
The Use of a Smartphone Application in Monitoring HRV during an Altitude Training Camp in Professional Female Cyclists: A Preliminary Study

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Design
2.3. Methods
2.4. Statistical Analysis
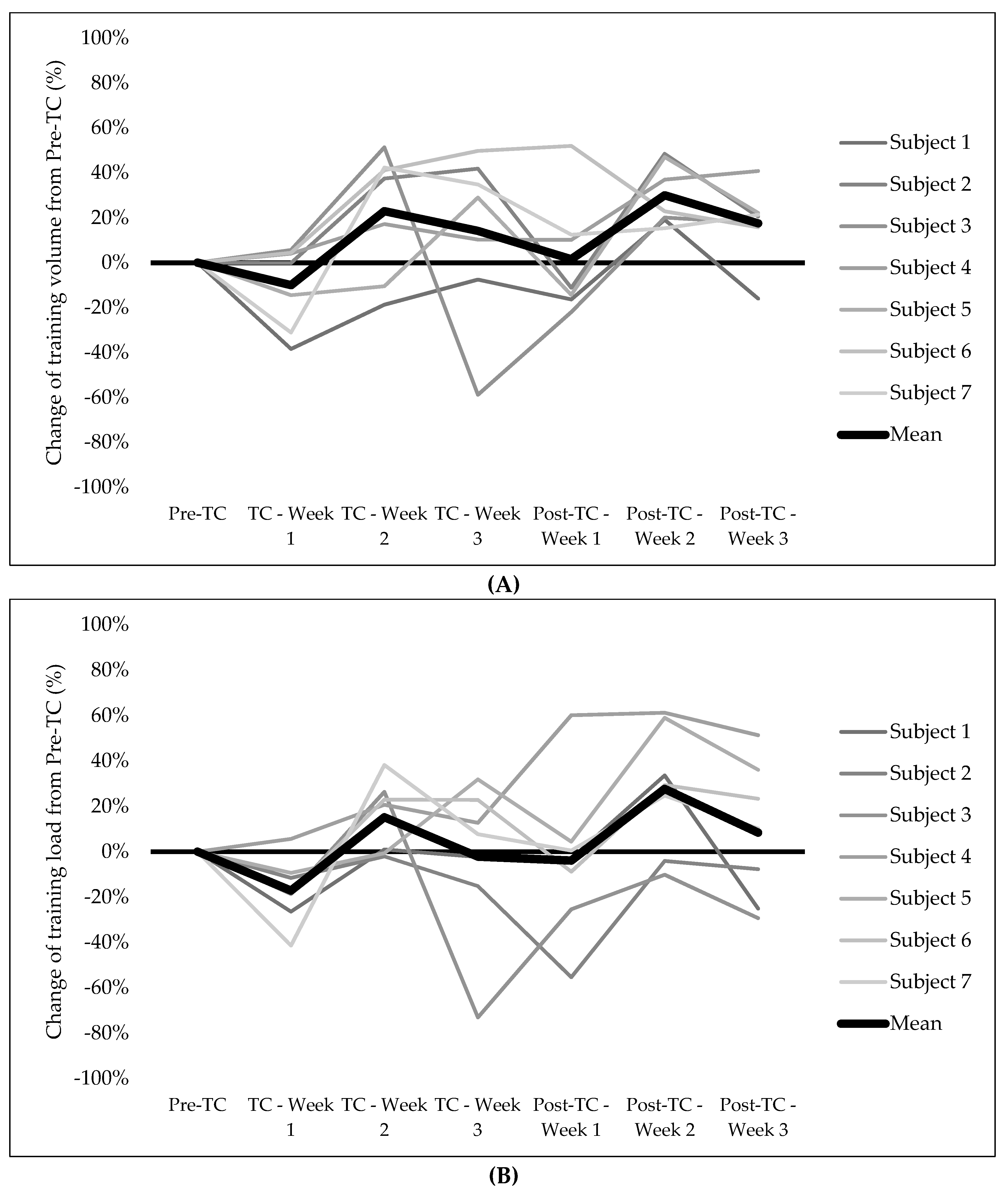
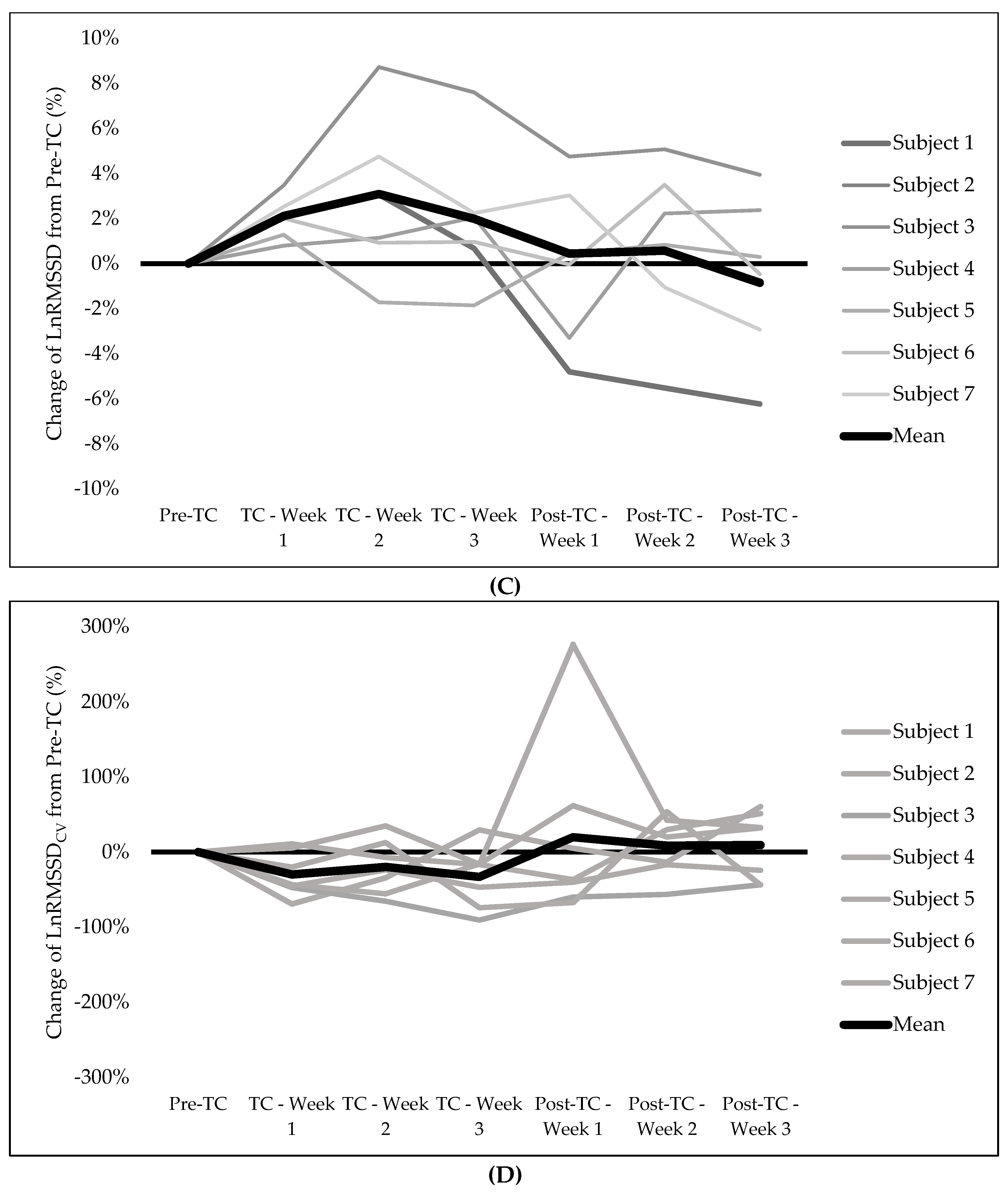
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lundby, C.; Robach, P. Does “altitude training” increase exercise performance in elite athletes? Exp. Physiol. 2016, 101, 783–788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Semenza, G.L. HIF-1: Mediator of physiological and pathophysiological responses to hypoxia. J. Appl. Physiol. 2000, 88, 1474–1480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saunders, P.U.; Garvican-Lewis, L.A.; Schmidt, W.F.; Gore, C.J. Relationship between changes in haemoglobin mass and maximal oxygen uptake after hypoxic exposure. Br. J. Sports Med. 2013, 47 (Suppl. 1), i26–i30. [Google Scholar] [CrossRef]
- Gore, C.J.; Clark, S.A.; Saunders, P.U. Nonhematological mechanisms of improved sea-level performance after hypoxic exposure. Med. Sci. Sports Exerc. 2007, 39, 1600–1609. [Google Scholar] [CrossRef] [PubMed]
- Mujika, I.; Sharma, A.P.; Stellingwerff, T. Contemporary Periodization of Altitude Training for Elite Endurance Athletes: A Narrative Review. Sports Med. 2019, 49, 1651–1669. [Google Scholar] [CrossRef] [PubMed]
- Chapman, R.F.; Karlsen, T.; Resaland, G.K.; Ge, R.L.; Harber, M.P.; Witkowski, S.; Stray-Gundersen, J.; Levine, B.D. Defining the “dose” of altitude training: How high to live for optimal sea level performance enhancement. J. Appl. Physiol. 2014, 116, 595–603. [Google Scholar] [CrossRef] [PubMed]
- Bourdon, P.C.; Cardinale, M.; Murray, A.; Gastin, P.; Kellmann, M.; Varley, M.; Gabbett, T.J.; Coutts, A.J.; Burgess, D.J.; Gregson, W.; et al. Monitoring athlete training loads: Consensus statement. Int. J. Sports Physiol. Perform. 2017, 12 (Suppl. 2), S2-161–S2-170. [Google Scholar] [CrossRef] [PubMed]
