Application of Wearables to Facilitate Virtually Supervised Intradialytic Exercise for Reducing Depression Symptoms

 ,
,  , ,
, ,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Demographics and Clinical Data
2.3. Assessment of Depression Symptom
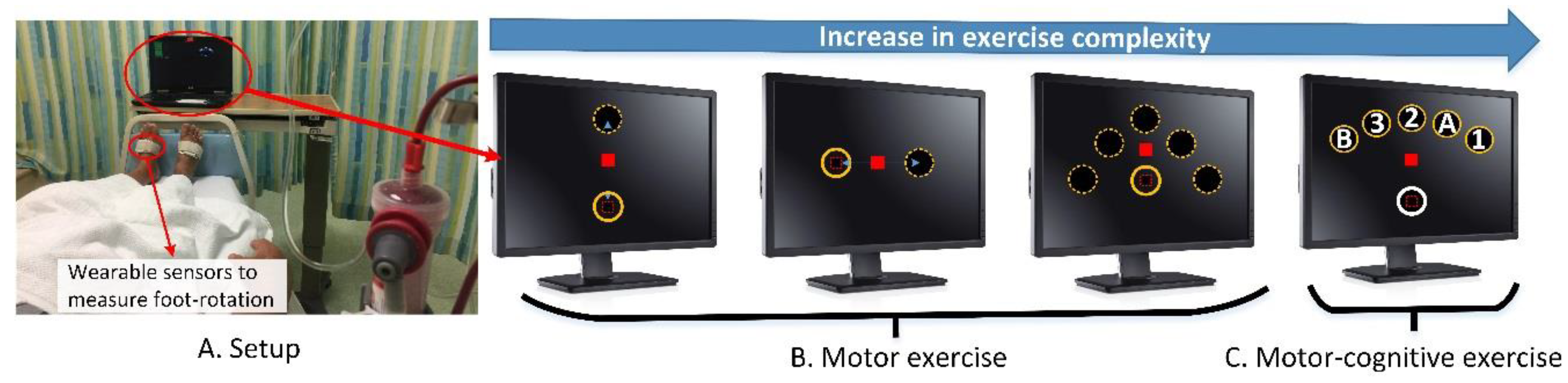
2.4. Intervention: Virtually Supervised Exercise using Intradialytic Exergame
2.5. Comparative Intervention: Nurse-Supervised Intradialytic Exercise
2.6. User Experience
2.7. Statistical Analysis
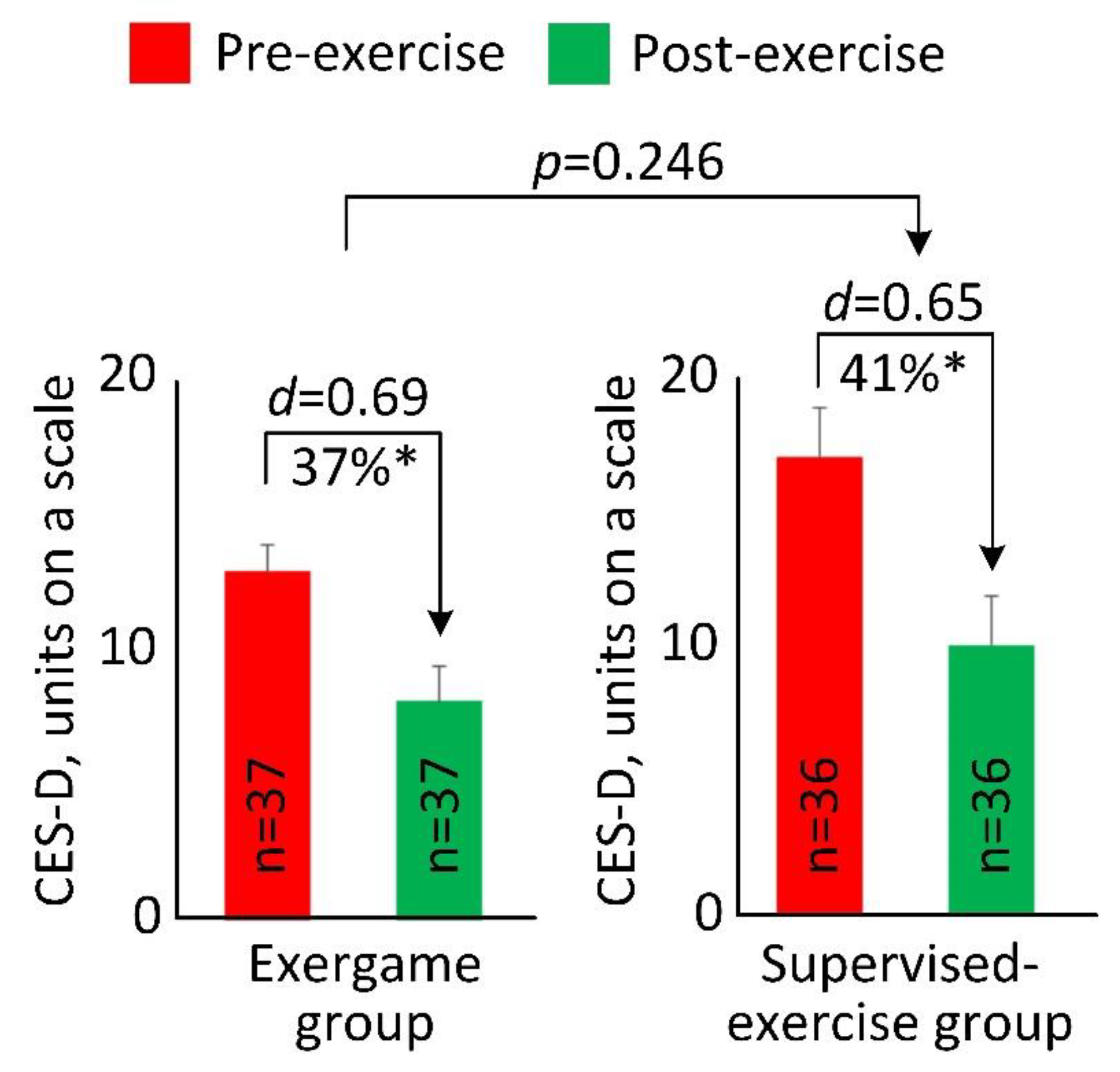
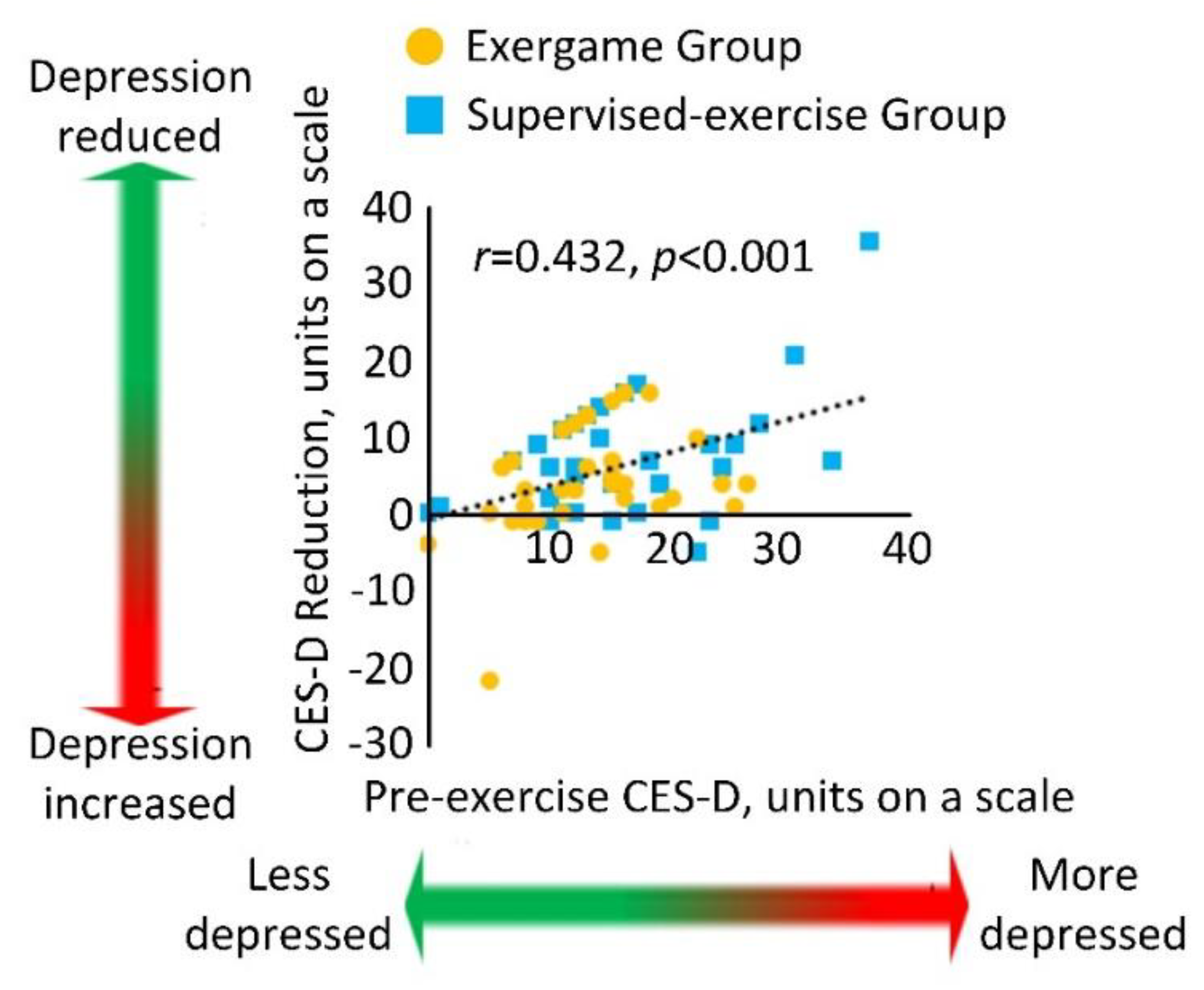
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Luyckx, V.A.; Tonelli, M.; Stanifer, J.W. The global burden of kidney disease and the sustainable development goals. Bull. World Health Organ. 2018, 96, 414–422D. [Google Scholar] [CrossRef] [PubMed]
- Levenson, J.L.; Glocheski, S. Psychological factors affecting end-stage renal disease. A review. Psychosomatics 1991, 32, 382–389. [Google Scholar] [CrossRef]
- Israel, M. Depression in dialysis patients: A review of psychological factors. Can. J. Psychiatry 1986, 31, 445–451. [Google Scholar] [CrossRef] [PubMed]
- Chilcot, J.; Wellsted, D.; Da Silva-Gane, M.; Farrington, K. Depression on dialysis. Nephron. Clin. Pract. 2008, 108, c256–c264. [Google Scholar] [CrossRef] [PubMed]
- Semaan, V.; Noureddine, S.; Farhood, L. Prevalence of depression and anxiety in end-stage renal disease: A survey of patients undergoing hemodialysis. Appl. Nurs. Res. 2018, 43, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Hedayati, S.S.; Grambow, S.C.; Szczech, L.A.; Stechuchak, K.M.; Allen, A.S.; Bosworth, H.B. Physician-diagnosed depression as a correlate of hospitalizations in patients receiving long-term hemodialysis. Am. J. Kidney Dis. 2005, 46, 642–649. [Google Scholar] [CrossRef]
- Lopes, A.A.; Bragg, J.; Young, E.; Goodkin, D.; Mapes, D.; Combe, C.; Piera, L.; Held, P.; Gillespie, B.; Port, F.K. Depression as a predictor of mortality and hospitalization among hemodialysis patients in the United States and Europe. Kidney Int. 2002, 62, 199–207. [Google Scholar] [CrossRef]
