Concurrent Validity of a Novel Wireless Inertial Measurement System for Assessing Trunk Impairment in People with Stroke

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Participant Characteristics
3.2. Concurrent Validity
3.3. Differences between Groups
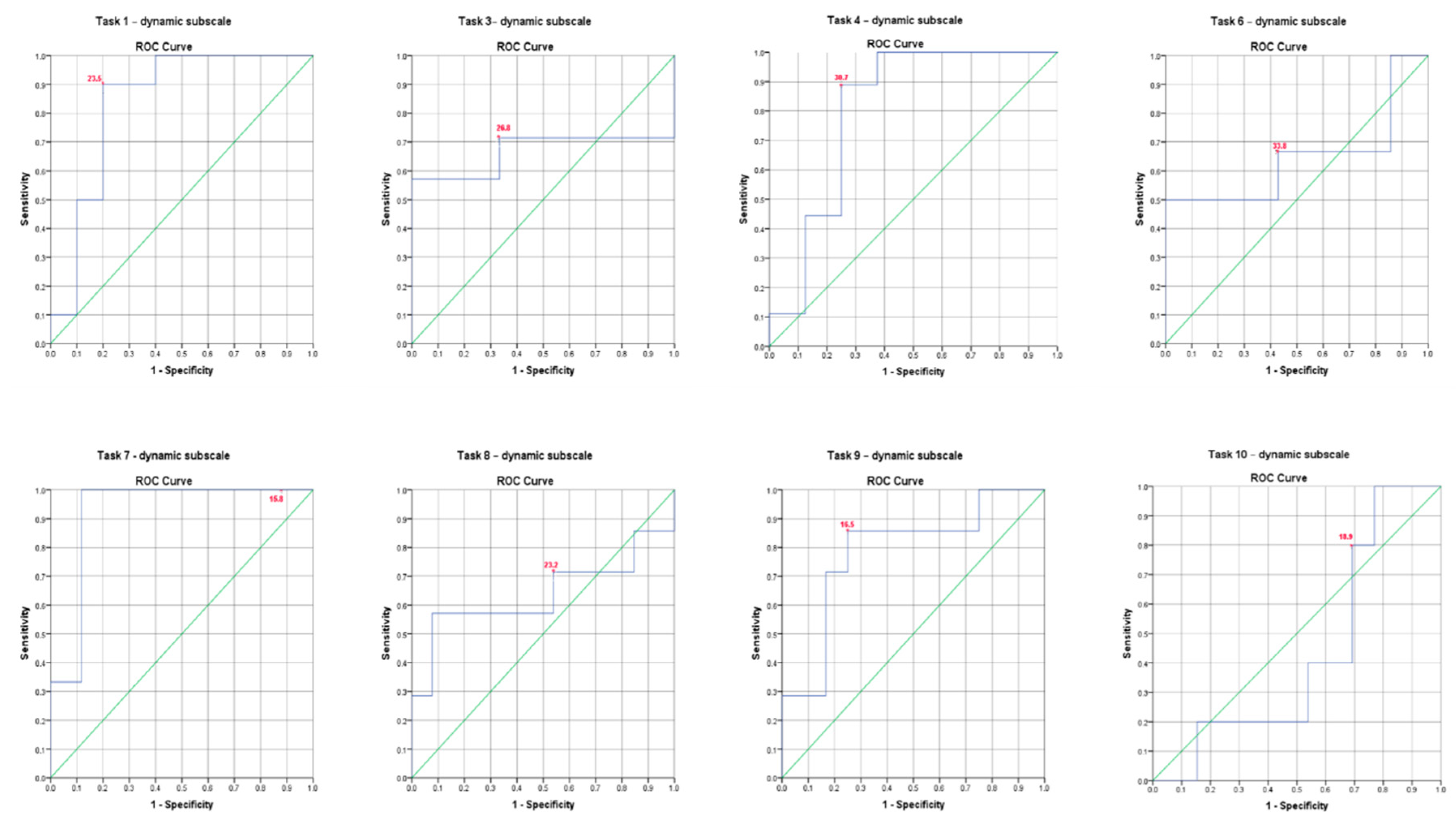
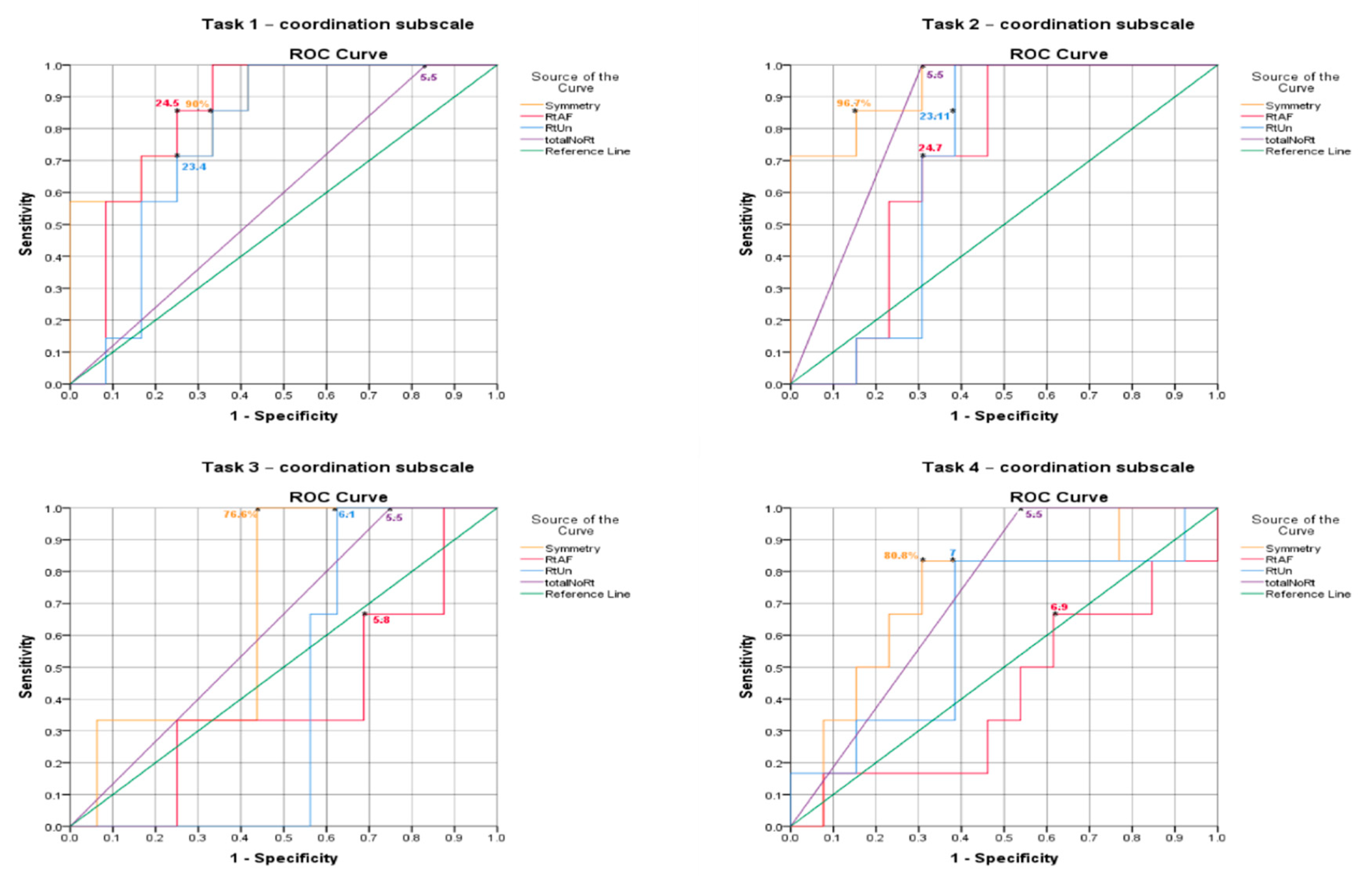
3.4. ROC Curve Analysis
4. Discussion
4.1. Validity
4.2. Differences between Groups
4.3. Limitations
5. Clinical Implications and Recommendations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Edwards, S. Neurological Physiotherapy: A Problem-solving Approach; Churchill Livingstone: London, UK, 1996. [Google Scholar]
- Davies, P.M.; Klein-Vogelbach, S. Right in the Middle: Selective Trunk Activity in the Treatment of Adult Hemiplegia; Springer: Berlin/Heidelberg, Germany, 2012. [Google Scholar]
- Sunderland, A.; Tinson, D.; Bradley, L.; Hewer, R.L. Arm function after stroke. An evaluation of grip strength as a measure of recovery and a prognostic indicator. J. Neurol. Neurosurg. Psychiatry 1989, 52, 1267–1272. [Google Scholar] [CrossRef] [PubMed]
- Ryerson, S.; Byl, N.N.; Brown, D.A.; Wong, R.A.; Hidler, J.M. Altered trunk position sense and its relation to balance functions in people post-stroke. J. Neurol. Phys. Ther. 2008, 32, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Langhorne, P.; Coupar, F.; Pollock, A. Motor recovery after stroke: A systematic review. Lancet Neurol. 2009, 8, 741–754. [Google Scholar] [CrossRef]
- Rosenblum, S.; Josman, N. The relationship between postural control and fine manual dexterity. Phys. Occup. Ther. Pediatr. 2003, 23, 47–60. [Google Scholar] [CrossRef] [PubMed]
- Franchignoni, F.P.; Tesio, L.; Ricupero, C.; Martino, M.T. Trunk control test as an early predictor of stroke rehabilitation outcome. Stroke 1997, 28, 1382–1385. [Google Scholar] [CrossRef] [PubMed]
- Verheyden, G.; Nieuwboer, A.; De Wit, L.; Feys, H.; Schuback, B.; Baert, I.; Jenni, W.; Schupp, W.; Thijs, V.; De Weerdt, W. Trunk performance after stroke: An eye catching predictor of functional outcome. J. Neurol. Neurosurg. Psychiatry 2007, 78, 694–698. [Google Scholar] [CrossRef] [PubMed]
- Collin, C.; Wade, D. Assessing motor impairment after stroke: A pilot reliability study. J. Neurol. Neurosurg. Psychiatry 1990, 53, 576–579. [Google Scholar] [CrossRef]
- Verheyden, G.; Nieuwboer, A.; Mertin, J.; Preger, R.; Kiekens, C.; De Weerdt, W. The Trunk Impairment Scale: A new tool to measure motor impairment of the trunk after stroke. Clin. Rehabil. 2004, 18, 326–334. [Google Scholar] [CrossRef]
- Sullivan, J.E.; Crowner, B.E.; Kluding, P.M.; Nichols, D.; Rose, D.K.; Yoshida, R.; Pinto Zipp, G. Outcome measures for individuals with stroke: Process and recommendations from the American Physical Therapy Association neurology section task force. Phys. Ther. 2013, 93, 1383–1396. [Google Scholar] [CrossRef]
- Verheyden, G.; Nieuwboer, A.; Feys, H.; Thijs, V.; Vaes, K.; De Weerdt, W. Discriminant ability of the Trunk Impairment Scale: A comparison between stroke patients and healthy individuals. Disabil. Rehabil. 2005, 27, 1023–1028. [Google Scholar] [CrossRef]
