Evaluation of the Validity, Reliability, and Kinematic Characteristics of Multi-Segment Foot Models in Motion Capture

 , ,
, ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
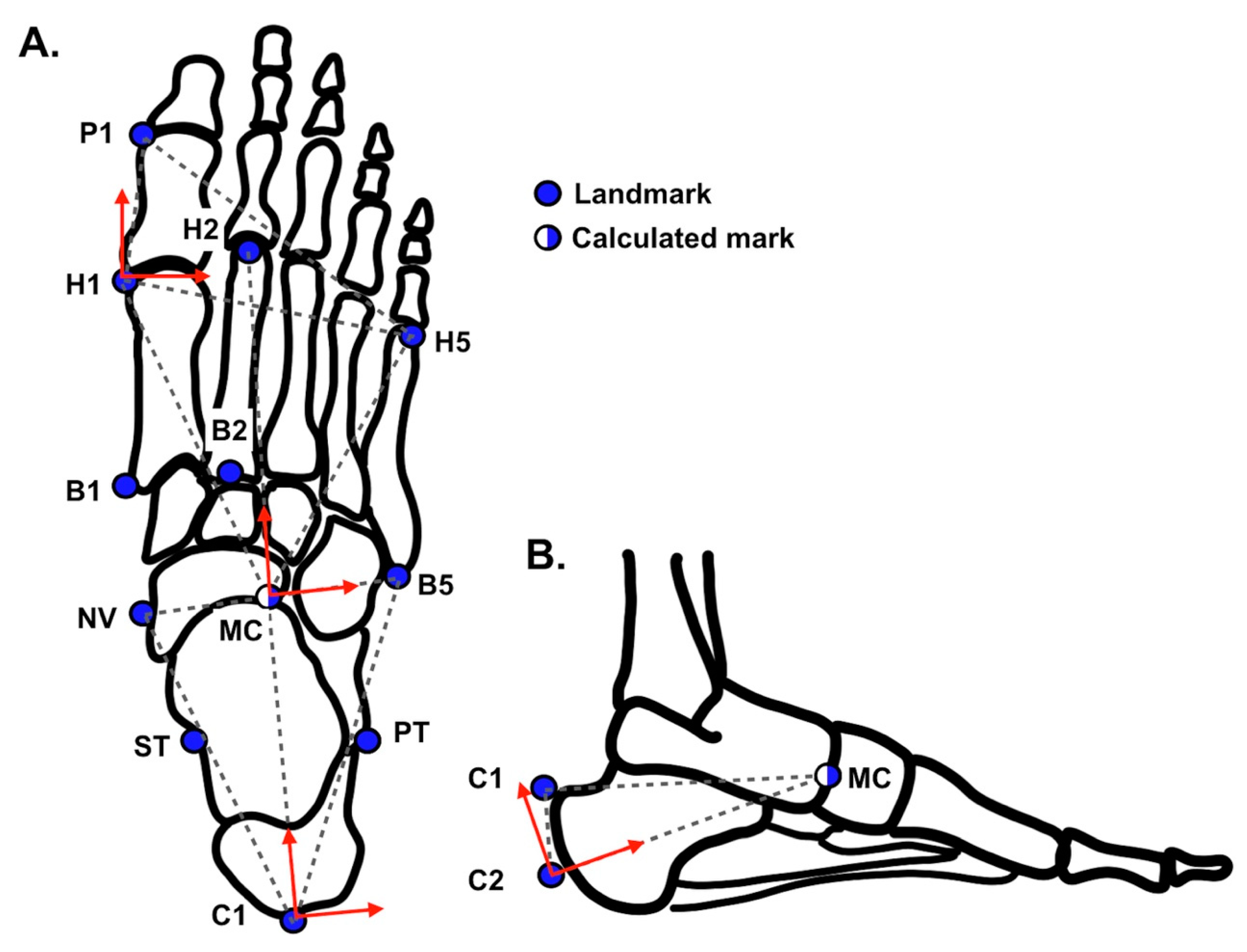
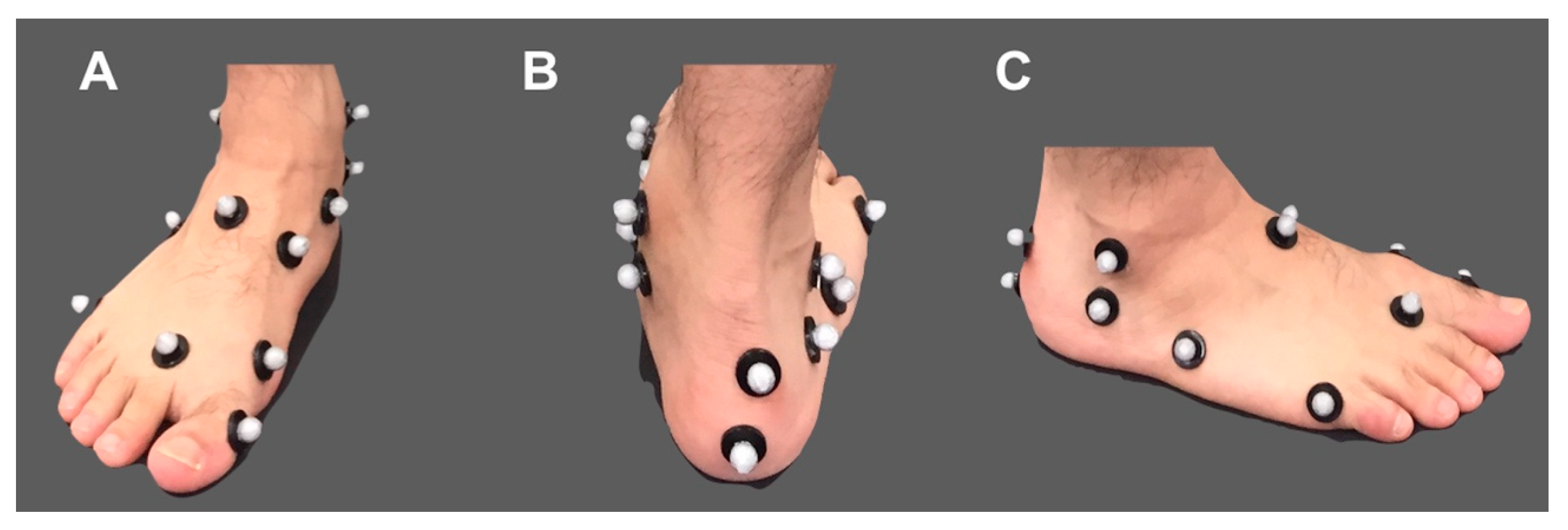
2.1. Multi-Segment Foot Model
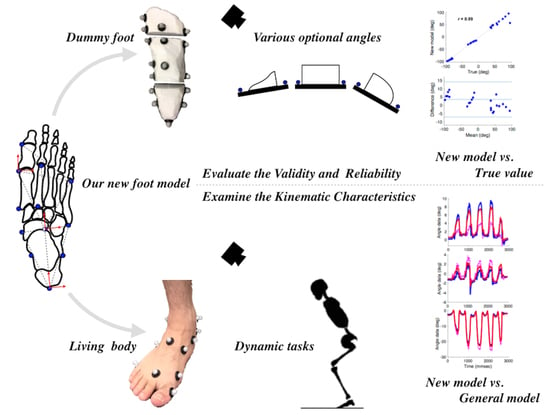
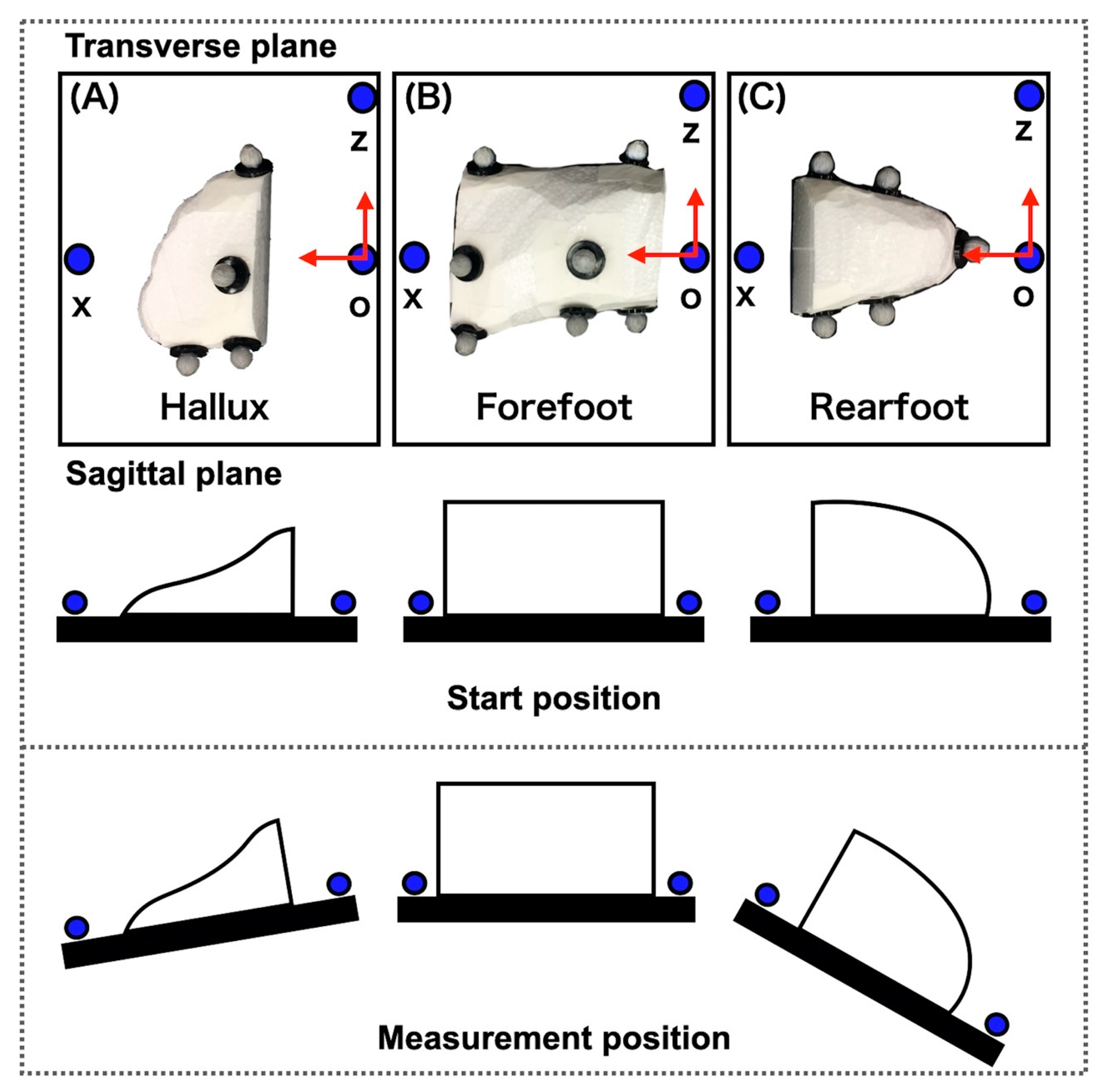
2.2. Dummy Foot
2.3. Participants
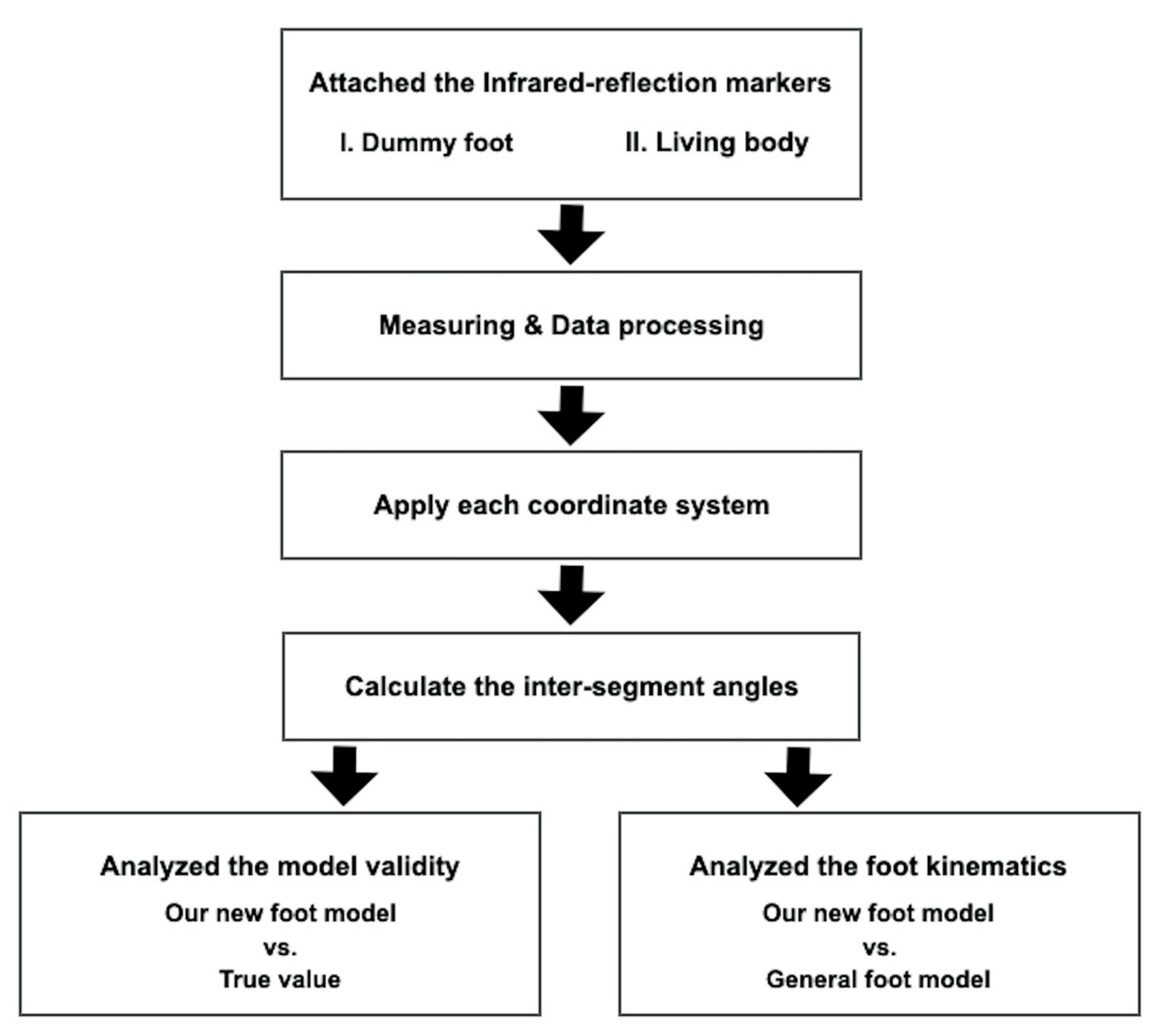
2.4. Experimental Protocol of Dummy Foot
2.5. Experimental Protocol of Living Body
2.6. Data Collecting
2.7. Data Analysis
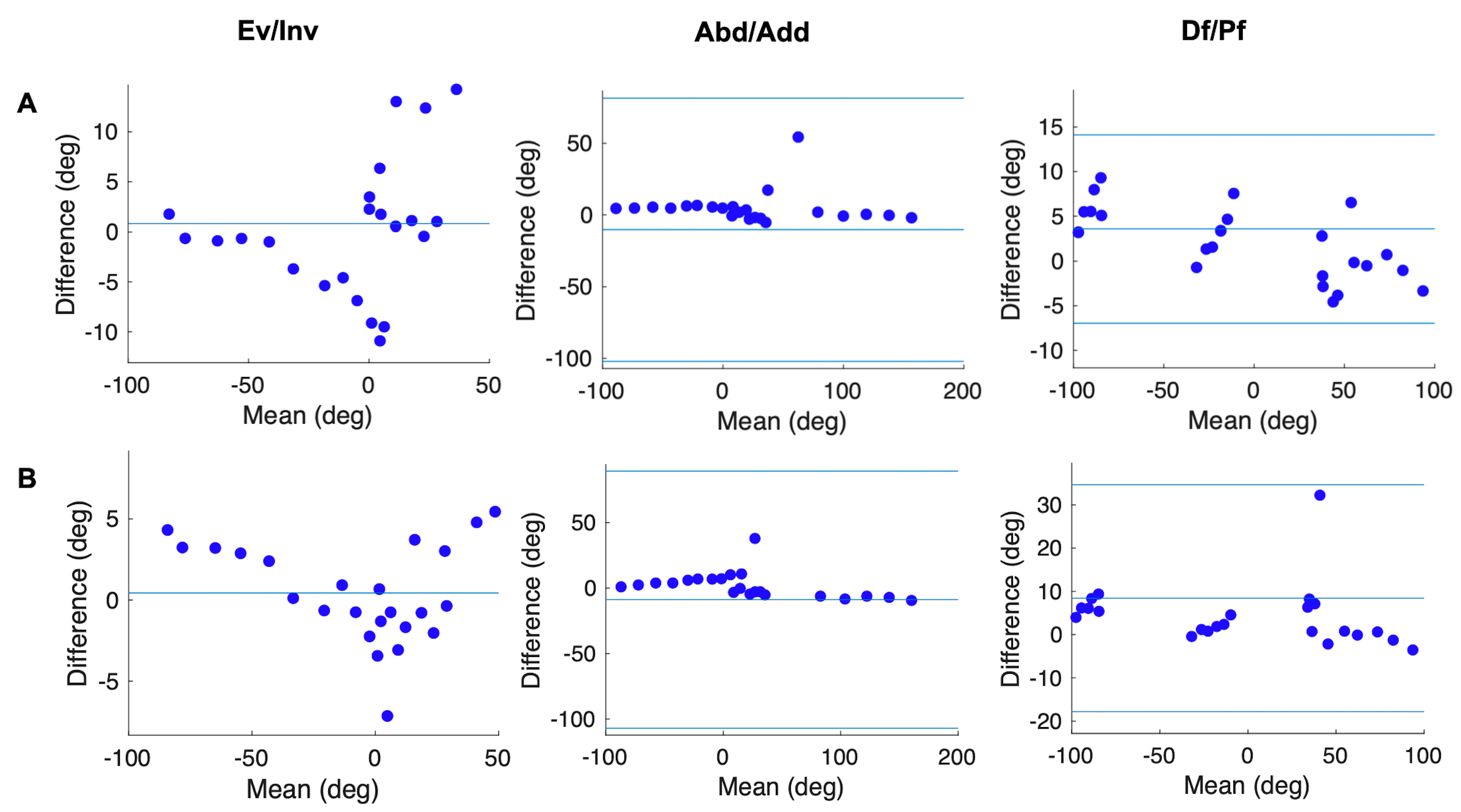
2.8. Statistical Analysis
3. Results
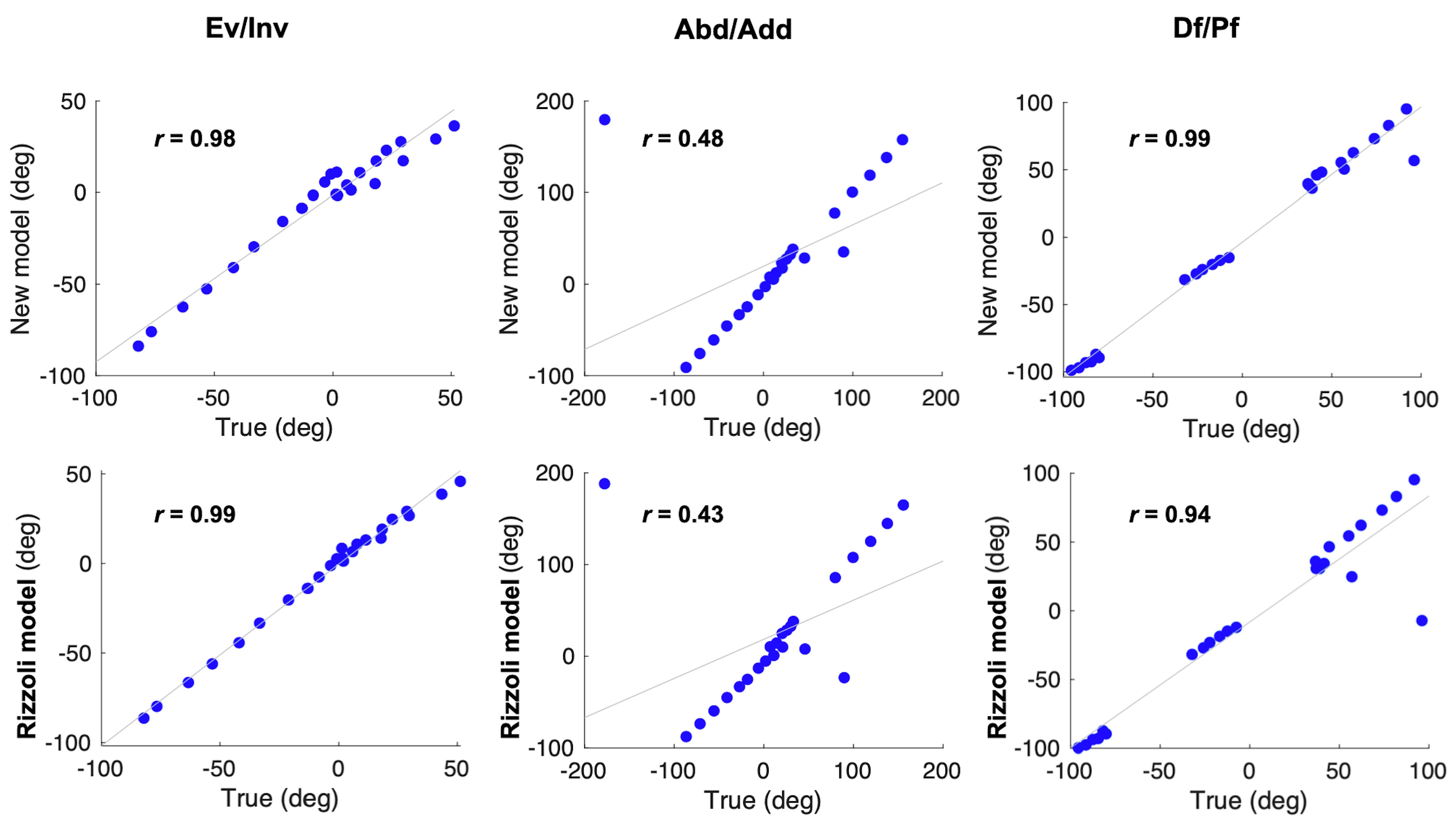
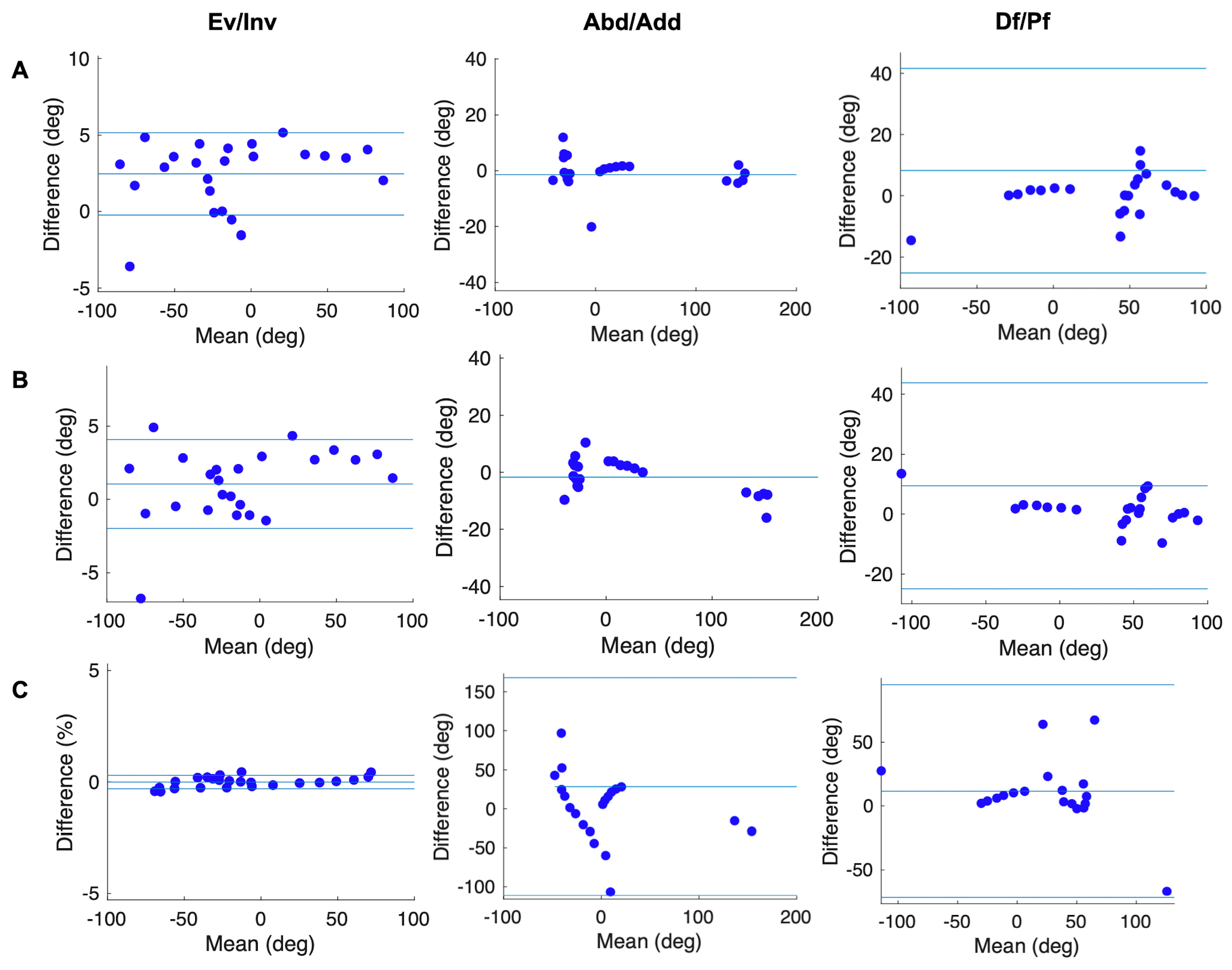
3.1. Experiment of Dummy Foot
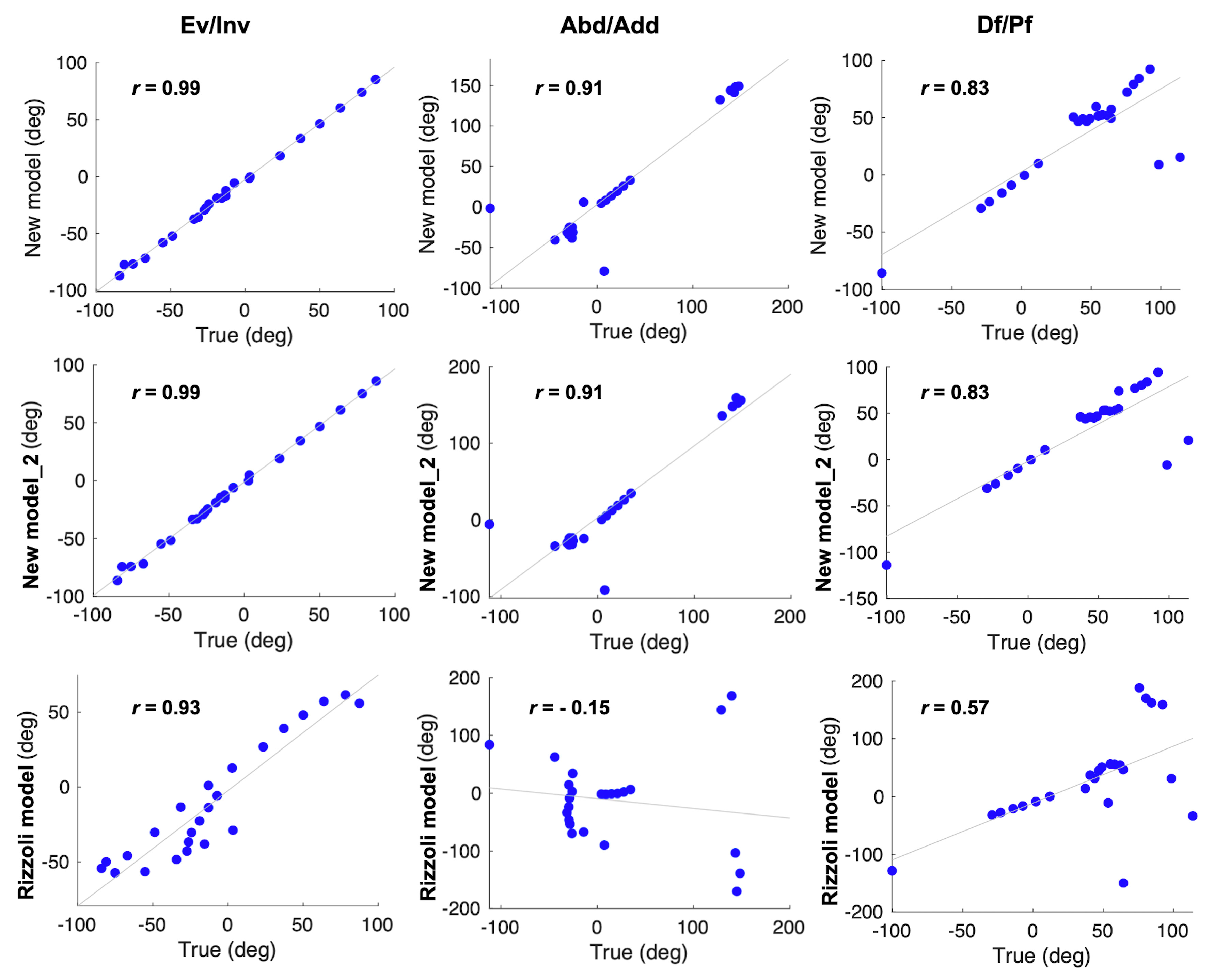
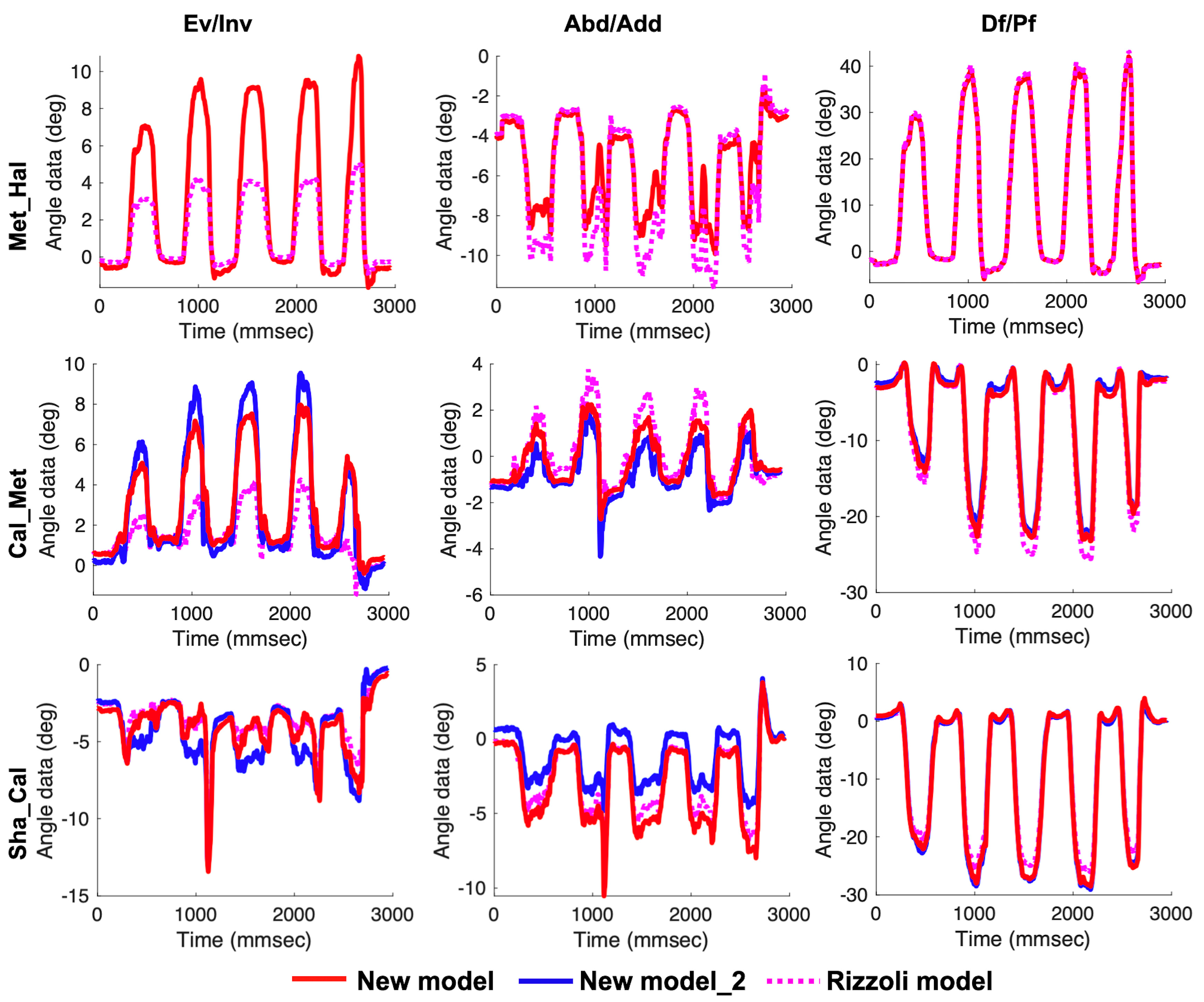
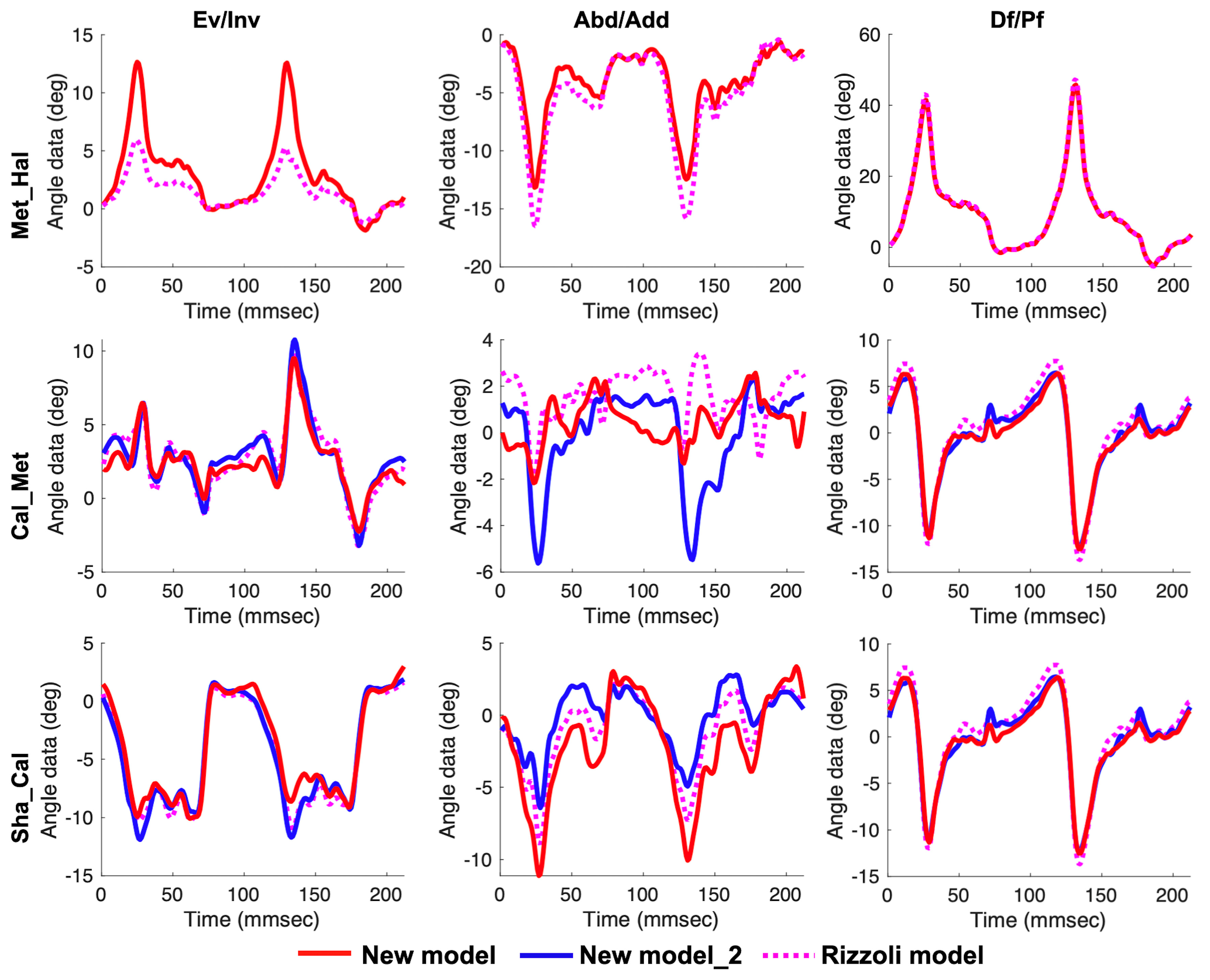
3.2. In Vivo Experiment
4. Discussion
4.1. Validity of Our New Multi-Segment Foot Model
4.2. Characteristics of Our New Multi-Segment Foot Model in Measuring Dynamic Tasks
4.3. Methodological Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Leardini, A.; Benedetti, M.G.; Berti, L.; Bettinelli, D.; Nativo, R.; Giannini, S. Rear-foot, mid-foot and fore-foot motion during the stance phase of gait. Gait Posture 2007, 25, 453–462. [Google Scholar] [CrossRef]
- Portinaro, N.; Leardini, A.; Panou, A.; Monzani, V.; Caravaggi, P. Modifying the Rizzoli foot model to improve the diagnosis of pes-planus: Application to kinematics of feet in teenagers. J. Foot Ankle Res. 2014, 7, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Elftman, H. The transverse tarsal joint and its control. Clin. Orthop. 1960, 16, 41–46. [Google Scholar]
