Dry Electrode-Based Body Fat Estimation System with Anthropometric Data for Use in a Wearable Device

 ,
, 
Abstract
:1. Introduction
2. Related Works
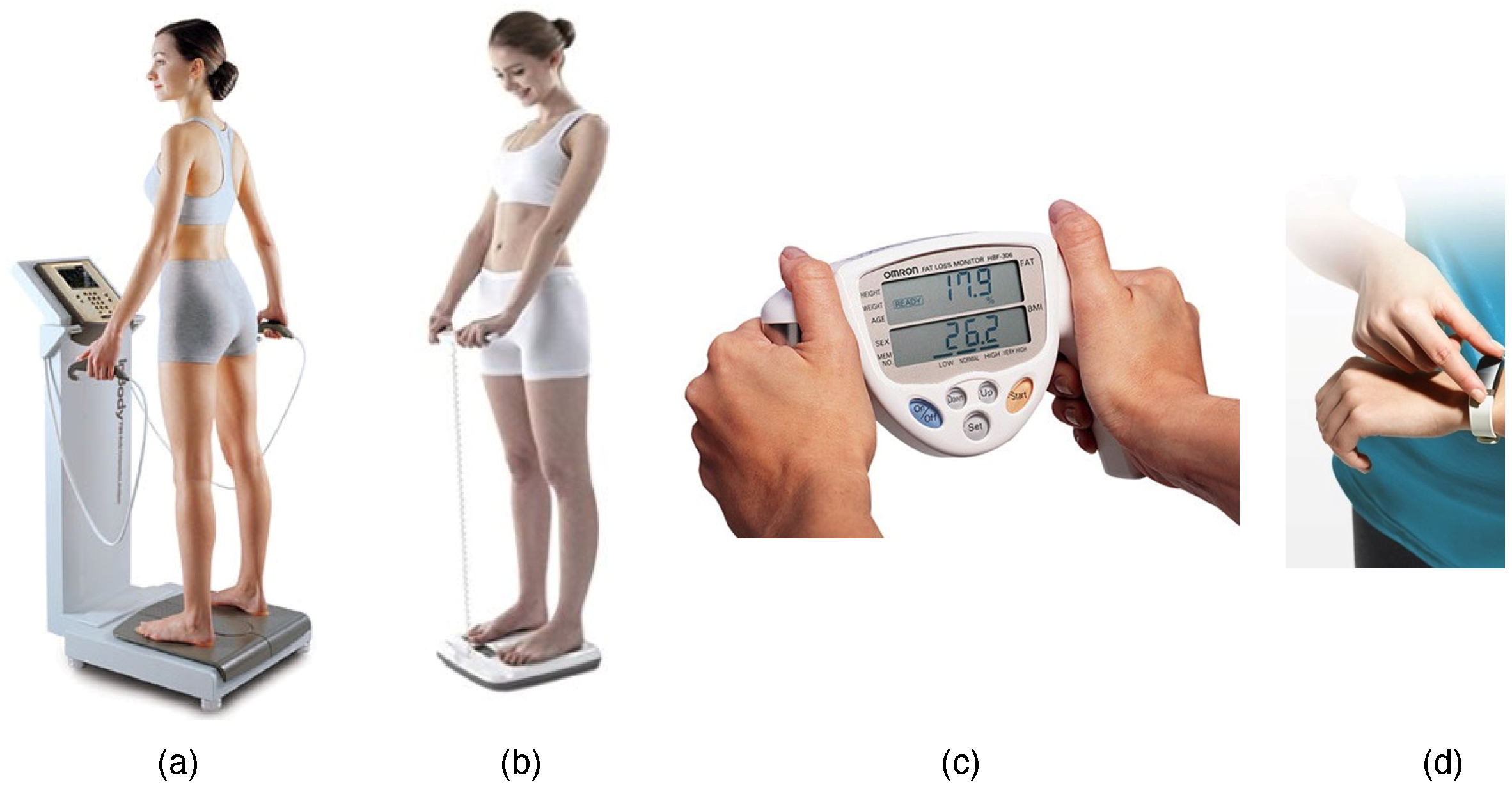
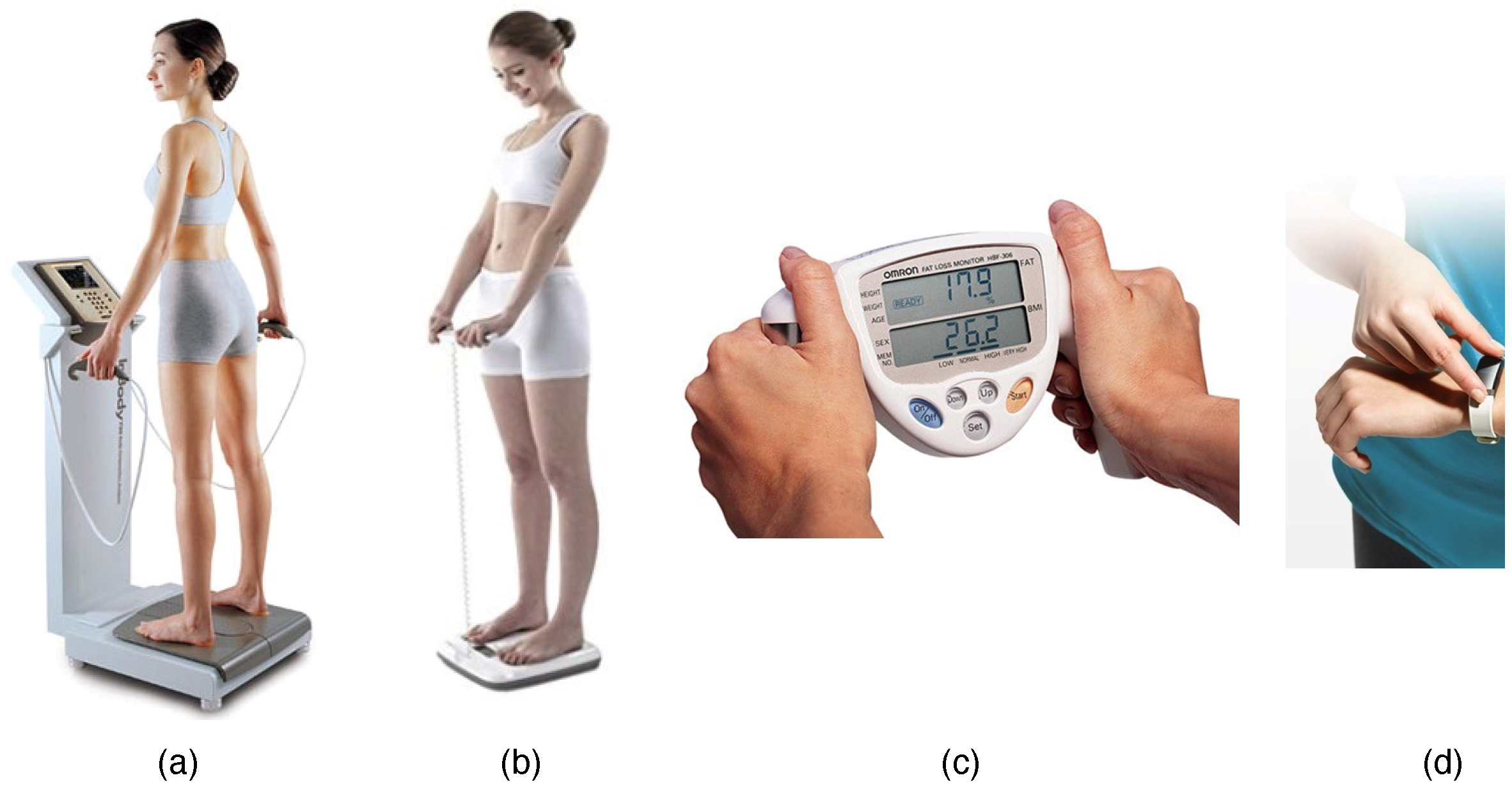
2.1. Various Types of Body Composition Measurement Methods
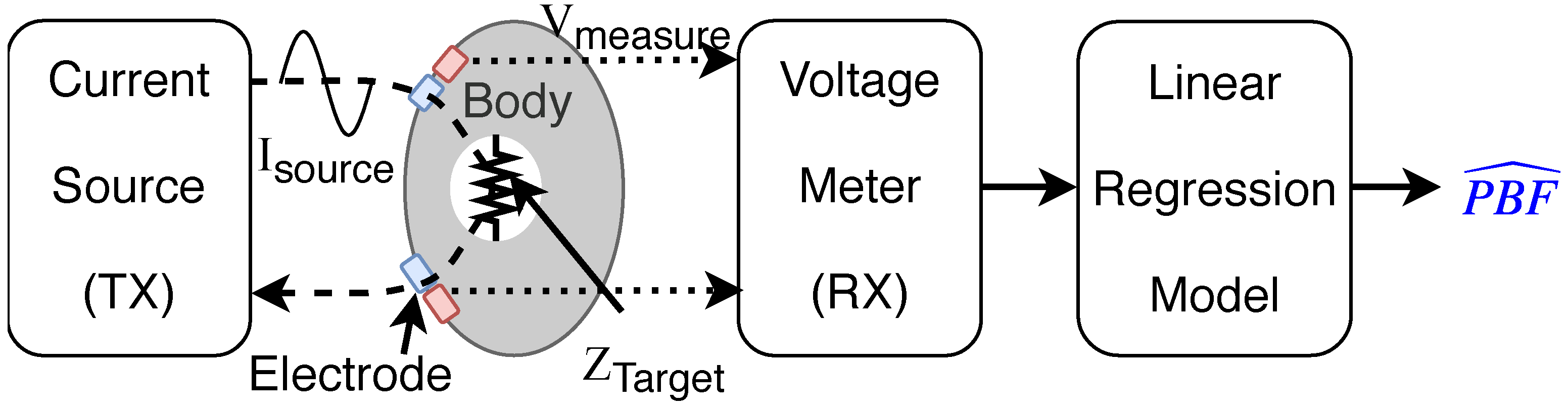
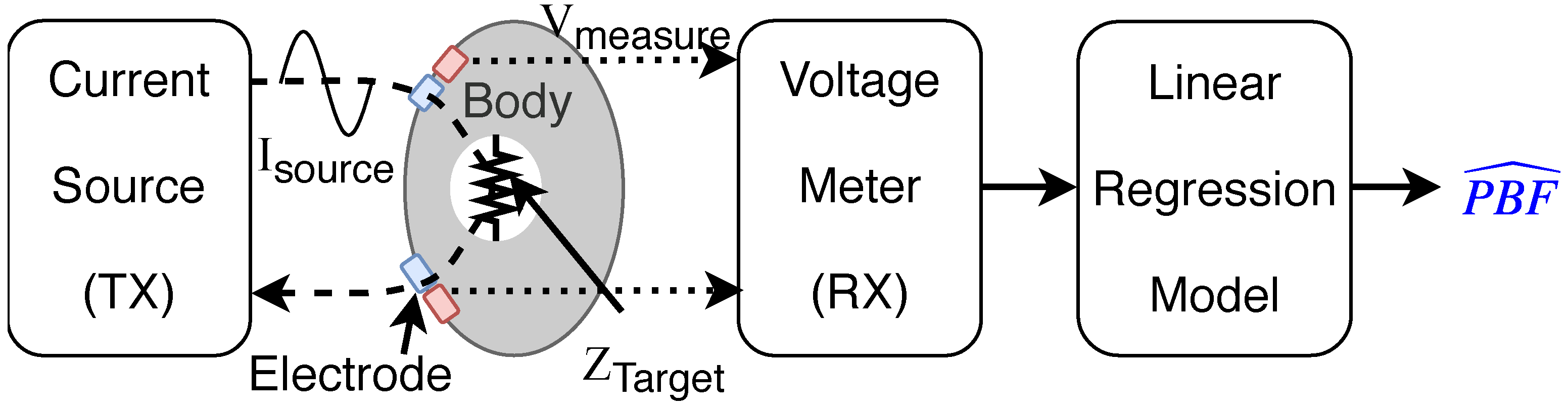
2.2. Body Composition Measurement Using Bioelectrical Impedance Analysis (BIA)
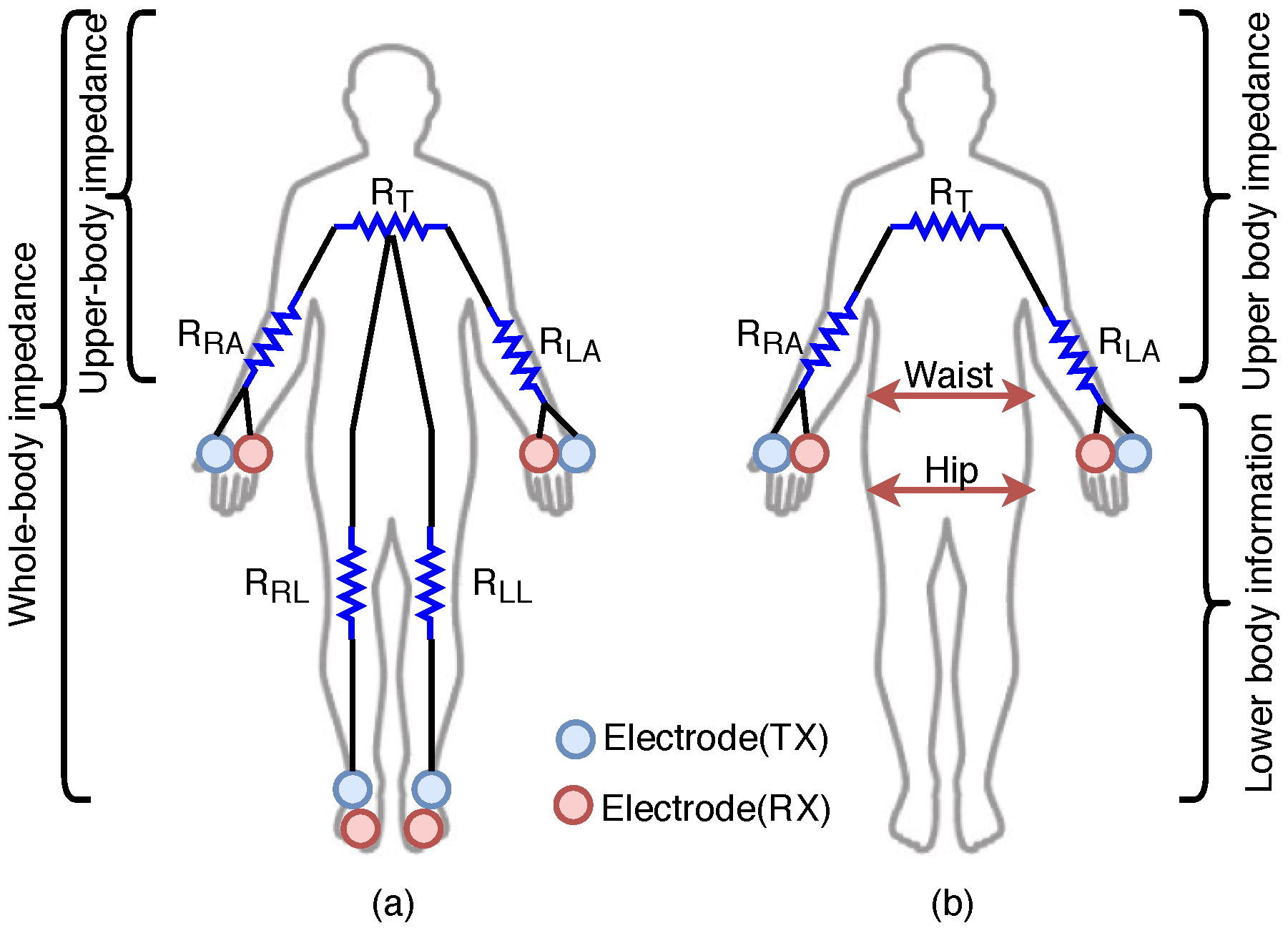
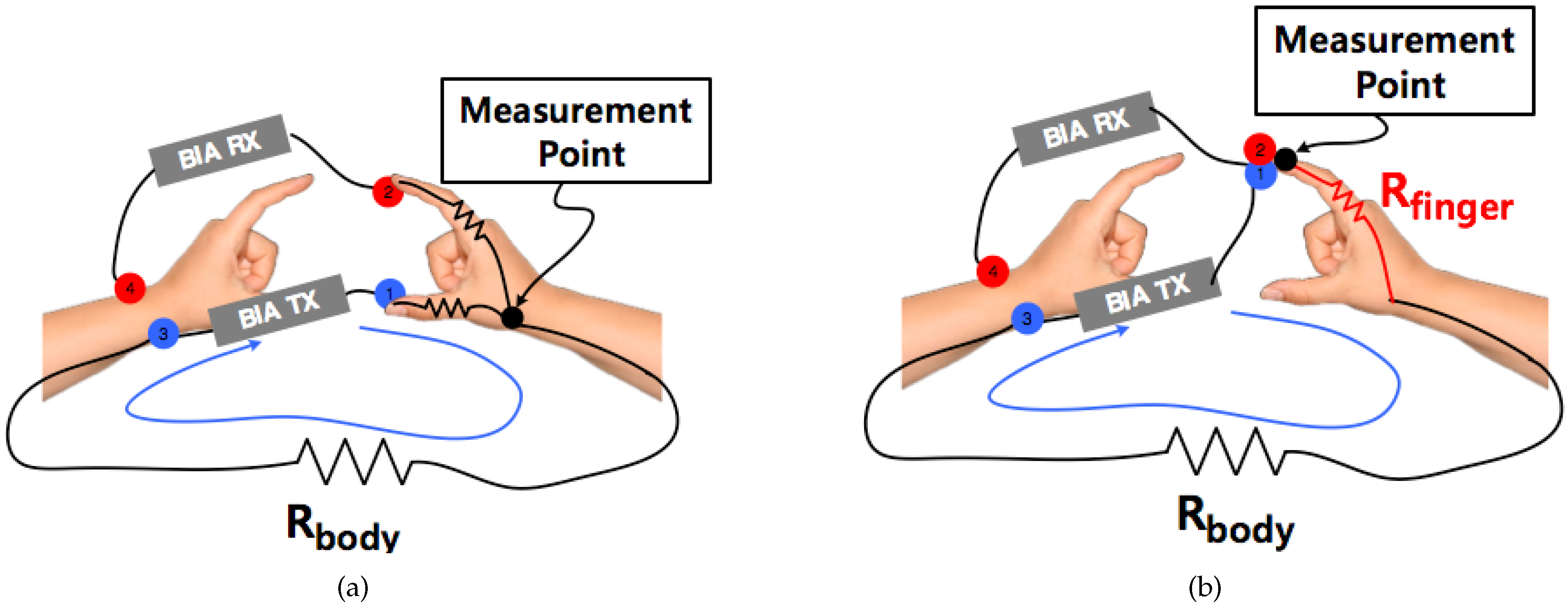
2.3. Effect of Measurement Position on BIA Method
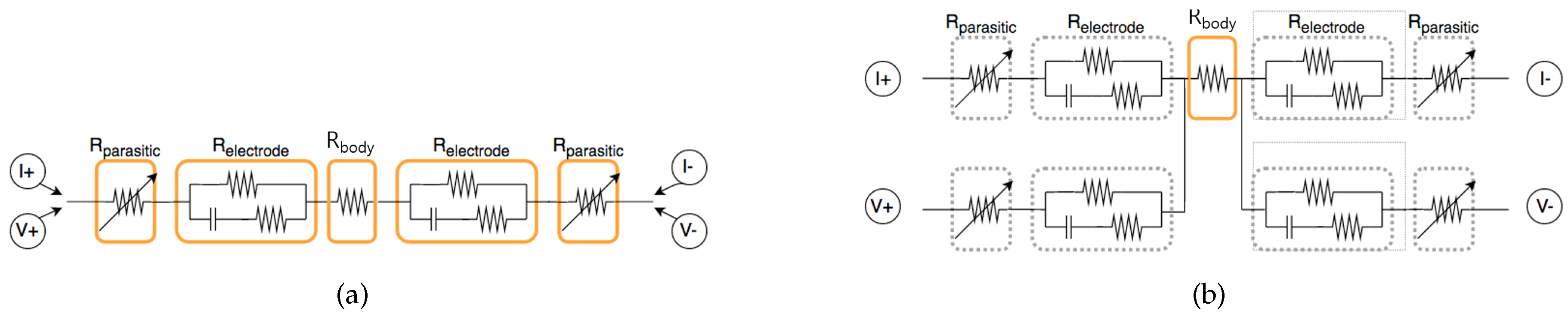
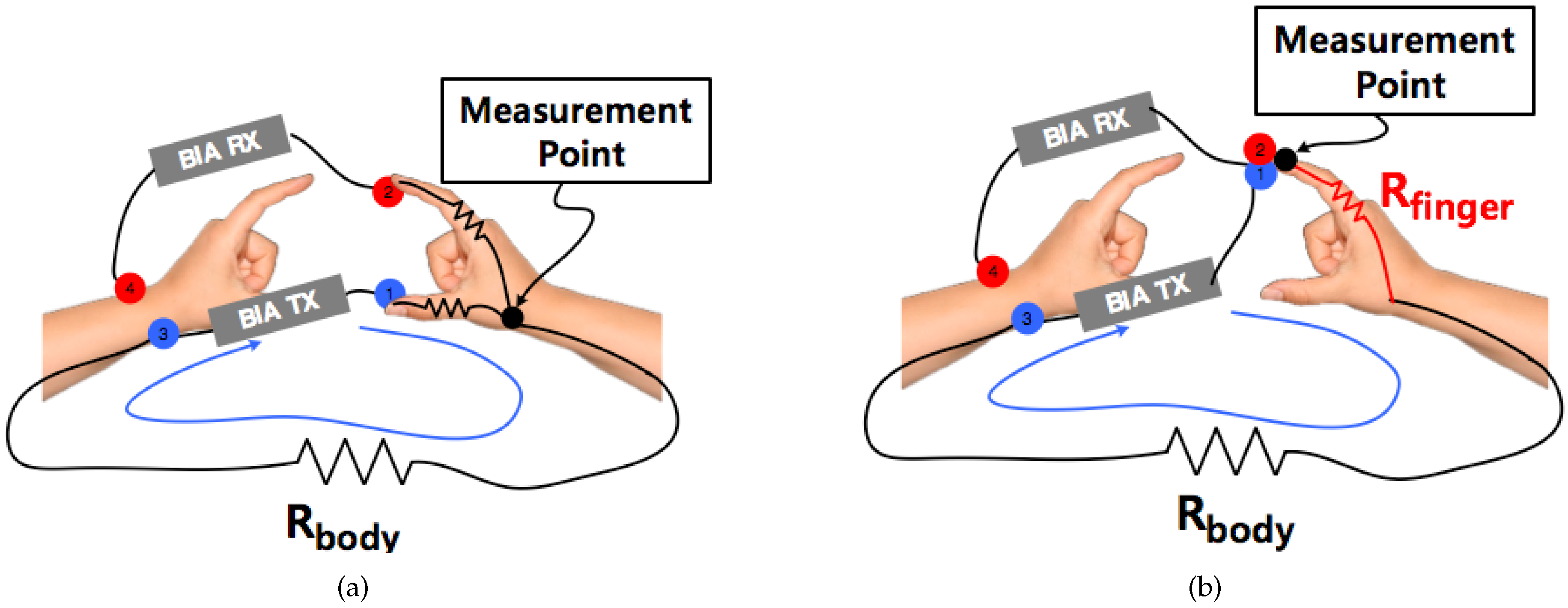
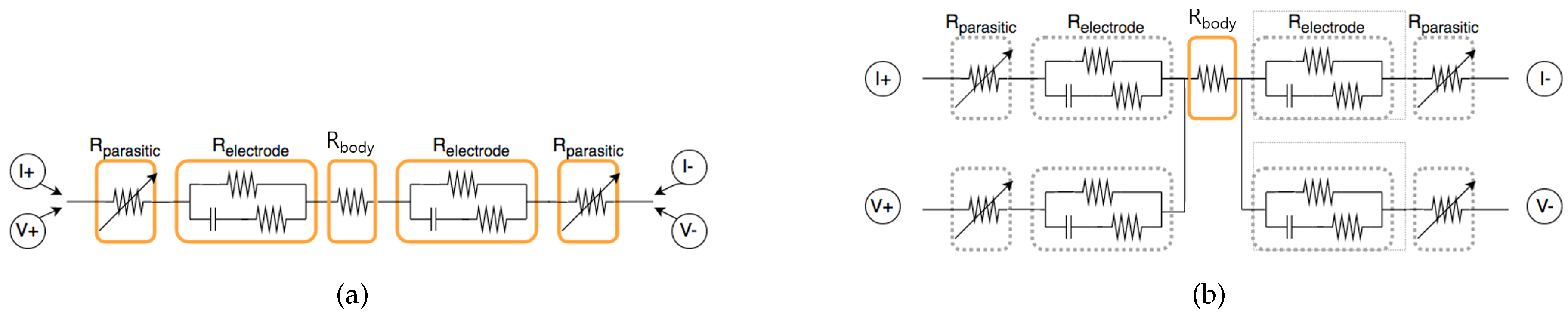
2.4. Electrode Separation Effect between TX and RX
3. System Design and Data Acquisition Method
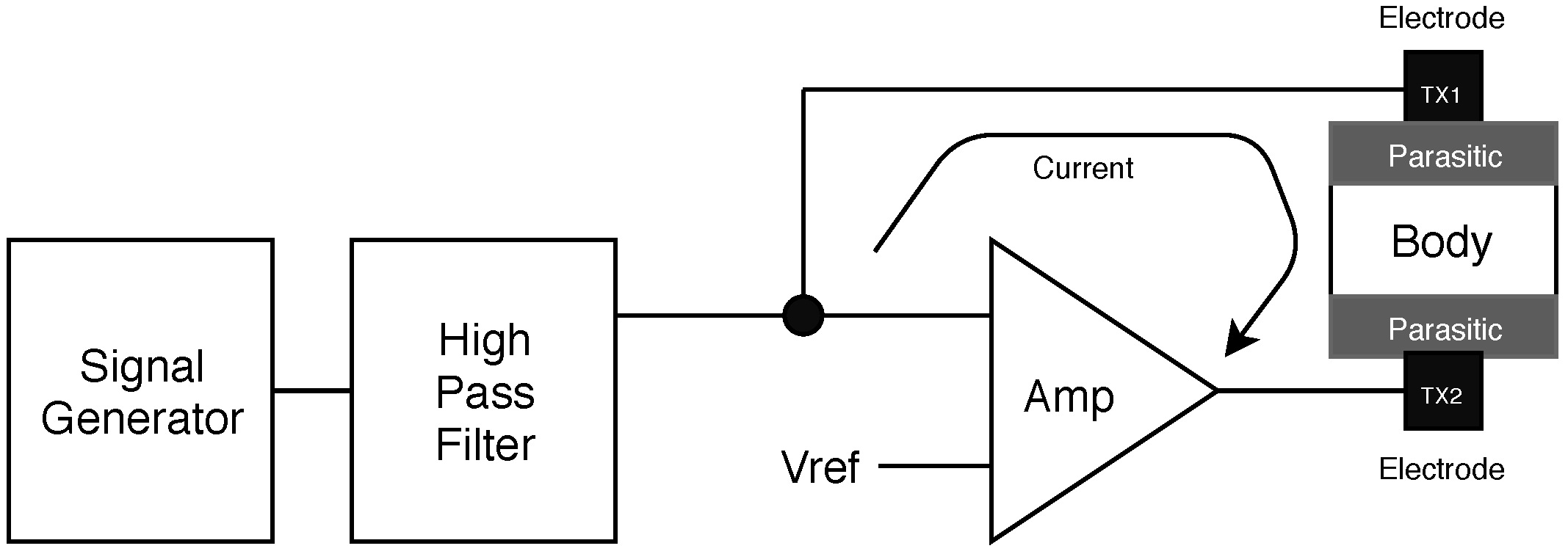
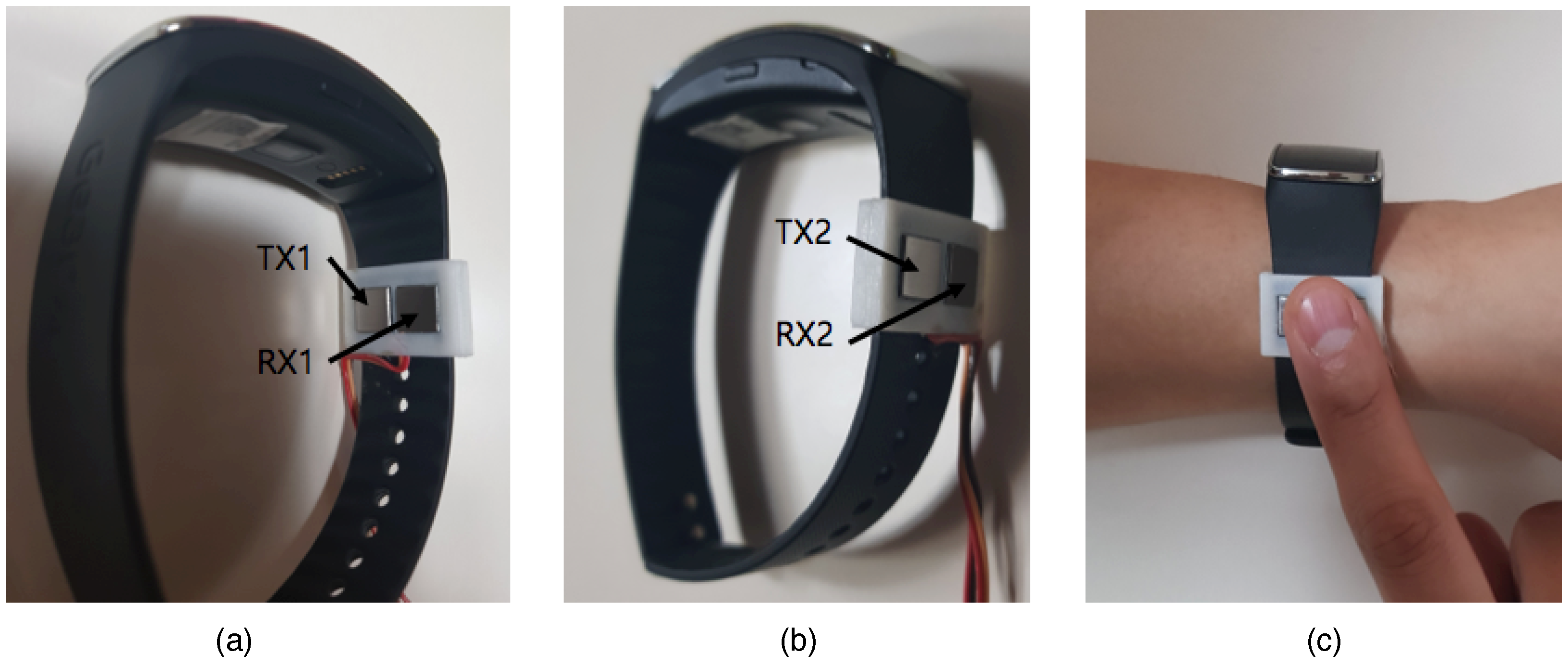
3.1. Hardware Design and Measurement Posture
3.2. Data Acquisition Process
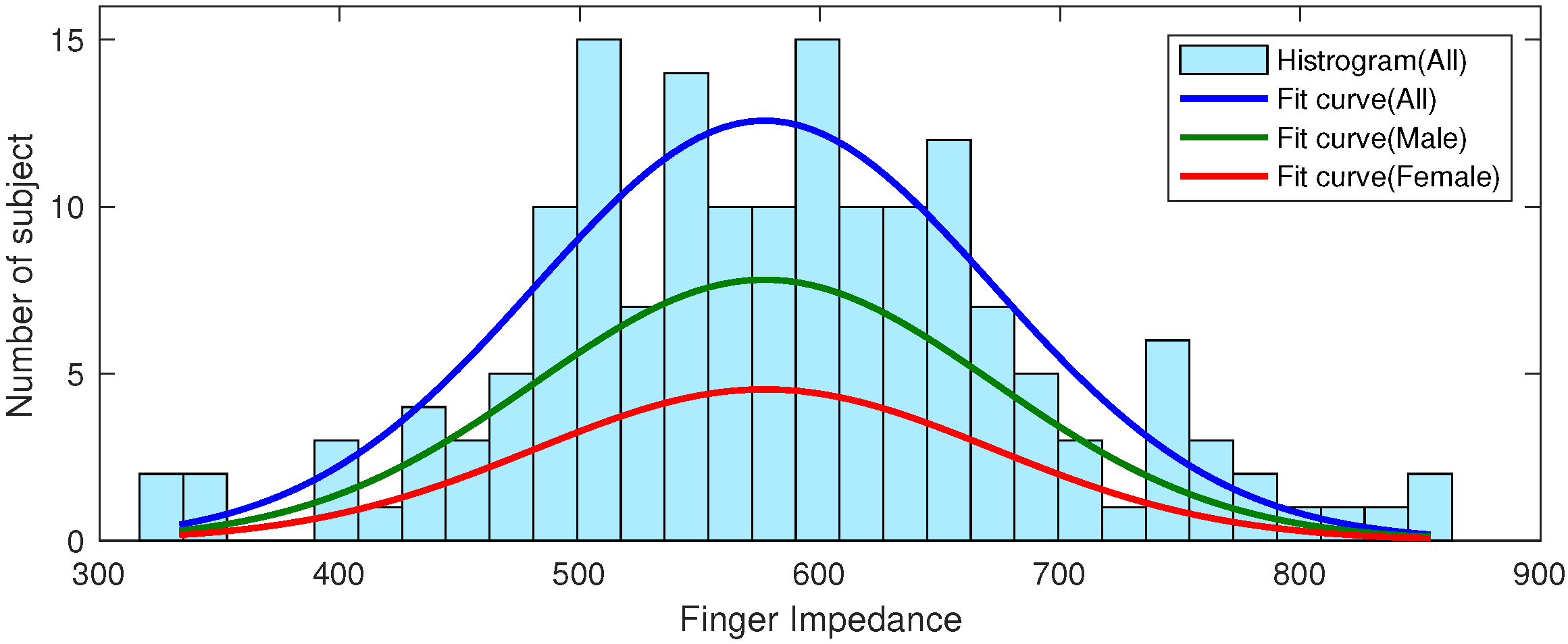
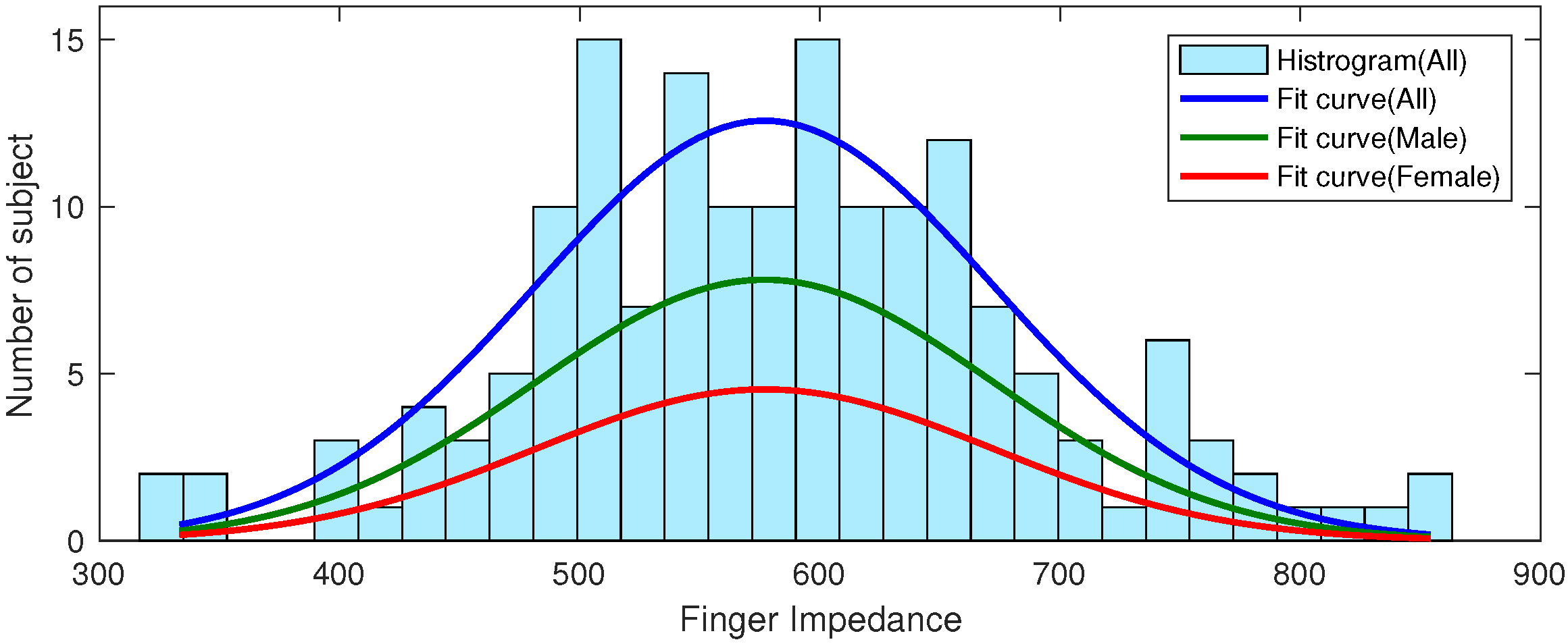
3.3. Subject Statistics
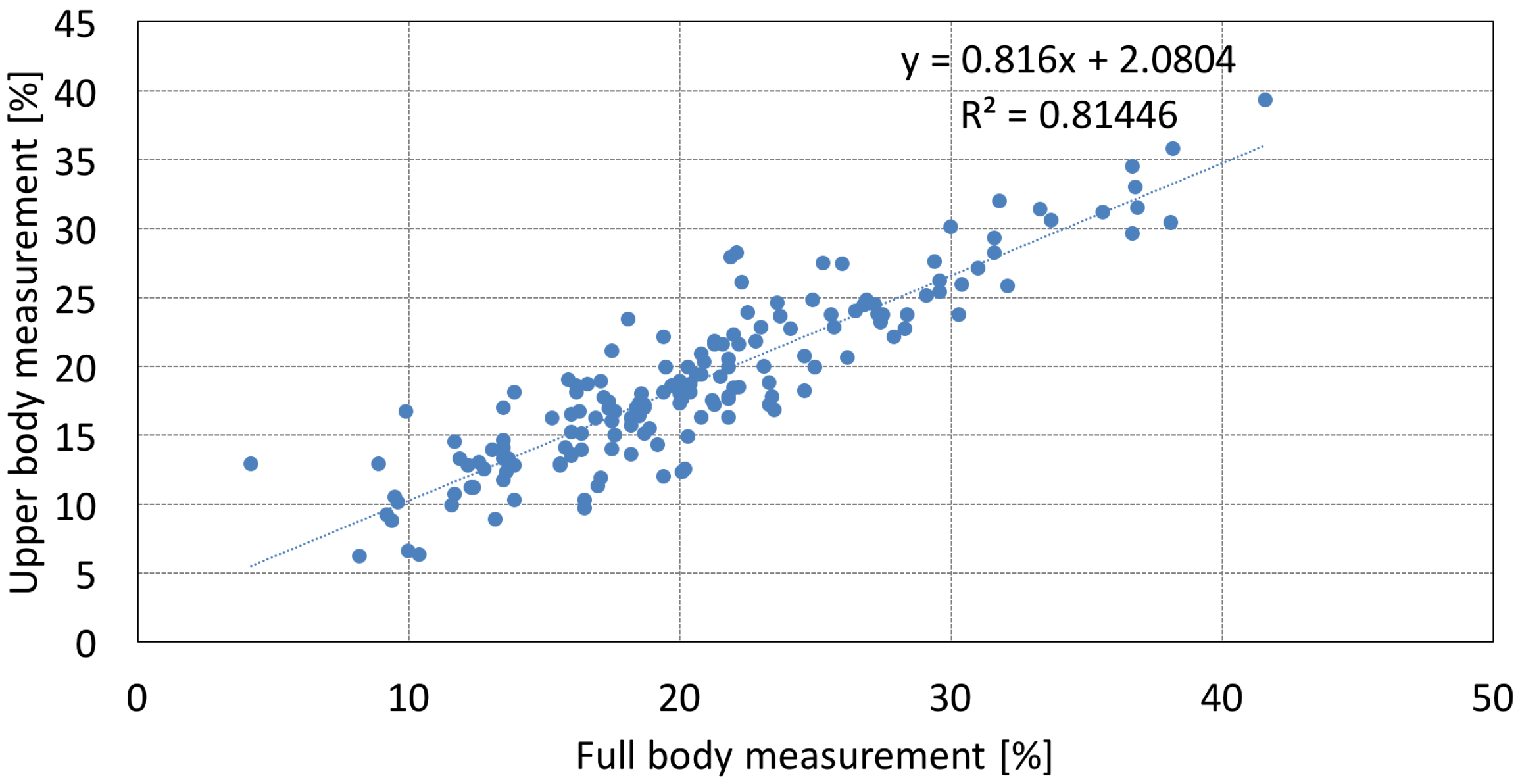
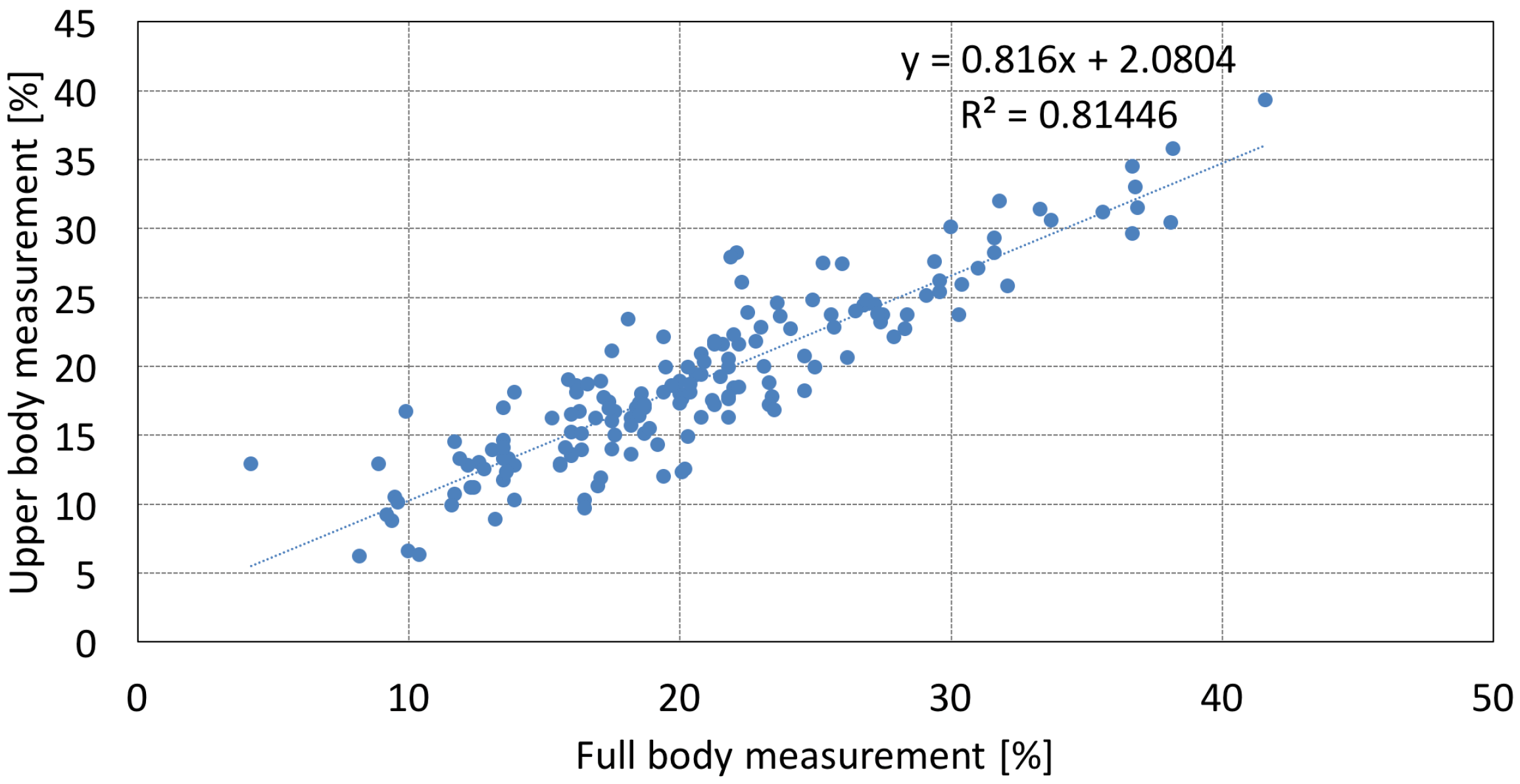
3.4. Comparison of the PBF Results of Whole-Body and Upper-Body Measurements
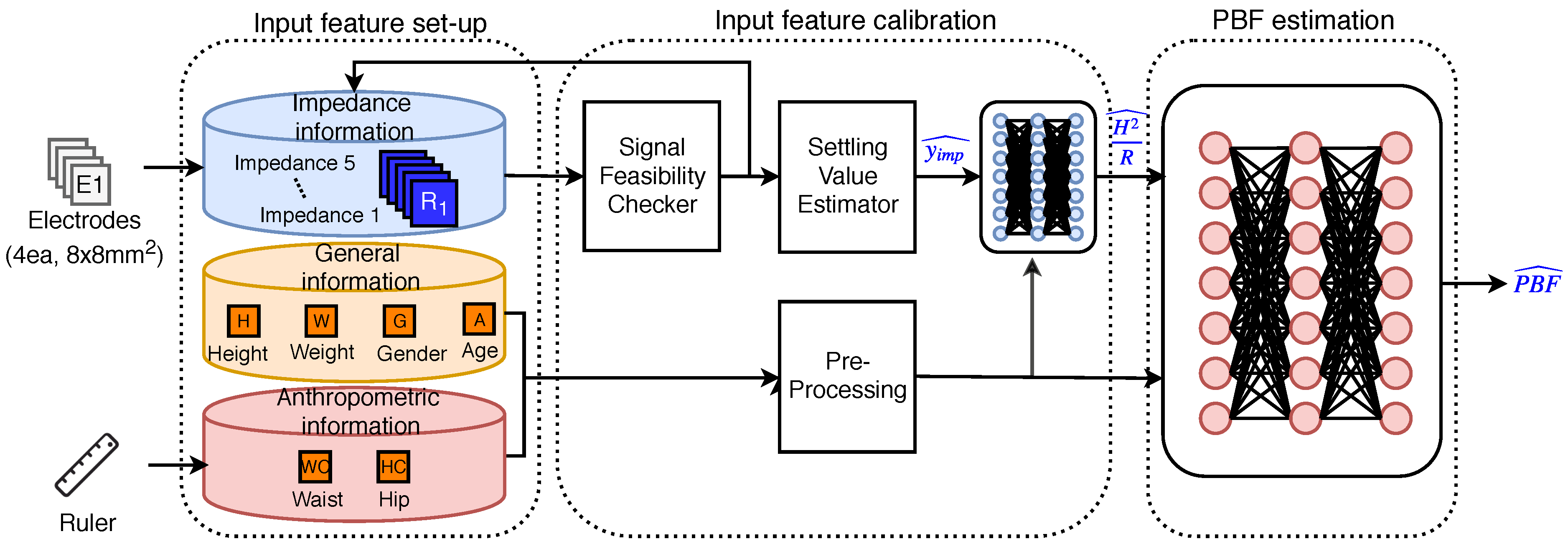
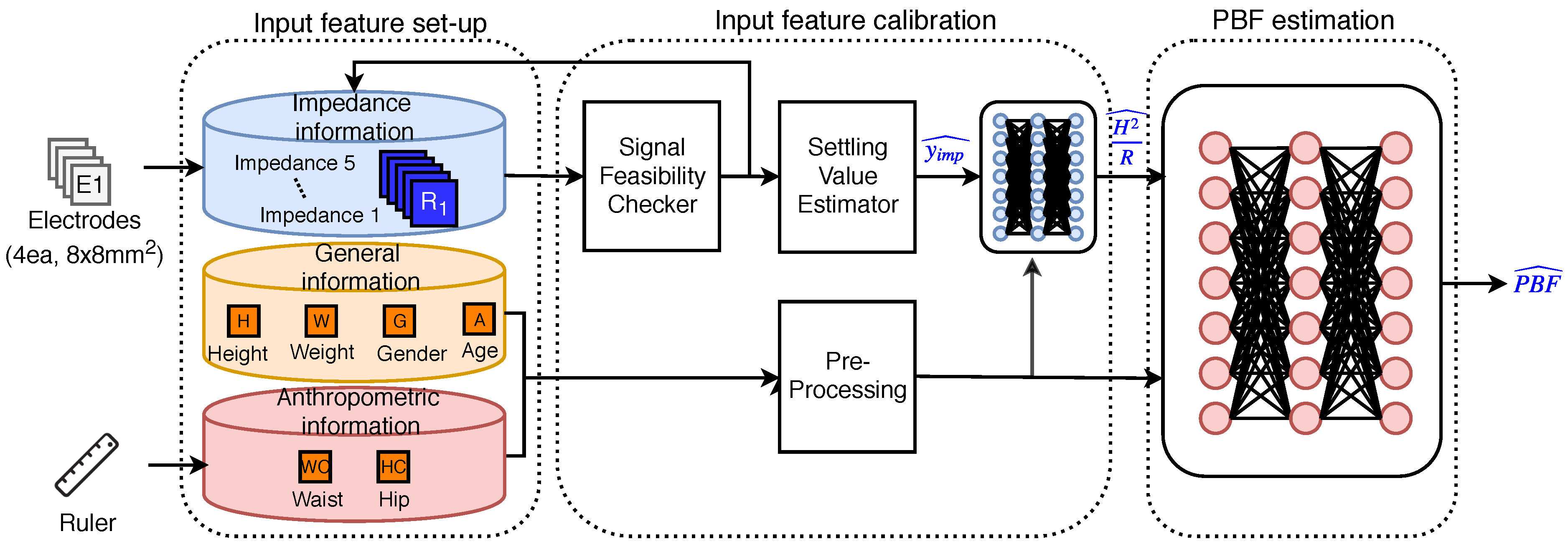
4. Input Feature Processing Methods
4.1. Signal Feasibility Checker
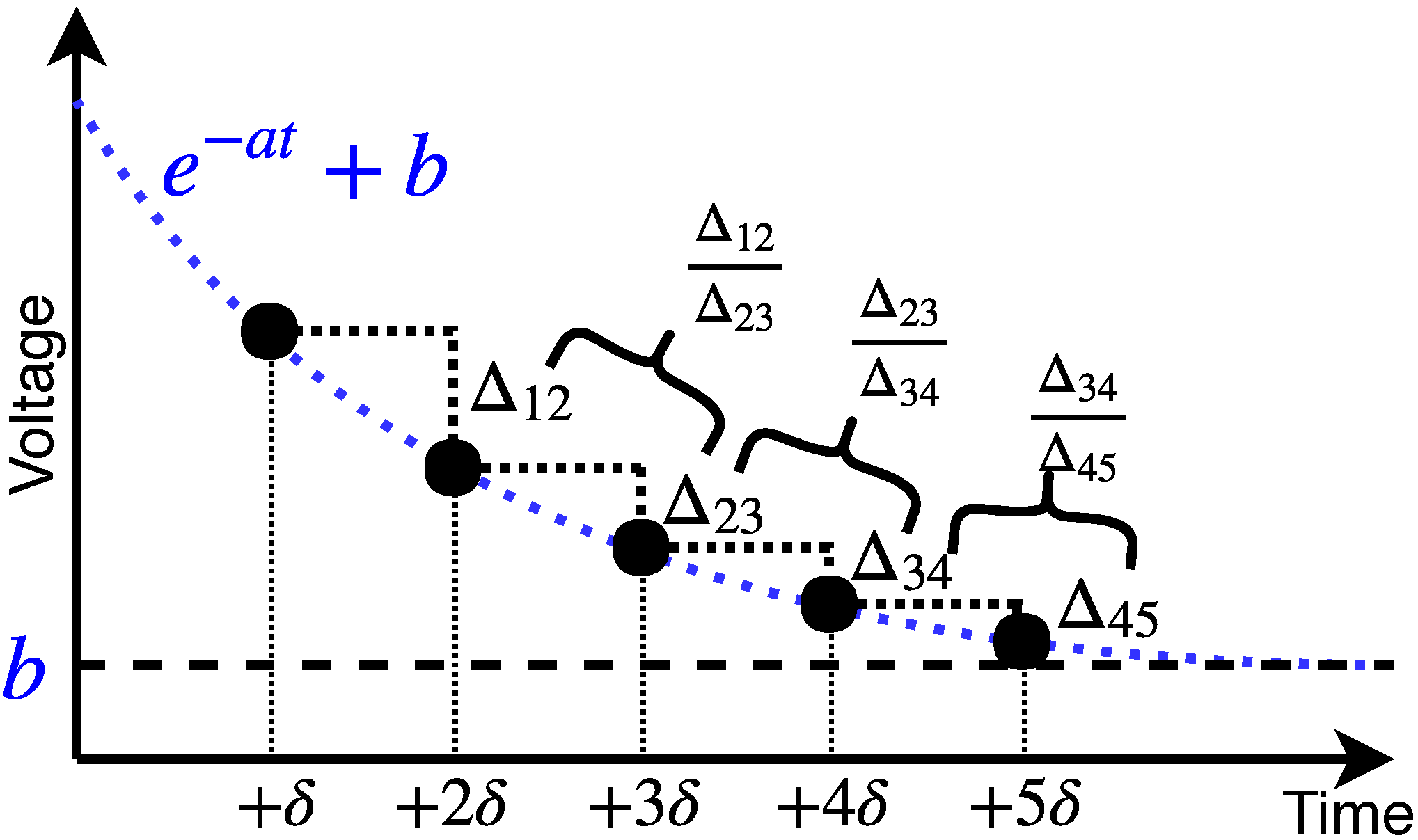
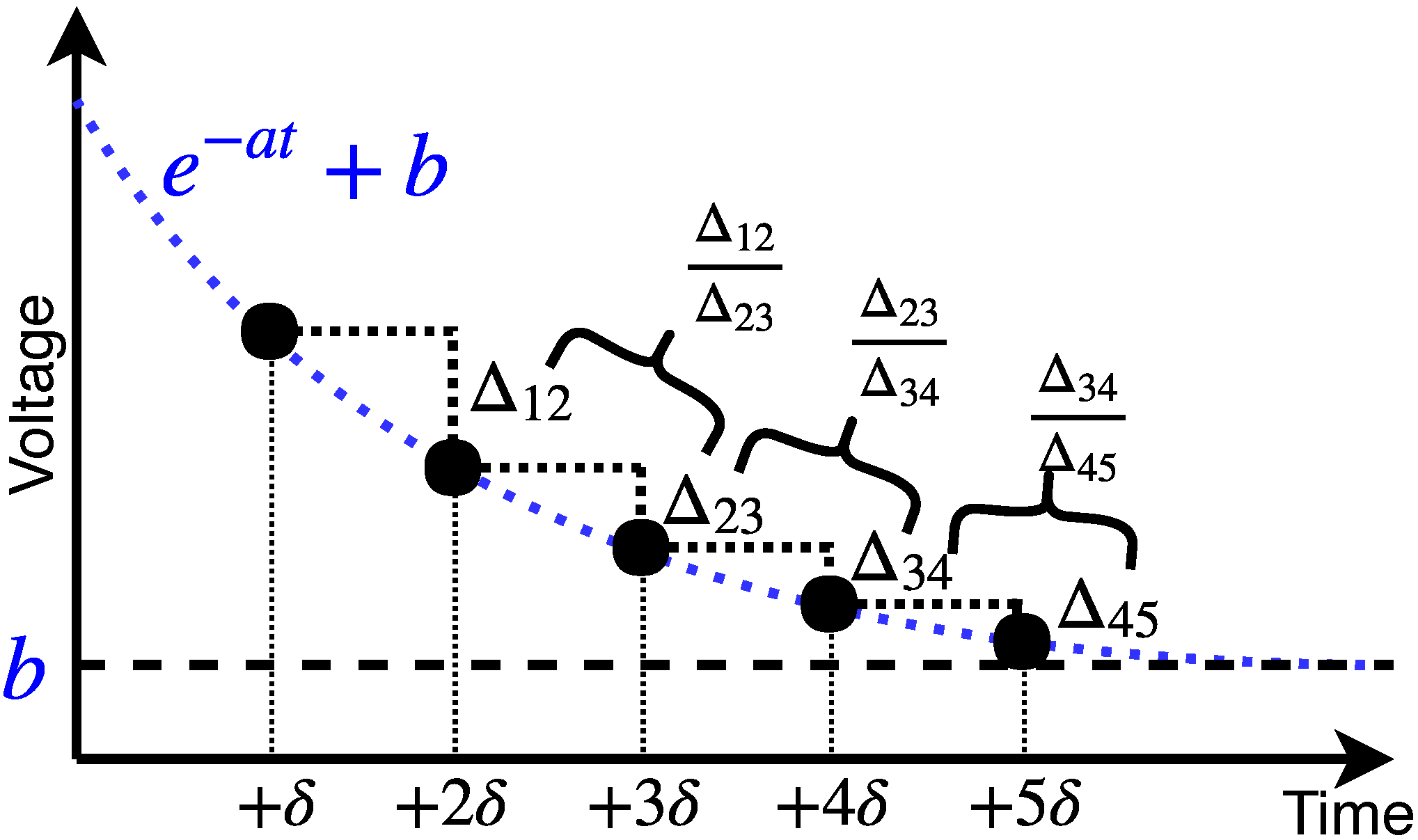
4.2. Settling Value Estimator
4.3. Predicting the Value of
