Evaluation of Vertical Ground Reaction Forces Pattern Visualization in Neurodegenerative Diseases Identification Using Deep Learning and Recurrence Plot Image Feature Extraction



Abstract
1. Introduction
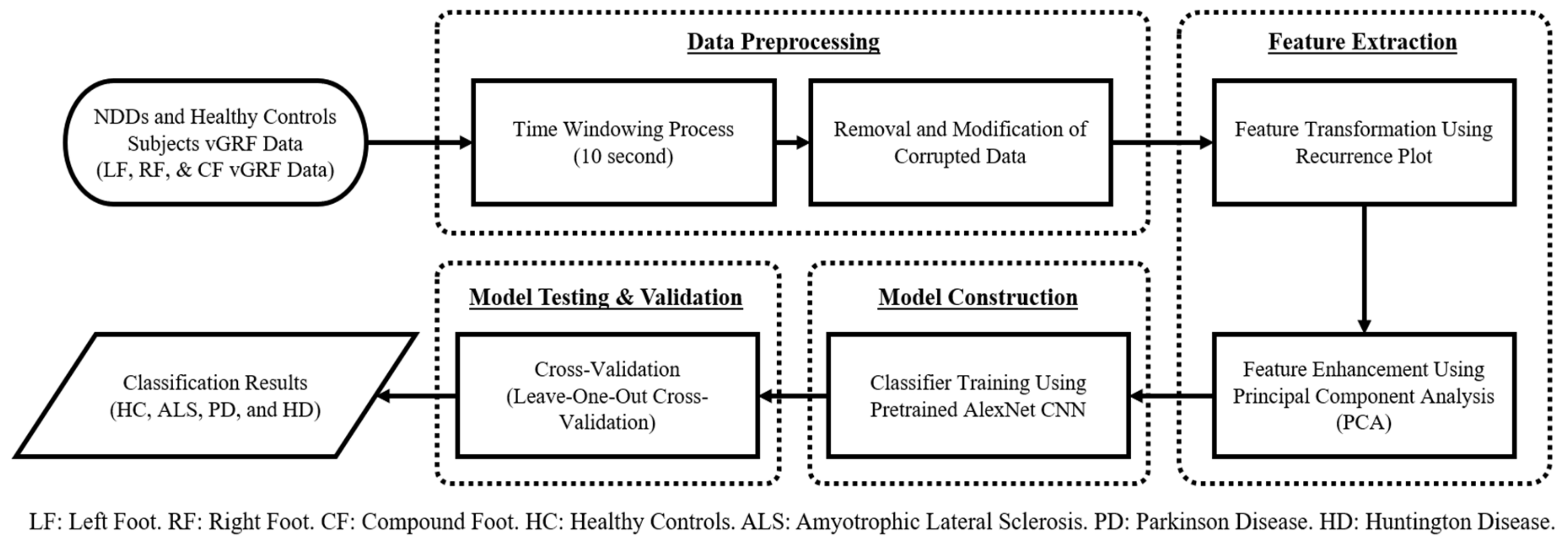
2. Materials and Methods
2.1. Neurodegenerative Diseases Gait Dynamics Database
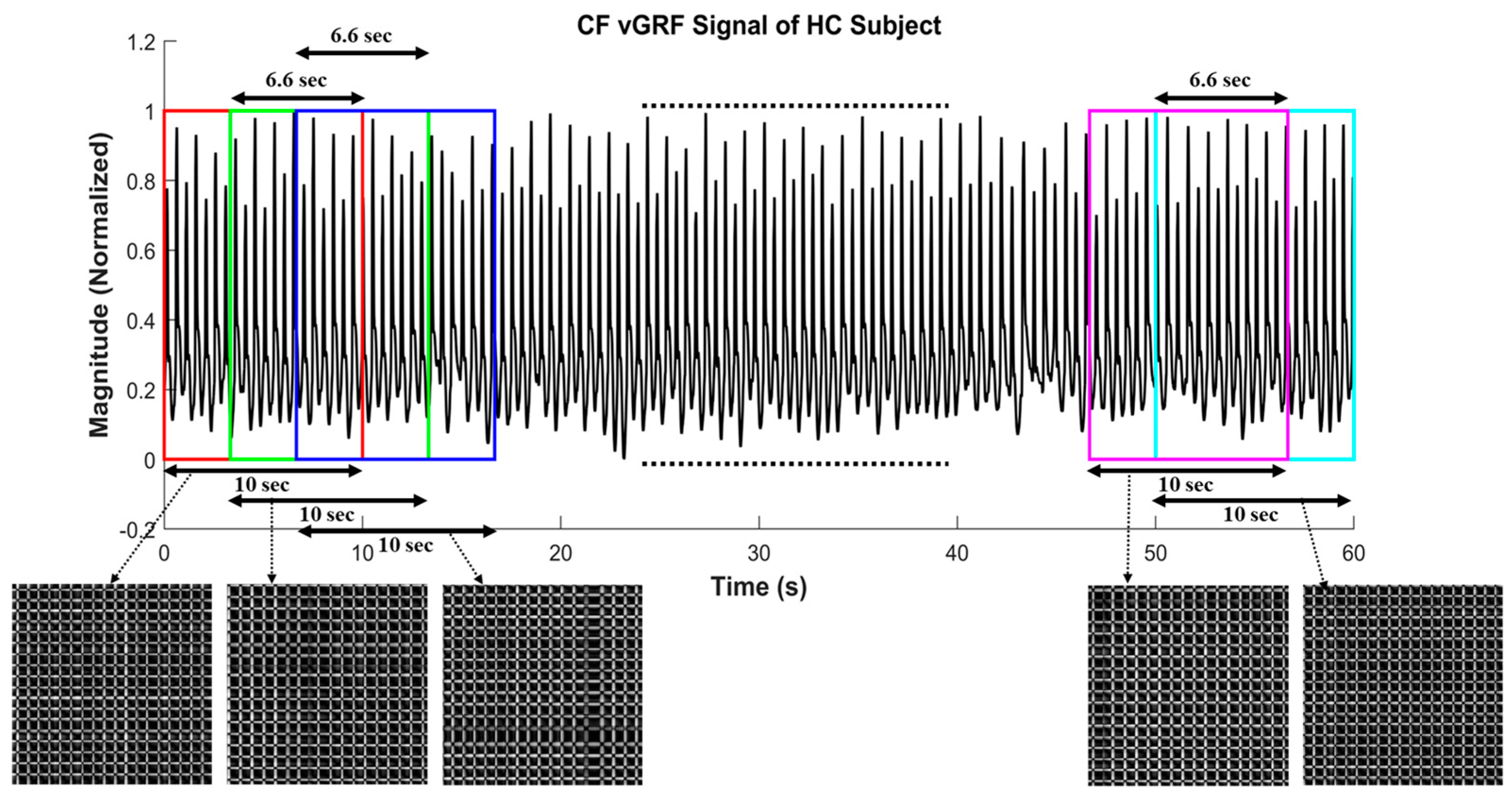
2.2. Data Preprocessing
Time-Windowing Process (10-s Window Length)
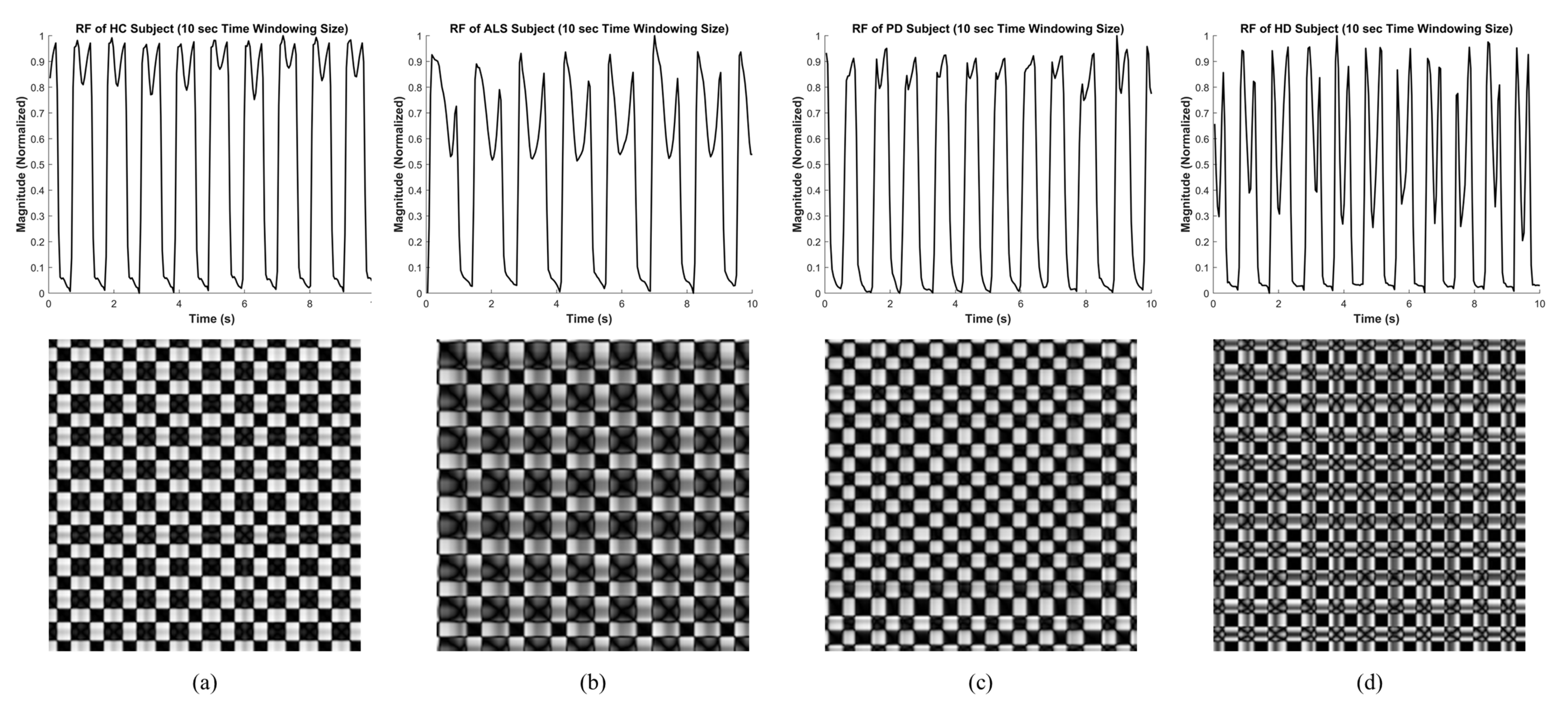
2.3. Recurrence Plot
2.4. Principal Component Analysis
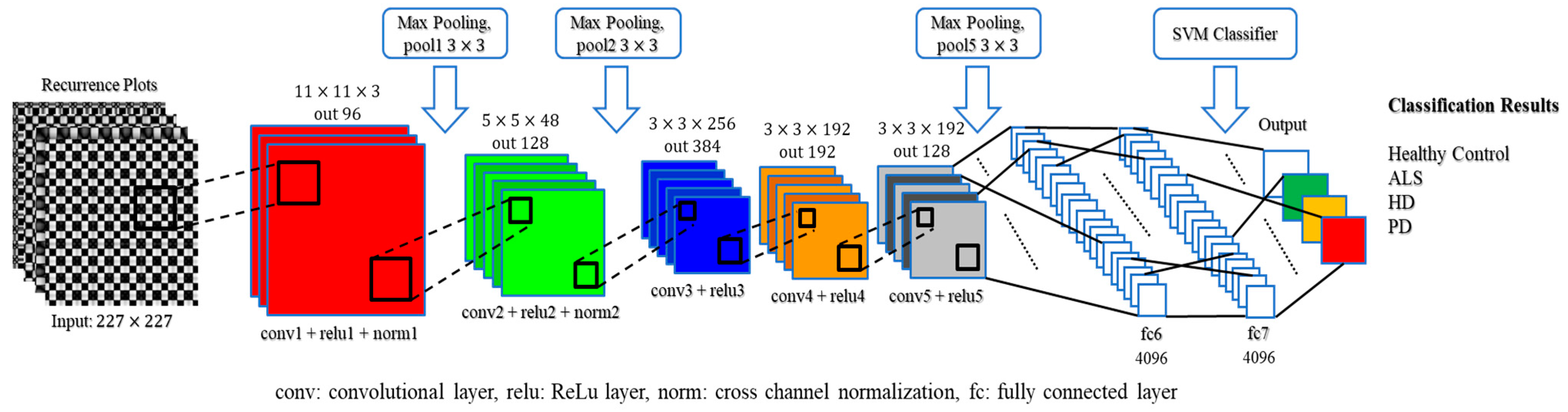
2.5. Convolutional Neural Network
2.6. Cross-Validation
3. Experimental Results
3.1. Two-Class Classification
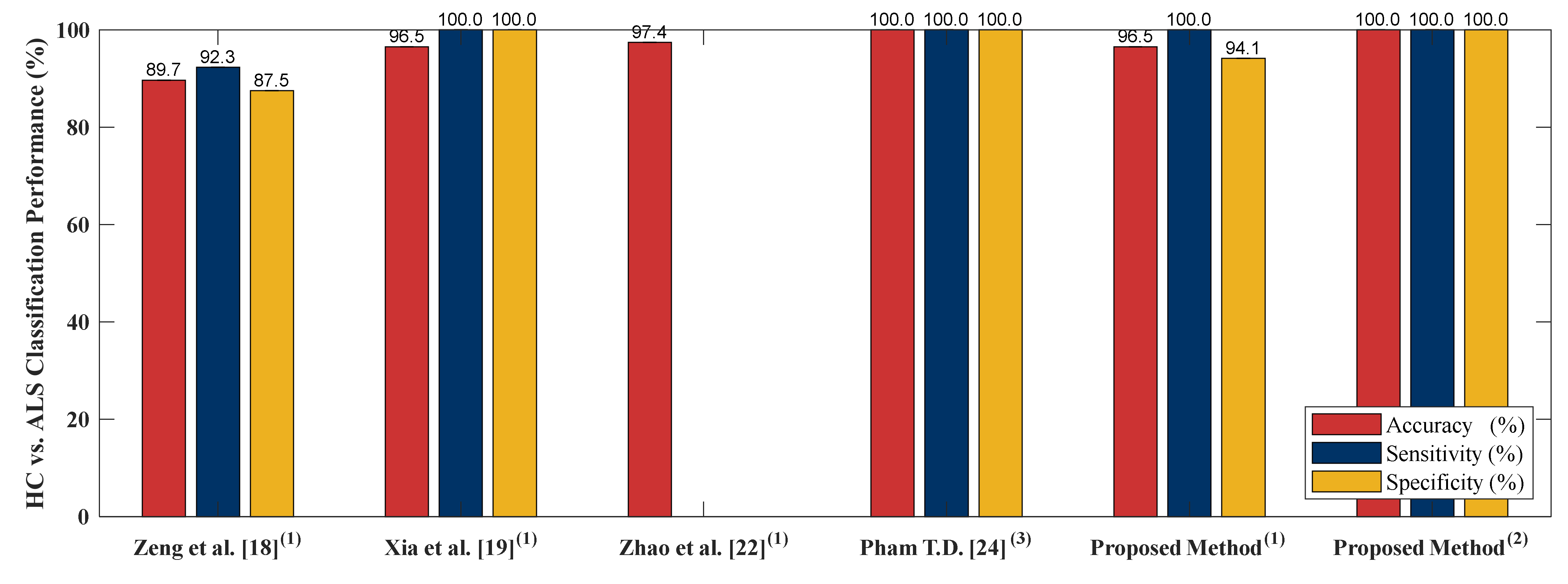
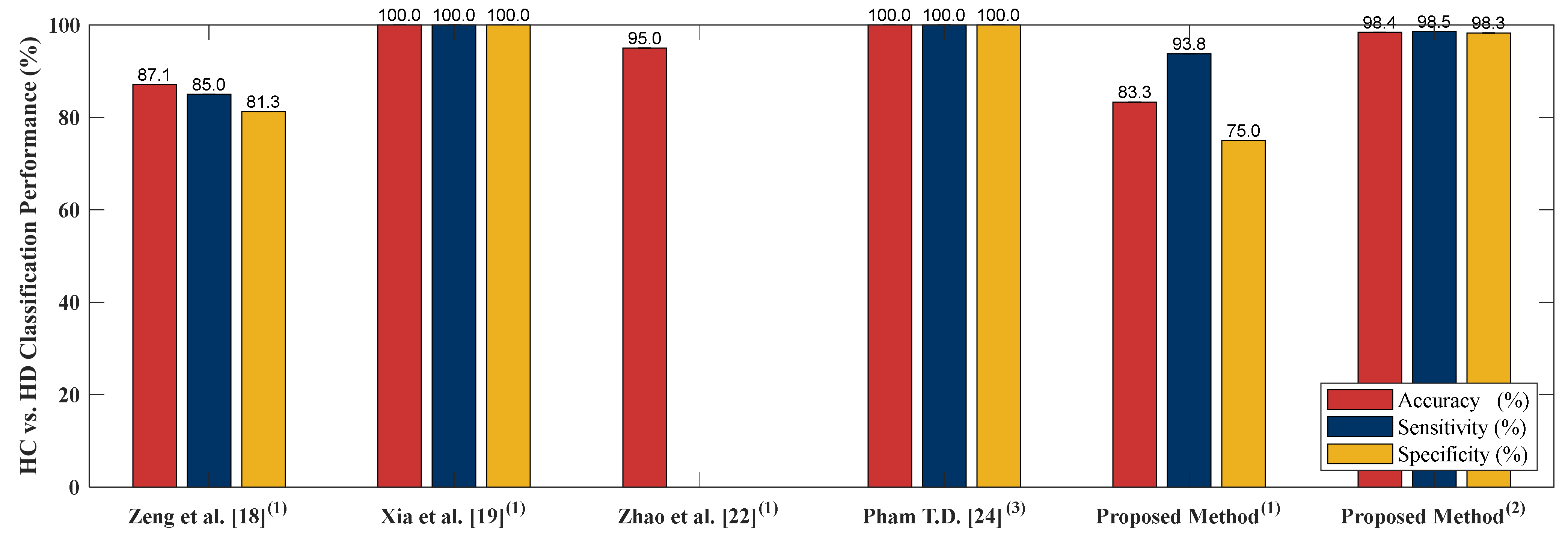
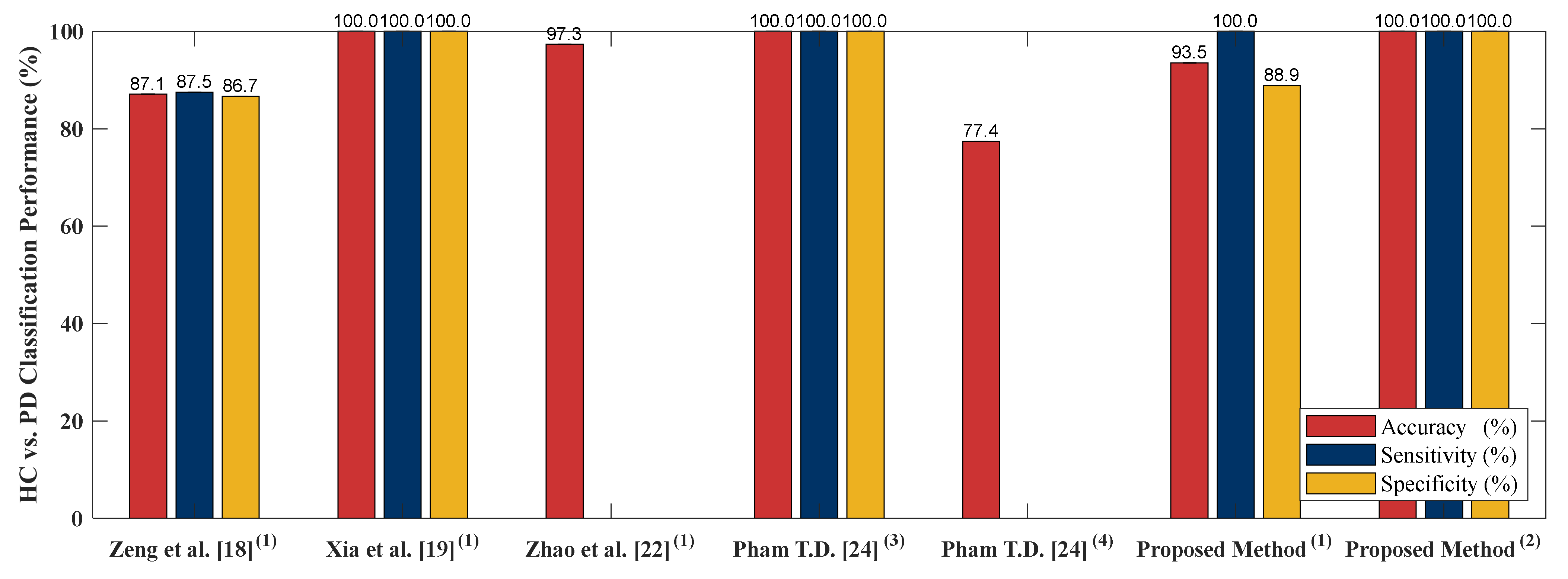
