Identification of Human Pathological Mitral Chordae Tendineae Using Polarization-sensitive Optical Coherence Tomography

 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Mitral Chordae Dpecimens
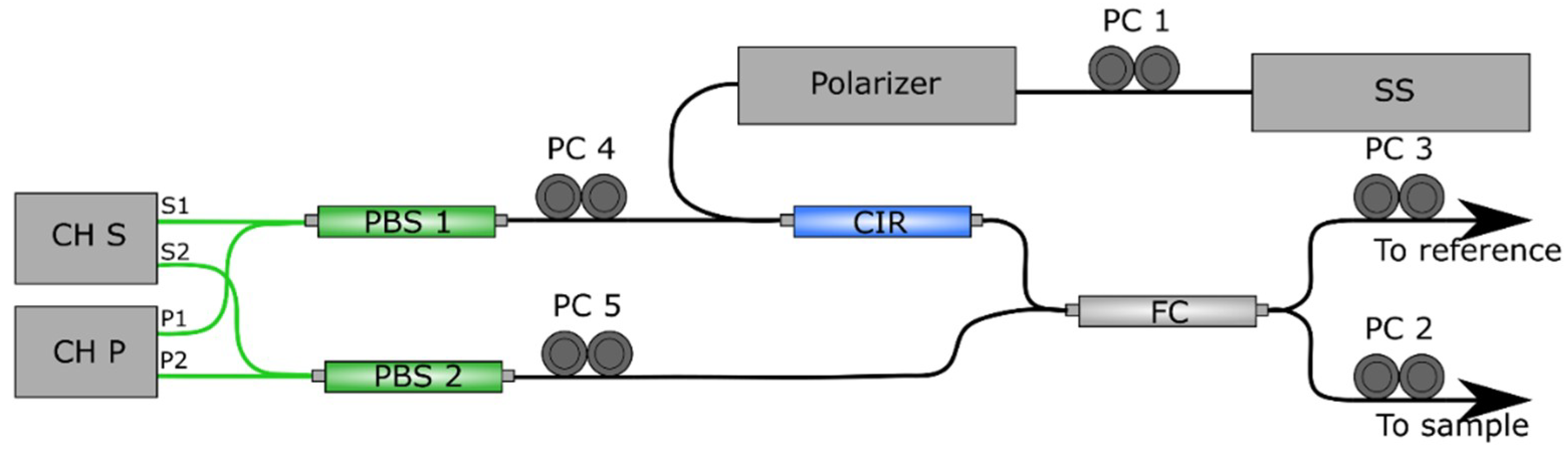
2.2. Polarization Sensitive Optical Coherence Tomography
2.3. Birefringence with PS-OCT
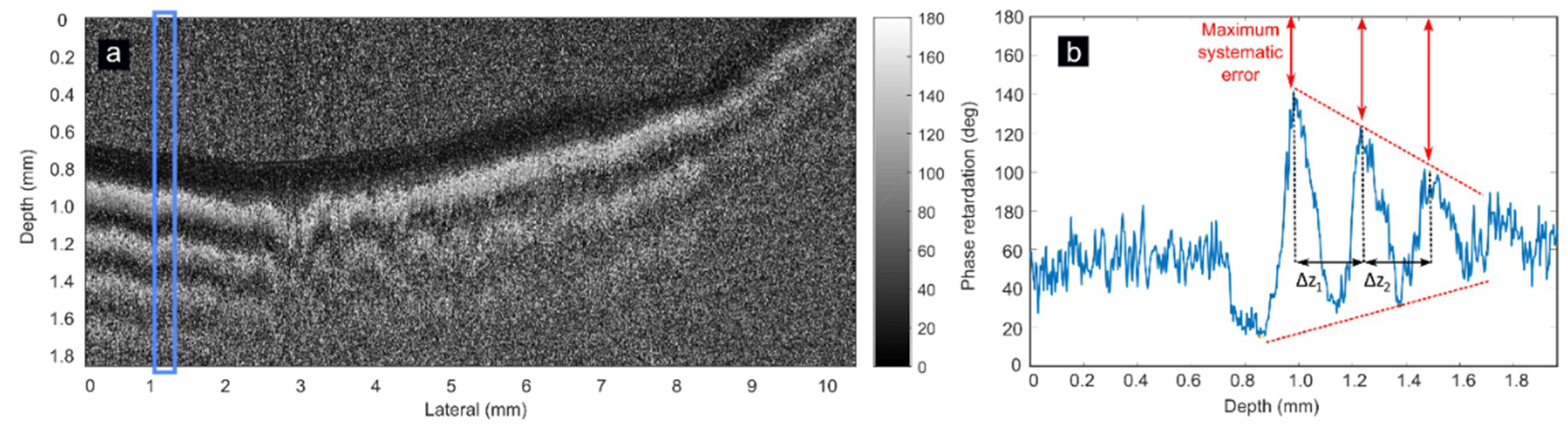
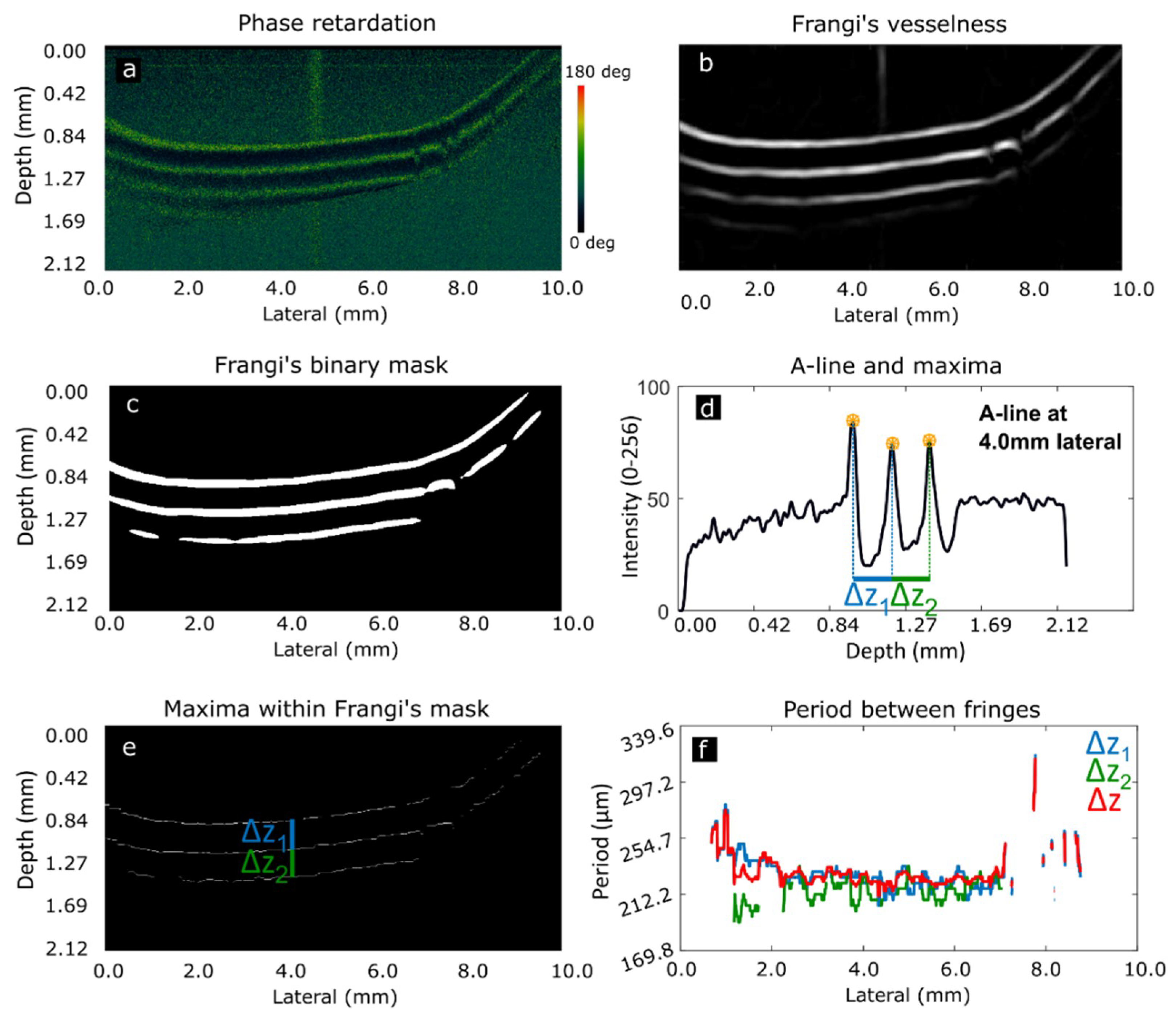
2.4. Image Processing
2.5. Scanning Electron Microscopy
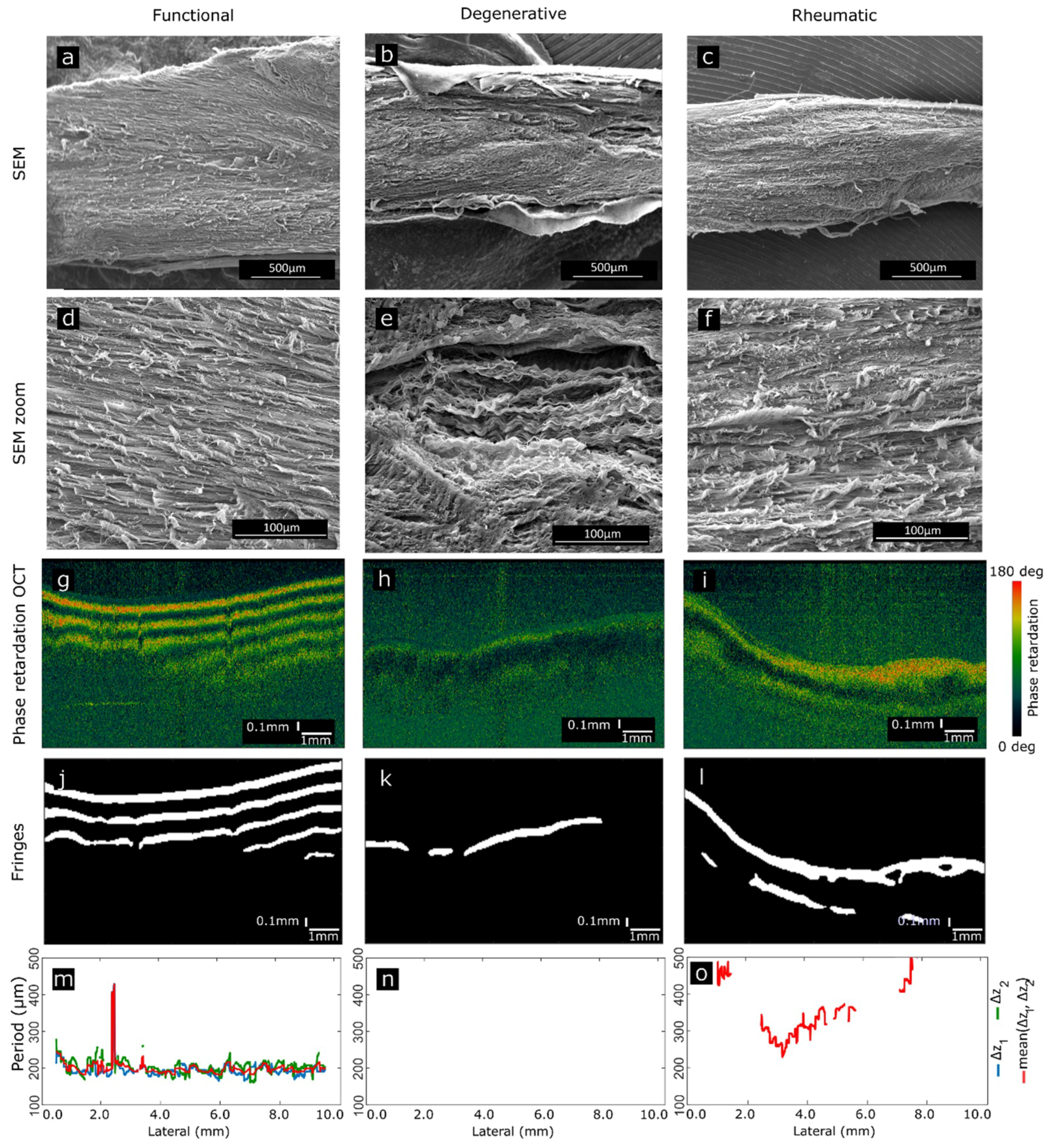
3. Results and Discussion
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Mick, S.L.; Keshavamurthy, S.; Gillinov, A.M. Mitral valve repair versus replacement. Ann. Cardiothorac. Surg. 2015, 4, 230–237. [Google Scholar] [PubMed]
- McCarthy, K.P.; Ring, L.; Rana, B.S. Anatomy of the mitral valve: understanding the mitral valve complex in mitral regurgitation. Eur. J. Echocardiogr. 2010, 11, i3–i9. [Google Scholar] [CrossRef] [PubMed]
- Millington-Sanders, C.; Meir, A.; Lawrence, L.; Stolinski, C. Structure of chordae tendineae in the leftventricle of the human heart. J. Anat. 1998, 192, 573–581. [Google Scholar] [CrossRef]
- Icardo, J.M.; Colvee, E.; Revuelta, J.M. Structural analysis of chordae tendineae in degenerative disease of the mitral valve. Int. J. Cardiol. 2012, 167, 1603–1609. [Google Scholar] [CrossRef]
- Gabbay, U.; Yosefy, C. The underlying causes of chordae tendineae rupture: A systematic review. Int. J. Cardiol. 2010, 143, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, R.A.; Otto, C.M.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., 3rd; Fleisher, L.A.; Jneid, H.; Mack, M.J.; McLeod, C.J.; O’Gara, P.T.; et al. 2017 AHA/ACC Focused Update of the 2014 AHA/ACC Guideline for the Management of Patients with Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2017, 135, e1159–e1195. [Google Scholar] [CrossRef]
