
Examination of Potential of Thermopile-Based Contactless Respiratory Gating




Abstract
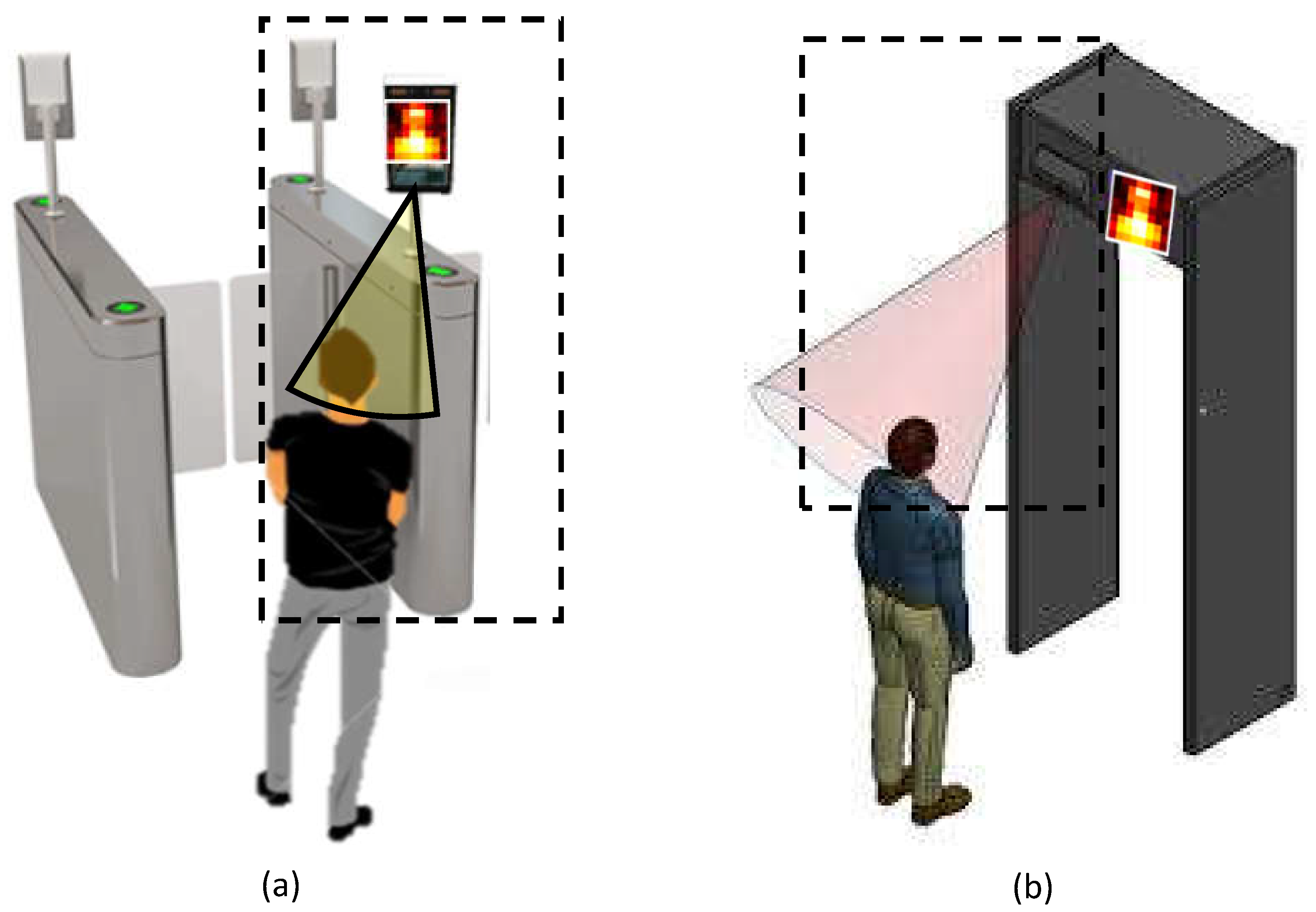
:1. Introduction
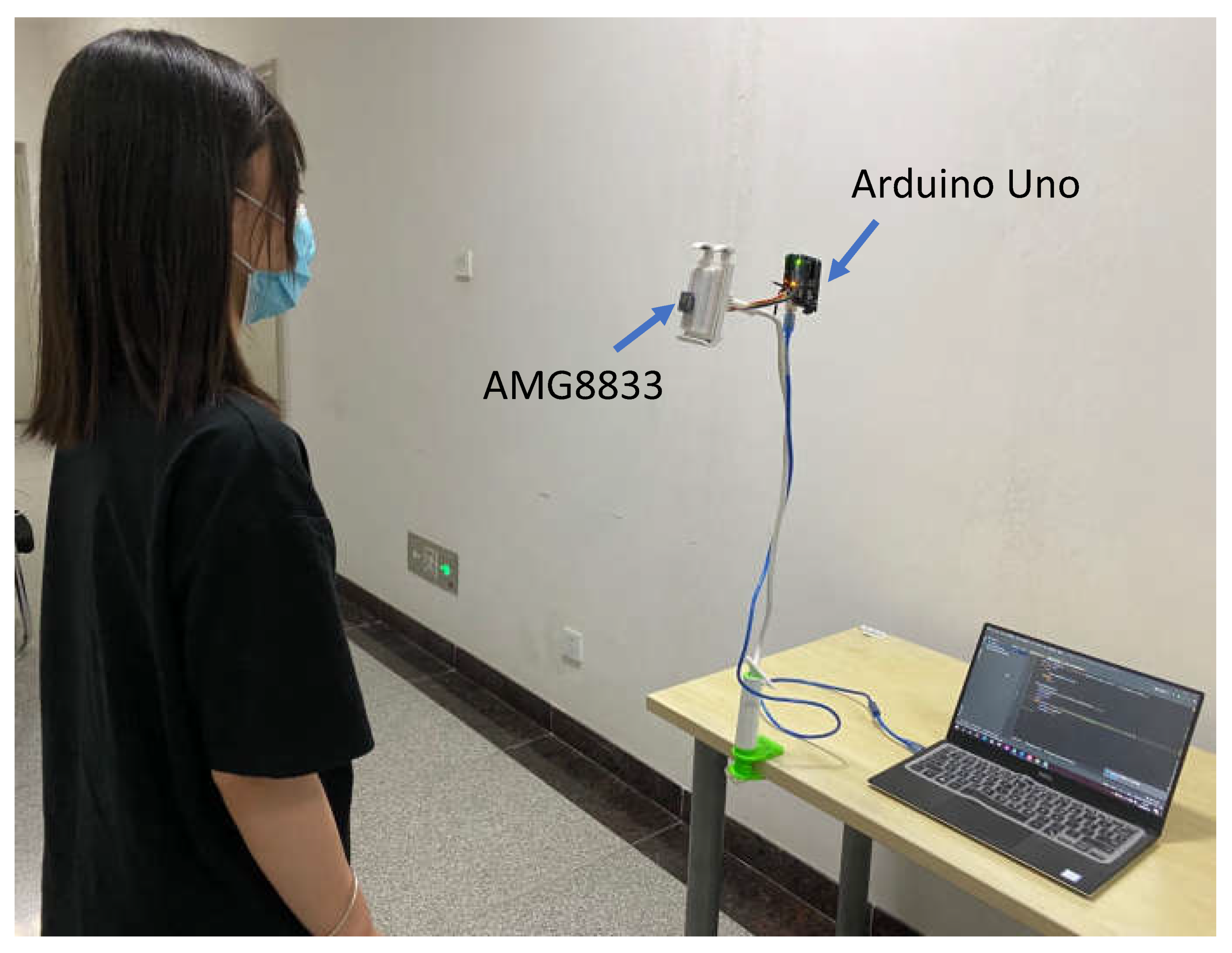
2. Setup and Measurement
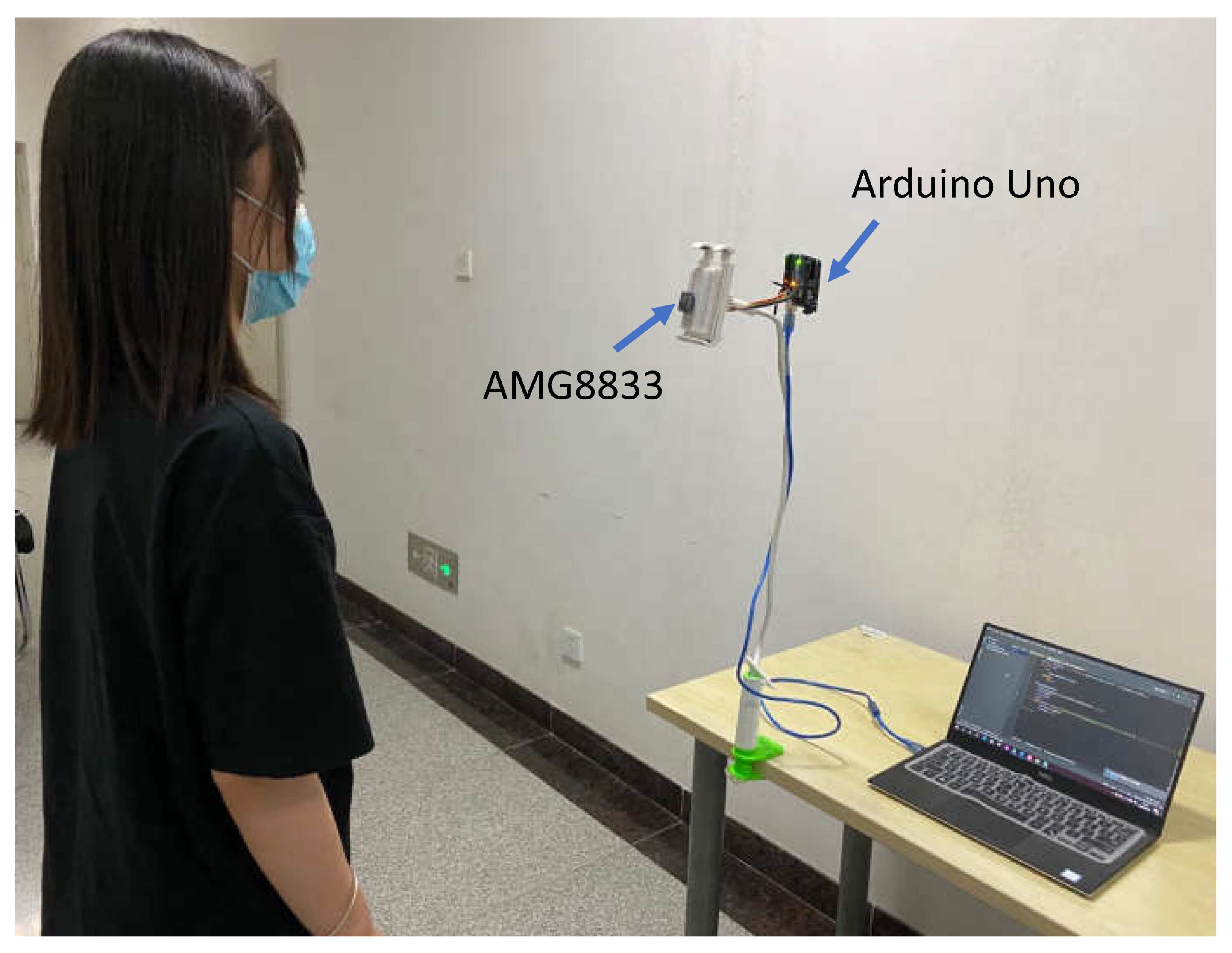
2.1. Experimental Setup
2.2. Benchmark Dataset
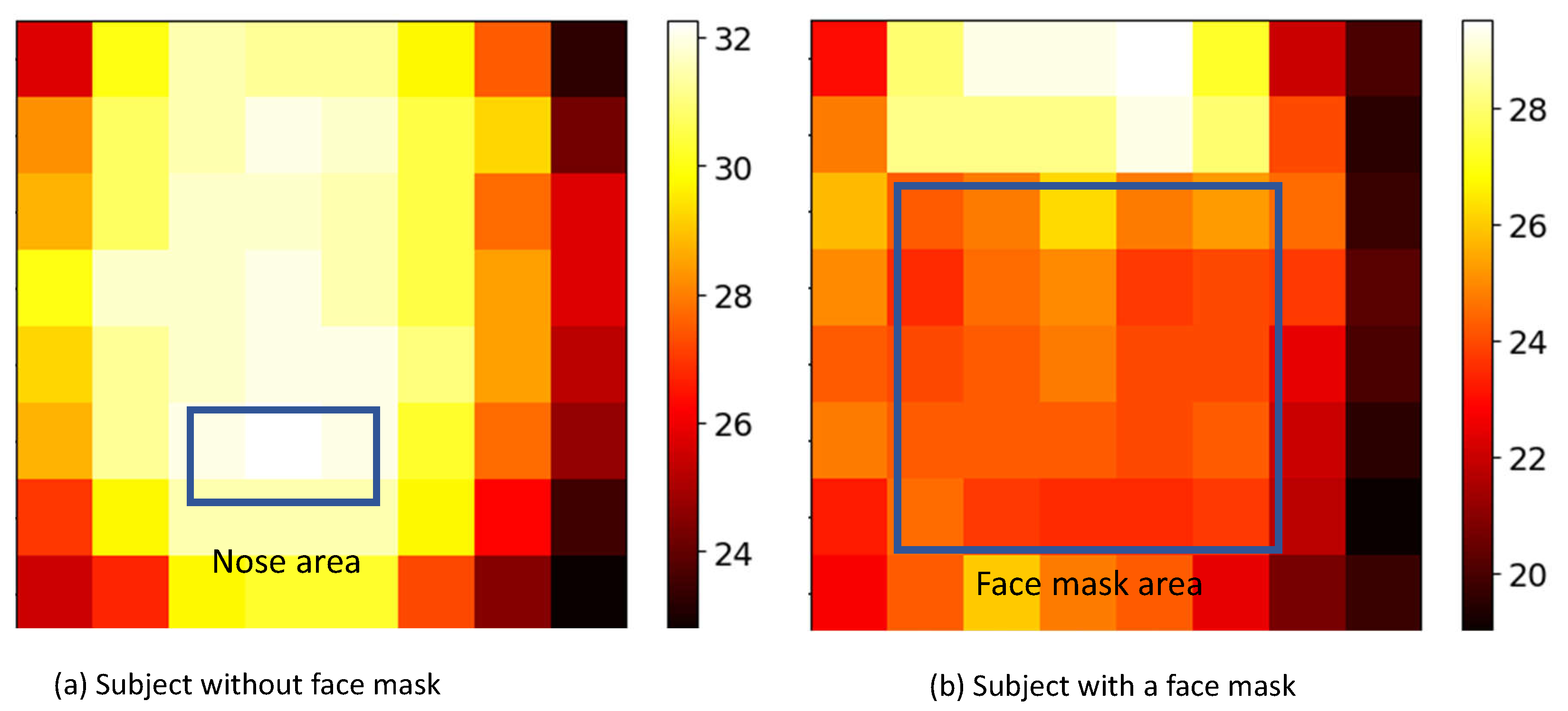
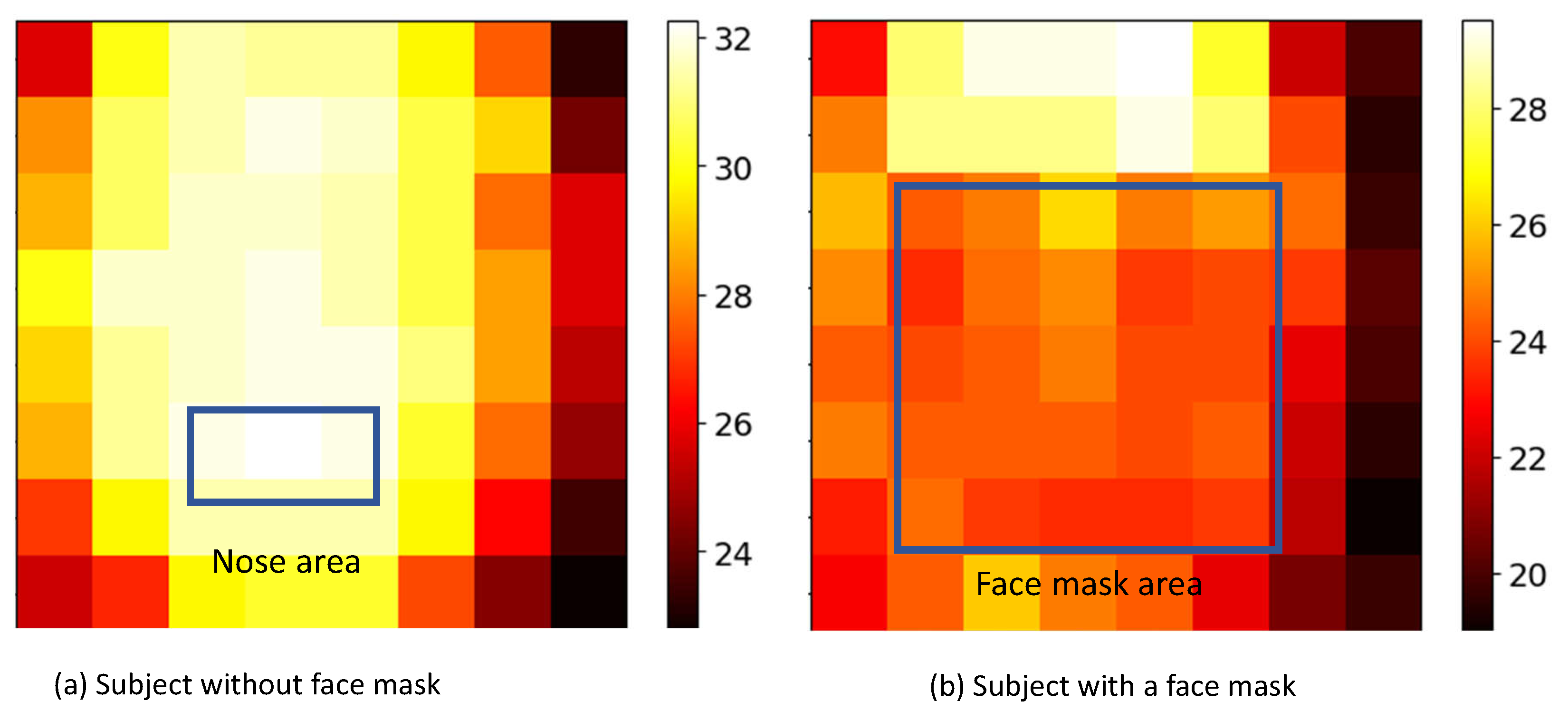
2.2.1. Dataset A: Guided Breathing with and without Face Mask
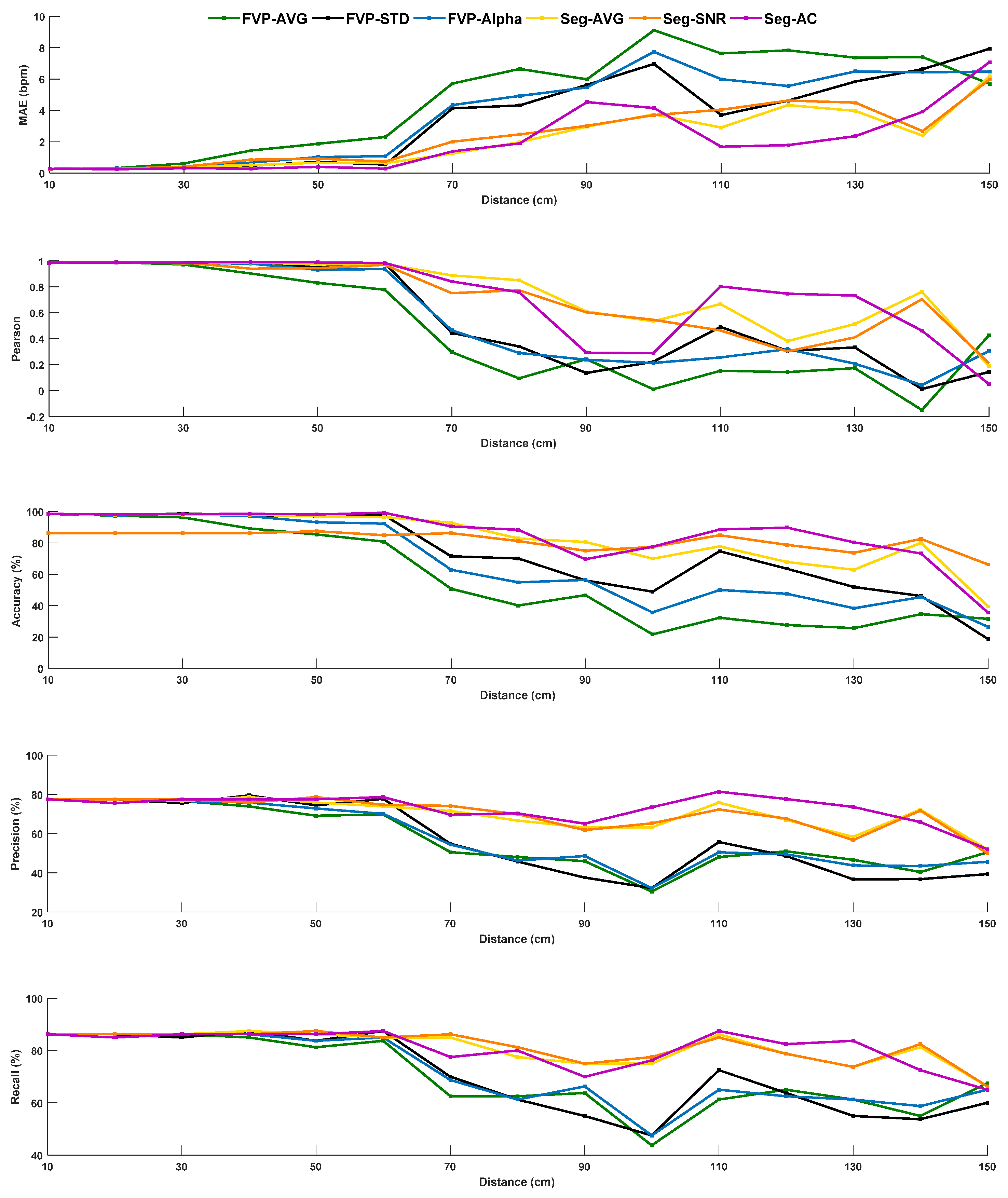
2.2.2. Dataset B: Guided Breathing at Different Subject-to-Sensor Distances (with Face Mask)
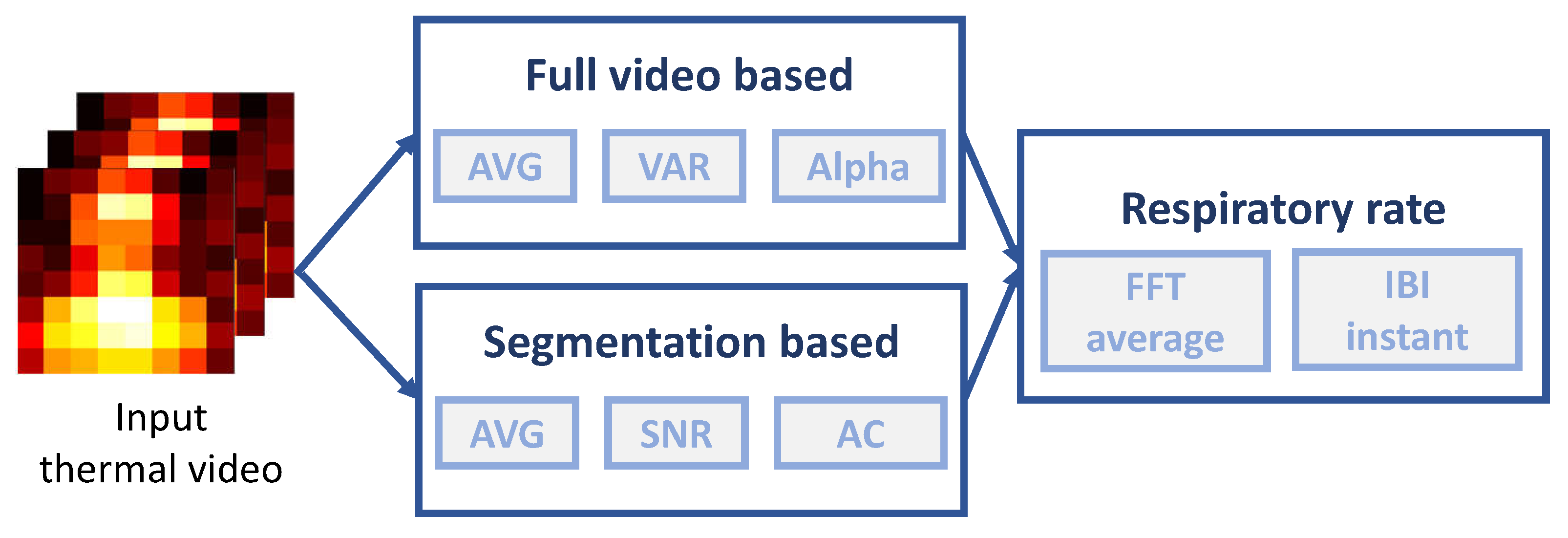