4.4. PBF Estimation Method Using Deep Neural-Networks
5. Results and Discussion
5.1. Input Feature Calibration Results
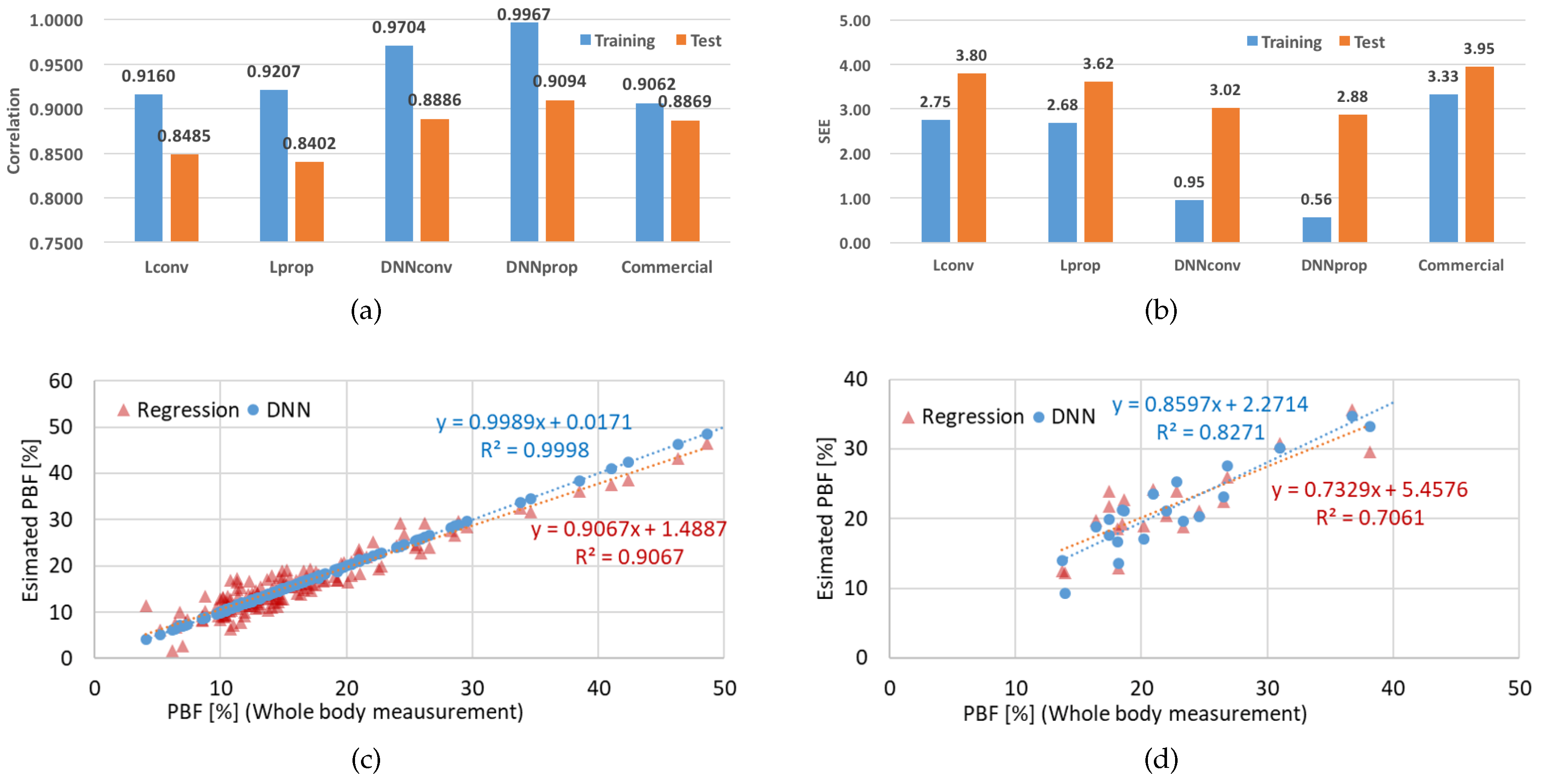
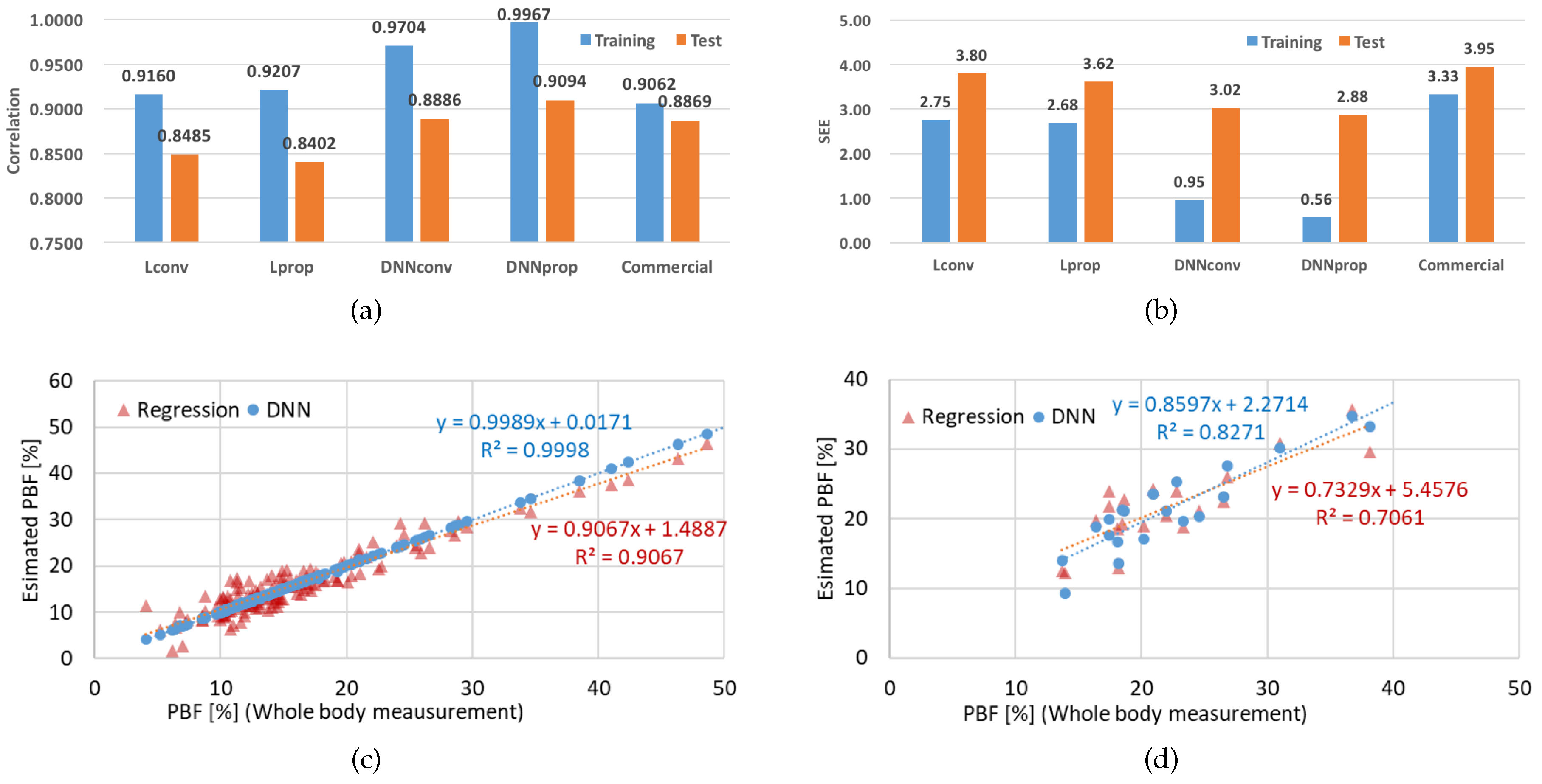
5.2. PBF Estimation Using Deep Neural Networks
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| BIA | Body impedance analysis |
| PBF | Percent body fat |
| SEE | Standard error of estimate |
| DEXA | Dual-energy X-ray absorptiometry |
| BMI | Body mass index |
| TBW | Total body water |
| FFM | Fat-free mass |
| FM | Fat mass |
| ReLU | Rectified linear unit |
References
- Casselman, J.; Onopa, N.; Khansa, L. Wearable healthcare: Lessons from the past and a peek into the future. Telemat. Inform. 2017, 34, 1011–1023. [Google Scholar] [CrossRef]
- Gutin, B.; Islam, S.; Manos, T.; Cucuzzo, N.; Smith, C.; Stachura, M.E. Relation of percentage of body fat and maximal aerobic capacity to risk factors for atherosclerosis and diabetes in black and white seven-to eleven-year-old children. J. Pediatr. 1994, 125, 847–852. [Google Scholar] [CrossRef]
- Renehan, A.G.; Tyson, M.; Egger, M.; Heller, R.F.; Zwahlen, M. Body-mass index and incidence of cancer: A systematic review and meta-analysis of prospective observational studies. Lancet 2008, 371, 569–578. [Google Scholar] [CrossRef]
- Vazquez, G.; Duval, S.; Jacobs, D.R., Jr.; Silventoinen, K. Comparison of body mass index, waist circumference, and waist/hip ratio in predicting incident diabetes: A meta-analysis. Epidemiol. Rev. 2007, 29, 115–128. [Google Scholar] [CrossRef]
