Sensors for Expert Grip Force Profiling: Towards Benchmarking Manual Control of a Robotic Device for Surgical Tool Movements †


Abstract
1. Introduction
2. Materials and Methods
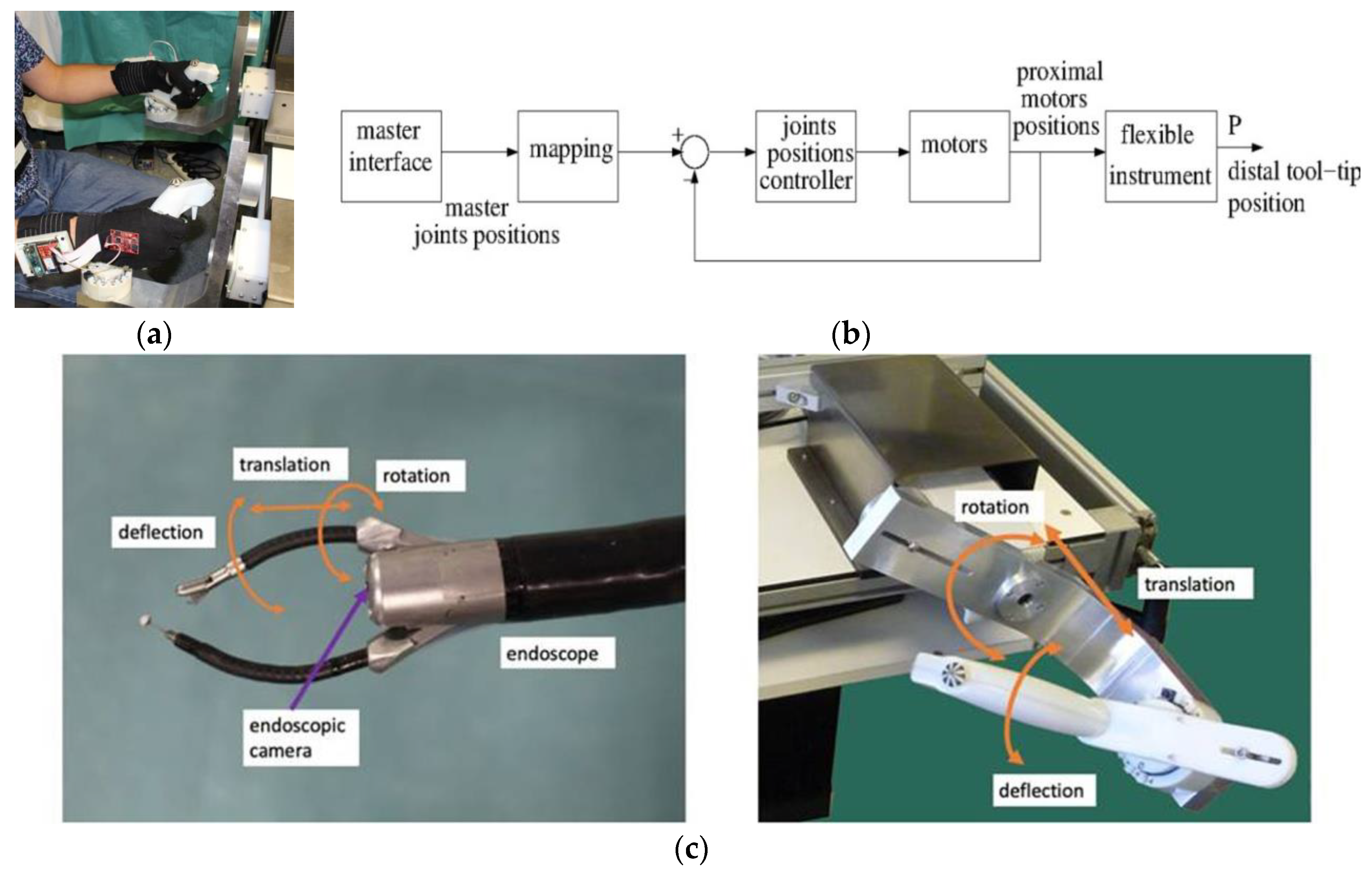
2.1. Slave Robotic System
2.2. Master/Slave Control
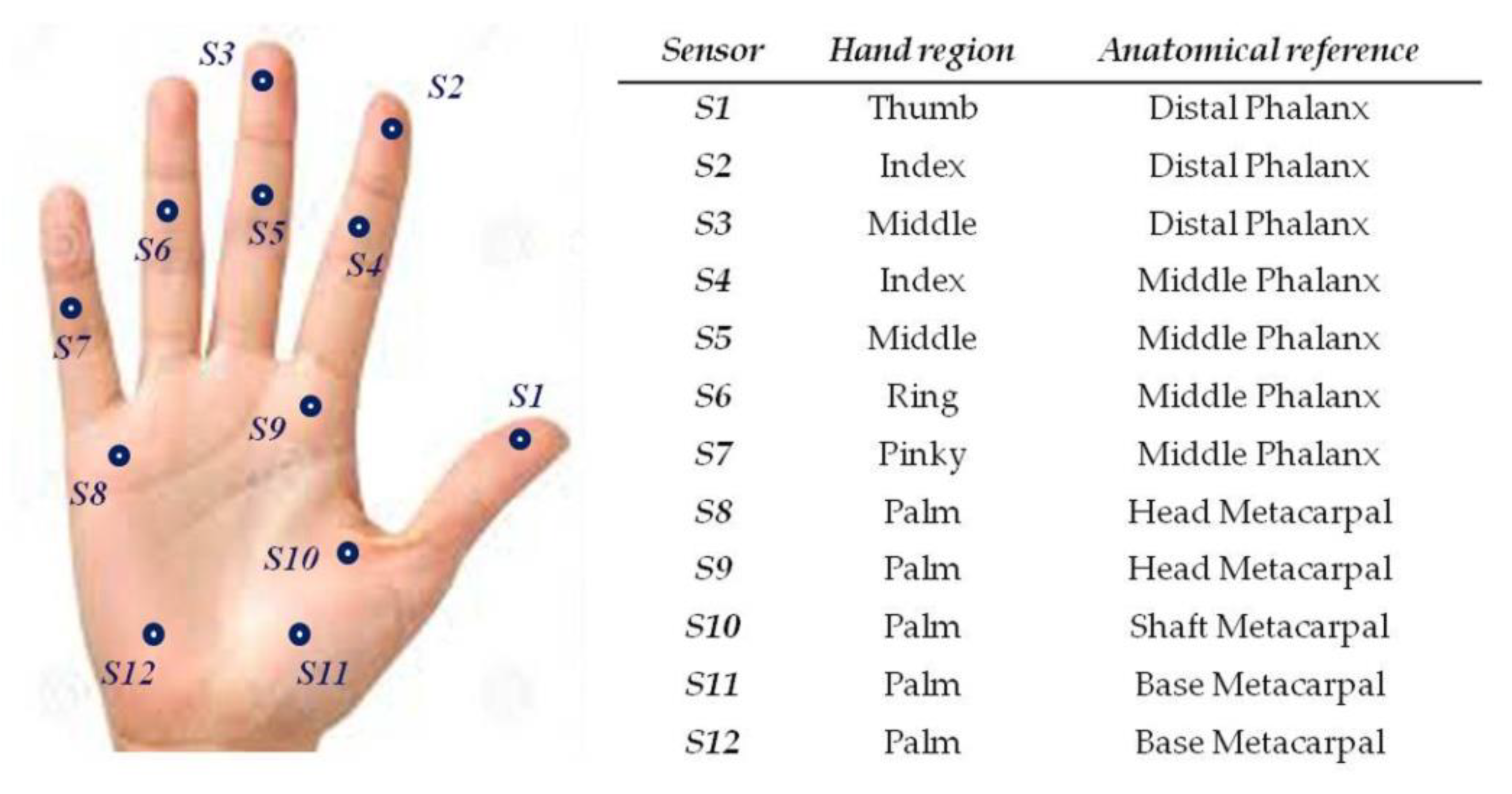
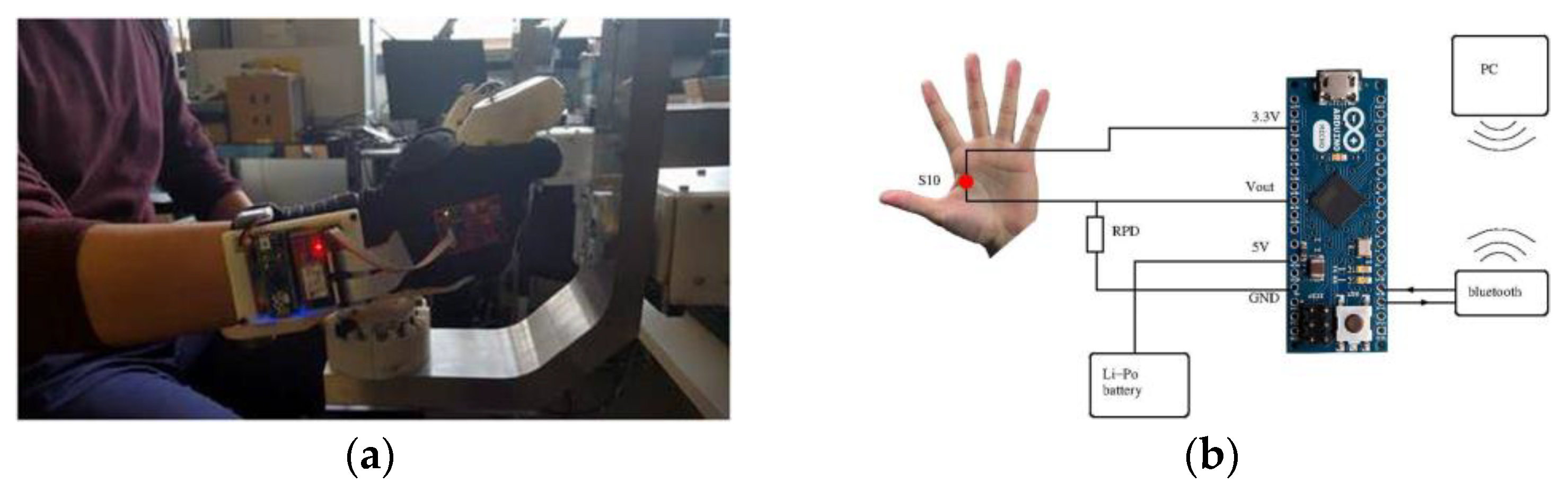
2.3. Glove Design for Grip Force Profiling
2.3.1. Hardware
2.3.2. Software
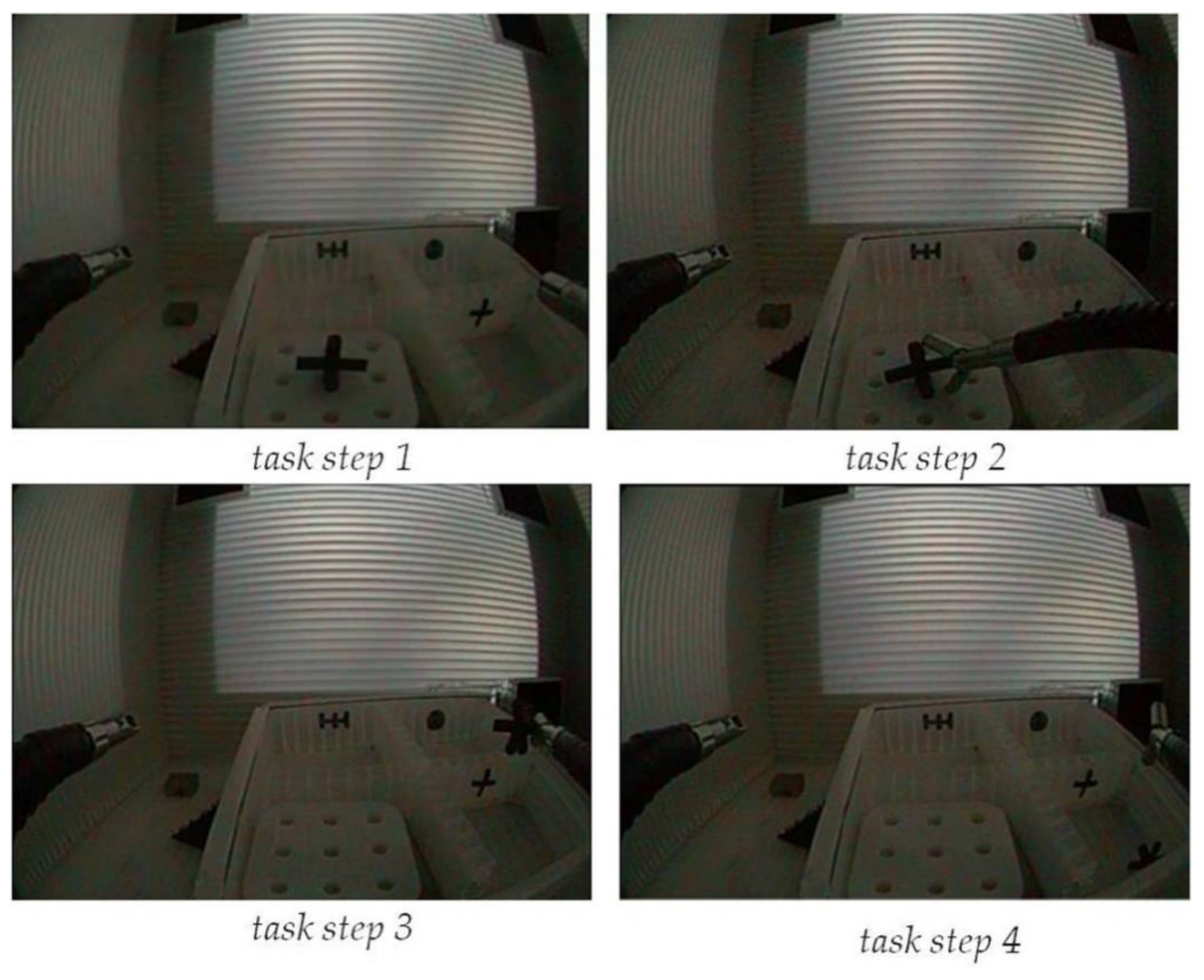
2.4. Experimental Task Design
3. Results
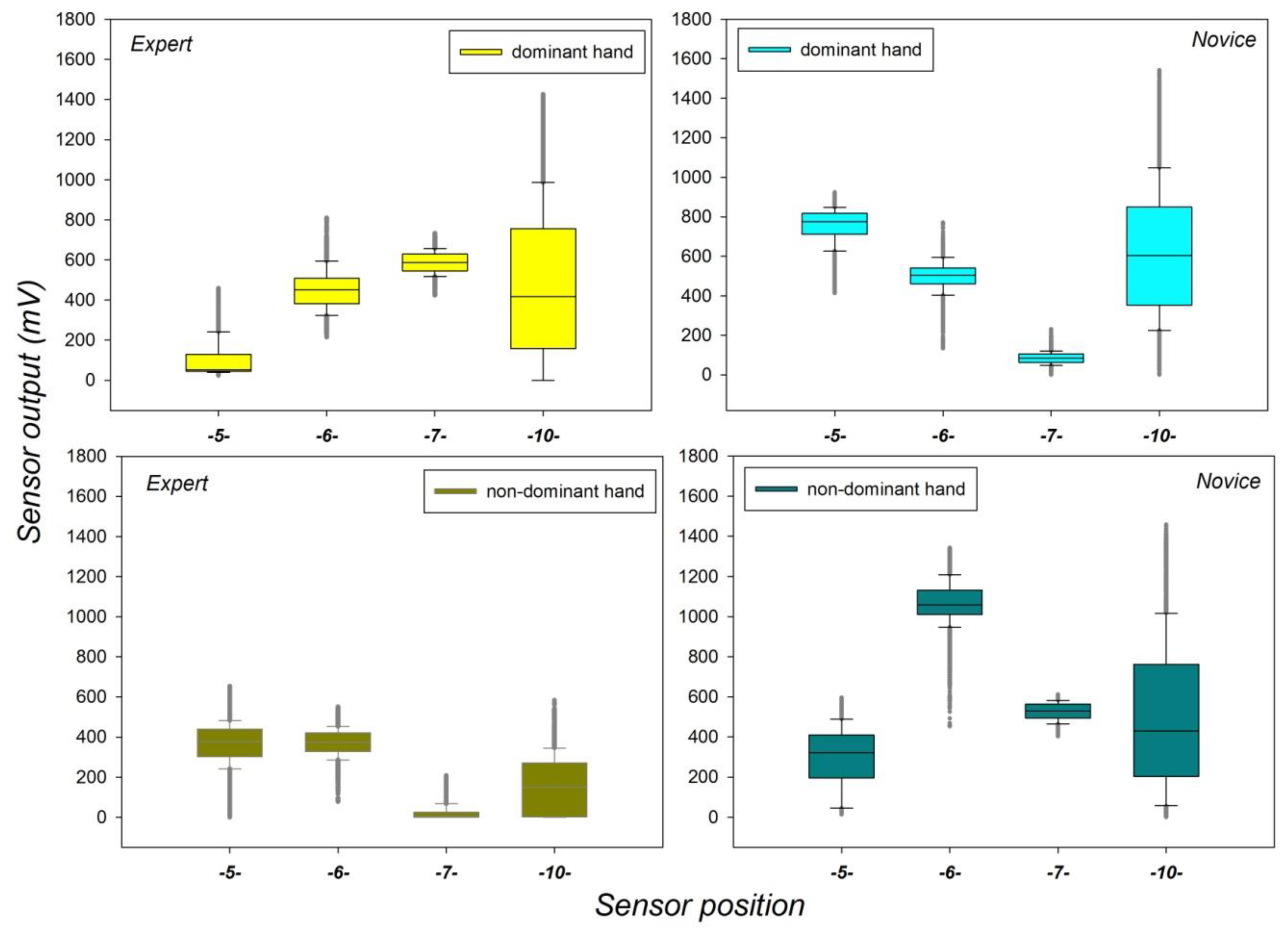
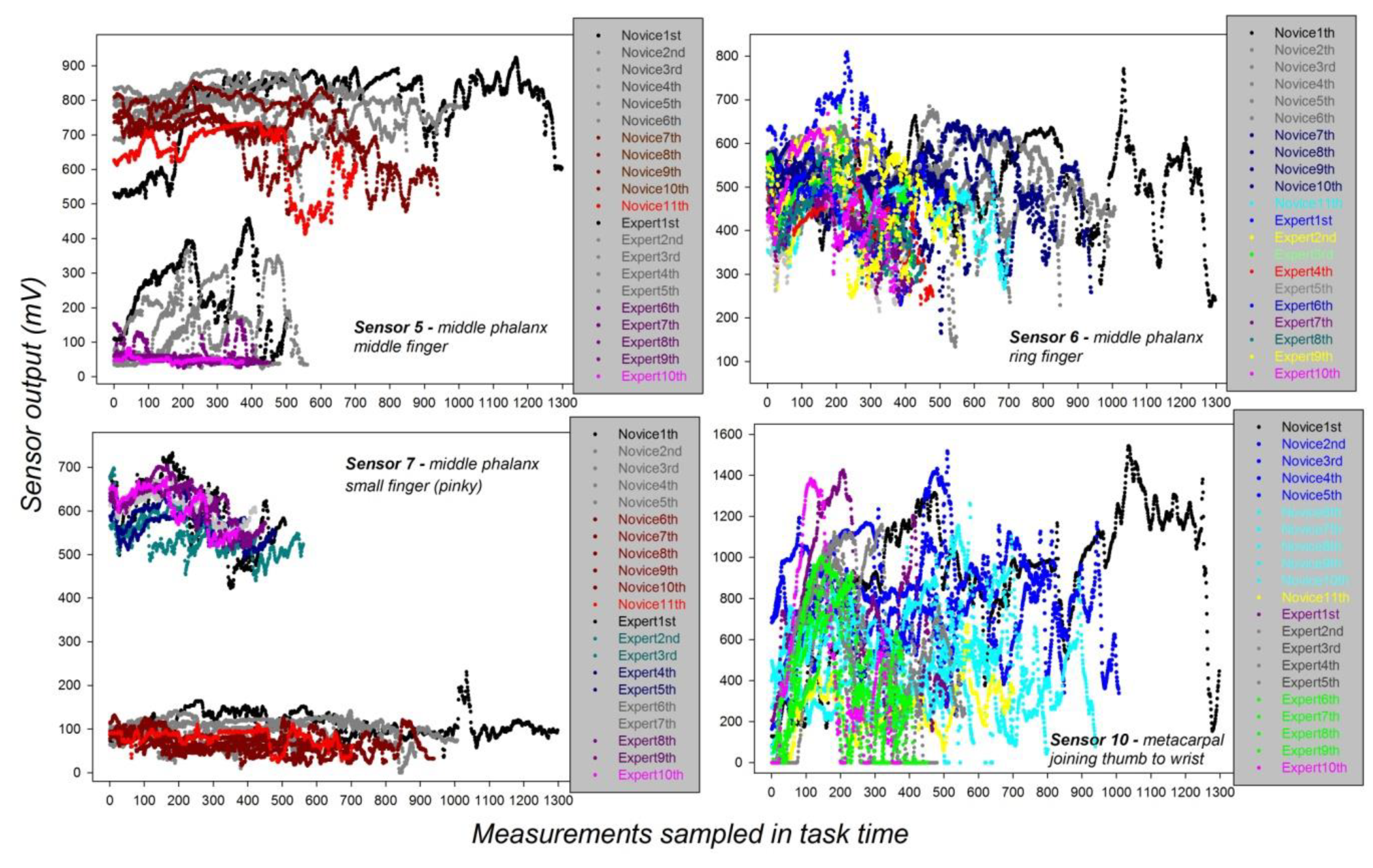
3.1. Dynamic Grip Force Range in the Expert and Novice Data at Selected Sensor Locations
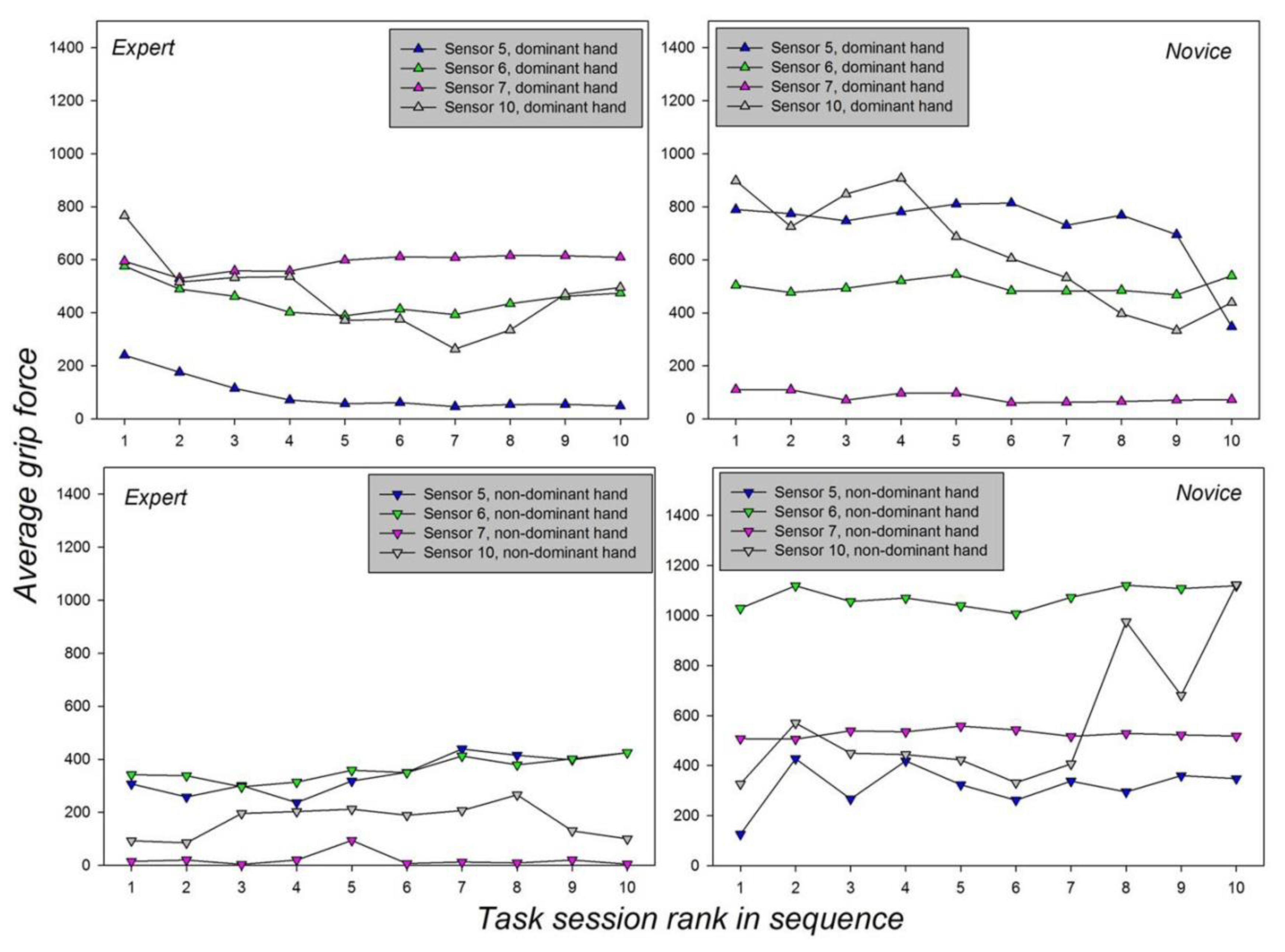
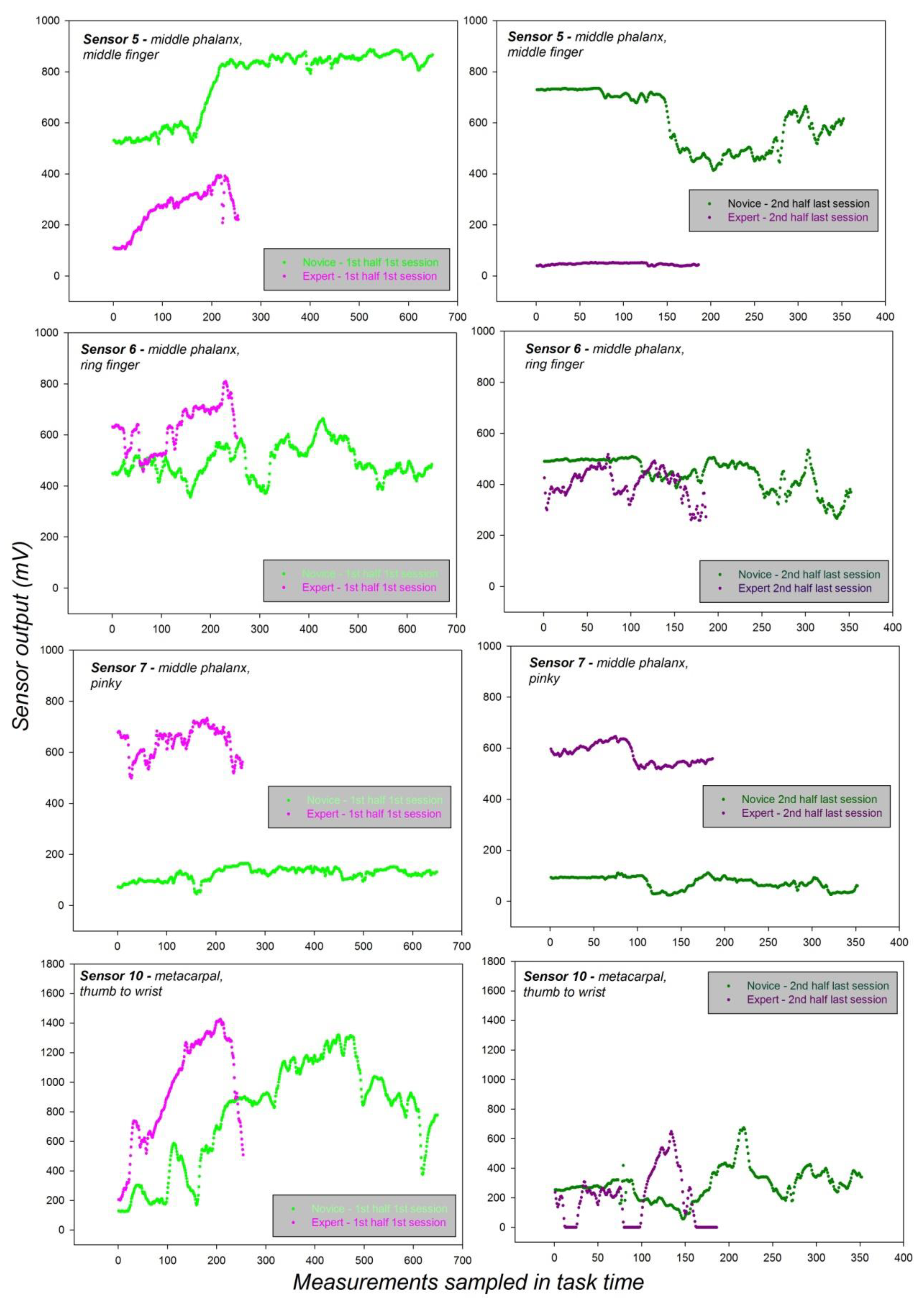
3.2. Individual Sensor-Specific Effects of Task Session and Handedness with Interactions
3.3. Effects of Expertise as a Function of Sensor Position
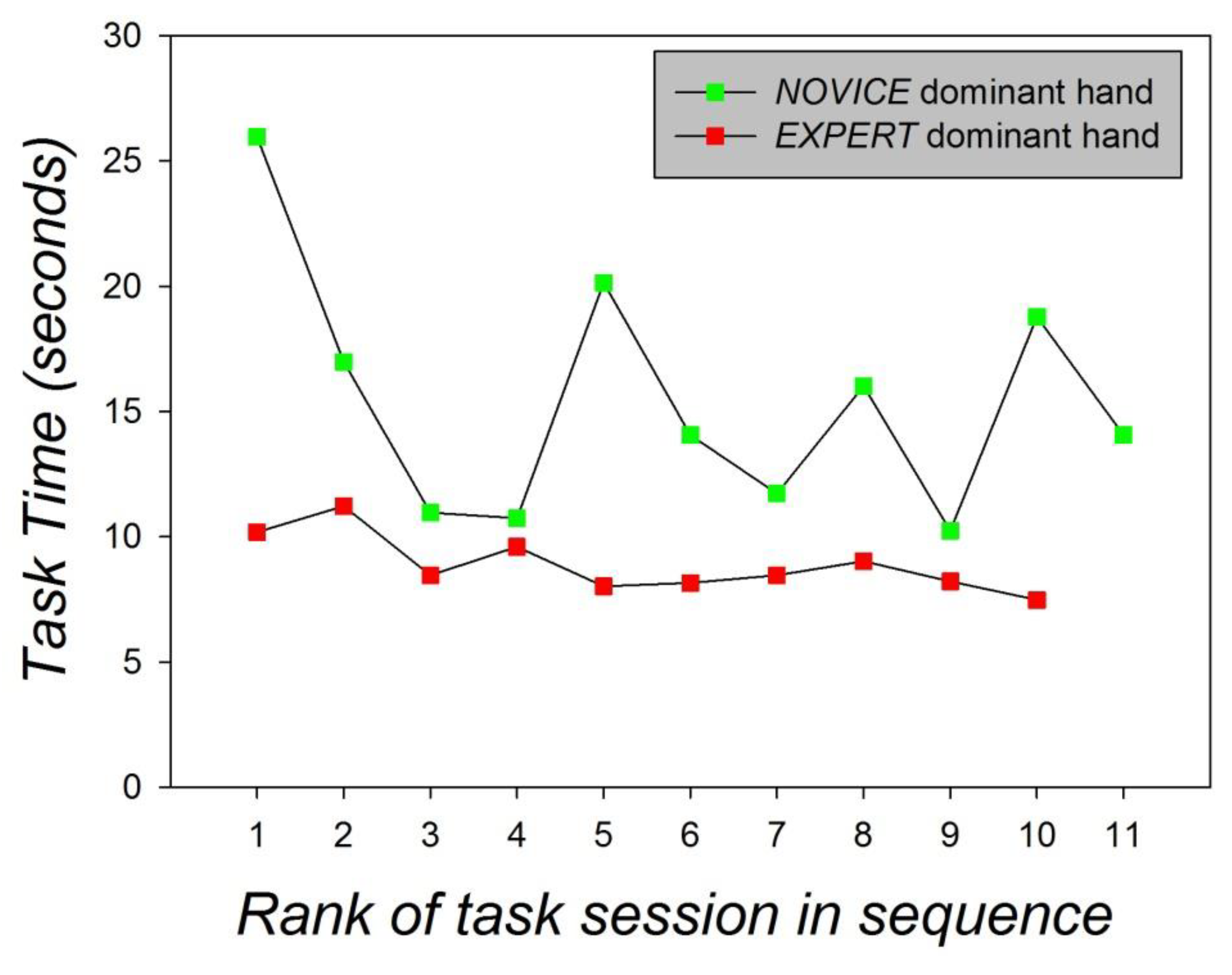
3.4. Task Times and Quantitative/Qualitative Analysis of the Task Videos
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Thompson, C.C.; Ryou, M.; Soper, N.J.; Hungess, E.S.; Rothstein, R.I.; Swanstrom, L.L. Evaluation of a manually driven, multitasking platform for complex endoluminal and natural orifice transluminal endoscopic surgery applications (with video). Gastrointest. Endosc. 2009, 70, 121–125. [Google Scholar] [CrossRef] [PubMed]
