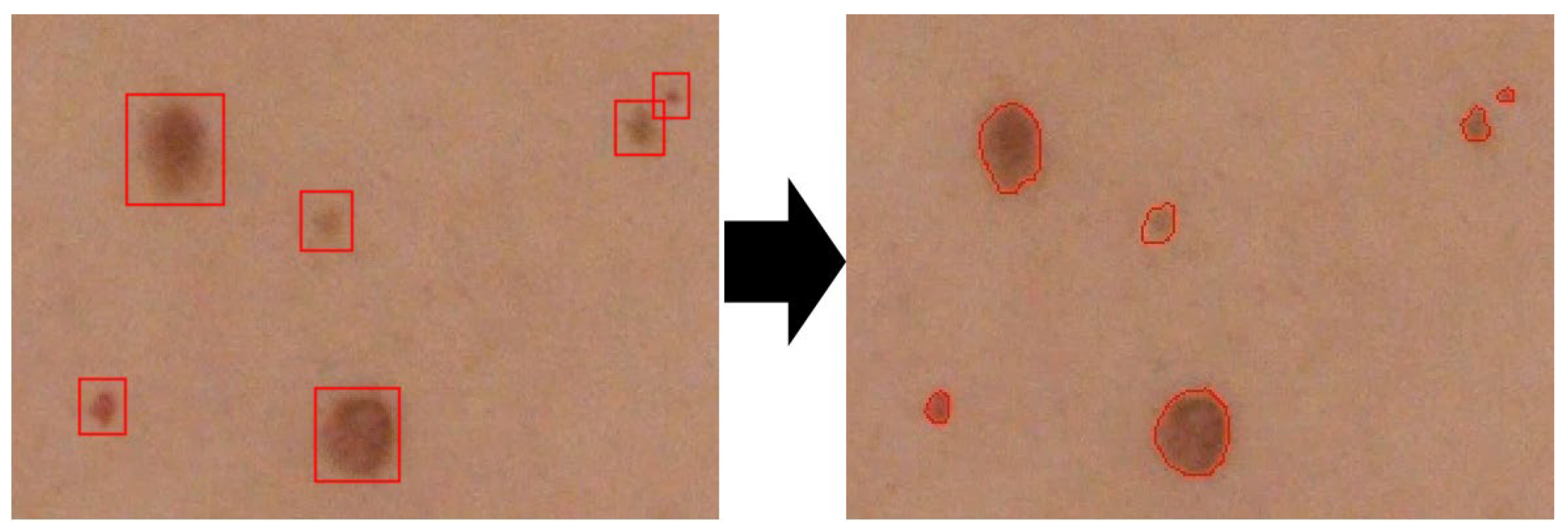
2.2.3. Deep Learning-Based Approach
| Algorithm 3 Spot detection based on CNN |
| Function spotDetectionCNN Data: JSKIN—input RGB image MW—weights of the trained model MC—net configuration Result: FDS—detected spots (location, area, confidencePrediction) Cut the original image into overlapping frames: JFRAMES ← JSKIN foreach jFRAME in JFRAMES Run network and gather predictions lists: NETOUT = netDetections(jFRAME, MW, MC) Add detection to list: NET += netOUT end Removing duplicated detections: NET = removeDuplicationsNMS(NET) foreach net in NET Detected spots segmentation: FDS = spotsSegmentation(net) end end where: netDetections (jFRAME, MW, MC)—the DNN model processes the image frame returning the detections in the form of a bounding box. removeDuplicationsNMS(NET)—Non Maximum Suppression method. spotsSegmentation(net)—processing areas of interest using the Otsu method and median filtering. |
3. Results and Discussion
- —the measured value of the parameter for nevi detected by various methods,
- —the parameter value measured for the outlines of lesion marked by a dermatologist.
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- De Carvalho, T.M.; Noels, E.; Wakkee, M.; Udrea, A.; Nijsten, T. Development of Smartphone Apps for Skin Cancer Risk Assessment: Progress and Promise. J. Med. Internet Res. 2019, 21. [Google Scholar] [CrossRef] [Green Version]
- SkinVision|Skin Cancer Melanoma Detection App. Available online: https://www.skinvision.com/ (accessed on 2 November 2020).
- SpotMole-Apps on Google Play. Available online: https://play.google.com/store/apps/details?id=com.spotmole&gl=PL (accessed on 2 November 2020).
