Agreement between Inertia and Optical Based Motion Capture during the VU-Return-to-Play- Field-Test


Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
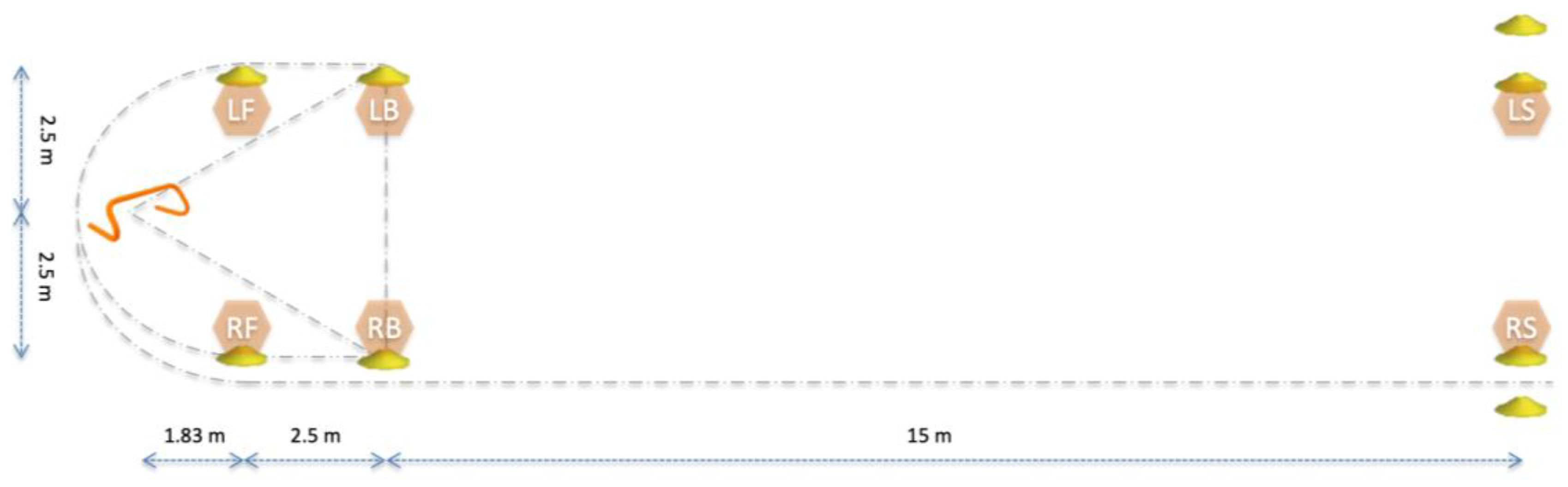
2.2. Field Test
2.3. Data Capture
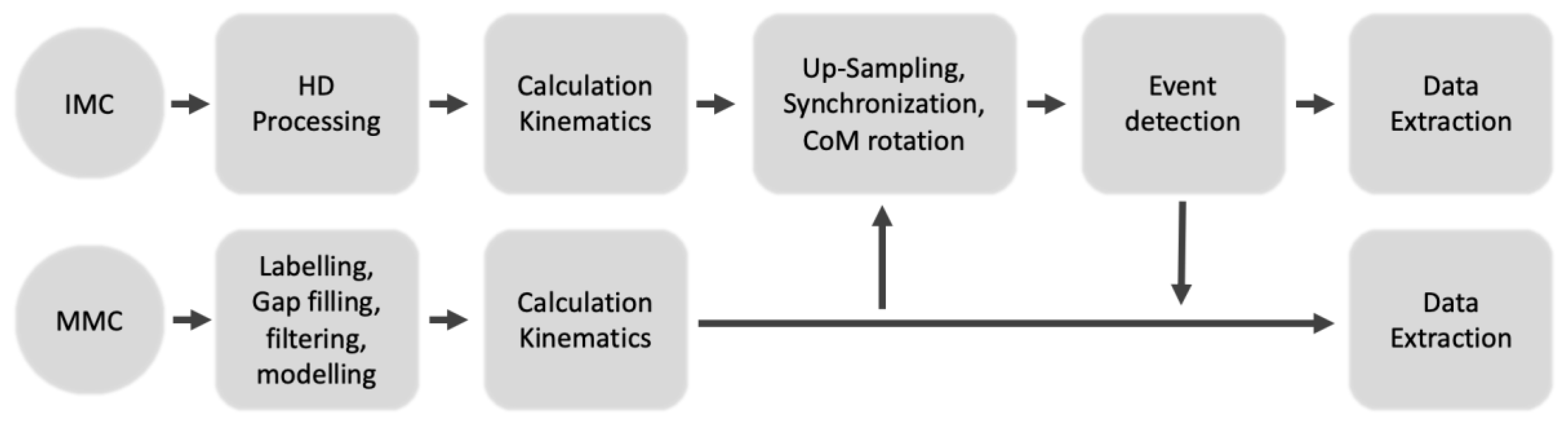
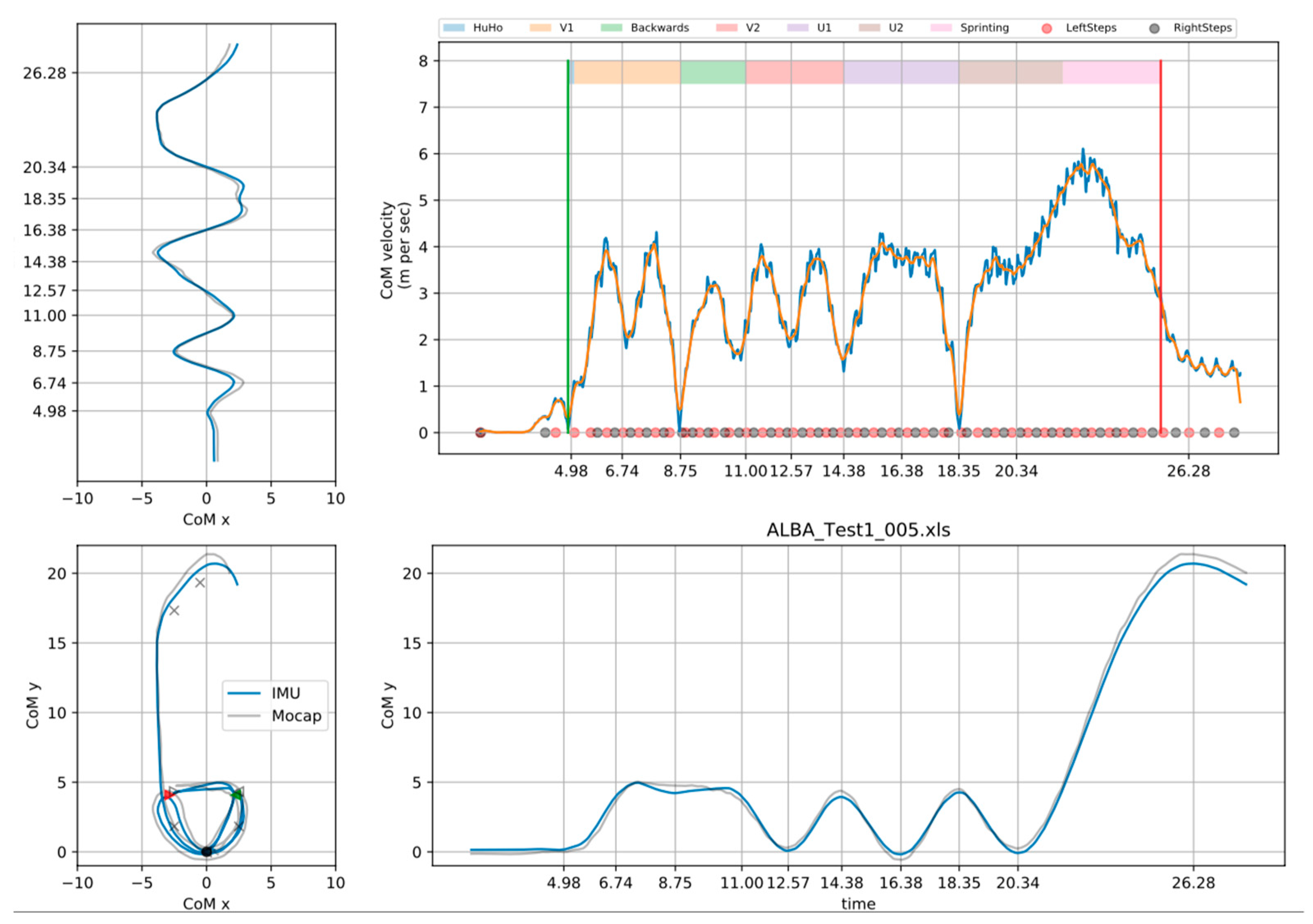
2.4. Data Preparation
2.5. Statistical Analysis
3. Results
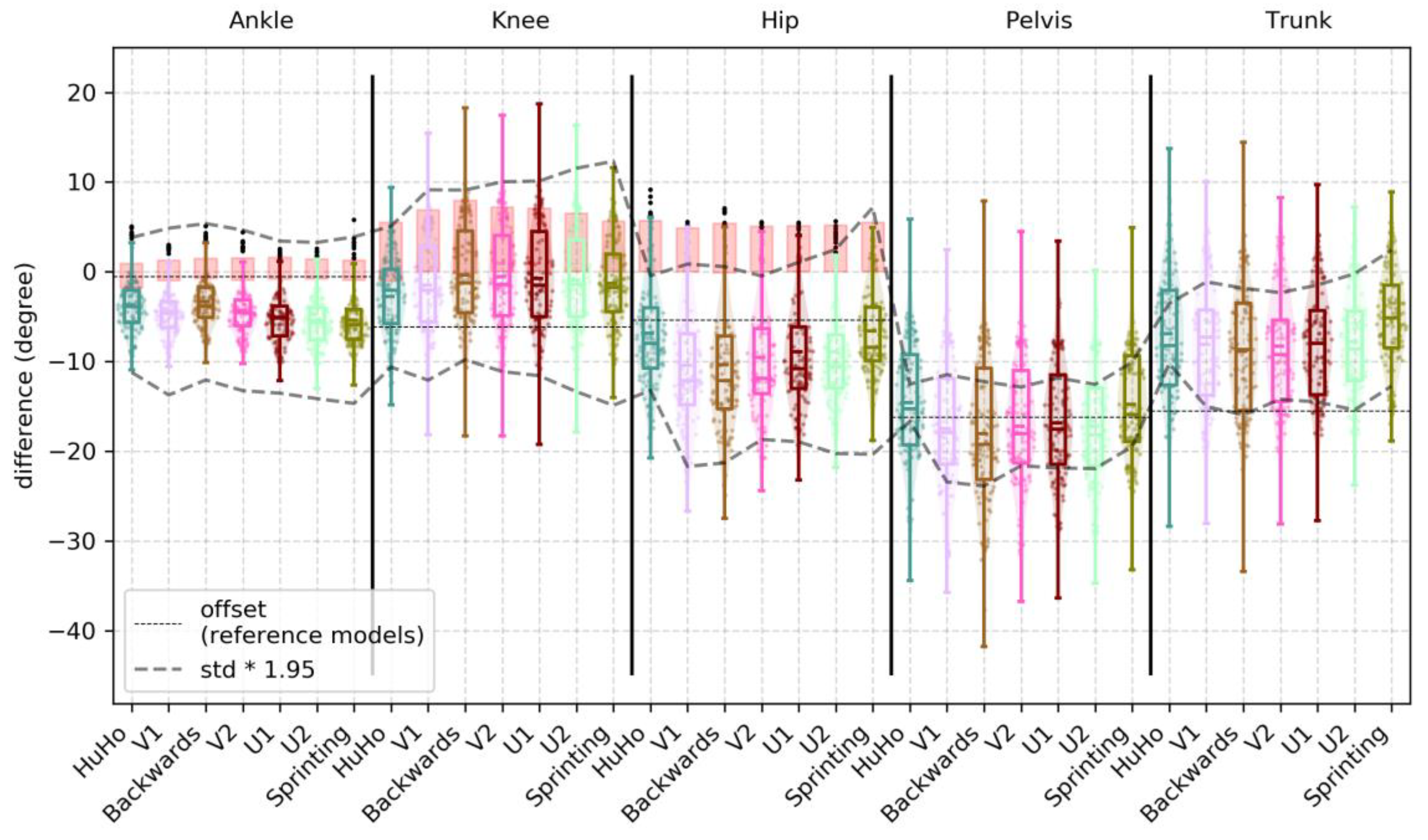
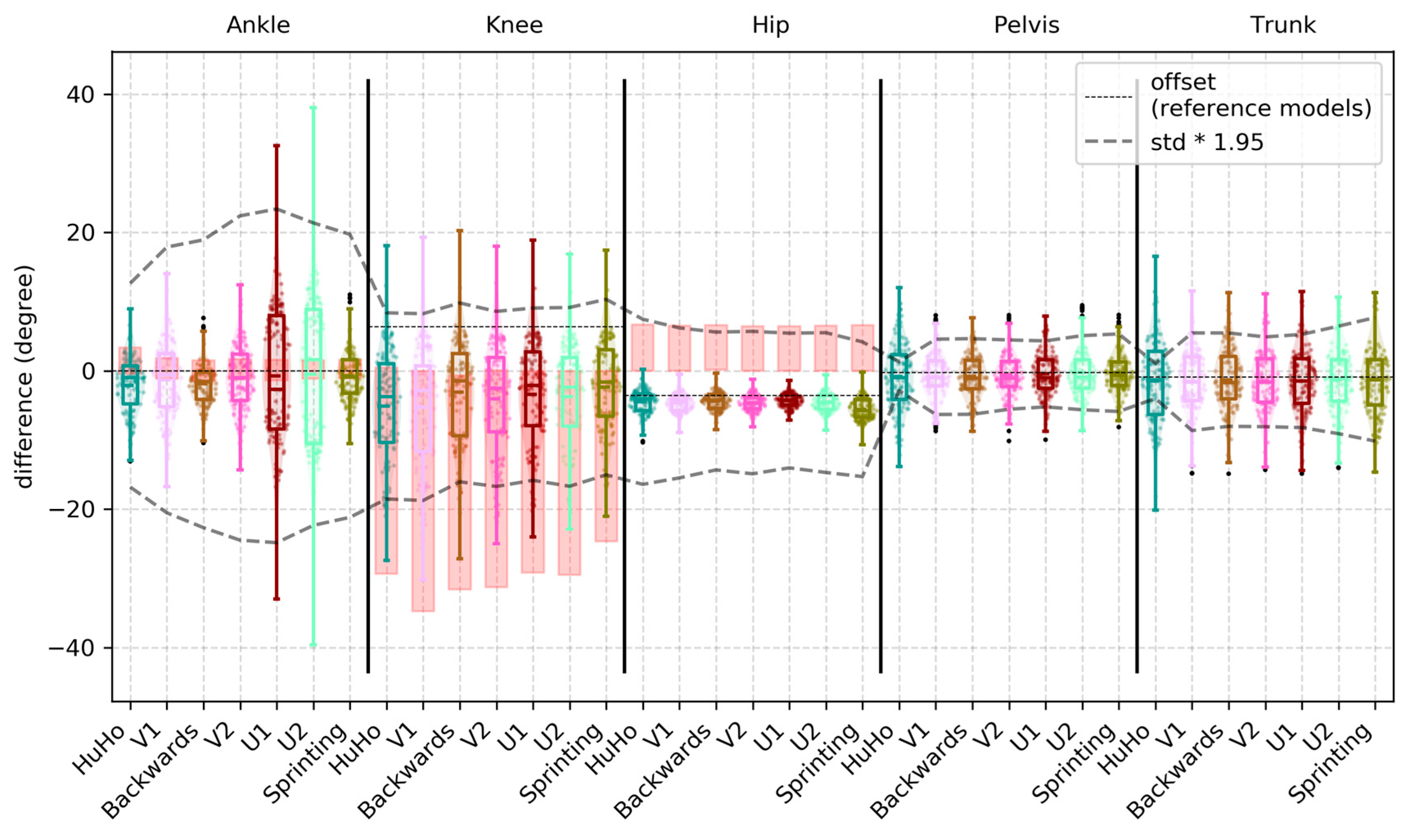
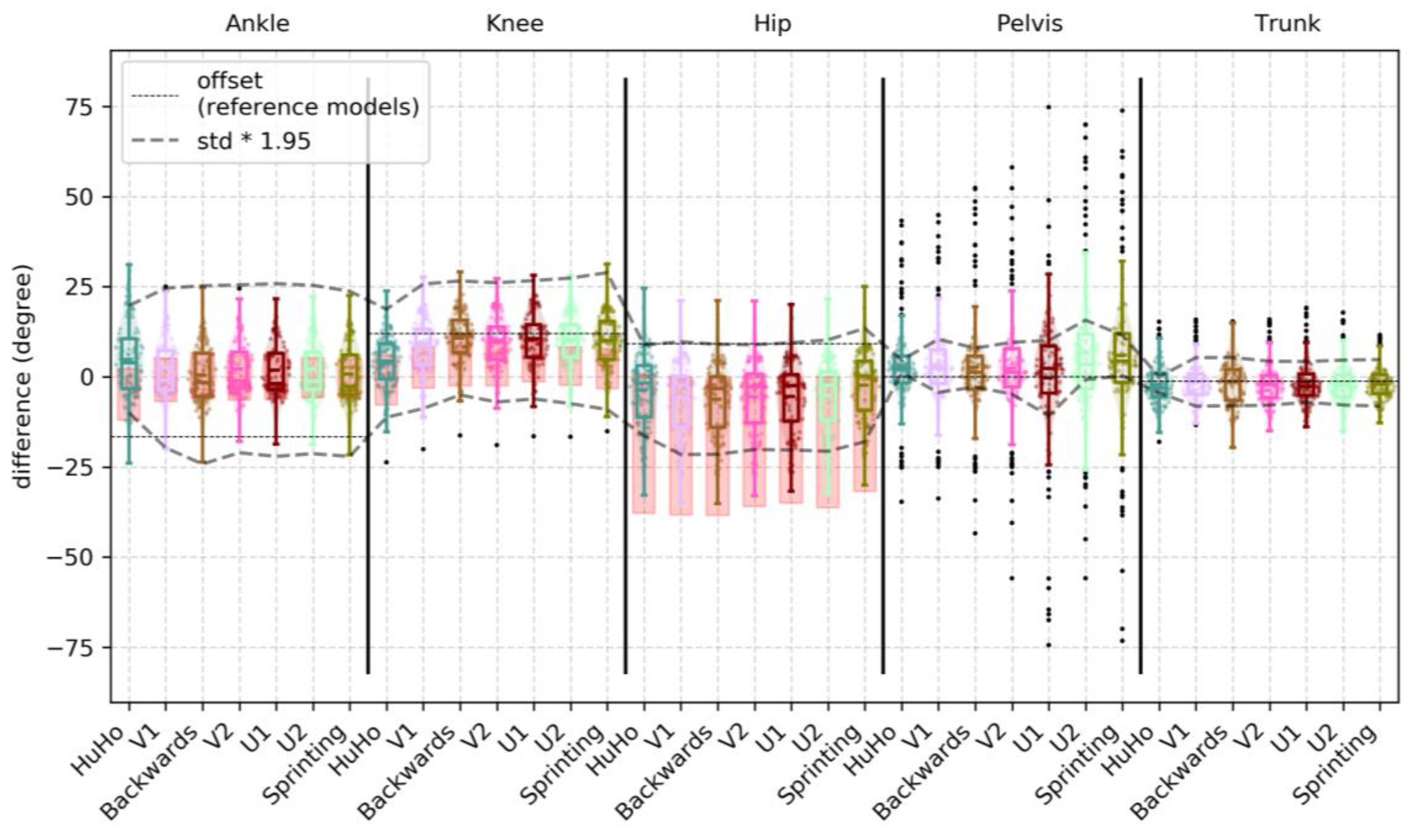
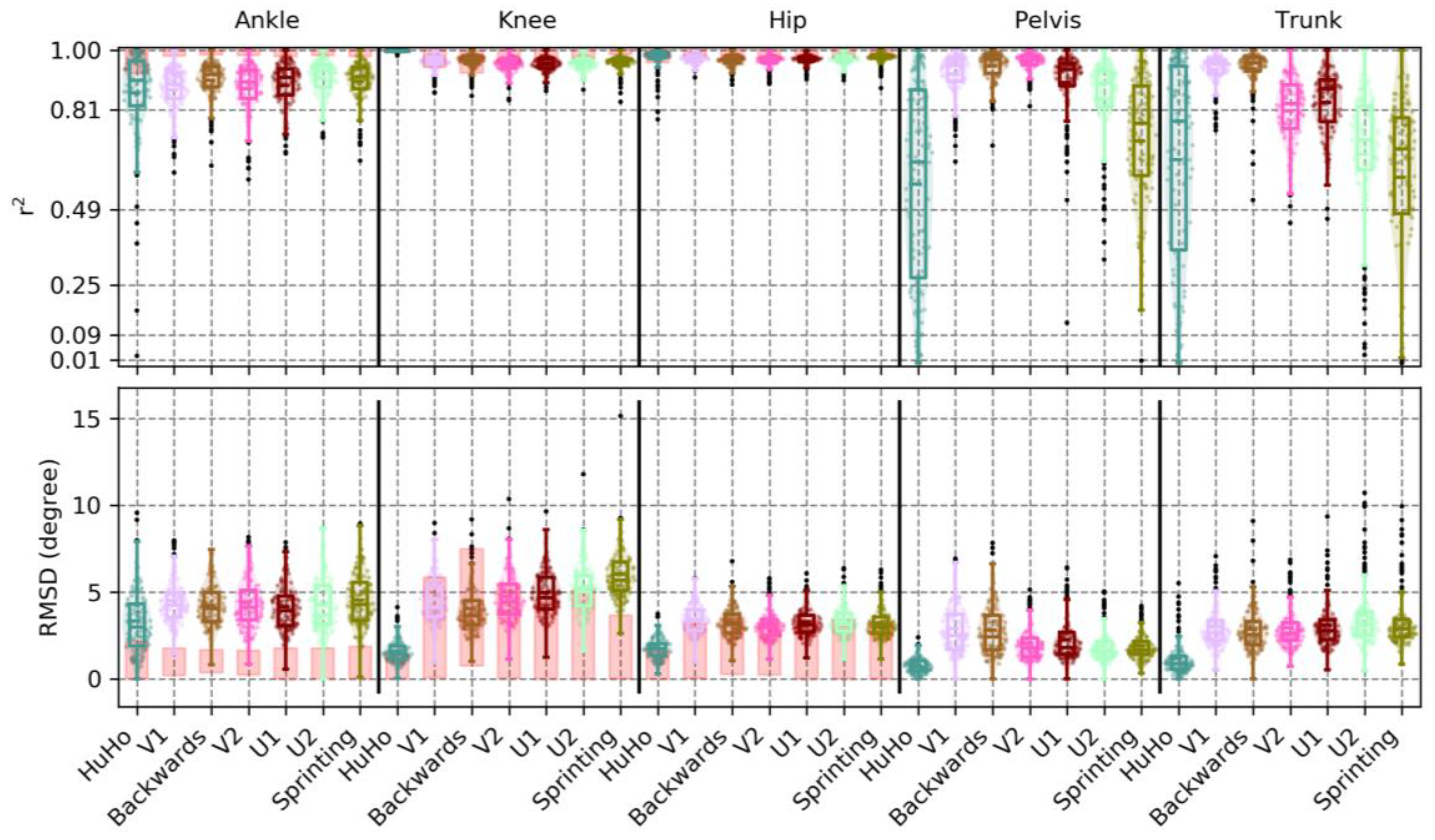
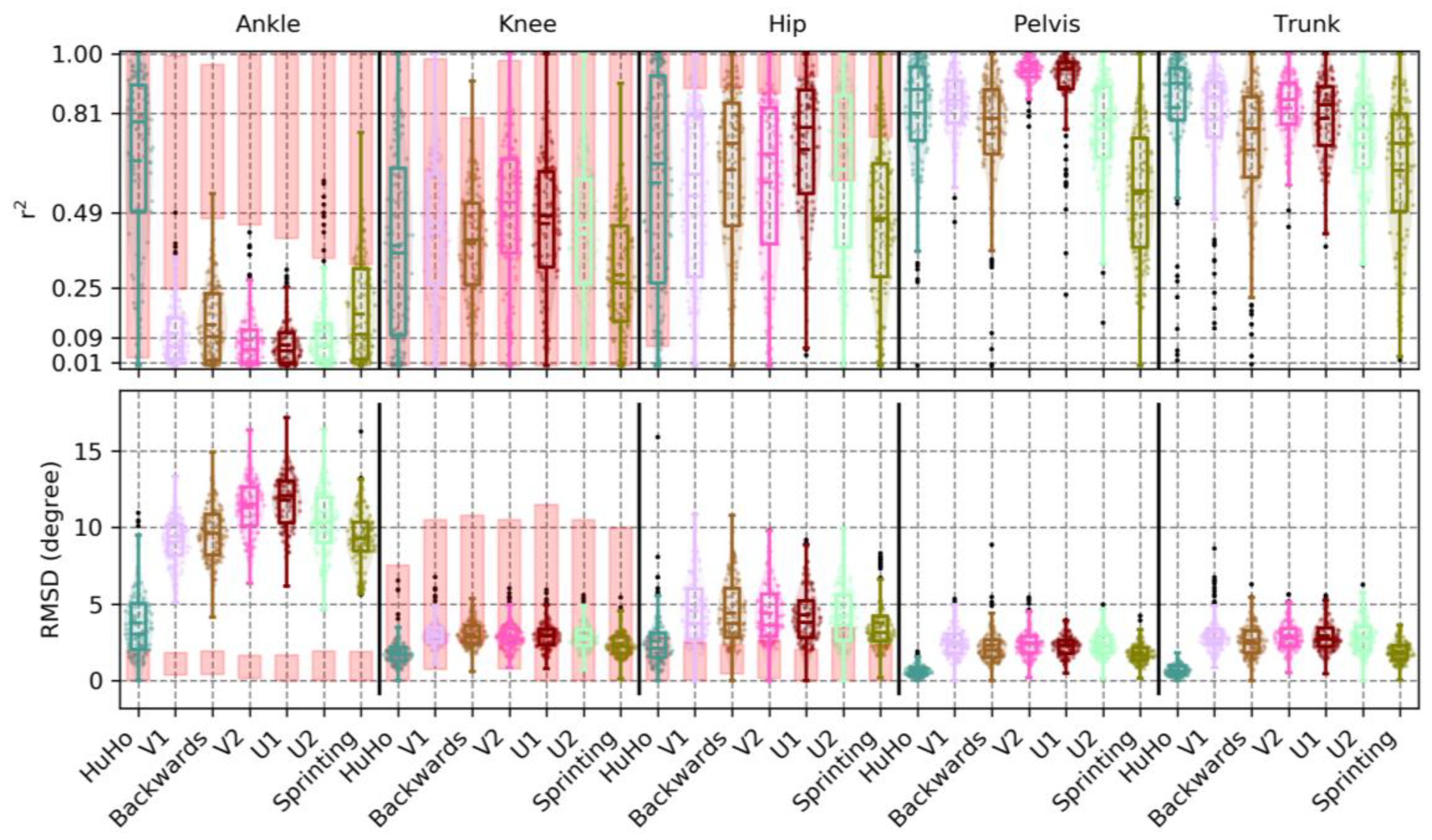
3.1. Accuracy
3.2. Precision
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Plane | Phase | Measure | R (±std) | RMSD (±std) | RMSD% (±std) | Bias (±std) | 95% Limit |
|---|---|---|---|---|---|---|---|
| sagittal | HuHo | Ankle | 0.87 (0.16) | 3.11 (1.84) | 0.08 (0.06) | −3.37 (3.33) | −10.62 to 3.88 |
| V1 | Ankle | 0.88 (0.08) | 4.45 (1.32) | 0.07 (0.02) | −4.43 (2.84) | −13.66 to 4.79 | |
| Backw. | Ankle | 0.90 (0.06) | 4.24 (1.22) | 0.06 (0.02) | −3.58 (2.91) | −12.41 to 5.25 | |
| V2 | Ankle | 0.88 (0.09) | 4.31 (1.50) | 0.07 (0.02) | −4.42 (2.86) | −13.19 to 4.35 | |
| U1 | Ankle | 0.89 (0.07) | 4.10 (1.31) | 0.07 (0.02) | −5.23 (3.02) | −13.59 to 3.12 | |
| U2 | Ankle | 0.91 (0.06) | 4.16 (1.50) | 0.06 (0.02) | −5.58 (2.97) | −14.17 to 3.02 | |
| Sprint | Ankle | 0.90 (0.08) | 4.51 (1.55) | 0.07 (0.02) | −5.44 (2.92) | −14.76 to 3.88 | |
| HuHo | Knee | 1.00 (0.00) | 1.71 (0.70) | 0.02 (0.01) | −4.99 (4.38) | −12.73 to 2.76 | |
| V1 | Knee | 0.96 (0.02) | 4.53 (1.09) | 0.04 (0.01) | −4.37 (4.07) | −14.22 to 5.49 | |
| Backw. | Knee | 0.97 (0.03) | 3.87 (1.24) | 0.04 (0.01) | −3.50 (4.31) | −12.18 to 5.18 | |
| V2 | Knee | 0.96 (0.03) | 4.64 (1.26) | 0.05 (0.01) | −3.70 (4.31) | −13.64 to 6.24 | |
| U1 | Knee | 0.95 (0.03) | 4.96 (1.24) | 0.05 (0.01) | −3.94 (4.46) | −14.34 to 6.47 | |
| U2 | Knee | 0.96 (0.02) | 5.25 (1.50) | 0.05 (0.01) | −4.03 (4.49) | −15.73 to 7.68 | |
| Sprint | Knee | 0.96 (0.03) | 6.13 (1.70) | 0.06 (0.01) | −4.23 (4.08) | −17.28 to 8.83 | |
| HuHo | Hip | 0.97 (0.05) | 1.77 (0.69) | 0.05 (0.03) | −10.25 (6.35) | −17.76 to −2.74 | |
| V1 | Hip | 0.97 (0.02) | 3.58 (0.92) | 0.04 (0.01) | −13.55 (7.06) | −24.63 to −2.48 | |
| Backw. | Hip | 0.96 (0.03) | 3.44 (1.03) | 0.04 (0.01) | −13.49 (7.53) | −24.15 to −2.82 | |
| V2 | Hip | 0.96 (0.03) | 3.31 (1.01) | 0.04 (0.01) | −12.86 (6.58) | −22.24 to −3.47 | |
| U1 | Hip | 0.96 (0.02) | 3.45 (0.97) | 0.04 (0.01) | −12.25 (6.27) | −22.46 to −2.04 | |
| U2 | Hip | 0.97 (0.02) | 3.51 (1.01) | 0.05 (0.01) | −12.22 (6.04) | −23.76 to −0.68 | |