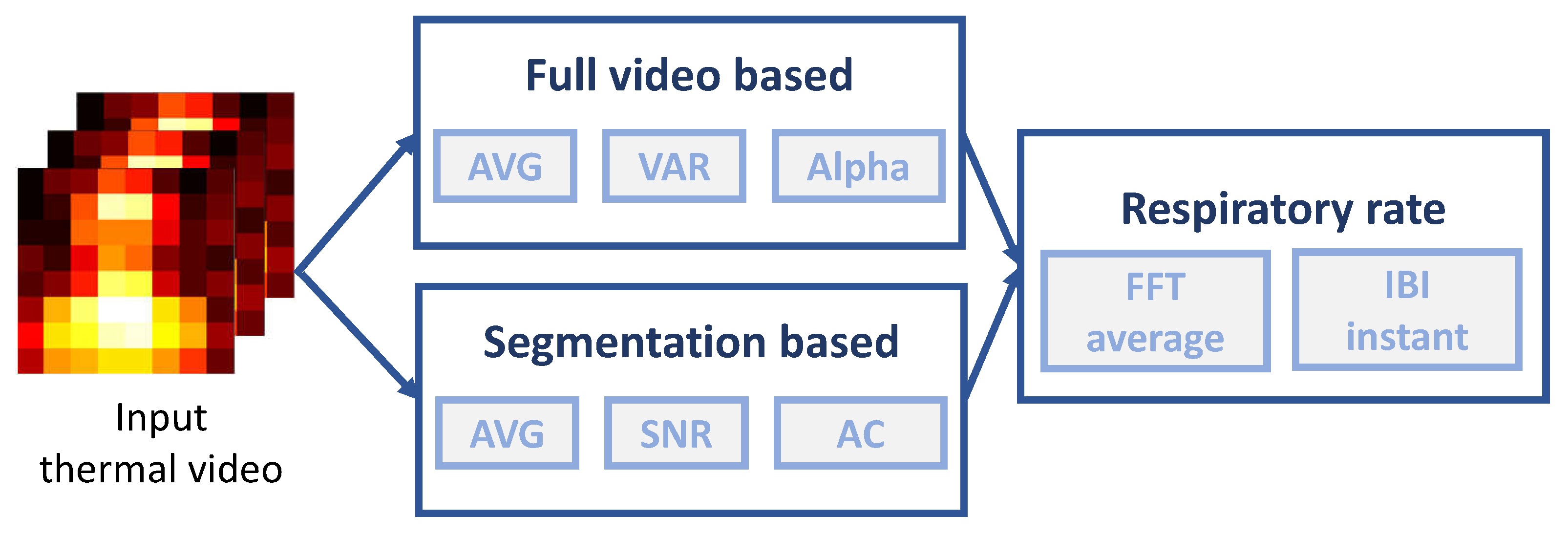
3. Methods
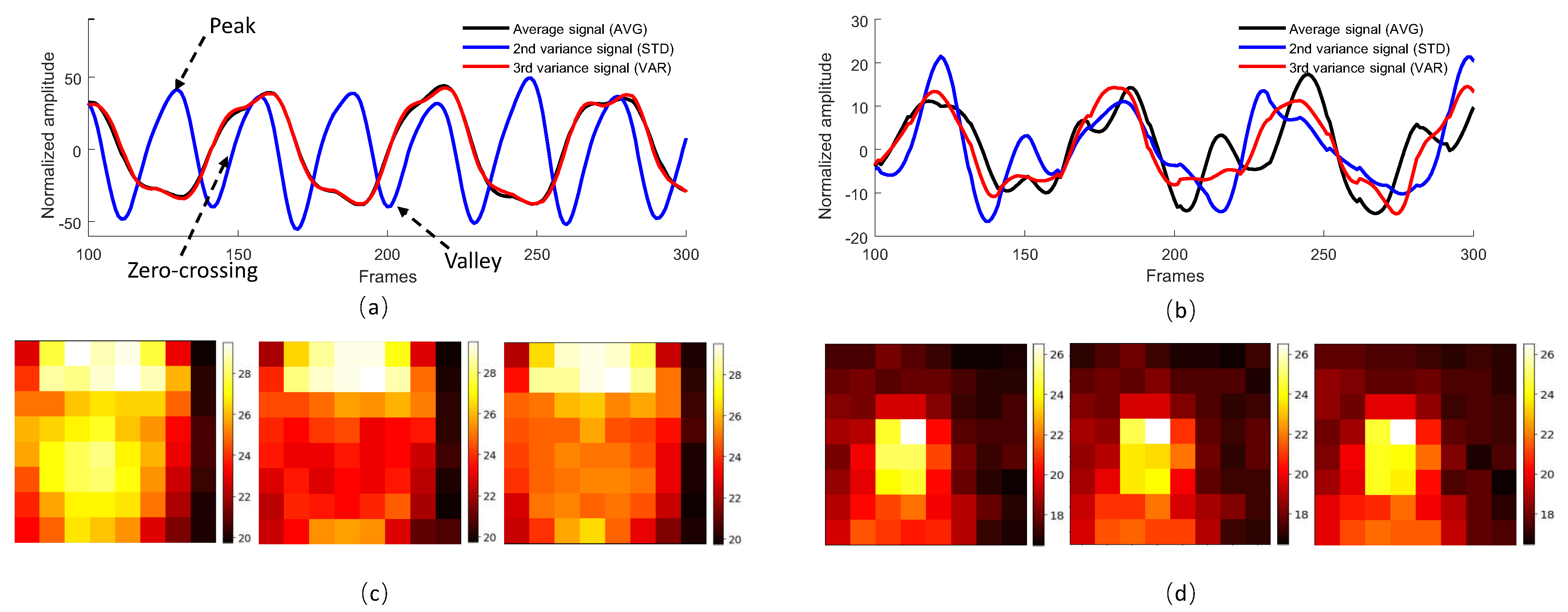
3.1. Full Video Processing-Based Methods (FVP)
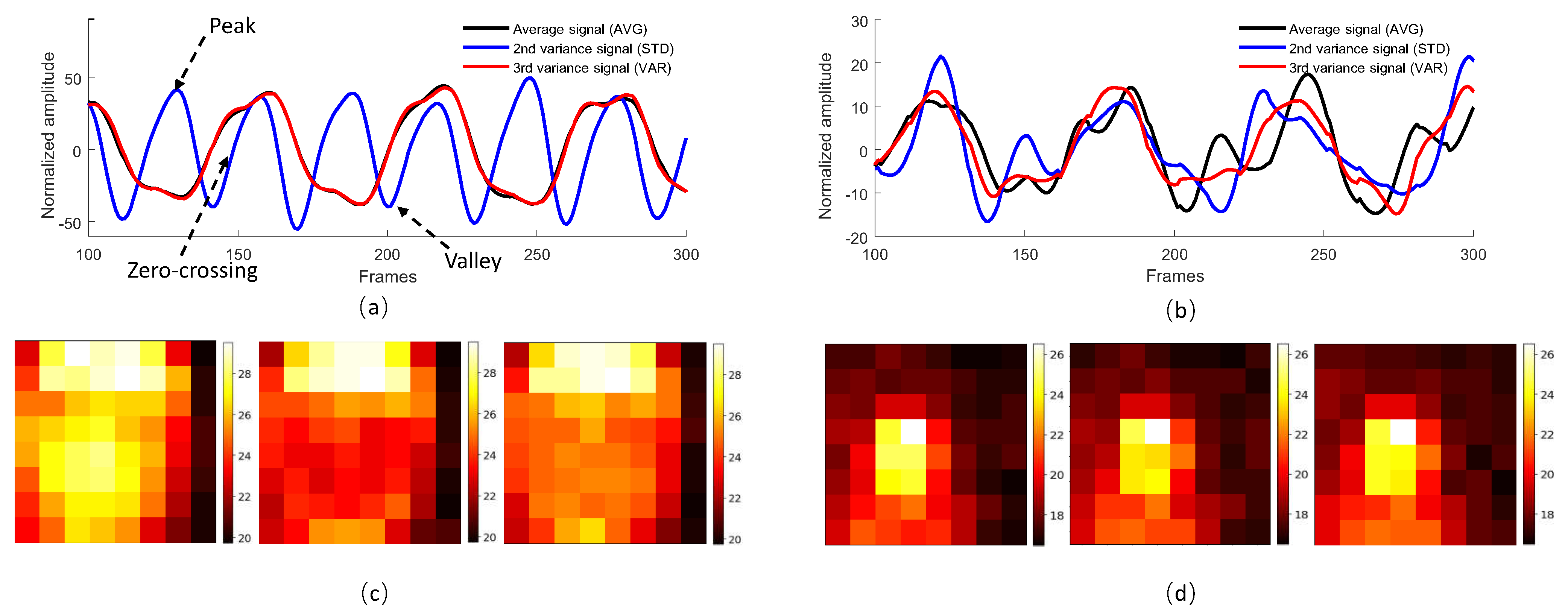
3.1.1. Averaging
3.1.2. Variation
3.1.3. Alpha Tuning
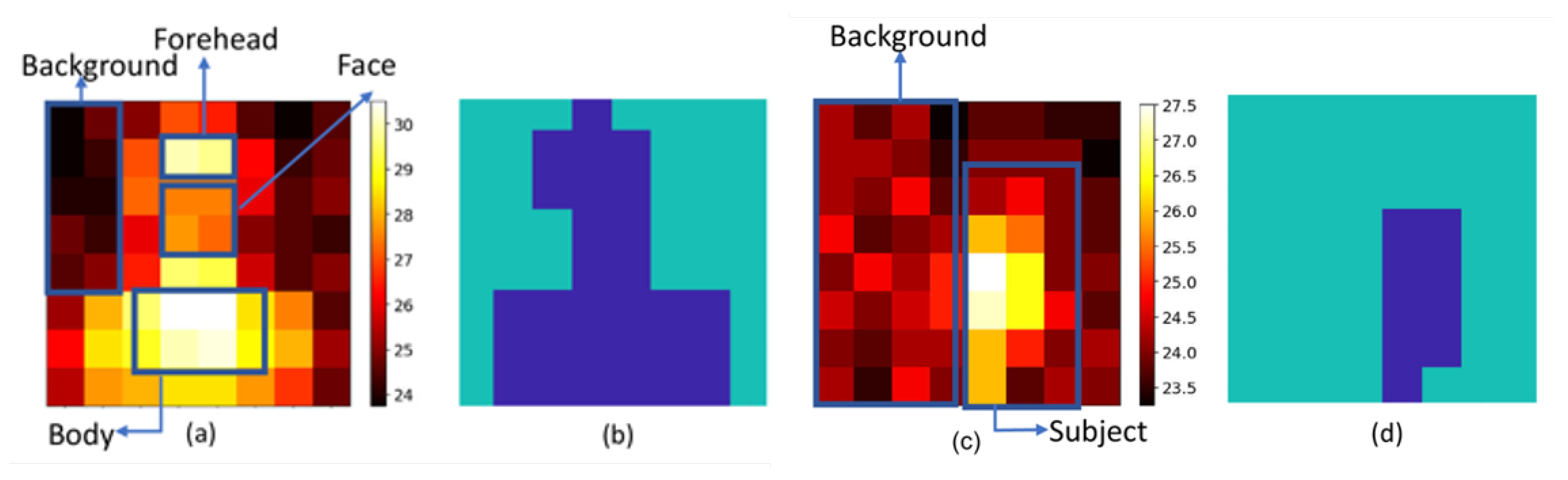
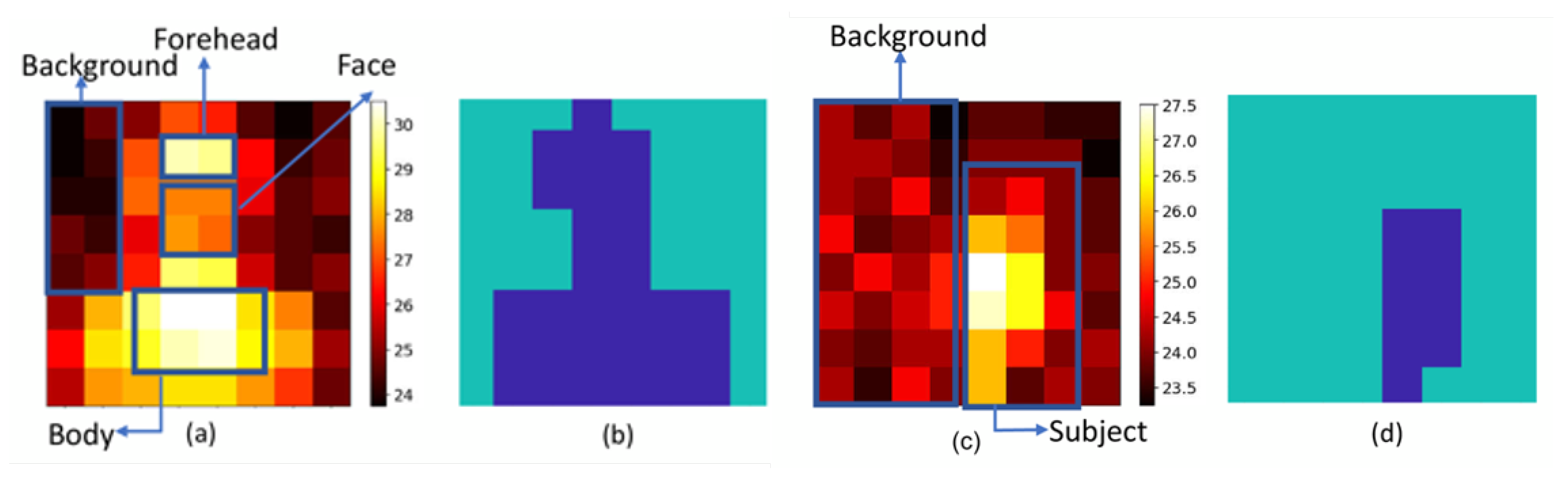
3.2. Segmentation-Based Methods (Seg)
3.2.1. Averaging
3.2.2. SNR
3.2.3. AC
3.3. Respiratory Rate Calculation
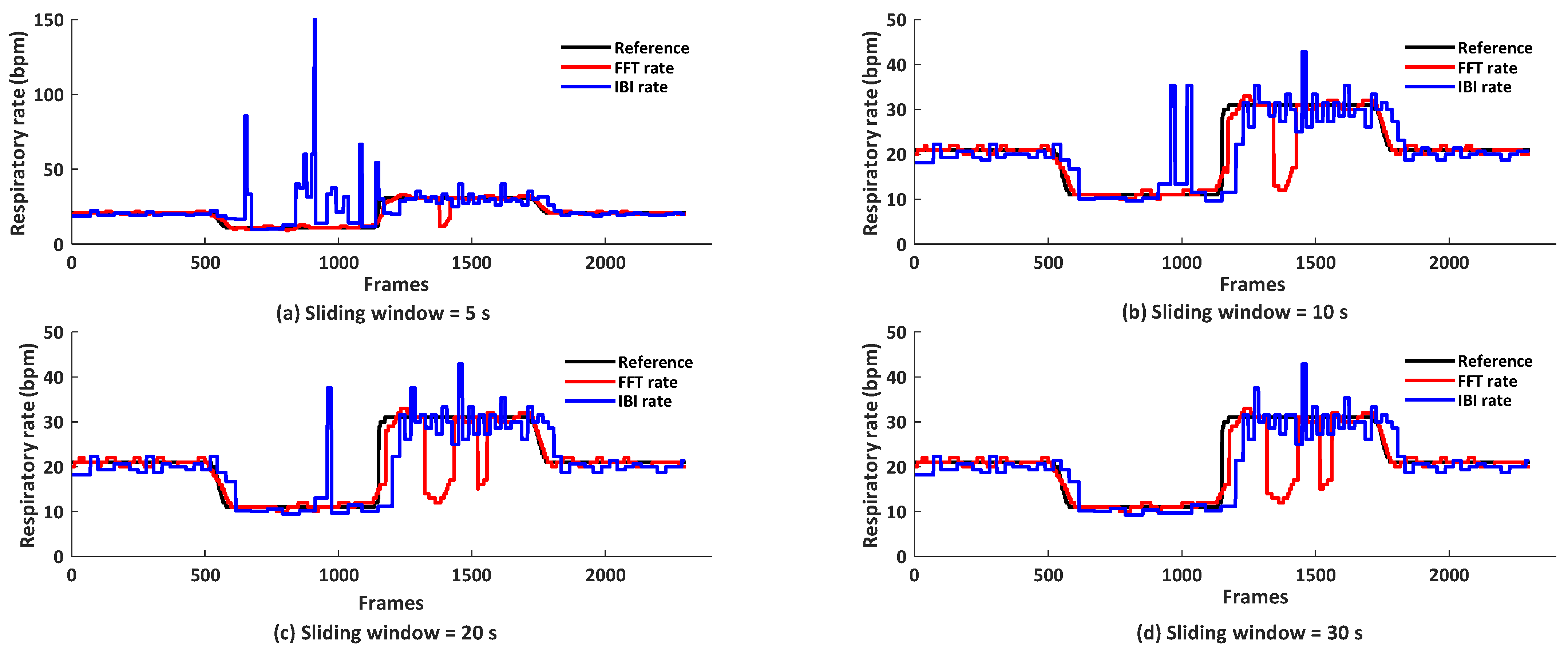
3.3.1. Averaged Respiratory Rate
3.3.2. Instantaneous Respiratory Rate
4. Results and Discussion
4.1. Feasibility of Thermopile-Based Respiratory Gating
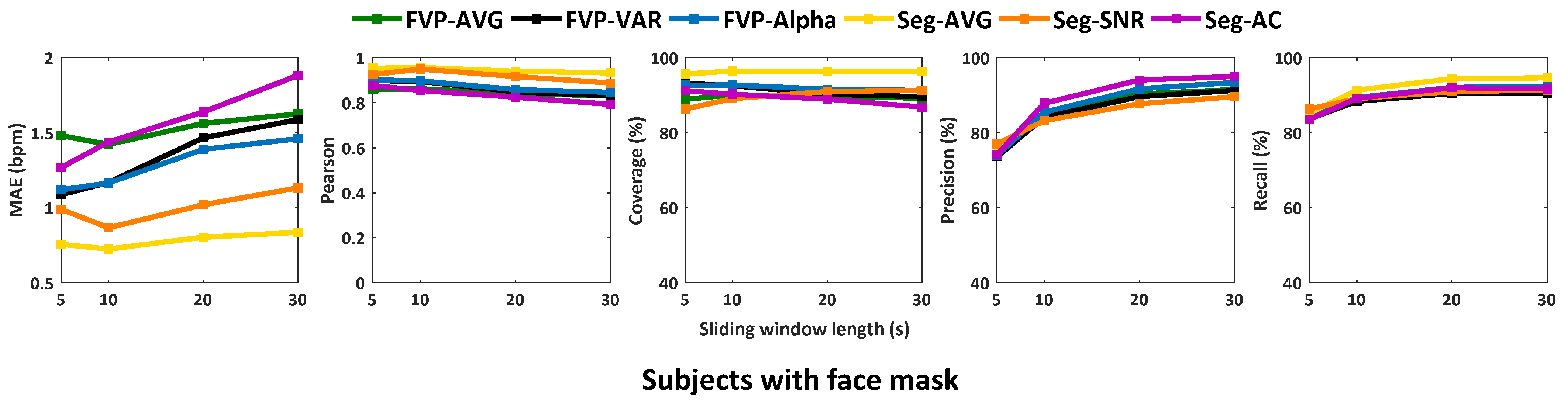