- Lancellotti, P.; Moura, L.; Pierard, L.A.; Agricola, E.; Popescu, B.A.; Tribouilloy, C.; Hagendorff, A.; Monin, J.L.; Badano, L.; Zamorano, J.L. European Association of Echocardiography recommendations for the assessment of valvular regurgitation. Part 2: mitral and tricuspid regurgitation (native valve disease). Eur. J. Echocardiogr. 2010, 11, 307–332. [Google Scholar] [CrossRef]
- Gunnal, S.A.; Wabale, R.N.; Farooqui, M.S. Morphological study of chordae tendinae in human cadaveric hearts. Heart Views 2015, 16, 1–12. [Google Scholar] [CrossRef]
- Revuelta, J.M. La reparación de la insuficiencia mitral entre 2 orillas. Mitral valve repair between 2 shores. Cir. Cardiov. 2015, 22, 5–9. [Google Scholar]
- Revuelta, J.M.; García-Rinaldi, R.; Gaite, L.; Val, F.; Garijo, F. Generation of chordae tendineae with polytetrafluoroethylene stents: Results of mitral valve chordae replacement in sheep. J. Thorac. Cardiovasc. Surg. 1989, 103, 98–103. [Google Scholar]
- Bernal, J.M.; Rabasa, J.M.; Olalla, J.J.; Carrión, M.F.; Alonso, A.; Revuelta, J.M. Repair of chordae tendineae for rheumatic mitral valve disease. A twenty-year experience. J. Thorac. Cardiov. Sur. 1996, 111, 211–217. [Google Scholar] [CrossRef]
- Hee, M.R.; Huang, D.; Swanson, E.A.; Fujimoto, J.G. Polarization-sensitive low-coherence reflectometer for birefringence characterization and ranging. J. Opt. Soc. Am. B 1992, 9, 903–908. [Google Scholar] [CrossRef]
- De Boer, J.F.; Milner, T.E.; van Gemert, M.J.; Nelson, J.S. Two-dimensional birefringence imaging in biological tissue by polarization-sensitive optical coherence tomography. Opt. Lett. 1997, 22, 934–936. [Google Scholar] [CrossRef] [PubMed]
