Demonstration of Optical Coherence Tomography Guided Big Bubble Technique for Deep Anterior Lamellar Keratoplasty (DALK)

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Methods and Materials
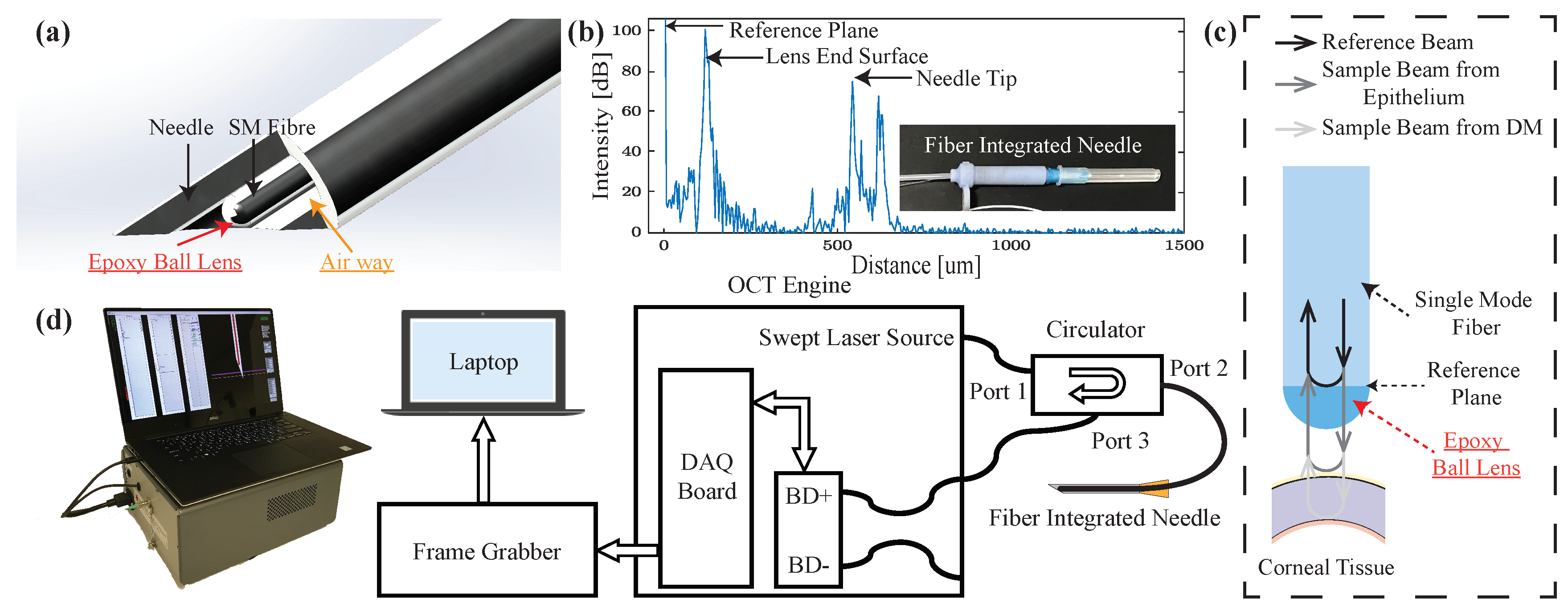
2.1. Common-Path OCT
2.2. OCT Distal Sensor Integrated Needle
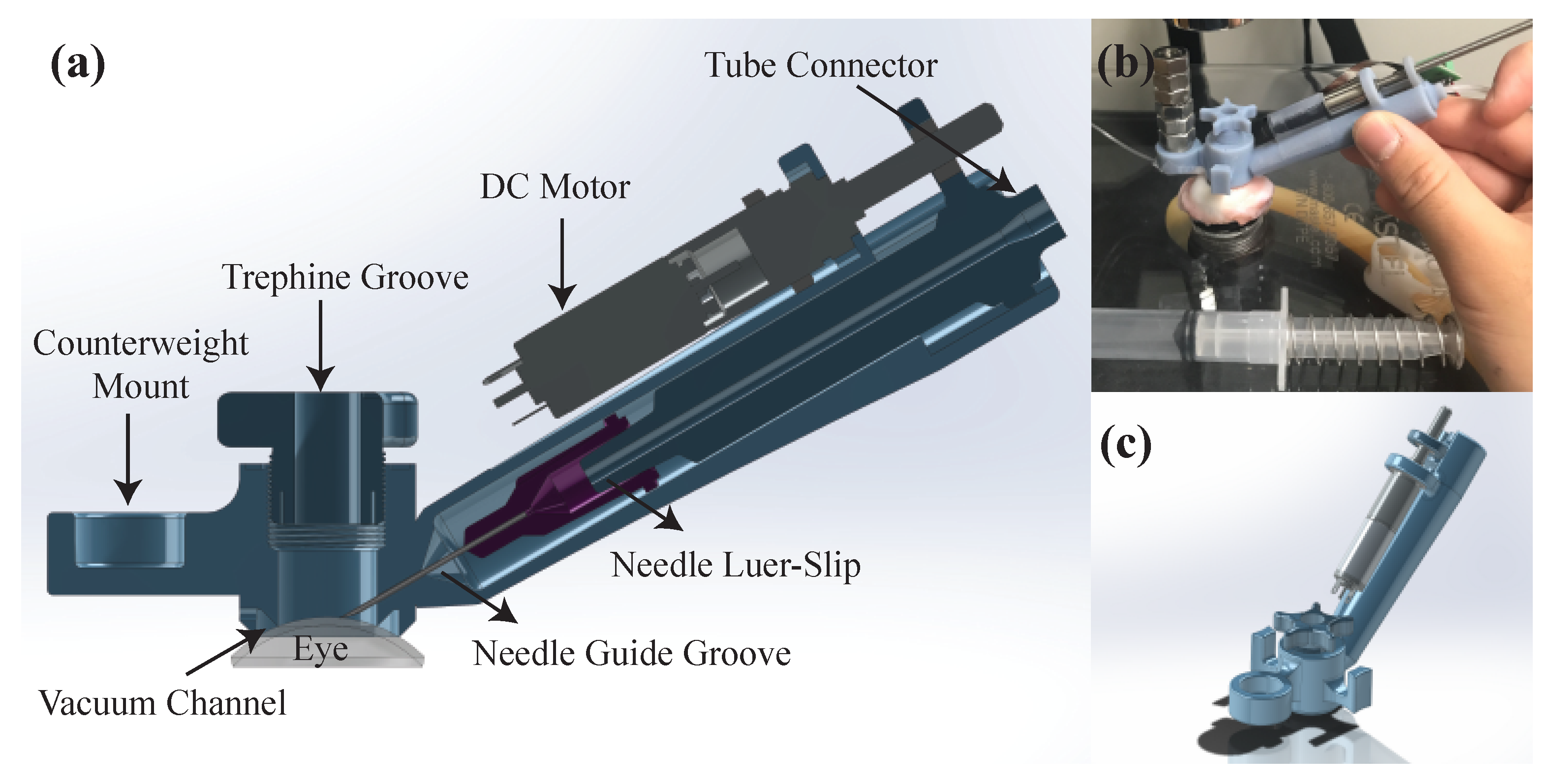
2.3. AUTO-DALK Device Design
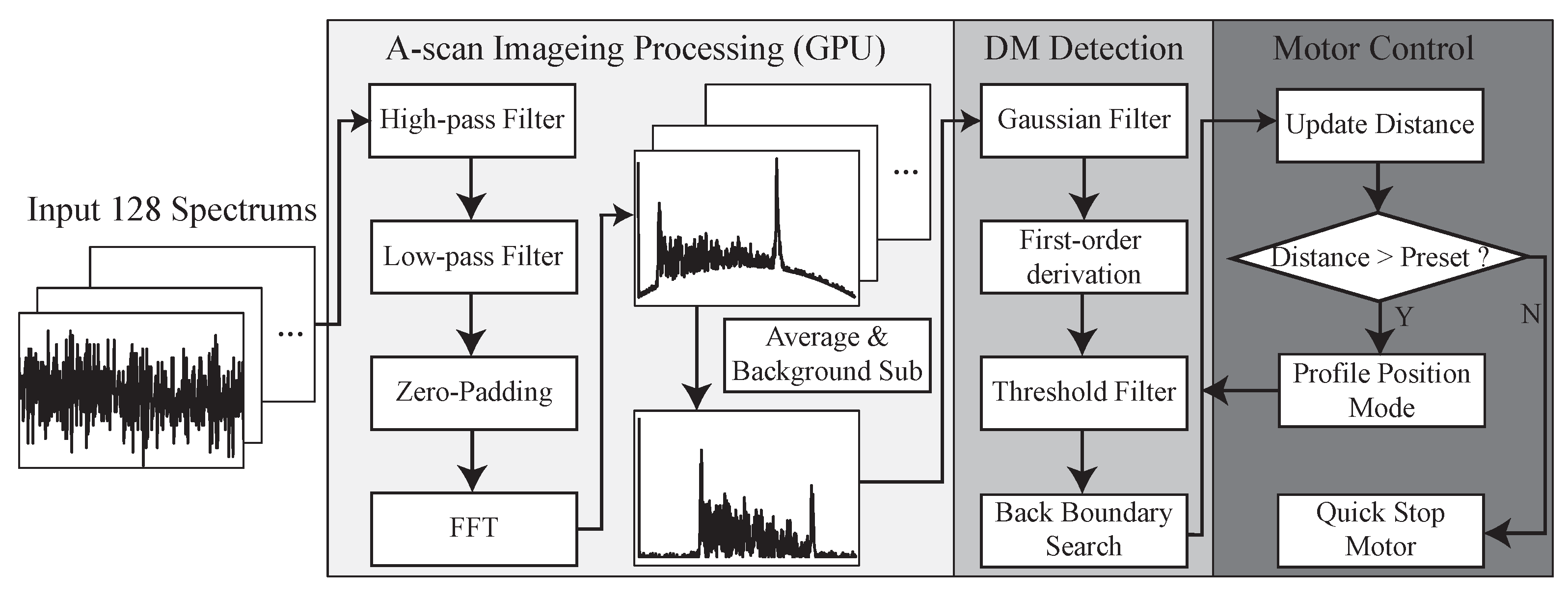
2.4. Signal Processing and Control Methods
3. Experiments and Results
3.1. Deformation Test
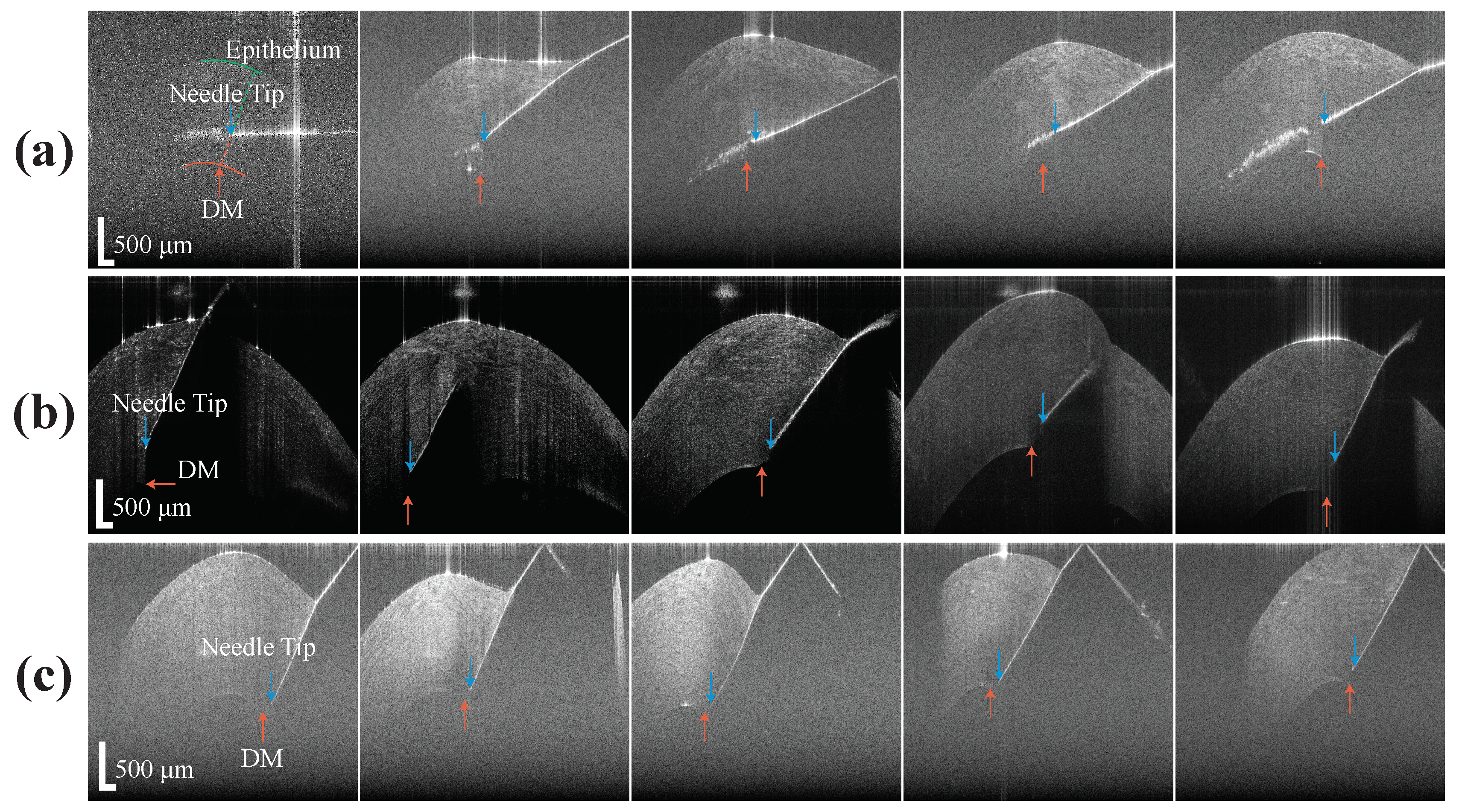
3.2. Unassisted and Assisted Freehand Insertion Test
3.3. AUTO-DALK Insertion Test
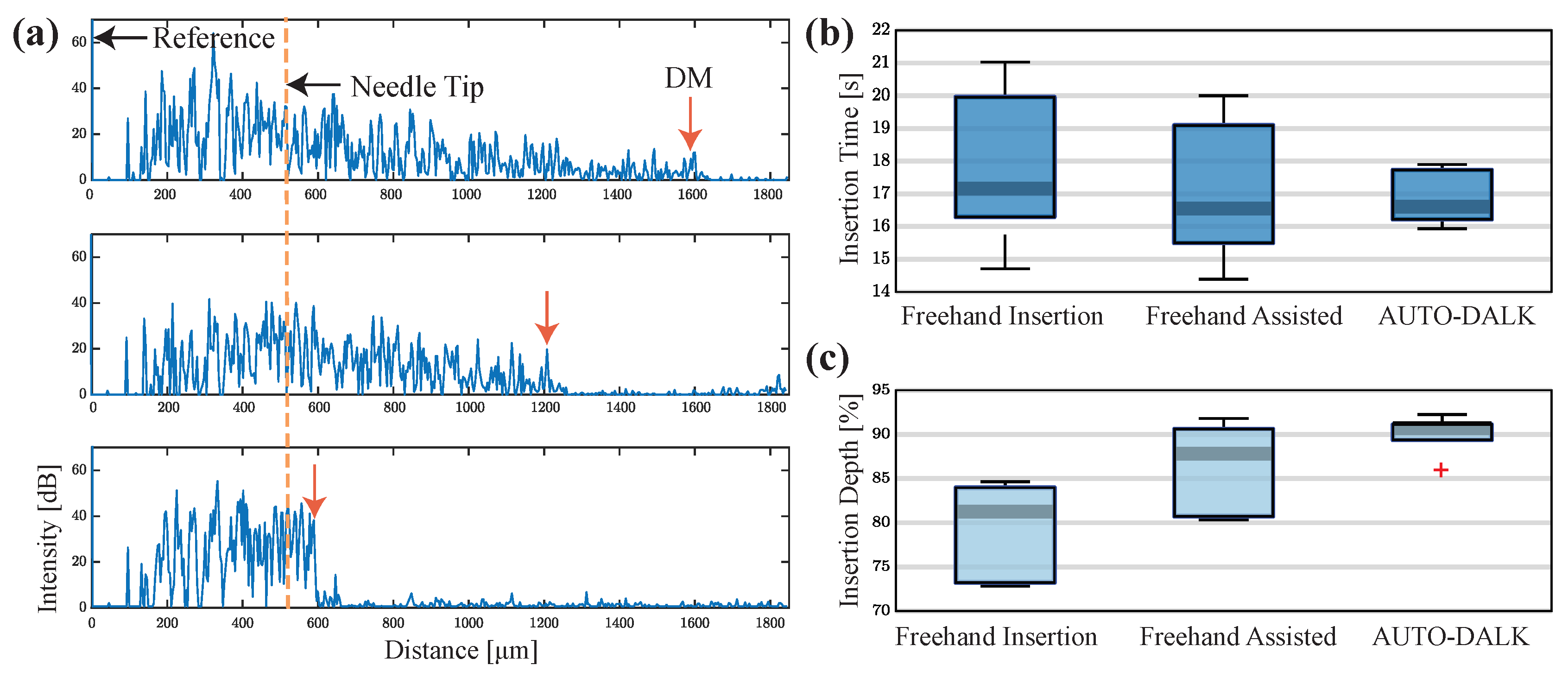
3.4. Comparison of Needle Insertion Tests
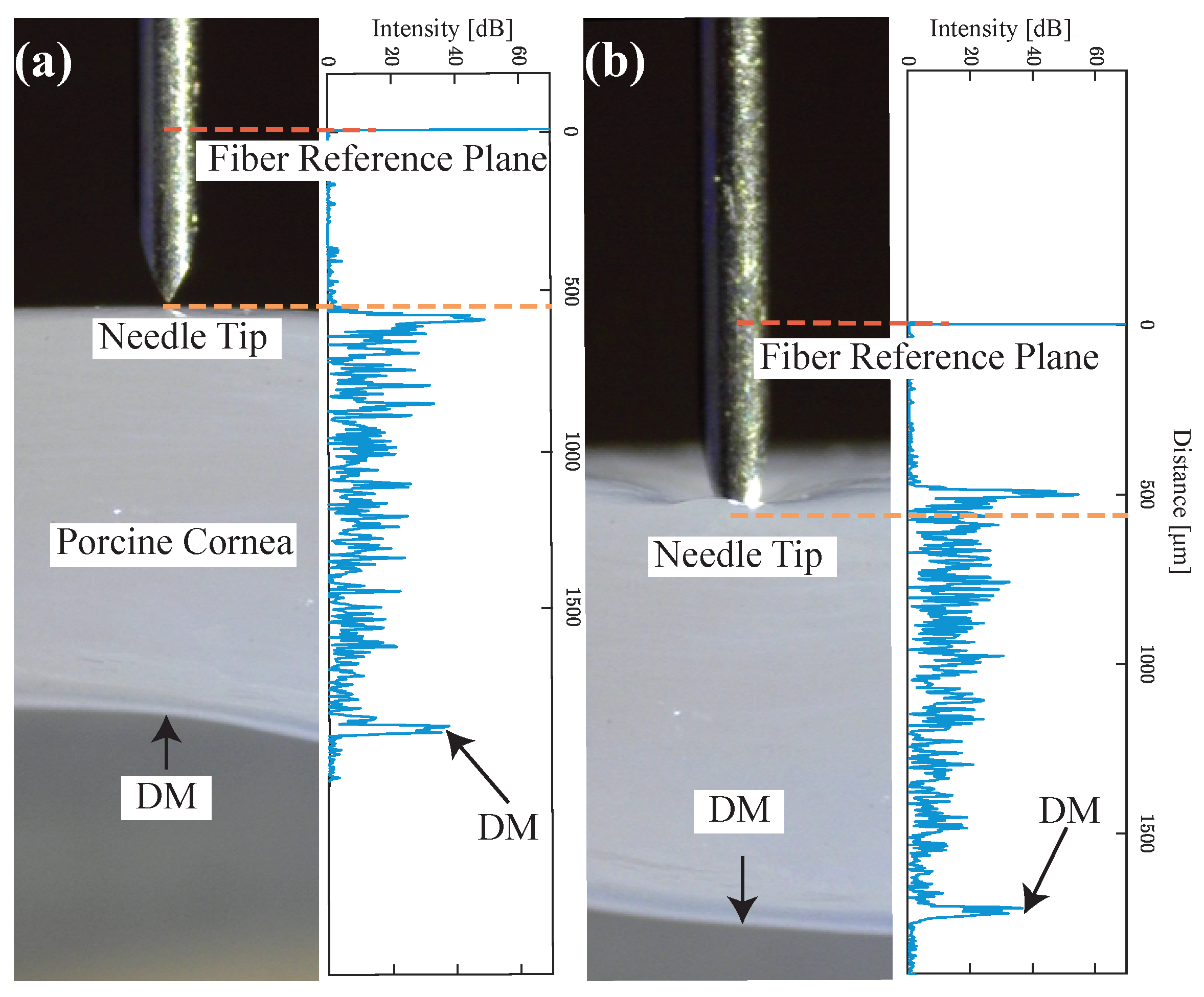
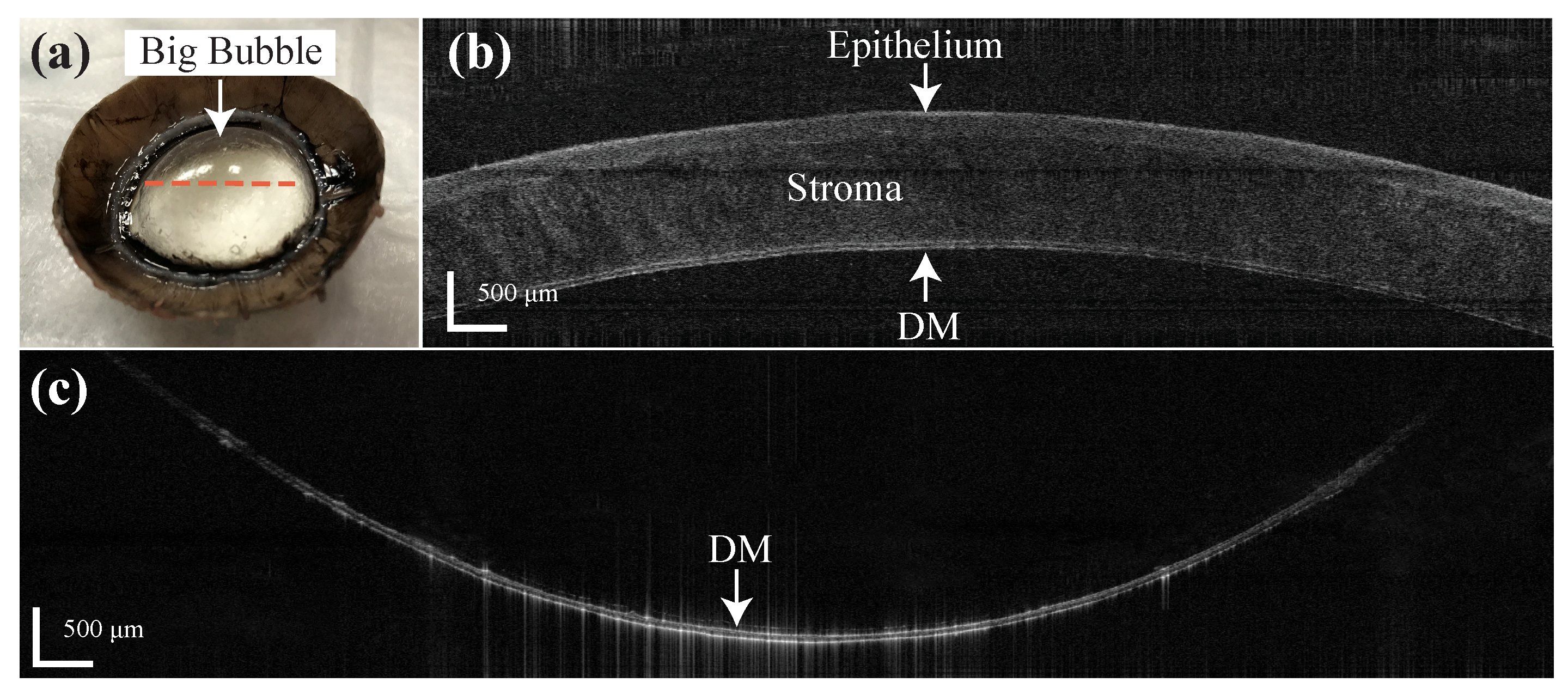
3.5. Feasibility Test of Pneumo-Dissection on Bovine Eyes
4. Discussion and Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| DM | Descemet’s membrane |
| PK | Penetrating keratoplasty |
| DALK | Deep anterior lamellar keratoplasty |
| BB | Big bubble |
| OCT | Optical coherence tomography |
| TD | Time domain |
| SS | Swept source |
| FD | Fourier domain |
| SNR | Signal to noise ratio |
| CP-SSOCT | Common-path swept source optical coherence tomography |
| BD | Balanced detector |
| CAD | Computer-aided design |
| GPU | Graphic processing unit |
| FFT | Fast Fourier transfer |
| AC | Anterior chamber |
| IOP | Intraocular pressure |
References
