1. Introduction
The rapid development of information communication and technology (ICT) has made possible the automatization of human-assisted tasks in a wide range of applications, such as asset tracking for logistics (mainly within the context of 4.0 Industry) or people monitoring for security and safety applications. In recent years, the Internet of Things (IoT) [
1,
2] and sensor networks [
2,
3,
4] have contributed dramatically towards this goal.
One of the reasons for increasing the automation level in low- and medium-complexity tasks is to reduce the risk of mistakes made by employees. Routinely tasks are under supervised due to an overestimation of the level of self-confidence of the employees. In sectors such as health, this is especially critical, as it has a direct impact in the health condition of the patients. For example, medication errors are behind 22,300 deaths per year in the National Health Service (NHS) [
5], having also a significant economic impact [
6].
Several factors related to medication error can be highlighted [
7]: (i) similarity in the packaging or names of the drugs; (ii) patients allergic to some drugs; (iii) drugs whose use is very specific. Up until 2008, the wrong route of drug administration, wrong medication, and wrong dose were responsible for 9.5%, 16%, and 40.9% of patient death due to medication errors, respectively [
7]. These figures support the need for automation and/or the introduction of additional ICT supervision systems in the aforementioned medical procedures.
The implementation of ICT systems for automation of logistics and management in hospitals should consider the following design requirements [
2,
8,
9]:
(i) the use of disposable, low-cost sensors, which will be tagged to the patients, medication, and medical assets to be tracked; and
(ii) the connectivity between hardware (readers, end-user mobile devices, servers with their databases located at the hospital ICT department) should be adapted to the existing network infrastructure of the hospital and/or be based on wireless networks.
Among the advantages provided by ICT systems for location and tracking in healthcare applications [
2], the following can be noted:
(i) Minimization of medical errors: on the one hand, patients labelled with a RFID wrist can be tracked in real-time, so doctors, physicians and nurses can know if there is an issue (e.g., a delay) in the medical treatment required by the patient. On the other hand, drugs can be better tracked, thus reducing the risk of wrong or forgotten drug administering to patients.
(ii) Optimization of resources: for example, doctors and nurses can know the exact amount of blood supplies. Some medical assets and instrumentation can also be located easily, including information about their availability.
ICT systems can be grouped according to the most extended technologies: optical identification systems (barcodes and QR codes) [
10] and radiofrequency-based systems [
11].
The use of QR codes and barcodes for traceability and logistics has been introduced in a wide range of sectors for decades, and also in the field of medicine (e.g., traceability of patients during the different stages of the medical treatment at the hospital). Aiming to overcome some of the limitations of these optical-based tracking systems (listed in
Table 1), radiofrequency-based technologies have been developed and gradually implemented, first in the area of transport and logistics (e.g., toll collection in highways, warehouses and retail stores), and recently in the field of medical services (e-health).
Radiofrequency-based systems for location and tracking consist mainly of tags (attached to the items or patients to be monitored) and tag readers. Two technologies can be distinguished: on the one hand, high-frequency (HF) radio frequency identification (RFID) [
12] and near-field communication (NFC) [
12] systems, in which wireless information transfer between the tags and the reader is based on electromagnetic field coupling [
13,
14]; and on the other hand, ultra high-frequency (UHF) RFID systems, in which electromagnetic backscattering is used to send information from the RFID tags to the reader [
13,
14].
Table 1 summarizes the advantages and disadvantages of NFC/HF RFID and UHF RFID technologies, also compared to optical systems.
Several examples of RFID systems already deployed in hospitals and medical services can be found in the literature [
15,
16], some of them highlighted in
Table 2. For example, [
15] presents a medication administration system which automatically verifies medication and generates the corresponding prescription, aiming to avoid errors related to paper-based procedures. After deploying the application, it was reported that the number of medical mistakes was significantly reduced. The introduction of a RFID system is described by [
17] for a better control of medical assets, providing faster response time (as the doctors and nurses spend less time searching for medical devices). Another example of fully operational RFID system for tracking and managing drugs and patients is presented in [
18]. In this case, a dual NFC/UHF RFID system is proposed to ensure the detectability and also to make traceability easier. In addition to this, the level of automation with respect to handheld NFC readers is improved.
A hybrid infrared/RFID real-time location system (RTLS) is described in [
20], providing detection ranges up to 2 m even in non line-of-sight (NLOS) conditions. This system was initially conceived for monitoring and tracking medical items (e.g., to detect those requiring maintenance), and later extended to track nurses when they respond to emergency calls or visit patients.