- Leahy, S.; O’Neill, C.; Sohun, R.; Jakeman, P. A comparison of dual energy X-ray absorptiometry and bioelectrical impedance analysis to measure total and segmental body composition in healthy young adults. Eur. J. Appl. Physiol. 2012, 112, 589–595. [Google Scholar] [CrossRef]
- Rubiano, F.; Nunez, C.; Heymsfield, S. A comparison of body composition techniques. Ann. N. Y. Acad. Sci. 2000, 904, 335–338. [Google Scholar] [CrossRef]
- Heyward, V.H.; Wagner, D.R. Applied Body Composition Assessment, 2nd ed.; Human Kinetics: Champaign, IL, USA, 2004. [Google Scholar]
- Lukaski, H.C.; Bolonchuk, W.W.; Hall, C.B.; Siders, W.A. Validation of tetrapolar bioelectrical impedance method to assess human body composition. J. Appl. Physiol. 1986, 60, 1327–1332. [Google Scholar] [CrossRef]
- Malavolti, M.; Mussi, C.; Poli, M.; Fantuzzi, A.; Salvioli, G.; Battistini, N.; Bedogni, G. Cross-calibration of eight-polar bioelectrical impedance analysis versus dual-energy X-ray absorptiometry for the assessment of total and appendicular body composition in healthy subjects aged 21–82 years. Ann. Hum. Biol. 2003, 30, 380–391. [Google Scholar] [CrossRef] [PubMed]
- Foster, K.R.; Lukaski, H.C. Whole-body impedance—What does it measure? Am. J. Clin. Nutr. 1996, 64, 388S–396S. [Google Scholar] [CrossRef] [PubMed]
- Omron-Healthcare. Body Fat Monitor HBF-306. Available online: https://images-eu.ssl-images-amazon.com/images/I/91U2Mvk%2B9cS.pdf (accessed on 10 May 2019).
