Tracking Foot Drop Recovery Following Lumbar-Spine Surgery, Applying Multiclass Gait Classification Using Machine Learning Techniques



Abstract
1. Introduction
2. Materials and Methods
2.1. Test Protocol
2.2. Participants
2.3. Data Preprocessing
2.4. Feature Extraction, Classification, and Regression
3. Results
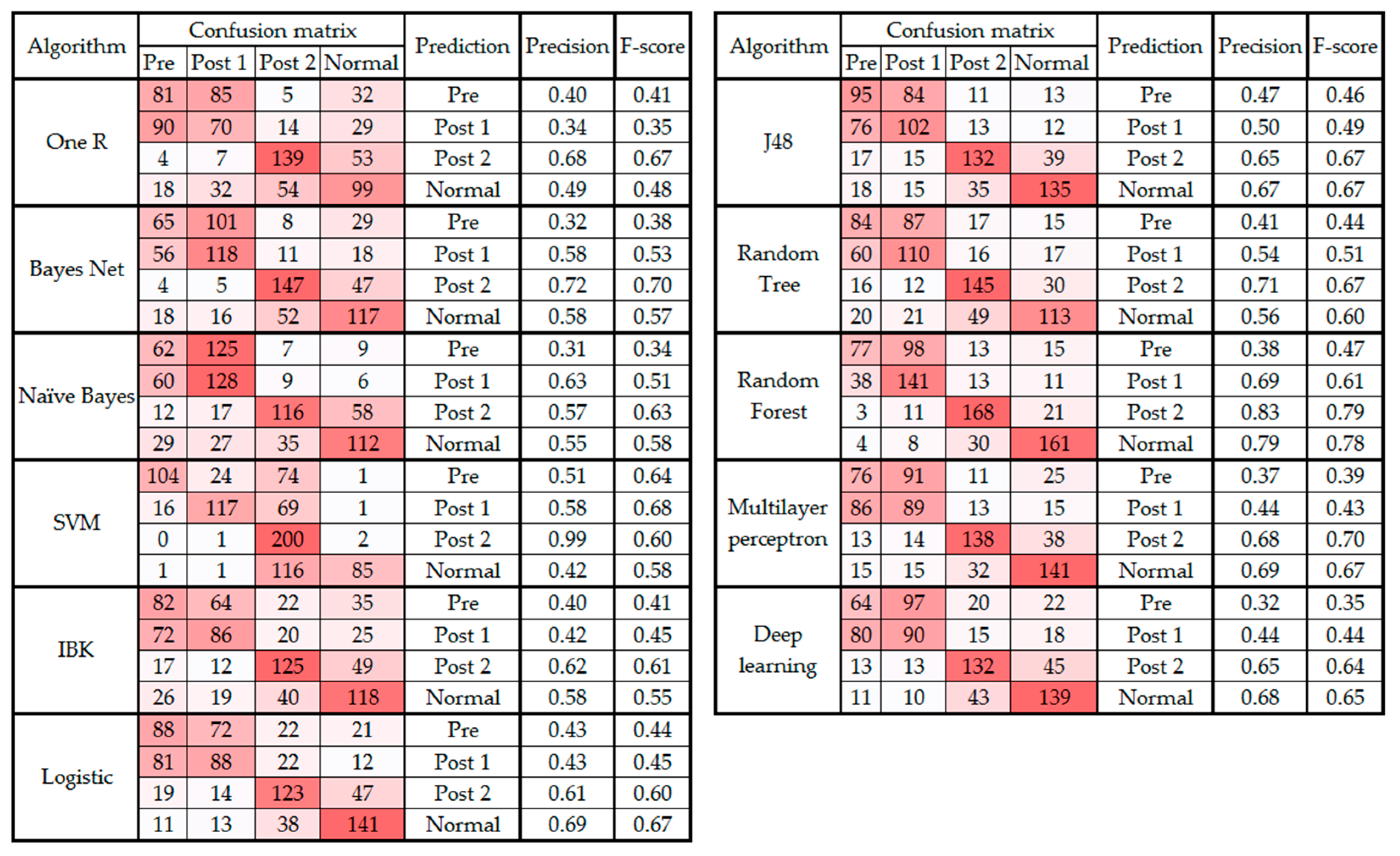
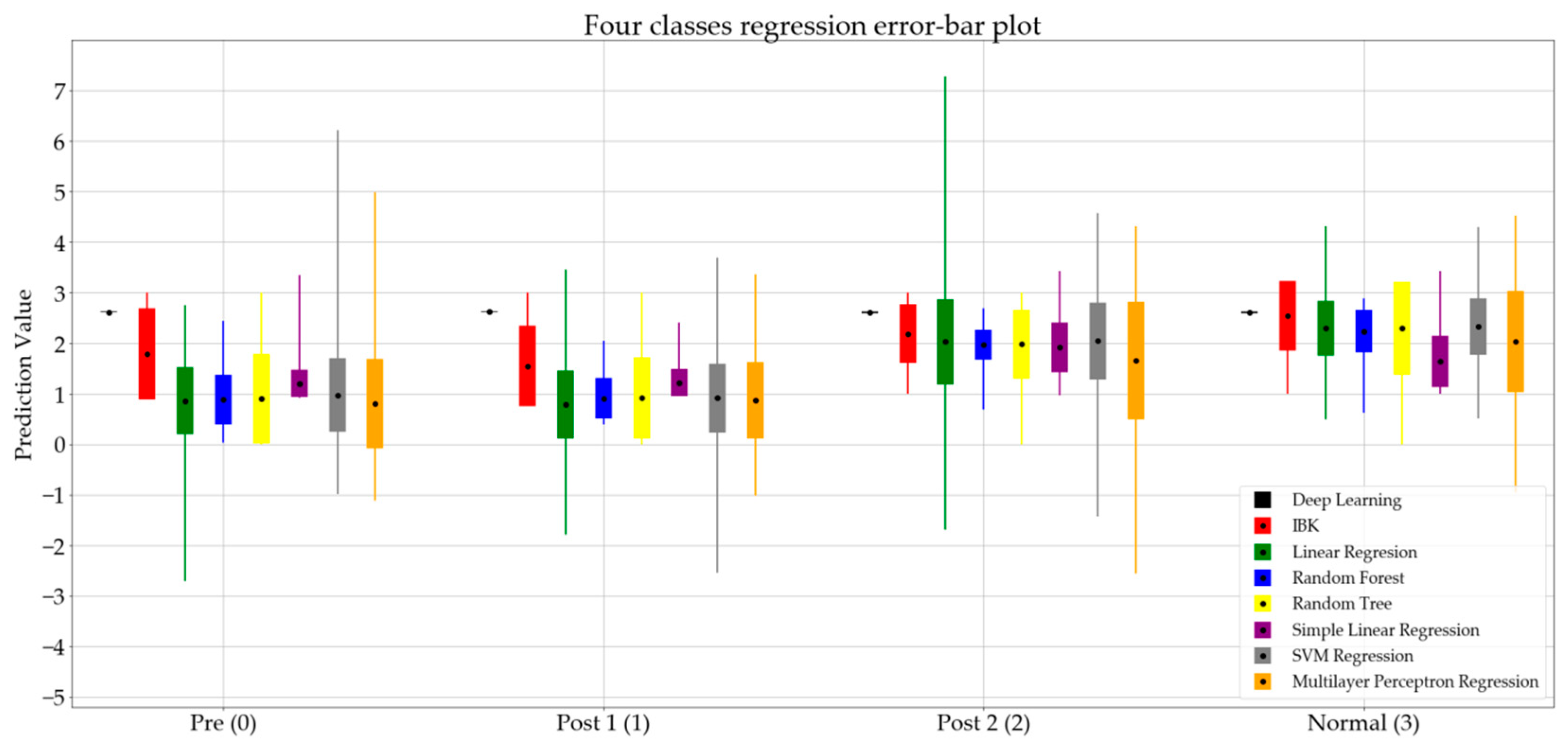
3.1. Analysis of the Four Classes
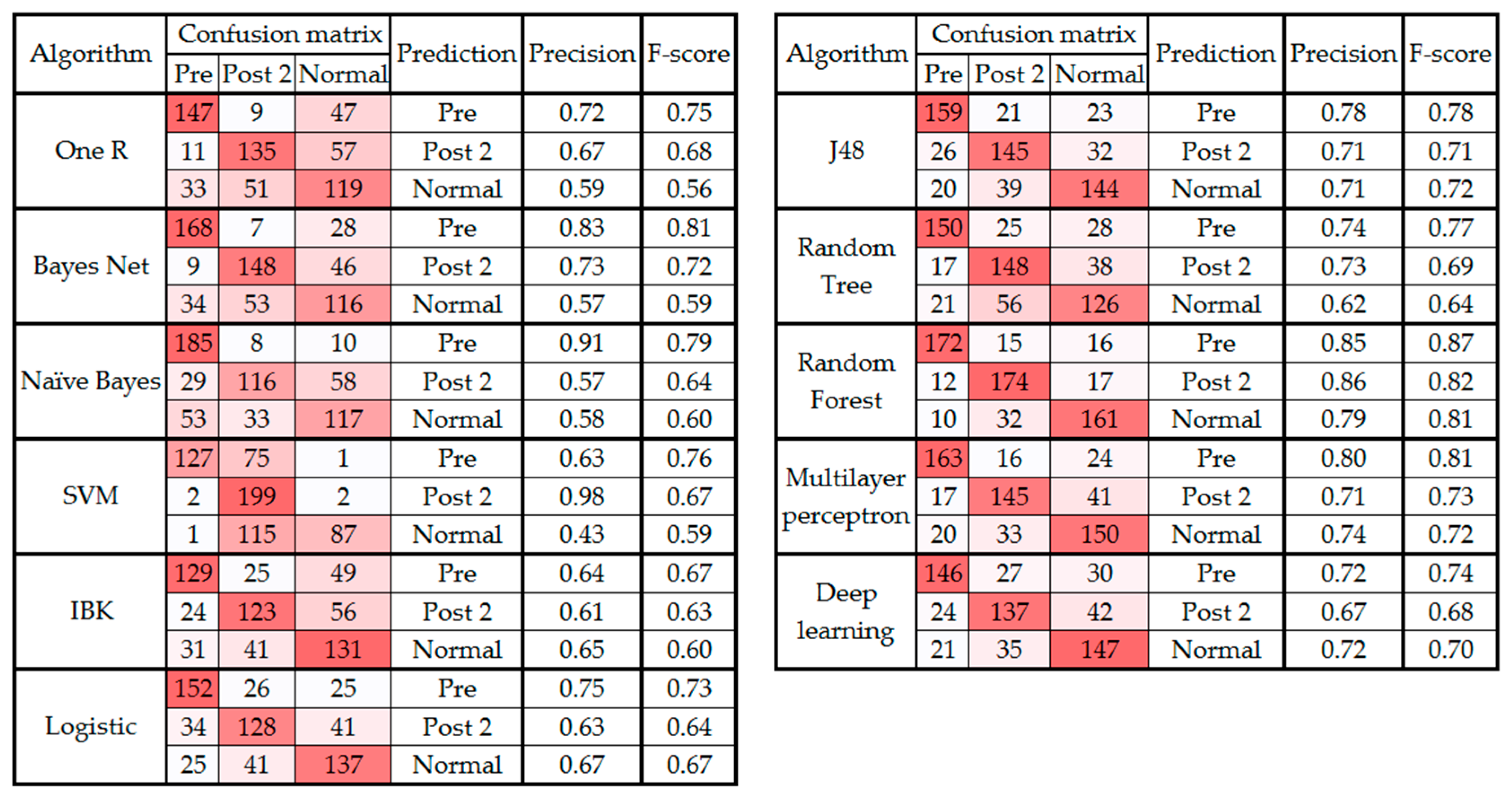
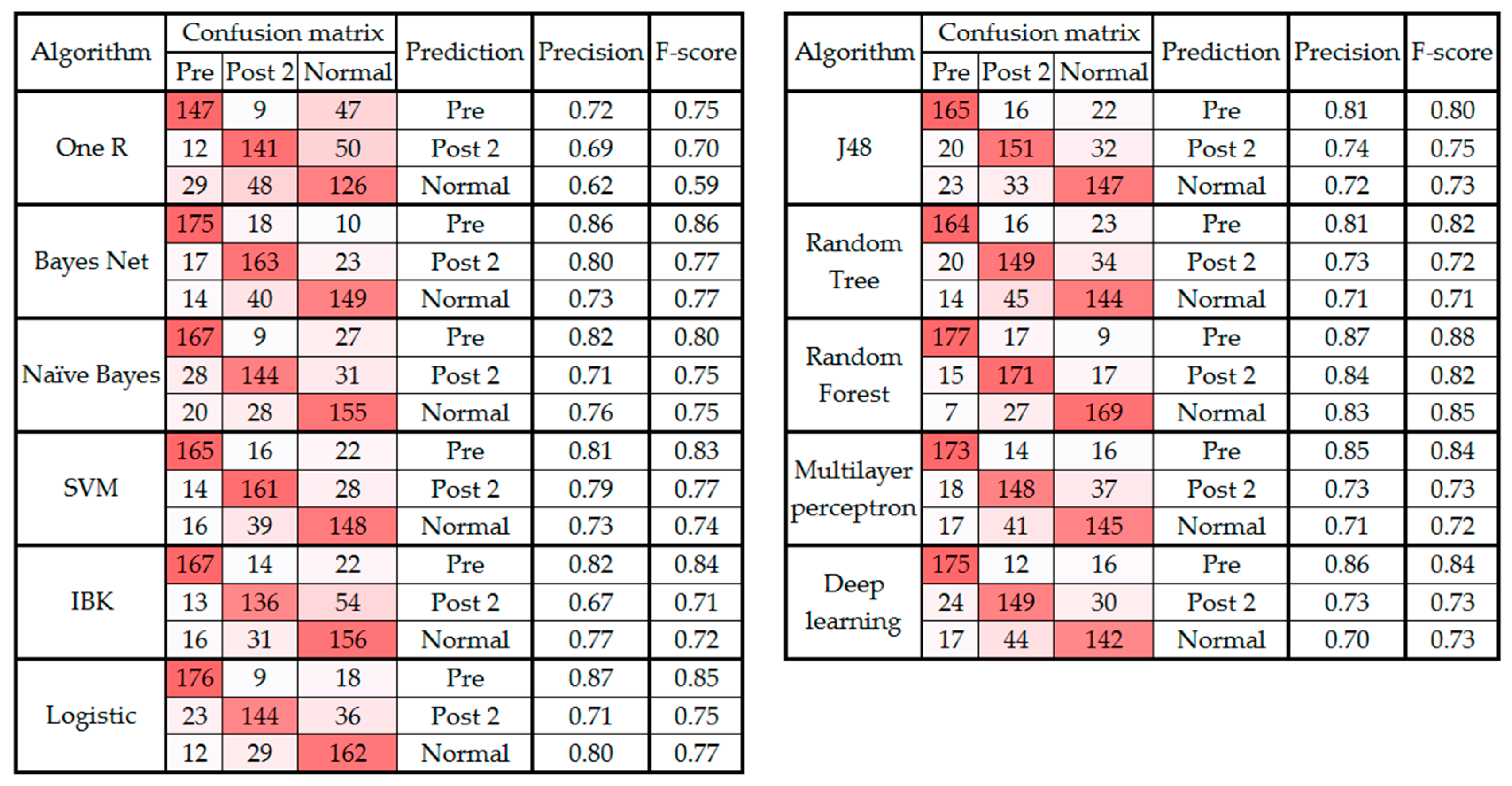
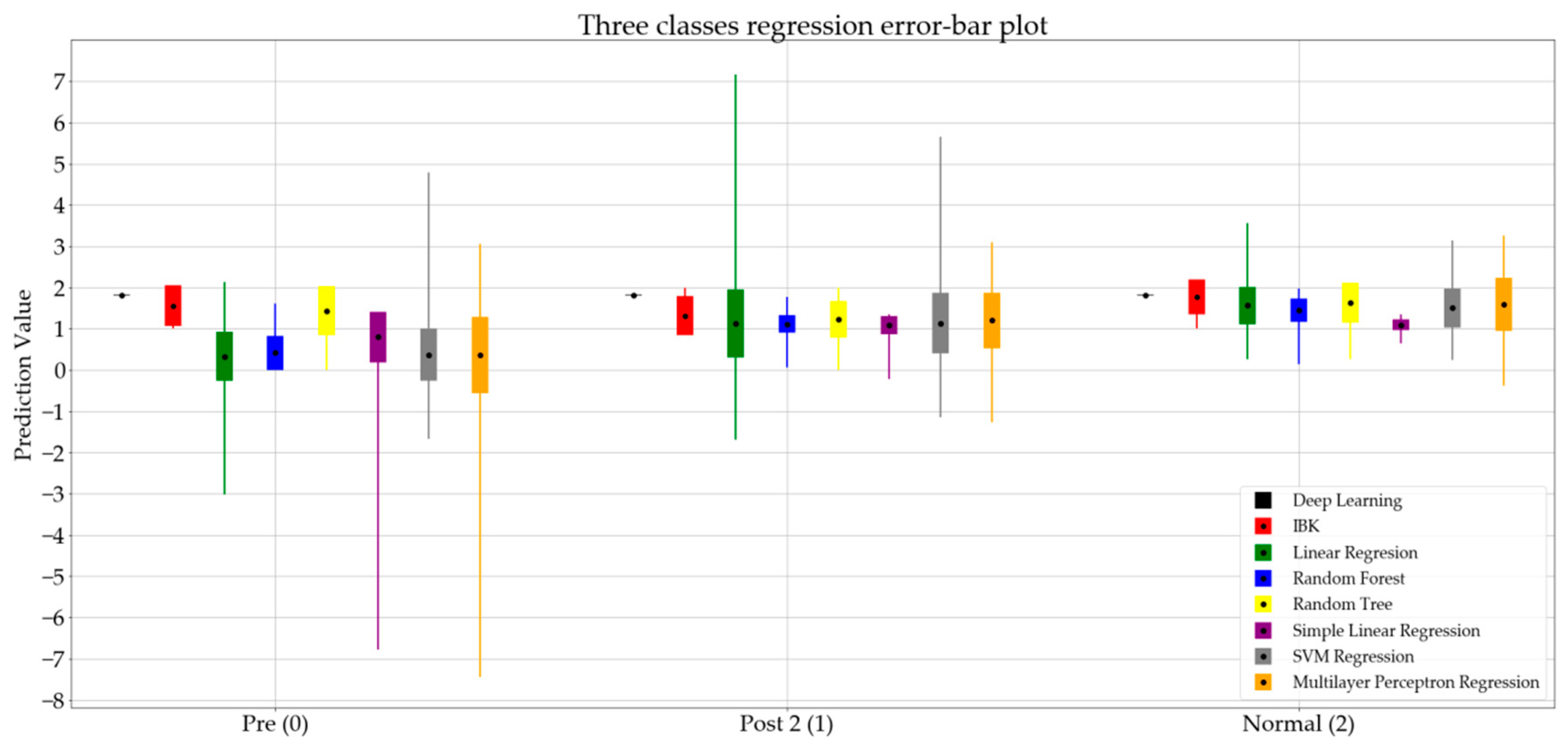
3.2. Analysis of Three Classes
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bussmann, J.B.J.; Culhane, K.M.; Horemans, H.L.D.; Lyons, G.M.; Stam, H.J. Validity of the prosthetic activity monitor to assess the duration and spatio-temporal characteristics of prosthetic walking. IEEE Trans. Neural Syst. Rehabil. Eng. 2004, 12, 379–386. [Google Scholar] [CrossRef] [PubMed]
