Physical Wellbeing Monitoring Employing Non-Invasive Low-Cost and Low-Energy Sensor Socks





Abstract
:1. Introduction
2. Related Work
3. Materials and Methods
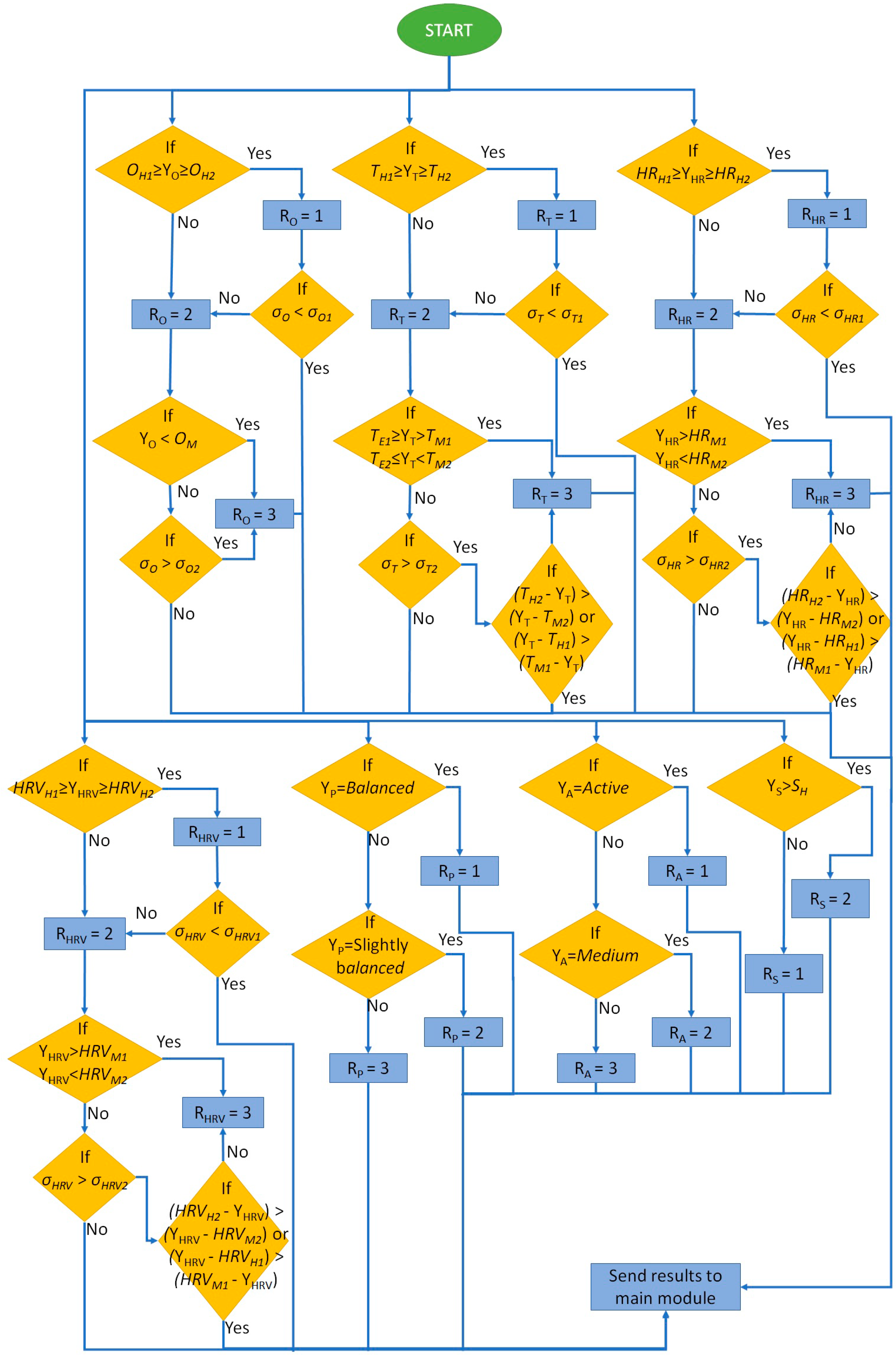
3.1. Wellness Parameters
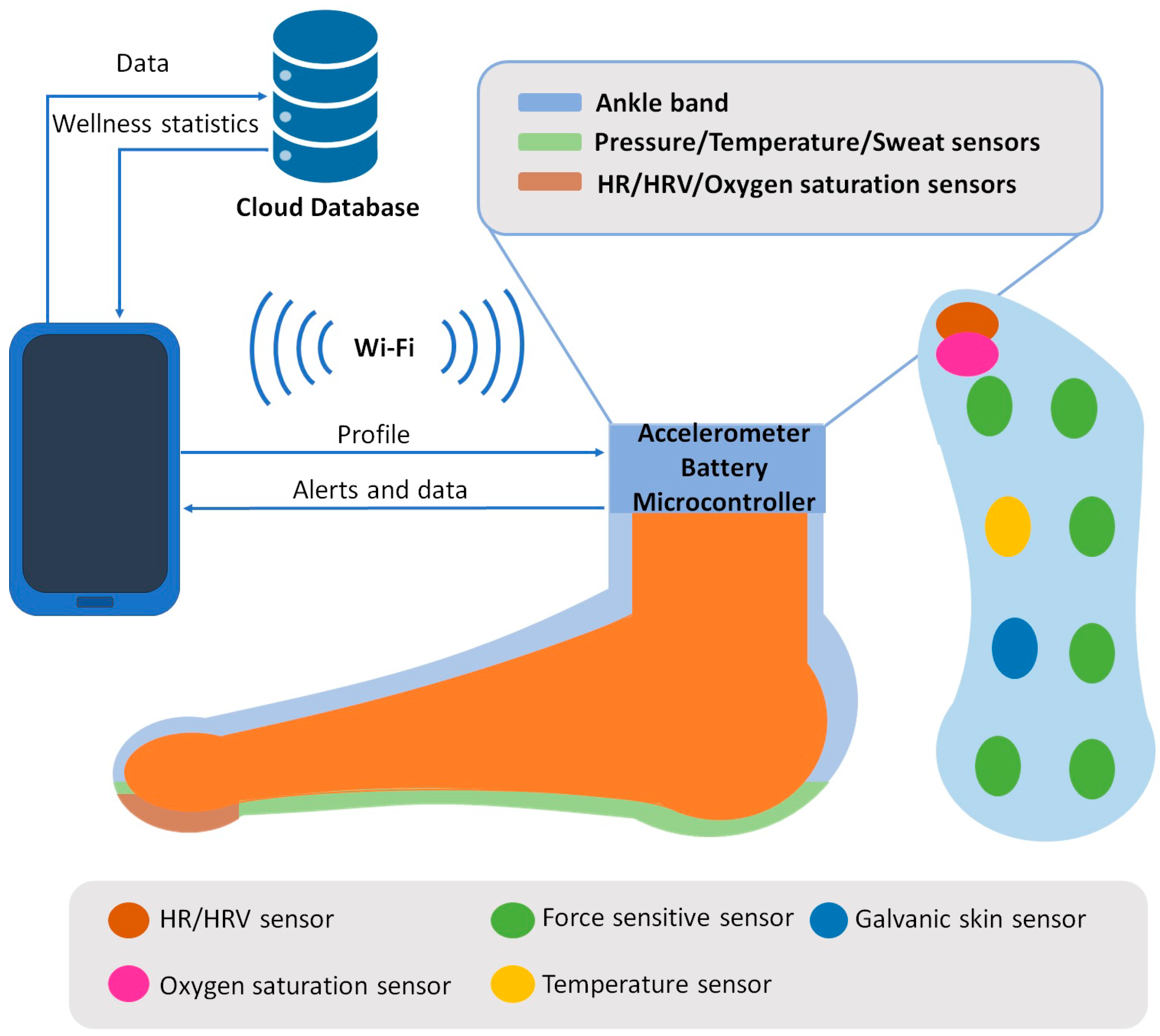
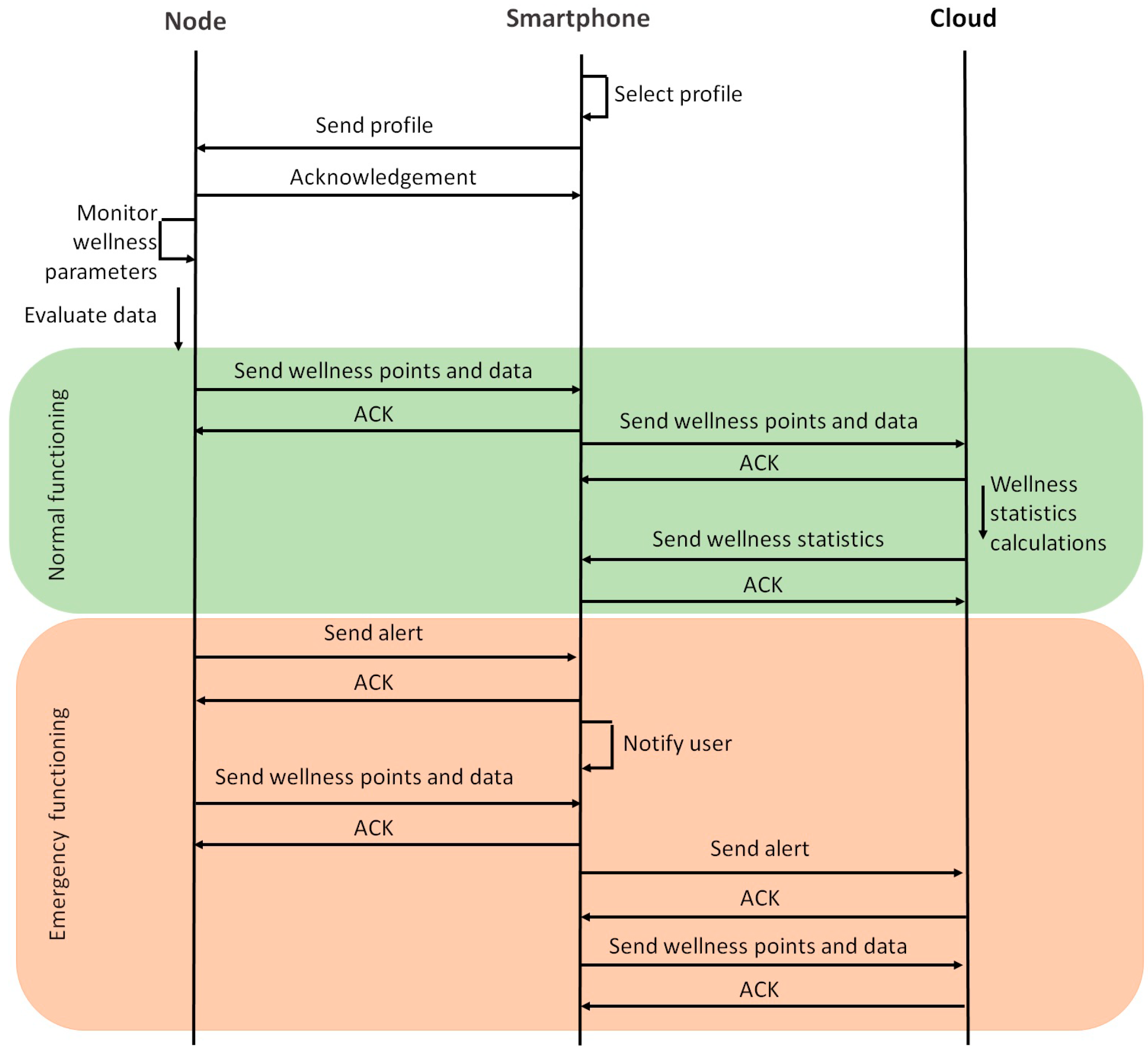
3.2. System Description
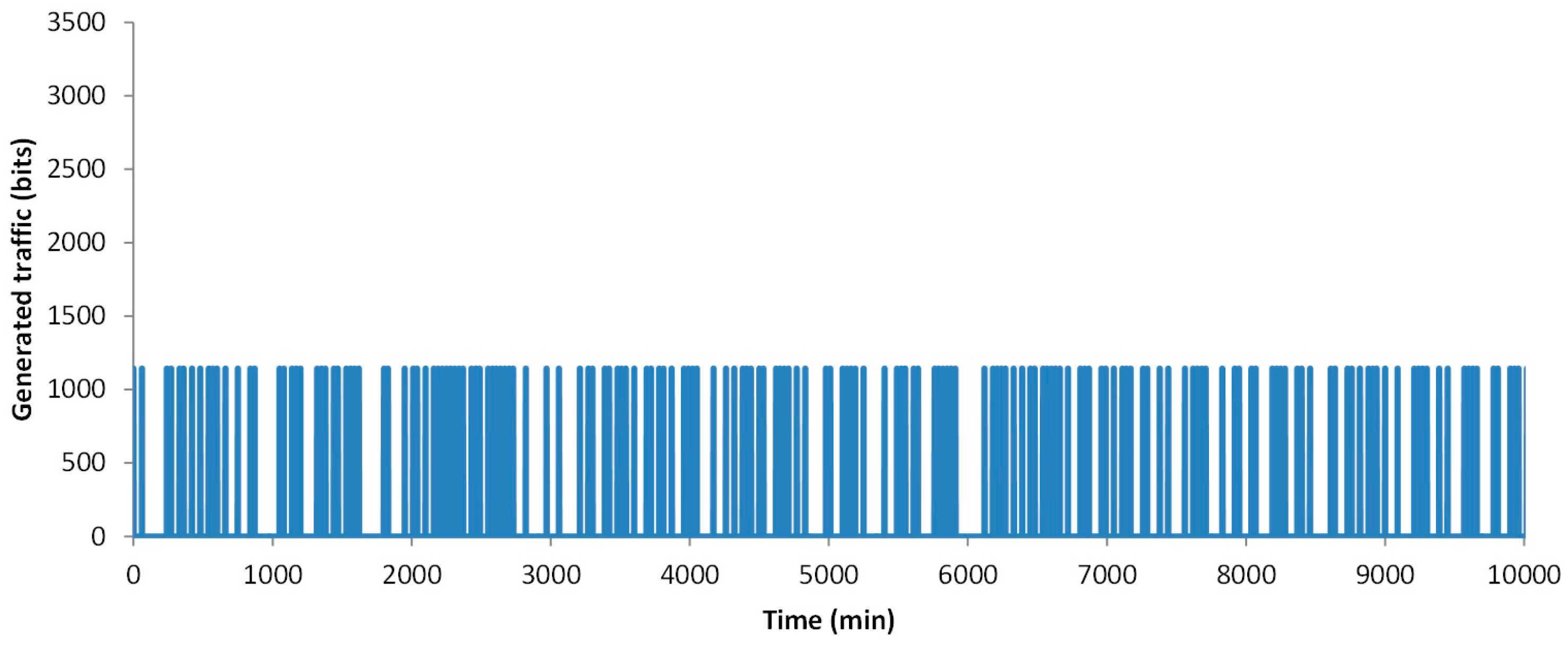
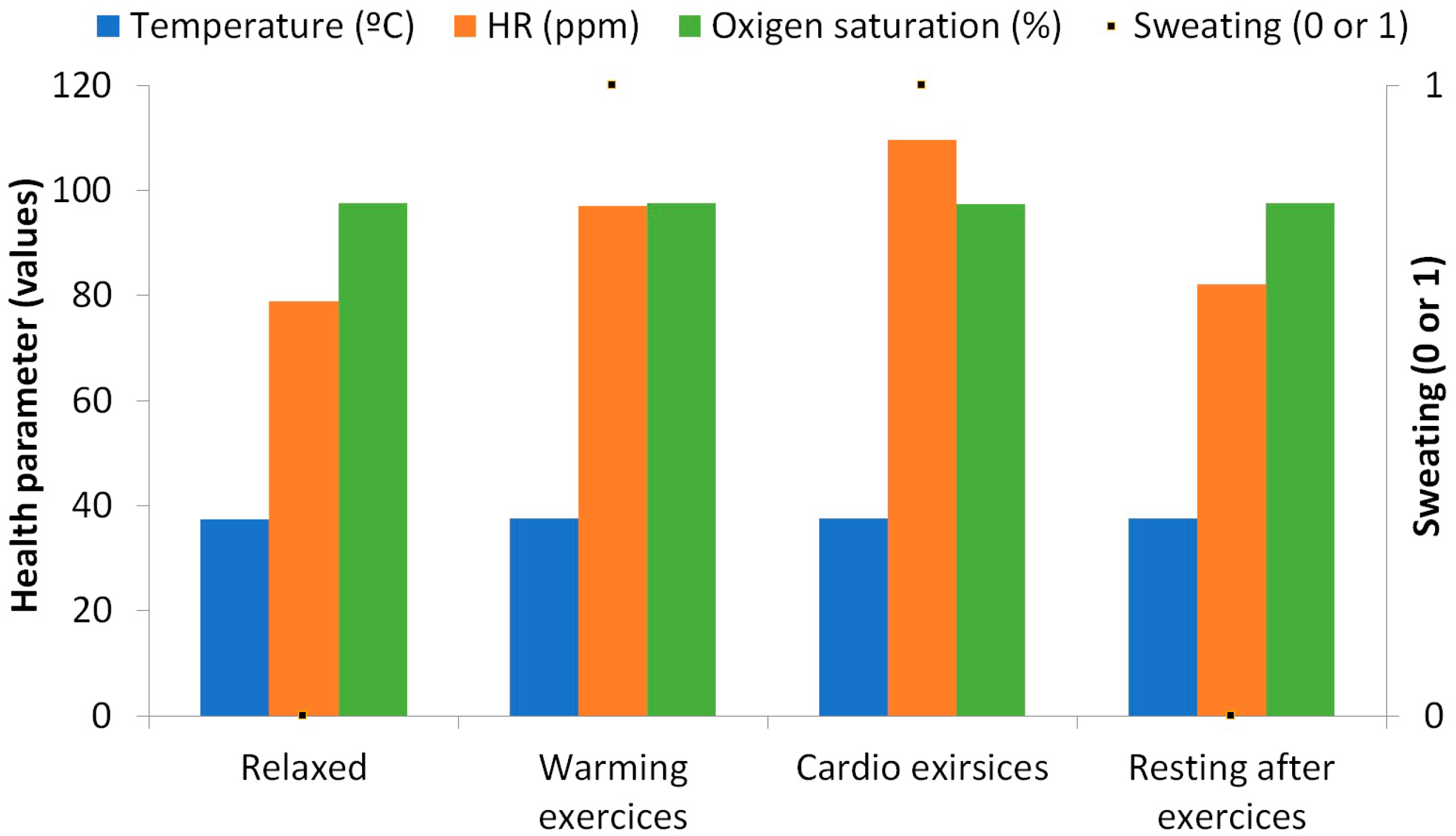
4. Results and Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- García, L.; Parra, L.; Romero, O.; Lloret, J. System for monitoring the wellness state of people in domestic environments employing emoticon-based HCI. J. Supercomput. 