- Porth, J.M.; Deiotte, E.; Dunn, M.; Bashshur, R. A Review of the Literature on the Global Epidemiology of Corneal Blindness. Cornea 2019, 38, 1602–1609. [Google Scholar] [CrossRef] [PubMed]
- Guilbert, E.; Bullet, J.; Sandali, O.; Basli, E.; Laroche, L.; Borderie, V.M. Long-term rejection incidence and reversibility after penetrating and lamellar keratoplasty. Am. J. Ophthalmol. 2013, 155, 560–569. [Google Scholar] [CrossRef] [PubMed]
- Reinhart, W.J.; Musch, D.C.; Jacobs, D.S.; Lee, W.B.; Kaufman, S.C.; Shtein, R.M. Deep anterior lamellar keratoplasty as an alternative to penetrating keratoplasty: A report by the American Academy of Ophthalmology. Ophthalmology 2011, 118, 209–218. [Google Scholar] [CrossRef] [PubMed]
- Borderie, V.M.; Sandali, O.; Bullet, J.; Gaujoux, T.; Touzeau, O.; Laroche, L. Long-term results of deep anterior lamellar versus penetrating keratoplasty. Ophthalmology 2012, 119, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.; Qi, X.; Zhao, J.; Zhai, H.; Xie, L. Comparison of penetrating keratoplasty and deep lamellar keratoplasty for macular corneal dystrophy and risk factors of recurrence. Ophthalmology 2013, 120, 34–39. [Google Scholar] [CrossRef] [PubMed]
- McKee, H.D.; Irion, L.C.; Carley, F.M.; Jhanji, V.; Brahma, A.K. Residual corneal stroma in big-bubble deep anterior lamellar keratoplasty: A histological study in eye-bank corneas. Br. J. Ophthalmol. 2011, 95, 1463–1465. [Google Scholar] [CrossRef]
- Goweida, M.B.B. Intraoperative review of different bubble types formed during pneumodissection (big-bubble) deep anterior lamellar keratoplasty. Cornea 2015, 34, 621–624. [Google Scholar] [CrossRef]
