
Reliability of Body Temperature Measurements Obtained with Contactless Infrared Point Thermometers Commonly Used during the COVID-19 Pandemic




Abstract
1. Introduction
2. Materials and Methods
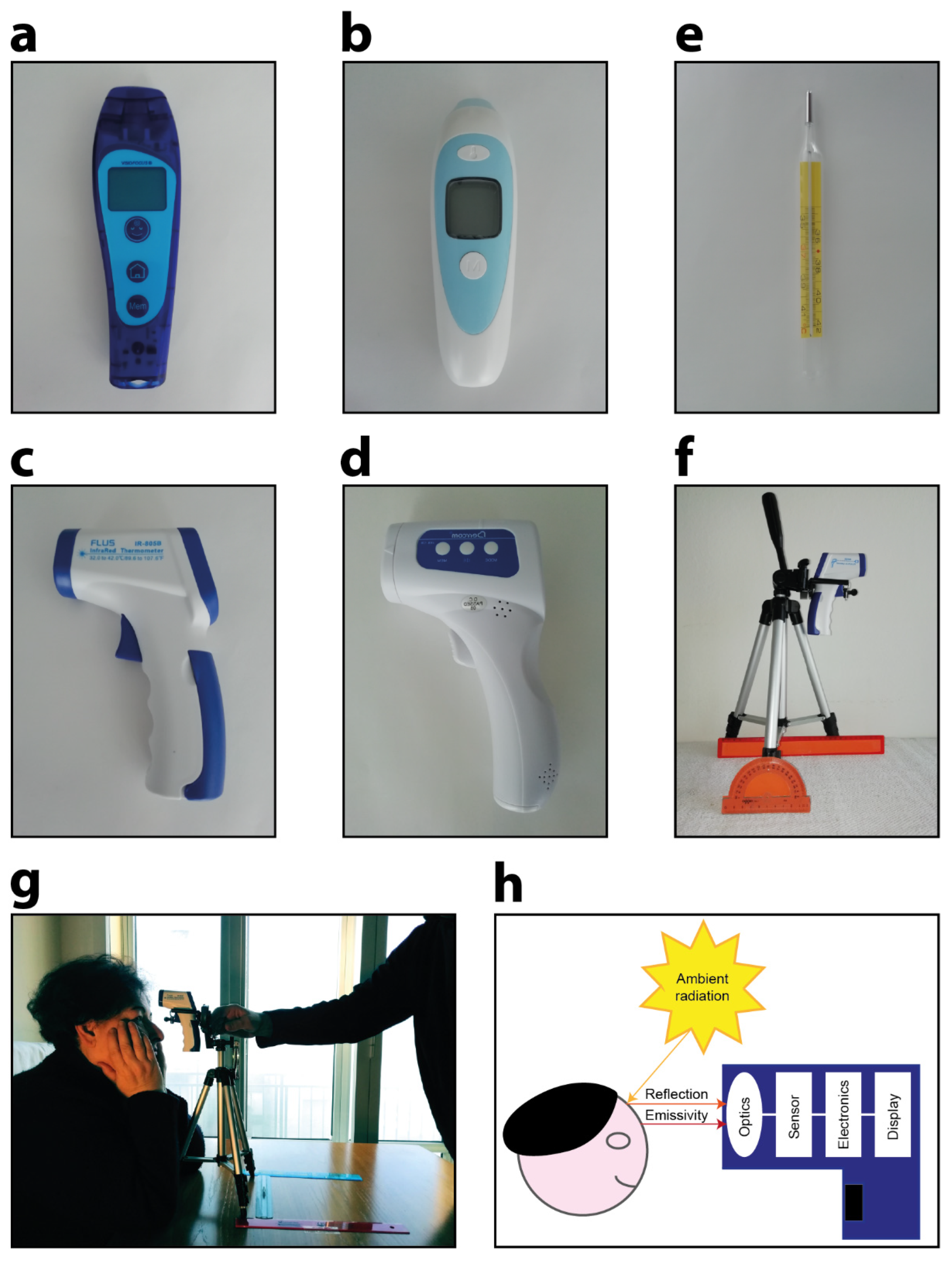
2.1. Devices Used in the Experiments
- Company: TECNIMED (Varese, Italy), model: VisioFocus PRO 06480; working distance automatically suggested in real-time (approximately 5–10 cm; Figure 1a);
- Company: Medek (Shenzhen, China), model: MDI261; working distance reported in the datasheet: 1–3 cm (Figure 1b);
- Company: FLUS (Shenzhen, China), model: IR-805B; working distance reported in the datasheet: 5 cm (Figure 1c);
- Company: Berrcom (Guangdong, Cina), model: JXB-178; working distance reported in the datasheet: 3–5 cm (Figure 1d).
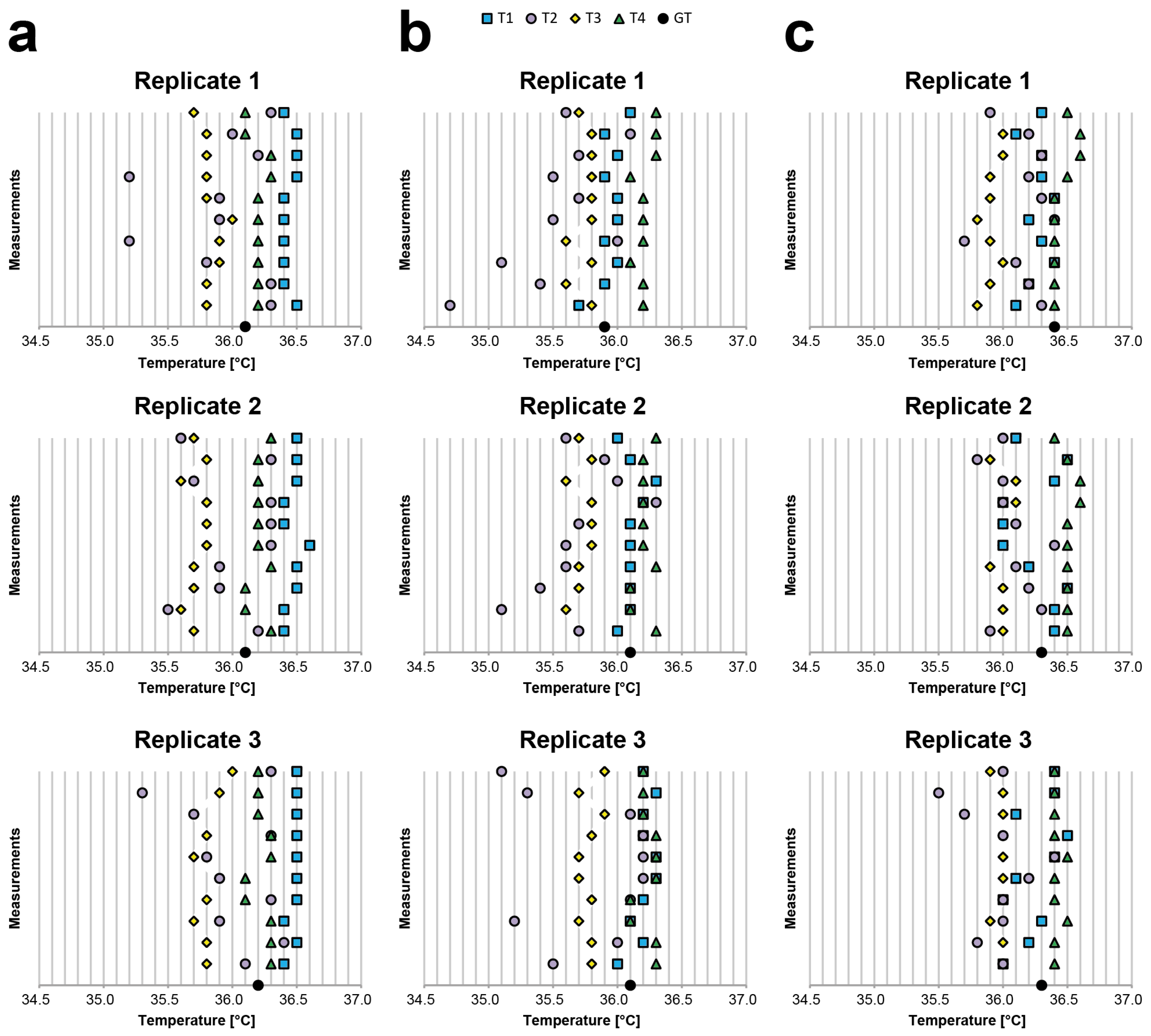
2.2. Inter- and Intra-Rater Reliability Experiment: Description
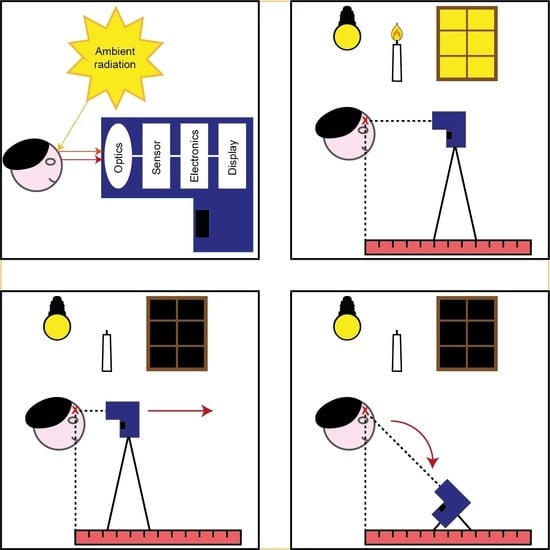
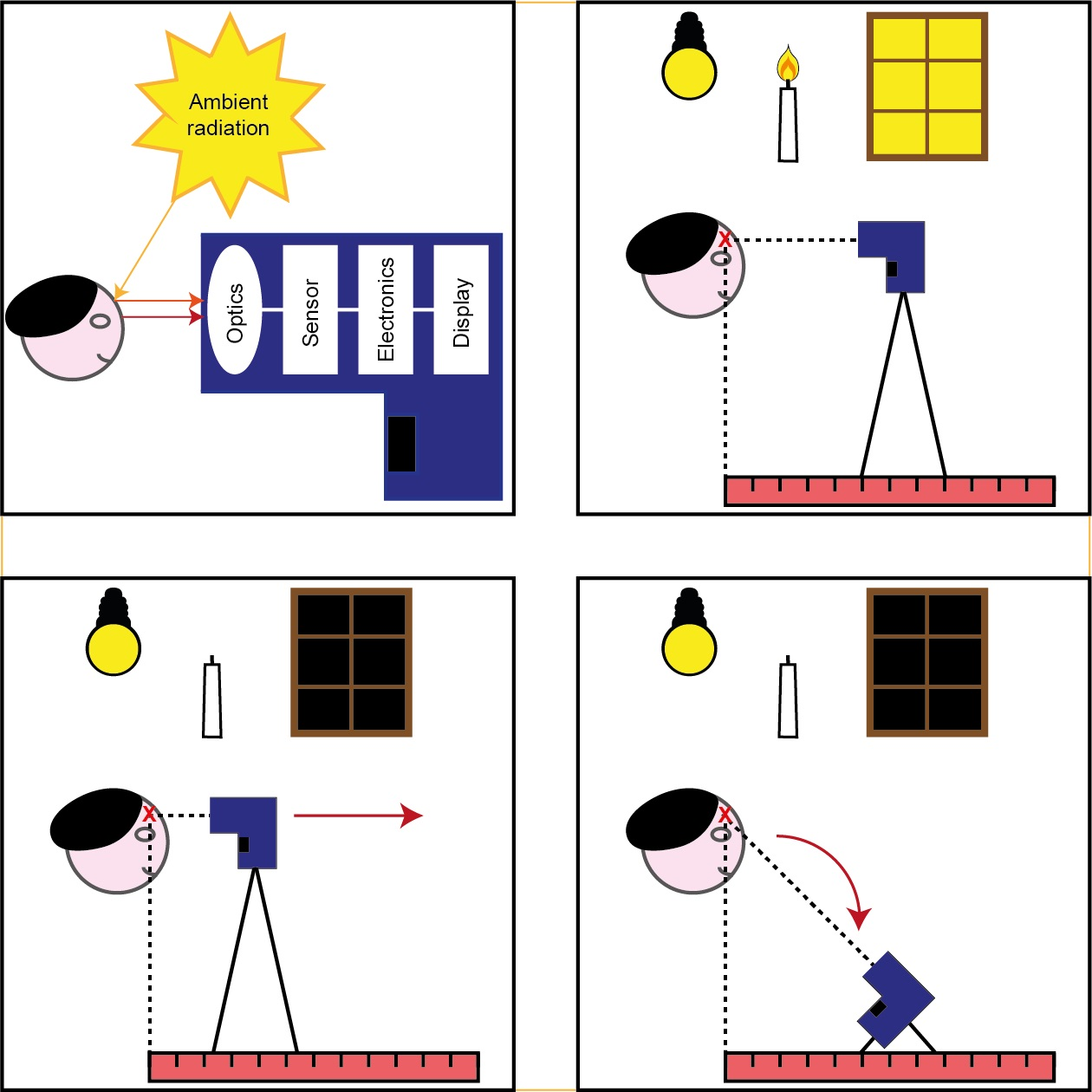
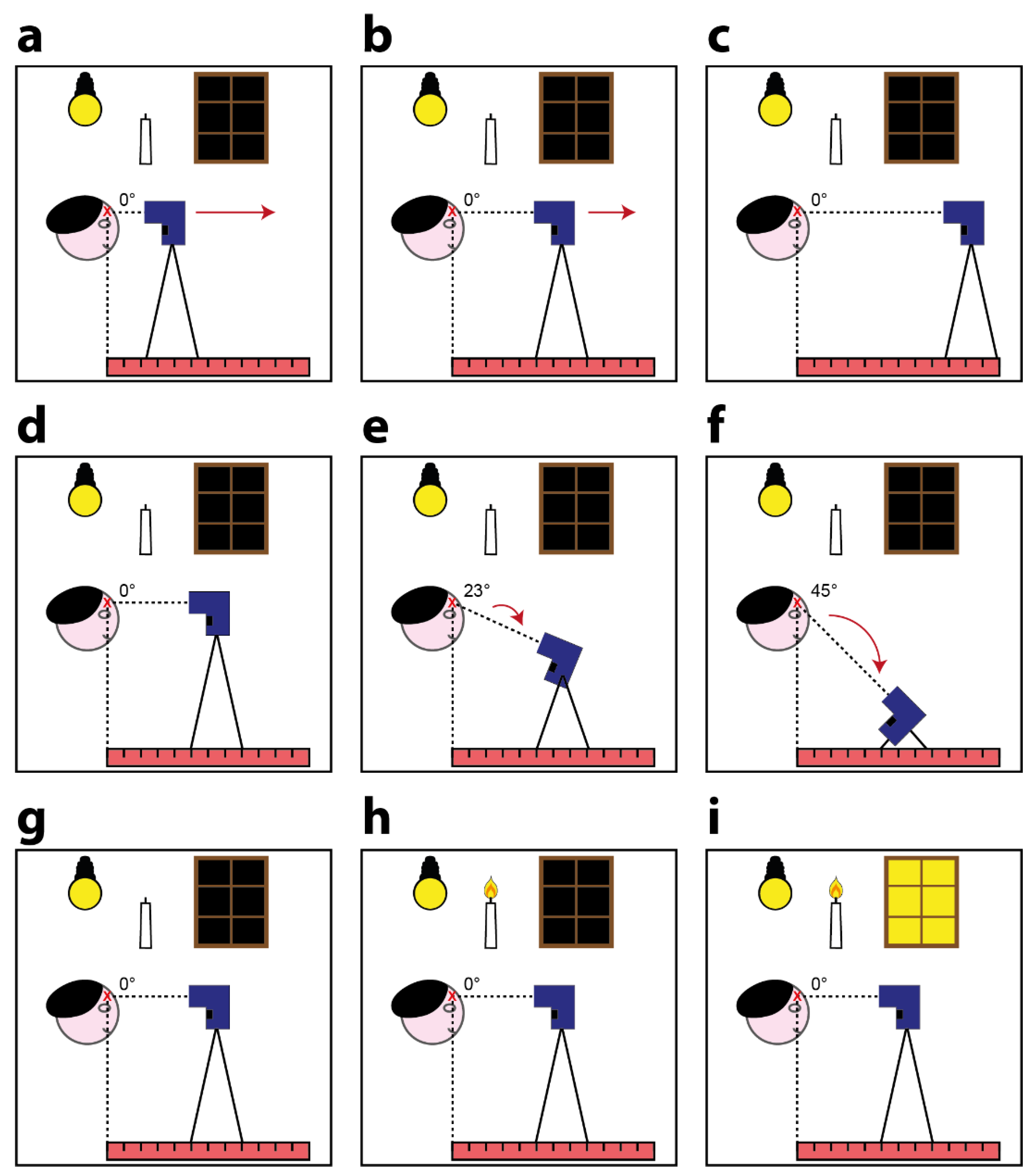
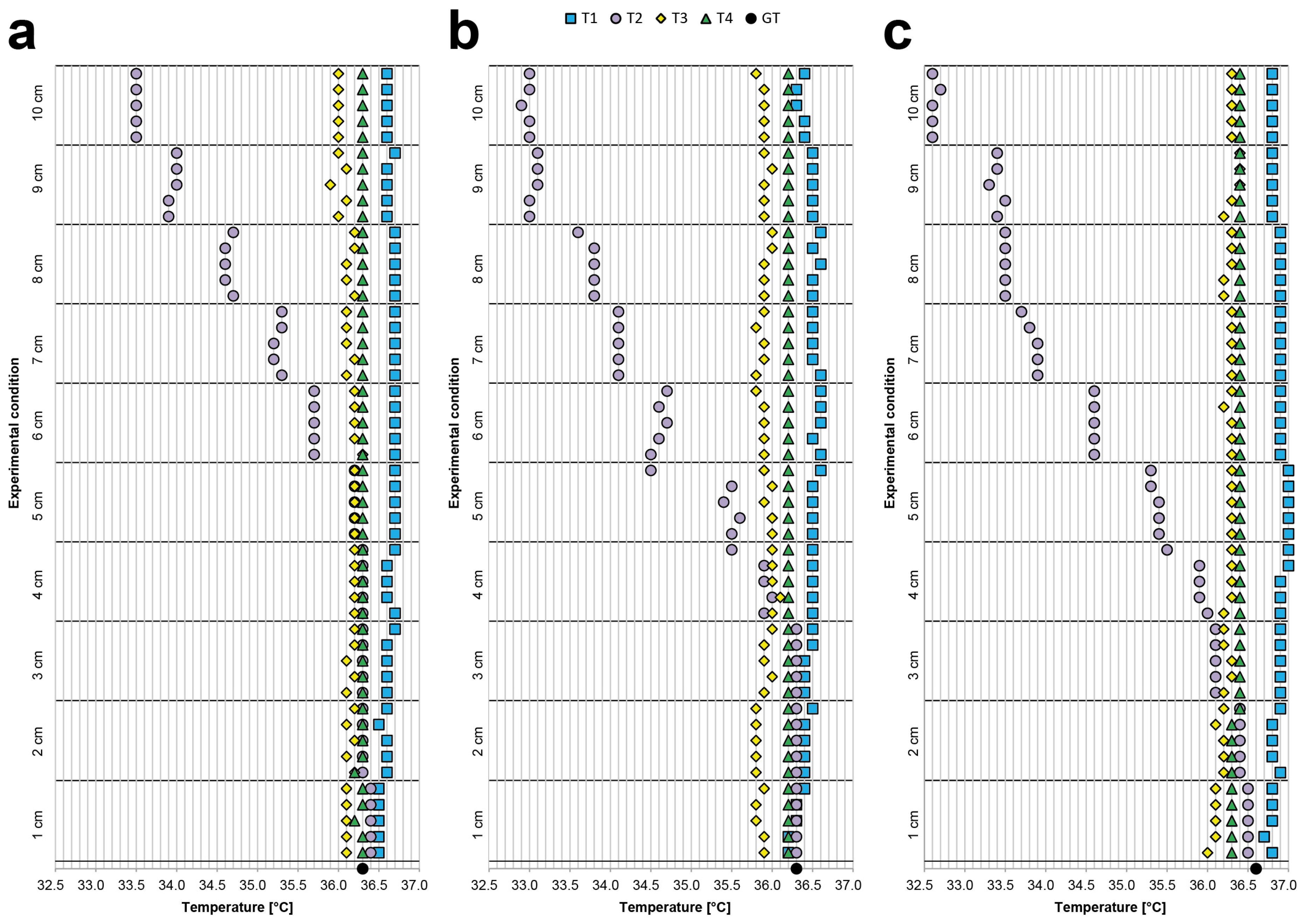
2.3. Body—Device Distance Experiment: Description
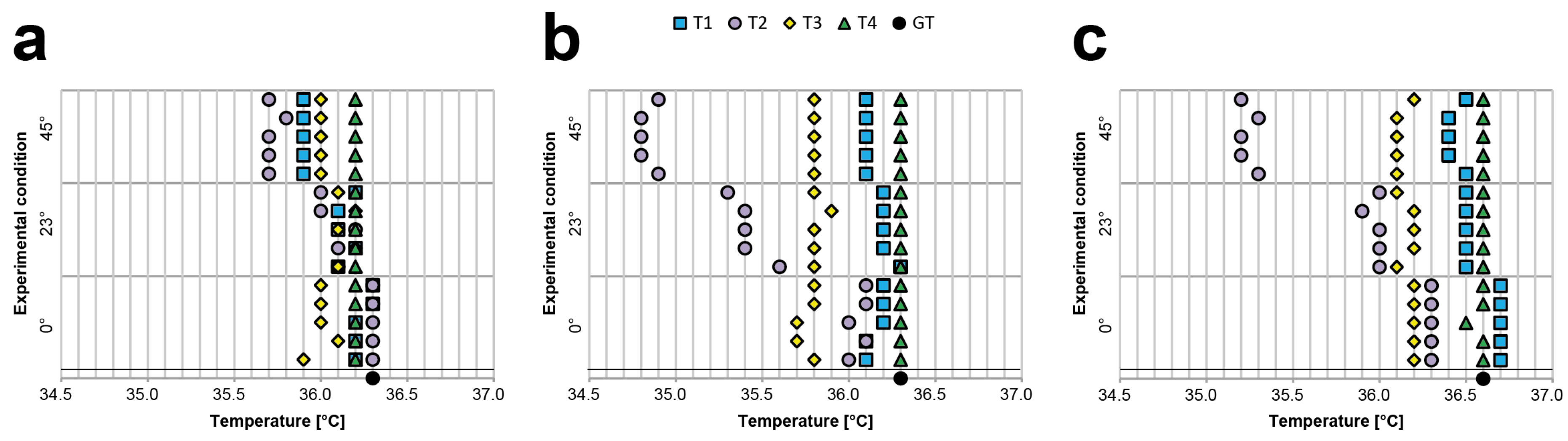