2017, 1–25. [Google Scholar] [CrossRef]
- OECD Health Policy Studies. “A Good Life in Old Age? MONITORING AND IMPROVING QUALITY IN LONG-TERM CARE”. Available online: http://www.oecd.org/health/health-systems/good-life-in-old-age.htm (accessed on 8 July 2018).
- Pantelopoulos, A.; Bourbakis, N.G. A Survey on Wearable Sensor-Based Systems for Health Monitoring and Prognosis. IEEE Trans. Syst. Man Cybern. C Appl. Rev. 2009, 40, 1–12. [Google Scholar] [CrossRef]
- Khodabandeh, H.; Ayatollahitafti, V.; Taghizadeh, M.S. Link aware and Energy efficient Routing Algorithm in Wireless Body Area Networks. Netw. Protoc. Algorithms 2017, 9, 126–138. [Google Scholar] [CrossRef]
- Masud, F.; Abdullah, A.H.; Abdul-Salaam, G.; Ishfaq, M.K. Emergency Traffic MAC Protocols in Wireless Body Area Networks. AD HOC Sens. Wirel. Netw. 2018, 41, 83–113. [Google Scholar]
- U.S. FOOD & DRUG ADMINISTRATION. Available online: https://www.fda.gov/ (accessed on 8 July 2018).
- NHS. Available online: https://www.nhs.uk/pages/home.aspx (accessed on 8 July 2018).