In most of the RFID-based systems for healthcare applications presented in
Table 2, a survey has been conducted to evaluate the level of satisfaction and comfort of the employees (doctors, nurses) and patients. In general, there is a good acceptance of these systems as they effectively contribute to reduce medical errors, enhancing patients’ monitoring and attention during hospitalization. The main complaints come from the need of adoption of new medical protocols (training of doctors and nurses), especially if they require additional tasks (e.g., approaching the items tagged to the NFC or RFID reader). This problem could be mitigated if UHF RFID systems, with longer reading range, were used.
The compatibility and coexistence of the RFID-based system with already implanted ICT systems in the hospital is also an important issue [
2,
22]. To achieve this goal, it is suggested to start with small RFID projects [
15] (as the proof-of-concept presented in this contribution) ensuring that the tested system can be later scaled up to cover the entire hospital needs.
Another issue, missed in the deployment and evaluation of the RFID systems cited in the literature review, is a proper characterization of the physical layer, such as the coverage of the RFID antennas or the selection of the RFID antennas’ placement, to fulfill coverage and detectability requirements.
Aim and Scope
This contribution aims to provide detailed information concerning the implementation and testing of a basic RFID system for e-Health applications, in particular, for tracking and managing assets (medication and patients) in hospitals. While the architecture of the proposed system is quite similar to those already deployed in hospitals worldwide, the aim here is to provide additional details about implementation features that must be taken into account to ensure proper functionality: (i) choice of the antennas depending on the coverage area and cost; (ii) item traceability depending on the RFID tags’ detectability; and (iii) simplicity and ease of use of the graphical user interface (GUI). Although the scope of the RFID system described in this contribution is restricted to a small area of the hospital, the architecture is fully scalable to cover the needs of the different medical services in a hospital.
The implemented system allows the tracking of medical assets that are tagged with RFID tags within a hospital. UHF RFID technology is selected over the most extended NFC and HF RFID technology to minimize the hardware infrastructure. The former also allows ease of coverage/reading area conformation by simply using different kind of antennas. Information is stored in a database, which can be accessed from end-user mobile devices (tablets, smartphones) where the position and status of the assets to be tracked is displayed.
2. System Architecture
2.1. Radio Frequency Identification (RFID) Hardware and Considerations about Signal Propagation
As outlined in
Table 2, the main advantage of UHF RFID over HF RFID systems is the capability of providing longer reading distances, thus minimizing the need for approaching items to the readers. Conventional UHF RFID antennas and readers can provide a reading distance up to 6–7 m far from the antenna even in NLOS and multipath conditions, so a single UHF RFID antenna is enough to provide coverage within a hospital room.
UHF RFID-based systems for management and tracking applications consist of [
12,
13]: (i) a set of UHF antennas; (ii) one or several RFID readers; (iii) a computer that manages the RFID readers; and (iv) UHF RFID tags attached to the items to be tracked. While the cost of a RFID tag is less than 0.05 EUR, UHF antennas are within the range of 20–200 EUR (depending on their specifications and requirements), and UHF RFID readers are in the range of 200–1100 EUR also depending on their specifications and performance. The use of antenna hubs enables increasing the number of antennas that can be controlled by a single RFID reader, thus cutting down the cost of the overall system. Typical specifications/performances of a reader involve the number of tags read per second, or the number of UHF antennas that can be controlled.
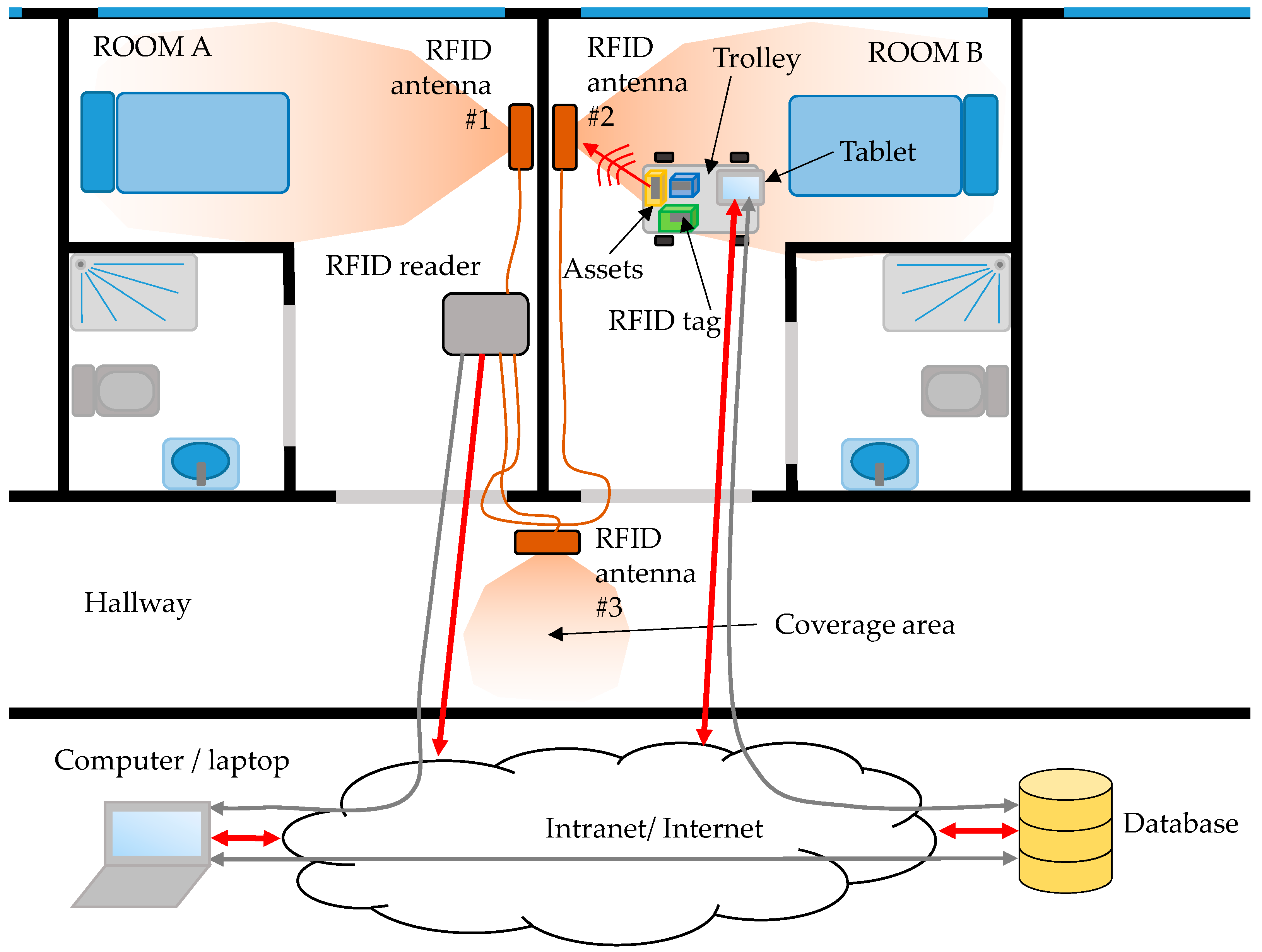
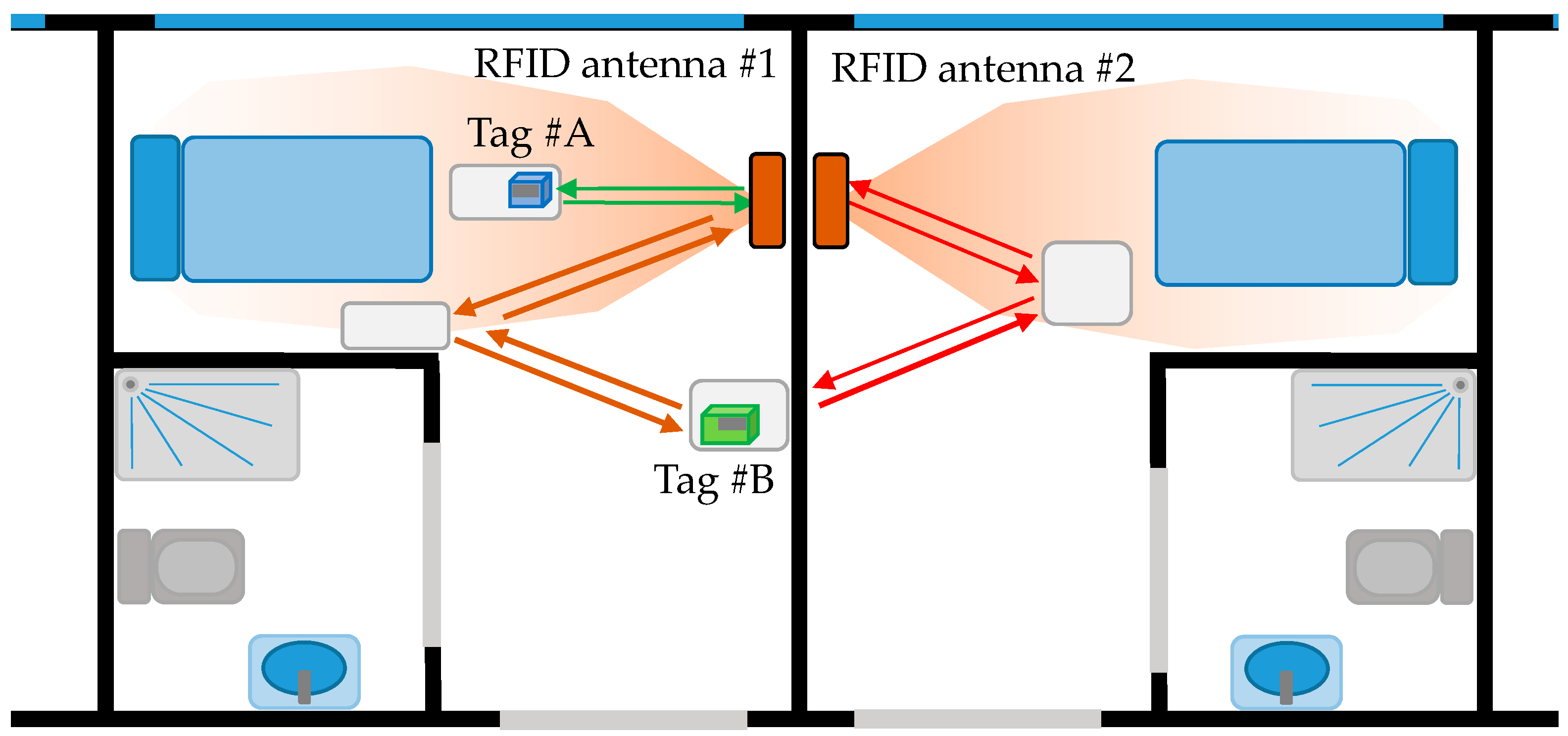
RFID antennas are placed to provide a coverage area within a place of interest, for example around the beds in hospitalization rooms (4–5 m
2). It is important to avoid coverage areas overlapping to ensure that RFID tags are detected by just one antenna. Another source of error is the presence of multipath [
23,
24], especially in indoor scenarios like the one illustrated in
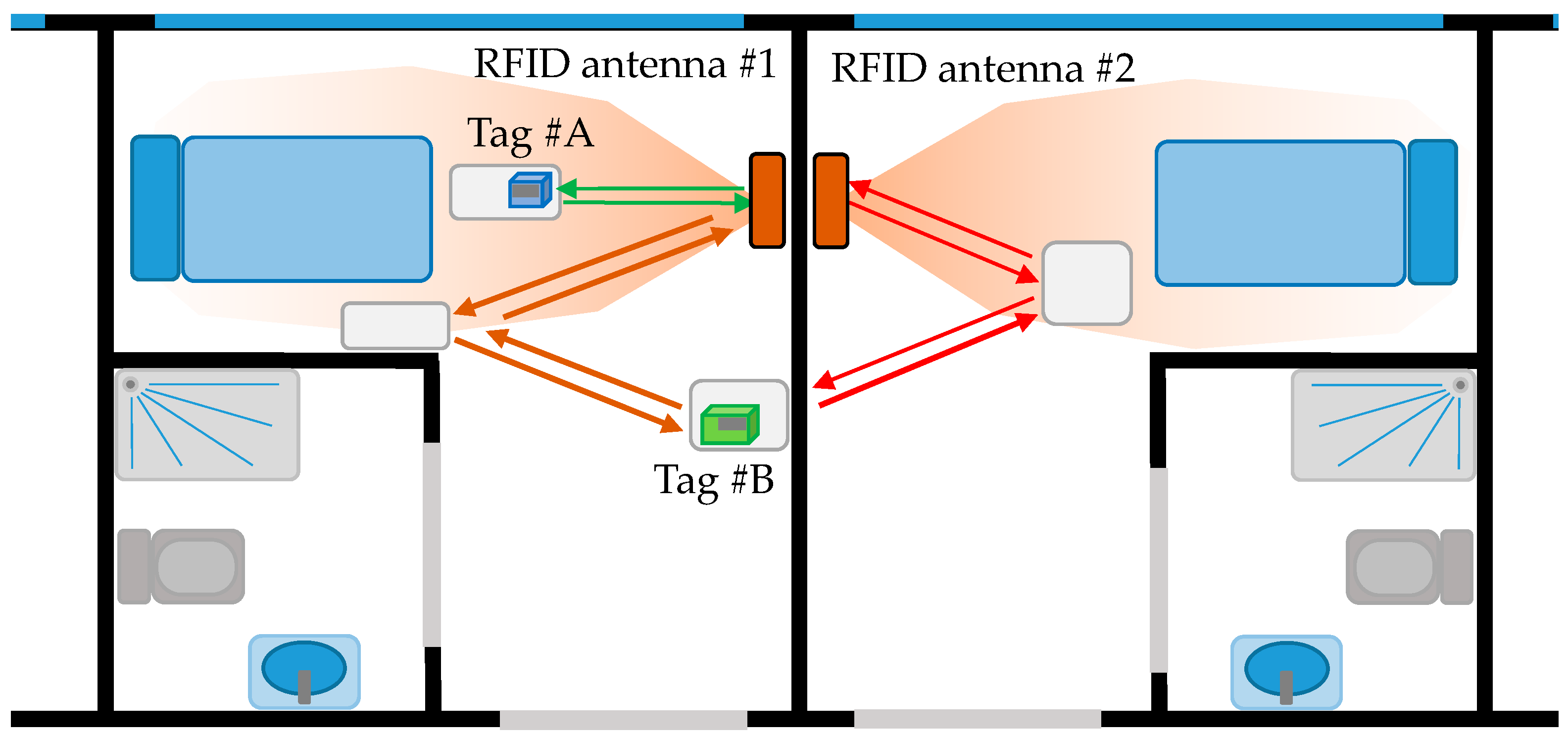
Figure 1. Under normal operation conditions, only those items within the coverage area of the RFID antenna are detected. However, multipath can result in the detection of RFID tags beyond the coverage area of the antenna (
in-channel interference [
25]). To overcome this problem, the following solutions can be adopted: (i) reducing the power transmitted by the RFID antenna while ensuring that the minimum level to detect RFID tags is achieved within the coverage area; (ii) using antennas whose radiation pattern fit the area of interest, thus minimizing reflections. For example, directive antennas are considered in the example shown in
Figure 1 to provide coverage around the beds. The use of directive antennas also contributes to mitigate multipath contributions.