- De Boer, J.F.; Milner, T.E. Review of polarization sensitive optical coherence tomography and Stokes vector determination. J. Biomed. Opt. 2002, 7, 359–371. [Google Scholar] [CrossRef] [PubMed]
- Hitzenberger, C.K.; Götzinger, E.; Sticker, M.; Pircher, M.; Fercher, A.F. Measurement and Imaging of Birefringence and Optic Axis Orientation by Phase Resolved Polarization Sensitive Optical Coherence Tomography. Opt. Exp. 2001, 9, 780–790. [Google Scholar] [CrossRef]
- Nadkarni, S.K.; Pierce, M.C.; Park, B.H.; de Boer, J.F.; Whittaker, P.; Bouma, B.E.; Bressner, J.E.; Halpern, E.; Houser, S.L.; Tearney, G.J. Measurement of collagen and smooth muscle cell content in atherosclerotic plaques using polarization-sensitive optical coherence tomography. J. Am. Coll. Cardiol. 2007, 49, 1474–1481. [Google Scholar] [CrossRef] [PubMed]
- Ignatieva, N.Y.; Zakharkina, O.L.; Sobol, E.N.; Lunin, V.V.; Kamensky, V.A.; Andreeva, I.V.; Averkiev, S.V.; Myakov, A.V. Changes in the Structure of Collagen in the Annulus Fibrosus under Thermal or IR-Laser Treatment. Dokl. Biochem. Biophys. 2007, 413, 92–94. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.; Chen, W.; Delgado, S.; Liu, Y.; Lin, Y.; Wang, J. Altered Birefringence of Peripapillary Retinal Nerve Fiber Layer in Multiple Sclerosis Measured by Polarization Sensitive Optical Coherence Tomography. Eye Vis. 2018, 5, 14. [Google Scholar] [CrossRef] [PubMed]
- Orfanoudaki, I.M.; Kappou, D.; Sifakis, S. Recent Advances in Optical Imaging for Cervical Cancer Detection. Arch. Gynecol. Obstet. 2011, 284, 1197. [Google Scholar] [CrossRef]
