A RGBD-Based Interactive System for Gaming-Driven Rehabilitation of Upper Limbs †



Abstract
1. Introduction
2. Related Work
3. Materials and Methods
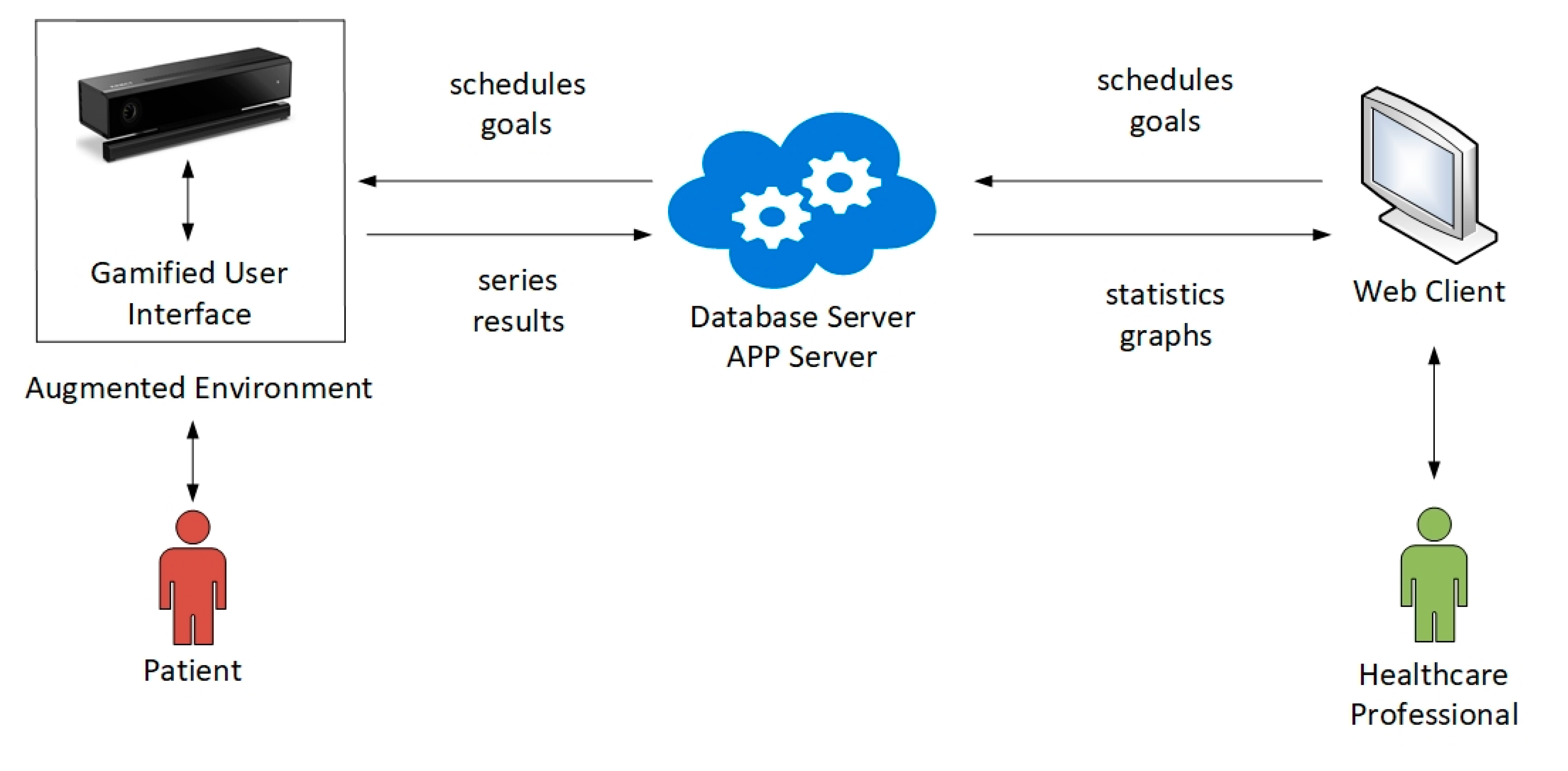
3.1. System Overview
- Calibration. The system captures the patient′s biometric data, and adapts exercises to each patient.