- InBody. Body Composition Analyzer Inbody-720. Available online: https://inbody.com/eng/product/inbody720.aspx (accessed on 10 May 2019).
- Tanita. Body Fat Scales. Available online: https://www.tanita.com/en/body-water-monitors-fat-scales/ (accessed on 10 May 2019).
- Jung, M.H.; Namkoong, K.; Lee, Y.; Koh, Y.J.; Eom, K.; Jang, H.; Bae, J.; Park, J. Wrist-wearable bioelectrical impedance analyzer with contact resistance compensation function. In Proceedings of the 2016 IEEE SENSORS, Orlando, FL, USA, 30 October–3 November 2016; pp. 1–3. [Google Scholar]
- Inbody. InBodyBAND2. Available online: https://www.inbody.com/global/product/InBodyBAND_2.aspx (accessed on 10 May 2019).
- Kyle, U.G.; Bosaeus, I.; De Lorenzo, A.D.; Deurenberg, P.; Elia, M.; Gómez, J.M.; Heitmann, B.L.; Kent-Smith, L.; Melchior, J.C.; Pirlich, M.; et al. Bioelectrical impedance analysis Part I: Review of principles and methods. Clin. Nutr. 2004, 23, 1226–1243. [Google Scholar] [CrossRef] [PubMed]
- Jia, W.; Lu, J.; Xiang, K.; Bao, Y.; Lu, H.; Chen, L. Prediction of abdominal visceral obesity from body mass index, waist circumference and waist-hip ratio in Chinese adults: Receiver operating characteristic curves analysis. Biomed. Environ. Sci. BES 2003, 16, 206–211. [Google Scholar] [PubMed]
- Brook, R.D.; Bard, R.L.; Rubenfire, M.; Ridker, P.M.; Rajagopalan, S. Usefulness of visceral obesity (waist/hip ratio) in predicting vascular endothelial function in healthy overweight adults. Am. J. Cardiol. 2001, 88, 1264–1269. [Google Scholar] [CrossRef]