- Singh, N.; Moneghetti, K.J.; Christle, J.W.; Hadley, D.; Froelicher, V.; Plews, D. Heart rate variability: An old metric with new meaning in the era of using mHealth technologies for health and exercise training guidance. Part two: Prognosis and training. Arrhythmia Electrophysiol. Rev. Radcl. Cardiol. 2018, 7, 247–255. [Google Scholar] [CrossRef] [PubMed]
- Camm, A.J.; Malik, M.; Bigger, J.T.; Breithardt, G.; Cerutti, S.; Cohen, R.J.; Coumel, P.; Fallen, E.L.; Kennedy, H.L.; Kleiger, R.E.; et al. Heart rate variability: Standards of measurement, physiological interpretation, and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Eur. Heart J. 1996, 17, 354–381. [Google Scholar]
- Oliveira, R.S.; Leicht, A.S.; Bishop, D.; Barbero-Alvarez, J.C.; Nakamura, F.Y. Seasonal changes in physical performance and heart rate variability in high level futsal players. Int. J. Sports Med. 2013, 34, 424–430. [Google Scholar] [CrossRef] [PubMed]
- Abad, C.C.C.; do Nascimento, A.M.; Gil, S.; Kobal, R.; Loturco, I.; Nakamura, F.Y.; Mostarda, C.T.; Irigoyen, M.C. Cardiac autonomic control in high level Brazilian power and endurance track-and-field athletes. Int. J. Sports Med. 2014, 35, 772–778. [Google Scholar] [CrossRef] [PubMed]
- Plews, D.J.; Laursen, P.B.; Buchheit, M. Day-to-day Heart Rate Variability (HRV) Recordings in World Champion Rowers: Appreciating Unique Athlete Characteristics. Int. J. Sports Physiol. Perform. 2016, 12, 697–703. [Google Scholar] [CrossRef] [PubMed]
- Flatt, A.A.; Hornikel, B.; Esco, M.R. Heart rate variability and psychometric responses to overload and tapering in collegiate sprint-swimmers. J. Sci. Med. Sport 2017, 20, 606–610. [Google Scholar] [CrossRef] [PubMed]
- Vesterinen, V.; Häkkinen, K.; Laine, T.; Hynynen, E.; Mikkola, J.; Nummela, A. Predictors of individual adaptation to high-volume or high-intensity endurance training in recreational endurance runners. Scand. J. Med. Sci. Sports 2016, 26, 885–893. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, L.; Regnard, J.; Parmentier, A.L.; Mauny, F.; Mourot, L.; Coulmy, N.; Millet, G.P. Typology of “Fatigue” by Heart Rate Variability Analysis in Elite Nordic-skiers. Int. J. Sports Med. 2015, 36, 999–1007. [Google Scholar] [CrossRef] [PubMed]
- Flatt, A.A.; Howells, D. Effects of varying training load on heart rate variability and running performance among an Olympic rugby sevens team. J. Sci. Med. Sport 2019, 22, 222–226. [Google Scholar] [CrossRef] [PubMed]