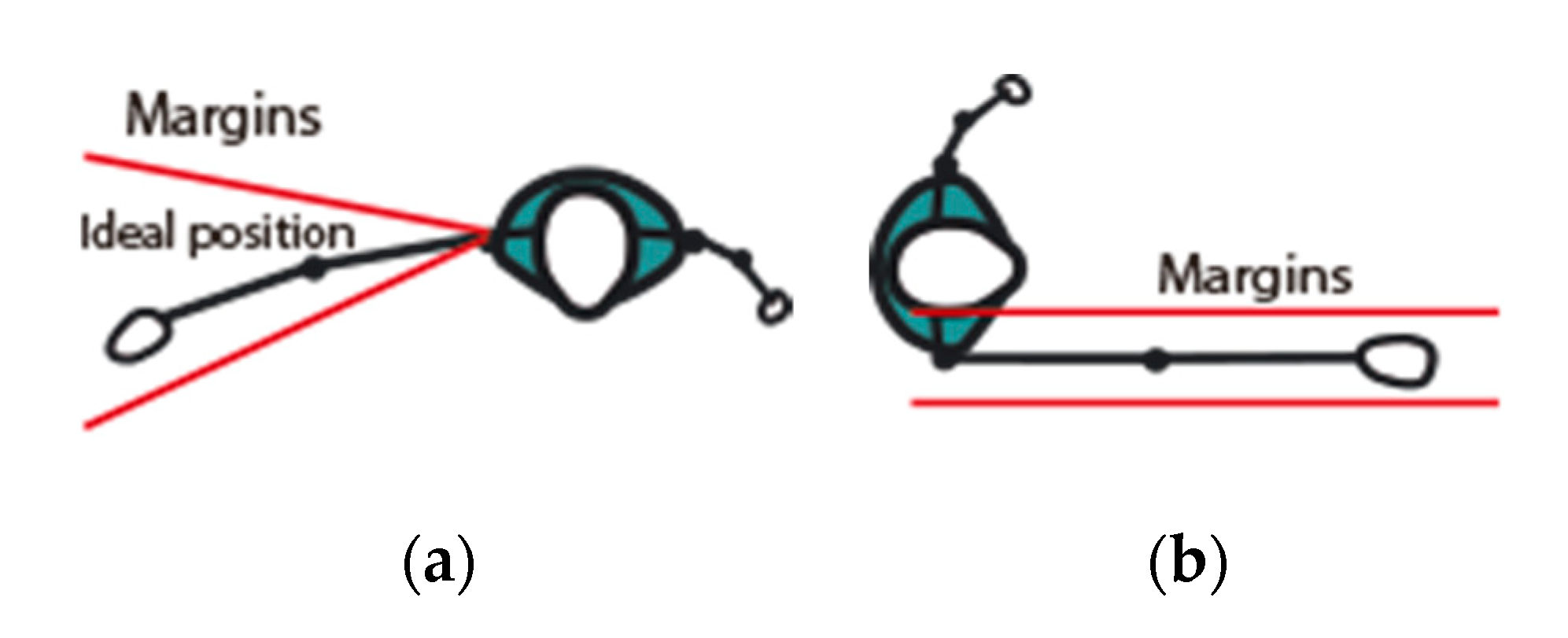
- Execution and control. Depending on the prescribed exercise, the system presents a customized game environment to the patient, where goals are represented through computer-generated visual elements. The patient is encouraged to perform the corresponding exercise. The system checks whether the execution meets the goal, according to configurable tolerance margins. The system provides real-time visual feedback to the patient, indicating to what extent the goal is reached. When the patient does not perform the exercise in a correct way, the system notifies the patient, and allows the patient to continue the series of exercises.