| Sprint | Hip | 0.97 (0.02) | 3.41 (1.02) | 0.05 (0.01) | −10.11 (4.69) | −24.02 to 3.79 | |
| HuHo | Pelvis | 0.57 (0.32) | 0.80 (0.45) | 0.20 (0.08) | −14.60 (6.35) | −16.68 to −12.52 | |
| V1 | Pelvis | 0.92 (0.07) | 2.91 (1.45) | 0.07 (0.03) | −17.44 (7.20) | −23.42 to −11.46 | |
| Backw. | Pelvis | 0.95 (0.05) | 2.82 (1.50) | 0.07 (0.03) | −18.06 (7.52) | −23.88 to −12.24 | |
| V2 | Pelvis | 0.96 (0.03) | 2.07 (1.05) | 0.05 (0.02) | −17.23 (6.69) | −21.61 to −12.84 | |
| U1 | Pelvis | 0.90 (0.12) | 2.25 (1.26) | 0.07 (0.03) | −16.84 (6.31) | −21.87 to −11.82 | |
| U2 | Pelvis | 0.84 (0.14) | 1.89 (0.92) | 0.09 (0.04) | −17.24 (6.40) | −21.93 to −12.55 | |
| Sprint | Pelvis | 0.71 (0.20) | 1.90 (0.77) | 0.12 (0.04) | −14.78 (5.38) | −19.48 to −10.08 | |
| HuHo | Trunk | 0.65 (0.33) | 1.18 (1.01) | 0.16 (0.09) | −6.89 (6.69) | −10.24 to −3.54 | |
| V1 | Trunk | 0.94 (0.05) | 3.01 (1.23) | 0.06 (0.02) | −8.08 (6.96) | −15.04 to −1.12 | |
| Backw. | Trunk | 0.94 (0.07) | 2.85 (1.30) | 0.06 (0.03) | −8.87 (6.92) | −15.92 to −1.82 | |
| V2 | Trunk | 0.81 (0.11) | 2.95 (1.19) | 0.10 (0.03) | −8.27 (6.84) | −14.22 to −2.33 | |
| U1 | Trunk | 0.83 (0.11) | 3.12 (1.34) | 0.09 (0.03) | −7.99 (6.09) | −14.50 to −1.47 | |
| U2 | Trunk | 0.67 (0.20) | 3.70 (1.86) | 0.11 (0.03) | −7.81 (6.02) | −15.40 to −0.22 | |
| Sprint | Trunk | 0.59 (0.27) | 3.44 (1.72) | 0.15 (0.05) | −5.15 (5.52) | −12.73 to 2.43 |
| Plane | Phase | Measure | R (±std) | RMSD (±std) | RMSD% (±std) | Bias (±std) | 95% Limit |
|---|---|---|---|---|---|---|---|
| fontal | HuHo | Ankle | 0.69 (0.29) | 3.45 (2.20) | 0.18 (0.09) | −2.98 (4.36) | −18.07 to 12.12 |
| V1 | Ankle | 0.09 (0.11) | 9.13 (1.58) | 0.19 (0.02) | −1.64 (5.41) | −21.11 to 17.84 | |
| Backw. | Ankle | 0.14 (0.12) | 9.60 (1.66) | 0.20 (0.02) | −1.81 (3.26) | −22.68 to 19.07 | |
| V2 | Ankle | 0.08 (0.09) | 11.37 (1.75) | 0.20 (0.01) | −1.22 (4.81) | −24.85 to 22.42 | |
| U1 | Ankle | 0.07 (0.06) | 11.78 (1.66) | 0.20 (0.01) | −0.79 (9.11) | −25.05 to 23.47 | |
| U2 | Ankle | 0.11 (0.12) | 10.38 (1.99) | 0.21 (0.02) | −0.56 (9.86) | −22.61 to 21.49 | |
| Sprint | Ankle | 0.15 (0.14) | 9.43 (1.99) | 0.22 (0.03) | −0.88 (3.88) | −21.52 to 19.76 | |
| HuHo | Knee | 0.39 (0.31) | 1.86 (0.87) | 0.21 (0.06) | 6.95 (5.46) | −4.34 to 18.23 | |
| V1 | Knee | 0.11 (0.14) | 3.94 (0.96) | 0.17 (0.02) | 9.79 (3.65) | −2.30 to 21.88 | |
| Backw. | Knee | 0.11 (0.13) | 3.73 (0.92) | 0.17 (0.02) | 10.64 (3.23) | −0.73 to 22.01 | |
| V2 | Knee | 0.10 (0.13) | 3.95 (0.89) | 0.16 (0.02) | 9.91 (3.62) | −1.94 to 21.76 | |
| U1 | Knee | 0.10 (0.13) | 3.88 (0.90) | 0.16 (0.02) | 9.79 (3.52) | −1.98 to 21.56 | |