- Ngoo, A.; Finnane, A.; McMeniman, E.; Tan, J.-M.; Janda, M.; Soyer, H.P. Efficacy of Smartphone Applications in High-Risk Pigmented Lesions. Australas. J. Dermatol. 2018, 59, e175–e182. [Google Scholar] [CrossRef] [Green Version]
- Marwaha, S.S.; Fevrier, H.; Alexeeff, S.; Crowley, E.; Haiman, M.; Pham, N.; Tuerk, M.J.; Wukda, D.; Hartmann, M.; Herrinton, L.J. Comparative Effectiveness Study of Face-to-Face and Teledermatology Workflows for Diagnosing Skin Cancer. J. Am. Acad. Dermatol. 2019, 81, 1099–1106. [Google Scholar] [CrossRef]
- Barata, C.; Celebi, M.E.; Marques, J.S. A Survey of Feature Extraction in Dermoscopy Image Analysis of Skin Cancer. IEEE J. Biomed. Health Inform. 2019, 23, 1096–1109. [Google Scholar] [CrossRef]
- Saba, T. Recent Advancement in Cancer Detection Using Machine Learning: Systematic Survey of Decades, Comparisons and Challenges. J. Infect. Public Health 2020, 13, 1274–1289. [Google Scholar] [CrossRef]
- Bi, L.; Kim, J.; Ahn, E.; Kumar, A.; Fulham, M.; Feng, D. Dermoscopic Image Segmentation via Multistage Fully Convolutional Networks. IEEE Trans. Biomed. Eng. 2017, 64, 2065–2074. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brinker, T.J.; Hekler, A.; Enk, A.H.; Klode, J.; Hauschild, A.; Berking, C.; Schilling, B.; Haferkamp, S.; Schadendorf, D.; Fröhling, S.; et al. A Convolutional Neural Network Trained with Dermoscopic Images Performed on Par with 145 Dermatologists in a Clinical Melanoma Image Classification Task. Eur. J. Cancer 2019, 111, 148–154. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Xie, Y.; Xia, Y.; Shen, C. Attention Residual Learning for Skin Lesion Classification. IEEE Trans. Med. Imaging 2019, 38, 2092–2103. [Google Scholar] [CrossRef]
- Liu, Y.; Jain, A.; Eng, C.; Way, D.H.; Lee, K.; Bui, P.; Kanada, K.; Marinho, G.d.O.; Gallegos, J.; Gabriele, S.; et al. A Deep Learning System for Differential Diagnosis of Skin Diseases. Nat. Med. 2020, 26, 900–908. [Google Scholar] [CrossRef] [PubMed]
- Bogo, F.; Romero, J.; Peserico, E.; Black, M.J. Automated Detection of New or Evolving Melanocytic Lesions Using a 3D Body Model. In International Conference on Medical Image Computing and Computer-Assisted Intervention; Golland, P., Hata, N., Barillot, C., Hornegger, J., Howe, R., Eds.; Springer: Cham, Switzerland, 2014; Volume 8673, pp. 593–600. [Google Scholar] [CrossRef] [Green Version]
- Korotkov, K.; Quintana, J.; Puig, S.; Malvehy, J.; Garcia, R. A New Total Body Scanning System for Automatic Change Detection in Multiple Pigmented Skin Lesions. IEEE Trans. Med. Imaging 2015, 34, 317–338. [Google Scholar] [CrossRef] [PubMed]
- Korotkov, K.; Quintana, J.; Campos, R.; Jesús-Silva, A.; Iglesias, P.; Puig, S.; Malvehy, J.; Garcia, R. An Improved Skin Lesion Matching Scheme in Total Body Photography. IEEE J. Biomed. Health Inform. 2019, 23, 586–598. [Google Scholar] [CrossRef]
- Birkenfeld, J.S.; Tucker-Schwartz, J.M.; Soenksen, L.R.; Avilés-Izquierdo, J.A.; Marti-Fuster, B. Computer-Aided Classification of Suspicious Pigmented Lesions Using Wide-Field Images. Comput. Methods Programs Biomed. 2020, 195, 105631. [Google Scholar] [CrossRef]
