
Automatic Artifact Removal in EEG of Normal and Demented Individuals Using ICA–WT during Working Memory Tasks


 ,
, 
Abstract
:1. Introduction
2. Methods and Materials
2.1. Methods
2.2. Subjects and EEG Recording
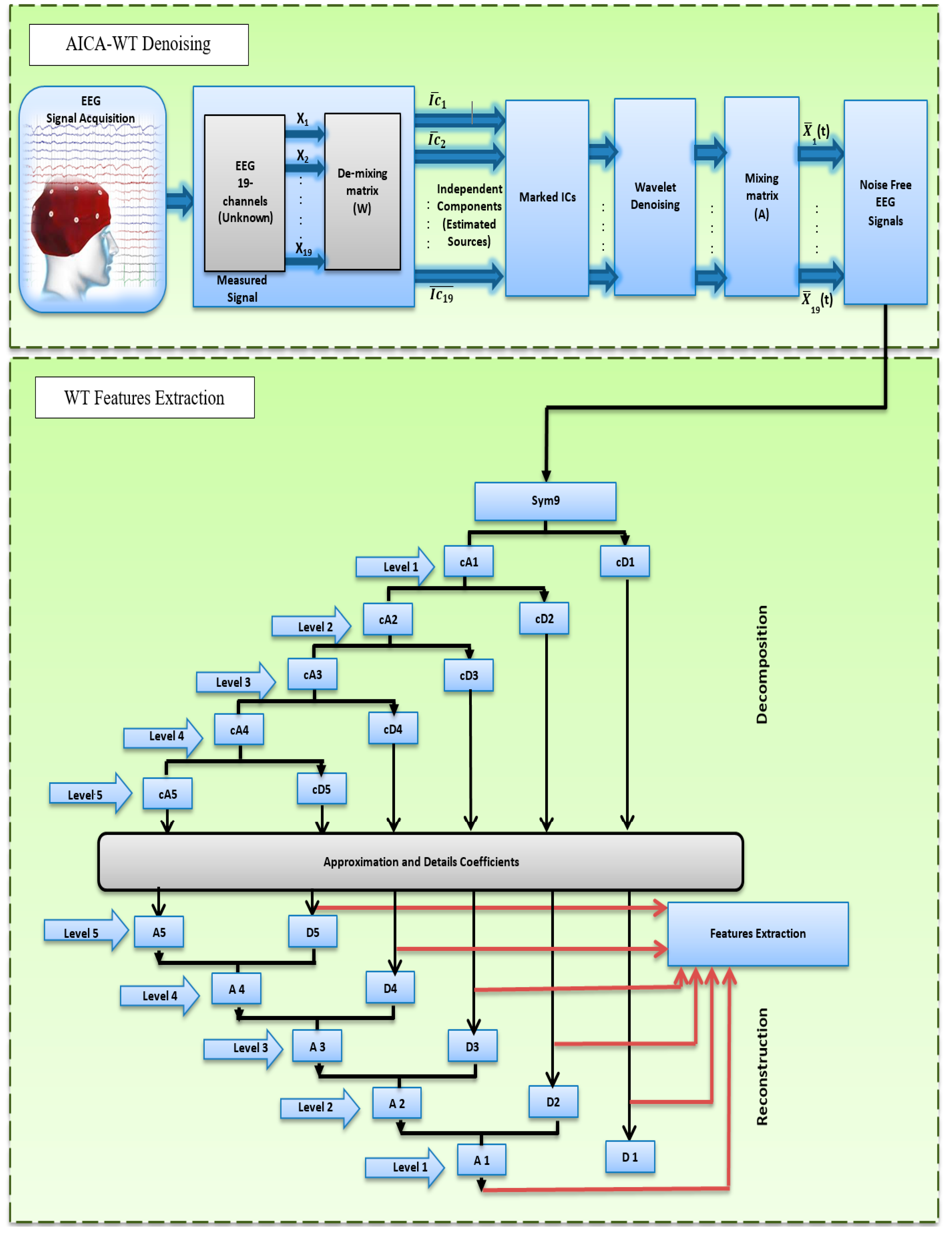
2.3. AICA–WT Technique Methodology
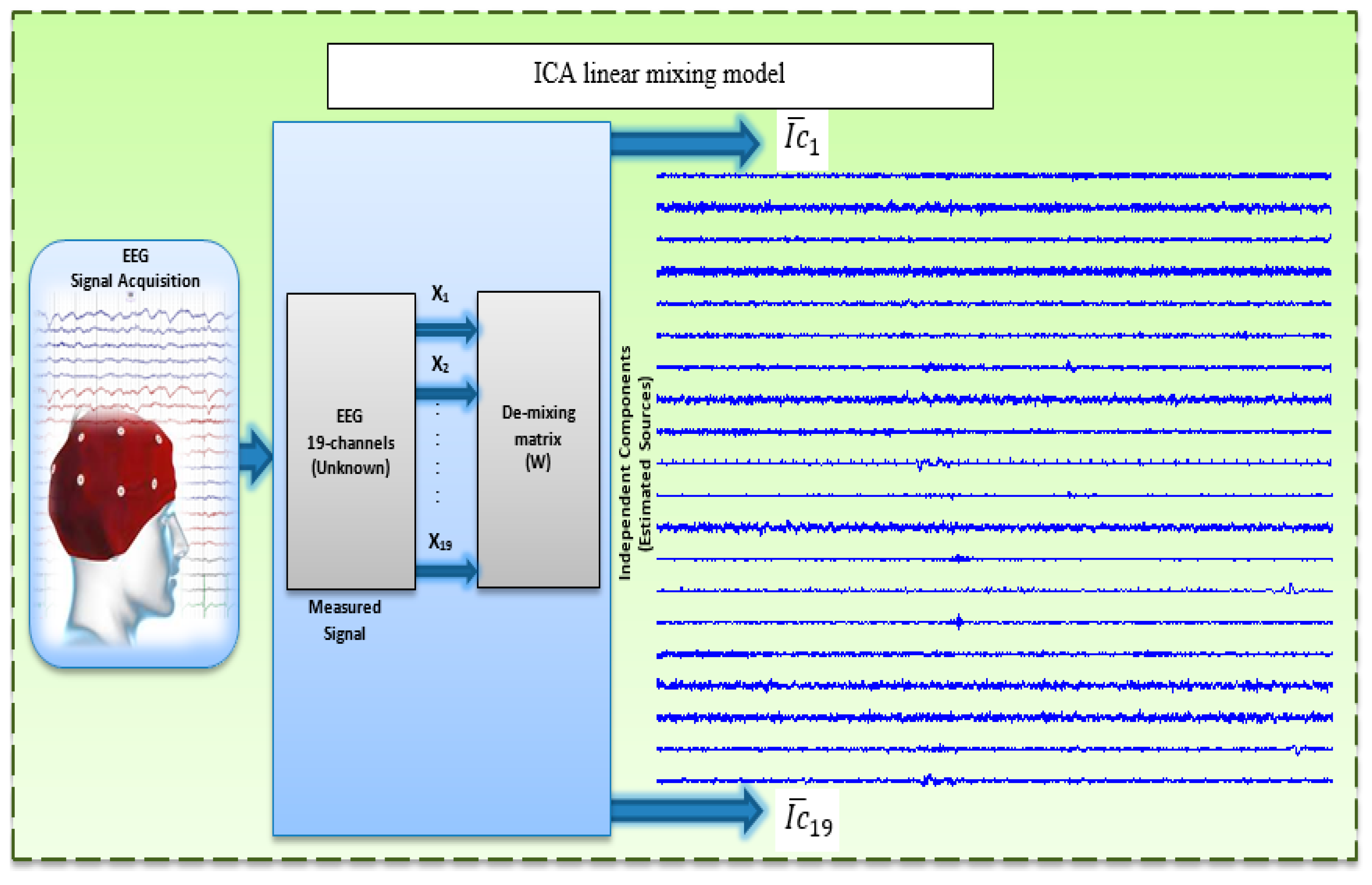
2.3.1. Linear Mixing Model and ICA Algorithm
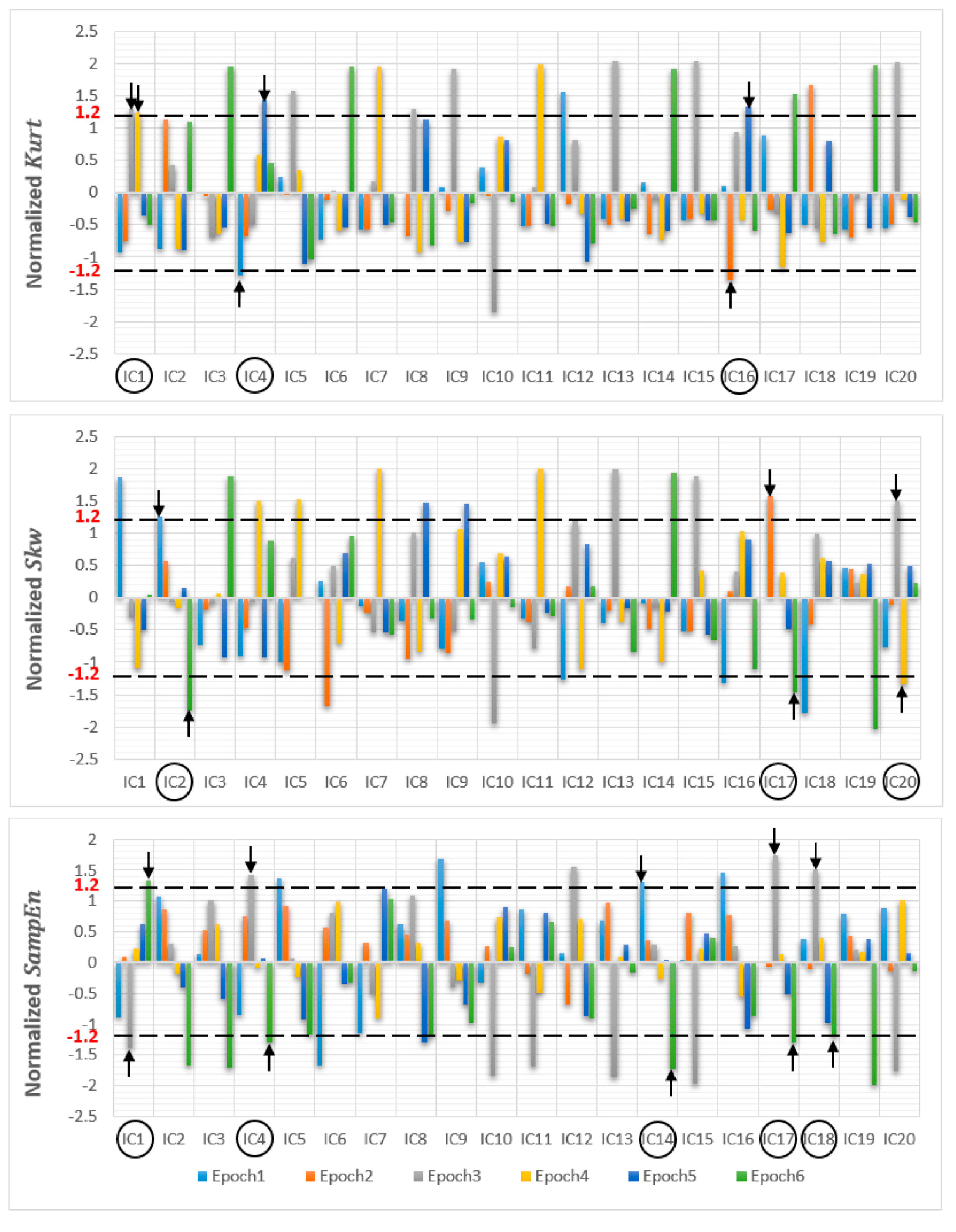
2.3.2. Artifact Detection Metrics
2.3.3. Reconstruction
2.4. WT Based Denoising and ICA Rejection
2.5. Wavelet Decomposition
2.6. Feature Extraction
3. Statistical Analysis
4. Results and Discussion
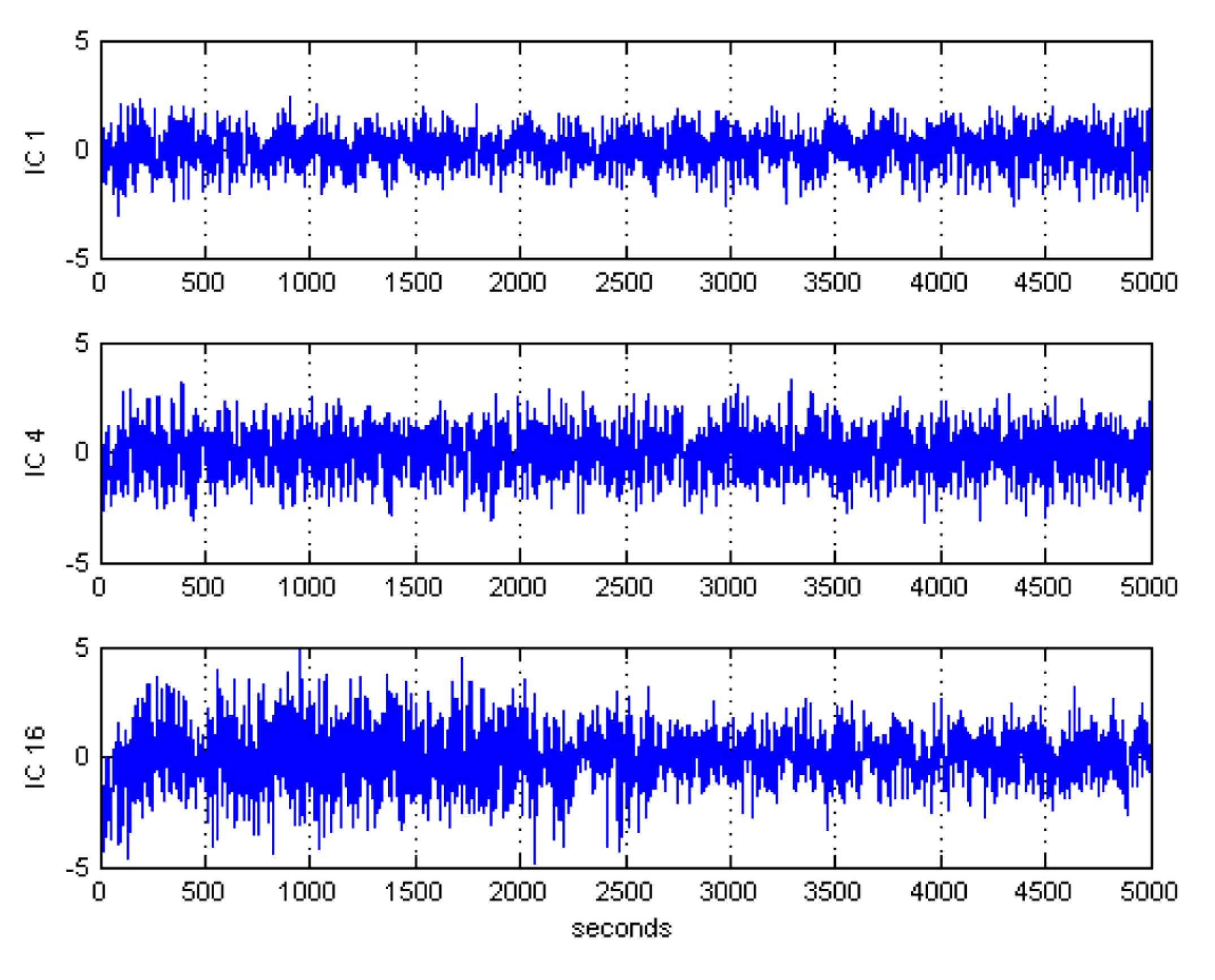
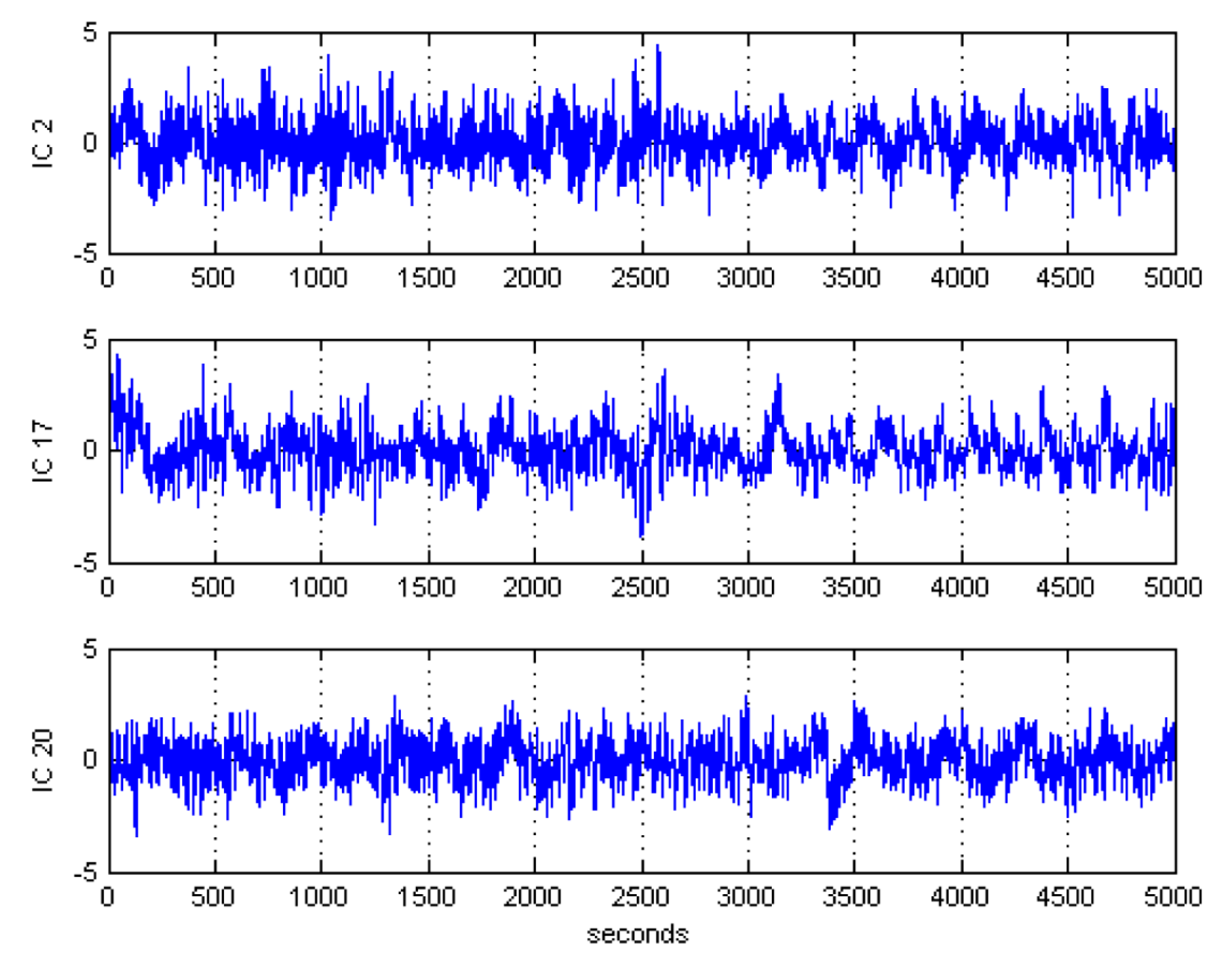
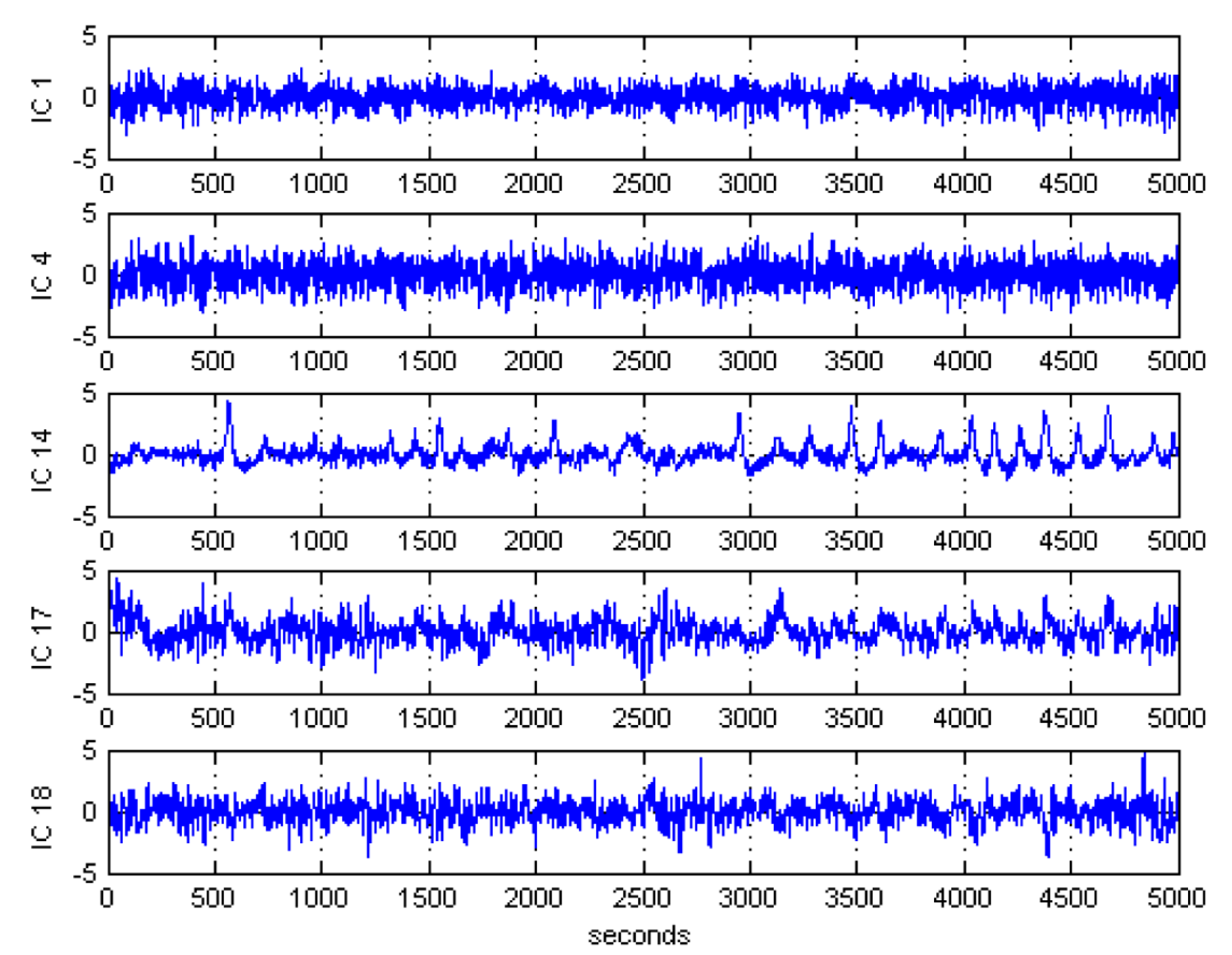
4.1. Automatic Artifactual Detection
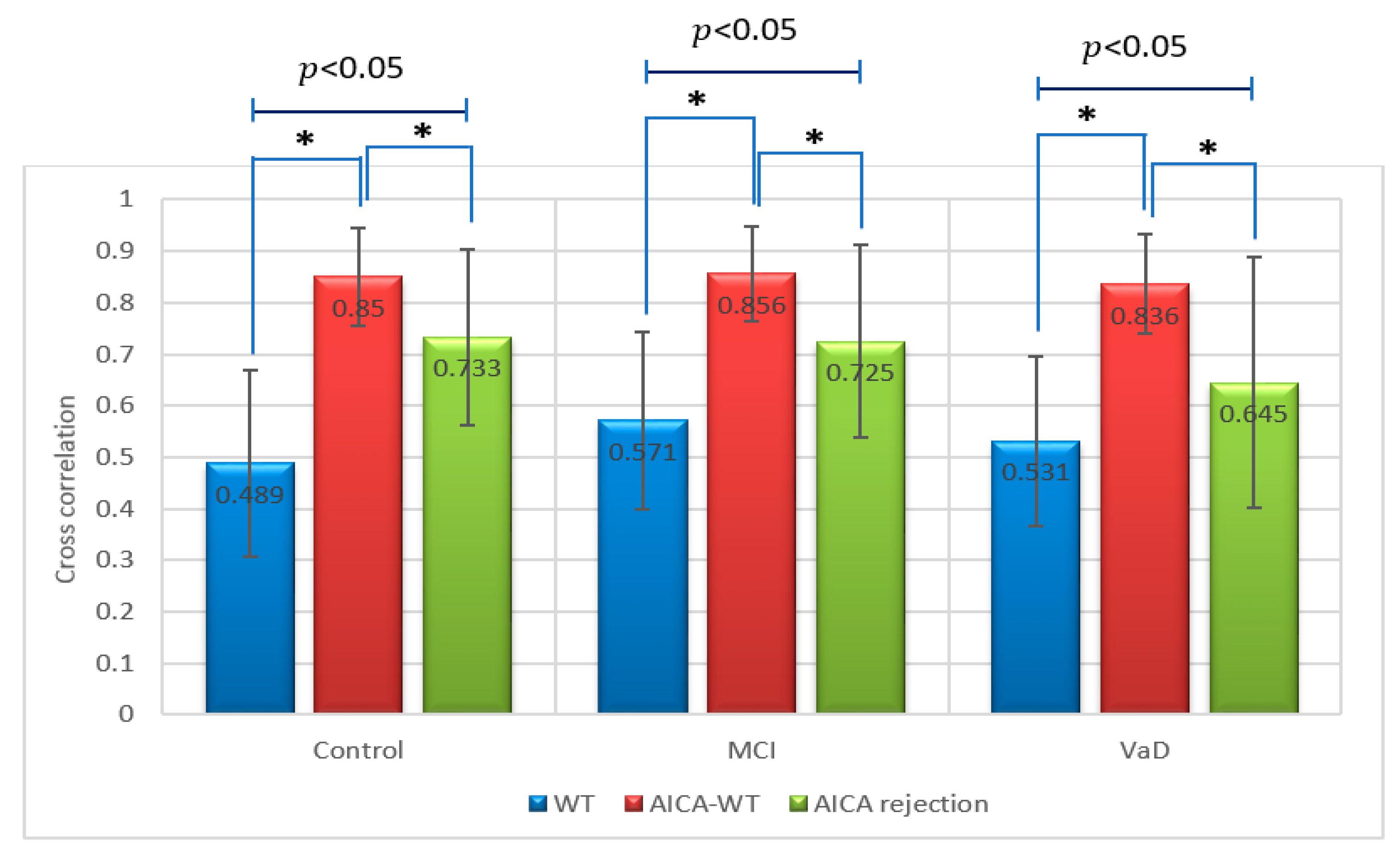
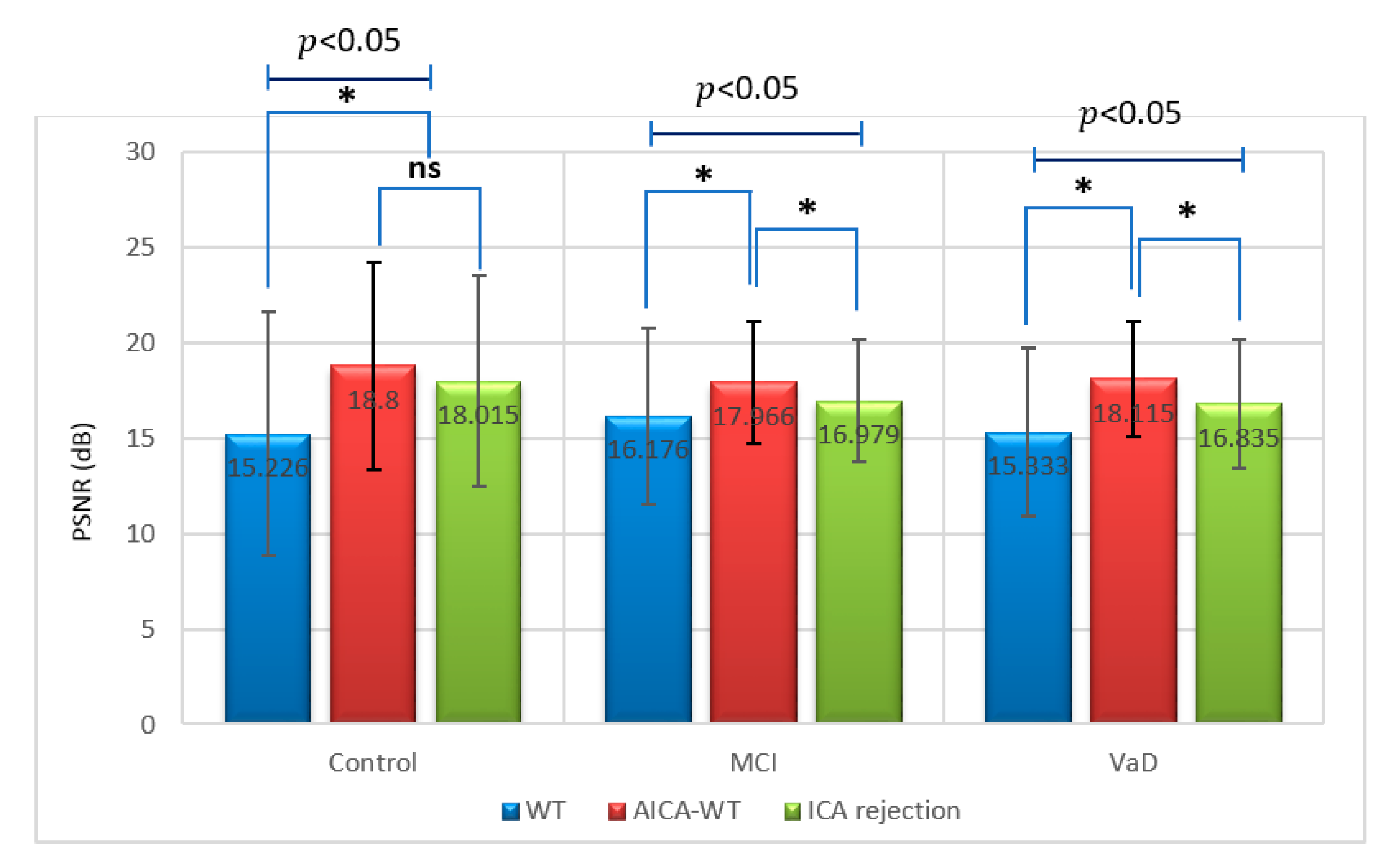
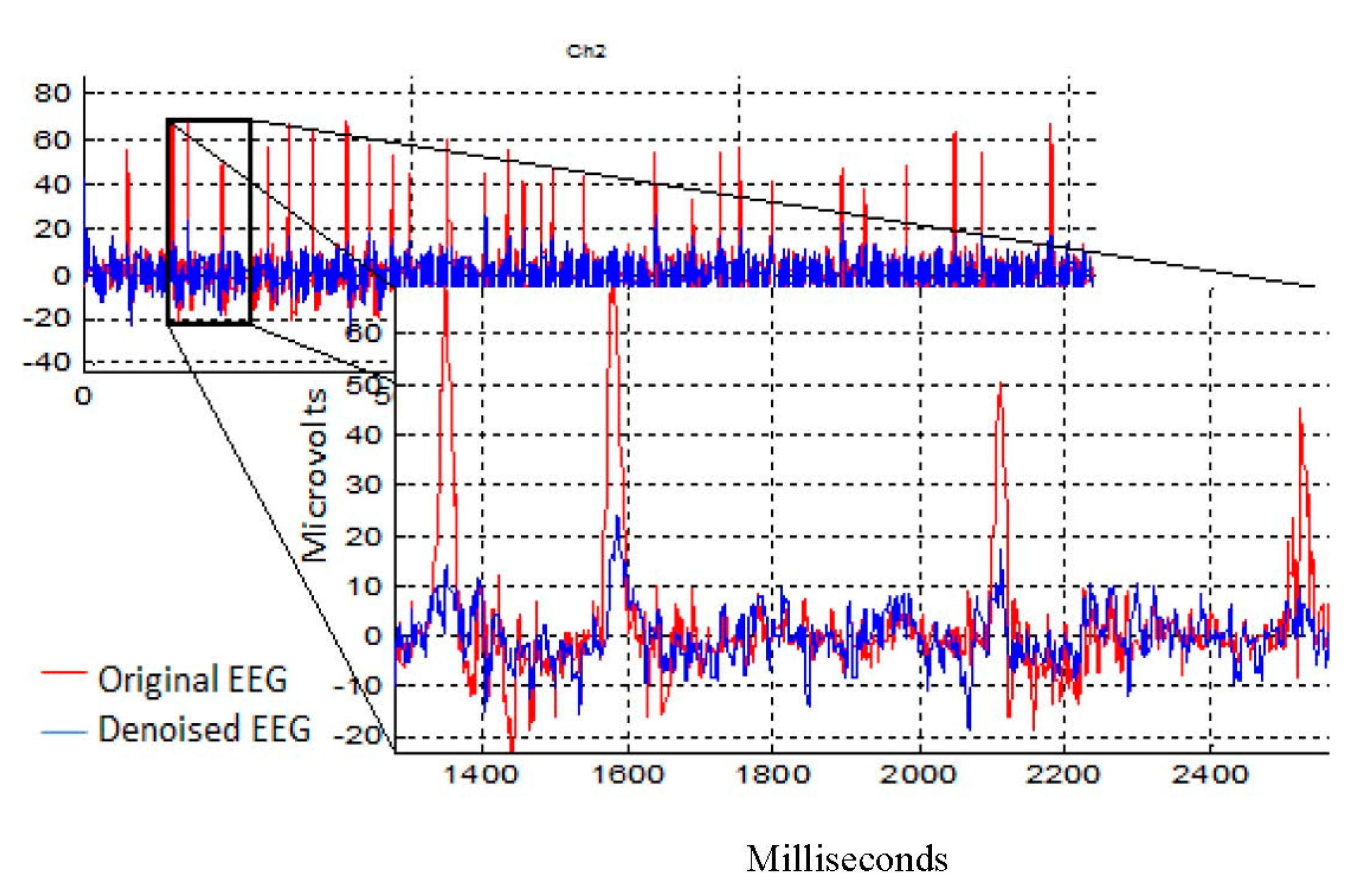
4.2. Denosing Technique Performance Evaluation
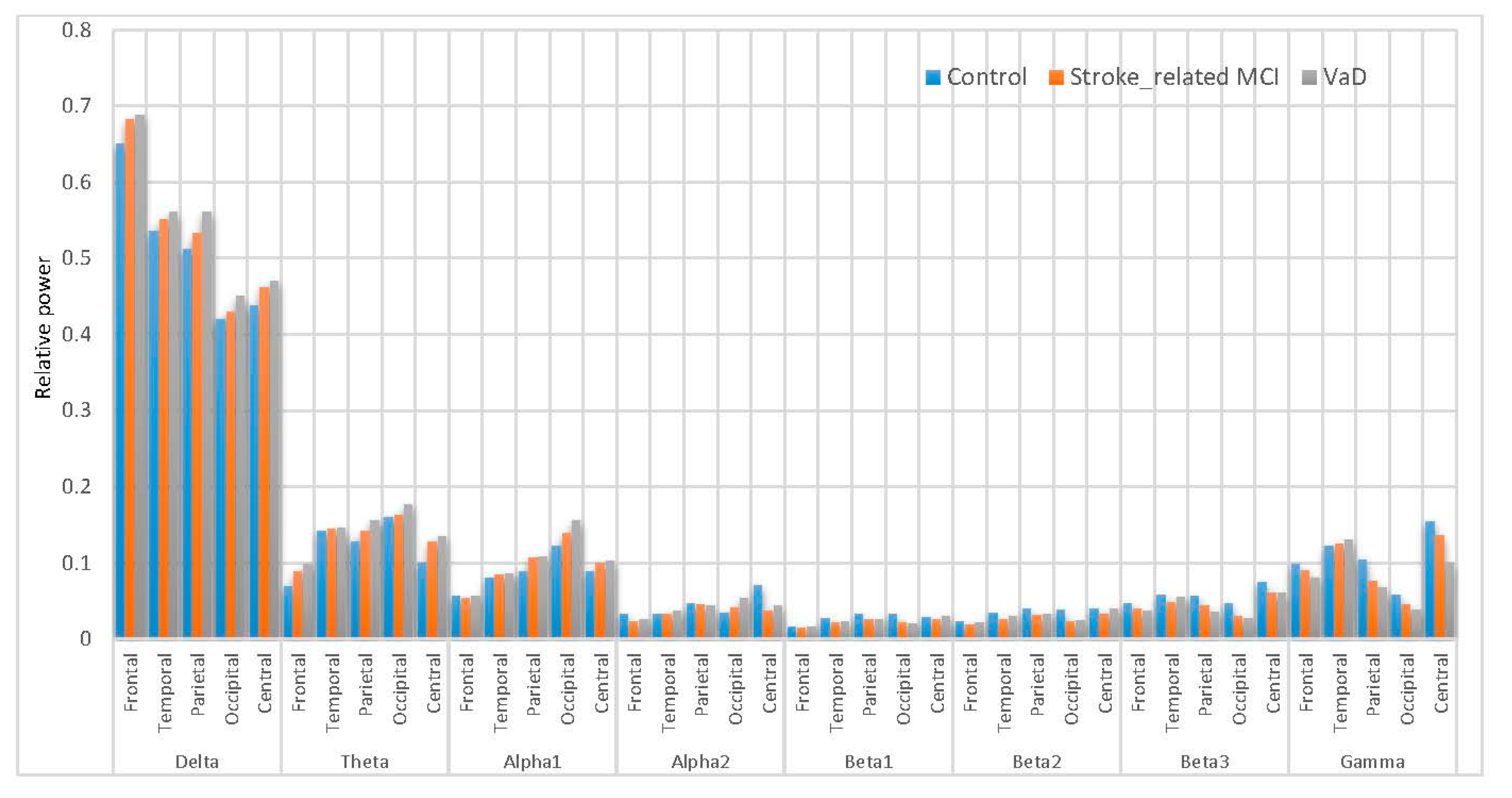
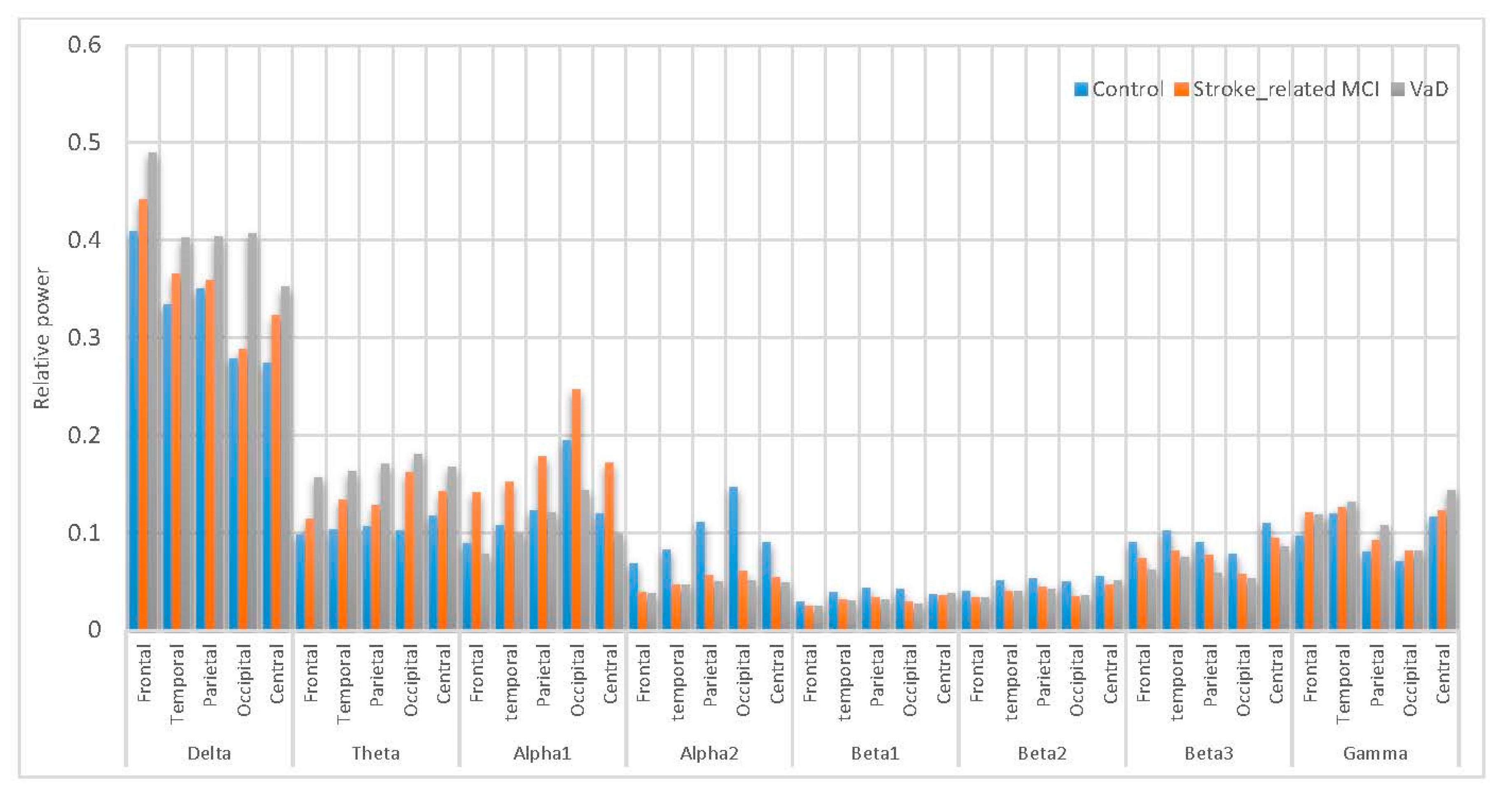
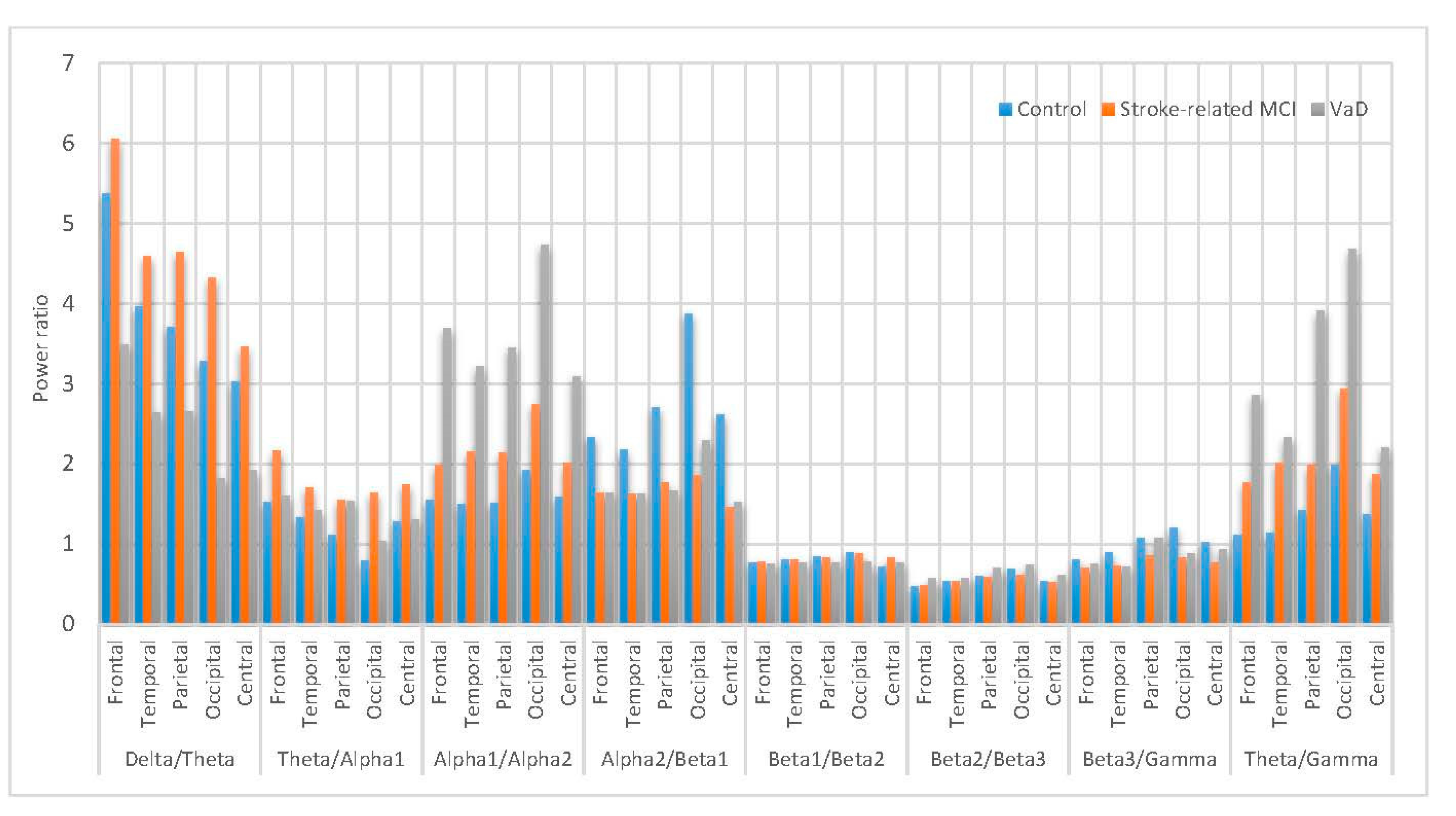
4.3. Differences in Spectral Power
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Al-Qazzaz, N.K.; Ali, S.H.B.; Ahmad, S.A.; Chellappan, K.; Islam, M.S.; Escudero, J. Role of EEG as Biomarker in the Early Detection and Classification of Dementia. Sci. World J. 2014, 2014, 906038. [Google Scholar] [CrossRef] [PubMed]
- Berger, H. Über das Elektrenkephalogramm des Menschen. Eur. Arch. Psychiatry Clin. Neurosci. 1929, 87, 527–570. [Google Scholar] [CrossRef]
- Pizzagalli, D.A. Electroencephalography and high-density electrophysiological source localization. Handb. Psychophysiol. 2007, 3, 56–84. [Google Scholar]
- Al-Kadi, M.I.; Reaz, M.B.I.; Ali, M.A.M.; Liu, C.Y. Reduction of the Dimensionality of the EEG Channels during Scoliosis Correction Surgeries Using a Wavelet Decomposition Technique. Sensors 2014, 14, 13046–13069. [Google Scholar] [CrossRef] [PubMed]
- Klimesch, W. EEG alpha and theta oscillations reflect cognitive and memory performance: A review and analysis. Brain Res. Rev. 1999, 29, 169–195. [Google Scholar] [CrossRef]
- Jacova, C.; Kertesz, A.; Blair, M.; Fisk, J.D.; Feldman, H.H. Neuropsychological testing and assessment for dementia. Alzheimer Dement. 2007, 3, 299–317. [Google Scholar] [CrossRef] [PubMed]
- Petersen, R.C. Mild cognitive impairment as a diagnostic entity. J. Intern. Med. 2004, 256, 183–194. [Google Scholar] [CrossRef] [PubMed]