- Data registration. When the execution of an exercise ends, all the series of results are stored in a database located on a server.
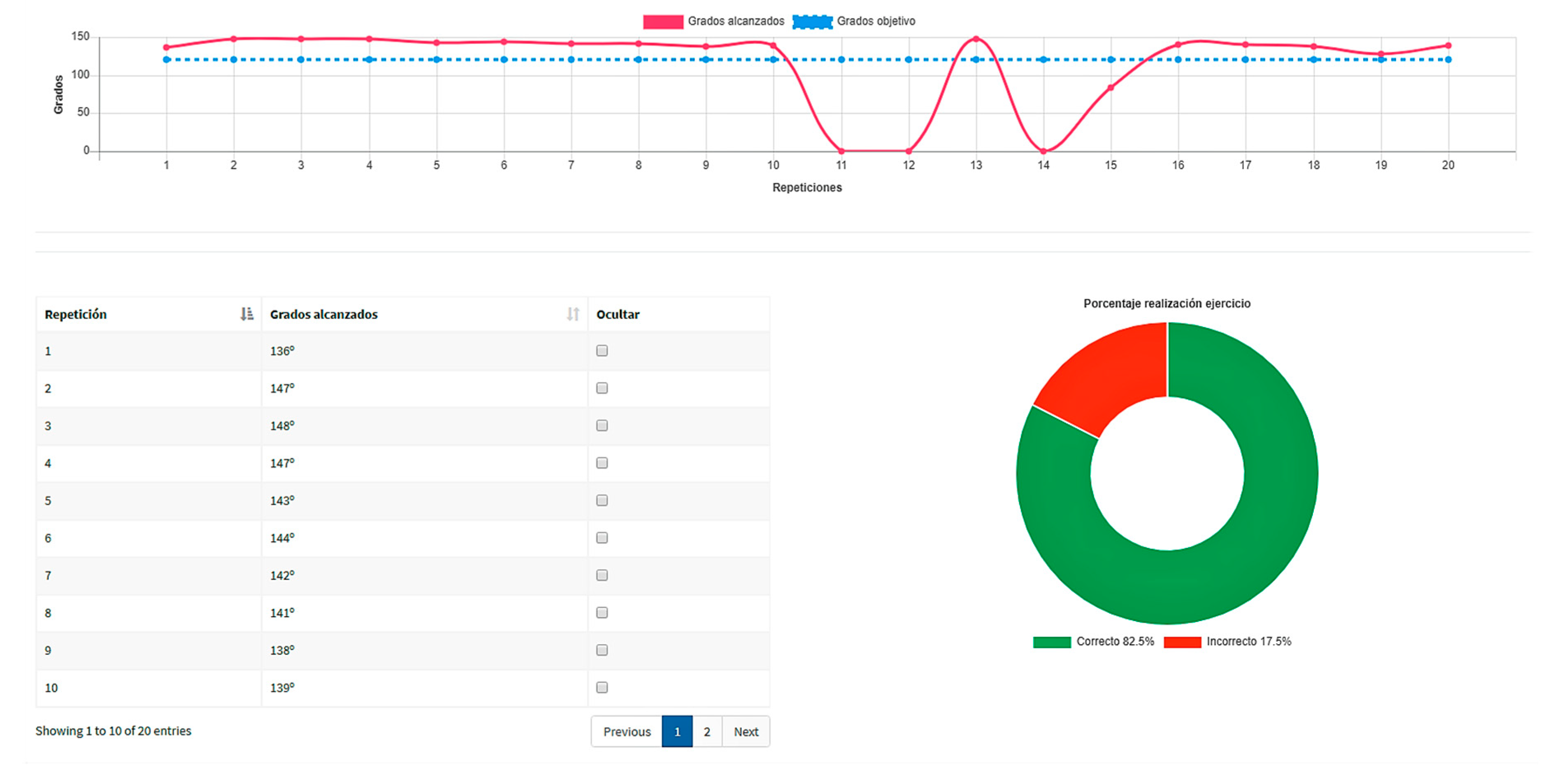
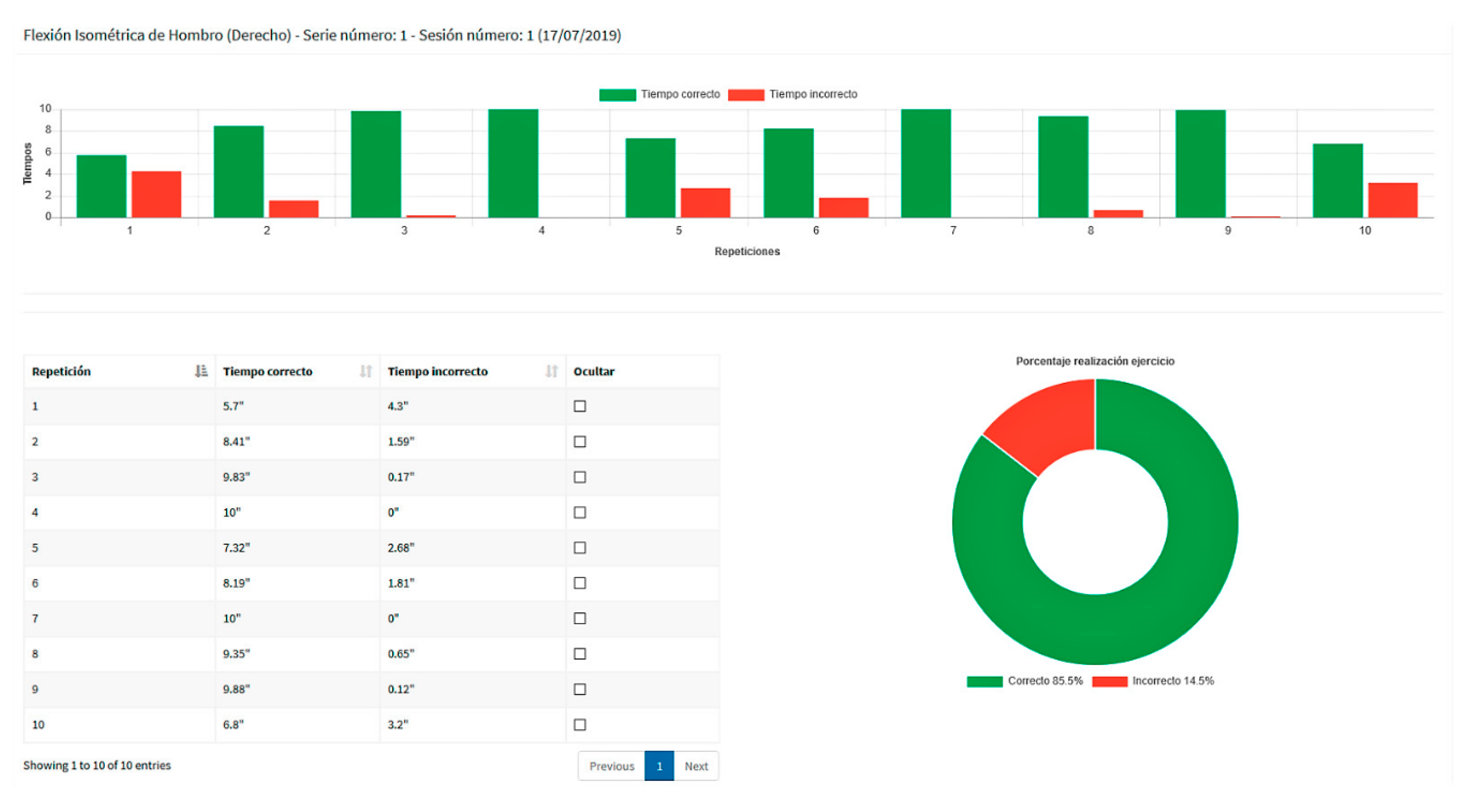
- Exercise analysis and scheduling. Healthcare professionals can access their private web areas, where statistics and charts provide details on the execution of the exercises, emphasizing the distance to the goal in each case. After judging results, new sessions can then be scheduled.