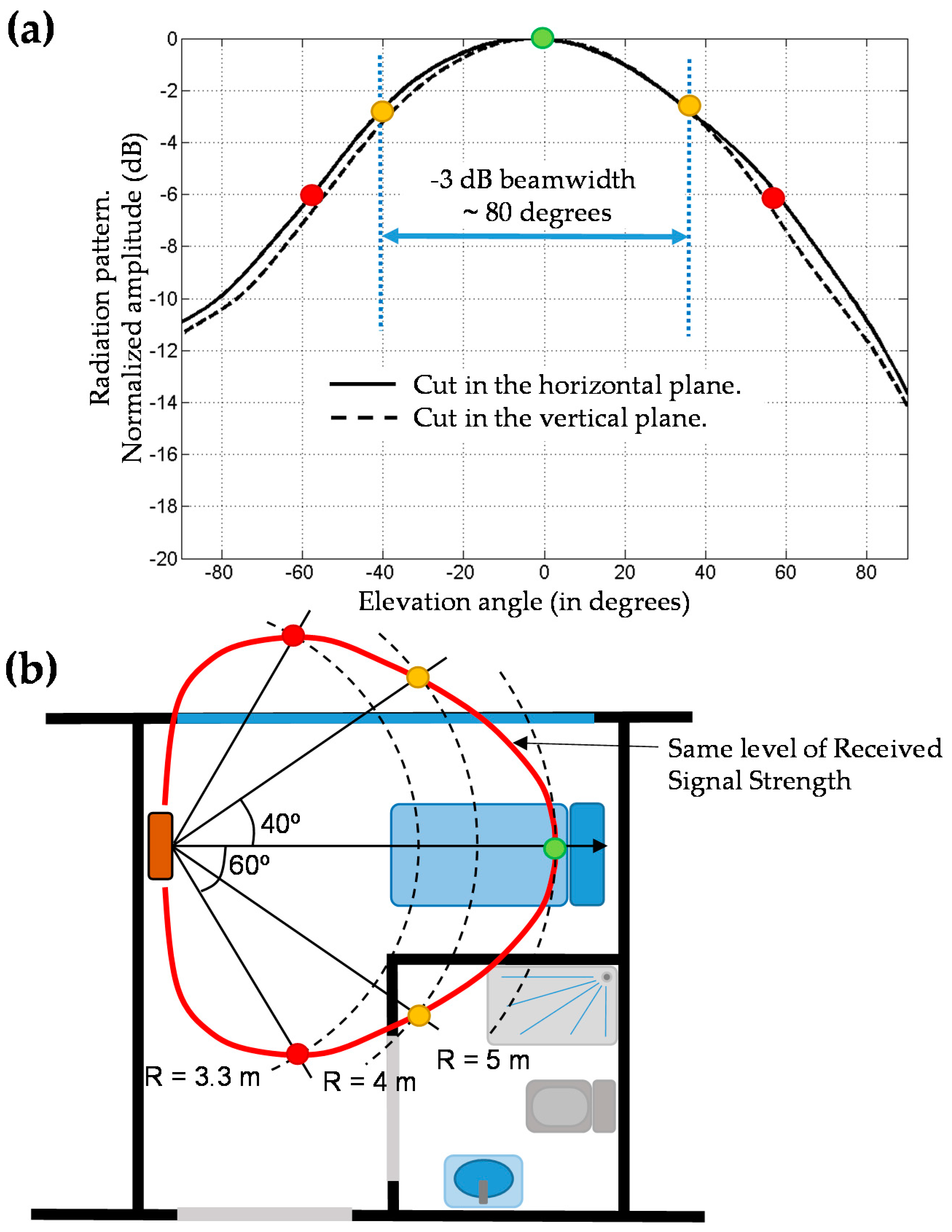
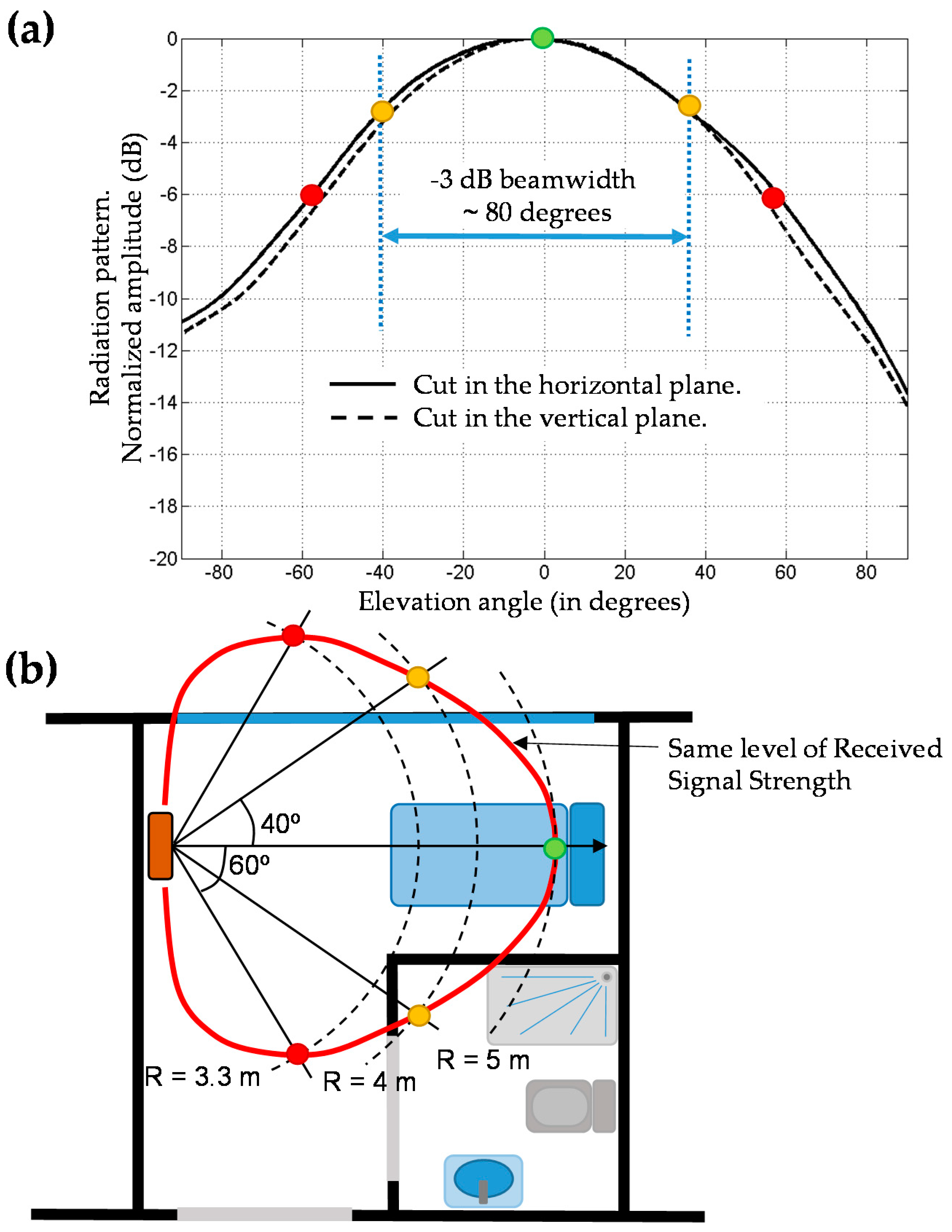
To illustrate the influence of the antenna radiation pattern,
Figure 2a shows the main cuts of the radiation pattern of a RFID antenna [
26], that has around 80° −3 dB beamwidth in both planes (resulting in ~8.1 dBi directivity). Given the radiation pattern, it is possible to obtain an estimate of the coverage area considering propagation losses (
Att). These losses are estimated according to a log-distance path loss model. Among the different methodologies and models proposed for indoor channel characterization [
27,
28], the International Telecommunication Union Radiocommunication Sector (ITU-R) path loss definition [
29] has been selected as a trade-off between accuracy and complexity (1):
where
f is the working frequency (in MHz) of the UHF RFID system (868 MHz in Europe),
R is the distance from the transmitter to the tag,
n is the path loss exponent (20 for free-space propagation, 33 for an indoor environment such as the one described in this contribution), and
Lf accounts for signal attenuation when passing from one floor to another (
Lf = 0 dB in this case, as the RFID reader and RFID tags are on the same floor).
An example is presented in
Figure 2b. Let us suppose that the UHF RFID antenna reading range reaches
R = 5 m at its pattern maximum (green dot in
Figure 2b). At an angle of 40°, the radiation pattern decays 3 dB. Thus, compensable attenuation for this pattern level is given by (2):
with
= 5 m and
Comp.Att (dB) = 3 dB. Applying Equation (1),
= 53.8 dB, so that
= 50.8 dB, yielding
~4 m.
Equation (2) can be used to predict the angle at which the same signal level as at the pattern maximum is reached given the distance from the antenna. For example, for
= 3.3 m,
= 47.8 dB, yielding
Comp.Att (dB) = 6 dB. From
Figure 2a, this corresponds to an angle of approximately 60°. Repeating this procedure for different angles and/or distances, an estimate of the UHF RFID antenna coverage area in the scenario to be deployed can be obtained, allowing users to decide whether this kind of antenna fulfills the coverage requirements or not.
