Feasibility and Reliability of SmartWatch to Obtain 3-Lead Electrocardiogram Recordings



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Data Collection
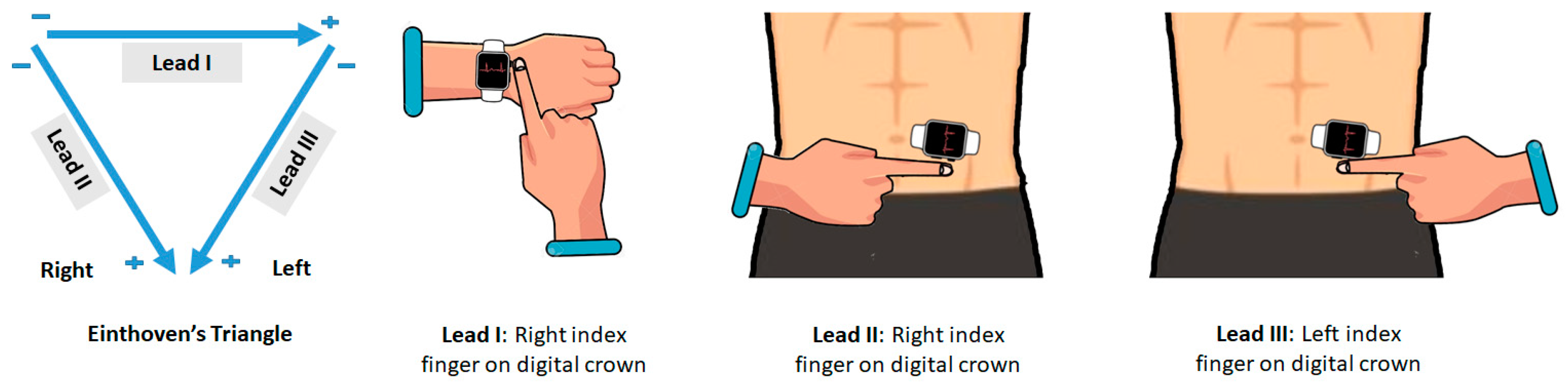
2.3. ECG Recording with Smartwatch
2.4. Data Transfer
2.5. Data Processing
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Heart Rate
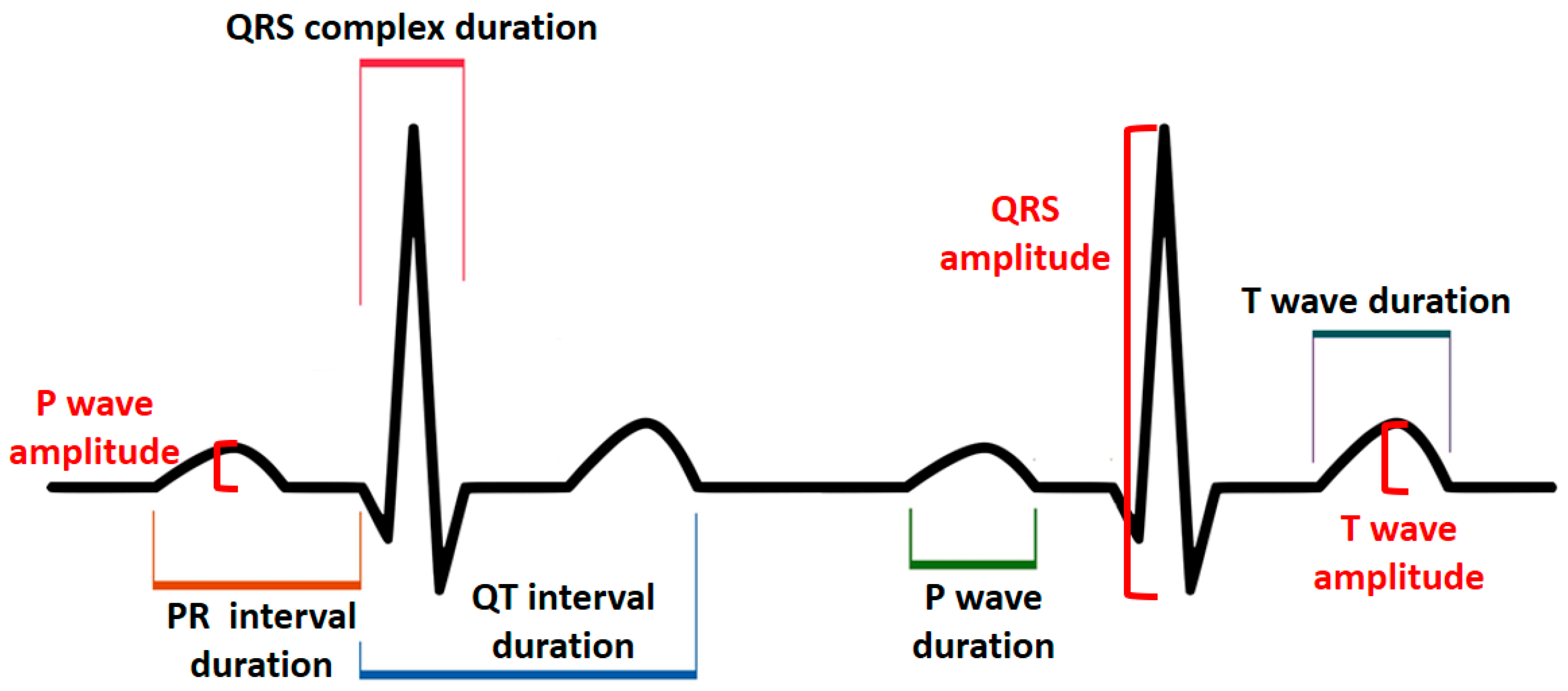
3.3. Duration, Amplitude, and Polarity
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Taggar, J.S.; Coleman, T.; Lewis, S.; Heneghan, C.; Jones, M. Accuracy of methods for diagnosing atrial fibrillation using 12-lead ECG: A systematic review and meta-analysis. Int. J. Cardiol. 2015, 184, 175–183. [Google Scholar] [CrossRef]
- Bansal, A.; Joshi, R. Portable out-of-hospital electrocardiography: A review of current technologies. J. Arrhythmia 2018, 34, 129–138. [Google Scholar] [CrossRef]
- Pevnick, J.M.; Birkeland, K.; Zimmer, R.; Elad, Y.; Kedan, I. Wearable technology for cardiology: An update and framework for the future. Trends Cardiovasc. Med. 2018, 28, 144–150. [Google Scholar] [CrossRef]
- Perez, M.V.; Mahaffey, K.W.; Hedlin, H.; Rumsfeld, J.S.; Garcia, A.; Ferris, T.; Balasubramanian, V.; Russo, A.M.; Rajmane, A.; Cheung, L.; et al. Large-Scale Assessment of a Smartwatch to Identify Atrial Fibrillation. N. Engl. J. Med. 2019, 381, 1909–1917. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Wang, H.; Zhang, H.; Liu, T.; Liang, Z.; Xia, Y.; Yan, L.; Xing, Y.; Shi, H.; Li, S.; et al. Mobile Photoplethysmographic Technology to Detect Atrial Fibrillation. J. Am. Coll. Cardiol. 2019, 74, 2365–2375. [Google Scholar] [CrossRef] [PubMed]
- Mehta, D.D.; Nazir, N.T.; Trohman, R.G.; Volgman, A.S. Single-lead portable ECG devices: Perceptions and clinical accuracy compared to conventional cardiac monitoring. J. Electrocardiol. 2015, 48, 710–716. [Google Scholar] [CrossRef] [PubMed]
- Avila, C.O. Novel Use of Apple Watch 4 to Obtain 3-Lead Electrocardiogram and Detect Cardiac Ischemia. Perm. J. 2019, 23, 19–25. [Google Scholar]
- Isakadze, N.; Martin, S.S. How useful is the smartwatch ECG? Trends Cardiovasc. Med. 2019, in press. [Google Scholar] [CrossRef]
- Shamloo, A.S.; Bollmann, A.; Dagres, N.; Arya, A.; Hindricks, G. Smart Watch Devices for Atrial Fibrillation Screening: It Has to Start Somewhere. J. Am. Coll. Cardiol. 2020, 75, 1364–1365. [Google Scholar] [CrossRef]