- Wang, J.; Thornton, J.C.; Russell, M.; Burastero, S.; Heymsfield, S.; Pierson, R.N., Jr. Asians have lower body mass index (BMI) but higher percent body fat than do whites: Comparisons of anthropometric measurements. Am. J. Clin. Nutr. 1994, 60, 23–28. [Google Scholar] [CrossRef]
- Lukaski, H.C. Methods for the assessment of human body composition: Traditional and new. Am. J. Clin. Nutr. 1987, 46, 537–556. [Google Scholar] [CrossRef] [PubMed]
- Durnin, J.; Rahaman, M.M. The assessment of the amount of fat in the human body from measurements of skinfold thickness. Br. J. Nutr. 1967, 21, 681–689. [Google Scholar] [CrossRef] [PubMed]
- Heyward, V. ASEP methods recommendation: Body composition assessment. J. Exerc. Physiol. Online 2001, 4, 1–12. [Google Scholar]
- Fürstenberg, A.; Davenport, A. Comparison of multifrequency bioelectrical impedance analysis and dual-energy X-ray absorptiometry assessments in outpatient hemodialysis patients. Am. J. Kidney Dis. 2011, 57, 123–129. [Google Scholar] [CrossRef]
- Mialich, M.S.; Sicchieri, J.F.; Junior, A.A.J. Analysis of body composition: A critical review of the use of bioelectrical impedance analysis. Int. J. Clin. Nutr. 2014, 2, 1–10. [Google Scholar]
- Segal, K.R.; Burastero, S.; Chun, A.; Coronel, P.; Pierson, R.N., Jr.; Wang, J. Estimation of extracellular and total body water by multiple-frequency bioelectrical-impedance measurement. Am. J. Clin. Nutr. 1991, 54, 26–29. [Google Scholar] [CrossRef] [PubMed]