- Borson, S.; Frank, L.; Bayley, P.J.; Boustani, M.; Dean, M.; Lin, P.-J.; McCarten, J.R.; Morris, J.C.; Salmon, D.P.; Schmitt, F.A. Improving dementia care: The role of screening and detection of cognitive impairment. Alzheimer Dement. 2013, 9, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Cumming, T.B.; Marshall, R.S.; Lazar, R.M. Stroke, cognitive deficits, and rehabilitation: Still an incomplete picture. Int. J. Stroke 2013, 8, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Ankolekar, S.; Geeganage, C.; Anderton, P.; Hogg, C.; Bath, P.M. Clinical trials for preventing post stroke cognitive impairment. J. Neurol. Sci. 2010, 299, 168–174. [Google Scholar] [CrossRef] [PubMed]
- Cullen, B.; O’Neill, B.; Evans, J.J.; Coen, R.F.; Lawlor, B.A. A review of screening tests for cognitive impairment. J. Neurol. Neurosurg. Psychiatry 2007, 78, 790–799. [Google Scholar] [CrossRef] [PubMed]
- Al-Qazzaz, N.K.; Ali, S.H.; Ahmad, S.A.; Islam, S.; Mohamad, K. Cognitive impairment and memory dysfunction after a stroke diagnosis: A post-stroke memory assessment. Neuropsychiatr. Dis. Treatm. 2014, 10, 1677. [Google Scholar] [CrossRef] [PubMed]
- Baddeley, A. Working memory. Science 1992, 255, 556–559. [Google Scholar] [CrossRef] [PubMed]
- Chellappan, K.; Mohsin, N.K.; Bin Md Ali, S.; Islam, M. Post-stroke brain memory assessment framewor. In Proceedings of the 2012 IEEE EMBS Conference on Biomedical Engineering and Sciences (IECBES 2012), Langkawi, Malaysia, 17–19 December 2012; pp. 189–194. [Google Scholar]
- D’Esposito, M. Chapter 11 Working memory. In Handbook of Clinical Neurology; Michael, J., Aminoff, F.B., Bruce, L.M., Eds.; Elsevier: Amsterdam, The Netherlands, 2008; Volume 88, pp. 237–247. [Google Scholar]
- Jeong, J. EEG dynamics in patients with Alzheimer’s disease. Clin. Neurophysiol. 2004, 115, 1490–1505. [Google Scholar] [CrossRef] [PubMed]
- John, E.; Prichep, L.; Fridman, J.; Easton, P. Neurometrics: Computer-Assisted differential diagnosis of brain dysfunctions. Science 1988, 239, 162–169. [Google Scholar] [CrossRef] [PubMed]
- Leuchter, A.F.; Cook, I.A.; Newton, T.F.; Dunkin, J.; Walter, D.O.; Rosenberg-Thompson, S.; Lachenbruch, P.A.; Weiner, H. Regional differences in brain electrical activity in dementia: Use of spectral power and spectral ratio measures. Electroencephalogr. Clin. Neurophysiol. 1993, 87, 385–393. [Google Scholar] [CrossRef]
- Lizio, R.; Vecchio, F.; Frisoni, G.B.; Ferri, R.; Rodriguez, G.; Babiloni, C. Electroencephalographic rhythms in Alzheimer’s disease. Int. J. Alzheimer Dis. 2011, 2011, 927573. [Google Scholar] [CrossRef] [PubMed]
- Gevins, A.; Smith, M.E.; McEvoy, L.; Yu, D. High-resolution EEG mapping of cortical activation related to working memory: Effects of task difficulty, type of processing, and practice. Cereb. Cortex 1997, 7, 374–385. [Google Scholar] [CrossRef] [PubMed]