- Anwar, M.; Teichmann, K.D. Big-bubble technique to bare Descemet’s membrane in anterior lamellar keratoplasty. J. Cataract Refract. Surg. 2002, 28, 398–403. [Google Scholar] [CrossRef]
- Fogla, R.; Padmanabhan, P. Results of deep lamellar keratoplasty using the big-bubble technique in patients with keratoconus. Am. J. Ophthalmol. 2006, 141, 254–259. [Google Scholar] [CrossRef]
- Feizi, S.; Javadi, M.A.; Jamali, H.; Mirbabaee, F. Deep anterior lamellar keratoplasty in patients with keratoconus: Big-bubble technique. Cornea 2010, 29, 177–182. [Google Scholar] [CrossRef]
- Parthasarathy, A.; Yong, M.P.; Tan, D.T.H. Use of a “small-bubble technique” to increase the success of Anwar’s "big-bubble technique" for deep lamellar keratoplasty with complete baring of Descemet’s membrane. Br. J. Ophthalmol. 2007, 91, 1369–1373. [Google Scholar] [CrossRef] [PubMed]
- Smadja, D.; Colin, J.; Krueger, R.R.; Mello, G.R.; Gallois, A.; Mortemousque, B.; Touboul, D. Outcomes of deep anterior lamellar keratoplasty for keratoconus: Learning curve and advantages of the big bubble technique. Cornea 2012, 31, 859–863. [Google Scholar] [CrossRef] [PubMed]
- Ünal, M.; Bilgin, B.; Yucel, I.; Akar, Y.; Apaydin, C. Conversion to deep anterior lamellar keratoplasty (DALK): Learning curve with big-bubble technique. Ophthalmic Surg. Lasers Imaging Retin. 2010, 41, 642–650. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, U.K.; Fares, U.; Rahman, I.; Said, D.G.; Maharajan, S.V.; Dua, H.S. Outcomes of deep anterior lamellar keratoplasty following successful and failed ‘big bubble’. Br. J. Ophthalmol. 2012, 96, 564–569. [Google Scholar] [CrossRef] [PubMed]