- Nielsen, J.C.; Lin, Y.J.; Figueiredo, M.J.d.O.; Shamloo, A.S.; Alfie, A.; Boveda, S.; Dagres, N.; Di Toro, D.; Eckhardt, L.L.; Ellenbogen, K.; et al. European Heart Rhythm Association (EHRA)/Heart Rhythm Society (HRS)/Asia Pacific Heart Rhythm Society (APHRS)/Latin American Heart Rhythm Society (LAHRS) expert consensus on risk assessment in cardiac arrhythmias: Use the right tool for the right outcome, in the right population. EP Eur. 2020, 22, 1147–1148. [Google Scholar]
- Cho, D.J. Beyond the early adopter: The smartwatch ECG goes mainstream. Trends Cardiovasc. Med. 2019, in press. [Google Scholar] [CrossRef] [PubMed]
- Gil, M.C. Standard and Precordial Leads Obtained with an Apple Watch. Ann. Intern. Med. 2020, 172, 436–437. [Google Scholar] [CrossRef]
- Samol, A.; Bischof, K.; Luani, B.; Pascut, D.; Wiemer, M.; Kaese, S. Patient Directed Recording of a Bipolar Three-Lead Electrocardiogram using a Smartwatch with ECG Function. J. Vis. Exp. 2019, 11, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Samol, A.; Bischof, K.; Luani, B.; Pascut, D.; Wiemer, M.; Kaese, S. Recording of Bipolar Multichannel ECGs by a Smartwatch: Modern ECG Diagnostic 100 Years after Einthoven. Sensors 2019, 19, 2894. [Google Scholar] [CrossRef] [PubMed]
- Samol, A.; Bischof, K.; Luani, B.; Pascut, D.; Wiemer, M.; Kaese, S. Single-Lead ECG Recordings Including Einthoven and Wilson Leads by a Smartwatch: A New Era of Patient Directed Early ECG Differential Diagnosis of Cardiac Diseases? Sensors 2019, 19, 4377. [Google Scholar] [CrossRef] [PubMed]
- Li, K.H.C.; White, F.A.; Tipoe, T.; Liu, T.; Wong, M.C.; Jesuthasan, A.; Baranchuk, A.; Tse, G.; Yan, B.P. The Current State of Mobile Phone Apps for Monitoring Heart Rate, Heart Rate Variability, and Atrial Fibrillation: Narrative Review. JMIR mHealth uHealth 2019, 7, e11606. [Google Scholar] [CrossRef] [PubMed]
- Schukraft, S.; Mancinetti, M.; Hayoz, D.; Faucherre, Y.; Cook, S.; Arroyo, D.; Puricel, S. Handheld ECG Tracking of in-hOspital Atrial Fibrillation the HECTO-AF trial Clinical Study Protocol. Trials 2019, 20, 92. [Google Scholar] [CrossRef] [PubMed]