- Verheyden, G.; Kersten, P. Investigating the internal validity of the Trunk Impairment Scale (TIS) using Rasch analysis: The TIS 2.0. Disabil. Rehabil. 2010, 32, 2127–2137. [Google Scholar] [CrossRef] [PubMed]
- Carozzo, S.; Serra, S.; Pignolo, L.; Tonin, P.; Cerasa, A. The assessment of trunk recovery in stroke patients using 3D kinematic measures. Med. Eng. Phys. 2020. [Google Scholar] [CrossRef] [PubMed]
- Karthikbabu, S.; Chakrapani, M.; Ganeshan, S.; Rakshith, K.C.; Nafeez, S.; Prem, V. A review on assessment and treatment of the trunk in stroke: A need or luxury. Neural Regen. Res. 2012, 7, 1974–1977. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, A.; Kanzler, C.M.; Lambercy, O.; Luft, A.R.; Veerbeek, J.M. Systematic Review on Kinematic Assessments of Upper Limb Movements After Stroke. Stroke 2019, 50, 718–727. [Google Scholar] [CrossRef]
- Cuesta-Vargas, A.; Galán-Mercant, A.; Williams, J. The use of inertial sensors system for human motion analysis. Phys. Ther. Rev. 2010, 15, 462–473. [Google Scholar] [CrossRef]
- Bauer, C.M.; Rast, F.M.; Ernst, M.J.; Kool, J.; Oetiker, S.; Rissanen, S.M.; Suni, J.H.; Kankaanpaa, M. Concurrent validity and reliability of a novel wireless inertial measurement system to assess trunk movement. J. Electromyogr. Kinesiol. 2015, 25, 782–790. [Google Scholar] [CrossRef]
- Hugli, A.S.; Ernst, M.J.; Kool, J.; Rast, F.M.; Rausch-Osthoff, A.K.; Mannig, A.; Oetiker, S.; Bauer, C.M. Adherence to home exercises in non-specific low back pain. A randomised controlled pilot trial. J. Bodyw. Mov. Ther. 2015, 19, 177–185. [Google Scholar] [CrossRef]
- Karras, D.J. Statistical methodology: II. Reliability and variability assessment in study design, Part A. Acad. Emerg. Med. 1997, 4, 64–71. [Google Scholar] [CrossRef]
- Munro, B.H. Statistical Methods for Health Care Research; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2001. [Google Scholar]
- Portney, L.G.; Watkins, M.P. Foundations of Clinical Research: Pearson New International Edition: Applications to Practice; Pearson Education Limited: Essex, UK, 2013. [Google Scholar]
- Fluss, R.; Faraggi, D.; Reiser, B. Estimation of the Youden Index and its associated cutoff point. Biom. J. 2005, 47, 458–472. [Google Scholar] [CrossRef]
- Jijimol, G.; Fayaz, R.K.; Vijesh, P.V. Correlation of trunk impairment with balance in patients with chronic stroke. NeuroRehabilitation 2013, 32, 323–325. [Google Scholar] [CrossRef]
- Messier, S.; Bourbonnais, D.; Desrosiers, J.; Roy, Y. Dynamic analysis of trunk flexion after stroke. Arch. Phys. Med. Rehabil. 2004, 85, 1619–1624. [Google Scholar] [CrossRef] [PubMed]
- Gillen, G. Stroke Rehabilitation—E-Book: A Function-Based Approach; Elsevier Health Sciences: St. Louis, MO, USA, 2015. [Google Scholar]