- Parra, L.; Sendra, S.; Jimenez, J.M.; Lloret, J. Multimedia sensors embedded in smartphones for ambient assisted living and e-health. Multi. Tools Appl. 2016, 75, 13271–13297. [Google Scholar] [CrossRef]
- Lane, N.; Rabbi, M.; Lin, M.; Campbell, A.T. BeWell: A Smartphone Application to Monitor, Model and Promote Wellbeing. In Proceedings of the 5th International ICST Conference on Pervasive Computing Technologies for Healthcare, Dublin, Ireland, 23–26 May 2011; pp. 23–26. [Google Scholar]
- Mundt, C.W.; Montgomery, K.N.; Udoh, U.E.; Barker, V.N.; Thonier, G.C.; Tellier, A.M.; Ricks, R.D.; Darling, R.B.; Cagle, Y.D.; Cabrol, N.A.; et al. A multiparameter wearable physiologic monitoring system for space and terrestrial applications. IEEE Trans. Inf. Tech. Biomed. 2005, 9, 382–391. [Google Scholar] [CrossRef]
- Miramontes, R.; Aquino, R.; Flores, A.; Rodríguez, G.; Anguiano, R.; Ríos, A.; Edwards, A. PlaIMoS:A remote mobile healthcare platform to monitor cardiovascular and respiratory variables. Sensors 2017, 17, 176. [Google Scholar] [CrossRef] [PubMed]
- Zio by iRhythm. Available online: https://www.irhythmtech.com/ (accessed on 8 July 2018).