- Lundqvist, M.; Herman, P.; Lansner, A. Theta and gamma power increases and alpha/beta power decreases with memory load in an attractor network model. J. Cogn. Neurosci. 2011, 23, 3008–3020. [Google Scholar] [CrossRef] [PubMed]
- Onton, J.; Delorme, A.; Makeig, S. Frontal midline EEG dynamics during working memory. Neuroimage 2005, 27, 341–356. [Google Scholar] [CrossRef] [PubMed]
- Guerrero-Mosquera, C.; Trigueros, A.M.; Navia-Vazquez, A.A. EEG Signal Processing for Epilepsy. In Epilepsy–Histological, Electroencephalographic and Psychological Aspects; InTech: Rijeka, Croatia, 2012. [Google Scholar]
- Núñez, I.M.B. EEG Artifact Dtection; Czech Technical University: Prague, Czech Republic, 2010. [Google Scholar]
- Jung, T.-P.; Makeig, S.; Westerfield, M.; Townsend, J.; Courchesne, E.; Sejnowski, T.J. Removal of eye activity artifacts from visual event-related potentials in normal and clinical subjects. Clin. Neurophysiol. 2000, 111, 1745–1758. [Google Scholar] [CrossRef]
- Kirkove, M.; François, C.; Verly, J. Comparative evaluation of existing and new methods for correcting ocular artifacts in electroencephalographic recordings. Signal Process. 2014, 98, 102–120. [Google Scholar] [CrossRef]
- Pham, T.; Croft, R.; Cadusch, P.; Barry, R. A test of four EOG correction methods using an improved validation technique (Published Conference Proceedings style). Int. J. Psychophysiol. 2011, 79, 203–210. [Google Scholar] [CrossRef] [PubMed]
- James, C.J.; Hesse, C.W. Independent component analysis for biomedical signals. Physiol. Meas. 2005, 26, R15–R39. [Google Scholar] [CrossRef] [PubMed]
- Vigário, R.; Oja, E. BSS and ICA in neuroinformatics: From current practices to open challenges. IEEE Rev. Biomed. Eng. 2008, 1, 50–61. [Google Scholar] [CrossRef] [PubMed]
- Papadelis, C.; Chen, Z.; Kourtidou-Papadeli, C.; Bamidis, P.D.; Chouvarda, I.; Bekiaris, E.; Maglaveras, N. Monitoring sleepiness with on-board electrophysiological recordings for preventing sleep-deprived traffic accidents. Clin. Neurophysiol. 2007, 118, 1906–1922. [Google Scholar] [CrossRef] [PubMed]
- Papadelis, C.; Maglaveras, N.; Kourtidou-Papadeli, C.; Bamidis, P.; Albani, M.; Chatzinikolaou, K.; Pappas, K. Quantitative multichannel EEG measure predicting the optimal weaning from ventilator in ICU patients with acute respiratory failure. Clin. Neurophysiol. 2006, 117, 752–770. [Google Scholar] [CrossRef] [PubMed]
- Dammers, J.; Schiek, M.; Boers, F.; Silex, C.; Zvyagintsev, M.; Pietrzyk, U.; Mathiak, K. Integration of amplitude and phase statistics for complete artifact removal in independent components of neuromagnetic recordings. IEEE Trans. Biomed. Eng. 2008, 55, 2353–2362. [Google Scholar] [CrossRef] [PubMed]