| U2 | Knee | 0.10 (0.14) | 3.65 (0.82) | 0.17 (0.03) | 9.63 (3.38) | −2.07 to 21.33 | |
| Sprint | Knee | 0.10 (0.12) | 2.73 (0.81) | 0.20 (0.03) | 9.10 (3.37) | −1.96 to 20.17 | |
| HuHo | Hip | 0.62 (0.33) | 2.43 (1.80) | 0.16 (0.09) | −8.34 (2.29) | −19.31 to 2.63 | |
| V1 | Hip | 0.59 (0.26) | 4.31 (2.11) | 0.13 (0.05) | −8.63 (1.96) | −18.22 to 0.96 | |
| Backw. | Hip | 0.68 (0.24) | 4.04 (1.93) | 0.12 (0.05) | −8.34 (2.03) | −17.04 to 0.36 | |
| V2 | Hip | 0.64 (0.25) | 4.11 (1.91) | 0.12 (0.05) | −8.49 (1.87) | −17.53 to 0.55 | |
| U1 | Hip | 0.74 (0.21) | 3.93 (1.80) | 0.10 (0.04) | −8.15 (1.80) | −16.72 to 0.42 | |
| U2 | Hip | 0.68 (0.25) | 3.96 (1.89) | 0.11 (0.04) | −8.38 (1.92) | −17.32 to 0.55 | |
| Sprint | Hip | 0.52 (0.25) | 3.56 (1.77) | 0.15 (0.05) | −9.23 (2.01) | −18.00 to −0.46 | |
| HuHo | Pelvis | 0.81 (0.20) | 0.65 (0.39) | 0.12 (0.07) | −0.79 (4.84) | −2.88 to 1.29 | |
| V1 | Pelvis | 0.84 (0.10) | 2.56 (1.00) | 0.10 (0.03) | −0.88 (3.79) | −6.32 to 4.56 | |
| Backw. | Pelvis | 0.74 (0.21) | 2.28 (1.11) | 0.11 (0.05) | −0.83 (3.09) | −6.29 to 4.64 | |
| V2 | Pelvis | 0.94 (0.04) | 2.48 (0.93) | 0.06 (0.02) | −0.56 (3.40) | −5.57 to 4.45 | |
| U1 | Pelvis | 0.89 (0.14) | 2.29 (0.68) | 0.07 (0.03) | −0.45 (3.22) | −5.22 to 4.31 | |
| U2 | Pelvis | 0.76 (0.16) | 2.42 (0.81) | 0.10 (0.03) | −0.28 (3.63) | −5.64 to 5.07 | |
| Sprint | Pelvis | 0.55 (0.20) | 1.80 (0.63) | 0.15 (0.04) | −0.28 (3.11) | −5.89 to 5.32 | |
| HuHo | Trunk | 0.83 (0.21) | 0.66 (0.35) | 0.11 (0.06) | −1.48 (5.67) | −4.01 to 1.05 | |
| V1 | Trunk | 0.79 (0.19) | 3.13 (1.30) | 0.10 (0.04) | −1.59 (4.63) | −8.64 to 5.46 | |
| Backw. | Trunk | 0.69 (0.23) | 2.61 (1.08) | 0.13 (0.05) | −1.28 (4.79) | −8.03 to 5.46 | |
| V2 | Trunk | 0.83 (0.10) | 2.93 (0.93) | 0.10 (0.03) | −1.60 (4.70) | −8.08 to 4.89 | |
| U1 | Trunk | 0.79 (0.13) | 2.94 (1.02) | 0.10 (0.03) | −1.48 (4.71) | −8.22 to 5.25 | |
| U2 | Trunk | 0.71 (0.16) | 2.88 (1.08) | 0.12 (0.04) | −1.32 (4.96) | −9.09 to 6.44 | |
| Sprint | Trunk | 0.63 (0.24) | 1.90 (0.69) | 0.14 (0.04) | −1.24 (4.96) | −10.17 to 7.68 |
| Plane | Phase | Measure | R (±std) | RMSD (±std) | RMSD% (±std) | Bias (±std) | 95% Limit |
|---|---|---|---|---|---|---|---|
| transversal | HuHo | Ankle | 0.48 (0.31) | 2.67 (1.88) | 0.21 (0.08) | 9.04 (12.08) | −11.76 to 29.85 |
| V1 | Ankle | 0.05 (0.08) | 6.26 (1.39) | 0.19 (0.03) | 4.03 (9.49) | −22.62 to 30.67 | |
| Backw. | Ankle | 0.05 (0.07) | 7.41 (1.42) | 0.20 (0.02) | 0.26 (9.27) | −27.73 to 28.24 | |
| V2 | Ankle | 0.06 (0.09) | 6.68 (1.46) | 0.19 (0.03) | 3.08 (9.34) | −23.83 to 30.00 | |
| U1 | Ankle | 0.09 (0.11) | 6.98 (1.49) | 0.20 (0.03) | 2.19 (8.85) | −25.42 to 29.80 | |