- Barrero, A.; Schnell, F.; Carrault, G.; Kervio, G.; Matelot, D.; Carré, F.; Le Douairon Lahaye, S. Daily fatigue-recovery balance monitoring with heart rate variability in well-trained female cyclists on the Tour de France circuit. PLoS ONE 2019, 14, e0213472. [Google Scholar] [CrossRef]
- Figueiredo, D.H.; Figueiredo, D.H.; Moreira, A.; Gonçalves, H.R.; Stanganelli, L.C. Effect of Overload and Tapering on Individual Heart Rate Variability, Stress Tolerance, and Intermittent Running Performance in Soccer Players During a Preseason. J. Strength Cond. Res. 2019, 33, 1222–1231. [Google Scholar] [CrossRef]
- Sanz-Quinto, S.; López-Grueso, R.; Brizuela, G.; Flatt, A.A.; Moya-Ramón, M. Influence of Training Models at 3900-m Altitude on the Physiological Response and Performance of a Professional Wheelchair Athlete: A Case Study. J. Strength Cond. Res. 2019, 33, 1714–1722. [Google Scholar] [CrossRef]
- Yamamoto, Y.; Hoshikawa, Y.; Miyashita, M. Effects of acute exposure to simulated altitude on heart rate variability during exercise. J. Appl. Physiol. 1996, 81, 1223–1229. [Google Scholar] [CrossRef] [PubMed]
- Bhattarai, P.; Paudel, B.H.; Thakur, D.; Bhattarai, B.; Subedi, B.; Khadka, R. Effect of long term high altitude exposure on cardiovascular autonomic adjustment during rest and post-exercise recovery. Ann. Occup. Environ. Med. 2018, 30, 34. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, L.; Willis, S.J.; Fardel, A.; Coulmy, N.; Millet, G.P. Live high-train low guided by daily heart rate variability in elite Nordic-skiers. Eur. J. Appl. Physiol. 2018, 118, 419–428. [Google Scholar] [CrossRef]
- Nakamura, F.Y.; Pereira, L.A.; Esco, M.R.; Flatt, A.A.; Moraes, J.E.; Abad, C.C.C.; Loturco, I. Intra- and inter-day reliability of ultra-short-term heart rate variability in rugby union players. J. Strength Cond. Res. 2016, 31, 548–551. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, F.Y.; Flatt, A.A.; Pereira, L.; Ramirez-Campillo, R.; Loturco, I.; Esco, M.R. Ultra-Short-Term Heart Rate Variability is Sensitive to Training Effects in Team Sports Players. J. Sports Sci. Med. 2015, 14, 602–605. [Google Scholar]