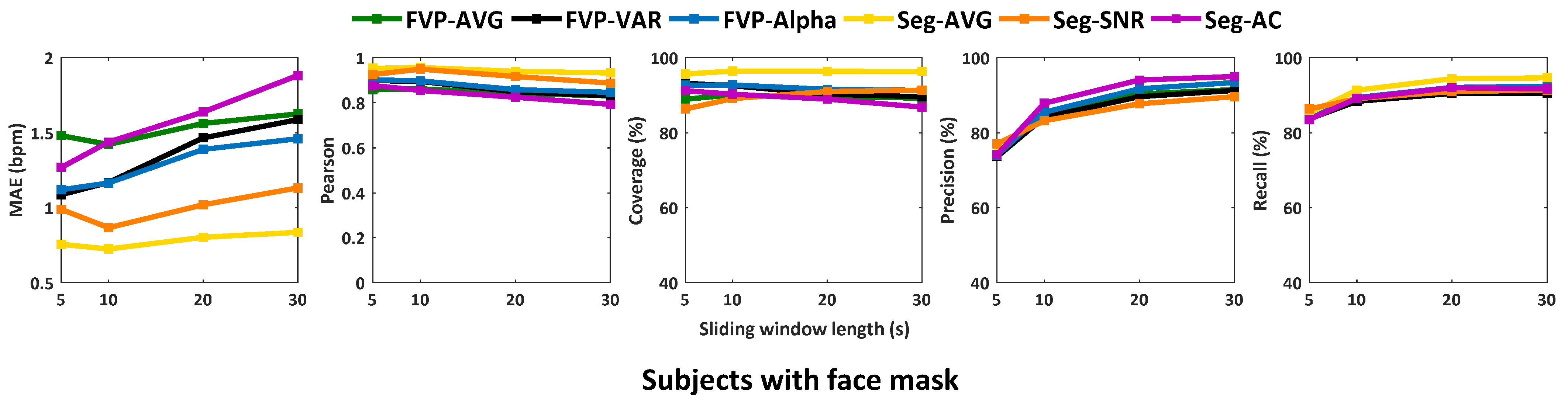
4.2. Analysis of Processing Time Latency (Sliding Window Lengths)
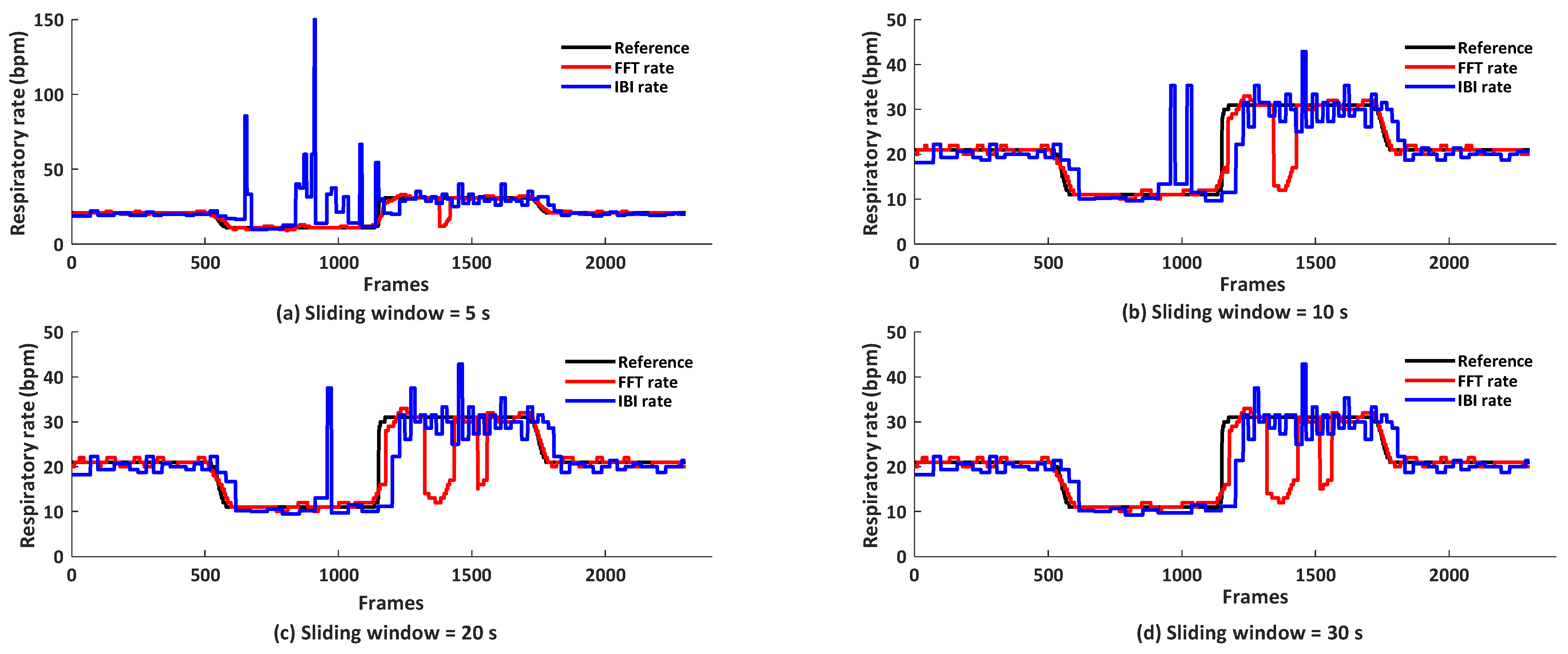
4.3. Analysis of Methods for Respiratory Rate Calculation
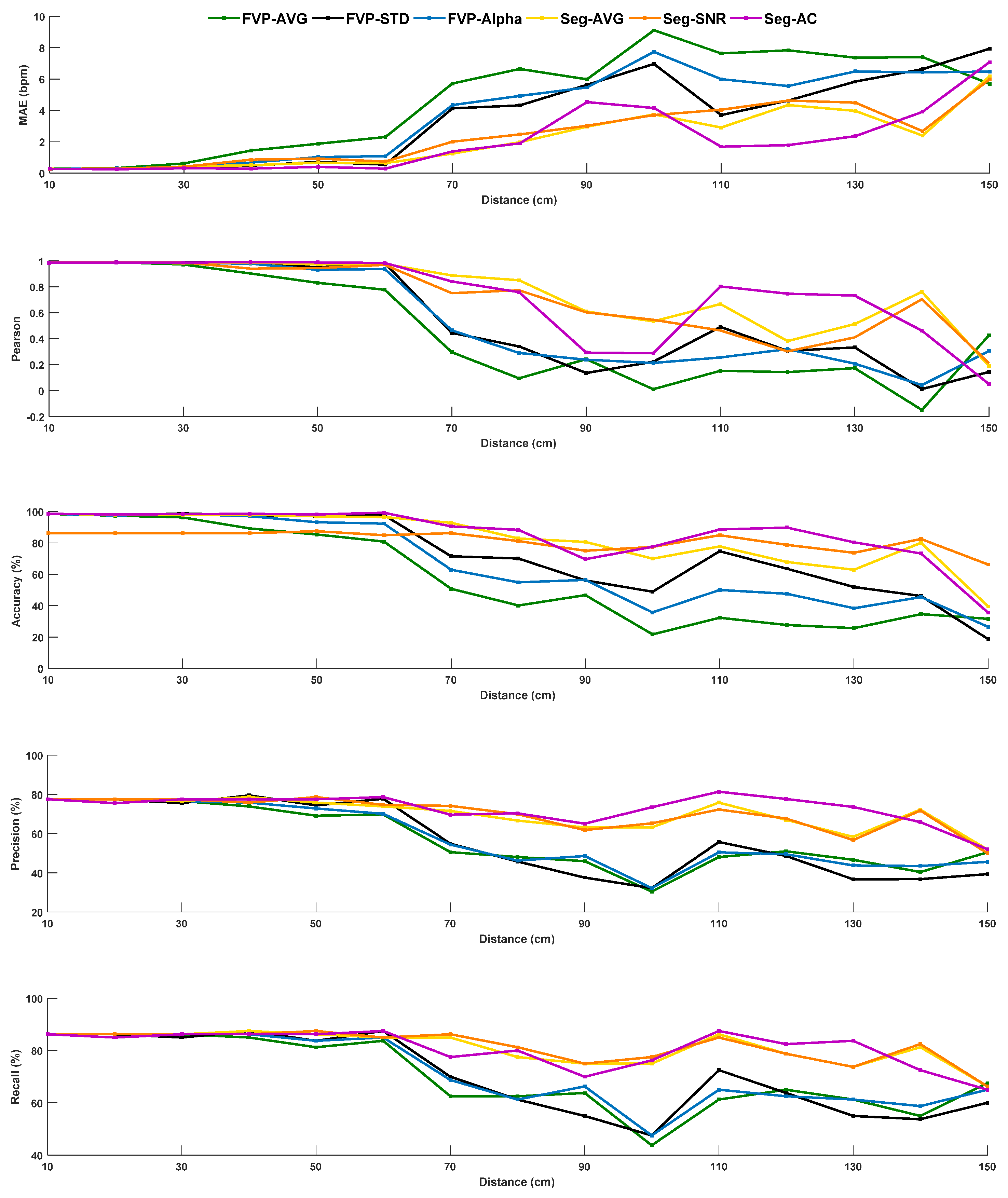
4.4. Distance Range for Respiratory Gating
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Available online: https://www.worldometers.info/coronavirus/ (accessed on 29 July 2021).
- Xu, Z. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet. Resp. Med. 2020, 8, 420–422. [Google Scholar] [CrossRef]