- O’brien, C.; Young, A.; Sawka, M. Bioelectrical impedance to estimate changes in hydration status. Int. J. Sports Med. 2002, 23, 361–366. [Google Scholar] [CrossRef]
- Talma, H.; Chinapaw, M.; Bakker, B.; HiraSing, R.; Terwee, C.; Altenburg, T. Bioelectrical impedance analysis to estimate body composition in children and adolescents: A systematic review and evidence appraisal of validity, responsiveness, reliability and measurement error. Obes. Rev. 2013, 14, 895–905. [Google Scholar] [CrossRef]
- Haroun, D.; Taylor, S.J.; Viner, R.M.; Hayward, R.S.; Darch, T.S.; Eaton, S.; Cole, T.J.; Wells, J.C. Validation of bioelectrical impedance analysis in adolescents across different ethnic groups. Obesity 2010, 18, 1252–1259. [Google Scholar] [CrossRef] [PubMed]
- Kyle, U.G.; Genton, L.; Karsegard, L.; Slosman, D.O.; Pichard, C. Single prediction equation for bioelectrical impedance analysis in adults aged 20–94 years. Nutrition 2001, 17, 248–253. [Google Scholar] [CrossRef]
- Lohman, T.G. Advances in body composition assessment. Med. Sci. Sports Exerc. 1993, 25, 762. [Google Scholar] [CrossRef]
- Kotler, D.P.; Burastero, S.; Wang, J.; Pierson, R. Prediction of body cell mass, fat-free mass, and total body water with bioelectrical impedance analysis: Effects of race, sex, and disease. Am. J. Clin. Nutr. 1996, 64, 489S–497S. [Google Scholar] [CrossRef]
- Deurenberg, P.; Leenen, R.; Weststrate, J.; Seidell, J. Sex and age specific prediction formulas for estimating body composition from bioelectrical impedance: A cross-validation study. Int. J. Obes. 1991, 15, 17–25. [Google Scholar]