- Dobbs, W.C.; Fedewa, M.V.; MacDonald, H.; Holmes, C.J.; Cicone, Z.S.; Plews, D.J.; Esco, M.R. The Accuracy of Acquiring Heart Rate Variability from Portable Devices: A Systematic Review and Meta-Analysis. Sports Med. 2019, 49, 417–435. [Google Scholar] [CrossRef] [PubMed]
- Plews, D.J.; Scott, B.; Altini, M.; Wood, M.; Kilding, A.E.; Laursen, P.B. Comparison of heart-rate-variability recording with smartphone photoplethysmography, Polar H7 chest strap, and electrocardiography. Int. J. Sports Physiol. Perform. 2017, 12, 1324–1328. [Google Scholar] [CrossRef] [PubMed]
- Flatt, A.A.; Esco, M.R. Smartphone-derived heart-rate variability and training load in a women’s soccer team. Int. J. Sports Physiol. Perform. 2015, 10, 994–1000. [Google Scholar] [CrossRef]
- Javaloyes, A.; Sarabia, J.M.; Lamberts, R.P.; Moya-Ramon, M. Training prescription guided by heart-rate variability in cycling. Int. J. Sports Physiol. Perform. 2019, 14, 23–32. [Google Scholar] [CrossRef] [Green Version]
- Maier, T.; Schmid, L.; Müller, B.; Steiner, T.; Wehrlin, J.P. Accuracy of cycling power meters against a mathematical model of treadmill cycling. Int. J. Sports Med. 2017, 38, 456–461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allen, H.; Coggan, A. Training and Racing with a Power Meter; VeloPress: Boulder, CO, USA, 2010; 326p. [Google Scholar]
- Van Erp, T.; Sanders, D. Demands of professional cycling races: Influence of race category and result. Eur. J. Sport Sci. 2020, 21, 666–677. [Google Scholar] [CrossRef]
- Esco, M.R.; Flatt, A.A. Ultra-short-term heart rate variability indexes at rest and post-exercise in athletes: Evaluating the agreement with accepted recommendations. J. Sports Sci. Med. 2014, 13, 535–541. [Google Scholar] [PubMed]
- Plews, D.J.; Laursen, P.B.; Le Meur, Y.; Hausswirth, C.; Kilding, A.E.; Buchheit, M. Monitoring training with heart rate-variability: How much compliance is needed for valid assessment? Int. J. Sports Physiol. Perform. 2014, 9, 783–790. [Google Scholar] [CrossRef]