- Swanstrom, L.L.; Kozarek, R.; Pasricha, P.J.; Gross, S.; Birkett, D.; Park, P.O.; Saadat, V.; Ewers, R.; Swain, P. Development of a new access device for transgastric surgery. J Gastrointest. Surg. 2005, 9, 1129–1137. [Google Scholar] [CrossRef] [PubMed]
- Phee, S.J.; Low, S.C.; Huynh, V.A.; Kencana, A.P.; Sun, Z.L.; Yang, K. Master and slave transluminal endoscopic robot (MASTER) for natural orifice transluminal endoscopic surgery (NOTES). In Proceedings of the 31st Annual International Conference of the IEEE Engineering in Medicine and Biology Society: Engineering the Future of Biomedicine, Minneapolis, MN, USA, 3–6 September 2009; pp. 1192–1195. [Google Scholar]
- Zorn, L.; Nageotte, F.; Zanne, P.; Legner, A.; Dallemagne, B.; Marescaux, J.; de Mathelin, M. A novel telemanipulated robotic assistant for surgical endoscopy: Preclinical application to ESD. IEEE Trans. Biomed. Eng. 2018, 65, 797–808. [Google Scholar] [CrossRef] [PubMed]
- Dallemagne, B.; Marescaux, J. The ANUBISTM Project. Minim. Invasive Ther. Allied Technol. 2010, 19, 257–261. [Google Scholar] [CrossRef] [PubMed]
- De Donno, A.; Nageotte, F.; Zanne, P.; Zorn, L.; de Mathelin, M. Master/slave control of flexible instruments for minimally invasive surgery. In Proceedings of the IEEE/RSJ International Conference on Intelligent Robots and Systems, Tokyo, Japan, 3–7 November 2013; pp. 483–489. [Google Scholar]