- Verma, Y.; Gautam, M.; Rao, K.D.; Swami, M.K.; Gupta, P.K. Imaging of Human Breast Tissue Using Polarization Sensitive Optical Coherence Tomography. Laser Phys. 2011, 21, 2143–2148. [Google Scholar] [CrossRef]
- Van Manen, L.; Dijkstra, J.; Boccara, C.; Benoit, E.; Vahrmeijer, A.L.; Gora, M.J.; Mieog, J.S.D. The Clinical Usefulness of Optical Coherence Tomography during Cancer Interventions. J. Cancer. Res. Clin. Oncol. 2018, 144, 1967–1990. [Google Scholar] [CrossRef]
- Whittaker, P.; Boughner, D.R.; Perkins, D.G.; Canham, P.B. Quantitative structural analysis of collagen in chordae tendineae and its relation to floppy mitral valves and proteoglycan infiltration. Br. Heart J. 1987, 57, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Real, E.; Revuelta, J.M.; Pontón, A.; Calvo-Díez, M.; López-Higuera, J.M.; Conde, O.M. OCT inspection of degenerative and rheumatic tendinous chords. In European Conference on Biomedical Optics; Optical Society of America: Munich, Germany, 2017; p. 104110W. [Google Scholar]
- Chin, L.; Yang, X.; McLaughlin, R.A.; Noble, P.B.; Sampson, D.D. En face parametric imaging of tissue birefringence using polarization-sensitive optical coherence tomography. J. Biomed. Opt. 2013, 18, 066005. [Google Scholar] [CrossRef] [PubMed]
- Adie, S.G.; Hillman, T.R.; Sampson, D.D. Detection of multiple scattering in optical coherence tomography using the spatial distribution of Stokes vectors. Opt. Express 2007, 15, 18033–18049. [Google Scholar] [CrossRef] [PubMed]
- De Boer, J.F.; Hitzenberger, C.K.; Yasuno, Y. Polarization sensitive optical coherence tomography—A review. Biomed. Opt. Express 2017, 8, 1838–1873. [Google Scholar] [CrossRef]