- Kadaba, M.P.; Ramakrishnan, H.K.; Wootten, M.E. Measurement of lower extremity kinematics during level walking. J. Orthop. Res. 1990, 8, 383–392. [Google Scholar] [CrossRef] [PubMed]
- Pothrat, C.; Authier, G.; Viehweger, E.; Berton, E.; Rao, G. One- and multi-segment foot models lead to opposite results on ankle joint kinematics during gait: Implications for clinical assessment. Clin. Biomech. 2015. [Google Scholar] [CrossRef] [PubMed]
- Carson, M.C.; Harrington, M.E.; Thompson, N.; O’Connor, J.J.; Theologis, T.N. Kinematic analysis of a multi-segment foot model for research and clinical applications: A repeatability analysis. J. Biomech. 2001, 34, 1299–1307. [Google Scholar] [CrossRef]
- Simon, J.; Doederlein, L.; McIntosh, A.S.; Metaxiotis, D.; Bock, H.G.; Wolf, S.I. The Heidelberg foot measurement method: Development, description and assessment. Gait Posture 2006, 23, 411–424. [Google Scholar] [CrossRef] [PubMed]
- Stebbins, J.; Harrington, M.; Thompson, N.; Zavatsky, A.; Theologis, T. Repeatability of a model for measuring multi-segment foot kinematics in children. Gait Posture 2006, 23, 401–410. [Google Scholar] [CrossRef]
- Caravaggi, P.; Benedetti, M.G.; Berti, L.; Leardini, A. Repeatability of a multi-segment foot protocol in adult subjects. Gait Posture 2011, 33, 133–135. [Google Scholar] [CrossRef]
- Deschamps, K.; Staes, F.; Bruyninckx, H.; Busschots, E.; Jaspers, E.; Atre, A.; Desloovere, K. Repeatability in the assessment of multi-segment foot kinematics. Gait Posture 2012, 35, 255–260. [Google Scholar] [CrossRef]
- Maurer, J.D.; Ward, V.; Mayson, T.A.; Davies, K.R.; Alvarez, C.M.; Beauchamp, R.D.; Black, A.H. A kinematic description of dynamic midfoot break in children using a multi-segment foot model. Gait Posture 2013, 38, 287–292. [Google Scholar] [CrossRef] [PubMed]