2.4. Body—Device Angle Experiment: Description
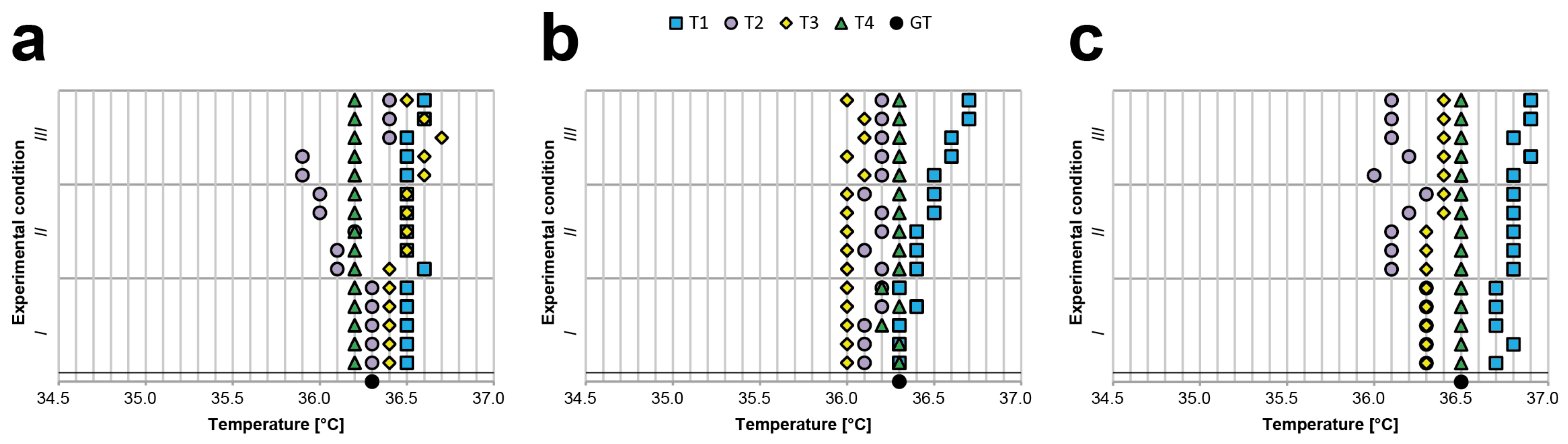
2.5. Light Influence Experiment: Description
- 1)
- With the shutters of the windows in the room closed and the room illuminated only by a constant artificial light (i.e., the same conditions as those in the other experiments, Figure 2g). This condition aimed to simulate real-life acquisitions performed, for instance, in an emergency triage room during the late afternoon/evening.
- 2)
- With the shutters of the windows in the room closed and the room illuminated only by constant artificial light and a small candle (Figure 2h). This condition again aimed to simulate real-life acquisitions performed in an emergency triage room during the late afternoon/evening but with a different source of light than that of the first condition.
- 3)
- With the shutters of the windows in the room kept fully open to allow sunlight to illuminate the room. The artificial light was retained, and the candle remained lit (Figure 2i). This condition aimed to simulate real-life acquisitions performed, for instance, in an emergency triage room in the morning/early-afternoon. We performed these experiments only on sunny days to ensure a significant difference compared to the other conditions featuring closed window shutters. However, the acquisitions were performed while ensuring that the rays of the sun did not touch the subjects’ foreheads.
3. Results
3.1. Inter- and Intra-Rater Reliability Experiment: Results
3.2. Body—Device Distance Experiment: Results
3.3. Body—Device Angle Experiment: Results
3.4. Light Influence Experiment: Results
4. Discussion
5. Conclusions
- 1)
- Acquiring measurements without carefully monitoring the working distance and angle of inclination can lead to a large discrepancy between subsequent body temperature estimations;
- 2)
- Light conditions influence the measurements, and, accordingly, the ambient radiation in the assessment room should be monitored, e.g., by using constant artificial lights.
- 1)
- By suggesting that operators use only thermometers from a list of approved devices;
- 2)
- By using public information methods (e.g., advertisements) to inform operators about the correct working distance, angle of inclination, and light conditions to obtain more reliable measurements.