- Trasischker, W.; Zotter, S.; Torzicky, T.; Baumann, B.; Haindl, R.; Pircher, M.; Hitzenberger, C.K. Single input state polarization sensitive swept source optical coherence tomography based on an all single mode fiber interferometer. Biomed. Opt. Express 2014, 5, 2798–2809. [Google Scholar] [CrossRef] [PubMed]
- Lippok, N.; Villiger, M.; Jun, C.; Bouma, B.E. Single input state, single-mode fiber-based polarization-sensitive optical frequency domain imaging by eigenpolarization referencing. Opt. Lett. 2015, 40, 2025–2028. [Google Scholar] [CrossRef]
- Sugiyama, S.; Hong, Y.J.; Kasaragod, D.; Makita, S.; Uematsu, S.; Ikuno, Y.; Miura, M.; Yasuno, Y. Birefringence imaging of posterior eye by multi-functional Jones matrix optical coherence tomography. Biomed. Opt. Express 2015, 6, 4951–4974. [Google Scholar] [CrossRef]
- Park, B.H.; Pierce, M.C.; Cense, B.; Yun, S.H.; Mujat, M.; Tearney, G.J.; Bouma, B.E.; de Boer, J.F. Real-time fiber-based multi-functional spectral-domain optical coherence tomography at 1.3 µm. Opt. Express 2005, 13, 3931–3944. [Google Scholar] [CrossRef]
- Duan, L.; Makita, S.; Yamanari, M.; Lim, Y.; Yasuno, Y. Monte-Carlo-based phase retardation estimator for polarization sensitive optical coherence tomography. Opt. Express 2011, 19, 16330–16345. [Google Scholar] [CrossRef]
- Xie, T.; Guo, S.; Zhang, J.; Chen, Z.; Peavy, G.M. Use of polarization-sensitive optical coherence tomography to determine the directional polarization sensitivity of articular cartilage and meniscus. J. Biomed. Opt. 2006, 11, 64001. [Google Scholar] [CrossRef] [PubMed]
- Fan, C.; Yao, G. Correcting Optical-Axis Calculation in Polarization-Sensitive Optical Coherence Tomography. IEEE Trans. Biomed. Eng. 2010, 57, 2556–2559. [Google Scholar] [PubMed]