- Boulier, A.; Fricker, J.; Thomasset, A.L.; Apfelbaum, M. Fat-free mass estimation by the two-electrode impedance method. Am. J. Clin. Nutr. 1990, 52, 581–585. [Google Scholar] [CrossRef]
- Stolarczyk, L.M.; Heyward, V.H.; Hicks, V.L.; Baumgartner, R.N. Predictive accuracy of bloelectrical impedance in estimating body composition of Native American women. Am. J. Clin. Nutr. 1994, 59, 964–970. [Google Scholar] [CrossRef]
- Sun, S.S.; Chumlea, W.C.; Heymsfield, S.B.; Lukaski, H.C.; Schoeller, D.; Friedl, K.; Kuczmarski, R.J.; Flegal, K.M.; Johnson, C.L.; Hubbard, V.S. Development of bioelectrical impedance analysis prediction equations for body composition with the use of a multicomponent model for use in epidemiologic surveys. Am. J. Clin. Nutr. 2003, 77, 331–340. [Google Scholar] [CrossRef] [PubMed]
- Heitmann, B. Prediction of body water and fat in adult Danes from measurement of electrical impedance. A validation study. Int. J. Obes. 1990, 14, 789–802. [Google Scholar]
- Choi, A.; Kim, J.Y.; Jo, S.; Jee, J.H.; Heymsfield, S.B.; Bhagat, Y.A.; Kim, I.; Cho, J. Smartphone-based bioelectrical impedance analysis devices for daily obesity management. Sensors 2015, 15, 22151–22166. [Google Scholar] [CrossRef] [PubMed]
- Tomtom. Fitness Tracker. Available online: https://www.tomtom.com/en_us/sports/fitness-trackers/fitness-tracker-touch/black-large/ (accessed on 10 May 2019).