- Chitwood, W.R.; Nifong, L.W.; Chapman, W.H.; Felger, J.E.; Bailey, B.M.; Ballint, T.; Mendelson, K.G.; Kim, V.B.; Young, J.; Albrecht, R. Robotic surgical training in an academic institution. Ann. Surg. 2001, 234, 475–484. [Google Scholar] [CrossRef] [PubMed]
- King, C.H.; Culjat, M.O.; Franco, M.L.; Lewis, C.E.; Dutson, E.P.; Grundfest, W.S.; Bisley, J.W. Tactile feedback induces reduced grasping force in robot-assisted surgery. IEEE Trans. Haptics 2009, 2, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Farnè, A.; Làdavas, E. Dynamic size-change of hand peripersonal space following tool use. Neuroreport 2000, 11, 1645–1649. [Google Scholar] [CrossRef] [PubMed]
- Maravita, A.; Husain, M.; Clarke, K.; Driver, J. Reaching with a tool extends visual–tactile interactions into far space: Evidence from cross-modal extinction. Neuropsychologia 2001, 39, 580–585. [Google Scholar] [CrossRef]
- Wilson, M.R.; McGrath, J.S.; Vine, S.J.; Brewer, J.; Defriend, D.; Masters, R.S.W. Perceptual impairment and psychomotor control in virtual laparoscopic surgery. Surg. Endosc. 2011, 25, 2268–2274. [Google Scholar] [CrossRef] [PubMed]
- Sarlegna, F.; Blouin, J.; Bresciani, J.P.; Bourdin, C.; Vercher, J.L.; Gauthier, G.M. Target and hand position information in the online control of goal-directed arm movements. Exp. Brain Res. 2003, 151, 524–535. [Google Scholar] [CrossRef] [PubMed]