- Fan, C.; Yao, G. Mapping local retardance in birefringent samples using polarization sensitive optical coherence tomography. Opt. Lett. 2012, 37, 1415–1417. [Google Scholar] [CrossRef] [PubMed]
- Schoenenberger, K.; Colston, B.W.; Maitland, D.J.; Da Silva, L.B.; Everett, M.J. Mapping of birefringence and thermal damage in tissue by use of polarization-sensitive optical coherence tomography. Appl. Opt. 1998, 37, 6026–6036. [Google Scholar] [CrossRef]
- Tearney, G.J.; Brezinski, M.E.; Southern, J.F.; Bouma, B.E.; Hee, M.R.; Fujimoto, J.G. Determination of the refractive index of highly scattering human tissue by optical coherence tomography. Opt. Lett. 1995, 20, 2258–2260. [Google Scholar] [CrossRef] [PubMed]
- Real, E.; Revuelta, J.M.; González-Vargas, N.; Pontón, A.; Calvo-Díez, M.; López-Higuera, J.M.; Conde, O.M. Collagen birefringence assessment in heart chordae tendineae through PS-OCT. Proc. SPIE Conf. 2017, 10053, 1005334. [Google Scholar]
- Real, E.; Val-Bernal, J.F.; Revuelta, J.M.; Pontón, A.; Calvo-Díez, M.; Mayorga, M.; López-Higuera, J.M.; Conde, O.M. Hessian analysis for the delineation of amorphous anomalies in optical coherence tomography images of the aortic wall. Biomed. Opt. Express 2016, 7, 1415–1429. [Google Scholar] [CrossRef]
- Frangi, A.F.; Niessen, W.J.; Hoogeveen, R.M.; van Walsum, T.; Viergever, M.A. Model-based quantitation of 3-D magnetic resonance angiographic images. IEEE Trans. Med. Imaging 1999, 18, 946–956. [Google Scholar] [CrossRef]
- Kroon, D.J. Hessian based Frangi Vesselness filter. Available online: http://www.mathworks.com/matlabcentral/fileexchange/24409-hessian-based-frangi-vesselness-filter (accessed on 12 March 2018).