- Agganis, B.T.; Weiner, D.E.; Giang, L.M.; Scott, T.; Tighiouart, H.; Griffith, J.L.; Sarnak, M.J. Depression and cognitive function in maintenance hemodialysis patients. Am. J. Kidney Dis. 2010, 56, 704–712. [Google Scholar] [CrossRef]
- Kutner, N.G.; Brogan, D.; Hall, W.D.; Haber, M.; Daniels, D.S. Functional impairment, depression, and life satisfaction among older hemodialysis patients and age-matched controls: A prospective study. Arch. Phys. Med. Rehabil. 2000, 81, 453–459. [Google Scholar] [CrossRef]
- Evans, R.W.; Manninen, D.L.; Garrison, L.P., Jr.; Hart, L.G.; Blagg, C.R.; Gutman, R.A.; Hull, A.R.; Lowrie, E.G. The quality of life of patients with end-stage renal disease. N. Engl. J. Med. 1985, 312, 553–559. [Google Scholar] [CrossRef]
- Finkelstein, F.O.; Wuerth, D.; Troidle, L.K.; Finkelstein, S.H. Depression and end-stage renal disease: A therapeutic challenge. Kidney Int. 2008, 74, 843–845. [Google Scholar] [CrossRef] [PubMed]
- Cleare, A.; Pariante, C.M.; Young, A.H.; Anderson, I.M.; Christmas, D.; Cowen, P.J.; Dickens, C.; Ferrier, I.N.; Geddes, J.; Gilbody, S.; Haddad, P.M.; Katona, C.; Lewis, G.; Malizia, A.; McAllister-Williams, R.H.; Ramchandani, P.; Scott, J.; Taylor, D.; Uher, R.; Members of the Consensus Meeting. Evidence-based guidelines for treating depressive disorders with antidepressants: A revision of the 2008 British Association for Psychopharmacology guidelines. J. Psychopharmacol. 2015, 29, 459–525. [Google Scholar] [CrossRef] [PubMed]
- Nagler, E.V.; Webster, A.C.; Vanholder, R.; Zoccali, C. Antidepressants for depression in stage 3-5 chronic kidney disease: A systematic review of pharmacokinetics, efficacy and safety with recommendations by European Renal Best Practice (ERBP). Nephrol. Dial. Transplant. 2012, 27, 3736–3745. [Google Scholar] [CrossRef] [PubMed]
- King-Wing Ma, T.; Kam-Tao Li, P. Depression in dialysis patients. Nephrology 2016, 21, 639–646. [Google Scholar] [PubMed]