- Pereira, R.; Moreira, A.H.J.; Leite, M.; Rodrigues, P.L.; Queirós, S.; Rodrigues, N.F.; Leão, P.; Vilaça, J.L. Hand-held robotic device for laparoscopic surgery and training. In Proceedings of the IEEE International Conference on Serious Games and Applications for Health, Rio de Janeiro, Brazil, 14–16 May 2014; pp. 1–8. [Google Scholar]
- Legner, A.; Diana, M.; Halvax, P.; Liu, Y.; Zorn, L.; Zanne, P.; Nageotte, F.; de Mathelin, M.; Dallemagne, B.; Marescaux, J. Endoluminal surgical triangulation 2.0: A new flexible surgical robot. Preliminary pre-clinical results with colonic submucosal dissection. Int. J. Med. Robot. Comput. Assist. Surg. 2017, 13, e1819. [Google Scholar] [CrossRef] [PubMed]
- Mascagni, P.; Lim, S.G.; Fiorillo, C.; Zanne, P.; Nageotte, F.; Zorn, L.; Peretta, S.; de Mathelin, M.; Marescaux, J.; Dallemagne, B. Democratizing endoscopic submucosal dissection: Single-operator fully robotic colorectal ESD in a pig model. Gastroenterology 2019, 156, 1559–1571. [Google Scholar] [CrossRef] [PubMed]
- Batmaz, A.U.; Falek, A.M.; Zorn, L.; Nageotte, F.; Zanne, P.; de Mathelin, M.; Dresp-Langley, B. Novice and expert behavior while using a robot controlled surgery system. In Proceedings of the 2017 13th IASTED International Conference on Biomedical Engineering (BioMed), Innsbruck, Austria, 20–21 February 2017; pp. 94–99. [Google Scholar]