- Baumann, B. Polarization Sensitive Optical Coherence Tomography: A Review of Technology and Applications. Appl. Sci. 2017, 7, 474. [Google Scholar] [CrossRef]
- Villiger, M.; Otsuka, K.; Karanasos, A.; Doradla, P.; Ren, J.; Lippok, N.; Shishkov, M.; Daemen, J.; Diletti, R.; van Geuns, R.J.; et al. Coronary Plaque Microstructure and Composition Modify Optical Polarization: A New Endogenous Contrast Mechanism for Optical Frequency Domain Imaging. JACC Cardiovasc. Imaging 2018, 11, 1666–1676. [Google Scholar] [CrossRef]
- Xiong, Q.; Tong, X.; Deng, C.; Zhang, C.; Wang, P.; Zheng, Z.; Liu, F. A Novel Mach-Zehnder Interferometer Using Eccentric-Core Fiber Design for Optical Coherence Tomography. Sensors 2018, 18, 1540. [Google Scholar] [CrossRef] [PubMed]
- Cho, N.; Park, K.; Wijesinghe, R.; Shin, Y.; Jung, W.; Kim, J. Development of Real-Time Dual-Display Handheld and Bench-Top Hybrid-Mode SD-OCTs. Sensors 2014, 14, 2171–2181. [Google Scholar] [CrossRef] [PubMed]
- Casado, J.A.; Diego, S.; Ferreño, D.; Ruiz, E.; Carrascal, I.; Méndez, D.; Revuelta, J.M.; Pontón, A.; Icardo, J.M.; Gutiérrez-Solana, F. Determination of the Mechanical Properties of Normal and Calcified Human Mitral Chordae Tendineae. J. Mech. Behav. Biomed. Mater. 2012, 13, 1–13. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Functional | Degenerative | Rheumatic | |
|---|---|---|---|
| N010 (4) | N025 (1) | N029 (4) | |
| N024 (2) | N031 (5) | N030 (1) | |
| N027 (4) | N038 (1) | N032 (5) | |
| N033 (2) | N040 (1) | N044 (2) | |
| N034 (4) | N041 (1) | N046 (3) | |
| N043 (4) | N049 (5) | V002 (2) | |
| N045 (2) | N052 (4) | V004 (1) | |
| Y002 (2) | |||
| Y004 (1) | |||
| Total | 9 (25) | 7 (18) | 7 (18) |
| Author | Tissue | Method | Birefringence |
|---|---|---|---|
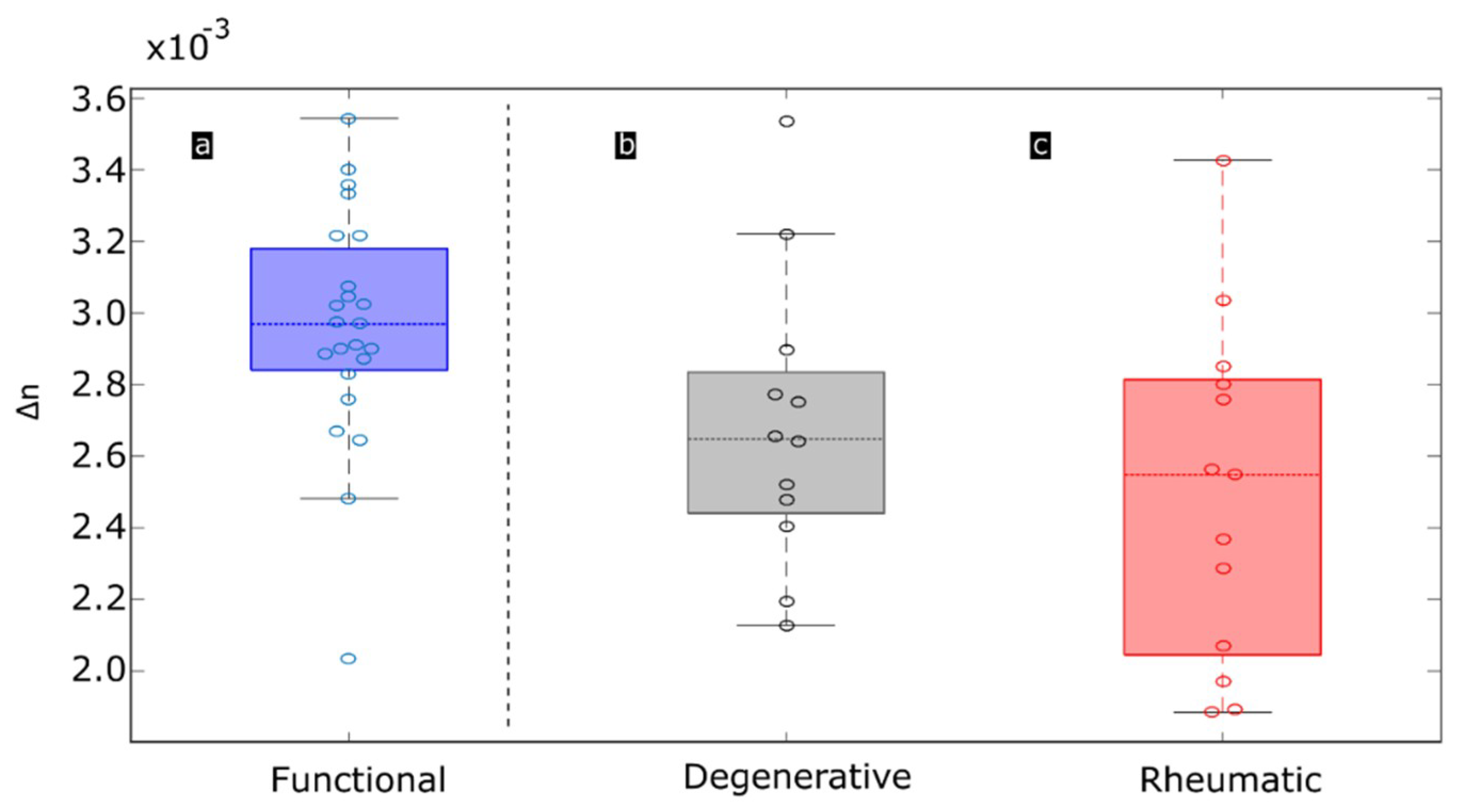