| U2 | Ankle | 0.08 (0.10) | 6.72 (1.53) | 0.20 (0.03) | 2.44 (9.10) | −25.07 to 29.95 | |
| Sprint | Ankle | 0.04 (0.06) | 5.93 (1.72) | 0.20 (0.03) | 1.55 (9.22) | −26.62 to 29.73 | |
| HuHo | Knee | 0.48 (0.33) | 1.83 (0.77) | 0.20 (0.08) | 3.87 (8.22) | −10.04 to 17.78 | |
| V1 | Knee | 0.15 (0.09) | 3.05 (0.45) | 0.15 (0.02) | 5.64 (8.21) | −13.43 to 24.70 | |
| Backw. | Knee | 0.19 (0.13) | 3.20 (0.48) | 0.16 (0.02) | 6.88 (7.58) | −11.53 to 25.29 | |
| V2 | Knee | 0.14 (0.09) | 3.27 (0.42) | 0.15 (0.02) | 6.23 (8.01) | −12.74 to 25.20 | |
| U1 | Knee | 0.14 (0.09) | 3.60 (0.62) | 0.15 (0.02) | 6.86 (7.75) | −11.76 to 25.47 | |
| U2 | Knee | 0.16 (0.10) | 3.58 (0.72) | 0.17 (0.02) | 6.93 (7.61) | −11.13 to 24.99 | |
| Sprint | Knee | 0.16 (0.09) | 3.72 (0.84) | 0.19 (0.02) | 7.49 (7.50) | −10.94 to 25.93 | |
| HuHo | Hip | 0.52 (0.32) | 2.97 (1.75) | 0.22 (0.09) | 10.27 (6.45) | −10.20 to 30.74 | |
| V1 | Hip | 0.17 (0.15) | 5.51 (1.41) | 0.18 (0.02) | 10.17 (4.26) | −8.66 to 29.00 | |
| Backw. | Hip | 0.27 (0.23) | 5.34 (1.58) | 0.17 (0.04) | 9.00 (3.89) | −8.76 to 26.76 | |
| V2 | Hip | 0.22 (0.19) | 5.16 (1.34) | 0.17 (0.03) | 9.44 (4.17) | −8.86 to 27.73 | |
| U1 | Hip | 0.26 (0.22) | 5.09 (1.38) | 0.16 (0.03) | 9.15 (4.29) | −9.73 to 28.03 | |
| U2 | Hip | 0.18 (0.17) | 5.07 (1.29) | 0.18 (0.03) | 9.97 (4.42) | −9.08 to 29.02 | |
| Sprint | Hip | 0.14 (0.14) | 3.62 (0.96) | 0.19 (0.03) | 11.38 (4.64) | −7.44 to 30.19 | |
| HuHo | Pelvis | 0.69 (0.35) | 0.61 (0.36) | 0.14 (0.09) | 2.85 (13.26) | 1.04 to 4.65 | |
| V1 | Pelvis | 1.00 (0.01) | 3.09 (1.69) | 0.02 (0.01) | 3.03 (13.78) | −4.36 to 10.42 | |
| Backw. | Pelvis | 0.98 (0.03) | 2.20 (1.44) | 0.03 (0.02) | 2.58 (16.92) | −2.80 to 7.95 | |
| V2 | Pelvis | 0.99 (0.02) | 3.40 (2.45) | 0.02 (0.02) | 2.37 (17.04) | −4.84 to 9.57 | |
| U1 | Pelvis | 0.99 (0.02) | 4.63 (5.14) | 0.02 (0.02) | −0.37 (21.09) | −10.84 to 10.09 | |
| U2 | Pelvis | 1.00 (0.01) | 3.58 (3.29) | 0.01 (0.01) | 6.69 (21.71) | −0.80 to 15.72 | |
| Sprint | Pelvis | 0.81 (0.22) | 2.49 (1.98) | 0.10 (0.05) | 5.91 (23.46) | 0.27 to 11.54 | |
| HuHo | Trunk | 0.69 (0.28) | 0.83 (0.42) | 0.15 (0.08) | −2.22 (5.99) | −4.47 to 0.03 | |
| V1 | Trunk | 0.82 (0.11) | 2.92 (1.06) | 0.09 (0.03) | −1.41 (5.69) | −8.14 to 5.32 | |
| Backw. | Trunk | 0.88 (0.10) | 3.11 (1.12) | 0.08 (0.03) | −1.35 (6.30) | −8.04 to 5.35 | |
| V2 | Trunk | 0.88 (0.08) | 2.57 (1.04) | 0.08 (0.03) | −1.79 (6.00) | −7.89 to 4.31 | |
| U1 | Trunk | 0.90 (0.06) | 2.45 (0.89) | 0.08 (0.02) | −1.41 (6.32) | −7.06 to 4.24 | |
| U2 | Trunk | 0.92 (0.05) | 2.48 (0.92) | 0.07 (0.02) | −1.60 (6.05) | −7.82 to 4.62 | |
