Several research studies have already focused on the investigation of objective measures and methods that could be used in the assessment of ADHD patients based on body worn sensors. In previous studies, the analysis of the data gathered from several body worn sensors has been used both for hypothesis testing and for pattern recognition. Hypothesis testing based on wearable sensors data has shown statistically significant differences in several parameters measured from ADHD patients compared with non-ADHD controls [
11,
12]. Pattern recognition based on a predefined set of features calculated from an inertial measurement unit (IMU) showed good classification results in distinguishing ADHD patients from non-ADHD controls when performing a continuous performance test in a controlled environment [
10].
The authors in [
11] used objective measures to find statistically significant differences between children with ADHD and non-ADHD controls based on the forces applied during manipulation of a novel object and movement rhythmicity measured by sensors. The DSM-IV-TR criteria [
6] was used to diagnose ADHD. A series of tests involving movements of the upper limb were administered while “off” medication. The results showed that significant differences could be observed between groups in movement rhythmicity, manipulation of a novel object, and dexterity. Moreover, the study showed that certain parameters such as the speed of execution of a requested movement and the measured tremor were unaffected.
As previous studies found differences in the way ADHD children move compared to typically developing non-ADHD controls, O’Mahoni et al. attempted to develop an objective measure to help in the diagnosis of ADHD by characterizing the movements of each group in terms of a set of features, and then quantifying these features to classify each individual into likely ADHD and non-ADHD groups. The authors used two inertial measurement units (IMUs) comprising a tri-axial accelerometer and a gyroscope, one attached to the waist and the other to the ankle of the dominant leg, and took continuous measurements during an approximately 1-h visit to a psychiatric consultancy. The authors combined time domain as well as frequency domain calculations to extract 668 different features. Using a support vector machine (SVM), the results showed up to 95% for both accuracy and sensitivity.