- Riss, S.; Heindl, L.M.; Bachmann, B.O.; Kruse, F.E.; Cursiefen, C. Pentacam-based big bubble deep anterior lamellar keratoplasty in patients with keratoconus. Cornea 2012, 31, 627–632. [Google Scholar] [CrossRef]
- Pasricha, N.D.; Shieh, C.; Carrasco-Zevallos, O.M.; Keller, B.; Cunefare, D.; Mehta, J.S.; Farsiu, S.; Izatt, J.A.; Toth, C.A.; Kuo, A.N. Needle Depth and Big Bubble Success in Deep Anterior Lamellar Keratoplasty: An Ex Vivo Microscope-Integrated OCT Study. Cornea 2016, 35, 1471. [Google Scholar] [CrossRef]
- Huang, D.; Swanson, E.A.; Lin, C.P.; Schuman, J.S.; Stinson, W.G.; Chang, W.; Hee, M.R.; Flotte, T.; Gregory, K.; Puliafito, C.A.; et al. Optical coherence tomography. Science 1991, 254, 1178–1181. [Google Scholar] [CrossRef]
- Drexler, W.; Fujimoto, J.G. State-of-the-art retinal optical coherence tomography. Prog. Retin. Eye Res. 2008, 27, 45–88. [Google Scholar] [CrossRef]
- Iordachita, I.; Sun, Z.; Balicki, M.; Kang, J.U.; Phee, S.J.; Handa, J.; Gehlbach, P.; Taylor, R. A sub-millimetric, 0.25 mN resolution fully integrated fiber-optic force-sensing tool for retinal microsurgery. Int. J. Comput. Assist. Radiol. Surg. 2009, 4, 383–390. [Google Scholar] [CrossRef]
- Huang, Y.; Liu, X.; Kang, J.U. Real-time 3D and 4D Fourier domain Doppler optical coherence tomography based on dual graphics processing units. Biomed. Opt. Express 2012, 3, 2162–2174. [Google Scholar] [CrossRef]