- To punctually establish the measurement conditions and method;
- To set a fixed temperature threshold reference, by considering an assigned measurement body site;
- To accurately estimate the measurement uncertainty, taking into account the main contributions at the real operative measurement conditions;
- To transpose the threshold reference value as a function of the body site used;
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Ethics Statements
Acknowledgments
Conflicts of Interest
Appendix

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Room temperature [°C] | 19.8 | |||
| Room humidity | 53% | |||
| Replicate 1 | ||||
| Body temperature GT [°C] | 36.1 | |||
| Number | T1 [°C] | T2 [°C] | T3 [°C] | T4 [°C] |
| 1 | 36.5 | 36.3 | 35.8 | 36.2 |
| 2 | 36.4 | 36.3 | 35.8 | 36.2 |
| 3 | 36.4 | 35.8 | 35.9 | 36.2 |
| 4 | 36.4 | 35.2 | 35.9 | 36.2 |
| 5 | 36.4 | 35.9 | 36.0 | 36.2 |
| 6 | 36.4 | 35.9 | 35.8 | 36.2 |
| 7 | 36.5 | 35.2 | 35.8 | 36.3 |
| 8 | 36.5 | 36.2 | 35.8 | 36.3 |
| 9 | 36.5 | 36.0 | 35.8 | 36.1 |
| 10 | 36.4 | 36.3 | 35.7 | 36.1 |
| Min [°C] | 36.4 | 35.2 | 35.7 | 36.1 |
| Max [°C] | 36.5 | 36.3 | 36.0 | 36.3 |
| Max–Min difference [°C] | 0.1 | 1.1 | 0.3 | 0.2 |
| Mean [°C] | 36.44 | 35.91 | 35.83 | 36.20 |
| GT–Mean difference [°C] | −0.34 | 0.19 | 0.27 | −0.10 |
| Replicate 2 | ||||
| Body temperature GT [°C] | 36.1 | |||
| Number | T1 [°C] | T2 [°C] | T3 [°C] | T4 [°C] |
| 1 | 36.4 | 36.2 | 35.7 | 36.3 |
| 2 | 36.4 | 35.5 | 35.6 | 36.1 |
| 3 | 36.5 | 35.9 | 35.7 | 36.1 |
| 4 | 36.5 | 35.9 | 35.7 | 36.3 |
| 5 | 36.6 | 36.3 | 35.8 | 36.2 |
| 6 | 36.4 | 36.3 | 35.8 | 36.2 |
| 7 | 36.4 | 36.3 | 35.8 | 36.2 |
| 8 | 36.5 | 35.7 | 35.6 | 36.2 |
| 9 | 36.5 | 36.3 | 35.8 | 36.2 |
| 10 | 36.5 | 35.6 | 35.7 | 36.3 |
| Min [°C] | 36.4 | 35.5 | 35.6 | 36.1 |
| Max [°C] | 36.6 | 36.3 | 35.8 | 36.3 |
| Max–Min difference [°C] | 0.2 | 0.8 | 0.2 | 0.2 |
| Mean [°C] | 36.47 | 36.00 | 35.72 | 36.21 |
| GT–Mean difference [°C] | −0.37 | 0.10 | 0.38 | −0.11 |
| Replicate 3 | ||||
| Body temperature GT [°C] | 36.2 | |||
| Number | T1 [°C] | T2 [°C] | T3 [°C] | T4 [°C] |
| 1 | 36.4 | 36.1 | 35.8 | 36.3 |
| 2 | 36.5 | 36.4 | 35.8 | 36.3 |
| 3 | 36.4 | 35.9 | 35.7 | 36.3 |
| 4 | 36.5 | 36.3 | 35.8 | 36.1 |
| 5 | 36.5 | 35.9 | 35.9 | 36.1 |
| 6 | 36.5 | 35.8 | 35.7 | 36.3 |
| 7 | 36.5 | 36.3 | 35.8 | 36.3 |
| 8 | 36.5 | 35.7 | 35.7 | 36.2 |
| 9 | 36.5 | 35.3 | 35.9 | 36.2 |
| 10 | 36.5 | 36.3 | 36.0 | 36.2 |
| Min [°C] | 36.4 | 35.3 | 35.7 | 36.1 |
| Max [°C] | 36.5 | 36.4 | 36.0 | 36.3 |
| Max–Min difference [°C] | 0.1 | 1.1 | 0.3 | 0.2 |
| Mean [°C] | 36.48 | 36.00 | 35.81 | 36.23 |
| GT–Mean difference [°C] | −0.28 | 0.20 | 0.39 | −0.03 |
| Room temperature[°C] | 19.8 | |||
| Room humidity | 53% | |||
| Replicate 1 | ||||
| Body temperature GT [°C] | 35.9 | |||
| Number | T1 [°C] | T2 [°C] | T3 [°C] | T4 [°C] |
| 1 | 35.7 | 34.7 | 35.8 | 36.2 |
| 2 | 35.9 | 35.4 | 35.6 | 36.2 |
| 3 | 36.0 | 35.1 | 35.8 | 36.1 |
| 4 | 35.9 | 36.0 | 35.6 | 36.2 |
| 5 | 36.0 | 35.5 | 35.8 | 36.2 |
| 6 | 36.0 | 35.7 | 35.8 | 36.2 |
| 7 | 35.9 | 35.5 | 35.8 | 36.1 |
| 8 | 36.0 | 35.7 | 35.8 | 36.3 |
| 9 | 35.9 | 36.1 | 35.8 | 36.3 |
| 10 | 36.1 | 35.6 | 35.7 | 36.3 |
| Min [°C] | 35.7 | 34.7 | 35.6 | 36.1 |
| Max [°C] | 36.1 | 36.1 | 35.8 | 36.3 |
| Max–Min difference [°C] | 0.4 | 1.4 | 0.2 | 0.2 |
| Mean [°C] | 35.94 | 35.53 | 35.75 | 36.21 |
| GT–Mean difference [°C] | −0.04 | 0.37 | 0.15 | −0.31 |
| Replicate 2 | ||||
| Body temperature GT [°C] | 36.1 | |||
| Number | T1 [°C] | T2 [°C] | T3 [°C] | T4 [°C] |
| 1 | 36.0 | 35.7 | 35.7 | 36.3 |
| 2 | 36.1 | 35.1 | 35.6 | 36.1 |
| 3 | 36.1 | 35.4 | 35.7 | 36.1 |
| 4 | 36.1 | 35.6 | 35.7 | 36.3 |
| 5 | 36.1 | 35.6 | 35.8 | 36.2 |
| 6 | 36.1 | 35.7 | 35.8 | 36.2 |
| 7 | 36.2 | 36.3 | 35.8 | 36.2 |
| 8 | 36.3 | 36.0 | 35.6 | 36.2 |
| 9 | 36.1 | 35.9 | 35.8 | 36.2 |
| 10 | 36.0 | 35.6 | 35.7 | 36.3 |
| Min [°C] | 36.0 | 35.1 | 35.6 | 36.1 |
| Max [°C] | 36.3 | 36.3 | 35.8 | 36.3 |
| Max–Min difference [°C] | 0.3 | 1.2 | 0.2 | 0.2 |
| Mean [°C] | 36.11 | 35.69 | 35.72 | 36.21 |
| GT–Mean difference [°C] | −0.01 | 0.41 | 0.38 | −0.11 |
| Replicate 3 | ||||
| Body temperature GT [°C] | 36.1 | |||
| Number | T1 [°C] | T2 [°C] | T3 [°C] | T4 [°C] |
| 1 | 36.0 | 35.5 | 35.8 | 36.3 |
| 2 | 36.2 | 36.0 | 35.8 | 36.3 |
| 3 | 36.1 | 35.2 | 35.7 | 36.1 |
| 4 | 36.2 | 36.1 | 35.8 | 36.1 |
| 5 | 36.3 | 36.2 | 35.7 | 36.3 |
| 6 | 36.3 | 36.2 | 35.7 | 36.3 |
| 7 | 36.2 | 36.2 | 35.8 | 36.3 |
| 8 | 36.2 | 36.1 | 35.9 | 36.2 |
| 9 | 36.3 | 35.3 | 35.7 | 36.2 |
| 10 | 36.2 | 35.1 | 35.9 | 36.2 |
| Min [°C] | 36.0 | 35.1 | 35.7 | 36.1 |
| Max [°C] | 36.3 | 36.2 | 35.9 | 36.3 |
| Max–Min difference [°C] | 0.3 | 1.1 | 0.2 | 0.2 |
| Mean [°C] | 36.20 | 35.79 | 35.78 | 36.23 |
| GT–Mean difference [°C] | −0.10 | 0.31 | 0.32 | −0.13 |
| Room temperature[°C] | 20.0 | |||
| Room humidity | 51% | |||
| Replicate 1 | ||||
| Body temperature GT [°C] | 36.4 | |||
| Number | T1 [°C] | T2 [°C] | T3 [°C] | T4 [°C] |
| 1 | 36.1 | 36.3 | 35.8 | 36.4 |
| 2 | 36.2 | 36.2 | 35.9 | 36.4 |
| 3 | 36.4 | 36.1 | 36.0 | 36.4 |
| 4 | 36.3 | 35.7 | 35.9 | 36.4 |
| 5 | 36.2 | 36.4 | 35.8 | 36.4 |
| 6 | 36.4 | 36.3 | 35.9 | 36.4 |
| 7 | 36.3 | 36.2 | 35.9 | 36.5 |
| 8 | 36.3 | 36.3 | 36.0 | 36.6 |
| 9 | 36.1 | 36.2 | 36.0 | 36.6 |
| 10 | 36.3 | 35.9 | 35.9 | 36.5 |