- Nicolas-Alonso, L.F.; Gomez-Gil, J. Brain computer interfaces, a review. Sensors 2012, 12, 1211–1279. [Google Scholar] [CrossRef] [PubMed]
- Kelly, J.W.; Siewiorek, D.P.; Smailagic, A.; Collinger, J.L.; Weber, D.J.; Wang, W. Fully automated reduction of ocular artifacts in high-dimensional neural data. IEEE Trans. Biomed. Eng. 2011, 58, 598–606. [Google Scholar] [CrossRef] [PubMed]
- Bell, A.J.; Sejnowski, T.J. An information-maximization approach to blind separation and blind deconvolution. Neural Comput. 1995, 7, 1129–1159. [Google Scholar] [CrossRef] [PubMed]
- Jung, T.-P.; Makeig, S.; Humphries, C.; Lee, T.-W.; Mckeown, M.J.; Iragui, V.; Sejnowski, T.J. Removing electroencephalographic artifacts by blind source separation. Psychophysiology 2000, 37, 163–178. [Google Scholar] [CrossRef] [PubMed]
- Hyvärinen, A.; Oja, E. Independent component analysis: Algorithms and applications. Neural Netw. 2000, 13, 411–430. [Google Scholar] [CrossRef]
- Akhtar, M.T.; Mitsuhashi, W.; James, C.J. Employing spatially constrained ICA and wavelet denoising, for automatic removal of artifacts from multichannel EEG data. Signal Process. 2012, 92, 401–416. [Google Scholar] [CrossRef]
- Mammone, N.; La Foresta, F.; Morabito, F.C. Automatic artifact rejection from multichannel scalp EEG by wavelet ICA. IEEE Sens. J. 2012, 12, 533–542. [Google Scholar] [CrossRef]
- Vázquez, R.R.; Velez-Perez, H.; Ranta, R.; Dorr, V.L.; Maquin, D.; Maillard, L. Blind source separation, wavelet denoising and discriminant analysis for EEG artefacts and noise cancelling. Biomed. Signal Process. Control 2012, 7, 389–400. [Google Scholar] [CrossRef]
- Radüntz, T.; Scouten, J.; Hochmuth, O.; Meffert, B. EEG artifact elimination by extraction of ICA-component features using image processing algorithms. J. Neurosci. Methods 2015, 243, 84–93. [Google Scholar] [CrossRef] [PubMed]
- Sameni, R.; Gouy-Pailler, C. An iterative subspace denoising algorithm for removing electroencephalogram ocular artifacts. J. Neurosci. Methods 2014, 225, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Zhou, W.; Gotman, J. Removing Eye-movement Artifacts from the EEG during the Intracarotid Amobarbital Procedure. Epilepsia 2005, 46, 409–414. [Google Scholar] [CrossRef] [PubMed]
- Zhou, W.; Gotman, J. Automatic removal of eye movement artifacts from the EEG using ICA and the dipole model. Prog. Nat. Sci. 2009, 19, 1165–1170. [Google Scholar] [CrossRef]
- Romero, S.; Mañanas, M.A.; Barbanoj, M.J. A comparative study of automatic techniques for ocular artifact reduction in spontaneous EEG signals based on clinical target variables: A simulation case. Comput. Biol. Med. 2008, 38, 348–360. [Google Scholar] [CrossRef] [PubMed]