- Henry, I.; Bernstein, D.; Banet, M.; Mulligan, J.; Moulton, S.; Grudic, G.; Convertino, C. Body-Worn, Non-Invasive Sensor for Monitoring Stroke Volume, Cardiac Output and Cardiovascular Reserve. In Proceedings of the 2nd Conference on Wireless Health, La Jolla, CA, USA, 10–13 October 2011; p. 26. [Google Scholar]
- Sahoo, P.K.; Thakkar, H.K.; Lin, W.Y.; Chang, P.C.; Lee, M.Y. On the Design of an Efficient Cardiac Health Monitoring System through Combined Analysis of ECG and SCG Signals. Sensors 2018, 18, 379. [Google Scholar] [CrossRef] [PubMed]
- Trung, T.Q.; Ramasundaram, S.; Hwang, B.U.; Lee, N.E. An All-Elastomeric Transparent and Stretchable Temperature Sensor for Body-Attachable Wearable Electronics. Adv. Mater. 2016, 28, 502–509. [Google Scholar] [CrossRef] [PubMed]
- Steinhubl, S.R.; Marriott, M.P.; Wegerich, S.W. Remote Sensing of Vital Signs: A Wearable, Wireless “Bad-Aid” Sensor with Personalized Analytics for Improved Ebola Patient Care and Worker Safety. Glob. Health Sci. Pract. 2015, 3, 516–519. [Google Scholar] [CrossRef] [PubMed]
- Ozemek, C.; Kirschner, M.M.; Wilkerson, B.S.; Byun, W.; Kaminsky, L.A. Intermonitor reliability of the GT3X+ accelerometer at hip, wrist and ankle sites during activities of daily living. Physiol. Meas. 2014, 35, 129–138. [Google Scholar] [CrossRef] [PubMed]
- Bouten, C.V.C.; Koekkoek, K.T.M.; Verduin, M.; Kodde, R.; Janssen, J.D. A Triaxial Accelerometer and Portable Data Processing Unit for the Assessment of Daily Physical Activity. IEEE Trans. Biomed. Engin. 1997, 44, 136–147. [Google Scholar] [CrossRef] [PubMed]
- Ghamari, M.; Soltanpur, C.; Cabrera, S.; Romero, R.; Martinek, R.; Nazeran, H. Design and Prototyping of a Wristband-Type Wireless Photoplethysmographic Device for Heart Rate Variability Signal Analysis. In Proceedings of the 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Orlando, FL, USA, 16–20 August 2016; pp. 4967–4970. [Google Scholar]
- Low, D.C.; Sixon, S.J. Footscan pressure insoles: Accuracy and reliability of force and pressure measurements in running. Gait Posture 2010, 32, 664–666. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, P.J.P. Sock for Integrated Biometric Monitoring. U.S. Patent Application No. 13/809,099, 30 May 2013. [Google Scholar]
- Ling, T.H.Y.; Wong, L.J.; Tan, J.E.H.; Kiu, K.Y. Non-Intrusive Human Body Temperature Acquisition and Monitoring System. In Proceedings of the 6th International Conference on Intelligent Systems, Modeling and Simulation, Kuala Lumpur, Malaysia, 9–11 February 2015; pp. 16–20. [Google Scholar]
- Sparkfun Body Temperature Sensor. Available online: https://www.sparkfun.com/products/8777 (accessed on 29 June 2018).
- Datasheet of the MCP9700/9700A and MCP9701/9701A Sensors. Available online: https://cdn.sparkfun.com/datasheets/E-Textiles/Lilypad/38512_SPCN.pdf (accessed on 16 August 2018).
- All about Heart Rate (Pulse). American Heart Association 2015. Available online: http://www.heart.org/HEARTORG/Conditions/HighBloodPressure/GettheFactsAboutHighBloodPressure/All-About-Heart-Rate-Pulse_UCM_438850_Article.jsp#.W0DrxfZuJu0 (accessed on 29 June 2018).
- Sparkfun Pulse Sensor. Available online: https://www.sparkfun.com/products/11574 (accessed on 29 June 2018).
- Datasheet of Sparkfun Pulse Sensor. Available online: https://media.digikey.com/pdf/Data%20Sheets/Pulse%20Sensor%20PDFs/Pulse_Sensor.pdf (accessed on 16 August 2018).
- Lacuesta, R.; García, L.; García-Magariño, I.; Lloret, I. System to recommend the best place to live based on wellness state of the user employing the heart rate variability. IEEE Access 2017, 5, 10594–10604. [Google Scholar] [CrossRef]
- Oxygen Saturation Sensor. Available online: https://www.sparkfun.com/products/14045?_ga=2.230342172.1255482369.1530462324-1642799772.1528990291 (accessed on 29 June 2018).