| Sprint | Trunk | 0.95 (0.03) | 2.17 (1.31) | 0.06 (0.02) | −1.67 (4.98) | −8.13 to 4.79 |
| Plane | Phase | Measure | R (±std) | RMSD (±std) | RMSD% (±std) | Bias (±std) | 95% Limit |
|---|---|---|---|---|---|---|---|
| HuHo | CoMx | 0.99 (0.02) | 0.00 (0.00) | 0.02 (0.02) | 0.01 (0.24) | −0.00 to 0.02 | |
| V1 | CoMx | 0.99 (0.01) | 0.08 (0.05) | 0.02 (0.01) | 0.03 (0.18) | −0.19 to 0.26 | |
| Backw. | CoMx | 1.00 (0.00) | 0.04 (0.02) | 0.01 (0.00) | 0.04 (0.22) | −0.11 to 0.18 | |
| V2 | CoMx | 1.00 (0.00) | 0.09 (0.05) | 0.02 (0.01) | −0.00 (0.13) | −0.28 to 0.28 | |
| U1 | CoMx | 1.00 (0.00) | 0.07 (0.04) | 0.01 (0.01) | 0.02 (0.12) | −0.32 to 0.35 | |
| U2 | CoMx | 1.00 (0.00) | 0.07 (0.04) | 0.01 (0.01) | 0.01 (0.16) | −0.27 to 0.29 | |
| Sprint | CoMx | 0.92 (0.15) | 0.02 (0.01) | 0.06 (0.05) | −0.01 (0.13) | −0.07 to 0.05 | |
| HuHo | CoMy | 0.71 (0.32) | 0.01 (0.01) | 0.14 (0.09) | 0.14 (0.14) | 0.12 to 0.16 | |
| V1 | CoMy | 1.00 (0.00) | 0.07 (0.03) | 0.02 (0.01) | 0.01 (0.12) | −0.28 to 0.30 | |
| Backw. | CoMy | 0.89 (0.18) | 0.04 (0.03) | 0.06 (0.05) | −0.10 (0.12) | −0.25 to 0.05 | |
| V2 | CoMy | 1.00 (0.01) | 0.09 (0.05) | 0.02 (0.01) | −0.01 (0.09) | −0.19 to 0.17 | |
| U1 | CoMy | 0.99 (0.01) | 0.09 (0.06) | 0.02 (0.01) | 0.16 (0.11) | −0.09 to 0.42 | |
| U2 | CoMy | 0.99 (0.02) | 0.16 (0.09) | 0.03 (0.02) | −0.21 (0.17) | −0.56 to 0.15 | |
| Sprint | CoMy | 1.00 (0.00) | 0.04 (0.02) | 0.00 (0.00) | −0.50 (0.30) | −0.70 to −0.29 |
References
- Van Der Kruk, E.; Reijne, M.M. Accuracy of human motion capture systems for sport applications; state-of-the-art review. Eur. J. Sport Sci. 2018, 18, 806–819. [Google Scholar] [CrossRef] [PubMed]
- Blair, S.; Duthie, G.; Robertson, S.; Hopkins, W.; Ball, K. Concurrent validation of an inertial measurement system to quantify kicking biomechanics in four football codes. J. Biomech. 2018, 73, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi, A.; Mitchell, E.; Richter, C.; Destelle, F.; Gowing, M.; O’Connor, N.E.; Moran, K. Toward Automatic Activity Classification and Movement Assessment During a Sports Training Session. IEEE Internet Things J. 2014, 2, 23–32. [Google Scholar] [CrossRef]
- Bolink, S.; Naisas, H.; Senden, R.; Essers, H.; Heyligers, I.; Meijer, K.; Grimm, B.; Information, P.E.K.F.C. Validity of an inertial measurement unit to assess pelvic orientation angles during gait, sit–stand transfers and step-up transfers: Comparison with an optoelectronic motion capture system*. Med Eng. Phys. 2016, 38, 225–231. [Google Scholar] [CrossRef]