3.2. System Stages
3.2.1. Acquisition
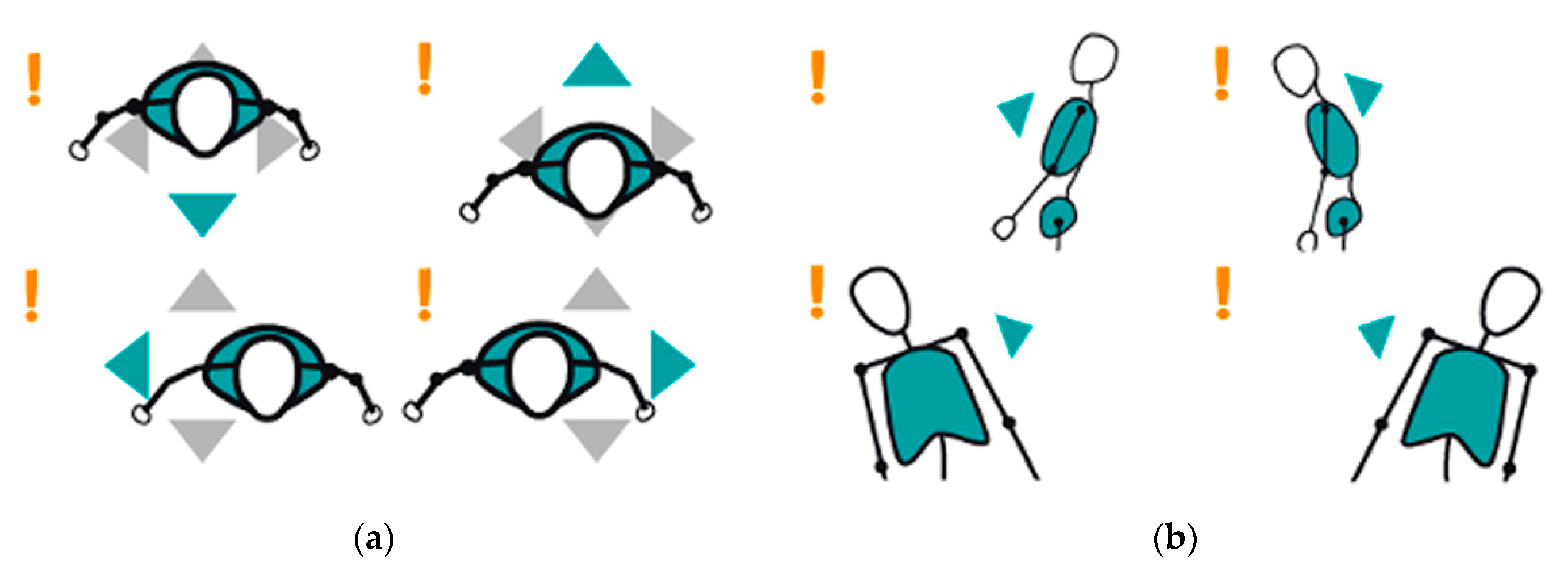
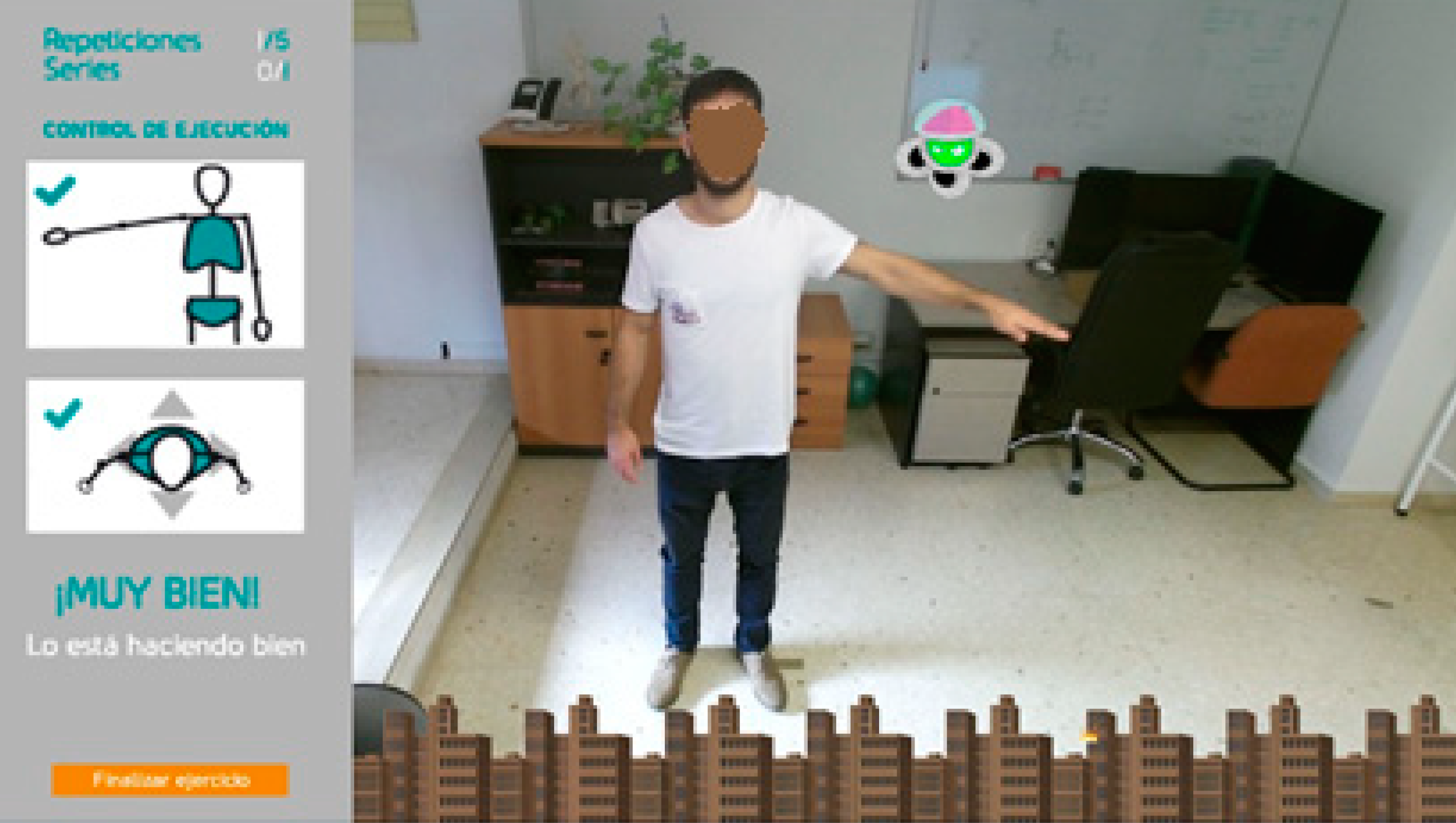
3.2.2. Gamified User Environments
- Positive. The patient performs a correct execution of the exercise, reaching the alien, so destroying it and keeping the city safe. Once the patient lowers the arm, another alien is generated at the same target position.