In addition to this, the power level of the RFID reader can be adjusted in most of commercial UHF RFID readers, so it can be tuned to modify the maximum reading distance (e.g., 5 m in the case of
Figure 2b example).
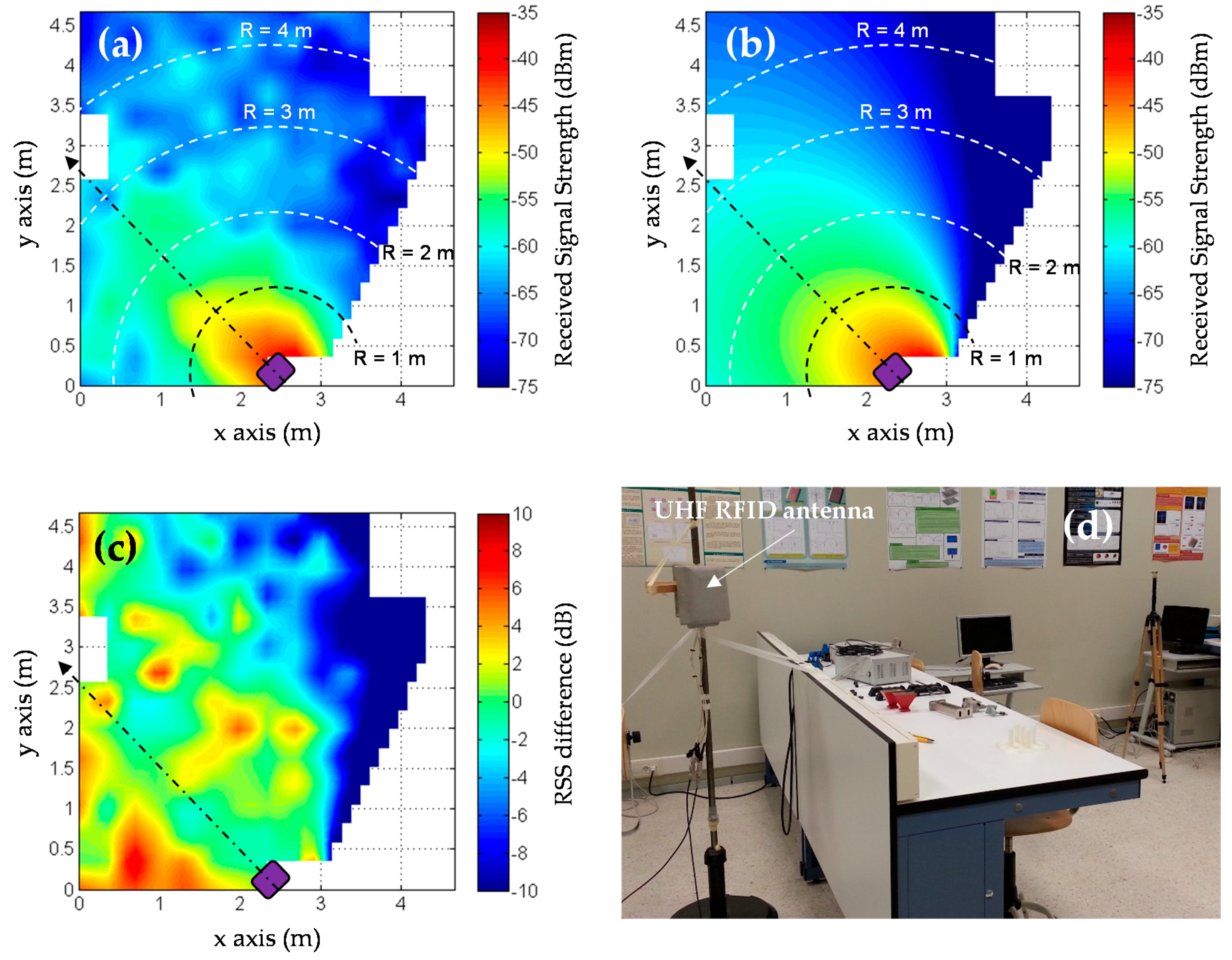
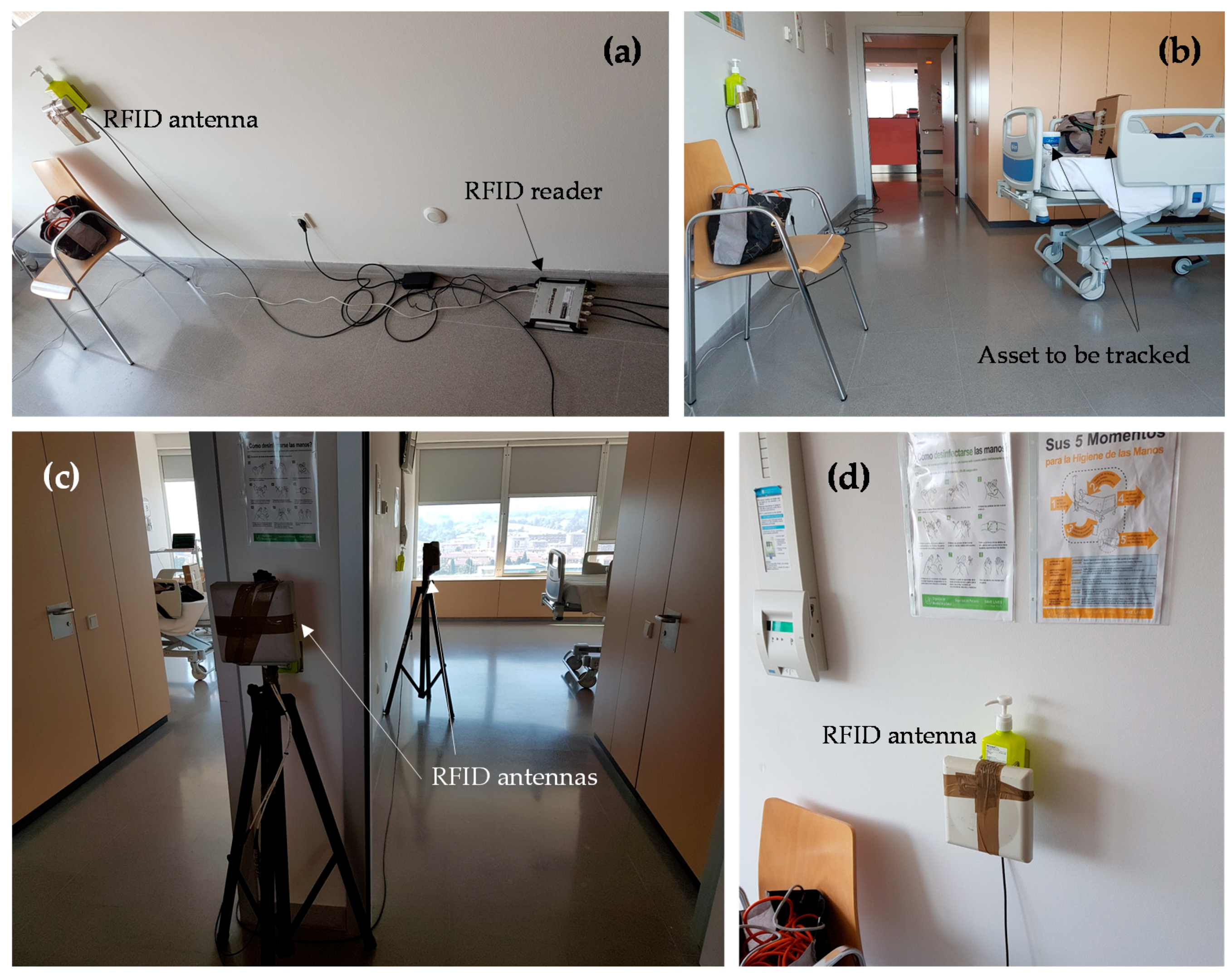
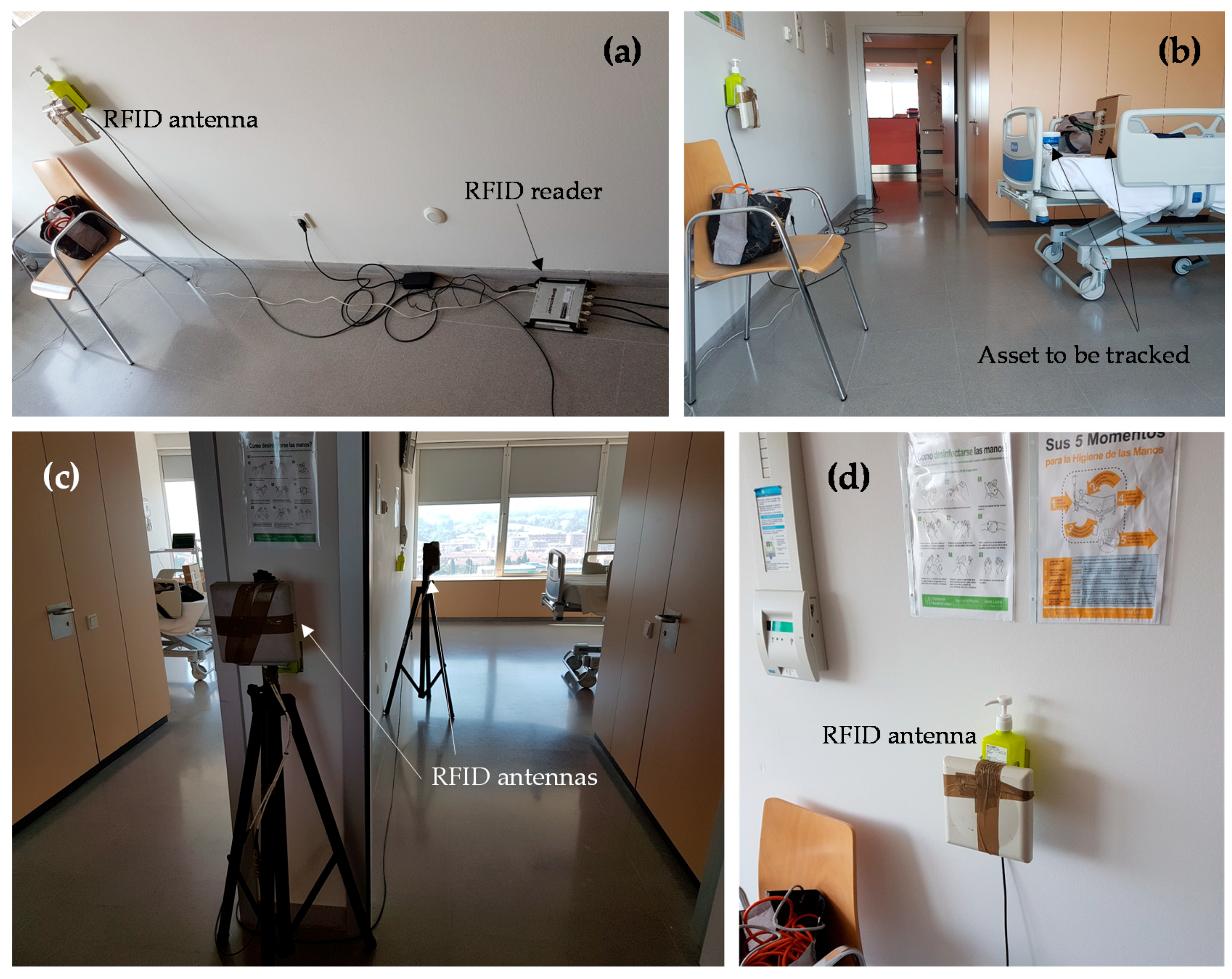
A better way to assess RFID coverage in the scenario where the system is going to be deployed is, of course, by means of measurements. In the case of RFID antennas, coverage can be evaluated empirically by simply placing one or several RFID tags at those positions of interest, recording the values of received signal strength (RSS) and then plotting the RSS values over a plane of the scenario [
30]. An application example is shown in
Figure 3, where RSS measurements, conducted in the scenario shown in
Figure 3d, were compared to theoretical RSS values calculated considering an indoor propagation losses model [
30] and taking into account the radiation pattern of the UHF RFID antenna [
30]. The effect of multipath can be clearly observed in the measurements (
Figure 3a): signal strength does not monotonically decay with distance. Of course, more accurate methodologies for coverage evaluation (such as the proposed in [
24]) can be considered depending on the system requirements.
In general, RFID tags exhibit a dipole-like radiation pattern [
31] with linear polarization. Because of this, most UHF RFID antennas are circularly polarized, so that the received signal strength is quite independent from RFID tag orientation with respect to the UHF RFID antenna.
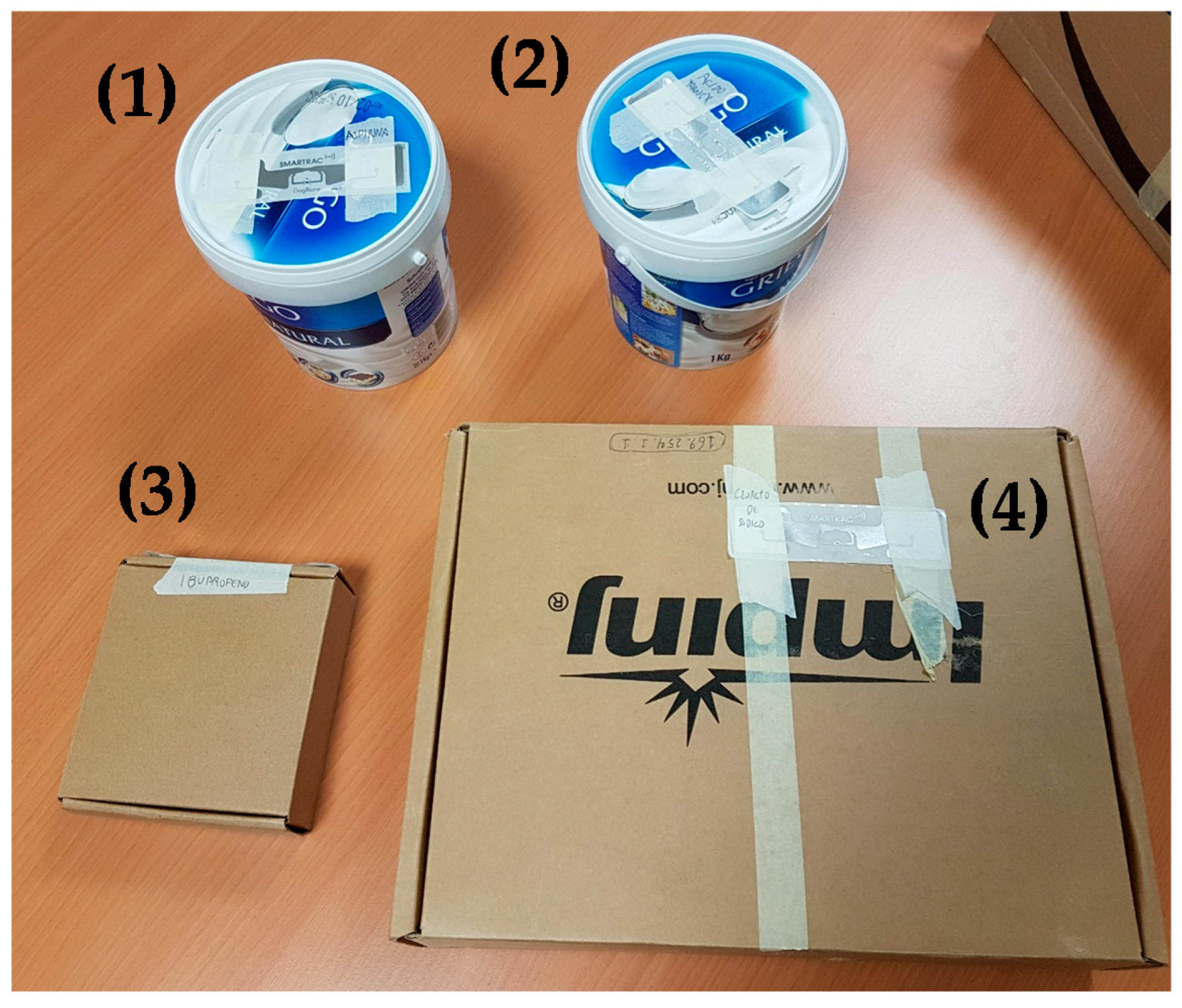
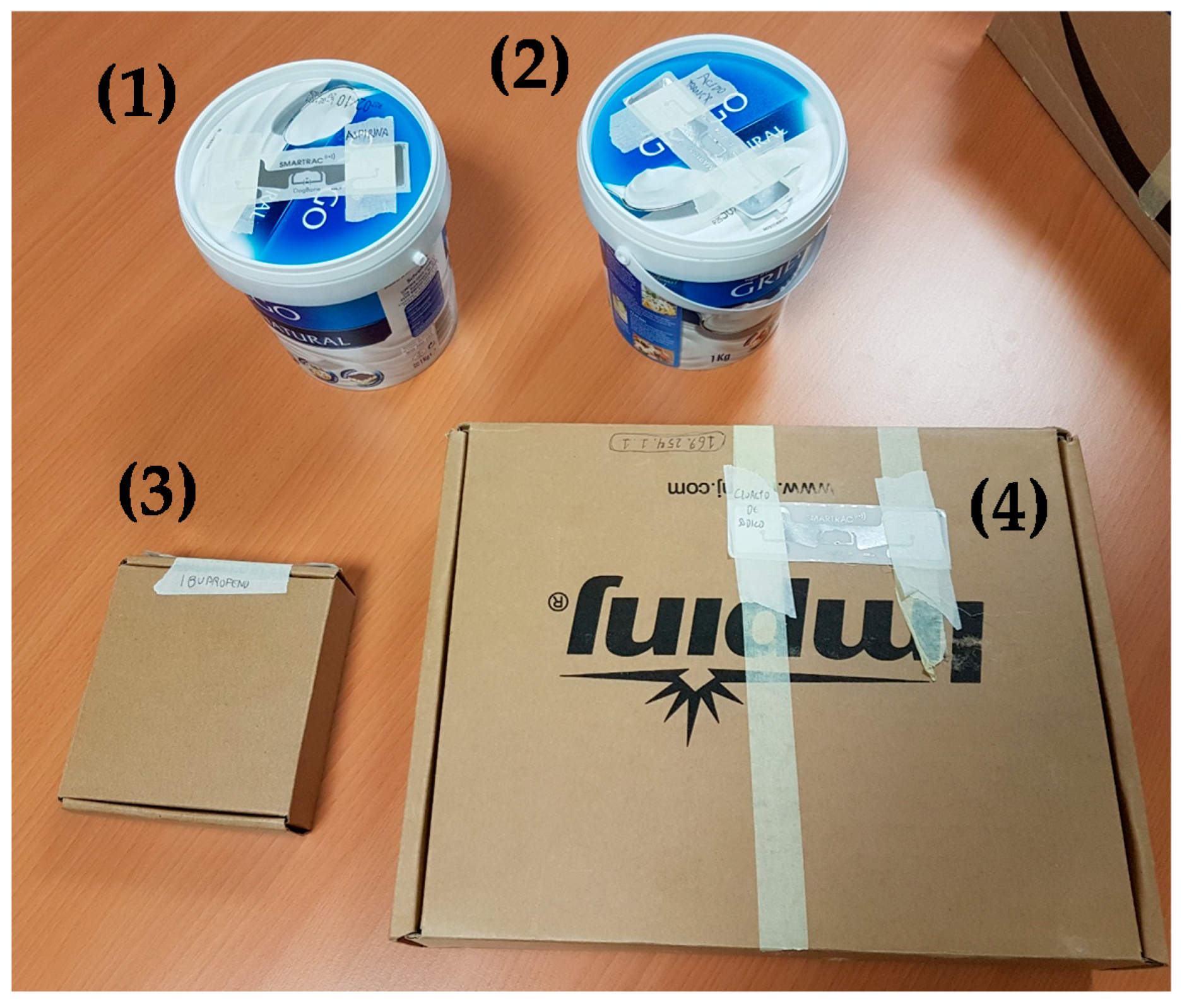
Another issue is the performance of RFID tags depending on the surface where they are placed. Low-cost UHF RFID tags do not perform well when placed on metallic containers or boxes, or recipients containing liquids, thus requiring a special kind of RFID tag (whose cost is typically 2–50 times higher). In the case of hospitals, most of the drugs are presented in cardboard or plastic containers, allowing the use of low-cost, conventional RFID tags.