- Verbrugge, F.H.; Proesmans, T.; Vijgen, J.; Mullens, W.; Rivero-Ayerza, M.; Van Herendael, H.; Vandervoort, P.; Nuyens, D. Atrial fibrillation screening with photo-plethysmography through a smartphone camera. EP Eur. 2019, 21, 1167–1175. [Google Scholar] [CrossRef]
- Wasserlauf, J.; You, C.; Patel, R.; Valys, A.; Albert, D.; Passman, R. Smartwatch Performance for the Detection and Quantification of Atrial Fibrillation. Circ. Arrhythmia Electrophysiol. 2019, 12, e006834. [Google Scholar] [CrossRef]
- Raja, J.M.; Elsakr, C.; Roman, S.; Cave, B.; Pour-Ghaz, I.; Nanda, A.; Maturana, M.; Khouzam, R.N. Apple Watch, Wearables, and Heart Rhythm: Where do we stand? Ann. Transl. Med. 2019, 7, 417. [Google Scholar] [CrossRef]
- Sajeev, J.K.; Koshy, A.N.; Teh, A.W. Wearable devices for cardiac arrhythmia detection: A new contender? Intern. Med. J. 2019, 49, 570–573. [Google Scholar] [CrossRef]
- Postema, P.G.; Wilde, A.A.M. The measurement of the QT interval. Curr. Cardiol. Rev. 2014, 10, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Rautaharju, P.M.; Surawicz, B.; Gettes, L.S.; Bailey, J.J.; Childers, R.; Deal, B.J.; Gorgels, A.; Hancock, E.W.; Josephson, M.; Kligfield, P.; et al. AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram: Part IV: The ST segment, T and U waves, and the QT interval: A scientific statement from the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society: Endorsed by the International Society for Computerized Electrocardiology. Circulation 2009, 119, e241–e250. [Google Scholar] [PubMed]
- Muhlestein, J.B.; Le, V.; Albert, D.; Moreno, F.L.; Anderson, J.L.; Yanowitz, F.; Vranian, R.B.; Barsness, G.W.; Bethea, C.F.; Severance, H.W.; et al. Smartphone ECG for evaluation of STEMI: Results of the ST LEUIS Pilot Study. J. Electrocardiol. 2015, 48, 249–259. [Google Scholar] [CrossRef] [PubMed]
- Nigolian, A.; Dayal, N.; Nigolian, H.; Stettler, C.; Burri, H. Diagnostic accuracy of multi-lead ECGs obtained using a pocket-sized bipolar handheld event recorder. J. Electrocardiol. 2018, 51, 278–281. [Google Scholar] [CrossRef] [PubMed]
- AlGhatrif, M.; Lindsay, J. A brief review: History to understand fundamentals of electrocardiography. J. Community Hosp. Intern. Med. Perspect. 2012, 2, 14383. [Google Scholar] [CrossRef]