- Dickstein, R.; Shefi, S.; Marcovitz, E.; Villa, Y. Anticipatory postural adjustment in selected trunk muscles in post stroke hemiparetic patients. Arch. Phys. Med. Rehabil. 2004, 85, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, S.; Hachisuka, K.; Ogata, H. Trunk rotatory muscle performance in post-stroke hemiplegic patients. Am. J. Phys. Med. Rehabil. 1997, 76, 366–369. [Google Scholar] [CrossRef] [PubMed]
- Stenlund, T.C.; Öhberg, F.; Lundström, R.; Lindroos, O.; Häger, C.; Rehn, B. Inter- and intra-tester reliability when measuring seated spinal postures with inertial sensors. Int. J. Ind. Ergon. 2014, 44, 732–738. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| cTIS-V2 Tasks | Sensor | Parameter of Interest | Plane of Movement |
|---|---|---|---|
| Dynamic Sitting Balance Subscale | |||
| 1—Touch the bed with the hemiplegic elbow | Sternum | ROM of lateral flexion to non-dominant/affected * side (degrees) | Frontal |
| 2—Repeat Item 1 | Sternum | ROM of lateral flexion to non-dominant/affected side (degrees) | Frontal |
| 3—Repeat Item 1 | Sternum | ROM of lateral flexion to non-dominant/affected side (degrees) | Frontal |
| 4—Touch the bed with the unaffected elbow | Sternum | ROM of lateral flexion to dominant/unaffected side (degrees) | Frontal |
| 5—Repeat Item 4 | Sternum | ROM of lateral flexion to dominant/unaffected side (degrees) | Frontal |
| 6—Repeat Item 4 | Sternum | ROM of lateral flexion to dominant/unaffected side (degrees) | Frontal |
| 7—Lift pelvis from bed at the hemiplegic side | Sacrum | ROM of lateral flexion to dominant/unaffected side (degrees) ** | Frontal |
| 8—Repeat Item 7 | Sacrum | ROM of lateral flexion to dominant/unaffected side (degrees) ** | Frontal |
| 9—Lift pelvis from bed at the unaffected side | Sacrum | ROM of lateral flexion to non-dominant/affected side (degrees) ** | Frontal |
| 10—Repeat Item 9 | Sacrum | ROM of lateral flexion to non-dominant/affected side (degrees) ** | Frontal |
| Coordination Subscale | |||
| 1—Rotate upper trunk 6 times | Sternum | Symmetry (%), ROM of average rotation to both side (degrees) and total no. of rotations | Transverse |
| 2—Repeat Item 1 within 6 s | Sternum | Symmetry (%), ROM of average rotation to both side (degrees) and total no. of rotations | Transverse |
| 3—Rotate lower trunk 6 times | Lumbar | Symmetry (%), ROM of average rotation to both side (degrees) and total no. of rotations | Transverse |
| 4—Repeat Item 3 within 6 s | Lumbar | Symmetry (%), ROM of average rotation to both side (degrees) and total no. of rotations | Transverse |
| Characteristics | Chronic Stroke (N = 20) | Healthy (N = 20) |
|---|---|---|
| Age (years) | 63.2 ± 11.12 | 62.75 ± 11.67 |
| Range: 44–79 | Range: 41–80 | |
| Gender | ||
| Male | 13 | 10 |
| Female | 7 | 10 |
| Hand dominance | ||
| Right | 17 | 16 |
| Left | 3 | 4 |
| Affected upper limb | ||
| Right | 5 | N/A |
| Left | 15 | |
| Trunk Impairment Scale (TIS) | 15.65 ± 2.70 | 22.8 ± 0.62 |
| Range: 10–23 | Range: 2–23 | |
| Number of participants with TIS: | ||
| ≤10 (poor trunk control) | 1 | 0 |
| 11–19 (fair trunk control) | 18 | 0 |
| ≥20 (good trunk control) | 1 | 20 |