3.1.1. Classification of the NDD and Healthy Controls Group
3.1.2. Classification among the NDDs
3.1.3. Classification of All NDDs in One Group and Healthy Controls Group
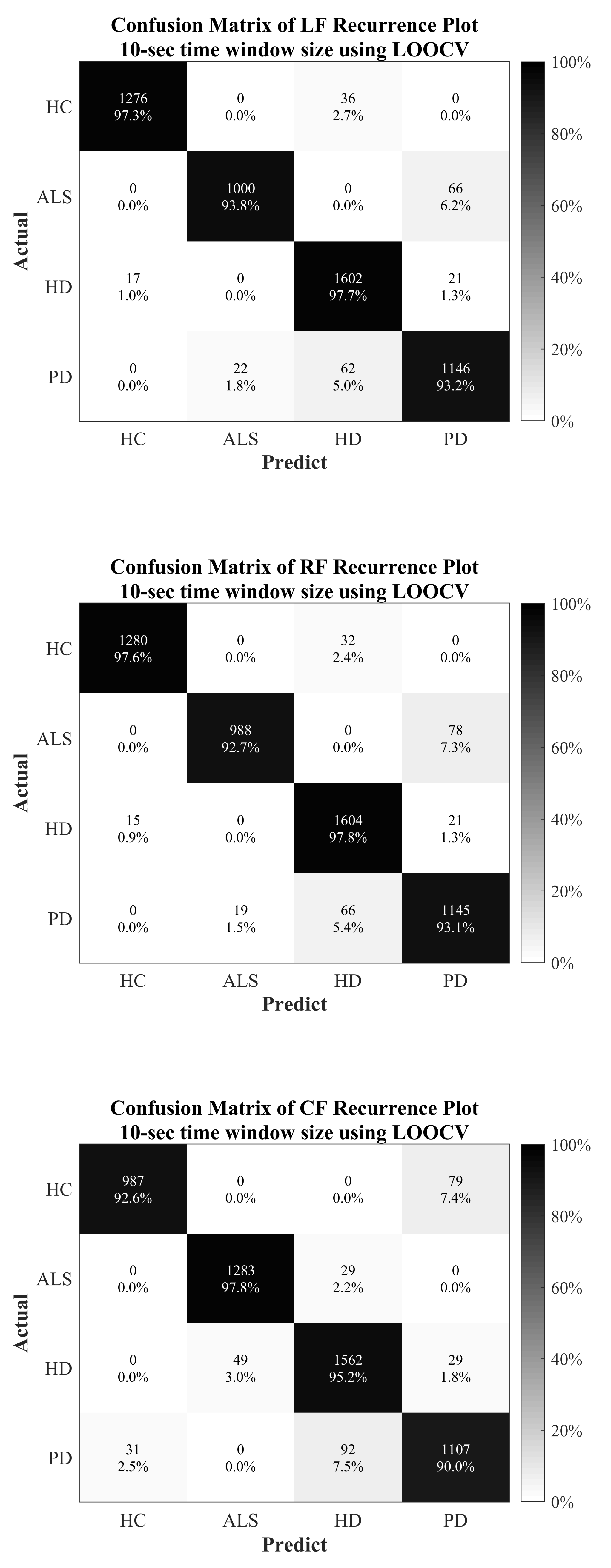
3.2. MultiClass Classification
4. Discussion
4.1. Healthy Control
4.2. Amyotrophic Lateral Sclerosis
4.3. Parkinson’s Disease
4.4. Huntington’s Disease
4.5. Classification Performance Comparison to Other Literature Based on PhysioNet Gait Dynamics in Neurodegenerative Disease Database
4.6. Limitations of the Proposed Method
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- JPND Research. What is Neurodegenerative Disease? 7 February 2015. Available online: http://bit.ly/2Hkzs9w (accessed on 12 July 2019).
- Lee, A.; Gilbert, R.M. Epidemiology of Parkinson’s disease. Neurol Clin. 2016, 34, 955–965. [Google Scholar] [CrossRef] [PubMed]