- Zhang, K.; Kang, J.U. Common-path low-coherence interferometry fiber-optic sensor guided microincision. J. Biomed. Opt. 2011, 16, 095003. [Google Scholar] [CrossRef] [PubMed]
- Ehlers, J.P.; Srivastava, S.K.; Feiler, D.; Noonan, A.I.; Rollins, A.M.; Tao, Y.K. Integrative advances for OCT-guided ophthalmic surgery and intraoperative OCT: Microscope integration, surgical instrumentation, and heads-up display surgeon feedback. PLoS ONE 2014, 9, e105224. [Google Scholar] [CrossRef] [PubMed]
- Choma, M.A.; Sarunic, M.V.; Yang, C.; Izatt, J.A. Sensitivity advantage of swept source and Fourier domain optical coherence tomography. Opt. Express 2003, 11, 2183–2189. [Google Scholar] [CrossRef] [PubMed]
- Cogliati, A.; Canavesi, C.; Hayes, A.; Tankam, P.; Duma, V.F.; Santhanam, A.; Thompson, K.P.; Rolland, J.P. MEMS-based handheld scanning probe with pre-shaped input signals for distortion-free images in Gabor-domain optical coherence microscopy. Opt. Express 2016, 24, 13365–13374. [Google Scholar] [CrossRef] [PubMed]
- Tao, Y.K.; LaBarbera, M.; Ehlers, J.P.; Srivastava, S.K.; Dupps, W.J., Jr. Image-guided modified deep anterior lamellar keratoplasty (DALK) corneal transplant using intraoperative optical coherence tomography. In Ophthalmic Technologies XXV; International Society for Optics and Photonics: Washington, DC, USA, 2015; Volume 9307, p. 930708. [Google Scholar]