| Min [°C] | 36.1 | 35.7 | 35.8 | 36.4 |
| Max [°C] | 36.4 | 36.4 | 36.0 | 36.6 |
| Max–Min difference [°C] | 0.3 | 0.7 | 0.2 | 0.2 |
| Mean [°C] | 36.26 | 36.16 | 35.91 | 36.46 |
| GT–Mean difference [°C] | 0.14 | 0.24 | 0.49 | −0.06 |
| Replicate 2 | ||||
| Body temperature GT [°C] | 36.3 | |||
| Number | T1 [°C] | T2 [°C] | T3 [°C] | T4 [°C] |
| 1 | 36.4 | 35.9 | 36.0 | 36.5 |
| 2 | 36.4 | 36.3 | 36.0 | 36.5 |
| 3 | 36.5 | 36.2 | 36.0 | 36.5 |
| 4 | 36.2 | 36.1 | 35.9 | 36.5 |
| 5 | 36.0 | 36.4 | 36.0 | 36.5 |
| 6 | 36.0 | 36.1 | 36.0 | 36.5 |
| 7 | 36.0 | 36.0 | 36.1 | 36.6 |
| 8 | 36.4 | 36.0 | 36.1 | 36.6 |
| 9 | 36.5 | 35.8 | 35.9 | 36.5 |
| 10 | 36.1 | 36.0 | 36.0 | 36.4 |
| Min [°C] | 36.0 | 35.8 | 35.9 | 36.4 |
| Max [°C] | 36.5 | 36.4 | 36.1 | 36.6 |
| Max–Min difference [°C] | 0.5 | 0.6 | 0.2 | 0.2 |
| Mean [°C] | 36.25 | 36.08 | 36.00 | 36.51 |
| GT–Mean difference [°C] | 0.05 | 0.22 | 0.30 | −0.21 |
| Replicate 3 | ||||
| Body temperature GT [°C] | 36.3 | |||
| Number | T1 [°C] | T2 [°C] | T3 [°C] | T4 [°C] |
| 1 | 36.0 | 36.0 | 36.0 | 36.4 |
| 2 | 36.2 | 35.8 | 36.0 | 36.4 |
| 3 | 36.3 | 36.0 | 35.9 | 36.5 |
| 4 | 36.0 | 36.0 | 36.0 | 36.4 |
| 5 | 36.1 | 36.2 | 36.0 | 36.4 |
| 6 | 36.4 | 36.4 | 36.0 | 36.5 |
| 7 | 36.5 | 36.0 | 36.0 | 36.4 |
| 8 | 36.1 | 35.7 | 36.0 | 36.4 |
| 9 | 36.4 | 35.5 | 36.0 | 36.4 |
| 10 | 36.4 | 36.0 | 35.9 | 36.4 |
| Min [°C] | 36.0 | 35.5 | 35.9 | 36.4 |
| Max [°C] | 36.5 | 36.4 | 36.0 | 36.5 |
| Max–Min difference [°C] | 0.5 | 0.9 | 0.1 | 0.1 |
| Mean [°C] | 36.24 | 35.96 | 35.98 | 36.42 |
| GT–Mean difference [°C] | 0.06 | 0.34 | 0.32 | −0.12 |
| Room temperature[°C] | 20.1 | |||
| Room humidity | 53% | |||
| Body temperature GT [°C] | 36.3 | |||
| Distance [cm]–number | T1 [°C] | T2 [°C] | T3 [°C] | T4 [°C] |
| 1 cm–1 | 36.5 | 36.4 | 36.1 | 36.3 |
| 1 cm–2 | 36.5 | 36.4 | 36.1 | 36.3 |
| 1 cm–3 | 36.5 | 36.4 | 36.1 | 36.2 |
| 1 cm–4 | 36.5 | 36.4 | 36.1 | 36.3 |
| 1 cm–5 | 36.5 | 36.4 | 36.1 | 36.3 |
| 2 cm–1 | 36.6 | 36.3 | 36.2 | 36.2 |
| 2 cm–2 | 36.6 | 36.3 | 36.1 | 36.3 |
| 2 cm–3 | 36.6 | 36.3 | 36.2 | 36.3 |
| 2 cm–4 | 36.5 | 36.3 | 36.1 | 36.3 |
| 2 cm–5 | 36.6 | 36.3 | 36.2 | 36.3 |
| 3 cm–1 | 36.6 | 36.3 | 36.1 | 36.3 |
| 3 cm–2 | 36.6 | 36.3 | 36.2 | 36.3 |
| 3 cm–3 | 36.6 | 36.3 | 36.1 | 36.3 |
| 3 cm–4 | 36.6 | 36.3 | 36.2 | 36.3 |
| 3 cm–5 | 36.7 | 36.3 | 36.2 | 36.3 |
| 4 cm–1 | 36.7 | 36.3 | 36.2 | 36.3 |
| 4 cm–2 | 36.6 | 36.3 | 36.2 | 36.3 |
| 4 cm–3 | 36.6 | 36.3 | 36.2 | 36.3 |
| 4 cm–4 | 36.6 | 36.3 | 36.2 | 36.3 |
| 4 cm–5 | 36.7 | 36.3 | 36.2 | 36.3 |
| 5 cm–1 | 36.7 | 36.2 | 36.2 | 36.3 |
| 5 cm–2 | 36.7 | 36.2 | 36.2 | 36.3 |
| 5 cm–3 | 36.7 | 36.2 | 36.2 | 36.3 |
| 5 cm–4 | 36.7 | 36.2 | 36.2 | 36.3 |
| 5 cm–5 | 36.7 | 36.2 | 36.2 | 36.3 |
| 6 cm–1 | 36.7 | 35.7 | 36.3 | 36.3 |
| 6 cm–2 | 36.7 | 35.7 | 36.2 | 36.3 |
| 6 cm–3 | 36.7 | 35.7 | 36.2 | 36.3 |
| 6 cm–4 | 36.7 | 35.7 | 36.2 | 36.3 |
| 6 cm–5 | 36.7 | 35.7 | 36.2 | 36.3 |
| 7 cm–1 | 36.7 | 35.3 | 36.1 | 36.3 |
| 7 cm–2 | 36.7 | 35.2 | 36.2 | 36.3 |
| 7 cm–3 | 36.7 | 35.2 | 36.1 | 36.3 |
| 7 cm–4 | 36.7 | 35.3 | 36.1 | 36.3 |
| 7 cm–5 | 36.7 | 35.3 | 36.1 | 36.3 |
| 8 cm–1 | 36.7 | 34.7 | 36.2 | 36.3 |
| 8 cm–2 | 36.7 | 34.6 | 36.1 | 36.3 |
| 8 cm–3 | 36.7 | 34.6 | 36.1 | 36.3 |
| 8 cm–4 | 36.7 | 34.6 | 36.2 | 36.3 |
| 8 cm–5 | 36.7 | 34.7 | 36.2 | 36.3 |
| 9 cm–1 | 36.6 | 33.9 | 36.0 | 36.3 |
| 9 cm–2 | 36.6 | 33.9 | 36.1 | 36.3 |
| 9 cm–3 | 36.6 | 34.0 | 35.9 | 36.3 |
| 9 cm–4 | 36.6 | 34.0 | 36.1 | 36.3 |
| 9 cm–5 | 36.7 | 34.0 | 36.0 | 36.3 |
| 10 cm–1 | 36.6 | 33.5 | 36.0 | 36.3 |
| 10 cm–2 | 36.6 | 33.5 | 36.0 | 36.3 |
| 10 cm–3 | 36.6 | 33.5 | 36.0 | 36.3 |
| 10 cm–4 | 36.6 | 33.5 | 36.0 | 36.3 |
| 10 cm–5 | 36.6 | 33.5 | 36.0 | 36.3 |
| Min [°C] | 36.5 | 33.5 | 35.9 | 36.2 |
| Max [°C] | 36.7 | 36.4 | 36.3 | 36.3 |
| Max–Min difference [°C] | 0.2 | 2.9 | 0.4 | 0.1 |
| Mean [°C] | 36.64 | 35.46 | 36.13 | 36.30 |
| Room temperature[°C] | 20.1 | |||
| Room humidity | 53% | |||
| Body temperature GT [°C] | 36.3 | |||
| Distance [cm]–number | T1 [°C] | T2 [°C] | T3 [°C] | T4 [°C] |
| 1 cm–1 | 36.2 | 36.3 | 35.9 | 36.2 |
| 1 cm–2 | 36.2 | 36.3 | 35.9 | 36.2 |
| 1 cm–3 | 36.3 | 36.3 | 35.8 | 36.2 |
| 1 cm–4 | 36.3 | 36.3 | 35.8 | 36.2 |
| 1 cm–5 | 36.4 | 36.3 | 35.9 | 36.2 |
| 2 cm–1 | 36.4 | 36.3 | 35.8 | 36.2 |
| 2 cm–2 | 36.4 | 36.3 | 35.8 | 36.2 |
| 2 cm–3 | 36.4 | 36.3 | 35.8 | 36.2 |
| 2 cm–4 | 36.4 | 36.3 | 35.8 | 36.2 |
| 2 cm–5 | 36.5 | 36.3 | 35.8 | 36.2 |
| 3 cm–1 | 36.4 | 36.3 | 35.9 | 36.2 |
| 3 cm–2 | 36.4 | 36.3 | 36.0 | 36.2 |
| 3 cm–3 | 36.4 | 36.3 | 35.9 | 36.2 |
| 3 cm–4 | 36.5 | 36.3 | 35.9 | 36.2 |
| 3 cm–5 | 36.5 | 36.3 | 36.0 | 36.2 |
| 4 cm–1 | 36.5 | 35.9 | 36.0 | 36.2 |
| 4 cm–2 | 36.5 | 36.0 | 36.1 | 36.2 |
| 4 cm–3 | 36.5 | 35.9 | 36.0 | 36.2 |
| 4 cm–4 | 36.5 | 35.9 | 36.0 | 36.2 |
| 4 cm–5 | 36.5 | 35.5 | 36.0 | 36.2 |
| 5 cm–1 | 36.5 | 35.5 | 36.0 | 36.2 |
| 5 cm–2 | 36.5 | 35.6 | 36.0 | 36.2 |
| 5 cm–3 | 36.5 | 35.4 | 35.9 | 36.2 |
| 5 cm–4 | 36.5 | 35.5 | 36.0 | 36.2 |
| 5 cm–5 | 36.6 | 34.5 | 35.9 | 36.2 |
| 6 cm–1 | 36.6 | 34.5 | 35.9 | 36.2 |
| 6 cm–2 | 36.5 | 34.6 | 35.9 | 36.2 |
| 6 cm–3 | 36.6 | 34.7 | 35.9 | 36.2 |
| 6 cm–4 | 36.6 | 34.6 | 35.9 | 36.2 |
| 6 cm–5 | 36.6 | 34.7 | 35.8 | 36.2 |
| 7 cm–1 | 36.6 | 34.1 | 35.8 | 36.2 |
| 7 cm–2 | 36.5 | 34.1 | 35.9 | 36.2 |
| 7 cm–3 | 36.5 | 34.1 | 35.9 | 36.2 |