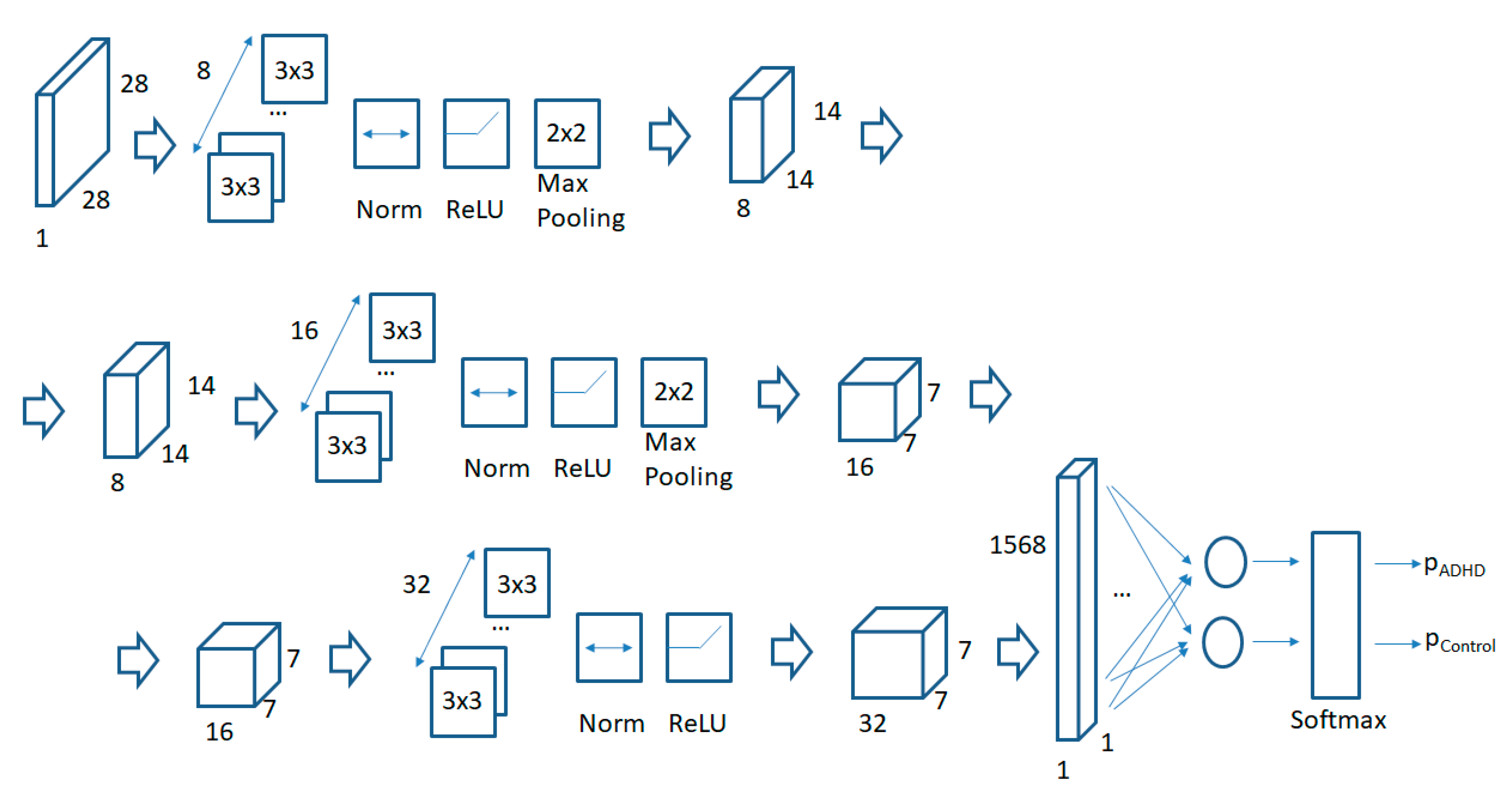
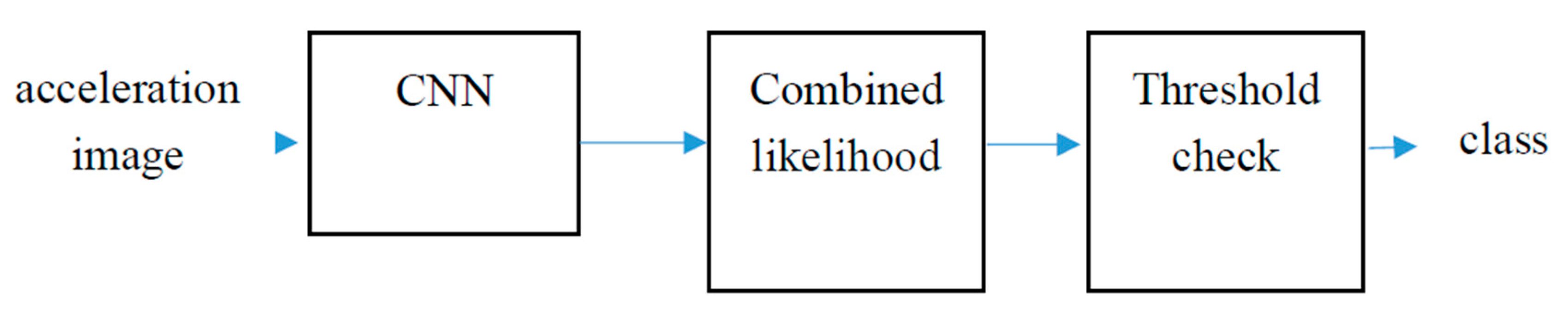
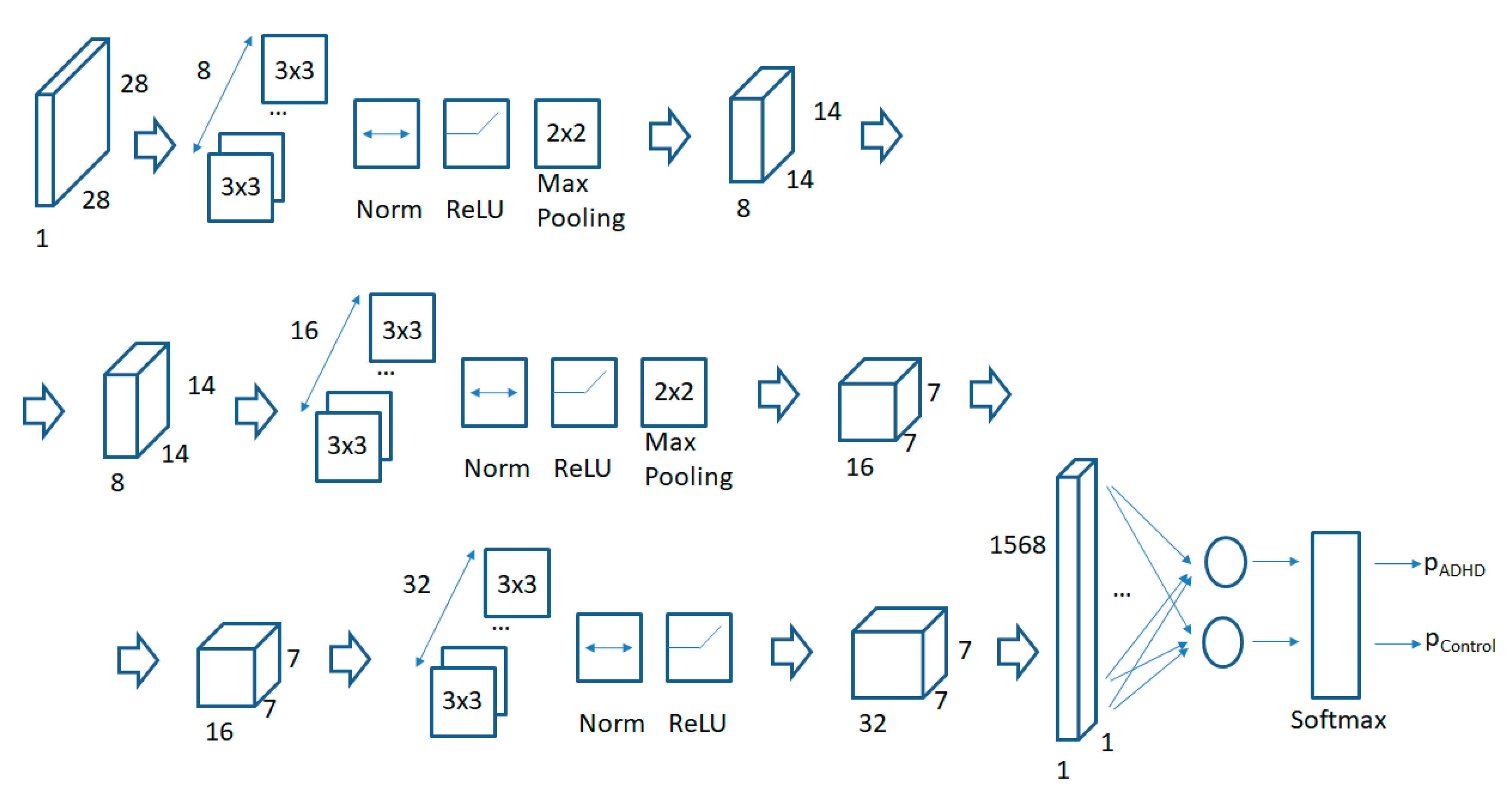
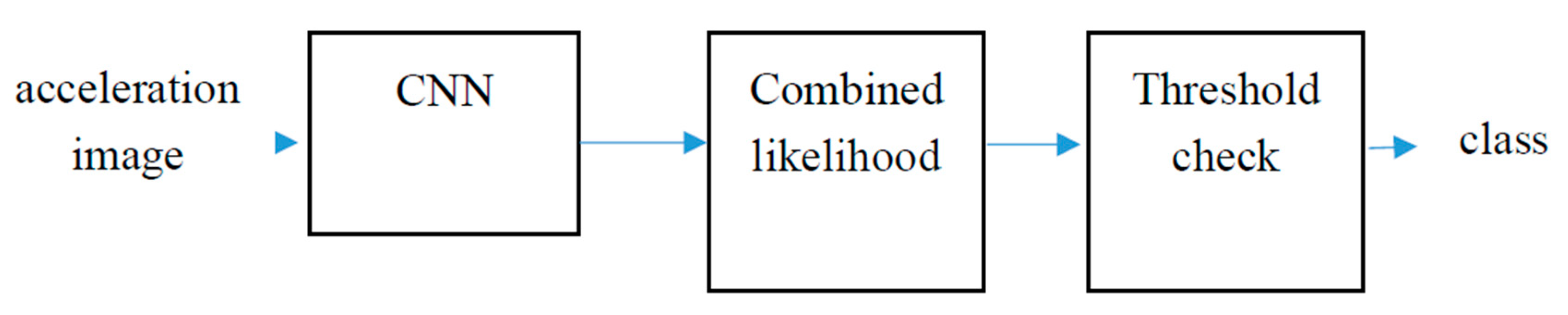
In summary, previous studies have shown statistically significant differences in the way children with ADHD and typically developing non-ADHD control children move as captured by body worn sensors attached to different parts of the body. Both dominant and non-dominant limbs have been used to record acceleration data. Moreover, previous studies have shown that, based on the results of the acceleration measures taken while performing a predefined and controlled set of activities, typically developing non-ADHD controls and non-medicated children with ADHD can be automatically classified with a relatively high accuracy. In the current paper, we extend these studies by using two minimally invasive tri-axial accelerometers to record movement data in a “free-living” environment while at school. By “free-living”, in the context of this study, we mean that no additional requirements was given to participants. They followed their normal, everyday activities. Moreover, there were no other requirements for two participants from two different schools (or from the same school but monitored on different days) to follow (a similar script of activities was not required). Although a first study presented in this paper only focuses on the data of two accelerometers (worn at school on both dominant limbs), a complete dataset including 4 tri-axial accelerometers during an entire day period, one on each wrist and ankle has been recorded., We have only used the data from the dominant hand and leg in order to simplify the data measuring and handling process in this first study. Moreover, in order to compare