- Romero, S.; Mañanas, M.; Barbanoj, M.J. Ocular reduction in EEG signals based on adaptive filtering, regression and blind source separation. Ann. Biomed. Eng. 2009, 37, 176–191. [Google Scholar] [CrossRef] [PubMed]
- Percival, D.B.; Walden, A.T. Wavelet Methods for Time Series Analysis; Cambridge University Press: Cambridge, NY, USA, 2006; Volume 4. [Google Scholar]
- Torrence, C.; Compo, G.P. A practical guide to wavelet analysis. Bull. Am. Meteorol. Soc. 1998, 79, 61–78. [Google Scholar] [CrossRef]
- Mowla, M.R.; Ng, S.-C.; Zilany, M.S.; Paramesran, R. Artifacts-matched blind source separation and wavelet transform for multichannel EEG denoising. Biomed. Signal Process. Control 2015, 22, 111–118. [Google Scholar] [CrossRef]
- Asaduzzaman, K.; Reaz, M.; Mohd-Yasin, F.; Sim, K.; Hussain, M. A study on discrete wavelet-based noise removal from EEG signals. In Advances in Computational Biology; Springer: New York, NY, USA, 2010; pp. 593–599. [Google Scholar]
- Adeli, H.; Zhou, Z.; Dadmehr, N. Analysis of EEG records in an epileptic patient using wavelet transform. J. Neurosci. Methods 2003, 123, 69–87. [Google Scholar] [CrossRef]
- Übeyli, E.D. Combined neural network model employing wavelet coefficients for EEG signals classification. Digit. Signal Process. 2009, 19, 297–308. [Google Scholar] [CrossRef]
- Castellanos, N.P.; Makarov, V.A. Recovering EEG brain signals: Artifact suppression with wavelet enhanced independent component analysis. J. Neurosci. Methods 2006, 158, 300–312. [Google Scholar] [CrossRef] [PubMed]
- Ghandeharion, H.; Erfanian, A. A fully automatic ocular artifact suppression from EEG data using higher order statistics: Improved performance by wavelet analysis. Med. Eng. Phys. 2010, 32, 720–729. [Google Scholar] [CrossRef] [PubMed]
- Klados, M.A.; Papadelis, C.; Braun, C.; Bamidis, P.D. REG-ICA: A hybrid methodology combining Blind Source Separation and regression techniques for the rejection of ocular artifacts. Biomed. Signal Process. Control 2011, 6, 291–300. [Google Scholar] [CrossRef]
- Brott, T.; Adams, H.; Olinger, C.P.; Marler, J.R.; Barsan, W.G.; Biller, J.; Spilker, J.; Holleran, R.; Eberle, R.; Hertzberg, V. Measurements of acute cerebral infarction: A clinical examination scale. Stroke 1989, 20, 864–870. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Smith, T.; Gildeh, N.; Holmes, C. The Montreal Cognitive Assessment: Validity and utility in a memory clinic setting. Can. J. Psychiatry 2007, 52, 329. [Google Scholar] [CrossRef] [PubMed]
- Al-Qazzaz, N.; Hamid Bin Mohd Ali, S.; Ahmad, S.; Islam, M.; Escudero, J. Selection of Mother Wavelet Functions for Multi-Channel EEG Signal Analysis during a Working Memory Task. Sensors 2015, 15, 29015–29035. [Google Scholar] [CrossRef] [PubMed]