- Giné-Garriga, M.; Guerra, M.; Manini, T.M.; Marí-Dell’Olmo, M.; Pagès, E.; Unnithan, V.B. Measuring balance, lower extremity strength and gait in the elderly: Construct validation of an instrument. Arch. Gerontol. Geriatr. 2010, 51, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Whitney, S.; Wrisley, D.; Furman, J. Concurrent validity of the Berg Balance Scale and the Dynamic Gait Index in people with vestibular dysfunction. Physiother. Res. Int. 2003, 8, 178–186. [Google Scholar] [CrossRef] [PubMed]
- Van Hedel, H.J.A. Gait dpeed in relation to categories of functional ambulation after spinal cord injury. Neurorehabilit. Neural Repair 2009, 23, 343–350. [Google Scholar] [CrossRef] [PubMed]
- Uszko-Lencer, N.H.; Mesquita, R.; Janssen, E.; Werter, C.; Brunner-La Rocca, H.P.; Pitta, F.; Wouters, E.F.; Spruit, M.A. Reliability, construct validity and determinants of 6-minute walk test performance in patients with chronic heart failure. Int. Cardiol. J. 2017, 240, 285–290. [Google Scholar] [CrossRef] [PubMed]
- Kesikburun, S.; Yavuz, F.; Güzelküçük, Ü.; Yaşar, E.; Balaban, B. Effect of ankle foot orthosis on gait parameters and functional ambulation in patients with stroke. Turk. J. Phys. Med. Rehab. 2017, 63, 143–149. [Google Scholar] [CrossRef]