results in a similar environment, only acceleration data while at school was analyzed. The complete dataset of all 4 tri-axial accelerometers for the full day will be presented in subsequent papers. Instead of predefining a set of features to be computed from the sensor data, a Convolutional Neural Network (CNN) was used to automatically learn the optimal features to separate children in each group. The use of CNNs in human activity recognition (HAR) applied to wearable sensor acceleration data has recently shown promising results compared to other non-deep learning approaches based on hand-crafted features [
14,
15,
16,
17,
18]. Previous studies have generated CNN input images from windowed segments of acceleration data by using the time series information to generate the horizontal image axis and each tri-axial component of each accelerometer [
14,
18], or the combination of different sensors [
15,
16], or the combination of the accelerometer and gyroscope of a single IMU [
17] to generate the associated vertical image information. In this paper we propose a different and novel approach to generate acceleration images that both produces square images and is able to compensate for sensor misplacements and movement drift by finding the acceleration projections over a geo-referenced space. The tri-axial acceleration is converted into the movement related linear acceleration by subtracting an estimation of the gravity acceleration. Using an estimation for the gravity force from the sensed acceleration data to compensate different sensor orientations and obtaining sensor orientation invariant information has been used in previous research studies such as [
19,
20,
21] for human activity recognition. The estimated linear acceleration is then decomposed into its vertical (gravity acceleration aligned) and horizontal components. Using a window of 5 consecutive seconds of acceleration data, a squared acceleration image is generated with all the acceleration samples (using the vertical and horizontal acceleration values to select the pixel in the image to modify). Other approaches have been previously used in related literature to compute orientation invariant data from wearable tri-axial accelerometers such as [