- Al-Amri, M.; Nicholas, K.; Button, K.; Sparkes, V.; Sheeran, L.; Davies, J.L. Inertial Measurement Units for Clinical Movement Analysis: Reliability and Concurrent Validity. Sensors 2018, 18, 719. [Google Scholar] [CrossRef]
- Robert-Lachaine, X.; Mecheri, H.; Larue, C.; Plamondon, A. Validation of inertial measurement units with an optoelectronic system for whole-body motion analysis. Med. Biol. Eng. Comput. 2017, 55, 609–619. [Google Scholar] [CrossRef]
- Schepers, M.; Giuberti, M.; Bellusci, G. Xsens MVN: Consistent Tracking of Human Motion Using Inertial Sensing. Xsens Technol. 2018, 1–8. [Google Scholar] [CrossRef]
- Kristianslund, E.; Krosshaug, T.; Bogert, A.J.V.D. Effect of low pass filtering on joint moments from inverse dynamics: Implications for injury prevention. J. Biomech. 2012, 45, 666–671. [Google Scholar] [CrossRef]
- Taylor, W.; Kornaropoulos, E.; Duda, G.; Kratzenstein, S.; Ehrig, R.; Arampatzis, A.; Heller, M. Repeatability and reproducibility of OSSCA, a functional approach for assessing the kinematics of the lower limb. Gait Posture 2010, 32, 231–236. [Google Scholar] [CrossRef]
- Taylor, W.R.; Ehrig, R.M.; Duda, G.N.; Schell, H.; Seebeck, P.; Heller, M.O. On the influence of soft tissue coverage in the determination of bone kinematics using skin markers. J. Orthop. Res. 2005, 23, 726–734. [Google Scholar] [CrossRef]
- Ehrig, R.M.; Taylor, W.R.; Duda, G.N.; Heller, M.O. A survey of formal methods for determining functional joint axes. J. Biomech. 2007, 40, 2150–2157. [Google Scholar] [CrossRef] [PubMed]
- Ehrig, R.M.; Taylor, W.R.; Duda, G.N.; Heller, M.O. A survey of formal methods for determining the centre of rotation of ball joints. J. Biomech. 2006, 39, 2798–2809. [Google Scholar] [CrossRef] [PubMed]
- Bishop, C.; Paul, G.; Thewlis, D. Recommendations for the reporting of foot and ankle models. J. Biomech. 2012, 45, 2185–2194. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Rankine, L.; Long, J.T.; Canseco, K.; Harris, G.F. Multisegmental foot modeling: A review. Crit. Rev. Biomed. Eng. 2008, 36, 127–181. [Google Scholar] [CrossRef] [PubMed]
- Stagni, R.; Leardini, A.; Cappozzo, A.; Benedetti, M.G.; Cappello, A. Effects of hip joint centre mislocation on gait analysis results. J. Biomech. 2000, 33, 1479–1487. [Google Scholar] [CrossRef]
- Davis, R.B.; Õunpuu, S.; Tyburski, D.; Gage, J.R. A gait analysis data collection and reduction technique. Hum. Mov. Sci. 1991, 10, 575–587. [Google Scholar] [CrossRef]
- Pini, A.; Markström, J.L.; Schelin, L. Test-retest reliability measures for curve data: An overview with recommendations and supplementary code. Sports Biomech. 2019, 1–22. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Measuring agreement in method comparison studies. Stat. Methods Med. Res. 1999, 8, 135–160. [Google Scholar] [CrossRef]