- Debono, B.; Bousquet, P.; Sabatier, P.; Plas, J.Y.; Lescure, J.P.; Hamel, O. Postoperative monitoring with a mobile application after ambulatory lumbar discectomy: An effective tool for spine surgeons. Eur. Spine J. 2016, 25, 3536–3542. [Google Scholar] [CrossRef] [PubMed]
- Cloete, T.; Scheffer, C. Repeatability of an off-the-shelf, full body inertial motion capture system during clinical gait analysis. In Proceedings of the 2010 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Buenos Aire, Argentina, 30 August–4 September 2010; pp. 5125–5128. [Google Scholar]
- Collen, F.M.; Wade, D.T.; Bradshaw, C.M. Mobility after stroke: Reliability of measures of impairment and disability. Int. Disabil. Stud. 1990, 12, 6–9. [Google Scholar] [CrossRef]
- Viosca, E.; Martínez, J.L.; Almagro, P.L.; Gracia, A.; González, C. Proposal and validation of a new functional ambulation classification scale for clinical use. Arch. Phys. Med. Rehabil. 2005, 86, 1234–1238. [Google Scholar] [CrossRef]
- Marino, M.; Nicholas, J.A.; Gleim, G.W.; Rosenthal, P.; Nicholas, S.J. The efficacy of manual assessment of muscle strength using a new device. Am. J. Sports Med. 1982, 10, 360–364. [Google Scholar] [CrossRef]
- Roche, B.; Simon, A.L.; Guilmin-Crepon, S.; Boizeau, P.; Andriss, B.; Alberti, C.; Presedo, A.; Ilharreborde, B.; Husson, I. Test-retest reliability of an instrumented electronic walkway system (GAITRite) for the measurement of spatio-temporal gait parameters in young patients with Friedreich’s ataxia. Gait Posture 2018, 66, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Windolf, M.; Götzen, N.; Morlock, M. Systematic accuracy and precision analysis of video motion capturing systems-exemplified on the Vicon-460 system. J. Biomech. 2008, 41, 2776–2780. [Google Scholar] [CrossRef] [PubMed]
- Higginson, B.K. Methods of running gait analysis. Curr. Sports Med. Rep. 2009, 8, 136–141. [Google Scholar] [CrossRef] [PubMed]
- Tao, W.; Liu, T.; Zheng, R.; Feng, H. Gait Analysis Using Wearable Sensors. Sensors 2012, 12, 2255–2283. [Google Scholar] [CrossRef] [PubMed]