- Plews, D.J.; Laursen, P.B.; Kilding, A.E.; Buchheit, M. Heart-rate variability and training-intensity distribution in elite rowers. Int. J. Sports Physiol. Perform. 2014, 9, 1026–1032. [Google Scholar] [CrossRef]
- Singh, N.; Moneghetti, K.J.; Christle, J.W.; Hadley, D.; Plews, D.; Froelicher, V. Heart rate variability: An old metric with new meaning in the era of using mhealth technologies for health and exercise training guidance. Part one: Physiology and methods. Arrhythmia Electrophysiol. Rev. Radcl. Cardiol. 2018, 7, 193–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buchheit, M.; Simon, C.; Piquard, F.; Ehrhart, J.; Brandenberger, G. Effects of increased training load on vagal-related indexes of heart rate variability: A novel sleep approach. Am. J. Physiol. Circ. Physiol. 2004, 287, H2813–H2818. [Google Scholar] [CrossRef] [Green Version]
- González-Fimbres, R.A.; Hernández-Cruz, G.; Flatt, A.A. Ultrashort Versus Criterion Heart Rate Variability Among International-Level Girls’ Field Hockey Players. Int. J. Sports Physiol. Perform. 2021, 16, 985–992. [Google Scholar] [CrossRef] [PubMed]
- Van Erp, T.; Sanders, D.; De Koning, J.J. Training Characteristics of Male and Female Professional Road Cyclists: A 4-Year Retrospective Analysis. Int. J. Sports Physiol. Perform. 2019, 15, 534–540. [Google Scholar] [CrossRef] [PubMed]
- Sztajzel, J.; Jung, M.; Sievert, K.; De Luna, A.B. Cardiac autonomic profile in different sports disciplines during all-day activity. J. Sports Med. Phys. Fit. 2008, 48, 495–501. [Google Scholar]
- Flatt, A.A.; Esco, M.R.; Nakamura, F.Y.; Plews, D.J. Interpreting daily heart rate variability changes in collegiate female soccer players. J. Sports Med. Phys. Fit. 2016, 57, 907–915. [Google Scholar]
- Kiviniemi, A.M.; Hautala, A.J.; Kinnunen, H.; Tulppo, M.P. Endurance training guided individually by daily heart rate variability measurements. Eur. J. Appl. Physiol. 2007, 101, 743–751. [Google Scholar] [CrossRef] [PubMed]
- Achten, J.; Jeukendrup, A.E. Heart rate monitoring: Applications and limitations. Sports Med. 2003, 33, 517–538. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Pre-TC | TC | Post-TC | Statistical Comparisons | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre-TC vs. TC | TC vs. Post-TC | Pre-TC vs. Post-TC | ||||||||||