- Gomes, R.D.C.; Meyer, P.M.; De Castro, A.L.; Netto, A.S.; Rodrigues, P.H.M. Accuracy, precision and robustness of different methods to obtain samples from silages in fermentation studies. Rev. Bras. Zootec. 2012, 41, 1369–1377. [Google Scholar] [CrossRef]
- Mukaka, M.M. Statistics corner: A guide to appropriate use of correlation coefficient in medical research. Malawi Med. J. 2012, 24, 69–71. [Google Scholar]
- Koska, D.; Gaudel, J.; Hein, T.; Maiwald, C. Validation of an inertial measurement unit for the quantification of rearfoot kinematics during running. Gait Posture 2018, 64, 135–140. [Google Scholar] [CrossRef]
- Szczerbik, E.; Kalinowska, M. The influence of knee marker placement error on evaluation of gait kinematic parameters. Acta Bioeng. Biomech. 2011, 13, 43–46. [Google Scholar] [PubMed]
- Cockcroft, J.; Louw, Q.; Baker, R. Proximal placement of lateral thigh skin markers reduces soft tissue artefact during normal gait using the Conventional Gait Model. Comput. Methods Biomech. Biomed. Eng. 2016, 19, 1–8. [Google Scholar] [CrossRef]
- Groen, B.; Geurts, M.; Nienhuis, B.; Duysens, J. Sensitivity of the OLGA and VCM models to erroneous marker placement: Effects on 3D-gait kinematics. Gait Posture 2012, 35, 517–521. [Google Scholar] [CrossRef] [PubMed]
- McFadden, C.; Daniles, K.; Strike, S. The sensitivity of joint kinematics and kinetics to marker placement during a change of direction task. J. Biomech. 2019, 37, 29. [Google Scholar] [CrossRef]
- McGinley, J.L.; Baker, R.; Wolfe, R.; Morris, M.E. The reliability of three-dimensional kinematic gait measurements: A systematic review. Gait Posture 2009, 29, 360–369. [Google Scholar] [CrossRef] [PubMed]
- Roewer, B.D.; Ford, K.R.; Myer, G.D.; Hewett, T.E. The “impact” of force fi ltering cut-off frequency on the peak knee abduction moment during landing: Artefact or “arti fi ction”? Br. J. Sport Med. 2014, 48, 464–468. [Google Scholar] [CrossRef] [PubMed]
- Baker, R.; Finney, L.; Orr, J. A new approach to determine the hip rotation profile from clinical gait analysis data. Hum. Mov. Sci. 1999, 18, 655–667. [Google Scholar] [CrossRef]









| Completion Time | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Subject | Session | Samples | Mean | Std | Best | Worst | 25% | 50% | 75% |
| S1 | Test1 | 10 | 18.336 | 0.733 | 17.210 | 19.290 | 17.784 | 18.320 | 18.910 |
| Test2 | 10 | 19.276 | 0.563 | 18.620 | 20.080 | 18.806 | 19.188 | 19.783 | |
| S2 | Test1 | 10 | 20.934 | 0.485 | 20.205 | 21.665 | 20.591 | 20.883 | 21.299 |