- Parkinson’s Disease Foundation. Statistics on Parkinson’s, EIN: 13-1866796. 2018. Available online: http://bit.ly/2RCeh9H (accessed on 12 July 2019).
- Chiò, A.; Logroscino, G.; Traynor, B.; Collins, J.; Simeone, J.; Goldstein, L.; White, L. Global epidemiology of amyotrophic lateral sclerosis: A systematic review of the published literature. Neuroepidemiology 2013, 41, 118–130. [Google Scholar] [CrossRef] [PubMed]
- Renton, A.E.; Chiò, A.; Traynor, B.J. State of play in amyotrophic lateral sclerosis genetics. Nat. Neurosci. 2014, 17, 17. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, M.; Biswas, A. Molecular diagnostics of neurodegenerative disorders. Front. Mol. Biosci. 2015, 2, 54. [Google Scholar] [CrossRef] [PubMed]
- Harvard NeuroDiscovery Center. The Challenge of Neurodegenerative Diseases. Available online: http://bit.ly/2soDGmD (accessed on 12 July 2019).
- Hausdorff, J.M.; Cudkowicz, M.E.; Firtion, R.; Wei, J.Y.; Goldberger, A.L. Gait variability and basal ganglia disorders: Stride-to-stride variations of gait cycle timing in Parkinson’s disease and Huntington’s disease. Mov. Disord. 1998, 13, 428–437. [Google Scholar] [CrossRef]
- Brown, R.H., Jr.; Al-Chalabi, A. Amyotrophic lateral sclerosis. N. Engl. J. Med. 2017, 377, 1602. [Google Scholar] [CrossRef]
- Hausdorff, J.M.; Lertratanakul, A.; Cudkowicz, M.E.; Peterson, A.L.; Kaliton, D.; Goldberger, A.L. Dynamic markers of altered gait rhythm in amyotrophic lateral sclerosis. J. Appl. Physiol. 2000, 88, 2045–2053. [Google Scholar] [CrossRef] [PubMed]
- Zarei, S.; Carr, K.; Reiley, L.; Diaz, K.; Guerra, O.; Altamirano, P.F.; Pagani, W.; Lodin, D.; Orozco, G.; Chinea, A. A Comprehensive Review of Amyotrophic Lateral Sclerosis. Surg. Neurol. Int. 2015, 6, 171. [Google Scholar] [CrossRef]
- Banaie, M.; Sarbaz, Y.; Gharibzadeh, S.; Towhidkhah, F. Huntington’s disease: Modeling the gait disorder and proposing novel treatments. J. Theor. Biol. 2008, 254, 361–367. [Google Scholar] [CrossRef] [PubMed]
- Dayalu, P.; Albin, R.L. Huntington disease: Pathogenesis and treatment. Neurol. Clin. 2015, 33, 101–114. [Google Scholar] [CrossRef] [PubMed]
- Pyo, S.J.; Kim, H.; Kim, I.S.; Park, Y.M.; Kim, M.J.; Lee, H.M.; Koh, S.B. Quantitative gait analysis in patients with Huntington’s disease. J. Mov. Disord. 2017, 10, 140. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Neurological Disorders and Stroke. Parkinson’s Disease Information Page. 2016. Available online: http://bit.ly/2xTA6rL (accessed on 12 July 2019).