| This work | Human chordae tendineae | PS-OCT (Proposed) | 1.9·10−3 (pathological) to 3.6·10−3 (functional) |
| De Boer et al. [13] | Bovine tendon | PS-OCT | 3.7·10−3 |
| Chin et al. [24] | Porcine tendon | PS-OCT | 4.0·10−3 |
| Whittaker et al. [22] | Human chordae tendineae | Sénarmont’s method | 3.8·10−3 (pathological) to 4.7·10−3 (functional) (*) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Real, E.; Icardo, J.M.; Fernández-Barreras, G.; Revuelta, J.M.; Calvo Díez, M.; Pontón, A.; Gutiérrez, J.F.; López Higuera, J.M.; Conde, O.M. Identification of Human Pathological Mitral Chordae Tendineae Using Polarization-sensitive Optical Coherence Tomography. Sensors 2019, 19, 543. https://doi.org/10.3390/s19030543
Real E, Icardo JM, Fernández-Barreras G, Revuelta JM, Calvo Díez M, Pontón A, Gutiérrez JF, López Higuera JM, Conde OM. Identification of Human Pathological Mitral Chordae Tendineae Using Polarization-sensitive Optical Coherence Tomography. Sensors. 2019; 19(3):543. https://doi.org/10.3390/s19030543
Chicago/Turabian StyleReal, Eusebio, José Manuel Icardo, Gaspar Fernández-Barreras, José Manuel Revuelta, Marta Calvo Díez, Alejandro Pontón, José Francisco Gutiérrez, José Miguel López Higuera, and Olga María Conde. 2019. "Identification of Human Pathological Mitral Chordae Tendineae Using Polarization-sensitive Optical Coherence Tomography" Sensors 19, no. 3: 543. https://doi.org/10.3390/s19030543
APA StyleReal, E., Icardo, J. M., Fernández-Barreras, G., Revuelta, J. M., Calvo Díez, M., Pontón, A., Gutiérrez, J. F., López Higuera, J. M., & Conde, O. M. (2019). Identification of Human Pathological Mitral Chordae Tendineae Using Polarization-sensitive Optical Coherence Tomography. Sensors, 19(3), 543. https://doi.org/10.3390/s19030543