| 7 cm–4 | 36.5 | 34.1 | 35.8 | 36.2 |
| 7 cm–5 | 36.5 | 34.1 | 35.9 | 36.2 |
| 8 cm–1 | 36.5 | 33.8 | 35.9 | 36.2 |
| 8 cm–2 | 36.5 | 33.8 | 35.9 | 36.2 |
| 8 cm–3 | 36.6 | 33.8 | 35.9 | 36.2 |
| 8 cm–4 | 36.5 | 33.8 | 36.0 | 36.2 |
| 8 cm–5 | 36.6 | 33.6 | 36.0 | 36.2 |
| 9 cm–1 | 36.5 | 33.0 | 35.9 | 36.2 |
| 9 cm–2 | 36.5 | 33.0 | 35.9 | 36.2 |
| 9 cm–3 | 36.5 | 33.1 | 35.9 | 36.2 |
| 9 cm–4 | 36.5 | 33.1 | 36.0 | 36.2 |
| 9 cm–5 | 36.5 | 33.1 | 35.9 | 36.2 |
| 10 cm–1 | 36.4 | 33.0 | 35.9 | 36.2 |
| 10 cm–2 | 36.4 | 33.0 | 35.9 | 36.2 |
| 10 cm–3 | 36.3 | 32.9 | 35.9 | 36.2 |
| 10 cm–4 | 36.3 | 33.0 | 35.9 | 36.2 |
| 10 cm–5 | 36.4 | 33.0 | 35.8 | 36.2 |
| Min [°C] | 36.2 | 32.9 | 35.8 | 36.2 |
| Max [°C] | 36.6 | 36.3 | 36.1 | 36.2 |
| Max-Min difference [°C] | 0.4 | 3.4 | 0.3 | 0.0 |
| Mean [°C] | 36.47 | 34.86 | 35.91 | 36.20 |
| Room temperature[°C] | 20.0 | |||
| Room humidity | 51% | |||
| Body temperature GT [°C] | 36.6 | |||
| Distance [cm]–number | T1 [°C] | T2 [°C] | T3 [°C] | T4 [°C] |
| 1 cm–1 | 36.8 | 36.5 | 36.0 | 36.3 |
| 1 cm–2 | 36.7 | 36.5 | 36.1 | 36.3 |
| 1 cm–3 | 36.8 | 36.5 | 36.1 | 36.3 |
| 1 cm–4 | 36.8 | 36.5 | 36.1 | 36.3 |
| 1 cm–5 | 36.8 | 36.5 | 36.1 | 36.3 |
| 2 cm–1 | 36.9 | 36.4 | 36.2 | 36.3 |
| 2 cm–2 | 36.8 | 36.4 | 36.2 | 36.3 |
| 2 cm–3 | 36.8 | 36.4 | 36.2 | 36.3 |
| 2 cm–4 | 36.8 | 36.4 | 36.1 | 36.3 |
| 2 cm–5 | 36.9 | 36.4 | 36.2 | 36.4 |
| 3 cm–1 | 36.9 | 36.1 | 36.2 | 36.4 |
| 3 cm–2 | 36.9 | 36.1 | 36.3 | 36.4 |
| 3 cm–3 | 36.9 | 36.1 | 36.3 | 36.4 |
| 3 cm–4 | 36.9 | 36.1 | 36.2 | 36.4 |
| 3 cm–5 | 36.9 | 36.1 | 36.2 | 36.4 |
| 4 cm–1 | 36.9 | 36.0 | 36.2 | 36.4 |
| 4 cm–2 | 36.9 | 35.9 | 36.3 | 36.4 |
| 4 cm–3 | 36.9 | 35.9 | 36.3 | 36.4 |
| 4 cm–4 | 37.0 | 35.9 | 36.3 | 36.4 |
| 4 cm–5 | 37.0 | 35.5 | 36.3 | 36.4 |
| 5 cm–1 | 37.0 | 35.4 | 36.3 | 36.4 |
| 5 cm–2 | 37.0 | 35.4 | 36.3 | 36.4 |
| 5 cm–3 | 37.0 | 35.4 | 36.3 | 36.4 |
| 5 cm–4 | 37.0 | 35.3 | 36.3 | 36.4 |
| 5 cm–5 | 37.0 | 35.3 | 36.3 | 36.4 |
| 6 cm–1 | 36.9 | 34.6 | 36.3 | 36.4 |
| 6 cm–2 | 36.9 | 34.6 | 36.3 | 36.4 |
| 6 cm–3 | 36.9 | 34.6 | 36.3 | 36.4 |
| 6 cm–4 | 36.9 | 34.6 | 36.2 | 36.4 |
| 6 cm–5 | 36.9 | 34.6 | 36.3 | 36.4 |
| 7 cm–1 | 36.9 | 33.9 | 36.3 | 36.4 |
| 7 cm–2 | 36.9 | 33.9 | 36.3 | 36.4 |
| 7 cm–3 | 36.9 | 33.9 | 36.3 | 36.4 |
| 7 cm–4 | 36.9 | 33.8 | 36.3 | 36.4 |
| 7 cm–5 | 36.9 | 33.7 | 36.3 | 36.4 |
| 8 cm–1 | 36.9 | 33.5 | 36.2 | 36.4 |
| 8 cm–2 | 36.9 | 33.5 | 36.2 | 36.4 |
| 8 cm–3 | 36.9 | 33.5 | 36.3 | 36.4 |
| 8 cm–4 | 36.9 | 33.5 | 36.3 | 36.4 |
| 8 cm–5 | 36.9 | 33.5 | 36.3 | 36.4 |
| 9 cm–1 | 36.8 | 33.4 | 36.2 | 36.4 |
| 9 cm–2 | 36.8 | 33.5 | 36.3 | 36.4 |
| 9 cm–3 | 36.8 | 33.3 | 36.4 | 36.4 |
| 9 cm–4 | 36.8 | 33.4 | 36.4 | 36.4 |
| 9 cm–5 | 36.8 | 33.4 | 36.4 | 36.4 |
| 10 cm–1 | 36.8 | 32.6 | 36.3 | 36.4 |
| 10 cm–2 | 36.8 | 32.6 | 36.3 | 36.4 |
| 10 cm–3 | 36.8 | 32.6 | 36.3 | 36.4 |
| 10 cm–4 | 36.8 | 32.7 | 36.3 | 36.4 |
| 10 cm–5 | 36.8 | 32.6 | 36.3 | 36.4 |
| Min [°C] | 36.7 | 32.6 | 36.0 | 36.3 |
| Max [°C] | 37.0 | 36.5 | 36.4 | 36.4 |
| Max-Min difference [°C] | 0.3 | 3.9 | 0.4 | 0.1 |
| Mean [°C] | 36.88 | 34.82 | 36.26 | 36.38 |
| Room temperature[°C] | 20.2 | |||
| Room humidity | 53% | |||
| Body temperature GT [°C] | 36.3 | |||
| Degree [°]–number | T1 [°C] | T2 [°C] | T3 [°C] | T4 [°C] |
| 0°–1 | 36.2 | 36.3 | 35.9 | 36.2 |
| 0°–2 | 36.2 | 36.3 | 36.1 | 36.2 |
| 0°–3 | 36.2 | 36.3 | 36.0 | 36.2 |
| 0°–4 | 36.3 | 36.3 | 36.0 | 36.2 |
| 0°–5 | 36.3 | 36.3 | 36.0 | 36.2 |
| 23°–1 | 36.1 | 36.1 | 36.1 | 36.2 |
| 23°–2 | 36.2 | 36.1 | 36.2 | 36.2 |
| 23°–3 | 36.1 | 36.2 | 36.1 | 36.2 |
| 23°–4 | 36.1 | 36.0 | 36.2 | 36.2 |
| 23°–5 | 36.2 | 36.0 | 36.1 | 36.2 |
| 45°–1 | 35.9 | 35.7 | 36.0 | 36.2 |
| 45°–2 | 35.9 | 35.7 | 36.0 | 36.2 |
| 45°–3 | 35.9 | 35.7 | 36.0 | 36.2 |
| 45°–4 | 35.9 | 35.8 | 36.0 | 36.2 |
| 45°–5 | 35.9 | 35.7 | 36.0 | 36.2 |
| Min [°C] | 35.9 | 35.7 | 35.9 | 36.2 |
| Max [°C] | 36.3 | 36.3 | 36.2 | 36.2 |
| Max-Min difference [°C] | 0.4 | 0.6 | 0.3 | 0.0 |
| Mean [°C] | 36.09 | 36.03 | 36.05 | 36.20 |
| Room temperature[°C] | 20.2 | |||
| Room humidity | 50% | |||
| Body temperature GT [°C] | 36.3 | |||
| Degree [°]–number | T1 [°C] | T2 [°C] | T3 [°C] | T4 [°C] |
| 0°–1 | 36.1 | 36.0 | 35.8 | 36.3 |
| 0°–2 | 36.1 | 36.1 | 35.7 | 36.3 |
| 0°–3 | 36.2 | 36.0 | 35.7 | 36.3 |
| 0°–4 | 36.2 | 36.1 | 35.8 | 36.3 |
| 0°–5 | 36.2 | 36.1 | 35.8 | 36.3 |
| 23°–1 | 36.3 | 35.6 | 35.8 | 36.3 |
| 23°–2 | 36.2 | 35.4 | 35.8 | 36.3 |
| 23°–3 | 36.2 | 35.4 | 35.8 | 36.3 |
| 23°–4 | 36.2 | 35.4 | 35.9 | 36.3 |
| 23°–5 | 36.2 | 35.3 | 35.8 | 36.3 |
| 45°–1 | 36.1 | 34.9 | 35.8 | 36.3 |
| 45°–2 | 36.1 | 34.8 | 35.8 | 36.3 |
| 45°–3 | 36.1 | 34.8 | 35.8 | 36.3 |
| 45°–4 | 36.1 | 34.8 | 35.8 | 36.3 |
| 45°–5 | 36.1 | 34.9 | 35.8 | 36.3 |
| Min [°C] | 36.1 | 34.8 | 35.7 | 36.3 |
| Max [°C] | 36.3 | 36.1 | 35.9 | 36.3 |
| Max-Min difference [°C] | 0.2 | 1.3 | 0.2 | 0.0 |
| Mean [°C] | 36.16 | 35.44 | 35.79 | 36.30 |
| Room temperature[°C] | 20.0 | |||
| Room humidity | 51% | |||
| Body temperature GT [°C] | 36.6 | |||
| Degree [°]–number | T1 [°C] | T2 [°C] | T3 [°C] | T4 [°C] |
| 0°–1 | 36.7 | 36.3 | 36.2 | 36.6 |
| 0°–2 | 36.7 | 36.3 | 36.2 | 36.6 |
| 0°–3 | 36.7 | 36.3 | 36.2 | 36.5 |
| 0°–4 | 36.7 | 36.3 | 36.2 | 36.6 |
| 0°–5 | 36.7 | 36.3 | 36.2 | 36.6 |
| 23°–1 | 36.5 | 36.0 | 36.1 | 36.6 |