- Maurer, J.D.; Ward, V.; Mayson, T.A.; Davies, K.R.; Alvarez, C.M.; Beauchamp, R.D.; Black, A.H. Classification of midfoot break using multi-segment foot kinematics and pedobarography. Gait Posture 2014, 39, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Kerr, C.M.; Stebbins, J.; Theologis, T.; Zavatsky, A.B. Static postural differences between neutral and flat feet in children with and without symptoms. Clin. Biomech. 2015, 30, 314–317. [Google Scholar] [CrossRef]
- Okamura, K.; Kanai, S.; Fukuda, K.; Tanaka, S.; Ono, T.; Oki, S. The effect of additional activation of the plantar intrinsic foot muscles on foot kinematics in flat-footed subjects. Foot 2019, 38, 19–23. [Google Scholar] [CrossRef] [PubMed]
- Deschamps, K.; Birch, I.; Desloovere, K.; Matricali, G.A. The impact of hallux valgus on foot kinematics: A cross-sectional, comparative study. Gait Posture 2010, 32, 102–106. [Google Scholar] [CrossRef]
- Hastings, M.K.; Woodburn, J.; Mueller, M.J.; Strube, M.J.; Johnson, J.E.; Beckert, K.S.; Stein, M.L.; Sinacore, D.R. Radiographic-directed local coordinate systems critical in kinematic analysis of walking in diabetes-related medial column foot deformity. Gait Posture 2014, 40, 128–133. [Google Scholar] [CrossRef] [PubMed]
- Nester, C.; Jones, R.K.; Liu, A.; Howard, D.; Lundberg, A.; Arndt, A.; Lundgren, P.; Stacoff, A.; Wolf, P. Foot kinematics during walking measured using bone and surface mounted markers. J. Biomech. 2007, 40, 3412–3423. [Google Scholar] [CrossRef]
- Shultz, R.; Kedgley, A.E.; Jenkyn, T.R. Quantifying skin motion artifact error of the hindfoot and forefoot marker clusters with the optical tracking of a multi-segment foot model using single-plane fluoroscopy. Gait Posture 2011, 34, 44–48. [Google Scholar] [CrossRef]