- Negative. The patient performs the exercise incorrectly, and fails to reach the objective position. Then, the alien attacks the city with fireballs.
- Positive. The patient performs a correct execution of the exercise, reaching the cage and keeping the bird in the cage during the prescribed period of time on a continuous basis, so the bird alights and rests.
- Negative. The patient performs the exercise incorrectly, failing to keep the bird in the cage during the prescribed period of time on a continuous basis, so the bird continues flying.
3.2.3. Monitoring and Measurement
- Patient-based calibration
- Tolerance margin setup
- Joint monitoring
- Occlusion handling
Patient-Based Calibration
Tolerance Margin Setup
Joint Monitoring
Occlusion Handling
3.2.4. Website
- To prescribe an exercise routine.
- To perform a system calibration.
- To assess a patient´s evolution.
- Visibility of system status. Reports reflect real-time results, which are updated as soon as the execution of the exercises ends.
- User´s preferred language. The terminology matches the specialized language used by medical personnel, approaching the system to the real world.
- Consistency with expectations. Graphics uses the green color to identify correct exercises and the red one to represent incorrect exercises.
3.2.5. Web Server
4. Results
4.1. Participants
4.2. Usability Study
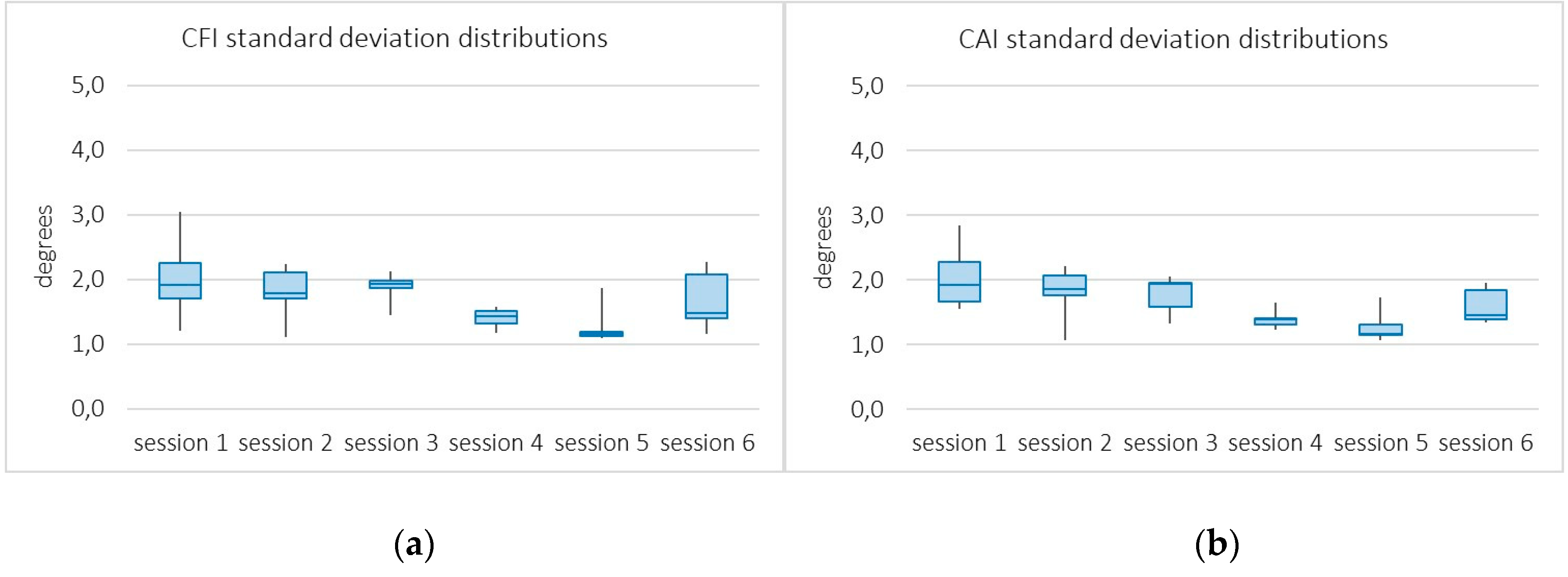
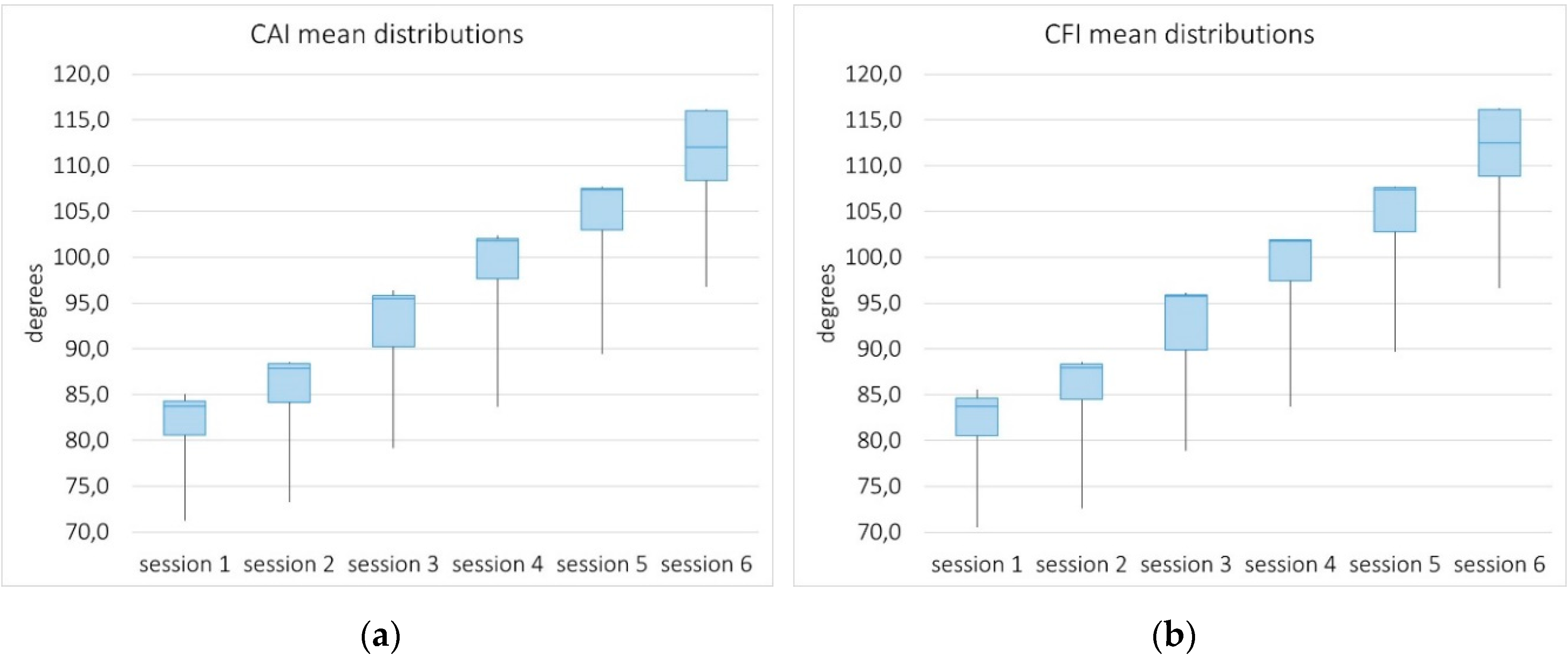
4.3. Performance Study
4.3.1. System Accuracy
4.3.2. System Sensitivity
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bai, J.; Song, A.; Xu, B.; Nie, J.; Li, H. A novel human-robot cooperative method for upper extremity rehabilitation. Int. J. Soc. Robot. 2017, 9, 265–275. [Google Scholar] [CrossRef]
- Shaughnessy, M.; Resnick, B.M.; Macko, R.F. Testing a Model of Post-Stroke Exercise Behavior. Rehabil. Nurs. 2006, 31, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Rand, D.; Kizony, R.; Weiss, P.L. Virtual reality rehabilitation for all: Vivid GX versus Sony PlayStation II Eye Toy. In Proceedings of the ICDVRAT, Oxford, UK, 20–22 September 2004; pp. 87–94. [Google Scholar]
- Chang, Y.J.; Chou, L.D.; Wang, F.T.Y.; Chen, S.F. A Kinect-based vocational task prompting system for individuals with cognitive impairments. Pers. Ubiquitous Comput. 2013, 17, 351–358. [Google Scholar] [CrossRef]
- Saposnik, G.; Teasell, R.; Mamdani, M.; Hall, J.; McIlroy, W.; Cheung, D.; Thorpe, K.E.; Cohen, L.G.; Bayley, M. Effectiveness of virtual reality using Wii gaming technology in stroke rehabilitation: A pilot randomized clinical trial and proof of principle. Stroke 2010, 41, 1477–1484. [Google Scholar] [CrossRef] [PubMed]
- Bai, J.; Song, A. Development of a Novel Home Based Multi-Scene Upper Limb Rehabilitation Training and Evaluation System for Post-Stroke Patients. IEEE Access 2019, 7, 9667–9677. [Google Scholar] [CrossRef]
- Fuertes-Muñoz, G.; Gallardo-Casero, J.; Mollineda-Cárdenas, R.A. Usability Study of a Kinect-Based Rehabilitation Tool for the Upper Limbs. In New Knowledge in Information Systems and Technologies; Rocha, Á., Adeli, H., Reis, L., Costanzo, S., Eds.; Springer: Cham, Switzerland, 2019; Volume 931. [Google Scholar]
- Naeemabadi, M.R.; Dinesen, B.; Andersen, O.K.; Najafi, S.; Hansen, J. Evaluating Accuracy and Usability of Microsoft Kinect Sensors and Wearable Sensor for Tele Knee Rehabilitation after Knee Operation. In Proceedings of the BIODEVICES, Funchal, Portugal, 19–21 January 2018; pp. 128–135. [Google Scholar]