| 23°–2 | 36.5 | 36.0 | 36.2 | 36.6 |
| 23°–3 | 36.5 | 36.0 | 36.2 | 36.6 |
| 23°–4 | 36.5 | 35.9 | 36.2 | 36.6 |
| 23°–5 | 36.5 | 36.0 | 36.1 | 36.6 |
| 45°–1 | 36.5 | 35.3 | 36.1 | 36.6 |
| 45°–2 | 36.4 | 35.2 | 36.1 | 36.6 |
| 45°–3 | 36.4 | 35.2 | 36.1 | 36.6 |
| 45°–4 | 36.4 | 35.3 | 36.1 | 36.6 |
| 45°–5 | 36.5 | 35.2 | 36.2 | 36.6 |
| Min [°C] | 35.9 | 35.7 | 35.9 | 36.2 |
| Max [°C] | 36.3 | 36.3 | 36.2 | 36.2 |
| Max-Min difference [°C] | 0.4 | 0.6 | 0.3 | 0.0 |
| Mean [°C] | 36.09 | 36.03 | 36.05 | 36.20 |
| Room temperature[°C] | 20.4 | |||
| Room humidity | 50% | |||
| Body temperature GT [°C] | 36.3 | |||
| Light setting–number | T1 [°C] | T2 [°C] | T3 [°C] | T4 [°C] |
| I-1 | 36.5 | 36.3 | 36.4 | 36.2 |
| I-2 | 36.5 | 36.3 | 36.4 | 36.2 |
| I-3 | 36.5 | 36.3 | 36.4 | 36.2 |
| I-4 | 36.5 | 36.3 | 36.4 | 36.2 |
| I-5 | 36.5 | 36.3 | 36.4 | 36.2 |
| II-1 | 36.6 | 36.1 | 36.4 | 36.2 |
| II-2 | 36.5 | 36.1 | 36.5 | 36.2 |
| II-3 | 36.5 | 36.2 | 36.5 | 36.2 |
| II-4 | 36.5 | 36.0 | 36.5 | 36.2 |
| II-5 | 36.5 | 36.0 | 36.5 | 36.2 |
| III-1 | 36.5 | 35.9 | 36.6 | 36.2 |
| III-2 | 36.5 | 35.9 | 36.6 | 36.2 |
| III-3 | 36.5 | 36.4 | 36.7 | 36.2 |
| III-4 | 36.6 | 36.4 | 36.6 | 36.2 |
| III-5 | 36.6 | 36.4 | 36.5 | 36.2 |
| Min [°C] | 36.5 | 35.9 | 36.4 | 36.2 |
| Max [°C] | 36.6 | 36.4 | 36.7 | 36.2 |
| Max-Min difference [°C] | 0.1 | 0.5 | 0.3 | 0.0 |
| Mean [°C] | 36.52 | 36.19 | 36.49 | 36.20 |
| Room temperature[°C] | 20.4 | |||
| Room humidity | 50% | |||
| Body temperature GT [°C] | 36.3 | |||
| Light setting–number | T1 [°C] | T2 [°C] | T3 [°C] | T4 [°C] |
| I–1 | 36.3 | 36.1 | 36.0 | 36.3 |
| I–2 | 36.3 | 36.1 | 36.0 | 36.3 |
| I–3 | 36.3 | 36.1 | 36.0 | 36.2 |
| I–4 | 36.4 | 36.2 | 36.0 | 36.3 |
| I–5 | 36.3 | 36.2 | 36.0 | 36.2 |
| II–1 | 36.4 | 36.2 | 36.0 | 36.3 |
| II–2 | 36.4 | 36.1 | 36.0 | 36.3 |
| II–3 | 36.4 | 36.2 | 36.0 | 36.3 |
| II–4 | 36.5 | 36.2 | 36.0 | 36.3 |
| II–5 | 36.5 | 36.1 | 36.0 | 36.3 |
| III–1 | 36.5 | 36.2 | 36.1 | 36.3 |
| III–2 | 36.6 | 36.2 | 36.0 | 36.3 |
| III–3 | 36.6 | 36.2 | 36.1 | 36.3 |
| III–4 | 36.7 | 36.2 | 36.1 | 36.3 |
| III–5 | 36.7 | 36.2 | 36.0 | 36.3 |
| Min [°C] | 36.3 | 36.1 | 36.0 | 36.2 |
| Max [°C] | 36.7 | 36.2 | 36.1 | 36.3 |
| Max-Min difference [°C] | 0.4 | 0.1 | 0.1 | 0.1 |
| Mean [°C] | 36.46 | 36.17 | 36.02 | 36.29 |
| Room temperature[°C] | 20.0 | |||
| Room humidity | 51% | |||
| Body temperature GT [°C] | 36.3 | |||
| Light setting–number | T1 [°C] | T2 [°C] | T3 [°C] | T4 [°C] |
| I–1 | 36.7 | 36.3 | 36.3 | 36.5 |
| I–2 | 36.8 | 36.3 | 36.3 | 36.5 |
| I–3 | 36.7 | 36.3 | 36.3 | 36.5 |
| I–4 | 36.7 | 36.3 | 36.3 | 36.5 |
| I–5 | 36.7 | 36.3 | 36.3 | 36.5 |
| II–1 | 36.8 | 36.1 | 36.3 | 36.5 |
| II–2 | 36.8 | 36.1 | 36.3 | 36.5 |
| II–3 | 36.8 | 36.1 | 36.3 | 36.5 |
| II–4 | 36.8 | 36.2 | 36.4 | 36.5 |
| II–5 | 36.8 | 36.3 | 36.4 | 36.5 |
| III–1 | 36.8 | 36.0 | 36.4 | 36.5 |
| III–2 | 36.9 | 36.2 | 36.4 | 36.5 |
| III–3 | 36.8 | 36.1 | 36.4 | 36.5 |
| III–4 | 36.9 | 36.1 | 36.4 | 36.5 |
| III–5 | 36.9 | 36.1 | 36.4 | 36.5 |
| Min [°C] | 36.7 | 36.0 | 36.3 | 36.5 |
| Max [°C] | 36.9 | 36.3 | 36.4 | 36.5 |
| Max-Min difference [°C] | 0.2 | 0.3 | 0.1 | 0.0 |
| Mean [°C] | 36.8 | 36.2 | 36.3 | 36.5 |
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- Chang, M.C.; Park, D. How Should Rehabilitative Departments of Hospitals Prepare for Coronavirus Disease 2019? Am. J. Phys. Med. Rehabil. 2020, 99, 475–476. [Google Scholar] [CrossRef]
- Manivannan, M.; Jogalekar, M.P.; Kavitha, M.S.; Maran, B.A.V.; Gangadaran, P. A mini-review on the effects of COVID-19 on younger individuals. Exp. Biol. Med. 2021, 246, 293–297. [Google Scholar] [CrossRef]
- Jin, J.-M.; Bai, P.; He, W.; Wu, F.; Liu, X.-F.; Han, D.-M.; Liu, S.; Yang, J.-K. Gender Differences in Patients With COVID-19: Focus on Severity and Mortality. Front. Public Health 2020, 8, 152. [Google Scholar] [CrossRef]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef]
- Struyf, T.; Deeks, J.J.; Dinnes, J.; Takwoingi, Y.; Davenport, C.; Leeflang, M.M.; Spijker, R.; Hooft, L.; Emperador, D.; Dittrich, S.; et al. Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19 disease. Cochrane Database Syst. Rev. 2020, 2020, CD013665. [Google Scholar] [CrossRef]
- Chang, M.C.; Park, Y.-K.; Kim, B.-O.; Park, D. Risk factors for disease progression in COVID-19 patients. BMC Infect. Dis. 2020, 20, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-H.; An, J.A.-R.; Min, P.-K.; Bitton, A.; Gawande, A.A. How South Korea Responded to the Covid-19 Outbreak in Daegu. NEJM Catal. 2020, 1. [Google Scholar] [CrossRef]
- Stella, A.B.; Manganotti, P.; Furlanis, G.; Accardo, A.; Ajčević, M. Return to school in the COVID-19 era: Considerations for temperature measurement. J. Med. Eng. Technol. 2020, 44, 468–471. [Google Scholar] [CrossRef] [PubMed]
- Dadashzadeh, A.; Alamdari, N.G.; Ala, A.; Dehghannejad, J.; Jabbarzadeh, F.; Babaie, N. Triage guidelines for emergency department patients with COVID-19. J. Res. Clin. Med. 2020, 8, 12. [Google Scholar] [CrossRef]