Coaxial cables are used to connect UHF antennas to the readers. In order to reuse existing hospital infrastructure, and thus minimize the cost of the RFID system deployment, connection between antennas and the RFID reader could be done using the radio and television distribution network based on 75 ohm coaxial cable. In that case, RFID antennas and readers which characteristic impedance of 75 ohm (instead of the most common 50 ohm) should be used. In Europe, the upper frequency band of radio and television broadcasting is more than 100 MHz below UHF RFID frequency band (865–868 MHz), so there would not be interferences between RFID and the signals of radios and televisions.
Next, to connect the RFID readers and the computer that manages them, the easiest solution is to provide local area network (LAN) connectivity, since most of the hospitals have several public and protected LAN domains, depending on the targeted users (visitors and patients, doctors and physicians, etc.). It must be pointed out that most of current RFID readers existing in the market can be connected via Wi-Fi (e.g., by means of an Ethernet/Wi-Fi Access Point), thus reducing the need for deploying additional Ethernet cable infrastructure.
2.2. RFID Software
RFID software architecture can be divided into two parts: the first one is devoted to managing the readings of RFID tags within the coverage area of the antennas, storing and updating the information in a database. The second one includes the GUI where the information stored in the database is displayed to end-users and administrators, as well as allowing the collecting of their inputs.