- Cha, S.M.; Shin, H.D.; Kim, K.C.; Park, J.W. Comparison of grip strength among six grip methods. J. Hand Surg. 2014, 39, 2277–2284. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W. Grip strength: A summary of studies comparing dominant and non-dominant limb measurements. Percept. Mot. Skills 2003, 96, 728–730. [Google Scholar] [CrossRef] [PubMed]
- Young, R.W. Evolution of the human hand: The role of throwing and clubbing. J. Anat. 2003, 202, 165–174. [Google Scholar] [CrossRef]
- González, A.G.; Rodríguez, D.R.; Sanz-Calcedo, J.G. Ergonomic analysis of the dimension of a precision tool handle: A case study. Procedia Manuf. 2017, 13, 1336–1343. [Google Scholar] [CrossRef]
- Batmaz, A.U.; de Mathelin, M.; Dresp-Langley, B. Seeing virtual while acting real: Visual display and strategy effects on the time and precision of eye-hand coordination. PLoS ONE 2017, 12, e0183789. [Google Scholar] [CrossRef] [PubMed]
- Dresp-Langley, B. Principles of perceptual grouping: Implications for image-guided surgery. Front. Psychol. 2015, 6, 1565. [Google Scholar] [CrossRef] [PubMed]
- Wandeto, J.M.; Dresp-Langley, B. The quantization error in a Self-Organizing Map as a contrast and color specific indicator of single-pixel change in large random patterns. Neural Netw. 2019, 119, 273–285. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dominant Hand | |||||||||||||