22] which uses the inner products of two acceleration samples to compute sensor orientation free features. Our proposal uses a similar approach but uses an estimation of the gravity acceleration vector in order to project acceleration samples onto a geo-referenced coordinate system. Acceleration images are therefore computed in a geo-referenced horizontal-vertical space. A different approach could have been, as described in [
23], to use the autocorrelation matrix from the FFT transform to provide a rotation free measurement of three-dimensional measurements. The time dimension for the generation of the acceleration image would then be transformed into a frequency domain image but a geo-referenced time-based approach has been used in this paper in order to minimize the required computations. Computing acceleration images instead of using raw data series is also an important factor for the expected results. Previous research studies applying CNN to Human Activity Recognition (HAR) such as [
14,
15,
16,
17,
18] has shown that a CNN is able to learn common acceleration patterns based on raw acceleration data. The results may be improved by transforming raw data into computed features. By using a simple architecture, the authors in [
14] obtained even better results than previous papers based on more complex architectures but only using the raw acceleration data showing that the way in which the acceleration image is computed plays a very important role in the results that can be achieved. Finally, we have taken measures from non-medicated and medicated children with ADHD. While the CNN has been trained with children with ADHD who are unmedicated and typically developing non-ADHD controls, once trained, the CNN has been used to evaluate how close children with ADHD who are taking medication become to a typically developing non-ADHD control pattern.






{kind=link}
{kind=link}
{kind=link}
{kind=link}