- Tanaka, R.; Ishikawa, Y.; Yamasaki, T.; Diez, A. Accuracy of classifying the movement strategy in the functional reach test using a markerless motion capture system. J. Med. Eng. Technol. 2019, 43, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.; Hu, H. Human motion tracking for rehabilitation–A survey. Biomed. Signal Process. Control 2008, 3, 1–18. [Google Scholar] [CrossRef]
- Napoli, A.; Glass, S.; Ward, C.; Tucker, C.; Obeid, I. Performance analysis of a generalized motion capture system using Microsoft Kinect 2.0. Biomed. Signal Process. Control 2017, 38, 265–280. [Google Scholar] [CrossRef]
- Rizzo, A.; Kim, G. A SWOT Analysis of the Field of Virtual Reality Rehabilitation and Therapy. Presence: Teleoperators Virtual Environ. 2005, 14, 119–146. [Google Scholar] [CrossRef]
- Betke, M.; Gips, J. The camera mouse: Visual tracking of body features to provide computer access for people with severe disabilities. IEEE Trans. Neural Syst. Rehabil. Eng. 2002, 10, 1–10. [Google Scholar] [CrossRef]
- Varona, J.; Manresa-Yee, C.; Perales, F.J. Hands-free vision-based interface for computer accessibility. J. Netw. Comput. Appl. 2008, 31, 357–374. [Google Scholar] [CrossRef]
- Zannatha, J.M.I.; Tamayo, A.J.M.; Sánchez, Á.D.G.; Delgado, J.E.L.; Cheu, L.E.R.; Arévalo, W.A.S. Development of a system based on 3D vision, interactive virtual environments, ergonometric signals and a humanoid for stroke rehabilitation. Comput. Methods Programs Biomed. 2013, 112, 239–249. [Google Scholar] [CrossRef] [PubMed]
- Funaya, H.; Shibata, T.; Wada, Y.; Yamanaka, T. Accuracy assessment of Kinect body tracker in instant posturography for balance disorders. In Proceedings of the 7th International Symposium on Medical Information and Communication Technology (ISMICT), Tokyo, Japan, 6–8 March 2013; pp. 213–217. [Google Scholar] [CrossRef]
- Yang, Y.; Fang, P.; Yan, L.; Shuyu, L.; Yubo, F.; Deyu, L. Reliability and validity of Kinect RGB-D sensor for assessing standing balance. IEEE Sens. J. 2014, 14, 1633–1638. [Google Scholar] [CrossRef]
- Obdrzalek, S.; Kurillo, G.; Ofli, F.; Bajcsy, R.; Seto, E.; Jimison, H.; Pavel, M. Accuracy and robustness of Kinect pose estimation in the context of coaching of elderly population. In Proceedings of the 2012 Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), San Diego, CA, USA, 28 August–1 September 2012; pp. 1188–1193. [Google Scholar] [CrossRef]
- Wang, P.; Kreutzer, I.A.; Bjärnemo, R.; Davies, R.C. A web-based cost-effective training tool with possible application to brain injury rehabilitation. Comput. Methods Programs Biomed. 2004, 74, 235–243. [Google Scholar] [CrossRef] [PubMed]
- da Costa, R.M.E.M.; de Carvalho, L.A.V. The acceptance of virtual reality devices for cognitive rehabilitation: A report of positive results with schizophrenia. Comput. Methods Programs Biomed. 2004, 73, 173–182. [Google Scholar] [CrossRef]
- Edmans, J.A.; Gladman, J.R.; Cobb, S.; Sunderland, A.; Pridmore, T.; Hilton, D.; Walker, M.F. Validity of a virtual environment for stroke rehabilitation. Stroke 2006, 37, 2770–2775. [Google Scholar] [CrossRef]
- Broeren, J.; Bjorkdahl, A.; Claesson, L.; Goude, D.; Lundgren-Nilsson, A.; Samuelsson, H.; Blomstrand, C.; Sunnerhagen, K.S.; Rydmark, M. Virtual rehabilitation after stroke. In Proceedings of the Medical Informatics Europe, Göteborg, Sweden, 25–28 May 2008; pp. 77–82. [Google Scholar]
- Pyk, P.; Wille, D.; Chevrier, E.; Hauser, Y.; Holper, L.; Fatton, I.; Greipl, R.; Schlegel, S.; Ottiger, L.; Ruckriem, B.; et al. A pediatric interactive therapy system for arm and hand rehabilitation. In Proceedings of the Virtual Rehabilitation Conference, Vancouver, BC, Canada, 25–27 August 2008; pp. 127–132. [Google Scholar]