- Bruening, D.A.; Cooney, K.M.; Buczek, F.L. Analysis of a kinetic multi-segment foot model. Part I: Model repeatability and kinematic validity. Gait Posture 2012, 35, 529–534. [Google Scholar] [CrossRef]
- Bruening, D.A.; Cooney, K.M.; Buczek, F.L. Analysis of a kinetic multi-segment foot model part II: Kinetics and clinical implications. Gait Posture 2012, 35, 535–540. [Google Scholar] [CrossRef]
- Kevin, D.; Maarten, E.; Dirk, D.; Matricali, G.A.; Wuite, S.; Filip, S. Estimation of foot joint kinetics in three and four segment foot models using an existing proportionality scheme: Application in paediatric barefoot walking. J. Biomech. 2017, 61, 168–175. [Google Scholar] [CrossRef]
- Magalhães, F.A.; Souza, T.R.; Araújo, V.L.; Oliveira, L.M.; de Silveira, L.P.; de Ocarino, J.M.; Fonseca, S.T. Comparison of the rigidity and forefoot—Rearfoot kinematics from three forefoot tracking marker clusters during walking and weight-bearing foot pronation-supination. J. Biomech. 2020, 98, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Brookshaw, M.; Sexton, A.; McGibbon, C.A. Reliability and validity of a novel wearable device for measuring elbow strength. Sensors 2020, 20, 3412. [Google Scholar] [CrossRef] [PubMed]
- Martin Bland, J.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 327, 307–310. [Google Scholar] [CrossRef]
- Ang, M.H.; Tourassis, V.D. Singularities of Euler and Roll-Pitch-Yaw Representations. IEEE Trans. Aerosp. Electron. Syst. 1987, AES-23, 317–324. [Google Scholar] [CrossRef]
- Siemens, M.; Hancock, J.; Siminovitch, D. Beyond Euler angles: Exploiting the angle-axis parametrization in a multipole expansion of the rotation operator. Solid State Nucl. Magn. Reson. 2007, 31, 35–54. [Google Scholar] [CrossRef]