- Suh, M.R.; Jung, H.H.; Kim, S.B.; Park, J.S.; Yang, W.S. Effects of regular exercise on anxiety, depression, and quality of life in maintenance hemodialysis patients. Ren. Fail. 2002, 24, 337–345. [Google Scholar] [PubMed]
- Levendoglu, F.; Altintepe, L.; Okudan, N.; Ugurlu, H.; Gokbel, H.; Tonbul, Z.; Guney, I.; Turk, S. A twelve week exercise program improves the psychological status, quality of life and work capacity in hemodialysis patients. J. Nephrol. 2004, 17, 826–832. [Google Scholar]
- Kouidi, E.; Karagiannis, V.; Grekas, D.; Iakovides, A.; Kaprinis, G.; Tourkantonis, A.; Deligiannis, A. Depression, heart rate variability, and exercise training in dialysis patients. Eur. J. Cardiovasc. Prev. Rehabil. 2010, 17, 160–167. [Google Scholar] [CrossRef]
- Carney, R.M.; Templeton, B.; Hong, B.A.; Harter, H.R.; Hagberg, J.M.; Schechtman, K.B.; Goldberg, A.P. Exercise training reduces depression and increases the performance of pleasant activities in hemodialysis patients. Nephron 1987, 47, 194–198. [Google Scholar] [CrossRef]
- Rezaei, J.; Abdi, A.; Rezaei, M.; Heydarnezhadian, J.; Jalali, R. Effect of Regular Exercise Program on Depression in Hemodialysis Patients. Int. Sch. Res. Not. 2015, 2015, 182030. [Google Scholar] [CrossRef]
- Santhi, A.; Samson, R.; Pethuru, D. Effectiveness of physical activity on depression, anxiety, stress and quality of life of patients on hemodialysis. Biomed. Res. 2018, 29. [Google Scholar] [CrossRef]
- Pu, J.; Jiang, Z.; Wu, W.H.; li, L.; Zhang, L.L.; Li, Y.; Liu, Q.; Ou, S.T. Efficacy and safety of intradialytic exercise in haemodialysis patients: A systematic review and meta-analysis. BMJ Open 2019, 9, e020633. [Google Scholar] [CrossRef] [PubMed]
- Kosmadakis, G.C.; Bevington, A.; Smith, A.C.; Clapp, E.L.; Viana, J.L.; Bishop, N.C.; Feehally, J. Physical exercise in patients with severe kidney disease. Nephron. Clin. Pract. 2010, 115, c7–c16. [Google Scholar] [CrossRef] [PubMed]