- Datasheet of MAX30105. Available online: https://cdn.sparkfun.com/assets/learn_tutorials/5/7/7/MAX30105_3.pdf (accessed on 16 August 2018).
- Force Sensitive Resistor. Available online: https://www.sparkfun.com/products/9375 (accessed on 29 June 2018).
- Datasheet of the FSR 0.5” Sparkfun Sensor. Available online: https://www.sparkfun.com/datasheets/Sensors/Pressure/fsrguide.pdf (accessed on 16 August 2018).
- Wannenburg, J.; Malekian, R. Physical Activity Recognition from Smartphone Accelerometer Data for User Context Awareness Sensing. IEEE Trans. Syst. Man Cybern. Syst. 2017, 47, 3142–3149. [Google Scholar] [CrossRef]
- ADXL335 Accelerometer. Available online: https://www.sparkfun.com/products/9269 (accessed on 29 June 2018).
- Datasheet of the ADXL335 Accelerometer. Available online: https://www.sparkfun.com/datasheets/Components/SMD/adxl335.pdf (accessed on 16 August 2018).
- Galvanic Skin Sensor. Available online: https://www.seeedstudio.com/Grove-GSR-sensor-p-1614.html (accessed on 29 June 2018).
- Specifications of Grove-GSR Sensor. Available online: https://www.mouser.com/catalog/specsheets/Seeed_101020052.pdf (accessed on 16 August 2018).
- Sendra, S.; Parra, L.; Lloret, J.; Tomás, J. Smart system for children’s chronic illness monitoring. Inf. Fusion 2018, 40, 76–86. [Google Scholar] [CrossRef]
- Wifi Bee ESP V1.0 Module. Available online: https://www.amazon.com/LilyPad-Arduino-Module-Wireless-Project/dp/B01LVZ4CC3 (accessed on 30 June 2018).
- Lavery, L.A.; Agrawal, C.M.; Athanaslou, K.A.; Constantinides, G.P.; Lanctot, D.R.; Zamorano, R.G. Foot Temperature and Health Monitoring System. U.S. Patent 6,767,330 B2, 27 July 2004. [Google Scholar]
- Monnard, C.R.; Fares, E.; Calonne, J.; Miles-Chan, J.L.; Montani, J.; Durrer, D.; Schutz, Y.; Dullo, G. Issues in Continuous 24-h Core Body Temperature Monitoring in Humand Using an Ingestible Capsule Telemetric Sensor. Front. Endocrinol. 2017, 8, 130. [Google Scholar] [CrossRef] [PubMed]
- Wu, K.; Zhang, Y. Contactless and Continuous Monitoring of Heart Electric Activities through Clothes on a Sleeping Bed. In Proceedings of the 5th International Conference on Information Technology and Application in Biomedicine, Shenzhen, China, 30–31 May 2008; pp. 282–285. [Google Scholar]
- Sendra, S.; Lloret, J.; García, M.; Toledo, J.F. Power saving and energy optimization techniques for Wireless Sensor Networks. J. Commun. 2011, 6, 439–459. [Google Scholar] [CrossRef]
- Heinzelman, W.R.; Chandrakasan, A.; Balakrishnan, H. Energy-Efficient Communication Protocol for Wireless Microsensor Networks. In Proceedings of the IEEE 33rd Annual Hawaii International Conference on System Sciences, Maui, HI, USA, 4–7 January 2000; pp. 1–10. [Google Scholar]
- Mohsen, N.A.; Mozaffari-Kermani, M.; Sur-Kolay, S.; Raghunathan, A.; Jha, N.K. Energy-Efficient Long-term Continuous Personal Health Monitoring. IEEE Trans. Multi-Scale Comp. Syst. 2015, 1, 85–98. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Healthy Range | Medium Range | Extreme Range | ||||
|---|---|---|---|---|---|---|---|
| Low | High | Points | Range | Points | Range | Points | |
| HR | 50 | 100 | 3 | ±20 | 2 | −30/+50 | −100 |
| HRV | 50 | 100 | 3 | ±20 | 2 | ±50 | 1 |
| Temperature | 35 | 37 | 3 | ±2 | 0 | −95 | −100 |
| Oxygen saturation | 95 | 100 | 3 | −2 | −10 | ±8 | −100 |
| Pressure | Balanced | 3 | Slightly unbalanced | 2 | Unbalanced | 1 | |
| Activity | Active | 3 | Medium | 2 | Sedentary | 1 | |
| Sweat | 0 | 0 | 1 | 1 | 0 | - | - |
| Points Range. | 0–4 | 5–9 | 10–13 | 14–16 |
| Description | Extremely bad | Bad | Good | Excellent |
| Parameter | Description | Parameter | Description |