- Lahiri, B.; Bagavathiappan, S.; Jayakumar, T.; Philip, J. Medical applications of infrared thermography: A review. Infrared Phys. Technol. 2012, 55, 221–235. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, N.; Garg, M.; Dwarakanathan, V.; Gautam, N.; Kumar, S.S.; Jadon, R.S.; Gupta, M.; Ray, A. Diagnostic accuracy of non-contact infrared thermometers and thermal scanners: A systematic review and meta-analysis. J. Travel Med. 2020, 27, 193. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.-Y.; Chen, A.; Chen, C. Investigation of the Impact of Infrared Sensors on Core Body Temperature Monitoring by Comparing Measurement Sites. Sensors 2020, 20, 2885. [Google Scholar] [CrossRef]
- Diwanji, M.M.; Hisvankar, S.M.; Khandelwal, C.S. Temperature Measurement using Infrared Contactless Thermal Gun. In Proceedings of the 2020 International Conference on Smart Innovations in Design, Environment, Management, Planning and Computing (ICSIDEMPC), Aurangabad, India, 30–31 October 2020; Institute of Electrical and Electronics Engineers (IEEE): Piscataway, NJ, USA, 2020; pp. 134–137. [Google Scholar]
- Osio, C.E.; Carnelli, V. Comparative study of body temperature measured with a non-contact infrared thermometer versus conventional devices. The first Italian study on 90 pediatric patients. Minerva Pediatr. 2007, 59, 327–336. [Google Scholar]
- Zhang, B.; Kreps, S.; McMurry, N.; McCain, R.M. Americans’ perceptions of privacy and surveillance in the COVID-19 pandemic. PLoS ONE 2020, 15, e0242652. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Yang, R. COVID-19 transmission through asymptomatic carriers is a challenge to containment. Influ. Other Respir. Viruses 2020, 14, 474–475. [Google Scholar] [CrossRef] [PubMed]
- Gerensea, H.; Murugan, R. Is There Significant Difference between Digital and Glass Mercury Thermometer? Adv. Nurs. 2016, 2016, 1–10. [Google Scholar] [CrossRef]
- Hsiao, S.-H.; Chen, T.-C.; Chien, H.-C.; Yang, C.-J.; Chen, Y.-H. Measurement of body temperature to prevent pandemic COVID-19 in hospitals in Taiwan: Repeated measurement is necessary. J. Hosp. Infect. 2020, 105, 360–361. [Google Scholar] [CrossRef]
- Qian, G.; Yang, N.; Ma, A.H.Y.; Wang, L.; Li, G.; Chen, X.; Chen, X. COVID-19 Transmission Within a Family Cluster by Presymptomatic Carriers in China. Clin. Infect. Dis. 2020, 71, 861–862. [Google Scholar] [CrossRef]
- Fletcher, T.; Whittam, A.; Simpson, R.; Machin, G. Comparison of non-contact infrared skin thermometers. J. Med. Eng. Technol. 2018, 42, 65–71. [Google Scholar] [CrossRef]
- Dell’Isola, G.B.; Cosentini, E.; Canale, L.; Ficco, G.; Dell’Isola, M. Noncontact body temperature measurement: Uncertainty evaluation and screening decision rule to prevent the dpread of COVID-19. Sensors 2021, 21, 346. [Google Scholar] [CrossRef]
- Quattrocchi, A.; Freni, F.; Montanini, R. Self-heat generation of embedded piezoceramic patches used for fabrication of smart materials. Sens. Actuators A Phys. 2018, 280, 513–520. [Google Scholar] [CrossRef]
- Piccinini, F.; Tesei, A.; Paganelli, G.; Zoli, W.; Bevilacqua, A. Improving reliability of live/dead cell counting through automated image mosaicing. Comput. Methods Programs Biomed. 2014, 117, 448–463. [Google Scholar] [CrossRef] [PubMed]
- Apa, H.; Gözmen, S.; Bayram, N.; Çatkoglu, A.; Devrim, F.; Karaarslan, U.; Günay, İ.; Ünal, N.; Devrim, İ. Clinical accuracy of tympanic thermometer and noncontact infrared skin thermometer in pediatric practice: An alternative for axillary digital thermometer. Pediatric Emerg. Care 2013, 29, 992–997. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.H.; Patel, M.M.; Bhavsar, R.H. Comparison of Non-Contact Forehead Infrared Thermometry with Axillary Digital Thermometry in Neonates. GCSMC J. Med. Sci. 2016, 20, 20–24. [Google Scholar]






| Company | TECNIMED | Medek | FLUS | Berrcom |
|---|---|---|---|---|
| Model | VisioFocus PRO 06480 | MDI261 | IR-805B | JXB-178 |
| Manufactured in: | Italy | China | China | China |
| Operating room temperature [°C] | 16–40 | 10–40 | 10–50 | 10–40 |
| Measuring range [°C] | 34–42.5 | 32–43 | 32–42 | 32–42.9 |
| Resolution [°C] | 0.1 | 0.1 | 0.1 | 0.1 |
| Accuracy [°C] | ±0.3 from 34 to 35.9 ±0.2 from 36 to 39 ±0.3 from 39.1 to 42.5 | ±0.3 from 34 to 35.4 ±0.2 from 35.5 to 42 ±0.3 from 42.1 to 42.9 | ±0.3 from 32 to 35.9 ±0.2 from 36 to 39 ±0.3 from 39.1 to 42 | ±0.3 from 32 to 34.9 ±0.2 from 35 to 42 ±0.3 from 42.1 to 42.9 |
| Working distance [cm] | 5–10 | 1–3 | 5 | 3–5 |
| Standards | ASTM E1965.98 | ASTM E1965.98 | ASTM E1965.98 | ASTM E1965.98 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piccinini, F.; Martinelli, G.; Carbonaro, A. Reliability of Body Temperature Measurements Obtained with Contactless Infrared Point Thermometers Commonly Used during the COVID-19 Pandemic. Sensors 2021, 21, 3794. https://doi.org/10.3390/s21113794
Piccinini F, Martinelli G, Carbonaro A. Reliability of Body Temperature Measurements Obtained with Contactless Infrared Point Thermometers Commonly Used during the COVID-19 Pandemic. Sensors. 2021; 21(11):3794. https://doi.org/10.3390/s21113794
Chicago/Turabian StylePiccinini, Filippo, Giovanni Martinelli, and Antonella Carbonaro. 2021. "Reliability of Body Temperature Measurements Obtained with Contactless Infrared Point Thermometers Commonly Used during the COVID-19 Pandemic" Sensors 21, no. 11: 3794. https://doi.org/10.3390/s21113794
APA StylePiccinini, F., Martinelli, G., & Carbonaro, A. (2021). Reliability of Body Temperature Measurements Obtained with Contactless Infrared Point Thermometers Commonly Used during the COVID-19 Pandemic. Sensors, 21(11), 3794. https://doi.org/10.3390/s21113794