- Bagnoli, S.; Failli, Y.; Piaceri, I.; Rinnoci, V.; Bessi, V.; Tedde, A.; Nacmias, B.; Sorbi, S. Suitability of neuropsychological tests in patients with vascular dementia (VaD). J. Neurol. Sci. 2012, 322, 41–45. [Google Scholar] [CrossRef] [PubMed]
- Sikaroodi, H.; Yadegari, S.; Miri, S.R. Cognitive impairments in patients with cerebrovascular risk factors: A comparison of Mini Mental Status Exam and Montreal Cognitive Assessment. Clin. Neurol. Neurosurg. 2013, 125, 1276–1280. [Google Scholar] [CrossRef] [PubMed]
- Kandiah, N.; Wiryasaputra, L.; Narasimhalu, K.; Karandikar, A.; Marmin, M.; Chua, E.V.; Sitoh, Y.Y. Frontal subcortical ischemia is crucial for post stroke cognitive impairment. J. Neurol. Sci. 2011, 309, 92–95. [Google Scholar] [CrossRef] [PubMed]
- Escudero, J.; Hornero, R.; Abásolo, D.; Fernández, A. Blind source separation to enhance spectral and non-linear features of magnetoencephalogram recordings. Application to Alzheimer’s disease. Med. Eng. Phys. 2009, 31, 872–879. [Google Scholar] [CrossRef] [PubMed]
- Barbati, G.; Porcaro, C.; Zappasodi, F.; Rossini, P.M.; Tecchio, F. Optimization of an independent component analysis approach for artifact identification and removal in magnetoencephalographic signals. Clin. Neurophysiol. 2004, 115, 1220–1232. [Google Scholar] [CrossRef] [PubMed]
- Vigário, R.; Oja, E. Independence: A new criterion for the analysis of the electromagnetic fields in the global brain? Neural Netw. 2000, 13, 891–907. [Google Scholar] [CrossRef]
- Escudero, J.; Hornero, R.; Abásolo, D.; Fernández, A.; López-Coronado, M. Artifact removal in magnetoencephalogram background activity with independent component analysis. IEEE Trans. Biomed. Eng. 2007, 54, 1965–1973. [Google Scholar] [CrossRef] [PubMed]
- Cichocki, A.; Shishkin, S.L.; Musha, T.; Leonowicz, Z.; Asada, T.; Kurachi, T. EEG filtering based on blind source separation (BSS) for early detection of Alzheimer’s disease. Clin. Neurophysiol. 2005, 116, 729–737. [Google Scholar] [CrossRef] [PubMed]
- Escudero, J.; Hornero, R.; Poza, J.; Abásolo, D.; Fernández, A. Assessment of classification improvement in patients with Alzheimer’s disease based on magnetoencephalogram blind source separation. Artif. Intell. Med. 2008, 43, 75–85. [Google Scholar] [CrossRef] [PubMed]
- Jin, S.-H.; Jeong, J.; Jeong, D.-G.; Kim, D.-J.; Kim, S.Y. Nonlinear dynamics of the EEG separated by independent component analysis after sound and light stimulation. Biol. Cybern. 2002, 86, 395–401. [Google Scholar] [CrossRef] [PubMed]