- Jang, E.J.; Kim, H.S. Effects of exercise intervention on physical fitness and health-relalted quality of life in hemodialysis patients. J. Korean Acad. Nurs. 2009, 39, 584–593. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.; Ibrahim, R.; Hamad, A.; Talal, T.; Al-Ali, F.; Najafi, B. Exergame: A Gamelike Exercise to Improve Motor Functions and Physical Activities in Diabetic Patients Undergoing Hemodialysis. In Proceedings of the Qatar Foundation Annual Research Conference, Doha, Qatar, 19–20 March 2018; Hamad bin Khalifa University Press (HBKU Press): Doha, Qatar, 2018; Volume 2018. [Google Scholar] [CrossRef]
- Zhou, H.; Ibrahim, R.; Hamad, A.; Talal, T.; Al-Ali, F.; Najafi, B. GameBased NonWeight Bearing Exercise to Improve Postural Balance in Diabetic Patients Underjoining Hemodialysis. In Proceedings of the Qatar Foundation Annual Research Conference, Doha, Qatar, 19–20 March 2018; Hamad bin Khalifa University Press (HBKU Press): Doha, Qatar, 2018; Volume 2018. [Google Scholar] [CrossRef]
- Wang, C.; Wang, Q.; Shi, S. A distributed wireless body area network for medical supervision. In Proceedings of the 2012 IEEE International Instrumentation and Measurement Technology Conference, Graz, Austria, 13–16 May 2012; IEEE: New York, NY, USA, 2012; pp. 2612–2616. [Google Scholar]
- Folstein, M.F.; Robins, L.N.; Helzer, J.E. The Mini-Mental State Examination. Arch. Gen. Psychiatry 1983, 40, 812. [Google Scholar] [CrossRef]
- Delbaere, K.; Close, J.C.; Mikolaizak, A.S.; Sachdev, P.S.; Brodaty, H.; Lord, S.R. The Falls Efficacy Scale International (FES-I). A comprehensive longitudinal validation study. Age Ageing 2010, 39, 210–216. [Google Scholar] [CrossRef]
- Bracewell, N.; Game, F.; Jeffcoate, W.; Scammell, B.E. Clinical evaluation of a new device in the assessment of peripheral sensory neuropathy in diabetes. Diabet. Med. 2012, 29, 1553–1555. [Google Scholar] [CrossRef]
- Wyatt, M.F.; Stickrath, C.; Shah, A.; Smart, A.; Hunt, J.; Casserly, I.P. Ankle-brachial index performance among internal medicine residents. Vasc. Med. 2010, 15, 99–105. [Google Scholar] [CrossRef]
- Rohlfing, C.L.; Little, R.R.; Wiedmeyer, H.M.; England, J.D.; Madsen, R.; Harris, M.I.; Flegal, K.M.; Eberhardt, M.S.; Goldstein, D.E. Use of GHb (HbA1c) in screening for undiagnosed diabetes in the U.S. population. Diabetes Care 2000, 23, 187–191. [Google Scholar] [CrossRef]