| cTIS-V2 Tasks | Parameter of Interest | cTIS-V2 Score = 0 Mean ± SD | cTIS-V2 Score = 1 Mean ± SD | r-Value | Sig. |
|---|---|---|---|---|---|
| Dynamic Sitting Balance Subscale | |||||
| 1, 2—Touch the bed with the hemiplegic elbow | ROM of lateral flexion to affected side (degrees) | 29.21 ± 5.18 | 21.70 ± 7.18 | −0.59 ** | 0.006 |
| 3—Touch the bed with the hemiplegic elbow without compensation | ROM of lateral flexion to affected side (degrees) | 32.41 ± 10.36 | 25.21 ± 3.61 | −0.26 | 0.45 |
| 4, 5—Touch the bed with the unaffected elbow | ROM of lateral flexion to unaffected side (degrees) | 35.82 ± 4.98 | 29.75 ± 5.95 | −0.52 * | 0.02 |
| 6—Touch the bed with the unaffected elbow without compensation | ROM of lateral flexion to unaffected side (degrees) | 36.31 ± 8.59 | 32.41 ± 5.30 | −0.24 | 0.41 |
| 7—Lift pelvis from bed at the hemiplegic side | ROM of lateral flexion to unaffected side (degrees) | 13.74 ± 3.5 | 21.46 ± 4.9 | 0.52 * | 0.01 |
| 8—Lift pelvis from bed at the hemiplegic side without compensation | ROM of lateral flexion to affected side (degrees) | 18.92 ± 6.96 | 21.04 ± 4.65 | 0.23 | 0.33 |
| 9—Lift pelvis from bed at the unaffected side | ROM of lateral flexion to unaffected side (degrees) | 15.29 ± 2.60 | 18.42 ± 3.24 | 0.47 * | 0.03 |
| 10—Lift pelvis from bed at the unaffected side without compensation | ROM of lateral flexion to unaffected side (degrees) | 17.81 ± 2.20 | 17.49 ± 4.04 | −0.10 | 0.67 |
| cTIS-V2 Tasks | Parameter of Interest | cTIS-V2 Score = 0 Mean ± SD | cTIS-V2 Score = 1 Mean ± SD | cTIS-V2 Score = 2 Mean ± SD | r-Value | Sig. |
|---|---|---|---|---|---|---|
| Coordination Subscale | ||||||
| 1—Rotate upper trunk 6 times | Symmetry (%) | 84.86 ± 14.40 | 78.46 ± 18.9 | 94.51 ± 3.61 | 0.54 * | 0.02 |
| ROM of average rotation to affected side (degrees) | 17.76 ± 9.00 | 21.45 ± 9.43 | 28.01 ± 4.21 | 0.57 ** | 0.01 | |
| ROM of average rotation to unaffected side (degrees) | 26.54 ± 19.73 | 15.65 ± 7.80 | 25.49 ± 4.20 | 0.32 | 0.17 | |
| Total number of rotations | 5 ± 0 | 6 ± 0 | 6 ± 0 | 0.59 ** | 0.007 | |
| 2—Repeat Item 1 within 6 s | Symmetry (%) | 78.94 ± 18.24 | 97.61 ± 1.29 | 0.71 **† | 0.001 | |
| ROM of average rotation to affected side (degrees) | 20.71 ± 12.04 | 26.53 ± 4.72 | 0.34 | 0.14 | ||
| ROM of average rotation to unaffected side (degrees) | 18.67 ± 11.91 | 26.07 ± 3.79 | 0.32 | 0.17 | ||
| Total number of rotations | 5.15 ± 0.68 | 6 ± 0 | 0.64 **† | 0.002 | ||
| 3—Rotate lower trunk 6 times | Symmetry (%) | 69.42 ± 16.52 | 74.36 ± 20.57 | 85.89 ± 8.80 | 0.28 | 0.24 |
| ROM of average rotation to affected side (degrees) | 9.22 ± 6.75 | 9.01 ± 4.48 | 7.46 ± 3.50 | −0.03 | 0.87 | |
| ROM of average rotation to unaffected side (degrees) | 7.20 ± 4.19 | 8.51 ± 4.29 | 6.87 ± 0.45 | 0.02 | 0.92 | |
| Total number of rotations | 6 ± 0 | 6 ± 0 | 5.20 ± 0.45 | 0.74 ** † | 0.001 | |
| 4—Repeat Item 3 within 6 s | Symmetry (%) | 77.20 ± 18.98 | 88.94 ± 11.02 | 0.37 | 0.11 | |
| ROM of average rotation to affected side (degrees) | 9.18 ± 4.98 | 8.08 ± 4.88 | −0.14 | 0.55 | ||