- Hyvarinen, A. Fast and robust fixed-point algorithms for independent component analysis. IEEE Trans. Neural Netw. 1999, 10, 626–634. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, J.-F.; Souloumiac, A. Blind Beamforming for non-Gaussian Signals. Proceedings of Radar and Signal Processing, London, UK, 6 December 1993; pp. 362–370. [Google Scholar]
- Oja, E.; Yuan, Z. The FastICA algorithm revisited: Convergence analysis. IEEE Trans. Neural Netw. 2006, 17, 1370–1381. [Google Scholar] [CrossRef] [PubMed]
- Zeng, H.; Song, A.; Yan, R.; Qin, H. EOG artifact correction from EEG recording using stationary subspace analysis and empirical mode decomposition. Sensors 2013, 13, 14839–14859. [Google Scholar] [CrossRef] [PubMed]
- Muthukumaraswamy, S.D. High-frequency brain activity and muscle artifacts in MEG/EEG: A review and recommendations. Front. Hum. Neurosci. 2013, 7, 138. [Google Scholar] [CrossRef] [PubMed]
- Inuso, G.; La Foresta, F.; Mammone, N.; Morabito, F.C. Wavelet-ICA methodology for efficient artifact removal from Electroencephalographic recordings. In Proceedings of the International Joint Conference on Neural Networks (IJCNN 2007), Orlando, FL, USA, 12–17 August 2007; pp. 1524–1529. [Google Scholar]
- Escudero, J.; Hornero, R.; Abásolo, D.; Fernández, A. Quantitative evaluation of artifact removal in real magnetoencephalogram signals with blind source separation. Ann. Biomed. Eng. 2011, 39, 2274–2286. [Google Scholar] [CrossRef] [PubMed]
- Zeng, H.; Song, A. Removal of EOG artifacts from EEG recordings using stationary subspace analysis. Sci. World J. 2014, 2014, 259121. [Google Scholar] [CrossRef] [PubMed]
- Mammone, N.; Morabito, F.C. Enhanced automatic artifact detection based on independent component analysis and Renyi’s entropy. Neural Netw. 2008, 21, 1029–1040. [Google Scholar] [CrossRef] [PubMed]
- Greco, A.; Mammone, N.; Morabito, F.C.; Versaci, M. Kurtosis, Renyi’s entropy and independent component scalp maps for the automatic artifact rejection from EEG data. Int. J. Signal Process. 2006, 2, 240–244. [Google Scholar]
- Mahajan, R.; Morshed, B. Unsupervised Eye Blink Artifact Denoising of EEG Data with Modified Multiscale Sample Entropy, Kurtosis, and Wavelet-ICA. IEEE J. Biomed. Health Inform. 2015, 19, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Mahajan, R.; Morshed, B. Sample Entropy enhanced wavelet-ICA denoising technique for eye blink artifact removal from scalp EEG dataset. In Proceedings of the 2013 6th International IEEE/EMBS Conference on Neural Engineering (NER 2013), San Diego, CA, USA, 6–8 November 2013; pp. 1394–1397. [Google Scholar]