- Weissman, M.M.; Sholomskas, D.; Pottenger, M.; Prusoff, B.A.; Locke, B.Z. Assessing depressive symptoms in five psychiatric populations: A validation study. Am. J. Epidemiol. 1977, 106, 203–214. [Google Scholar] [CrossRef]
- Grewal, G.; Sayeed, R.; Yeschek, S.; Menzies, R.A.; Talal, T.K.; Lavery, L.A.; Armstrong, D.G.; Najafi, B. Virtualizing the assessment: A novel pragmatic paradigm to evaluate lower extremity joint perception in diabetes. Gerontology 2012, 58, 463–471. [Google Scholar] [CrossRef]
- Najafi, B.; Lee-Eng, J.; Wrobel, J.S.; Goebel, R. Estimation of Center of Mass Trajectory using Wearable Sensors during Golf Swing. J. Sports Sci. Med. 2015, 14, 354–363. [Google Scholar] [PubMed]
- Najafi, B.; Horn, D.; Marclay, S.; Crews, R.T.; Wu, S.; Wrobel, J.S. Assessing postural control and postural control strategy in diabetes patients using innovative and wearable technology. J. Diabetes Sci. Technol. 2010, 4, 780–791. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.; Razjouyan, J.; Halder, D.; Naik, A.D.; Kunik, M.E.; Najafi, B. Instrumented Trail-Making Task: Application of Wearable Sensor to Determine Physical Frailty Phenotypes. Gerontology 2019, 65, 186–197. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.; Lee, H.; Lee, J.; Schwenk, M.; Najafi, B. Motor Planning Error: Toward Measuring Cognitive Frailty in Older Adults Using Wearables. Sensors 2018, 18, 926. [Google Scholar] [CrossRef]
- Zhou, H.; Sabbagh, M.; Wyman, R.; Liebsack, C.; Kunik, M.E.; Najafi, B. Instrumented Trail-Making Task to Differentiate Persons with No Cognitive Impairment, Amnestic Mild Cognitive Impairment, and Alzheimer Disease: A Proof of Concept Study. Gerontology 2017, 63, 189–200. [Google Scholar] [CrossRef]
- Schwenk, M.; Dutzi, I.; Englert, S.; Micol, W.; Najafi, B.; Mohler, J.; Hauer, K. An intensive exercise program improves motor performances in patients with dementia: Translational model of geriatric rehabilitation. J. Alzheimers Dis. 2014, 39, 487–498. [Google Scholar] [CrossRef]