- Demura, S.; Sato, S.; Kitabayashi, T. Percentage of total body fat as estimated by three automatic bioelectrical impedance analyzers. J. Physiol. Anthropol. Appl. Hum. Sci. 2004, 23, 93–99. [Google Scholar] [CrossRef]
- Chi, Y.M.; Jung, T.P.; Cauwenberghs, G. Dry-contact and noncontact biopotential electrodes: Methodological review. IEEE Rev. Biomed. Eng. 2010, 3, 106–119. [Google Scholar] [CrossRef] [PubMed]
- Kingma, D.P.; Ba, J. Adam: A method for stochastic optimization. arXiv 2014, arXiv:1412.6980. [Google Scholar]
- Strutz, T. Data Fitting and Uncertainty: A Practical Introduction to Weighted Least Squares and beyond; Vieweg and Teubner: New York, NY, USA, 2010. [Google Scholar]
- Nuzzo, R. Scientific method: Statistical errors. Nat. News 2014, 506, 150. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Items | Unit | Inbody-720 (Reference Device) | HBF-306 | This Work |
|---|---|---|---|---|
| Measurement Point | Whole body | Upper body | Upper body | |
| TX Frequency | kHz | 1, 5, 50, 250, 500, 1000 | 50 | 50 |
| Electrode | EA | 8 | 4 | 4 |
| Output Information | ICW ECW Dry Lean Mass Body Fat Mass | Body Fat Ratio | Body Fat Ratio | |
| Accuracy (PBF) | % | 94% with DEXA [39] |
| Summary | Basketball | Kendo | Ice Hockey | Baseball | Rugby | General | |
|---|---|---|---|---|---|---|---|
| 102 | 9 | 13 | 10 | 22 | 32 | 16 | |
| Height (cm) | 178.0 ± 7.2 | 190.0 ± 7.2 | 172.0 ± 7.7 | 176.9 ± 3.7 | 176.4 ± 4.7 | 179.6 ± 6.4 | 174.5 ± 5.7 |
| Age (year) | 21.3 ± 3.1 | 20.3 ± 1.6 | 19.1 ± 0.6 | 20.1 ± 1.1 | 21.0 ± 3.1 | 20.1 ± 1.4 | 26.2 ± 3.0 |
| Weight (kg) | 83.6 ± 13.0 | 84.6 ± 10.6 | 70.5 ± 8.3 | 81.7 ± 4.8 | 79.4 ± 10.4 | 93.1 ± 15.0 | 78.7 ± 9.8 |
| Waist (cm) | 83.5 ± 7.8 | 79.0 ± 3.6 | 78.5 ± 5.2 | 83.1 ± 4.0 | 82.2 ± 7.7 | 86.2 ± 14.0 | 81.4 ± 6.7 |
| Hip (cm) | 100.7 ± 6.4 | 97.8 ± 8.6 | 94.6 ± 4.5 | 102.8 ± 1.8 | 99.4 ± 5.2 | 104.4 ± 6.8 | 99.2 ± 5.0 |
| BF (%) | 17.9 ± 5.9 | 10.0 ± 2.7 | 15.3 ± 3.7 | 18.1 ± 2.9 | 17.3 ± 4.2 | 21.6 ± 6.8 | 18.3 ± 5.1 |
| BMI | 26.3 ± 3.5 | 23.3 ± 1.9 | 23.8 ± 1.8 | 26.2 ± 1.7 | 25.5 ± 3.1 | 28.8 ± 4.2 | 25.8 ± 2.6 |
| Correlation* | 0.8385 | 0.0489 | 0.4925 | 0.6574 | 0.7690 | 0.8797 | 0.9491 |
| Summary | Basketball | Kendo | Taekwondo | Judo | Table Tennis | General | |
|---|---|---|---|---|---|---|---|
| 61 | 8 | 4 | 14 | 23 | 6 | 6 | |
| Height (cm) | 165.2 ± 6.2 | 167.0 ± 4.6 | 166.0 ± 3.0 | 167.3 ± 5.1 | 163.8 ± 8.0 | 161.6 ± 3.5 | 166.9 ± 4.2 |
| Age (year) | 20.2 ± 2.4 | 20.9 ± 1.7 | 20.0 ± 1.4 | 19.1 ± 1.2 | 20.0 ± 1.4 | 20.2 ± 1.3 | 24.6 ± 6.1 |
| Weight (kg) | 65.4 ± 13.5 | 66.2 ± 9.5 | 62.6 ± 3.1 | 61.1 ± 9.4 | 72.0 ± 17.7 | 55.8 ± 6.0 | 62.4 ± 4.6 |
| Waist (cm) | 74.2 ± 8.8 | 73.3 ± 6.5 | 71.8 ± 3.5 | 70.4 ± 6.9 | 77.9 ± 10.0 | 73.6 ± 5.9 | 73.7 ± 13.2 |
| Hip (cm) | 97.7 ± 6.5 | 100.0 ± 5.9 | 95.0 ± 2.5 | 96.8 ± 5.4 | 99.8 ± 7.9 | 92.9 ± 5.0 | 95.4 ± 3.3 |
| BF (%) | 25.2 ± 6.0 | 26.8 ± 7.6 | 21.4 ± 4.2 | 23.2 ± 5.4 | 26.8 ± 6.7 | 25.8 ± 4.8 | 23.5 ± 4.5 |
| BMI | 24.1 ± 4.3 | 24.9 ± 5.2 | 22.7 ± 1.7 | 21.8 ± 3.3 | 26.6 ± 4.6 | 21.4 ± 2.3 | 23.0 ± 1.6 |
| Correlation* | 0.9201 | 0.9479 | 0.9909 | 0.9086 | 0.9337 | 0.9344 | 0.7773 |
| Network 1 | Network 2 | |
|---|---|---|
| () | (PBF) | |
| Training Set | 143 (male: 93, female: 50) | |
| Test Set | 20 (male: 10, female: 10) | |
| Input layer | 7 | 8 |
| Hidden layer | 3 | 3 |
| Output layer | 1 | 1 |
| Hidden node | 128 × 128 × 128 | 256 × 256 × 256 |
| Activation function | ReLU | |
| Optimizer | Adam Optimizer [41] (beta1 = 0.9, beta2 = 0.999, epsilon = 1 × 10) | |
| Cost function | Mean square error (MSE) | |
| Number of training cycles | maximum = 2000 (Early stopping adopted) | |
| Conventional Features | Proposed Features | |||
|---|---|---|---|---|
| Coefficient | p-Value | Coefficient | p-Value | |
| Intercept | 59.6240 | <0.0001 | −16.2929 | 0.6774 |
| Age | −0.0992 | 0.2170 | −0.1302 | 0.1059 |
| Gender | 7.4604 | <0.0001 | 7.5189 | <0.0001 |
| Height | −0.4174 | <0.0001 | −0.4005 | <0.0001 |
| Weight | 0.4673 | <0.0001 | 0.3763 | <0.0001 |
| −0.4217 | <0.0001 | −0.4021 | <0.0001 | |
| Waist | – | – | −0.6804 | 0.1224 |
| Hip | – | – | 0.7177 | 0.0674 |
| Waist to Hip | – | – | 78.5731 | 0.0837 |
| Case | Methods | Input Dimension | Detailed Information |
|---|---|---|---|
| Conventional | Regression | 5 | H, A, G, W, _5 |
| Estimated Impedance | Regression | 5 | H, A, G, W, _prop |
| Model I | DNN (Network1) | 5 | H, A, G, W, _prop |
| Model II | DNN (Network1) | 6 | H, A, G, W, _prop, H/Imp |
| Model III | DNN (Network1) | 7 | H, A, G, W, _prop, H/Imp, W/H |
| Conventional | Estimated Imp. | Model I | Model II | Model III | |
|---|---|---|---|---|---|
| Correlation* | 0.8420 | 0.9008 | 0.9344 | 0.9338 | 0.9403 |
| Improvement [%] | - | 37.2 | 58.4 | 58.1 | 62.2 |
| Initial | Methods | Input Dim. | Detailed Information |
|---|---|---|---|
| Lconv | Regression | 5 | H, A, G, W, H2/ |
| Lprop | Regression | 8 | H, A, G, W, H2/, hip Circ., waist Circ., waist/hip |
| DNNconv | DNN (Network2) | 5 | H, A, G, W, |
| DNNprop | DNN (Network2) | 8 | H, A, G, W, , hip Circ., waist Circ., waist/hip |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shin, S.-C.; Lee, J.; Choe, S.; Yang, H.I.; Min, J.; Ahn, K.-Y.; Jeon, J.Y.; Kang, H.-G. Dry Electrode-Based Body Fat Estimation System with Anthropometric Data for Use in a Wearable Device. Sensors 2019, 19, 2177. https://doi.org/10.3390/s19092177
Shin S-C, Lee J, Choe S, Yang HI, Min J, Ahn K-Y, Jeon JY, Kang H-G. Dry Electrode-Based Body Fat Estimation System with Anthropometric Data for Use in a Wearable Device. Sensors. 2019; 19(9):2177. https://doi.org/10.3390/s19092177
Chicago/Turabian StyleShin, Seung-Chul, Jinkyu Lee, Soyeon Choe, Hyuk In Yang, Jihee Min, Ki-Yong Ahn, Justin Y. Jeon, and Hong-Goo Kang. 2019. "Dry Electrode-Based Body Fat Estimation System with Anthropometric Data for Use in a Wearable Device" Sensors 19, no. 9: 2177. https://doi.org/10.3390/s19092177
APA StyleShin, S.-C., Lee, J., Choe, S., Yang, H. I., Min, J., Ahn, K.-Y., Jeon, J. Y., & Kang, H.-G. (2019). Dry Electrode-Based Body Fat Estimation System with Anthropometric Data for Use in a Wearable Device. Sensors, 19(9), 2177. https://doi.org/10.3390/s19092177