| S1 | S2 | S3 | S4 | S5 | S6 | S7 | S8 | S9 | S10 | S11 | S12 | Sensor | |
| Expert | 0 | 1.4 | 4.5 | 2 | 99 | 452 | 587 | 0 | 0.5 | 474 | 0 | 1.2 | Mean |
| 0 | 0.7 | 1.6 | 1.2 | 89 | 102 | 53 | 0 | 7.7 | 70 | 0 | 1.7 | Std.dev. | |
| Novice | 0 | 23 | 674 | 0.7 | 754 | 498 | 85 | 651 | 1132 | 617 | 847 | 858 | Mean |
| 0 | 150 | 207 | 5.5 | 188 | 74 | 49 | 192 | 483 | 312 | 418 | 280 | Std.dev. | |
| Non-dominant hand | |||||||||||||
| S1 | S2 | S3 | S4 | S5 | S6 | S7 | S8 | S9 | S10 | S11 | S12 | Sensor | |
| Expert | 1 | 0 | 0 | 9 | 364 | 371 | 71 | 109 | 90 | 160 | 825 | 418 | Mean |
| 1.5 | 0 | 0 | 27 | 107 | 68 | 37 | 118 | 170 | 138 | 450 | 250 | Std.dev. | |
| Novice | 0 | 69 | 0 | 0 | 296 | 1063 | 526 | 233 | 0 | 500 | 0 | 0.4 | Mean |
| 0 | 27 | 0 | 0 | 148 | 120 | 64 | 257 | 2 | 365 | 0 | 0.5 | Std.dev. | |
| Expert | ||||
| S5 | S6 | S7 | S10 | |
| Hand | F (1,9685) = 3017; p < 0.001 | F (1,9685) = 3734; p < 0.001 | F (1,9685) = 5745; p < 0.001 | F (1,9685) = 3339; p < 0.001 |
| Session | F (9,9685) = 213; p < 0.001 | F (9,9685) = 209; p < 0.001 | F (9,9685) = 307; p < 0.001 | F (9,9685) = 47; p < 0.001 |
| Hand × Session | F (9,9685) = 747; p < 0.001 | F (9,9685) = 277; p < 0.001 | F (9,9685) = 295; p < 0.001 | F (9,9685) = 138; p < 0.001 |
| Novice | ||||
| S5 | S6 | S7 | S10 | |
| Hand | F (1,13613) = 8655; p < 0.001 | F (1,13613) = 1499; p < 0.001 | F (1,13613) = 6755; p < 0.001 | F (1,13613) = 200; p < 0.001 |