- Xu, R. Saliva: Potential diagnostic value and transmission of 2019-nCoV. Int. J. Oral Sci. 2020, 12, 1–6. [Google Scholar] [CrossRef]
- Leung, N.H. Respiratory virus shedding in exhaled breath and efficacy of face masks. Nat. Med. 2020, 26, 676–680. [Google Scholar] [CrossRef] [Green Version]
- Mohammad, M. Potential effects of coronaviruses on the cardiovascular system: A review. JAMA Cardiol. 2020, 5, 831–840. [Google Scholar]
- Htun, T.P. Clinical features for diagnosis of pneumonia among adults in primary care setting: A systematic and meta-review. Sci. Rep. 2019, 9, 7600. [Google Scholar] [CrossRef] [PubMed]
- Li, M.H.; Yadollahi, A.; Taati, B. A non-contact vision-based system for respiratory rate estimation. In Proceedings of the 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 26–30 August 2014; pp. 2119–2122. [Google Scholar]
- Zhan, Q. Revisiting motion-based respiration measurement from videos. In Proceedings of the 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Montreal, QC, Canada, 20–24 July 2020; pp. 5909–5912. [Google Scholar]
- Bartula, M.; Tigges, T.; Muehlsteff, J. Camera-based system for contactless monitoring of respiration. In Proceedings of the 35th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Osaka, Japan, 3–7 July 2013; pp. 2672–2675. [Google Scholar]