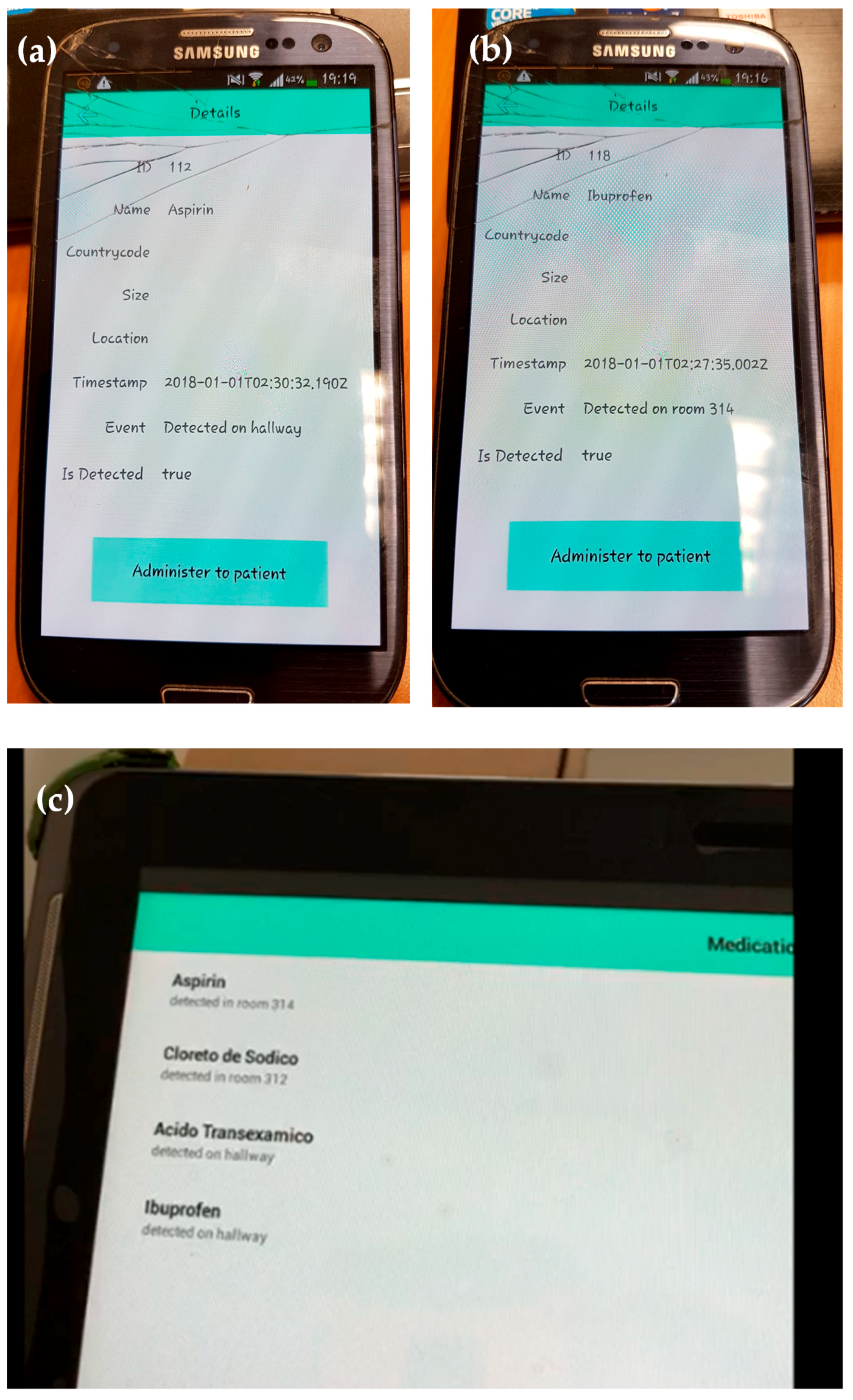
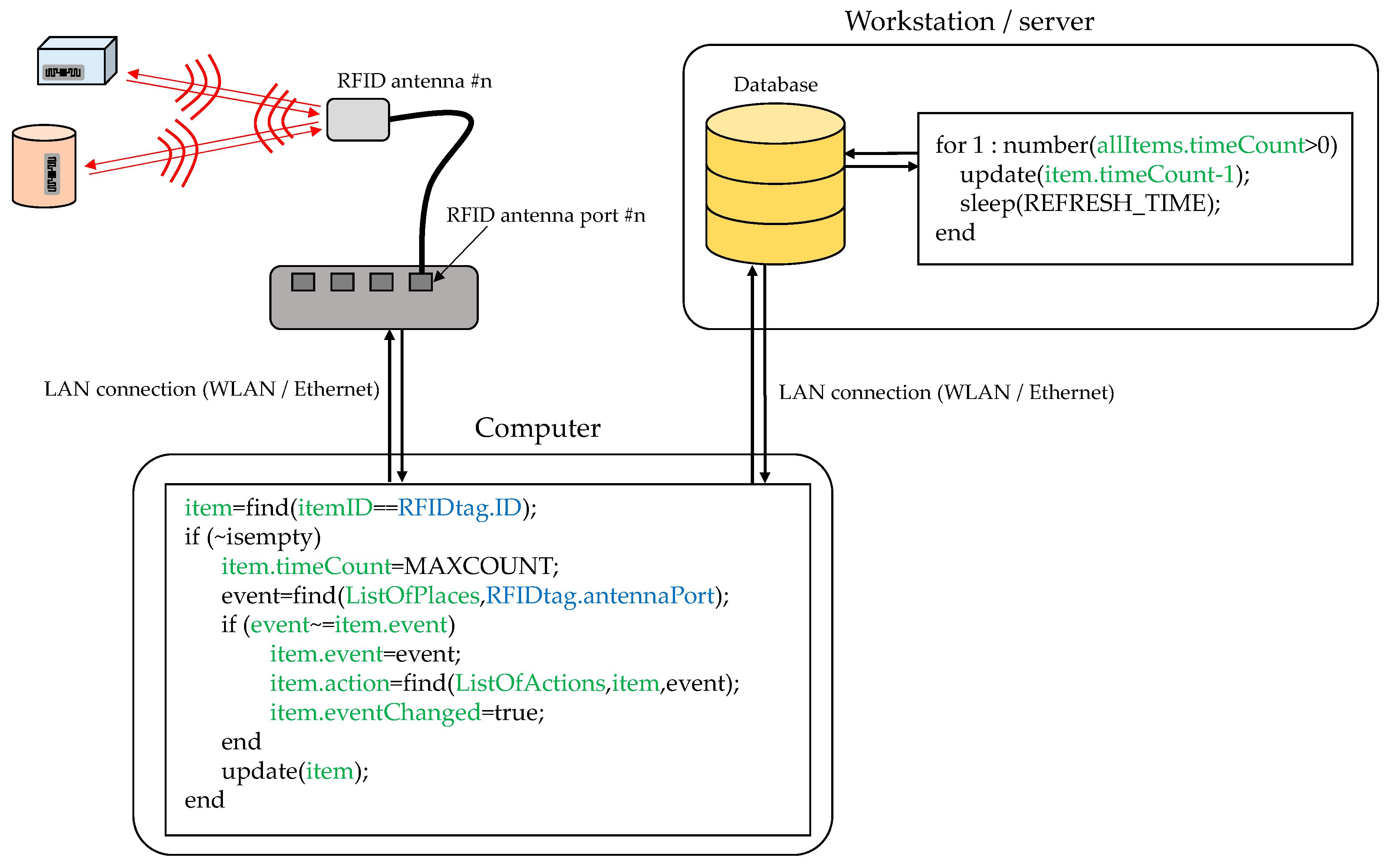
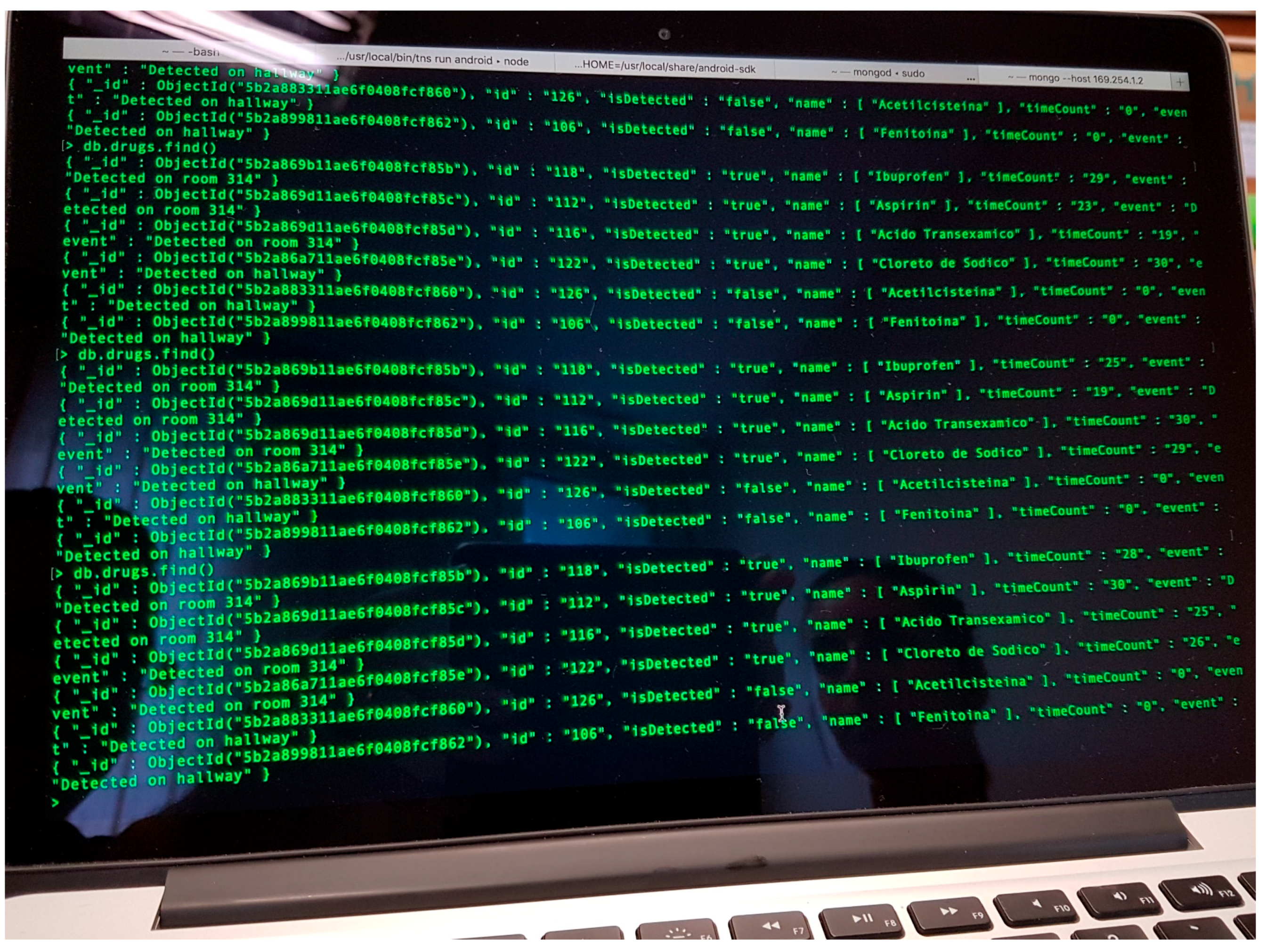
RFID tags (especially passive ones) can store a limited amount of information about the associated item. Because of this, RFID tags are typically used as pointers to registers in a database where information about the item is stored. In the example shown in
Figure 4 and
Figure 5, each tagged item has an associated entry in a database containing the following information: (i)
item ID: RFID tag identifier or pointer; (ii)
item name: name of the medical asset or associated medicine/drug; (iii) event: indicates where the RFID tags are detected; (iv)
action: depending on the kind of item and the event, different actions are triggered (e.g., administering the item to the patient on the room); (v)
eventChanged: flag that tells if, during the period of two consecutive readings, the event has changed (e.g., if the item has been moved from one room to another); (vi)
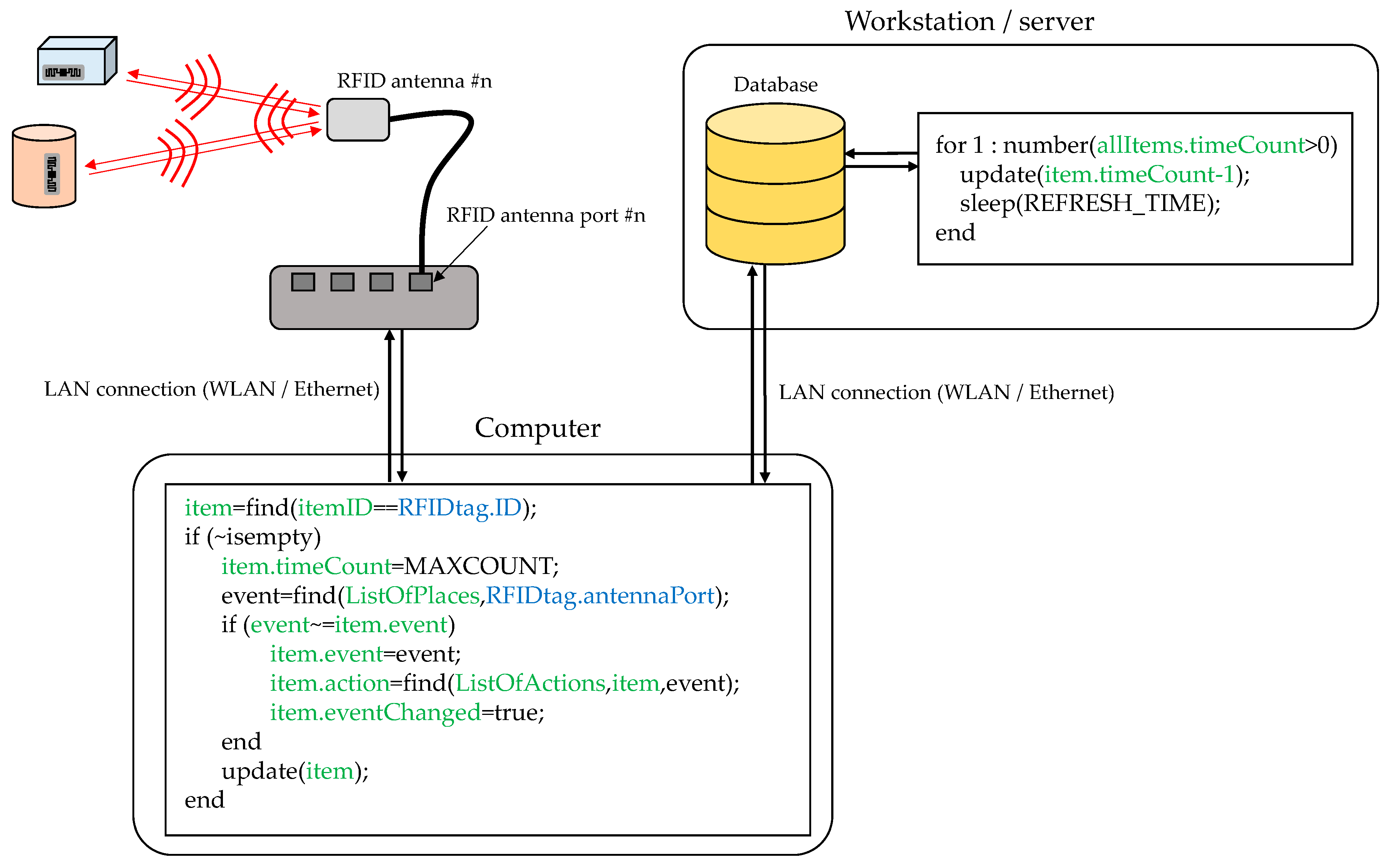
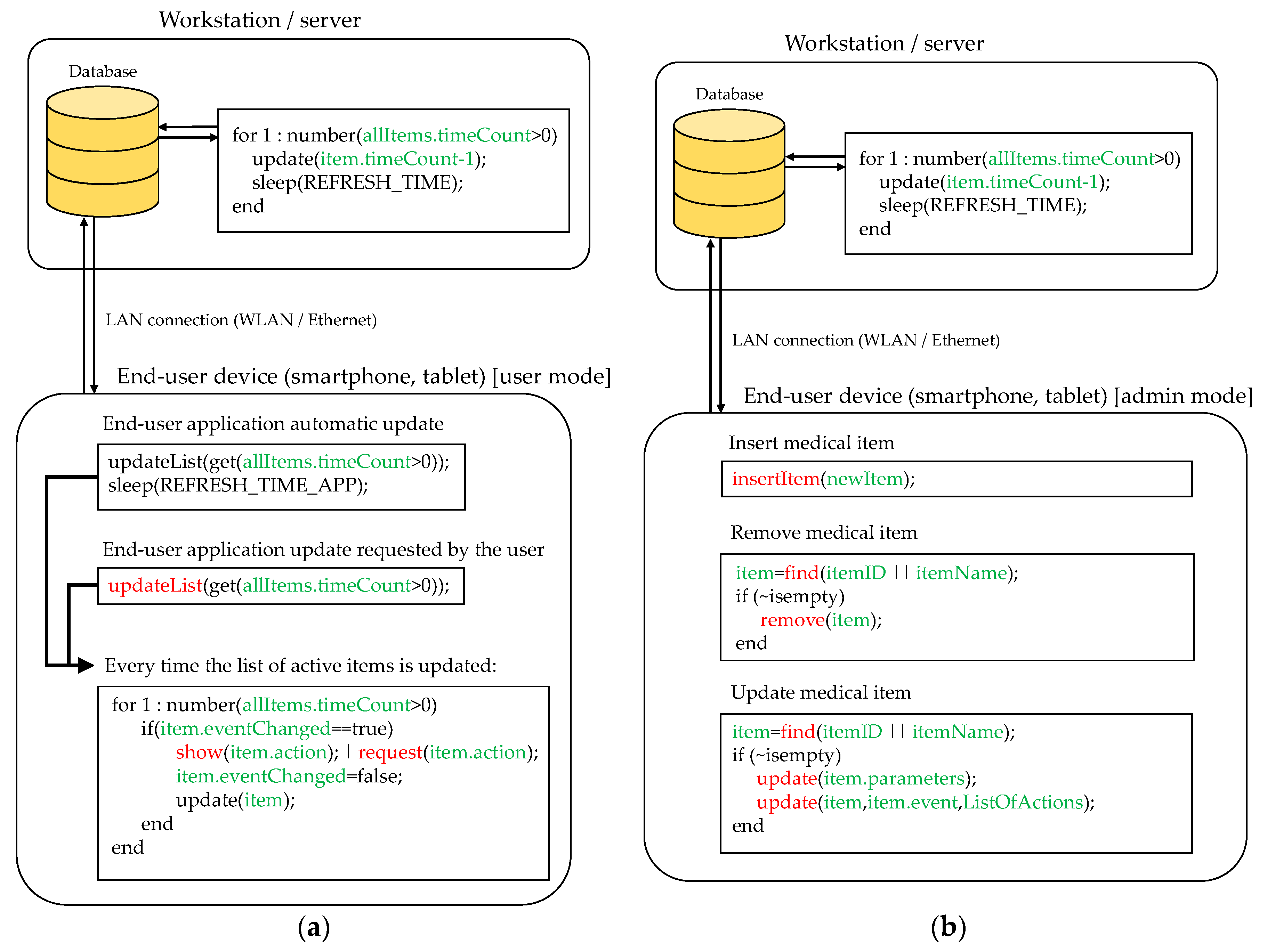
timeCount: counter to consider if the item is active or not within the coverage area of an antenna. This database can be stored in a workstation/server, eventually integrating them together with other information systems and services of the hospital.