- Frisch, D.R. A Novel Technique to Expand the Electrocardiographic Recording Capability from an Apple Watch. Am. J. Med. 2019, 132, 940–941. [Google Scholar] [CrossRef]
- Ahmed, A.S.; Golden, K.M.; Foreman, J.R.; Padanilam, B.J. Using a smartwatch to identify the morphology of atrial flutter. HeartRhythm Case Rep. 2020, in press. [Google Scholar] [CrossRef]
- Drexler, M.; Elsner, C.; Gabelmann, V.; Gori, T.; Münzel, T. Apple Watch detecting coronary ischaemia during chest pain episodes or an apple a day may keep myocardial infarction away. Eur. Heart J. 2020, 41, 2224. [Google Scholar] [CrossRef] [PubMed]
- Rajakariar, K.; Koshy, A.N.; Sajeev, J.K.; Nair, S.; Roberts, L.; Teh, A.W. Modified positioning of a smartphone based single-lead electrocardiogram device improves detection of atrial flutter. J. Electrocardiol. 2018, 51, 884–888. [Google Scholar] [CrossRef] [PubMed]
- Dasari, T.W.; Roe, M.T.; Chen, A.Y.; Peterson, E.D.; Giugliano, R.P.; Fonarow, G.C.; Saucedo, J.F. Impact of time of presentation on process performance and outcomes in ST-segment-elevation myocardial infarction: A report from the American Heart Association: Mission Lifeline program. Circ. Cardiovasc. Qual. Outcomes 2014, 7, 656–663. [Google Scholar] [CrossRef] [PubMed]
- Foo, C.Y.; Bonsu, K.O.; Nallamothu, B.K.; Reid, C.M.; Dhippayom, T.; Reidpath, D.D.; Chaiyakunapruk, N. Coronary intervention door-to-balloon time and outcomes in ST-elevation myocardial infarction: A meta-analysis. Heart Br. Cardiac. Soc. 2018, 104, 1362–1369. [Google Scholar] [CrossRef] [PubMed]
- Strik, M.; Caillol, T.; Ramirez, F.D.; Abu-Alrub, S.; Marchand, H.; Welte, N.; Ritter, P.; Haïssaguerre, M.; Ploux, S.; Bordachar, P. Validating QT-Interval Measurement Using the Apple Watch ECG to Enable Remote Monitoring During the COVID-19 Pandemic. Circulation 2020, 142, 416–418. [Google Scholar] [CrossRef] [PubMed]
- Bailey, J.J.; Berson, A.S.; Garson, A., Jr.; Horan, L.G.; Macfarlane, P.W.; Mortara, D.W.; Zywietz, C. Recommendations for standardization and specifications in automated electrocardiography: Bandwidth and digital signal processing. A report for health professionals by an ad hoc writing group of the Committee on Electrocardiography and Cardiac Electrophysiology of the Council on Clinical Cardiology, American Heart Association. Circulation 1990, 81, 730–739. [Google Scholar] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables, Units | n (%) |