- Pappas, I.P.I.; Keller, T.; Mangold, S.; Popovic, M.R.; Dietz, V.; Morari, M. A Reliable Gyroscope-Based Gait-Phase Detection Sensor Embedded in a Shoe Insole. IEEE Sens. J. 2004, 4, 268–274. [Google Scholar] [CrossRef]
- Li, Q.; Young, M.; Naing, V.; Donelan, J.M. Walking speed and slope estimation using shank-mounted inertial measurement units. In Proceedings of the 2009 IEEE International Conference on Rehabilitation Robotics, Kyoto, Japan, 23–26 June 2009; pp. 839–844. [Google Scholar]
- Foster, K.R.; Koprowski, R.; Skufca, J.D. Machine learning, medical diagnosis, and biomedical engineering research-commentary. Biomed. Eng. Online 2014, 13, 94. [Google Scholar] [CrossRef]
- Begg, R.K.; Palaniswami, M.; Owen, B. Support vector machines for automated gait classification. IEEE Trans. Biomed. Eng. 2005, 52, 828–838. [Google Scholar] [CrossRef]
- Hu, B.; Dixon, P.C.; Jacobs, J.V.; Dennerlein, J.T.; Schiffman, J.M. Machine learning algorithms based on signals from a single wearable inertial sensor can detect surface- and age-related differences in walking. J. Biomech. 2018, 71, 37–42. [Google Scholar] [CrossRef]