RFID readers are configured to periodically send interrogation signals, each one associated to the n-th RFID reader port (which is connected to the n-th RFID antenna). If a RFID tag receives this interrogation signal with enough intensity, it will send a response signal. Collision avoidance protocols are implemented for those cases in which two or more RFID tags respond at the same time to the interrogation signal. That means that only one response is received every time. This could result in missed tags for those cases where there are tens of RFID tags within the coverage area of the antenna and the RFID reader throughput is low. This also leads to another problem associated with latency.
For example, if there are 10 RFID tags within the coverage area of the n-th antenna, and the RFID reader throughput is 10 tags per second, each tag is detected 1 time per second on average. Thus, a protocol that tells the end-user that the tag is within the coverage area, although it is not constantly read, must be implemented. The solution proposed in this contribution is shown in
Figure 4: every time a RFID tag is read, the field
timeCount is set to its maximum value (
MAXCOUNT). Then, the value of this counter is decreased periodically in the database. If the value of the counter reaches zero, then it is considered that the item is no longer within the coverage area of the antenna. However, if a new reading is done before the counter reaches zero it is set back to
MAXCOUNT. The value of
MAXCOUNT can be adjusted depending on the throughput of the RFID readers and the expected maximum number of RFID tags within the coverage area. Thanks to this, items can be considered “active” for a few seconds in the location associated to the n-th antenna where they have been detected.
RFID tags attached to items that are not stored in the database (e.g., clothing of hospital visitors) will be detected as well, thus reducing the effective throughput of the readers. This issue must be considered when selecting the value of
MAXCOUNT. As shown in
Figure 4, once a RFID tag is detected, the first action is to check whether the item associated to the tag exists in the database and, otherwise, the reading is discarded.
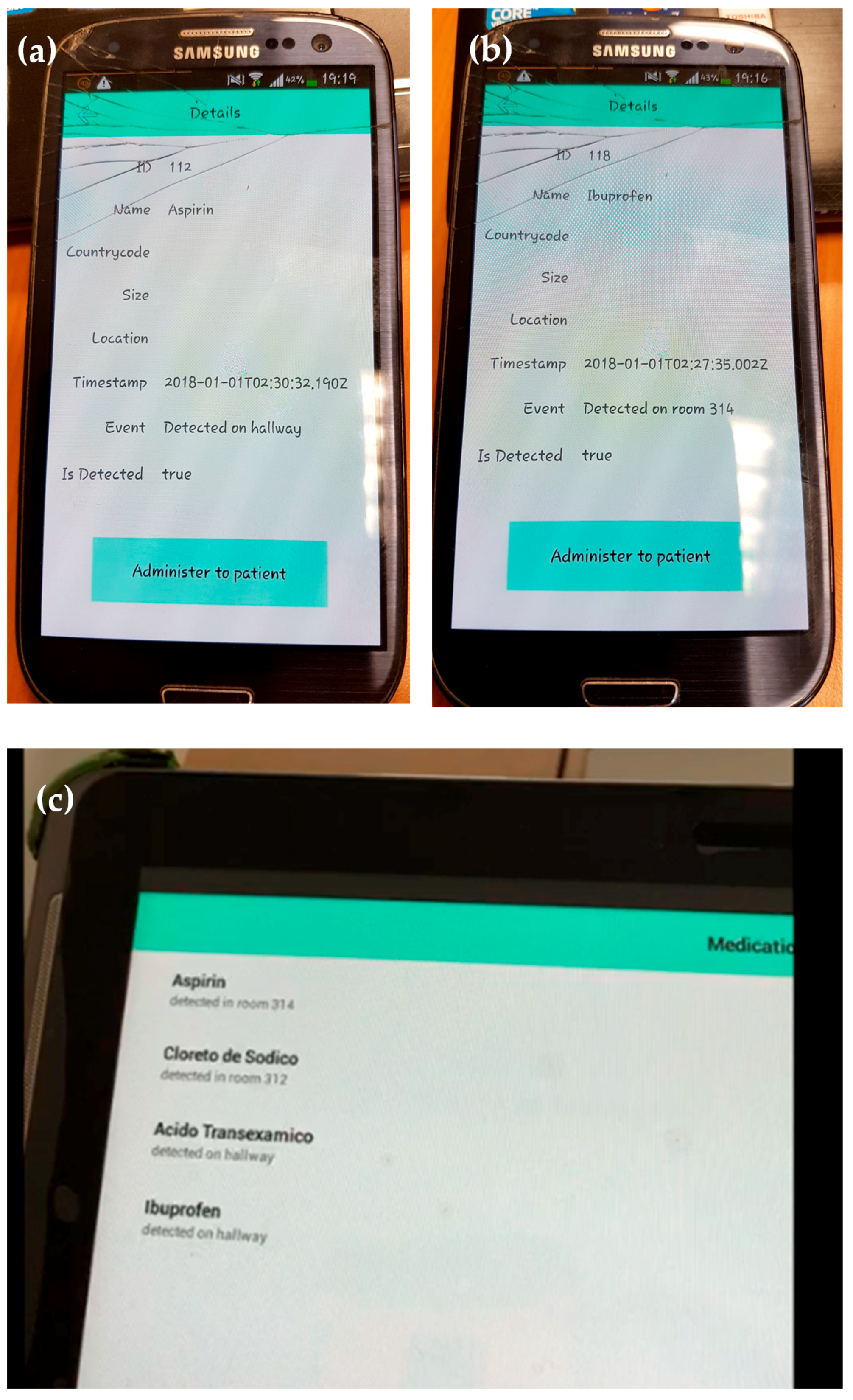
The information stored in the database eventually has to be displayed to end-users (doctors, physicians) and system administrators. Hospitals including e-health procedures usually provide mobile devices (such as smartphones, tablets) to their employees, giving them access to real-time information about patients, supplies, etc. In this regard, mobile applications for these devices have been implemented to make easier the visualization of the information and the collecting of inputs. Furthermore, these devices can be connected to the hospital wireless LAN to access different information systems (such as the RFID system database), thus avoiding the need for additional network infrastructure.
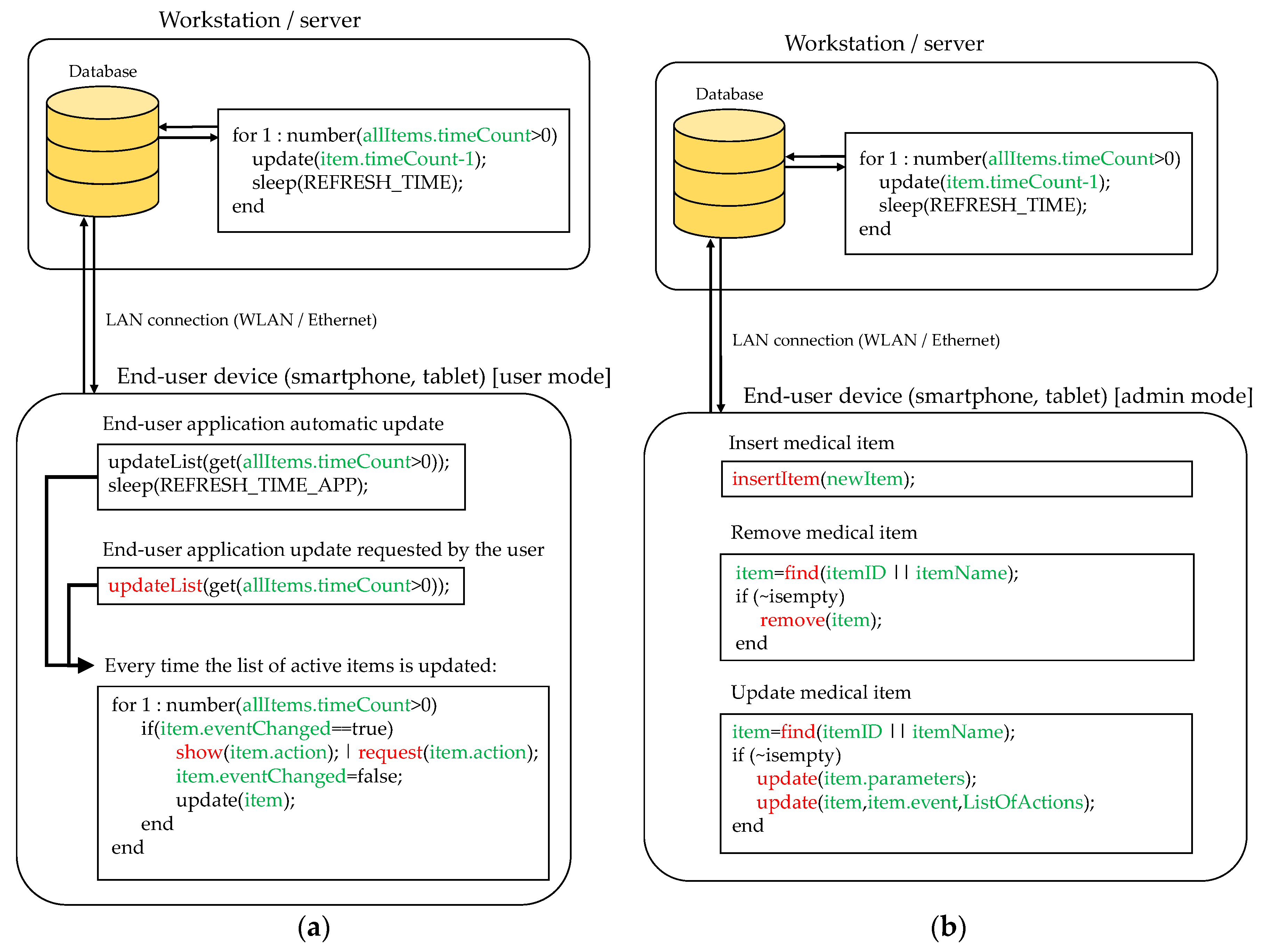
Figure 5 illustrates two basic functionalities of the proposed mobile application.
Figure 5a corresponds to user mode functionality. In this configuration, the mobile application shows those items considered “active” within one of the coverage areas of the RFID system (that is,
timeCount > 0). The list of active items is periodically refreshed (controlled by the variable
REFRESH_TIME_APP). Besides, the user can manually request an update of this list (
Figure 5a, function
updateList). Every time the list is updated, the application checks if there was an update in the event associated to each active item and, if so, the application checks if there is an action required, whose type will depend on the event and the kind of detected item.