| ROM of average rotation to unaffected side (degrees) | 7.39 ± 4.48 | 9.21 ± 4.66 | 0.20 | 0.39 | ||
| Total number of rotations | 5.53 ± 0.51 | 6 ± 0 | 0.46 * | 0.04 | ||
| cTIS-V2 Tasks | Parameter of Interest | Stroke Mean ± SD | Healthy Mean ± SD | Mean Diff ± SD | 95% CI for Mean Diff | p-Value |
|---|---|---|---|---|---|---|
| Dynamic Sitting Balance Subscale | ||||||
| Task 1 | ROM of lateral flexion to non-dominant/affected side (degrees) | 24.66 ± 7.75 | 37.23 ± 5.70 | −12.57 ± 7.49 | −16.93 to −8.21 | 0.000 * |
| Task 2 | ROM of lateral flexion to non-dominant/affected side (degrees) | 21.51 ± 11.22 | 34 ± 10.89 | 12.49 ± 13.95 | −21.21 to −3.75 | 0.007 * |
| Task 3 | ROM of lateral flexion to non-dominant/affected side (degrees) | 28.78 ± 7.7 | 35.39 ± 8.09 | 6.61 ± 10.49 | −13.18 to −0.037 | 0.05 * |
| Task 4 | ROM of lateral flexion to dominant/unaffected side (degrees) | 34.04 ± 6.62 | 35.04 ± 7.09 | −1 ± 12.8 | −5.57 to 3.57 | 0.66 |
| Task 5 | ROM of lateral flexion to dominant/unaffected side (degrees) | 33.21 ± 9.55 | 34.37 ± 8.26 | −1.16 ± 14.25 | −7.40 to 5.10 | 0.71 |
| Task 6 | ROM of lateral flexion to dominant/unaffected side (degrees) | 27.01 ± 9.23 | 34.87 ± 8.43 | 7.86 ± 12.71 | −14.08 to −1.63 | 0.01 * |
| Task 7 | ROM of lateral flexion to dominant/unaffected side (degrees) | 20.11 ± 5.54 | 22.44 ± 5.2 | −2.32 ± 8.94 | −5.97 to 1.31 | 0.20 |
| Task 8 | ROM of lateral flexion to dominant/unaffected side (degrees) | 19.02 ± 5.51 | 23.29 ± 6.99 | −4.27 ± 9.97 | −8.46 to −0.082 | 0.05 * |
| Task 9 | ROM of lateral flexion to non-dominant/affected side (degrees) | 16.38 ± 4.41 | 23.74 ± 6.18 | −7.36 ± 7.25 | −10.86 to −3.86 | 0.000 * |
| Task 10 | ROM of lateral flexion to non-dominant/affected side (degrees) | 16.50 ± 5.02 | 25.93 ± 6.54 | −9.42 ± 8.31 | −13.45 to −5.39 | 0.000 * |
| Coordination Subscale | ||||||
| Task 1 | Symmetry (%) | 87.58 ± 13.15 | 93.75 ± 7.92 | −6.17 ± 17.30 | −14.08 to 1.74 | 0.12 |
| ROM of average rotation to non-dominant/affected side (degrees) | 22.17 ± 6.32 | 16.86 ± 7.19 | 5.31 ± 11.06 | 0.32 to 10.30 | 0.04 * | |
| ROM of average rotation to dominant/unaffected side (degrees) | 20.92 ± 8.70 | 30.68 ± 6.86 | −9.76 ± 10.83 | −15.50 to −4.01 | 0.002 * | |
| Total number of rotations | 5.93 ± 0.25 | 6 ± 0.00 | −0.06 ± 0.31 | −0.19 to 0.06 | 0.310 | |
| Task 2 | Symmetry (%) | 86.34 ± 13.16 | 91.72 ± 5.90 | −5.37 ± 13.27 | −12.41 to 1.66 | 0.129 |
| ROM of average rotation to non-dominant/affected side (degrees) | 32.59 ± 7.18 | 22.70 ± 8.69 | 9.88 ± 10.74 | 4.15 to 15.62 | 0.001 * | |
| ROM of average rotation to dominant/unaffected side (degrees) | 21.85 ± 8.28 | 29.15 ± 7.91 | −7.30 ± 10.53 | −13.06 to −1.54 | 0.015 * | |
| Total number of rotations | 5.60 ± 0.73 | 6 ± 0.00 | −0.40 ± 0.76 | −0.75 to −0.046 | 0.03 * | |
| Task 3 | Symmetry (%) | 78.42 ± 17.92 | 87.16 ± 9.84 | −8.74 ± 25.58 | −19.36 to 1.87 | 0.10 |
| ROM of average rotation to non-dominant/affected side (degrees) | 7.43 ± 3.83 | 14.95 ± 7.52 | −7.51 ± 9.49 | −12.37 to −2.64 | 0.004 * | |