- Soenksen, L.R.; Kassis, T.; Conover, S.T.; Marti-Fuster, B.; Birkenfeld, J.S.; Tucker-Schwartz, J.; Naseem, A.; Stavert, R.R.; Kim, C.C.; Senna, M.M.; et al. Using Deep Learning for Dermatologist-Level Detection of Suspicious Pigmented Skin Lesions from Wide-Field Images. Sci. Transl. Med. 2021, 13. [Google Scholar] [CrossRef]
- Taeg, S.C.; Freeman, W.T.; Tsao, H. A Reliable Skin Mole Localization Scheme. Proc. IEEE Int. Conf. Comput. Vis. 2007. [Google Scholar] [CrossRef] [Green Version]
- Choudhury, A.K.R. Characteristics of Light Sources. Princ. Colour Appear. Meas. 2014, 1–52. [Google Scholar] [CrossRef]
- Sawicki, D.J.; Miziolek, W. Human Colour Skin Detection in CMYK Colour Space. IET Image Process. 2015, 9, 751–757. [Google Scholar] [CrossRef]
- Abbas, Q.; Celebi, M.E.; García, I.F. Hair Removal Methods: A Comparative Study for Dermoscopy Images. Biomed. Signal Process. Control 2011, 6, 395–404. [Google Scholar] [CrossRef]
- Chan, T.F.; Vese, L.A. Active Contours without Edges. IEEE Trans. Image Process. 2001, 10, 266–277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Redmon, J.; Farhadi, A. Yolov3: An Incremental Improvement. arXiv 2018, arXiv:1804.02767. [Google Scholar]
- Ju, M.; Luo, H.; Wang, Z.; Hui, B.; Chang, Z.; Zhang, X.; Wang, W.; Zhao, Y.; Xie, H. The Application of Improved YOLO V3 in Multi-Scale Target Detection. Appl. Sci. 2019, 9, 3775. [Google Scholar] [CrossRef] [Green Version]
- Redmon, J. Darknet: Open Source Neural Networks in C. 2013–2016. Available online: http://pjreddie.com/darknet/. (accessed on 1 October 2021).
- Zhang, Z.; He, T.; Zhang, H.; Zhang, Z.; Xie, J.; Li, M. Bag of Freebies for Training Object Detection Neural Networks. arXiv 2019, arXiv:1902.04103. [Google Scholar]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. Imagenet Classification with Deep Convolutional Neural Networks. Commun. ACM 2017, 60, 84–90. [Google Scholar] [CrossRef]
- Bodla, N.; Singh, B.; Chellappa, R.; Davis, L.S. Soft-NMS–Improving Object Detection with One Line of Code. In Proceedings of the IEEE International Conference on Computer Vision, Venice, Italy, 22–29 October 2017; pp. 5561–5569. [Google Scholar]
- Otsu, N. A Threshold Selection Method from Gray-Level Histograms. IEEE Trans. Syst. ManCybern. 1979, 9, 62–66. [Google Scholar] [CrossRef] [Green Version]
- Vala, H.J.; Baxi, A. A Review on Otsu Image Segmentation Algorithm. Int. J. Adv. Res. Comput. Eng. Technol. 2013, 2, 387–389. [Google Scholar]
- Abbasi, N.R.; Yancovitz, M.; Gutkowicz-Krusin, D.; Panageas, K.S.; Mihm, M.C.; Googe, P.; King, R.; Prieto, V.; Osman, I.; Friedman, R.J.; et al. Utility of Lesion Diameter in the Clinical Diagnosis of Cutaneous Melanoma. Arch. Dermatol. 2008, 144, 469–474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shields, C.L.; Furuta, M.; Thangappan, A.; Nagori, S.; Mashayekhi, A.; Lally, D.R.; Kelly, C.C.; Rudich, D.S.; Nagori, A.V.; Wakade, O.A.; et al. Metastasis of Uveal Melanoma Millimeter-by-Millimeter in 8033 Consecutive Eyes. Arch. Ophthalmol. 2009, 127, 989–998. [Google Scholar] [CrossRef] [PubMed]