|---|---|---|---|
| YO | Oxygen saturation average | RA | Current range of accelerometer |
| YT | Body temperature average | σO | Standard deviation of oxygen saturation |
| YHR | HR average | σT | Standard deviation of body temperature |
| YHRV | HRV average | σHR | Standard deviation of HR |
| YS | Sweat average | σHRV | Standard deviation of HRV |
| YP | Pressure average | YO-1 | Previous oxygen saturation average |
| YA | Accelerometer average | YT-1 | Previous body temperature average |
| RO | Current range of oxygen saturation | YHR-1 | Previous HR average |
| RT | Current range of body temperature | YHRV-1 | Previous HRV average |
| RHR | Current range of HR | YS-1 | Previous sweat average |
| RHRV | Current range of HRV | YP-1 | Previous pressure average |
| RS | Current range of sweat parameter | YA-1 | Previous accelerometer average |
| RP | Current range of pressure |
| Parameter | Description | Value | Parameter | Description | Value |
|---|---|---|---|---|---|
| OH1 | Oxygen saturation healthy range max. value | 100 | TE2 | Body temperature extreme range min. value | 30 |
| OH2 | Oxygen saturation healthy range min. value | 95 | σT1 | Max. value for standard deviation of the healthy range of body temperatures | 1 |
| OM | Oxygen saturation medium range value | 93 | σT2 | Max. value for standard deviation of the middle range of body temperature | 0.95 |
| σO1 | Max. value for standard deviation of the healthy range of oxygen saturation | 2.5 | HRVH1 | HRV healthy range max. value | 100 |
| σO2 | Max. value for standard deviation of the middle range of oxygen saturation | 0.5 | HRVH2 | HRV healthy range min. value | 50 |
| HRH1 | HR healthy range max. value | 100 | HRVM1 | HRV medium range max. value | 120 |
| HRH2 | HR healthy range min. value | 50 | HRVM2 | HRV medium range min. value | 30 |
| HRM1 | HR medium range max. value | 120 | σHRV1 | Max. value for standard deviation of the healthy range of HRV | 25 |
| HRM2 | HR medium range min. value | 30 | σHRV2 | Max. value for standard deviation of the middle range of HRV | 9.5 |
| σHR1 | Max. value for standard deviation of the healthy HR range | 25 | SH | Value for sweat average | 0.5 |
| σHR2 | Max. value for standard deviation of the middle range of HR | 9.5 | t1 | Time for forwarding data | 30 min |
| TH1 | Body temperature healthy range max. value | 37 | αO | Oxygen saturation threshold | 4 |
| TH2 | Body temperature healthy range min. value | 35 | αT | Body temperature saturation threshold | 0.4 |
| TM1 | Body temperature medium range max. value | 39 | αHR | HR threshold | 14 |
| TM2 | Body temperature medium range min. value | 33 | αHRV | HRV threshold | 14 |
| TE1 | Body temperature extreme range max. value | 43 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
García, L.; Parra, L.; Jimenez, J.M.; Lloret, J. Physical Wellbeing Monitoring Employing Non-Invasive Low-Cost and Low-Energy Sensor Socks. Sensors 2018, 18, 2822. https://doi.org/10.3390/s18092822
García L, Parra L, Jimenez JM, Lloret J. Physical Wellbeing Monitoring Employing Non-Invasive Low-Cost and Low-Energy Sensor Socks. Sensors. 2018; 18(9):2822. https://doi.org/10.3390/s18092822
Chicago/Turabian StyleGarcía, Laura, Lorena Parra, Jose M. Jimenez, and Jaime Lloret. 2018. "Physical Wellbeing Monitoring Employing Non-Invasive Low-Cost and Low-Energy Sensor Socks" Sensors 18, no. 9: 2822. https://doi.org/10.3390/s18092822
APA StyleGarcía, L., Parra, L., Jimenez, J. M., & Lloret, J. (2018). Physical Wellbeing Monitoring Employing Non-Invasive Low-Cost and Low-Energy Sensor Socks. Sensors, 18(9), 2822. https://doi.org/10.3390/s18092822