| ROM of average rotation to dominant/unaffected side (degrees) | 7.89 ± 2.73 | 13.11 ± 5.55 | −5.21 ± 5.95 | −8.79 to −1.64 | 0.006 * | |
| Total number of rotations | 5.83 ± 0.38 | 6 ± 0.00 | −0.16 ± 0.30 | −0.35 to 0.02 | 0.08 | |
| Task 4 | Symmetry (%) | 80.89 ± 18.03 | 87 ± 11.34 | −6.11 ± 21.50 | −16.98 to 4.76 | 0.26 |
| ROM of average rotation to non-dominant/affected side (degrees) | 9.71 ± 4.78 | 15.38 ± 5.04 | −5.67 ± 9.51 | −9.22 to −2.12 | 0.003 * | |
| ROM of average rotation to dominant/unaffected side (degrees) | 8.57 ± 4.60 | 13.27 ± 4.61 | −4.69 ± 7.21 | −8.03 to −1.36 | 0.007 * | |
| Total number of rotations | 5.75 ± 0.44 | 6 ± 0.00 | −0.25 ± 0.74 | −0.47 to −0.021 | 0.033 * | |
| TIS-V2 Tasks | Parameter of Interest | cTIS Score = 0 Mean ± SD | cTIS Score = 1 Mean ± SD | Mean Diff ± SD | 95% CI for Mean Diff | p-Value |
|---|---|---|---|---|---|---|
| Dynamic Sitting Balance Subscale | ||||||
| 1, 2—Touch the bed or table with the hemiplegic elbow | ROM of lateral flexion to affected side (degrees) | 29.21 ± 5.18 | 21.70 ± 7.18 | 7.51 ± 2.80 | 1.62 to 13.39 | 0.01 * |
| 3—Touch the bed or table with the hemiplegic elbow without compensation | ROM of lateral flexion to affected side (degrees) | 32.41 ± 10.36 | 25.21 ± 3.61 | 7.19 ± 6.31 | −7.36 to 21.76 | 0.28 |
| 4, 5—Touch the bed or table with the unaffected elbow | ROM of lateral flexion to unaffected side (degrees) | 35.82 ± 4.98 | 29.75 ± 5.95 | 6.07 ± 2.65 | 0.42 to 11.72 | 0.03 * |
| 6—Touch the bed or table with the unaffected elbow without compensation | ROM of lateral flexion to unaffected side (degrees) | 36.31 ± 8.59 | 32.41 ± 5.30 | 3.89 ± 3.89 | −4.67 to 12.46 | 0.33 |
| 7—Lift pelvis from bed or table at the hemiplegic side | ROM of lateral flexion to affected side (degrees) | 13.74 ± 3.5 | 21.46 ± 4.9 | −7.71 ± 3.02 | −14.07 to −1.36 | 0.02 * |
| 8—Lift pelvis from bed or table at the hemiplegic side without compensation | ROM of lateral flexion to affected side (degrees) | 18.92 ± 6.96 | 21.04 ± 4.65 | −2.12 ± 2.59 | −7.57 to 3.32 | 0.42 |
| 9—Lift pelvis from bed or table at the unaffected side | ROM of lateral flexion to unaffected side (degrees) | 15.29 ± 2.60 | 18.42 ± 3.24 | −3.12 ± 1.44 | −6.17 to −0.07 | 0.04 * |
| 10—Lift pelvis from bed or table at the unaffected side without compensation | ROM of lateral flexion to unaffected side (degrees) | 17.81 ± 2.20 | 17.49 ± 4.04 | 0.32 ± 1.93 | −3.76 to 4.41 | 0.86 |
| Coordination Subscale | ||||||
| Task 2 & 4 (Independent Samples t-Test) | ||||||
| 2—Repeat Item 1 within 6 s | Symmetry (%) | 78.94 ± 18.24 | 97.61 ± 1.29 | −18.66 ± 6.99 | −33.35 to −3.97 | 0.01 * |
| ROM of average rotation to non-dominant/affected side (degrees) | 20.71 ± 12.04 | 26.53 ± 4.72 | −5.81 ± 4.78 | −15.86 to 4.23 | 0.24 | |
| ROM of average rotation to dominant/unaffected side (degrees) | 18.67 ± 11.91 | 26.07 ± 3.79 | −7.40 ± 4.67 | −17.22 to 2.41 | 0.13 | |
| Total number of rotations | 5.15 ± 0.68 | 6 ± 0 | −0.84 ± 0.26 | −1.40 to −0.29 | 0.001 * | |