- Mazilu, S.; Hardegger, M.; Zhu, Z.; Roggen, D.; Tröster, G.; Plotnik, M.; Hausdorff, J.M. Online Detection of Freezing of Gait with Smartphones and Machine Learning Techniques. In Proceedings of the 6th International Conference on Pervasive Computing Technologies for Healthcare (PervasiveHealth) and Workshops, San Diego, CA, USA, 21–24 May 2012; pp. 123–130. [Google Scholar]
- Tahir, N.M.; Manap, H.H. Parkinson Disease Gait Classification based on Machine Learning Approach. J. Appl. Sci. 2012, 12, 180–185. [Google Scholar] [CrossRef]
- Pogorelc, B.; Bosnić, Z.; Gams, M. Automatic recognition of gait-related health problems in the elderly using machine learning. Multimed. Tools Appl. 2012, 58, 333–354. [Google Scholar] [CrossRef]
- Williamson, R.; Andrews, B.J. Gait event detection for FES using accelerometers and supervised machine learning. IEEE Trans. Rehabil. Eng. 2000, 8, 312–319. [Google Scholar] [CrossRef] [PubMed]
- Nowlan, M.F. Human Identification via Gait Recognition Using Accelerometer Gyro Forces. Available online: https://pdfs.semanticscholar.org/a63e/04fefd2be621488646ae11bfe66c98d9649e.pdf (accessed on 3 May 2017).