- Aubakir, B.; Nurimbetov, B.; Tursynbek, I. Vital sign monitoring utilizing Eulerian video magnification and thermography. In Proceedings of the 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; pp. 3527–3530. [Google Scholar]
- Tarassenko, L. Non-contact video-based vital sign monitoring using ambient light and auto-regressive models. Physiol. Meas. 2014, 35, 807. [Google Scholar] [CrossRef] [PubMed]
- Poh, M.Z.; McDuff, D.J.; Picard, R.W. Advancements in noncontact, multiparameter physiological measurements using a webcam. IEEE Trans. Biomed. Eng. 2010, 58, 7–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, W.; McDuff, D. Deepphys: Video-based physiological measurement using convolutional attention networks. In Proceedings of the 15th European Conference on Computer Vision, Munich, Germany, 8–14 September 2018; pp. 349–365. [Google Scholar]
- Coşar, S. Thermal Camera Based Physiological Monitoring with an Assistive Robot. In Proceedings of the 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 17–21 July 2018; pp. 5010–5013. [Google Scholar]
- Usman, M. Non-invasive respiration monitoring by thermal imaging to detect sleep apnoea. Med. Biol. Eng. Comput. 2019. Available online: http://shura.shu.ac.uk/id/eprint/24964 (accessed on 28 July 2021).