|---|---|
| Age (year), mean ± SD | 63.66 ± 14.00 |
| Gender (male/female), n | 62/38 |
| Body mass index (kg/m2), mean ± SD | 28.44 ± 4.77 |
| Ischemic heart disease | 41 (41) |
| Hypertension | 88 (88) |
| Diabetes | 31 (31) |
| Prior stroke | 10 (10) |
| Renal failure | 31 (31) |
| Chronic obstructive pulmonary disease | 10 (10) |
| Beta-blocker | 82 (82) |
| Digoxin | 3 (3) |
| Amiodarone | 16 (16) |
| Diuretic | 55 (55) |
| Angiotensin receptor blocker (ARB) | 31 (31) |
| Angiotensin-converting enzyme (ACE)-inhibitor | 39 (39) |
| Antiplatelet drug | 33 (33) |
| Anticoagulant | 62 (62) |
| Variables, Units | Lead | Standard ECG | Smartwatch ECG | Correlation Coefficient | p-Value | Bias * (95% LoA) | |
|---|---|---|---|---|---|---|---|
| Duration (millisecond), mean ± SD | P Wave | I | 76.79 ± 11.69 | 76.54 ± 11.58 | 0.94 | 0.001 | 0.25 (−7.44 to +7.94) |
| II | 77.27 ± 13.15 | 77.89 ± 13.15 | 0.94 | 0.001 | −0.62 (−9.82 to +8.58) | ||
| III | 77.39 ± 14.66 | 78.64 ± 13.91 | 0.96 | 0.001 | −0.01 (−7.28 to +7.26) | ||
| PR Interval | I | 172.21 ± 24.55 | 171.36 ± 24.69 | 0.98 | 0.001 | 0.85 (−8.01 to +9.71) | |
| II | 173.73 ± 29.99 | 172.69 ± 29.17 | 0.97 | 0.001 | 1.04 (−11.55 to +13.63) | ||
| III | 172.07 ± 28.26 | 172.65 ± 27.62 | 0.96 | 0.001 | −0.68 (−16.32 to +14.95) | ||
| QRS Complex | I | 87.44 ± 11.70 | 87.67 ± 11.18 | 0.94 | 0.001 | −0.23 (−7.86 to +7.39) | |
| II | 88.84 ± 10.73 | 89.01 ± 10.46 | 0.93 | 0.001 | −0.17 (−8.18 to +7.84) | ||
| III | 87.08 ± 14.54 | 87.23 ± 14.00 | 0.95 | 0.001 | −0.14 (−9.30 to +9.01) | ||
| QT Interval | I | 369.66 ± 44.26 | 369.93 ± 44.36 | 0.99 | 0.001 | 0.04 (−11.05 to +11.13) | |
| II | 368.42 ± 42.19 | 367.44 ± 40.67 | 0.98 | 0.001 | 0.09 (−9.90 to +11.87) | ||
| III | 369.57 ± 42.36 | 369.22 ± 42.18 | 0.99 | 0.001 | 0.35 (−9.98 to +10.96) | ||
| T Wave | I | 132.41 ± 24.72 | 133.10 ± 24.81 | 0.97 | 0.001 | −0.32 (−12.53 to +11.88) | |
| II | 132.81 ± 24.43 | 133.13 ± 23.93 | 0.97 | 0.001 | −0.32 (−12.53 to +11.88) | ||
| III | 133.76 ± 24.15 | 133.82 ± 23.17 | 0.98 | 0.001 | −0.06 (−8.34 to +8.21) | ||
| Amplitude (millivolts), mean ± SD | P Wave | I | 0.20 ± 0.06 | 0.22 ± 0.07 | 0.78 | 0.001 | −0.01 (−0.10 to +0.07) |