- Lange, B.; Flynn, S.; Proffitt, R.; Chang, C.Y.; “Skip” Rizzo, A. Development of an interactive game-based rehabilitation tool for dynamic balance training. Top. Stroke Rehabil. 2010, 17, 345–352. [Google Scholar] [CrossRef]
- Flynn, S.M.; Lange, B.S. Games for the rehabilitation: The voice of the players. In Proceedings of the Intl. Conf. Disability, Virtual Reality & Associated Technologies (ICDVRAT 2010), Serpa, Portugal, 9–10 September 2010; pp. 185–194. [Google Scholar]
- Lozano, J.A.; Montesa, J.; Juan, M.C.; Alcañiz, M.; Rey, B.; Gil, J.; Martinez, J.M.; Gaggioli, A.; Morganti, F. VR-Mirror: A virtual reality system for mental practice in post-stroke rehabilitation. In International Symposium on Smart Graphics; Springer: Berlin/Heidelberg, Germany, 2005; pp. 241–245. [Google Scholar]
- Cabrera, R.; Molina, A.; Gómez, I.; García-Heras, J. Kinect as an access device for people with cerebral palsy: A preliminary study. Int. J. Hum. Comput. Stud. 2017, 108, 62–69. [Google Scholar] [CrossRef]
- Jung, I.; Lee, J.; Kim, J.; Choi, C. Ubiquitous gamification framework for stroke rehabilitation treatment based on the web service. In Proceedings of the 4th Workshop on ICTs for improving Patients Rehabilitation Research Techniques, Oldenburg, Germany, 20–23 May 2014; pp. 117–120. [Google Scholar]
- Jonsdottir, J.; Bertoni, R.; Lawo, M.; Montesano, A.; Bowman, T.; Gabrielli, S. Serious games for arm rehabilitation of persons with multiple sclerosis. A randomized controlled pilot study. Mult. Scler. Relat. Disord. 2018, 19, 25–29. [Google Scholar] [CrossRef]
- Alankus, G.; Lazar, A.; May, M.; Kelleher, C. Towards Customizable Games for Stroke Rehabilitation. In Proceedings of the CHI 2010: Therapy and Rehabilitation, Atlanta, GA, USA, 10–15 April 2010; pp. 2113–2122. [Google Scholar]
- Wollersheim, D.; Merkes, M.; Shields, N.; Liamputtong, P.; Wallis, L.; Reynolds, F.; Koh, L. Physical and psychosocial effects of Wii video game use among older women. Int. J. Emerg. Technol. Soc. 2010, 8, 85–98. [Google Scholar]
- Pastor, I.; Hayes, H.A.; Bamberg, S.J. A feasibility study of an upper limb rehabilitation system using Kinect and computer games. In Proceedings of the 2012 annual international conference of the IEEE engineering in medicine and biology society, San Diego, CA, USA, 28 August–1 September 2012; pp. 1286–1289. [Google Scholar]
- Wang, Z.; Walsh, K.; Verma, B. On-tree mango fruit size estimation using RGB-D images. Sensors 2017, 17, 2738. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, A.V.; Ong, Y.L.A.; Luo, C.X.; Thuraisingam, T.; Rubino, M.; Levin, M.F.; Archambault, P.S. Virtual reality exergaming as adjunctive therapy in a sub-acute stroke rehabilitation setting: Facilitators and barriers. Disabil. Rehabil. Assist. Technol. 2019, 14, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, J. Enhancing the explanatory power of usability heuristics. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, Boston, MA, USA, 24–28 April 1994; pp. 152–158. [Google Scholar]
- Parmanto, B.; Lewis, A.N.J.; Graham, K.M.; Bertolet, M.H. Development of the telehealth usability questionnaire (TUQ). Int. J. Telerehabilitation 2016, 8, 3. [Google Scholar] [CrossRef] [PubMed]
- Gil-Gómez, J.A.; Gil-Gómez, H.; Lozano-Quilis, J.A.; Manzano-Hernández, P.; Albiol-Pérez, S.; Aula-Valero, C. SEQ: Suitability evaluation questionnaire for virtual rehabilitation systems. Application in a virtual rehabilitation system for balance rehabilitation. In Proceedings of the 7th International Conference on Pervasive Computing Technologies for Healthcare, Venice, Italy, 5–8 May 2013; pp. 335–338. [Google Scholar]