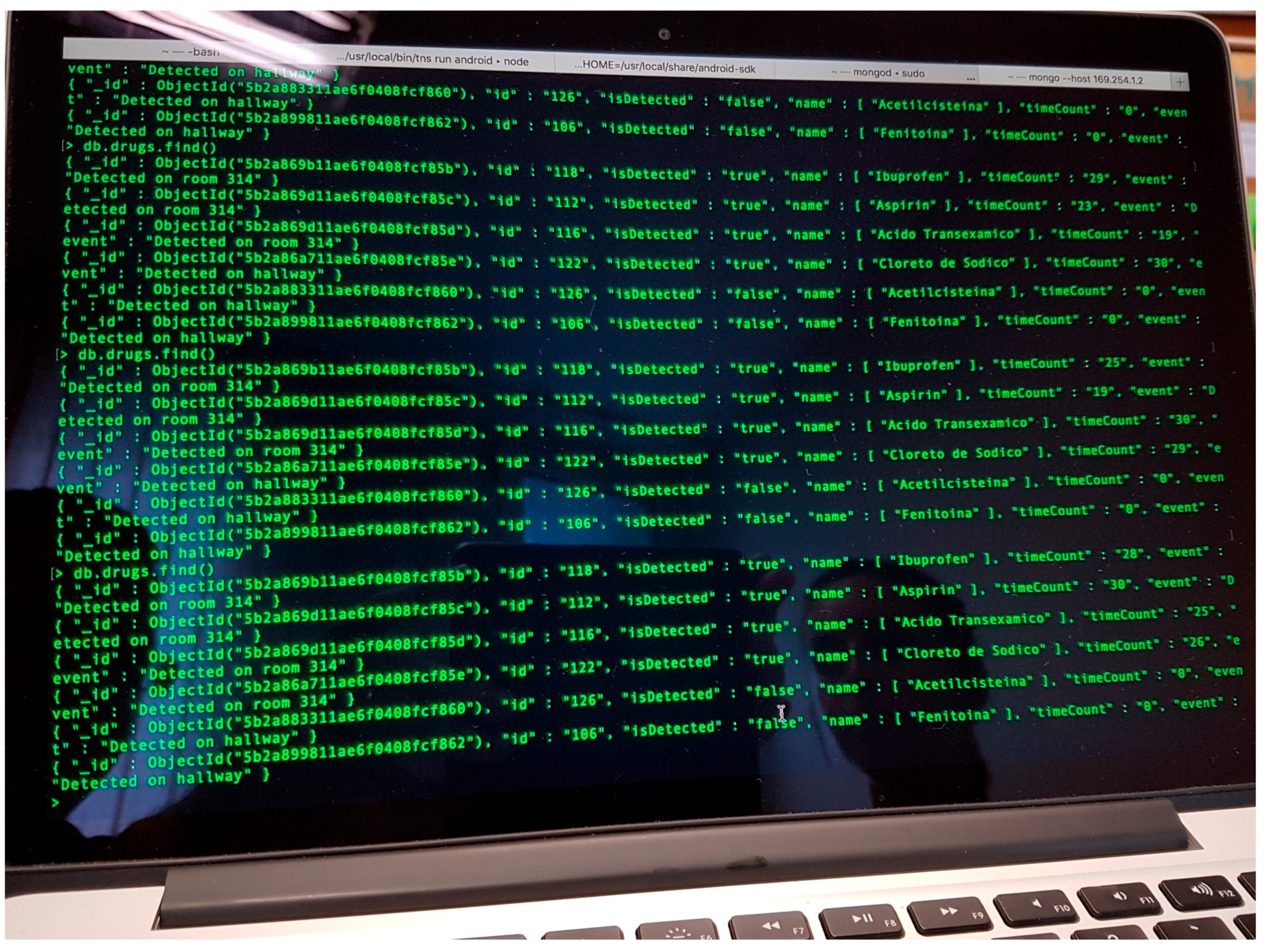
To illustrate this, let us suppose that a box containing ibuprofen has to be administered to the patient in room 312. First, this item is detected in the hallway (event: “detected on hallway”). Later, a nurse goes into room 312 carrying the box of ibuprofen, so when the box is within the coverage area of the RFID antenna located in room 312, the event in the system database is updated to “detected in room 312”. Then, taking into account the event (“detected in room 312”) and the item (“ibuprofen”), the system checks if there is an action that should be performed (for example, “administer medicine to patient”). If so, the system will require the end-user to complete the action, e.g., by displaying a message in the mobile application (together with another kind of alarm such as smartphone vibration or short ring). Once the end-user completes the required task, the action associated to the item is updated.
Moreover, the mobile application can be used for administration purposes. In this case, the user must log in as administrator. Three basic actions are considered (see
Figure 5b): (i) register a new medical item in the database; (ii) remove an existing medical item; and (iii) update the information associated to the item (e.g., action to be done when a certain event happens). Of course, more complex functionalities can be added, but these are beyond the scope of the proof-of-concept presented in this contribution.
4. Discussion
The RFID system presented in
Section 2, although quite simple, shares several characteristics with others already operational in hospitals worldwide cited in the literature review of
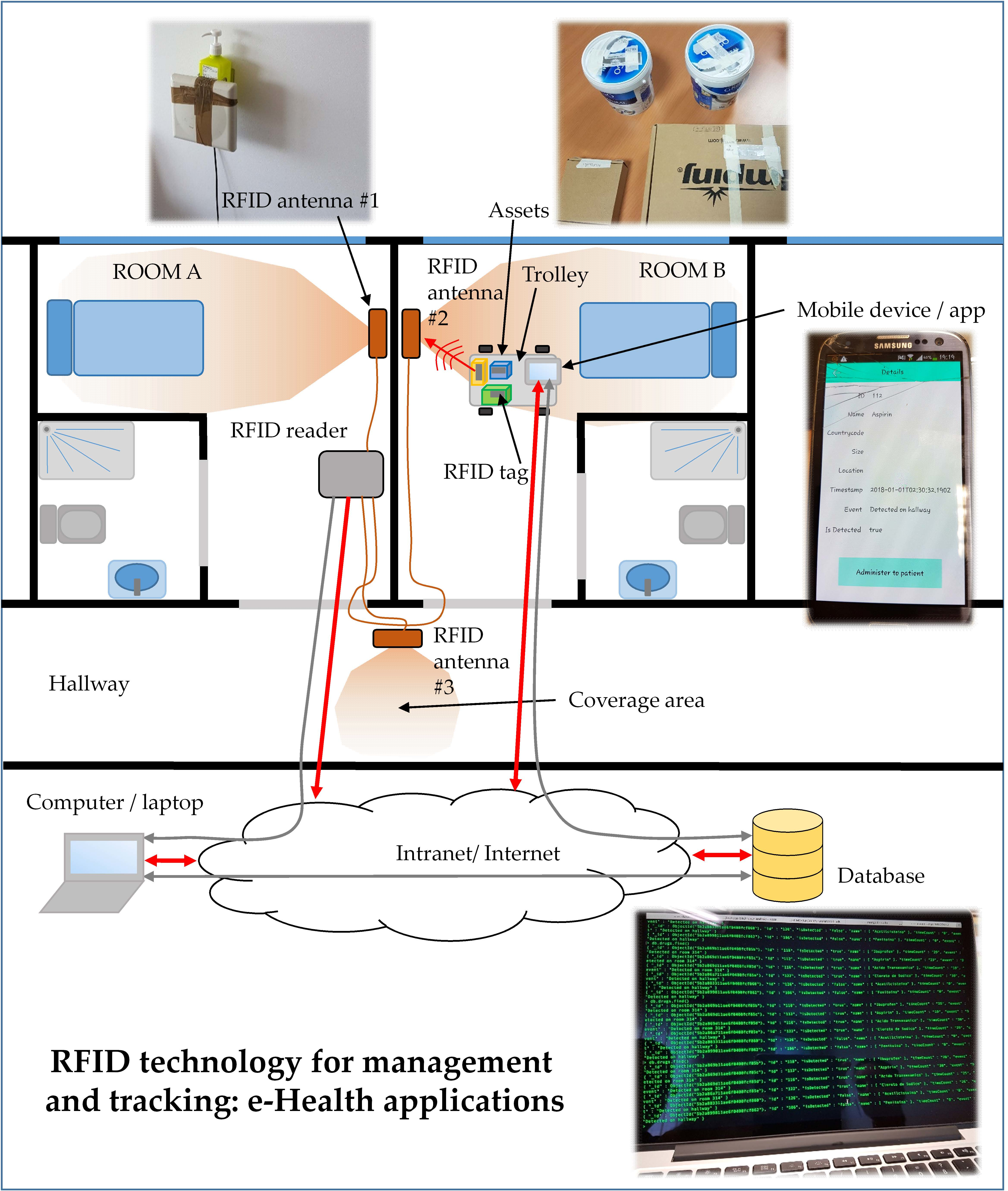
Section 1. As in those systems, the hardware front-end consists of several antennas placed in the areas of interest within the hospital connected to an RFID reader. Items and patients to be monitored are tagged with passive RFID tags. Information about the tags detected by the reader is sent to a database that stores the status of these tags and the associated items. Using a mobile application, end-users can retrieve information about the items in real-time (events, location, etc.).
The simple proof-of-concept shown in this contribution proves the feasibility and ease of implementation and use of these systems. In this case, it should be remarked that once the items are tagged with RFID tags, potential users (doctors, nurses) do not need to interact with the hardware front-end. Furthermore, RFID antennas and readers could be hidden on the roof of the rooms and hallways so that employees, patients and visitors would not notice this hardware infrastructure. This is an important advantage over other RFID technologies that require the users to come closer to RFID readers (e.g., NFC, HF RFID).
Physical layer characterization, and, in particular, assessment of the radioelectric coverage should be taken into account when deploying UHF RFID systems, as reflections in walls and objects (especially in those with large metallic surfaces) may result in unexpected readings of tags outside the designed coverage area. Depending on the scenario, a basic coverage analysis as the one described in
Section 2.1 can be enough. RSS information of the backscattered signal could be used to ensure that the detected RFID tag is actually within the coverage area of the RFID antenna. For example, RSS values could be stored in the database of the system and, if they are below a certain threshold, a message could be displayed (e.g., “item #n not detected properly. Please place it in another location”).
As mentioned in
Section 1, one of the design goals of IoT-based systems for management and logistics is to minimize human interaction with the system, not only increasing the level of comfort of the users, but also minimizing the risk of mistakes. Even though this kind of RFID system is conceived to increase the level of automation of routine tasks such as drug administration, it still requires a minimum interaction from the users (e.g., pressing the button “medicine successfully administered” in the case of the example presented in this contribution), and, as stated in
Section 1, this procedure still has some risk of human failure/mistake (e.g., pressing the button in advance, and then not administering the drug). Nevertheless, these RFID systems can also contribute to making the location and identification of medical errors easier, as they provide location and time information about the items registered within the system (medical assets, medicines, etc.).
Another possible improvement, already introduced in other areas where RFID systems are used for management and logistics could be related to automatic registration and removal of medical assets in the database, without requiring an end-user to manually insert the information associated to each item. These procedures can be implemented by placing several RFID antennas and readers devoted to registering new medical items, so every time a RFID tag is read by these antennas a new register in the database is created. Similarly, several RFID antennas and tags can be located in the area devoted to medical assets and drug disposal: every time an RFID tag is read in this area of the hospital, the item is deleted from the database.

 ,
, 

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}