- Hoff, J.; van den Plas, A.; Wagemans, E.; Van Hilten, J. Accelerometric assessment of levodopa-induced dyskinesias in Parkinson’s disease. Mov. Disord. 2001, 16, 58–61. [Google Scholar] [CrossRef]
- Pistacchi, M.; Gioulis, M.; Sanson, F.; De Giovannini, E.; Filippi, G.; Rossetto, F.; Marsala, S.Z. Gait analysis and clinical correlations in early Parkinson’s disease. Funct. Neurol. 2017, 32, 28. [Google Scholar] [CrossRef] [PubMed]
- Zeng, W.; Wang, C. Classification of neurodegenerative diseases using gait dynamics via deterministic learning. Inf. Sci. 2015, 317, 246–258. [Google Scholar] [CrossRef]
- Xia, Y.; Gao, Q.; Ye, Q. Classification of Gait rhythm signals between patients with neurodegenerative diseases and normal subjects: Experiments with statistical features and different classification models. Biomed. Signal Process. Control 2015, 18, 254–262. [Google Scholar] [CrossRef]
- Ertuğrul, Ö.F.; Kaya, Y.; Tekin, R.; Almalı, M.N. Detection of Parkinson’s disease by shifted one-dimensional local binary patterns from gait. Expert Syst. Appl. 2016, 56, 156–163. [Google Scholar] [CrossRef]
- Wu, Y.; Chen, P.; Luo, X.; Wu, M.; Liao, L.; Yang, S.; Rangayyan, R.M. Measuring signal fluctuations in gait rhythm time series of patients with Parkinson’s disease using entropy parameters. Biomed. Signal Process. Control. 2017, 31, 265–271. [Google Scholar] [CrossRef]
- Zhao, A.; Qi, L.; Dong, J.; Yu, H. Dual-channel LSTM based multi-feature extraction in gait for diagnosis of neurodegenerative diseases. Knowl.-Based Syst. 2018, 145, 91–97. [Google Scholar] [CrossRef]
- Bilgin, S. The impact of feature extraction for the classification of amyotrophic lateral sclerosis among neurodegenerative diseases and healthy subjects. Biomed. Signal Process. Control 2017, 31, 288–294. [Google Scholar] [CrossRef]
- Pham, T.D. Texture classification and visualization of time series of gait dynamics in patients with neurodegenerative diseases. IEEE Trans. Neural Syst. Rehabil. Eng. 2017, 26, 188–196. [Google Scholar] [CrossRef]
- Hausdorff, J.M.; Lertratanakul, A.; Cudkowicz, M.E.; Peterson, A.L.; Kaliton, D.; Goldberger, A.L. PhytioBank, PhysioToolkit, and PhysioNet: Components of a new research resource for complex physiologic signals. Circulation 2000, 101, e215–e220. [Google Scholar]
- Hausdorff, J.M.; Ladin, Z.; Wei, J.Y. Footswitch system for measurement of the temporal parameters of gait. J. Biomech. 1995, 28, 347–351. [Google Scholar] [CrossRef]
- Hoehn, M.M.; Yahr, M.D. Parkinsonism: Onset, progression, and mortality. Neurology 1967, 17, 427. [Google Scholar] [CrossRef]
- Rorabaugh, C.B. DSP Primer; McGraw Hill: New York, NY, USA, 1999. [Google Scholar]
- Dehghani, A.; Sarbishei, O.; Glatard, T.; Shihab, E. A quantitative comparison of overlapping and non-overlapping sliding windows for human activity recognition using inertial sensors. Sensors 2019, 19, 5026. [Google Scholar] [CrossRef] [PubMed]
- Morris, D.; Saponas, T.S.; Guillory, A.; Kelner, I. RecoFit: Using a wearable sensor to find, recognize, and count repetitive exercises. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, Toronto, ON, Canada, 14 April–26 May 2014; pp. 3225–3234. [Google Scholar]
- Lara, O.D.; Pérez, A.J.; Labrador, M.A.; Posada, J.D. Centinela: A human activity recognition system based on acceleration and vital sign data. Pervasive Mob. Comput. 2012, 8, 717–729. [Google Scholar] [CrossRef]
- Tapia, E.M.; Intille, S.S.; Haskell, W.; Larson, K.; Wright, J.; King, A.; Friedman, R. Real-time recognition of physical activities and their intensities using wireless accelerometers and a heart rate monitor. In Proceedings of the 2007 11th IEEE International Symposium on Wearable Computers, Boston, MA, USA, 11–13 October 2007; pp. 37–40. [Google Scholar]
- Marwan, N.; Romano, M.C.; Thiel, M.; Kurths, J. Recurrence plots for the analysis of complex systems. Phys. Rep. 2007, 438, 237–329. [Google Scholar] [CrossRef]
- Jolliffe, I.T. Principal Component Analysis, 2nd ed.; Springer: New York, NY, USA, 2002; Chapter 1, Introduction; p. 1. [Google Scholar]
- O’Shea, K.; Nash, R. An introduction to convolutional neural networks. arXiv, 2015; arXiv:1511.08458. [Google Scholar]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. Imagenet classification with deep convolutional neural networks. Adv. Neural Inf. Process. Syst. 2012, 25, 1097–1105. [Google Scholar] [CrossRef]