- Cohen, J. Statistical power analysis for the behavioral sciences. Technometrics 1988, 31, 499–500. [Google Scholar]
- Rosenthal, J.A. Qualitative descriptors of strength of association and effect size. J. Soc. Serv. Res. 1996, 21, 37–59. [Google Scholar] [CrossRef]
- Smart, N.; Steele, M. Exercise training in haemodialysis patients: A systematic review and meta-analysis. Nephrology 2011, 16, 626–632. [Google Scholar]
- Zhou, H.; Al-Ali, F.; Rahemi, H.; Kulkarni, N.; Hamad, A.; Ibrahim, R.; Talal, T.K.; Najafi, B. Hemodialysis Impact on Motor Function beyond Aging and Diabetes-Objectively Assessing Gait and Balance by Wearable Technology. Sensors 2018, 18, 3939. [Google Scholar] [CrossRef]
- Rosenberg, D.; Depp, C.A.; Vahia, I.V.; Reichstadt, J.; Palmer, B.W.; Kerr, J.; Norman, G.; Jeste, D.V. Exergames for subsyndromal depression in older adults: A pilot study of a novel intervention. Am. J. Geriatr. Psychiatry 2010, 18, 221–226. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Exergame Group (EG, n = 37) | Supervised Exercise Group (SG, n = 36) | p-Value | |
|---|---|---|---|
| Demographics | |||
| Age, years | 62.7 ± 6.8 | 66.5 ± 10.0 | 0.060 |
| Sex (female), n (%) | 18 (49%) | 22 (61%) | 0.285 |
| Height, m | 157.1 ± 25.4 | 157.5 ± 10.2 | 0.932 |
| Weight, kg | 77.8 ± 17.2 | 82.4 ± 22.9 | 0.328 |
| BMI, kg/m2 | 30.0 ± 6.3 | 33.2 ± 8.4 | 0.068 |
| Clinical data | |||
| At risk for clinical depression (CES-D ≥ 16), n (%) | 11 (30%) | 16 (44%) | 0.193 |
| Duration of hemodialysis, years | 4.8 ± 5.0 | 4.0 ± 3.8 | 0.487 |
| Had fall in last 12-month, n (%) | 8 (22%) | 9 (25%) | 0.733 |
| MMSE, units on a scale | 27.5 ± 2.8 | 25.4 ± 4.9 | 0.052 |
| Concern for fall (FES-I score), units on a scale | 12.7 ± 5.2 | 14.7 ± 6.3 | 0.134 |
| High concern about falling (FES-I ≥ 11), n (%) | 19 (51%) | 24 (67%) | 0.184 |
| Number of prescription medications, n | 8 ± 3 | 7 ± 3 | 0.835 |
| Plantar sensation (VPT), Volt | 33.2 ± 17.1 | 33.7 ± 15.9 | 0.885 |
| Diabetic peripheral neuropathy (VPT ≥ 25), n (%) | 22 (60%) | 23 (64%) | 0.697 |