| Session | F (9,13613) = 413; p < 0.001 | F (9,13613) = 102; p < 0.001 | F (9,13613) = 188; p < 0.001 | F (9,13613) = 201; p < 0.001 |
| Hand × Session | F (9,13613) = 677; p < 0.001 | F (9,13613) = 152; p < 0.001 | F (9,13613) = 359; p < 0.001 | F (9,13613) = 1073; p < 0.001 |
| Subject (expertise) | F (1,51692) = 2680; p < 0.001 |
| Sensor | F (3,51692) = 2840; p < 0.001 |
| Subject× Sensor | F (3,51692) = 2569; p < 0.001 |
| Diff of Means | t | Unadjusted P | Critical Level | |
| Expertversus Novice | 655.653 | 198.175 | <0.001 | 0.05 |
| Sensor 6 | Diff of Means | t | Unadjusted P | Critical Level |
| Expertversus Novice | 46.167 | 13.954 | <0.001 | 0.05 |
| Sensor 7 | Diff of Means | t | Unadjusted P | Critical Level |
| Expertversus Novice | 502.306 | 151.825 | <0.001 | 0.05 |
| Sensor 10 | Diff of Means | t | Unadjusted P | Critical Level |
| Expertversus Novice | 14.069 | 43.24 | < 0.001 | 0.05 |
| Group Name | N | Missing | Mean | Stand. Dev. | SEM |
|---|---|---|---|---|---|
| Time Novice | 11 | 0 | 15.424 | 4.832 | 1.457 |
| Time Expert | 10 | 0 | 8882 | 1.141 | 0.361 |
| Difference between means: 6.542 | |||||
| t = 4.168 with 19 degrees of freedom; p ≤ 0.001. | |||||
| 95 percent confidence interval for difference of means: 3.257 to 9.827 | |||||
| Expert | Novice | |
|---|---|---|