| Test2 | 10 | 21.417 | 0.274 | 21.040 | 21.915 | 21.249 | 21.430 | 21.525 | |
| S3 | Test1 | 10 | 20.576 | 0.419 | 19.730 | 21.195 | 20.323 | 20.663 | 20.826 |
| Test2 | 10 | 21.695 | 0.908 | 20.845 | 23.945 | 21.153 | 21.428 | 21.714 | |
| S4 | Test1 | 10 | 20.236 | 0.347 | 19.860 | 20.935 | 19.960 | 20.115 | 20.325 |
| Test2 | 8 | 20.685 | 0.217 | 20.340 | 21.075 | 20.619 | 20.658 | 20.756 | |
| S5 | Test1 | 9 | 18.627 | 0.380 | 18.340 | 19.360 | 18.351 | 18.493 | 18.653 |
| Test2 | 10 | 18.661 | 0.285 | 18.135 | 19.095 | 18.536 | 18.723 | 18.833 | |
| S6 | Test1 | 10 | 18.237 | 0.217 | 18.075 | 18.765 | 18.100 | 18.135 | 18.325 |
| Test2 | 10 | 17.593 | 0.307 | 17.085 | 17.935 | 17.445 | 17.633 | 17.819 | |
| Ankle | Knee | Hip | Pelvis | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| fle. | abd. | rot. | fle. | abd. | rot. | fle. | abd. | rot. | fle. | abd. | rot. | ||
| Marker error | |||||||||||||
| Cockcroft [23] | bias | - | - | - | 4 | −6 | - | - | - | −17 | - | - | - |
| Szczerbik [22] b | bias | 15 | - | 22 | 10 | 15 | - | 6 | - | 11 | - | - | - |
| Groen [24] VCM | RMSD | ~2 | ~3 | ~9 | ~4 | ~6 | ~8 | ~3 | ~2 | ~9 | ~1 c | ~1 c | ~1 c |
| Groen [24] OLGA | RMSD | ~2 | ~1 | ~8 | ~3 | ~2 | ~6 | ~2 | ~3 | ~6 | ~1 c | ~2 c | ~1 c |
| McFadden [25] | bias | - | ~1 | ~6 | ~4 | ~5 | ~5 | - | - | ~5 | - | - | - |
| Inter-assessor error | |||||||||||||
| McGinley [26] a | Std | 2 | - | - | 3 | 2 | 5 | 4 | 2 | 5 | 3 | 2 | 2 |
| Study findings | |||||||||||||
| bias | 4 | 1 | 3 | 4 | 9 | 6 | 12 | 8 | 9 | 16 | 1 | 3 | |
| (95% limit) | (13) | (22) | (29) | (14) | (20) | (24) | (22) | (17) | (28) | (21) | (5) | (10) | |
| RMSD | 4 | 9 | 6 | 4 | 3 | 3 | 3 | 4 | 5 | 2 | 2 | 3 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Richter, C.; Daniels, K.A.J.; King, E.; Franklyn-Miller, A. Agreement between Inertia and Optical Based Motion Capture during the VU-Return-to-Play- Field-Test. Sensors 2020, 20, 831. https://doi.org/10.3390/s20030831
Richter C, Daniels KAJ, King E, Franklyn-Miller A. Agreement between Inertia and Optical Based Motion Capture during the VU-Return-to-Play- Field-Test. Sensors. 2020; 20(3):831. https://doi.org/10.3390/s20030831
Chicago/Turabian StyleRichter, Chris, Katherine A. J. Daniels, Enda King, and Andrew Franklyn-Miller. 2020. "Agreement between Inertia and Optical Based Motion Capture during the VU-Return-to-Play- Field-Test" Sensors 20, no. 3: 831. https://doi.org/10.3390/s20030831
APA StyleRichter, C., Daniels, K. A. J., King, E., & Franklyn-Miller, A. (2020). Agreement between Inertia and Optical Based Motion Capture during the VU-Return-to-Play- Field-Test. Sensors, 20(3), 831. https://doi.org/10.3390/s20030831