| 4—Repeat Item 3 within 6 s | Symmetry (%) | 77.20 ± 18.98 | 88.94 ± 11.02 | −11.74 ± 8.40 | −29.47 to 5.99 | 0.18 |
| ROM of average rotation to non-dominant/affected side (degrees) | 9.18 ± 4.98 | 8.08 ± 4.88 | 1.09 ± 2.44 | −4.06 to 6.25 | 0.65 | |
| ROM of average rotation to dominant/unaffected side (degrees) | 7.39 ± 4.48 | 9.21 ± 4.66 | −1.82 ± 2.23 | −6.54 to 2.90 | 0.42 | |
| Total number of rotations | 5.53 ± 0.51 | 6 ± 0 | −0.46 ± 0.21 | −0.91 to −0.007 | 0.04 * | |
| Task 1 & 3 (One-Way ANOVA Test) | ||||||
| cTIS-V2 Tasks | Parameter of Interest | cTIS Score = 0 Mean ± SD | cTIS Score = 1 Mean ± SD | cTIS Score = 2 Mean ± SD | p-Value | |
| 1—Rotate upper trunk 6 times | Symmetry (%) | 84.86 ± 14.40 | 78.46 ± 18.99 | 94.51 ± 3.61 | 0.04 * | |
| ROM of average rotation to non-dominant/affected side (degrees) | 17.76 ± 9.00 | 21.45 ± 9.43 | 28.01 ± 4.21 | 0.31 | ||
| ROM of average rotation to dominant/unaffected side (degrees) | 26.54 ± 19.73 | 15.65 ± 7.80 | 25.49 ± 4.20 | 0.002 * | ||
| Total number of rotations | 5 ± 0 | 6 ± 0 | 6 ± 0 | 0.001 | ||
| 3—Rotate lower trunk 6 times | Symmetry (%) | 69.42 ± 16.52 | 74.36 ± 20.57 | 85.89 ± 8.80 | 0.48 | |
| ROM of average rotation to non-dominant/affected side (degrees) | 9.22 ± 6.75 | 9.01 ± 4.48 | 7.46 ± 3.50 | 0.87 | ||
| ROM of average rotation to dominant/unaffected side (degrees) | 7.20 ± 4.19 | 8.51 ± 4.29 | 6.87 ± 0.45 | 0.74 | ||
| Total number of rotations | 5.20 ± 0.45 | 6 ± 0 | 6 ± 0 | 0.001 | ||
| TIS-V2 Tasks | iTIS Parameter | AUC | Std. Error | Sig. | 95% CI | Cut-Off Point (Degrees) to be Scored Zero in cTIS | Sensitivity | Specificity |
|---|---|---|---|---|---|---|---|---|
| Dynamic Sitting Balance Subscale | ||||||||
| 1, 2—Touch the bed or table with the hemiplegic elbow | ROM of lateral flexion to affected side (degrees) | 0.84 | 0.09 | 0.01 | 0.64–1 | ≥23.5 | 0.90 | 0.80 |
| 3—Touch the bed or table with the hemiplegic elbow without compensation | ROM of lateral flexion to affected side (degrees) | 0.67 | 0.17 | 0.42 | 0.32–1 | ≥26.8 | 0.71 | 0.67 |
| 4, 5—Touch the bed or table with the unaffected elbow | ROM of lateral flexion to unaffected side (degrees) | 0.80 | 0.12 | 0.03 | 0.57–1 | ≥30.7 | 0.88 | 0.75 |
| 6—Touch the bed or table with the unaffected elbow without compensation | ROM of lateral flexion to unaffected side (degrees) | 0.64 | 0.17 | 0.39 | 0.30–98 | ≥33.8 | 0.66 | 0.58 |
| 7—Lift pelvis from bed or table at the hemiplegic side | ROM of lateral flexion to affected side (degrees) | 0.92 | 0.06 | 0.02 | 0.79–1 | ≤15.8 | 1 | 0.88 |
| 8—Lift pelvis from bed or table at the hemiplegic side without compensation | ROM of lateral flexion to affected side (degrees) | 0.63 | 0.15 | 0.32 | 0.33–0.94 | ≤23.2 | 0.71 | 0.46 |
| 9—Lift pelvis from bed or table at the unaffected side | ROM of lateral flexion to unaffected side (degrees) | 0.78 | 0.11 | 0.04 | 0.56–1 | ≤16.5 | 0.85 | 0.75 |
| 10—Lift pelvis from bed or table at the unaffected side without compensation | ROM of lateral flexion to unaffected side (degrees) | 0.43 | 0.14 | 0.65 | 0.14–0.71 | ≤18.9 | 0.80 | 0.30 |