| Peripheral artery disease (ABI < 0.8 or ABI > 1.2), n (%) | 20 (54%) | 25 (69%) | 0.176 |
| HbA1c, % | 6.6 ± 1.6 | 6.9 ± 1.6 | 0.378 |
| Question | Mean | Standard Deviation | Median | Range |
|---|---|---|---|---|
| 1: It was fun to use the sensor-based exercise technology | 3.22 | 0.19 | 4 | 0–4 |
| 2: Usage of the technology was possible without problems at any time | 3.56 | 0.13 | 4 | 1–4 |
| 3: The form and design of the technology are optimal for me | 3.50 | 0.13 | 4 | 2–4 |
| 4: I feel more energetic at home after doing exercise | 3.03 | 0.20 | 4 | 1–4 |
| 5: Thanks to the sensor feedback, I could quickly learn all exercises | 3.67 | 0.10 | 4 | 2–4 |
| 6: I feel that the exercises were going too fast and exhausting me | 0.25 | 0.12 | 0 | 0–3 |
| 7: Some of the movements were difficult to perform | 0.86 | 0.19 | 0 | 0–3 |
| 8: I felt safe using the exercise technology | 3.75 | 0.07 | 4 | 3–4 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, H.; Al-Ali, F.; Kang, G.E.; Hamad, A.I.; Ibrahim, R.A.; Talal, T.K.; Najafi, B. Application of Wearables to Facilitate Virtually Supervised Intradialytic Exercise for Reducing Depression Symptoms. Sensors 2020, 20, 1571. https://doi.org/10.3390/s20061571
Zhou H, Al-Ali F, Kang GE, Hamad AI, Ibrahim RA, Talal TK, Najafi B. Application of Wearables to Facilitate Virtually Supervised Intradialytic Exercise for Reducing Depression Symptoms. Sensors. 2020; 20(6):1571. https://doi.org/10.3390/s20061571
Chicago/Turabian StyleZhou, He, Fadwa Al-Ali, Gu Eon Kang, Abdullah I. Hamad, Rania A. Ibrahim, Talal K. Talal, and Bijan Najafi. 2020. "Application of Wearables to Facilitate Virtually Supervised Intradialytic Exercise for Reducing Depression Symptoms" Sensors 20, no. 6: 1571. https://doi.org/10.3390/s20061571
APA StyleZhou, H., Al-Ali, F., Kang, G. E., Hamad, A. I., Ibrahim, R. A., Talal, T. K., & Najafi, B. (2020). Application of Wearables to Facilitate Virtually Supervised Intradialytic Exercise for Reducing Depression Symptoms. Sensors, 20(6), 1571. https://doi.org/10.3390/s20061571