| F | p | η2 | p | SMD | p | SMD | p | SMD | ||||
| Training volume (min) | 16,1245.00 ± 7989.85 | 174,100.00 ± 10008.96 | 185,993.00 ± 6449.65 | 4.195 | 0.042 | 0.411 | 0.656 | 0.804 | 0.284 | 0.744 | 0.041 | 1.548 |
| Distance (km) | 1209.90 ± 77.30 | 1095.70 ± 64.10 | 1407.31 ± 42.99 | 14.474 | <0.001 | 0.707 | 0.343 | −1.042 | 0.005 | 2.842 | 0.024 | 1.801 |
| Intensity (%) | 76.95 ± 1.44 | 76.09 ± 1.73 | 77.12 ± 3.10 | 0.096 | 0.910 | 0.016 | 0.979 | −0.182 | 0.962 | 0.218 | 0.999 | 0.035 |
| TL (au) | 2926.48 ± 183.19 | 2969.94 ± 100.18 | 3286.35 ± 184.83 | 1.536 | 0.255 | 0.204 | 0.993 | 0.104 | 0.379 | 0.754 | 0.605 | 0.858 |
| LnRMSSD | 4.67 ± 0.08 | 4.76 ± 0.07 | 4.66 ± 0.11 | 2.756 | 0.104 | 0.315 | 0.179 | 1.063 | 0.229 | −1.111 | 0.999 | −0.045 |
| LnRMSSDcv | 5.65 ± 1.26 | 3.64 ± 0.49 | 5.33 ± 0.61 | 1.947 | 0.185 | 0.245 | 0.367 | −0.980 | 0.024 | 0.827 | 0.995 | −0.153 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Javaloyes, A.; Mateo-March, M.; Manresa-Rocamora, A.; Sanz-Quinto, S.; Moya-Ramón, M. The Use of a Smartphone Application in Monitoring HRV during an Altitude Training Camp in Professional Female Cyclists: A Preliminary Study. Sensors 2021, 21, 5497. https://doi.org/10.3390/s21165497
Javaloyes A, Mateo-March M, Manresa-Rocamora A, Sanz-Quinto S, Moya-Ramón M. The Use of a Smartphone Application in Monitoring HRV during an Altitude Training Camp in Professional Female Cyclists: A Preliminary Study. Sensors. 2021; 21(16):5497. https://doi.org/10.3390/s21165497
Chicago/Turabian StyleJavaloyes, Alejandro, Manuel Mateo-March, Agustín Manresa-Rocamora, Santiago Sanz-Quinto, and Manuel Moya-Ramón. 2021. "The Use of a Smartphone Application in Monitoring HRV during an Altitude Training Camp in Professional Female Cyclists: A Preliminary Study" Sensors 21, no. 16: 5497. https://doi.org/10.3390/s21165497
APA StyleJavaloyes, A., Mateo-March, M., Manresa-Rocamora, A., Sanz-Quinto, S., & Moya-Ramón, M. (2021). The Use of a Smartphone Application in Monitoring HRV during an Altitude Training Camp in Professional Female Cyclists: A Preliminary Study. Sensors, 21(16), 5497. https://doi.org/10.3390/s21165497