- Bergenmar, M.; Ringborg, U.; Månsson Brahme, E.; Brandberg, Y. Nodular Histogenetic Type—The Most Significant Factor for Thick Melanoma: Implications for Prevention. Melanoma Res. 1998, 8, 403–411. [Google Scholar] [CrossRef]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Size [mm] | Histogram | Correlation | CNN | Fusion (Majority Voting) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T | TP | FN | FP | T | TP | FN | FP | T | TP | FN | FP | T | TP | FN | FP | |
| 1–2 | 626 | 578 | 48 | 635 | 523 | 112 | 619 | 559 | 60 | 623 | 575 | 48 | ||||
| 2–5 | 725 | 705 | 20 | 728 | 704 | 24 | 715 | 700 | 15 | 725 | 712 | 13 | ||||
| >5 | 25 | 24 | 1 | 25 | 24 | 1 | 25 | 24 | 1 | 25 | 24 | 1 | ||||
| All | 1376 | 1307 | 69 | 854 | 1388 | 1251 | 137 | 292 | 1359 | 1283 | 76 | 75 | 1373 | 1311 | 62 | 157 |
| Size [mm] (# Lesions) | Histogram | Correlation | CNN | Fusion (Majority Voting) | ||||
|---|---|---|---|---|---|---|---|---|
| Sensitivity | Precision | Sensitivity | Precision | Sensitivity | Precision | Sensitivity | Precision | |
| 1–2 (628) | 0.92 | 0.82 | 0.90 | 0.92 | ||||
| 2–5 (726) | 0.97 | 0.97 | 0.98 | 0.98 | ||||
| >5 (25) | 0.96 | 0.96 | 0.96 | 0.96 | ||||
| All (1379) | 0.95 | 0.60 | 0.90 | 0.81 | 0.94 | 0.94 | 0.96 | 0.91 |
| Reference | Size [mm] | Sensitivity | Precison |
|---|---|---|---|
| Bogo et al. [12] | 1–3 | 0.90 | 0.50 |
| >5 | 0.90 | 0.80 | |
| Taeg et al. [17] | all | 0.80–0.85 | - |
| Ours (Fusion approach) | 1–2 | 0.92 | - |
| >5 | 0.96 | - | |
| all | 0.96 | 0.91 |
| Size [mm] | Area | Diameter of Equivalent Circle | Ellipse Major Axis | Ellipse Minor Axis | Ellipse Angle | Dice Coefficient | |
|---|---|---|---|---|---|---|---|
| Histogram (brightness distribution) | 1–3 | 24.62 | 12.49 | 0.54 | 14.36 | 16.18 | 0.79 |
| >3 | 14.80 | 8.19 | 0.45 | 8.74 | 10.69 | 0.86 | |
| Correlation (Active contour) | 1–3 | 20.14 | 10.89 | 0.56 | 12.91 | 14.42 | 0.74 |
| >3 | 23.79 | 13.54 | 0.35 | 12.55 | 14.12 | 0.81 | |
| CNN (Otsu threshold.) | 1–3 | 28.53 | 15.99 | 0.47 | 18.27 | 19.65 | 0.77 |
| >3 | 21.72 | 12.46 | 0.51 | 13.09 | 13.17 | 0.79 | |
| Fusion (majority voting) | 1–3 | 24.35 | 15.41 | 0.56 | 16.76 | 24.28 | 0.80 |
| >3 | 9.84 | 4.95 | 0.41 | 7.33 | 8.37 | 0.86 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Strzelecki, M.H.; Strąkowska, M.; Kozłowski, M.; Urbańczyk, T.; Wielowieyska-Szybińska, D.; Kociołek, M. Skin Lesion Detection Algorithms in Whole Body Images. Sensors 2021, 21, 6639. https://doi.org/10.3390/s21196639
Strzelecki MH, Strąkowska M, Kozłowski M, Urbańczyk T, Wielowieyska-Szybińska D, Kociołek M. Skin Lesion Detection Algorithms in Whole Body Images. Sensors. 2021; 21(19):6639. https://doi.org/10.3390/s21196639
Chicago/Turabian StyleStrzelecki, Michał H., Maria Strąkowska, Michał Kozłowski, Tomasz Urbańczyk, Dorota Wielowieyska-Szybińska, and Marcin Kociołek. 2021. "Skin Lesion Detection Algorithms in Whole Body Images" Sensors 21, no. 19: 6639. https://doi.org/10.3390/s21196639
APA StyleStrzelecki, M. H., Strąkowska, M., Kozłowski, M., Urbańczyk, T., Wielowieyska-Szybińska, D., & Kociołek, M. (2021). Skin Lesion Detection Algorithms in Whole Body Images. Sensors, 21(19), 6639. https://doi.org/10.3390/s21196639