- Özdemir, A.; Barshan, B. Detecting Falls with Wearable Sensors Using Machine Learning Techniques. Sensors 2014, 14, 10691–10708. [Google Scholar] [CrossRef]
- Zhang, J.; Lockhart, T.E.; Soangra, R. Classifying lower extremity muscle fatigue during walking using machine learning and inertial sensors. Ann. Biomed. Eng. 2014, 42, 600–612. [Google Scholar] [CrossRef] [PubMed]
- LeMoyne, R.; Heerinckx, F.; Aranca, T.; De Jager, R.; Zesiewicz, T.; Saal, H.J. Wearable body and wireless inertial sensors for machine learning classification of gait for people with Friedreich’s ataxia. In Proceedings of the 13th International Conference on Wearable and Implantable Body Sensor Networks (BSN), San Francisco, CA, USA, 14–17 June 2016; pp. 147–151. [Google Scholar]
- Westhout, F.D.; Paré, L.S.; Linskey, M.E. Central causes of foot drop: Rare and underappreciated differential diagnoses. J. Spinal Cord Med. 2007, 30, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Sackley, C.; Disler, P.B.; Turner-Stokes, L.; Wade, D.T.; Brittle, N.; Hoppitt, T. Rehabilitation interventions for foot drop in neuromuscular disease. In Cochrane Database of Systematic Reviews; Sackley, C., Ed.; John Wiley & Sons, Ltd.: Chichester, UK, 2009. [Google Scholar]
- Stewart, J.D. Foot drop: Where, why and what to do? Pract. Neurol. 2008, 8, 158–169. [Google Scholar] [CrossRef] [PubMed]
- Young, A.; Getty, J.; Jackson, A.; Kirwan, E.; Sullivan, M.; Parry, C.W. Variations in the pattern of muscle innervation by the L5 and S1 nerve roots. Spine 1983, 8, 616–624. [Google Scholar] [CrossRef] [PubMed]
- Sharif Bidabadi, S.; Murray, I.; Lee, G. The application of Inertial Measurements Unit for the clinical evaluation and assessment of gait events. Med. J. Eng. Technol. 2017, 41, 612–622. [Google Scholar] [CrossRef] [PubMed]
- Sharif Bidabadi, S.; Murray, I.; Lee, G.Y.F. Validation of foot pitch angle estimation using inertial measurement unit against marker-based optical 3D motion capture system. Biomed. Eng. Lett. 2018, 8, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Yoo, J.H.; Nixon, M.S.; Harris, C.J. Model-driven statistical analysis of human gait motion. Time 2002, 1, 285–288. [Google Scholar]
- Wong, A.M.; Simon, S.R.; Olshen, R.A. Statistical analysis of gait patterns of persons with cerebral palsy. Stat. Med. 1983, 2, 345–354. [Google Scholar] [CrossRef]
- Frank, E.; Hall, M.; Holmes, G.; Kirkby, R.; Pfahringer, B.; Witten, I.H.; Trigg, L. Weka-A Machine Learning Workbench for Data Mining. In Data Mining and Knowledge Discovery Handbook; Springer: Boston, MA, USA, 2009; pp. 1269–1277. [Google Scholar]
- Guan, C.; Qin, S.; Ling, W.; Ding, G. Apparel recommendation system evolution: An empirical review. Int. J. Cloth. Sci. Technol. 2016, 28, 854–879. [Google Scholar] [CrossRef]
- El Aboudi, N.; Benhlima, L. Review on wrapper feature selection approaches. In Proceedings of the 2016 International Conference on Engineering and MIS, ICEMIS 2016, Agadir, Morocco, 22–24 September 2016; pp. 1–5. [Google Scholar]
- MacKi, M.; Syeda, S.; Kerezoudis, P.; Gokaslan, Z.L.; Bydon, A.; Bydon, M. Preoperative motor strength and time to surgery are the most important predictors of improvement in foot drop due to degenerative lumbar disease. J. Neurol. Sci. 2016, 361, 133–136. [Google Scholar] [CrossRef] [PubMed]
- Patane, F.; Rossi, S.; Del Sette, F.; Taborri, J.; Cappa, P. WAKE-Up Exoskeleton to Assist Children With Cerebral Palsy: Design and Preliminary Evaluation in Level Walking. IEEE Trans. Neural Syst. Rehabil. Eng. 2017, 25, 906–916. [Google Scholar] [CrossRef] [PubMed]