| Coordination Subscale | ||||||||
| 1—Rotate upper trunk 6 times | Symmetry (%) | 0.87 | 0.08 | 0.01 | 0.70–1 | 90 | 0.85 | 0.66 |
| ROM of average rotation to non-dominant/affected side (degrees) | 0.85 | 0.09 | 0.01 | 0.66–1 | 24.5 | 0.85 | 0.75 | |
| ROM of average rotation to dominant/unaffected side (degrees) | 0.77 | 0.11 | 0.05 | 0.56–0.99 | 23.4 | 0.71 | 0.75 | |
| Total number of rotations | 0.58 | 0.13 | 0.55 | 0.32–0.85 | 5.5 | 1 | 0.17 | |
| 2—Repeat Item 1 within 6 s | Symmetry (%) | 0.93 | 0.05 | 0.002 | 0.82–1 | 96.7 | 0.85 | 0.84 |
| ROM of average rotation to non-dominant/affected side (degrees) | 0.70 | 0.11 | 0.14 | 0.47–0.93 | 24.7 | 0.71 | 0.69 | |
| ROM of average rotation to dominant/unaffected side (degrees) | 0.70 | 0.12 | 0.16 | 0.45–0.93 | 23.11 | 0.85 | 0.61 | |
| Total number of rotations | 0.84 | 0.08 | 0.01 | 0.67–1 | 5.5 | 1 | 0.69 | |
| 3—Rotate lower trunk 6 times | Symmetry (%) | 0.70 | 0.14 | 0.31 | 0.41–0.96 | 76.6 | 1 | 0.56 |
| ROM of average rotation to non-dominant/affected side (degrees) | 0.40 | 0.17 | 0.58 | 0.05–0.74 | 5.8 | 0.66 | 0.31 | |
| ROM of average rotation to dominant/unaffected side (degrees) | 0.42 | 0.12 | 0.65 | 0.18–0.66 | 6.1 | 1 | 0.37 | |
| Total number of rotations | 0.63 | 0.16 | 0.50 | 0.32–0.93 | 5.5 | 1 | 0.25 | |
| 4—Repeat Item 3 within 6 s | Symmetry (%) | 0.73 | 0.12 | 0.11 | 0.48–0.98 | 80.8 | 0.83 | 0.69 |
| ROM of average rotation to non-dominant/affected side (degrees) | 0.41 | 0.14 | 0.53 | 0.12–0.69 | 6.9 | 0.66 | 0.38 | |
| ROM of average rotation to dominant/unaffected side (degrees) | 0.62 | 0.14 | 0.38 | 0.34–0.91 | 7 | 0.83 | 0.61 | |
| Total number of rotations | 0.73 | 0.11 | 0.11 | 0.50–0.95 | 5.5 | 1 | 0.46 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alhwoaimel, N.; Warner, M.; Hughes, A.-M.; Ferrari, F.; Burridge, J.; Wee, S.K.; Verheyden, G.; Turk, R. Concurrent Validity of a Novel Wireless Inertial Measurement System for Assessing Trunk Impairment in People with Stroke. Sensors 2020, 20, 1699. https://doi.org/10.3390/s20061699
Alhwoaimel N, Warner M, Hughes A-M, Ferrari F, Burridge J, Wee SK, Verheyden G, Turk R. Concurrent Validity of a Novel Wireless Inertial Measurement System for Assessing Trunk Impairment in People with Stroke. Sensors. 2020; 20(6):1699. https://doi.org/10.3390/s20061699
Chicago/Turabian StyleAlhwoaimel, Norah, Martin Warner, Ann-Marie Hughes, Federico Ferrari, Jane Burridge, Seng Kwee Wee, Geert Verheyden, and Ruth Turk. 2020. "Concurrent Validity of a Novel Wireless Inertial Measurement System for Assessing Trunk Impairment in People with Stroke" Sensors 20, no. 6: 1699. https://doi.org/10.3390/s20061699
APA StyleAlhwoaimel, N., Warner, M., Hughes, A.-M., Ferrari, F., Burridge, J., Wee, S. K., Verheyden, G., & Turk, R. (2020). Concurrent Validity of a Novel Wireless Inertial Measurement System for Assessing Trunk Impairment in People with Stroke. Sensors, 20(6), 1699. https://doi.org/10.3390/s20061699