| Tool trajectories towards target requiring adjustment | 3 | 20 |
| Number of times object was accidentally released | 0 | 1 |
| Unsuccessful attempts to grasp object | 1 | 8 |
| Tool collisions with task-space boundary | 0 | 2 |
| Number of times object was dropped outside target area | 0 | 1 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Mathelin, M.; Nageotte, F.; Zanne, P.; Dresp-Langley, B. Sensors for Expert Grip Force Profiling: Towards Benchmarking Manual Control of a Robotic Device for Surgical Tool Movements. Sensors 2019, 19, 4575. https://doi.org/10.3390/s19204575
de Mathelin M, Nageotte F, Zanne P, Dresp-Langley B. Sensors for Expert Grip Force Profiling: Towards Benchmarking Manual Control of a Robotic Device for Surgical Tool Movements. Sensors. 2019; 19(20):4575. https://doi.org/10.3390/s19204575
Chicago/Turabian Stylede Mathelin, Michel, Florent Nageotte, Philippe Zanne, and Birgitta Dresp-Langley. 2019. "Sensors for Expert Grip Force Profiling: Towards Benchmarking Manual Control of a Robotic Device for Surgical Tool Movements" Sensors 19, no. 20: 4575. https://doi.org/10.3390/s19204575
APA Stylede Mathelin, M., Nageotte, F., Zanne, P., & Dresp-Langley, B. (2019). Sensors for Expert Grip Force Profiling: Towards Benchmarking Manual Control of a Robotic Device for Surgical Tool Movements. Sensors, 19(20), 4575. https://doi.org/10.3390/s19204575