- LeCun, Y.; Boser, B.; Denker, J.S.; Henderson, D.; Howard, R.E.; Hubbard, W.; Jackel, L.D. Backpropagation applied to handwritten zip code recognition. Neural Comput. 1989, 1, 541–551. [Google Scholar] [CrossRef]
- Szegedy, C.; Liu, W.; Jia, Y.; Sermanet, P.; Reed, S.; Anguelov, D.; Erhan, D.; Vanhoucke, V.; Rabinovich, A. Going deeper with convolutions. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Boston, MA, USA, 7–12 June 2015; pp. 1–9. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Chengdu, China, 15–17 December 2017; pp. 770–778. [Google Scholar]
- Refaeilzadeh, P.; Tang, L.; Liu, H. Cross-validation. Encycl. Database Syst. 2009, 532–538. [Google Scholar] [CrossRef]
- Fawcett, T. An introduction to ROC analysis. Pattern Recognit. Lett. 2006, 27, 861–874. [Google Scholar] [CrossRef]
- Youden, W.J. Index for rating diagnostic tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef]
- Farooq, A.; Anwar, S.; Awais, M.; Rehman, S. A deep CNN based multi-class classification of Alzheimer’s disease using MRI. In Proceedings of the 2017 IEEE International Conference on Imaging Systems and Techniques, Beijing, China, 18–20 October 2017; pp. 1–6. [Google Scholar]
- Mehmood, A.; Maqsood, M.; Bashir, M.; Shuyuan, Y. A Deep Siamese Convolution Neural Network for Multi-Class Classification of Alzheimer Disease. Brain Sci. 2020, 10, 84. [Google Scholar] [CrossRef] [PubMed]
- Dutta, A.; Batabyal, T.; Basu, M.; Acton, S.T. An Efficient Convolutional Neural Network for Coronary Heart Disease Prediction. Expert Syst. Appl. 2020, 159, 113408. [Google Scholar] [CrossRef]
- Yao, Q.; Wang, R.; Fan, X.; Liu, J.; Li, Y. Multi-class Arrhythmia detection from 12-lead varied-length ECG using Attention-based Time-Incremental Convolutional Neural Network. Inf. Fusion 2020, 53, 174–182. [Google Scholar] [CrossRef]
- Lui, H.W.; Chow, K.L. Multiclass classification of myocardial infarction with convolutional and recurrent neural networks for portable ECG devices. Inform. Med. Unlocked 2018, 13, 26–33. [Google Scholar] [CrossRef]
- Yang, M.; Zheng, H.; Wang, H.; McClean, S. Feature selection and construction for the discrimination of neurodegenerative diseases based on gait analysis. In Proceedings of the 2009 3rd International Conference on Pervasive Computing Technologies for Healthcare, London, UK, 1–3 April 2009; pp. 1–7. [Google Scholar]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Literature | Summary of the Classification Algorithm | ||
|---|---|---|---|
| Feature Extraction | Classifier | Cross-Validation | |
| [18] | Radial basis function (RBF) neural networks | RBF neural networks | All training all testing and LOOCV |
| [19] | Mean, standard deviation, max, min, skewness, kurtosis, Lempel-Ziv complexity, fuzzy entropy and Teager–Kaiser energy feature | Support vector machine (SVM), random forest (RandF), multilayer perceptron (MLP) and k-nearest neighbor (KNN) | LOOCV |
| [20] | shifted 1D-LBP | Bayes Network (BayesNT), naïve Bayes (NB), logistic regression (LR), MLP, Partial C4.5 decision tree (PART), RandF and functional tree (FT) | 10-fold cross-validation |
| [21] | Approximate entropy (ApEn), normalized symbolic entropy (NSE), signal turns count (STC) | Generalized linear regression analysis (GLRA) and SVM | LOOCV |
| [22] | Dual channel LSTM | Dual channel LSTM | LOOCV |
| [23] | Discrete wavelet transform (DWT) | Linear discriminant analysis (LDA) and NBC | All training all testing and LOOCV |
| [24] | Fuzzy recurrence plot (FRP) + Gray-level co-occurrence matrix (GLCM) | Least squares support vector machine (LS-SVM) and LDA | LOOCV |
| Class | Gender | Ages (Year) | Height (m) | Weight (kg) | Gait Speed (m/s) | Severity/Duration |
|---|---|---|---|---|---|---|
| Male/ Female | (<50)/(50–70)/(≥70) | |||||
| HC | 2/14 | 11/4/1 | 1.83 ± 0.08 | 66.81 ± 11.08 | 1.35 ± 0.16 | 0 |
| ALS | 10/3 | 4/7/2 | 1.74 ± 0.10 | 77.11 ± 21.15 | 1.05 ± 0.22 | 18.31 ± 17.82 1 |
| PD | 10/5 | 1/7/7 | 1.87 ± 0.15 | 75.07 ± 16.9 | 1.0 ± 0.2 | 3 2 |
| HD | 6/14 | 13/5/2 | 1.84 ± 0.09 | 73.47 ± 16.23 | 1.15 ± 0.35 | 8 3 |
| Class | Number of vGRF Data | |
|---|---|---|
| Number of Subjects (Original) | Samples of Time-Windowing Process (10-s) | |
| HC | 16 | 1312 |
| ALS | 13 | 1066 |
| PD | 15 | 1230 |
| HD | 20 | 1640 |
| Total | 64 | 5248 |
| Proposed Action Methods | Execution Time (s) | |
|---|---|---|
| 10-s Length (5248 Input Samples) | 5-min Length (60 Input Samples) | |