- Kang, J.; Cheon, G. Demonstration of Subretinal Injection Using Common-Path Swept Source OCT Guided Microinjector. Appl. Sci. 2018, 8, 1287. [Google Scholar] [CrossRef]
- Cheon, G.W.; Huang, Y.; Cha, J.; Gehlbach, P.L.; Kang, J.U. Accurate real-time depth control for CP-SSOCT distal sensor based handheld microsurgery tools. Biomed. Opt. Express 2015, 6, 1942–1953. [Google Scholar] [CrossRef]
- Kang, J.U.; Huang, Y.; Cha, J.; Zhang, K.; Ibrahim, Z.; Lee, W.A.; Brandacher, G.; Gehlbach, P. Real-time three-dimensional Fourier-domain optical coherence tomography video image guided microsurgeries. J. Biomed. Opt. 2012, 17, 081403. [Google Scholar] [CrossRef]
- Wei, S.; Guo, S.; Kang, J.U. Analysis and evaluation of BC-mode OCT image visualization for microsurgery guidance. Biomed. Opt. Express 2019, 10, 5268–5290. [Google Scholar] [CrossRef]
- Viehland, C.; Keller, B.; Carrasco-Zevallos, O.M.; Nankivil, D.; Shen, L.; Mangalesh, S.; Kuo, A.N.; Toth, C.A.; Izatt, J.A. Enhanced volumetric visualization for real time 4D intraoperative ophthalmic swept-source OCT. Biomed. Opt. Express 2016, 7, 1815–1829. [Google Scholar] [CrossRef]
- Draelos, M.; Keller, B.; Tang, G.; Kuo, A.; Hauser, K.; Izatt, J. Real-Time Image-Guided Cooperative Robotic Assist Device for Deep Anterior Lamellar Keratoplasty. In Proceedings of the 2018 IEEE International Conference on Robotics and Automation (ICRA), Brisbane, QLD, Australia, 21–25 May 2018; pp. 1–9. [Google Scholar]