- Deschamps, K.; Staes, F.; Peerlinck, K.; Van Geet, C.; Hermans, C.; Matricali, G.A.; Lobet, S. 3D Multi-segment foot kinematics in children: A developmental study in typically developing boys. Gait Posture 2017, 52, 40–44. [Google Scholar] [CrossRef]
- Kirby, K.A. Longitudinal arch load-sharing system of the foot. Rev. Esp. Podol. 2017, 28, e18–e26. [Google Scholar] [CrossRef]
- Hicks, J.H. The mechanics of the foot. II. The plantar aponeurosis and the arch. J. Anat. 1954, 88, 25–30. [Google Scholar]
- Peters, A.; Galna, B.; Sangeux, M.; Morris, M.; Baker, R. Quantification of soft tissue artifact in lower limb human motion analysis: A systematic review. Gait Posture 2010, 31, 1–8. [Google Scholar] [CrossRef]
- Stagni, R.; Fantozzi, S.; Cappello, A.; Leardini, A. Quantification of soft tissue artefact in motion analysis by combining 3D fluoroscopy and stereophotogrammetry: A study on two subjects. Clin. Biomech. 2005, 20, 320–329. [Google Scholar] [CrossRef] [PubMed]
- Leardini, A.; Chiari, A.; Della Croce, U.; Cappozzo, A. Human movement analysis using stereophotogrammetry Part 3. Soft tissue artifact assessment and compensation. Gait Posture 2005, 21, 212–225. [Google Scholar] [CrossRef]
- Powell, D.W.; Long, B.; Milner, C.E.; Zhang, S. Frontal plane multi-segment foot kinematics in high- and low-arched females during dynamic loading tasks. Hum. Mov. Sci. 2011, 30, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Takabayashi, T.; Edama, M.; Inai, T.; Kubo, M. Sex-related differences in coordination and variability among foot joints during running. J. Foot Ankle Res. 2018, 11. [Google Scholar] [CrossRef] [PubMed]