- Brooke, J. SUS-A quick and dirty usability scale. Usability Eval. Ind. 1996, 189, 4–7. [Google Scholar]
- Pei, Y.-C.; Chen, J.-L.; Wong, A.M.K.; Tseng, K.C. An Evaluation of the Design and Usability of a Novel Robotic Bilateral Arm Rehabilitation Device for Patients with Stroke. Front. Neurorobot. 2017, 11, 36. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.H.; Ryu, H.; Jang, S.H. A task-specific interactive game-based virtual reality rehabilitation system for patients with stroke: A usability test and two clinical experiments. J. Neuroeng. Rehabil. 2014, 11, 32. [Google Scholar] [CrossRef]
- Park, J.; Parsons, D.; Ryu, H. To flow and not to freeze: Applying flow experience to mobile learning. IEEE Trans. Learn. Technol. 2010, 3, 56–67. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Id | Gender | Age | Injury |
|---|---|---|---|
| 1 | male | 42 | joint dislocation |
| 2 | male | 47 | tendinopathy |
| 3 | female | 64 | humerus fracture |
| 4 | male | 67 | joint dislocation |
| 5 | male | 38 | tendinopathy |
| 6 | female | 55 | tendinopathy |
| 7 | female | 57 | calcification |
| 8 | male | 83 | osteoarthritis |
| 9 | male | 45 | shoulder impingement |
| 10 | female | 50 | shoulder impingement |
| Question | Average Value | Standard Deviation |
|---|---|---|
| 1. I think I would like to use KineActiv frequently | 4.7 | 0.48 |
| 2. I think that KineActiv is unnecessarily complex | 1.4 | 0.52 |
| 3. I think that KineActiv is easy to use | 4.5 | 0.53 |
| 4. I think that I would need help to use KineActiv | 2.3 | 1.06 |
| 5. I think that the various functions in KineActiv are well integrated | 4.3 | 0.67 |
| 6. I think there is too much inconsistency in KineActiv | 1.4 | 0.52 |
| 7. I imagine that most people would learn to use KineActiv very quickly | 4.6 | 0.52 |
| 8. I found KineActiv very cumbersome to use | 1.5 | 0.53 |
| 9. I felt very confident using KineActiv | 4.4 | 0.52 |
| 10. I would have needed to learn a lot of things before using KineActiv | 2.1 | 0.88 |
| 11. I thought about other things when using KineActiv | 2.5 | 0.85 |
| 12. I was aware of distractions when using KineActiv | 3.0 | 0.47 |
| 13. Using KineActiv was boring for me | 1.6 | 0.52 |
| 14. KineActiv was fun for me to use | 4.4 | 0.52 |
| 15. I felt that I had the control over my rehabilitation process with KineActiv | 3.9 | 0.74 |
| 16. I was frustrated with what I was doing when using KineActiv | 1.4 | 0.52 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fuertes Muñoz, G.; Mollineda, R.A.; Gallardo Casero, J.; Pla, F. A RGBD-Based Interactive System for Gaming-Driven Rehabilitation of Upper Limbs. Sensors 2019, 19, 3478. https://doi.org/10.3390/s19163478
Fuertes Muñoz G, Mollineda RA, Gallardo Casero J, Pla F. A RGBD-Based Interactive System for Gaming-Driven Rehabilitation of Upper Limbs. Sensors. 2019; 19(16):3478. https://doi.org/10.3390/s19163478
Chicago/Turabian StyleFuertes Muñoz, Gabriel, Ramón A. Mollineda, Jesús Gallardo Casero, and Filiberto Pla. 2019. "A RGBD-Based Interactive System for Gaming-Driven Rehabilitation of Upper Limbs" Sensors 19, no. 16: 3478. https://doi.org/10.3390/s19163478
APA StyleFuertes Muñoz, G., Mollineda, R. A., Gallardo Casero, J., & Pla, F. (2019). A RGBD-Based Interactive System for Gaming-Driven Rehabilitation of Upper Limbs. Sensors, 19(16), 3478. https://doi.org/10.3390/s19163478