- Shin, S.; Bae, J.K.; Ahn, Y.; Kim, H.; Choi, G.; Yoo, Y.S.; Joo, C.K.; Moon, S.; Jung, W. Lamellar keratoplasty using position-guided surgical needle and M-mode optical coherence tomography. J. Biomed. Opt. 2017, 22, 125005. [Google Scholar] [CrossRef]
- Guo, S.; Sarfaraz, N.; Gensheimer, W.G.; Krieger, A.; Kang, J.U. Optical Coherence Tomography Guided Robotic Device for Autonomous Needle Insertion in Cornea Transplant Surgery. In Proceedings of the 2019 IEEE/RSJ International Conference on Intelligent Robots and Systems (IROS), Macau, China, 3–8 November 2019. [Google Scholar]
- Kang, J.U.; Han, J.H.; Liu, X.; Zhang, K.; Song, C.G.; Gehlbach, P. Endoscopic functional Fourier domain common-path optical coherence tomography for microsurgery. IEEE J. Sel. Top. Quantum Electron. 2009, 16, 781–792. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Lee, C.; Verkade, R.; Cheon, G.W.; Kang, J.U. Common-path all-fiber optical coherence tomography probe based on high-index elliptical epoxy-lensed fiber. Opt. Eng. 2019, 58, 026116. [Google Scholar] [CrossRef]
- Park, S.; Rim, S.; Kim, J.; Park, J.; Sohn, I.B.; Lee, B. Analysis of Design and Fabrication Parameters for Lensed Optical Fibers as Pertinent Probes for Sensing and Imaging. Sensors 2018, 18, 4150. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Y.; Yang, J.; Huang, K.; Lee, Z.; Lee, X. A comparison of biomechanical properties between human and porcine cornea. J. Biomech. 2001, 34, 533–537. [Google Scholar] [CrossRef]
- Bhogal, M.; Lwin, C.N.; Seah, X.Y.; Murugan, E.; Adnan, K.; Lin, S.J.; Peh, G.; Mehta, J.S. Real-time assessment of corneal endothelial cell damage following graft preparation and donor insertion for DMEK. PLoS ONE 2017, 12, e0184824. [Google Scholar] [CrossRef]