- Glowinski, S.; Łosiński, K.; Kowiański, P.; Waśkow, M.; Bryndal, A.; Grochulska, A. Inertial sensors as a tool for diagnosing discopathy lumbosacral pathologic gait: A preliminary research. Diagnostics 2020, 10, 342. [Google Scholar] [CrossRef] [PubMed]
- Hou, Y.R.; Chiu, Y.L.; Chiang, S.L.; Chen, H.Y.; Sung, W.H. Development of a smartphone-based balance assessment system for subjects with stroke. Sensors 2020, 20, 88. [Google Scholar] [CrossRef]
- Qiu, S.; Wang, H.; Li, J.; Zhao, H.; Wang, Z.; Wang, J.; Wang, Q.; Plettemeier, D.; Bärhold, M.; Bauer, T.; et al. Towards wearable-inertial-sensor-based gait posture evaluation for subjects with unbalanced gaits. Sensors 2020, 20, 1193. [Google Scholar] [CrossRef]
- Anwary, A.R.; Yu, H.; Vassallo, M. Optimal Foot Location for Placing Wearable IMU Sensors and Automatic Feature Extraction for Gait Analysis. IEEE Sens. J. 2018, 18, 2555–2567. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Name | Description | For the Rizzoli Model |
|---|---|---|
| P1 | Dorso-medial aspect of the first proximal phalanx head | PM |
| H1 | Dorso-medial aspect of the first metatarsal head | FMH |
| H2 | Dorso-medial aspect of the second metatarsal head | SMH |
| H5 | Dorso-lateral aspect of the fifth metatarsal head | VMH |
| B1 | Dorso-medial aspect of the first metatarsal base | FMB |
| B2 | Dorso-medial aspect of the second metatarsal base | SMB |
| B5 | Dorso-lateral aspect of the fifth metatarsal base | VMB |
| NV | Most medial apex of the navicular bone | TN |
| ST | Most medial apex of the sustentaculum tali | ST |
| PT | Lateral apex of the peroneal tubercle | PT |
| C1 | Superior apex of calcaneus | CA (FCP) |
| C2 | Apex of calcaneal tuberosity | HL (FCD) |
| LM | Distal apex of the lateral malleolus | LM |
| MM | Distal apex of the medial malleolus | MM |