| Feature transformation using recurrence plot | 51.676 | 1.381 |
| Feature enhancement using PCA | 550.350 | 1.945 |
| AlexNet CNN model training and testing using LOOCV | 38,198.402 | 23.702 |
| Classification Tasks | 10-sTime Window Size | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Acc. (%) | Sens. (%) | Spec. (%) | AUC | (Youden’s Index) | |||||||||||
| LF | RF | CF | LF | RF | CF | LF | RF | CF | LF | RF | CF | LF | RF | CF | |
| ALS vs. HC | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 1 | 1 | 1 | 1 | 1 | 1 |
| HD vs. HC | 98.41 | 98.04 | 97.56 | 98.54 | 97.59 | 98.51 | 98.25 | 98.60 | 96.41 | 0.9839 | 0.9810 | 0.9746 | 0.9679 | 0.9619 | 0.9492 |
| PD vs. HC | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 1 | 1 | 1 | 1 | 1 | 1 |
| ALS vs. HD | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 1 | 1 | 1 | 1 | 1 | 1 |
| PD vs. ALS | 95.64 | 95.95 | 94.21 | 94.07 | 94.59 | 92.95 | 97.63 | 97.65 | 95.78 | 0.9585 | 0.9612 | 0.9437 | 0.9170 | 0.9224 | 0.8873 |
| HD vs. PD | 97.11 | 97.25 | 94.98 | 96.81 | 96.54 | 93.54 | 97.51 | 98.24 | 97.14 | 0.9711 | 0.9739 | 0.9534 | 0.9432 | 0.9478 | 0.9068 |
| NDD vs. HC | 98.86 | 98.91 | 98.93 | 99.01 | 99.04 | 99.44 | 98.38 | 98.53 | 97.43 | 0.9870 | 0.9878 | 0.9844 | 0.9739 | 0.9757 | 0.9687 |
| Classification Tasks | 5-min Time Window Size | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Acc. (%) | Sens. (%) | Spec. (%) | AUC | (Youden’s Index) | |||||||||||
| LF | RF | CF | LF | RF | CF | LF | RF | CF | LF | RF | CF | LF | RF | CF | |
| ALS vs. HC | 96.55 | 96.55 | 86.21 | 100 | 100 | 90.91 | 94.12 | 94.12 | 83.33 | 0.9706 | 0.9706 | 0.8712 | 0.9412 | 0.9412 | 0.7424 |
| HD vs. HC | 77.78 | 83.33 | 77.78 | 83.33 | 93.75 | 92.86 | 72.22 | 75 | 68.18 | 0.7778 | 0.8438 | 0.8052 | 0.5555 | 0.6875 | 0.6104 |
| PD vs. HC | 93.55 | 90.32 | 80.65 | 100 | 100 | 90.91 | 88.89 | 84.21 | 75 | 0.9444 | 0.9211 | 0.8295 | 0.8889 | 0.8421 | 0.6591 |
| ALS vs. HD | 87.88 | 90.91 | 81.82 | 100 | 100 | 100 | 83.33 | 86.96 | 76.92 | 0.9167 | 0.9348 | 0.8846 | 0.8333 | 0.8696 | 0.7692 |
| PD vs. ALS | 71.43 | 71.43 | 71.43 | 76.92 | 73.33 | 70.59 | 66.67 | 69.23 | 72.73 | 0.7179 | 0.7128 | 0.7166 | 0.4359 | 0.4256 | 0.4332 |
| HD vs. PD | 82.86 | 77.14 | 68.57 | 79.17 | 75 | 69.57 | 90.91 | 81.82 | 66.67 | 0.8504 | 0.7899 | 0.6812 | 0.7008 | 0.5682 | 0.3624 |
| NDD vs. HC | 89.06 | 92.19 | 85.94 | 97.67 | 95.74 | 93.33 | 71.43 | 82.35 | 68.42 | 0.8455 | 0.8905 | 0.8088 | 0.6910 | 0.7809 | 0.6175 |
| Classification Tasks | LF + 10-s Time Window Size | RF + 10-s Time Window Size | CF + 10-s Time Window Size | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Acc. (%) | Sens. (%) | Spec. (%) | AUC | Acc. (%) | Sens. (%) | Spec. (%) | AUC | Acc. (%) | Sens. (%) | Spec. (%) | AUC | |
| HC | 98.99 | 97.26 | 99.57 | 0.9841 | 99.10 | 97.56 | 99.62 | 0.9859 | 98.51 | 97.79 | 98.76 | 0.9827 |
| ALS | 98.32 | 93.81 | 99.47 | 0.9664 | 98.15 | 92.68 | 99.55 | 0.9611 | 97.90 | 92.59 | 99.26 | 0.9592 |
| HD | 97.41 | 97.68 | 97.28 | 0.9748 | 97.45 | 97.80 | 97.28 | 0.9754 | 96.21 | 95.24 | 96.65 | 0.9595 |
| PD | 96.74 | 93.17 | 97.83 | 0.9550 | 96.49 | 93.09 | 97.54 | 0.9531 | 95.60 | 90 | 97.31 | 0.9366 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, C.-W.; Wen, T.-C.; Setiawan, F. Evaluation of Vertical Ground Reaction Forces Pattern Visualization in Neurodegenerative Diseases Identification Using Deep Learning and Recurrence Plot Image Feature Extraction. Sensors 2020, 20, 3857. https://doi.org/10.3390/s20143857
Lin C-W, Wen T-C, Setiawan F. Evaluation of Vertical Ground Reaction Forces Pattern Visualization in Neurodegenerative Diseases Identification Using Deep Learning and Recurrence Plot Image Feature Extraction. Sensors. 2020; 20(14):3857. https://doi.org/10.3390/s20143857
Chicago/Turabian StyleLin, Che-Wei, Tzu-Chien Wen, and Febryan Setiawan. 2020. "Evaluation of Vertical Ground Reaction Forces Pattern Visualization in Neurodegenerative Diseases Identification Using Deep Learning and Recurrence Plot Image Feature Extraction" Sensors 20, no. 14: 3857. https://doi.org/10.3390/s20143857
APA StyleLin, C.-W., Wen, T.-C., & Setiawan, F. (2020). Evaluation of Vertical Ground Reaction Forces Pattern Visualization in Neurodegenerative Diseases Identification Using Deep Learning and Recurrence Plot Image Feature Extraction. Sensors, 20(14), 3857. https://doi.org/10.3390/s20143857