- Pereira, C.B. Noncontact monitoring of respiratory rate in newborn infants using thermal imaging. IEEE Trans. Biomed. Eng. 2018, 66, 1105–1114. [Google Scholar] [CrossRef]
- Lorato, I. Unobtrusive respiratory flow monitoring using a thermopile array: A feasibility study. Appl. Sci. 2019, 9, 2449. [Google Scholar] [CrossRef] [Green Version]
- Jiang, Z. Detection of Respiratory Infections using RGB-infrared sensors on Portable Device. IEEE Sens. J. 2020, 20, 13674–13681. [Google Scholar] [CrossRef]
- Scebba, G.; Da Poian, G.; Karlen, W. Multispectral Video Fusion for Non-contact Monitoring of Respiratory Rate and Apnea. IEEE Trans. Biomed. Eng. 2020, 68, 350–359. [Google Scholar] [CrossRef]
- Pereira, C.B. Estimation of breathing rate in thermal imaging videos: A pilot study on healthy human subjects. J. Clin. Monit. Comput. 2017, 31, 1241–1254. [Google Scholar] [CrossRef] [PubMed]
- Shetty, A.D.; Toney, G. Detection of intruders in warehouses using Infrared based Thermopile Sensor Array. In Proceedings of the IOP Conference Series Materials Science and Engineering, Nanjing, China, 17–19 August 2018. [Google Scholar]
- Cerutti, G.; Prasad, R.; Farella, E. Convolutional neural network on embedded platform for people presence detection in low resolution thermal images. In Proceedings of the ICASSP 2019—2019 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), Brighton, UK, 12–17 May 2019; pp. 7610–7614. [Google Scholar]
- Cerutti, G.; Milosevic, B.; Farella, E. Outdoor People Detection in Low Resolution Thermal Images. In Proceedings of the 2018 3rd International Conference on Smart and Sustainable Technologies (SpliTech), Split, Croatia, 26–29 June 2018; pp. 1–6. [Google Scholar]
- Hanosh, O. Convulsive Movement Detection Using Low-Resolution Thermopile Sensor Array. In Proceedings of the 2020 IEEE/CVF Conference on Computer Vision and Pattern Recognition Workshops (CVPRW), Seattle, WA, USA, 14–19 June 2020; pp. 300–301. [Google Scholar]
- Chen, Z.; Wang, Y. Infrared-ltrasonic sensor fusion for support vector machine-based fall detection. J. Intell. Mater. Syst. Struct. 2018, 29, 2027–2039. [Google Scholar] [CrossRef]
- Chen, W.H.; Ma, H.P. A fall detection system based on infrared array sensors with tracking capability for the elderly at home. In Proceedings of the 2015 17th International Conference on E-health Networking, Application & Services (HealthCom), Boston, MA, USA, 14–17 October 2015; pp. 428–434. [Google Scholar]
- Chen, Z.; Wang, Y.S. Sleep monitoring using an infrared thermal array sensor. In Proceedings of the Sensors and Smart Structures Technologies for Civil, Mechanical, and Aerospace Systems, Denver, CO, USA, 4–7 March 2019. [Google Scholar] [CrossRef]
- Hsiao, R. Sleeping posture recognition using fuzzy c-means algorithm. Biomed. Eng. Online 2018, 17, 157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hevesi, P. Monitoring household activities and user location with a cheap, unobtrusive thermal sensor array. In Proceedings of the 2014 ACM International Joint Conference on Pervasive and Ubiquitous Computing: Adjunct Publication, New York, NY, USA, 13–17 September 2014; pp. 141–145. [Google Scholar]
- Chiu, S.Y. A Convolutional Neural Networks Approach with Infrared Array Sensor for Bed-Exit Detection. In Proceedings of the 2018 International Conference on System Science and Engineering (ICSSE), New Taipei, Taiwan, 28–30 June 2018; pp. 1–6. [Google Scholar]
- Chen, Z.; Wang, Y.; Liu, H. Unobtrusive Sensor-Based Occupancy Facing Direction Detection and Tracking Using Advanced Machine Learning Algorithms. IEEE Sens. J. 2018, 18, 6360–6368. [Google Scholar] [CrossRef]
- Unakafov, A.M. Pulse rate estimation using imaging photoplethysmography: Generic framework and comparison of methods on a publicly available dataset. Biomed. Phys. Eng. Express 2018, 4, 045001. [Google Scholar] [CrossRef]
- Wang, W.; den Brinker, A.C.; De Haan, G. Full video pulse extraction. Biomed. Opt. Express 2018, 9, 3898–3914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, W.; den Brinker, A.C.; Stuijk, S.; De Haan, G. Algorithmic principles of remote PPG. IEEE Trans. Biomed. Eng. 2016, 64, 1479–1491. [Google Scholar] [CrossRef] [Green Version]
- De Haan, G.; Jeanne, V. Robust pulse rate from chrominance-based rPPG. IEEE Trans. Biomed. Eng. 2013, 60, 2878–2886. [Google Scholar] [CrossRef]
- Feng, L. Dynamic ROI based on K-means for remote photoplethysmography. In Proceedings of the 2015 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), South Brisbane, QLD, Australia, 19–24 April 2015; pp. 1310–1314. [Google Scholar]
- Coleman, G.B.; Andrews, H.C. Image segmentation by clustering. Proc. IEEE 1979, 67, 773–785. [Google Scholar] [CrossRef]
- Wang, W.; Stuijk, S.; De Haan, G. Exploiting spatial redundancy of image sensor for motion robust rPPG. IEEE Trans. Biomed. Eng. 2014, 62, 415–425. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Metric | Mask | FVP | Seg | ||||
|---|---|---|---|---|---|---|---|
| AVG | VAR | Alpha | AVG | SNR | AC | ||
| MAE (bpm) | N | 5.1 | 5.3 | 5.1 | 4.9 | 4.8 | 5.1 |
| Y | 1.5 | 1.3 | 1.3 | 0.8 | 1.0 | 1.6 | |
| Pearson | N | 0.33 | 0.29 | 0.32 | 0.36 | 0.32 | 0.36 |
| Y | 0.85 | 0.87 | 0.88 | 0.95 | 0.92 | 0.84 | |
| Coverage (%) | N | 49.5 | 46.6 | 48.8 | 53.2 | 73.4 | 48.2 |
| Y | 89.5 | 91.4 | 92.1 | 96.2 | 89.5 | 89.4 | |
| Precision (%) | N | 71.4 | 68.5 | 68.9 | 71.3 | 71.2 | 70.1 |
| Y | 85.3 | 84.7 | 86.2 | 87.8 | 84.4 | 87.8 | |
| Recall (%) | N | 72.50 | 69.9 | 71.3 | 73.2 | 73.0 | 70.2 |
| Y | 88.9 | 88.3 | 89.5 | 91.4 | 89.5 | 89.1 | |
| Metric | L = 5 s | L = 10 s | L = 20 s | L = 30 s | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| AVG | SNR | AC | AVG | SNR | AC | AVG | SNR | AC | AVG | SNR | AC | |
| MAE (bpm) | 0.76 | 0.99 | 1.27 | 0.73 | 0.87 | 1.44 | 0.80 | 1.02 | 1.64 | 0.84 | 1.13 | 1.88 |
| Pearson | 0.95 | 0.93 | 0.88 | 0.96 | 0.95 | 0.86 | 0.94 | 0.92 | 0.82 | 0.93 | 0.89 | 0.79 |
| Coverage (%) | 95.7 | 86.4 | 91.2 | 96.5 | 89.1 | 90.3 | 96.4 | 91.0 | 89.0 | 96.4 | 91.4 | 86.9 |
| Precision (%) | 74.9 | 77.1 | 74.2 | 87.8 | 83.2 | 87.9 | 94.0 | 87.8 | 94.0 | 94.7 | 89.6 | 95.0 |
| Recall (%) | 85.2 | 86.4 | 83.6 | 91.4 | 89.1 | 89.2 | 94.4 | 91.0 | 92.0 | 94.7 | 91.4 | 91.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhan, Q.; Wang, W.; Ding, X. Examination of Potential of Thermopile-Based Contactless Respiratory Gating. Sensors 2021, 21, 5525. https://doi.org/10.3390/s21165525
Zhan Q, Wang W, Ding X. Examination of Potential of Thermopile-Based Contactless Respiratory Gating. Sensors. 2021; 21(16):5525. https://doi.org/10.3390/s21165525
Chicago/Turabian StyleZhan, Qi, Wenjin Wang, and Xiaorong Ding. 2021. "Examination of Potential of Thermopile-Based Contactless Respiratory Gating" Sensors 21, no. 16: 5525. https://doi.org/10.3390/s21165525
APA StyleZhan, Q., Wang, W., & Ding, X. (2021). Examination of Potential of Thermopile-Based Contactless Respiratory Gating. Sensors, 21(16), 5525. https://doi.org/10.3390/s21165525