| TT | Most anterior prominence of the tibial tuberosity | TT |
| HF | Most proximal apex of the head of the fibula | HF |
| MC | Midpoint between NV and B5 | ID |
| IM | Midpoint between MM and LM | IM |
| Segment | Long Axis | Plane |
|---|---|---|
| Hallux | H1 to P1 | H1, P1, H5 (Transverse) |
| Forefoot | MC to H2 | MC, H1, H5 (Transverse) |
| Rearfoot | C1 to MC | C1, NV, B5 (Transverse) |
| Rearfoot_2 | C2 to MC | C2, MC, C1 (Sagittal) |
| Shank | IM to TT | IM, LM, HF (Frontal) |
| Angle Name | Definition |
|---|---|
| Met_Hal | Hallux relative to forefoot |
| Cal_Met | Forefoot relative to rearfoot |
| Cal_Met_2 | Forefoot relative to rearfoot_2 |
| Sha_Cal | Rearfoot relative to shank |
| Sha_Cal_2 | Rearfoot_2 relative to shank |
| Calf Raise/Maximum (SD 1), Minimum (SD) | Drop Jump/Maximum (SD), Minimum (SD) | |||||
|---|---|---|---|---|---|---|
| Ev/Inv | Abd/Add | Df/Pf | Ev/Inv | Abd/Add | Df/Pf | |
| Met_Hal | 7.5 (1.9) *, −1.3 (0.8) | 3.1 (3.1), −8.4 (4.2) | 37.6 (7.7), −6.5 (4.0) | 5.5 (1.8) *, −1.6 (0.6) | 6.1 (2.5), −4.4 (2.6) | 26.6 (4.9), −6.9 (3.9) |
| Cal_Met | 6.2 (3.0), −2.3 (2.3) | 3.6 (2.2), −3.0 (1.8) | 2.5 (1.4), −16.8 (6.0) | 4.1 (2.1), −7.1 (2.5) | 2.8 (1.4), −3.7 (1.5) * | 11.1 (1.9) *, −17.5 (5.1) * |
| Cal_Met_2 | 6.0 (3.0), −3.9 (3.1) | 2.4 (1.8), −6.7 (6.3) | 2.2 (1.3), −17.2 (5.4) | 4.6 (2.8), −9.8 (4.6) | 4.0 (2.5), −7.6 (2.3) * | 12.4 (3.3) *, −17.9 (4.2) * |
| Sha_Cal | 1.4 (1.8) *, −11.6 (5.2) * | 2.0 (1.7), −14.6 (5.9) | 6.1 (2.6) *, −35.9 (6.9) * | 2.7 (2.3) *, −10.7 (3.3) | 7.1 (2.4), −12.1 (3.7) | 27.6 (5.4), −36.5 (5.8) |
| Sha_Cal_2 | 1.3 (1.3), −12.6 (5.4) | 2.4 (1.3), −8.9 (4.4) | 6.5 (3.1), −32.7 (6.5) | 5.3 (3.6), −11.4 (3.5) | 7.3 (2.3), −8.6 (3.8) | 26.1 (5.2), −35.6 (7.0) |