| II | 0.23 ± 0.09 | 0.24 ± 0.95 | 0.89 | 0.001 | −0.01 (-0.09 to +0.08) | ||
| III | 0.21 ± 0.08 | 0.21 ± 0.08 | 0.83 | 0.001 | −0.01 (−0.09 to +0.09) | ||
| QRS Complex | I | 1.79 ± 0.68 | 1.84 ± 0.70 | 0.96 | 0.001 | −0.04 (−0.38 to +0.28) | |
| II | 1.97 ± 0.84 | 1.94 ± 0.78 | 0.89 | 0.001 | 0.02 (−0.73 to +0.78) | ||
| III | 1.94 ± 0.64 | 1.97 ± 0.65 | 0.90 | 0.001 | −0.02 (−0.60 to +0.55) | ||
| T Wave | I | 0.29 ± 0.15 | 0.32 ± 0.15 | 0.89 | 0.001 | −0.02 (−0.16 to +0.11) | |
| II | 0.32 ± 0.17 | 0.32 ± 0.15 | 0.82 | 0.001 | 0.00 (−0.19 to +0.20) | ||
| III | 0.28 ± 0.16 | 0.29 ± 0.18 | 0.72 | 0.001 | −0.01 (−0.27 to +0.23) | ||
| Variables, Units | Lead | Standard ECG | Smartwatch ECG | Concordance (%) | p-Value | |
|---|---|---|---|---|---|---|
| Polarity (Positive/Negative), n | P Wave | I | 100/0 | 100/0 | 100% | - |
| II | 99/1 | 99/1 | 100% | 0.001 | ||
| III | 93/7 | 94/6 | 99% | 0.001 | ||
| QRS Complex | I | 94/6 | 94/6 | 100% | 0.001 | |
| II | 88/12 | 87/13 | 99% | 0.001 | ||
| III | 54/46 | 53/47 | 99% | 0.001 | ||
| T Wave | I | 82/18 | 81/19 | 99% | 0.001 | |
| II | 83/17 | 84/16 | 99% | 0.001 | ||
| III | 70/30 | 72/28 | 98% | 0.001 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Behzadi, A.; Sepehri Shamloo, A.; Mouratis, K.; Hindricks, G.; Arya, A.; Bollmann, A. Feasibility and Reliability of SmartWatch to Obtain 3-Lead Electrocardiogram Recordings. Sensors 2020, 20, 5074. https://doi.org/10.3390/s20185074
Behzadi A, Sepehri Shamloo A, Mouratis K, Hindricks G, Arya A, Bollmann A. Feasibility and Reliability of SmartWatch to Obtain 3-Lead Electrocardiogram Recordings. Sensors. 2020; 20(18):5074. https://doi.org/10.3390/s20185074
Chicago/Turabian StyleBehzadi, Amirali, Alireza Sepehri Shamloo, Konstantinos Mouratis, Gerhard Hindricks, Arash Arya, and Andreas Bollmann. 2020. "Feasibility and Reliability of SmartWatch to Obtain 3-Lead Electrocardiogram Recordings" Sensors 20, no. 18: 5074. https://doi.org/10.3390/s20185074
APA StyleBehzadi, A., Sepehri Shamloo, A., Mouratis, K., Hindricks, G., Arya, A., & Bollmann, A. (2020). Feasibility and Reliability of SmartWatch to Obtain 3-Lead Electrocardiogram Recordings. Sensors, 20(18), 5074. https://doi.org/10.3390/s20185074