- Teng, S.W.; Tan, H.Y.; Peng, J.L.; Lin, H.H.; Kim, K.H.; Lo, W.; Sun, Y.; Lin, W.C.; Lin, S.J.; Jee, S.H.; et al. Multiphoton autofluorescence and second-harmonic generation imaging of the ex vivo porcine eye. Investig. Ophthalmol. Vis. Sci. 2006, 47, 1216–1224. [Google Scholar] [CrossRef]








© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, S.; Sarfaraz, N.R.; Gensheimer, W.G.; Krieger, A.; Kang, J.U. Demonstration of Optical Coherence Tomography Guided Big Bubble Technique for Deep Anterior Lamellar Keratoplasty (DALK). Sensors 2020, 20, 428. https://doi.org/10.3390/s20020428
Guo S, Sarfaraz NR, Gensheimer WG, Krieger A, Kang JU. Demonstration of Optical Coherence Tomography Guided Big Bubble Technique for Deep Anterior Lamellar Keratoplasty (DALK). Sensors. 2020; 20(2):428. https://doi.org/10.3390/s20020428
Chicago/Turabian StyleGuo, Shoujing, Nicolas R. Sarfaraz, William G. Gensheimer, Axel Krieger, and Jin U. Kang. 2020. "Demonstration of Optical Coherence Tomography Guided Big Bubble Technique for Deep Anterior Lamellar Keratoplasty (DALK)" Sensors 20, no. 2: 428. https://doi.org/10.3390/s20020428
APA StyleGuo, S., Sarfaraz, N. R., Gensheimer, W. G., Krieger, A., & Kang, J. U. (2020). Demonstration of Optical Coherence Tomography Guided Big Bubble Technique for Deep Anterior Lamellar Keratoplasty (DALK). Sensors, 20(2), 428. https://doi.org/10.3390/s20020428