| Calf Raise/Maximum (SD 1), Minimum (SD) | Drop Jump/Maximum (SD), Minimum (SD) | |||||
|---|---|---|---|---|---|---|
| Ev/Inv | Abd/Add | Df/Pf | Ev/Inv | Abd/Add | Df/Pf | |
| Met_Hal | 3.7 (1.5), −1.1 (0.8) | 3.6 (4.2), −9.3 (5.1) | 38.4 (7.7), −6.6 (4.0) | 2.8 (1.1), −1.4 (0.69) | 6.4 (2.5), −5.2 (2.8) | 27.1 (5.0), −6.9 (3.9) |
| Cal_Met | 5.1 (3.8), −3.6 (3.6) | 2.9 (2.5), −4.4 (2.7) | 3.1 (1.7), −21.2 (7.1) | 4.7 (2.5), −8.2 (4.1) | 3.7 (3.1), −10.6 (5.2) | 15.0 (4.1), −24.4 (6.9) |
| Sha_Cal | 1.6 (2.2), −9.3 (4.1) | 1.9 (1.5), −11.6 (5.3) | 5.6 (2.4), −30.1 (6.2) | 5.7 (4.1), −10.3 (3.4) | 7.2 (2.4), −10.7 (4.1) | 25.7 (5.3), −32.8 (7.9) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sekiguchi, Y.; Kokubun, T.; Hanawa, H.; Shono, H.; Tsuruta, A.; Kanemura, N. Evaluation of the Validity, Reliability, and Kinematic Characteristics of Multi-Segment Foot Models in Motion Capture. Sensors 2020, 20, 4415. https://doi.org/10.3390/s20164415
Sekiguchi Y, Kokubun T, Hanawa H, Shono H, Tsuruta A, Kanemura N. Evaluation of the Validity, Reliability, and Kinematic Characteristics of Multi-Segment Foot Models in Motion Capture. Sensors. 2020; 20(16):4415. https://doi.org/10.3390/s20164415
Chicago/Turabian StyleSekiguchi, Yuka, Takanori Kokubun, Hiroki Hanawa, Hitomi Shono, Ayumi Tsuruta, and Naohiko Kanemura. 2020. "Evaluation of the Validity, Reliability, and Kinematic Characteristics of Multi-Segment Foot Models in Motion Capture" Sensors 20, no. 16: 4415. https://doi.org/10.3390/s20164415
APA StyleSekiguchi, Y., Kokubun, T., Hanawa, H., Shono, H., Tsuruta, A., & Kanemura, N. (2020). Evaluation of the Validity, Reliability, and Kinematic Characteristics of Multi-Segment Foot Models in Motion Capture. Sensors, 20(16), 4415. https://doi.org/10.3390/s20164415