- Mileti, I.; Taborri, J.; Rossi, S.; Petrarca, M.; Patane, F.; Cappa, P. Evaluation of the effects on stride-to-stride variability and gait asymmetry in children with Cerebral Palsy wearing the WAKE-up ankle module. In Proceedings of the 2016 IEEE International Symposium on Medical Measurements and Applications (MeMeA), Benevento, Italy, 15–18 May 2016; pp. 1–6. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Algorithm | Accuracy (%) |
|---|---|
| Bayes net | 55.0493 |
| Deep learning | 52.3399 |
| IBK | 50.6158 |
| J48 | 57.1429 |
| Logistic regression | 54.1872 |
| Multilayer perceptron | 54.6798 |
| Naïve Bayes | 51.4778 |
| OneR | 47.9064 |
| Random forest | 67.3645 |
| Random tree | 55.665 |
| SVM | 62.3153 |
| Average | 55.3400 |
| Algorithm | Correlation Coefficient | Mean Absolute Error | Root Mean Squared Error | Relative Absolute Error | Root Relative Squared Error |
|---|---|---|---|---|---|
| Deep learning | –0.0856 | 1.3104 | 1.5825 | 130.8814 | 141.4032 |
| IBk | 0.4181 | 0.7808 | 1.2217 | 77.9844 | 109.1655 |
| Linear regression | 0.6430 | 0.7003 | 0.8910 | 69.9453 | 79.6130 |
| Multilayer perceptron | 0.0026 | 1.2089 | 9.3257 | 120.7437 | 833.2870 |
| Random forest | 0.7807 | 0.5426 | 0.7119 | 54.1923 | 63.6136 |
| Random tree | 0.5748 | 0.6252 | 1.0010 | 62.4422 | 89.4466 |
| Simple linear regression | 0.4454 | 0.7936 | 1.0010 | 79.2604 | 89.4430 |
| SVM | 0.6244 | 0.7062 | 0.9067 | 70.5317 | 81.0133 |
| Algorithm | All Features (n = 144) | Selected Features | |
|---|---|---|---|
| Accuracy (%) | Accuracy (%) | Number of Selected Features | |
| Bayes net | 70.94 | 79.97 | 20 |
| Deep learning | 70.61 | 76.52 | 21 |
| IBk | 62.89 | 75.37 | 46 |
| J48 | 73.56 | 76.03 | 22 |
| Logistic regression | 68.47 | 79.15 | 22 |
| Multilayer perceptron | 75.21 | 76.52 | 20 |
| Naïve Bayes | 68.64 | 76.52 | 44 |
| OneR | 65.85 | 67.98 | 1 |
| Random forest | 83.25 | 84.89 | 33 |
| Random tree | 69.62 | 75.04 | 21 |
| SVM | 67.82 | 77.83 | 30 |
| Average | 70.62 | 76.89 | NA |
| Feature Type | Foot | Shank | Thigh | Total |
|---|---|---|---|---|
| Pitch | 5 | 5 | 6 | 16 |
| Roll | 6 | 4 | 1 | 11 |
| Yaw | 4 | 1 | 1 | 6 |
| Total | 15 | 10 | 8 | 33 |
| Algorithm | Correlation Coefficient | Mean Absolute Error | Root Mean Squared Error | Relative Absolute Error (%) | Root Relative Squared Error (%) |
|---|---|---|---|---|---|
| Deep learning | −0.0598 | 0.9396 | 1.1555 | 140.4993 | 141.4422 |
| IBk | 0.4966 | 0.4631 | 0.8245 | 69.2432 | 100.9249 |
| Linear regression | 0.6109 | 0.5319 | 0.5319 | 79.5453 | 88.4125 |
| Random forest | 0.7931 | 0.3785 | 0.5099 | 56.6055 | 62.4162 |
| Random tree | 0.5861 | 0.3992 | 0.7267 | 59.6992 | 88.9477 |
| Simple linear regression | 0.2998 | 0.6580 | 0.7963 | 98.3908 | 97.4729 |
| SVM | 0.5930 | 0.5470 | 0.7221 | 81.8015 | 88.3848 |
| Multilayer perceptron | 0.5469 | 0.5649 | 0.8279 | 84.4696 | 101.3445 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sharif Bidabadi, S.; Tan, T.; Murray, I.; Lee, G. Tracking Foot Drop Recovery Following Lumbar-Spine Surgery, Applying Multiclass Gait Classification Using Machine Learning Techniques. Sensors 2019, 19, 2542. https://doi.org/10.3390/s19112542
Sharif Bidabadi S, Tan T, Murray I, Lee G. Tracking Foot Drop Recovery Following Lumbar-Spine Surgery, Applying Multiclass Gait Classification Using Machine Learning Techniques. Sensors. 2019; 19(11):2542. https://doi.org/10.3390/s19112542
Chicago/Turabian StyleSharif Bidabadi, Shiva, Tele Tan, Iain Murray, and Gabriel Lee. 2019. "Tracking Foot Drop Recovery Following Lumbar-Spine Surgery, Applying Multiclass Gait Classification Using Machine Learning Techniques" Sensors 19, no. 11: 2542. https://doi.org/10.3390/s19112542
APA StyleSharif Bidabadi, S., Tan, T., Murray, I., & Lee, G. (2019). Tracking Foot Drop Recovery Following Lumbar-Spine Surgery, Applying Multiclass Gait Classification Using Machine Learning Techniques. Sensors, 19(11), 2542. https://doi.org/10.3390/s19112542