- Richman, J.S.; Moorman, J.R. Physiological time-series analysis using approximate entropy and sample entropy. Am. J. Physiol. Heart Circul. Physiol. 2000, 278, H2039–H2049. [Google Scholar]
- Lake, D.E.; Richman, J.S.; Griffin, M.P.; Moorman, J.R. Sample entropy analysis of neonatal heart rate variability. Am. J. Physiol.-Regul. Integr. Comp. Physiol. 2002, 283, R789–R797. [Google Scholar] [CrossRef] [PubMed]
- Messer, S.R.; Agzarian, J.; Abbott, D. Optimal wavelet denoising for phonocardiograms. Microelectron. J. 2001, 32, 931–941. [Google Scholar] [CrossRef]
- German-Sallo, Z.; Ciufudean, C. Waveform-adapted wavelet denoising of ECG signals. Adv. Math. Computat. Methods 2012, 172175. [Google Scholar]
- Shoeb, A.; Cliord, G. Chapter 16—Wavelets; Multiscale Activity in Physiological Signals. In Biomedical Signal and Image Processing; Springer: New York, NY, USA, 2005. [Google Scholar]
- Rosso, O.A.; Blanco, S.; Yordanova, J.; Kolev, V.; Figliola, A.; Schürmann, M.; Başar, E. Wavelet entropy: A new tool for analysis of short duration brain electrical signals. J. Neurosci. Methods 2001, 105, 65–75. [Google Scholar] [CrossRef]
- Rosso, O.; Martin, M.; Plastino, A. Brain electrical activity analysis using wavelet-based informational tools. Phys. A Stat. Mech. Appl. 2002, 313, 587–608. [Google Scholar] [CrossRef]
- Mallat, S.G. A theory for multiresolution signal decomposition: The wavelet representation. IEEE Trans. Pattern Anal. Mach. Intell. 1989, 11, 674–693. [Google Scholar] [CrossRef]
- German-Sallo, Z. Nonlinear filtering in ECG signal denoising. Acta Univ. Sapientiae Electr. Mech. Eng. 2010, 2, 136–145. [Google Scholar]
- Mallat, S. A Wavelet Tour of Signal Processing; Academic Press: Waltham, MA, USA, 1999. [Google Scholar]
- Stein, C.M. Estimation of the mean of a multivariate normal distribution. Ann. Stat. 1981, 1135–1151. [Google Scholar] [CrossRef]
- Romo-Vazquez, R.; Ranta, R.; Louis-Dorr, V.; Maquin, D. EEG ocular artefacts and noise removal. In Proceedings of the 29th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBS 2007), Lyon, France, 22–26 August 2007; pp. 5445–5448. [Google Scholar]
- Estrada, E.; Nazeran, H.; Sierra, G.; Ebrahimi, F.; Setarehdan, S.K. Wavelet-based EEG denoising for automatic sleep stage classification. In Proceedings of the 2011 21st International Conference on Electrical Communications and Computers (CONIELECOMP), San Andres Cholula, Mexico, 28 February–2 March 2011; pp. 295–298. [Google Scholar]
- Al-Qazzaz, N.K.; Ali, S.; Ahmad, S.A.; Islam, M.S.; Ariff, M.I. Selection of mother wavelets thresholding methods in denoising multi-channel EEG signals during working memory task. In Proceedings of the 2014 IEEE Conference on Biomedical Engineering and Sciences (IECBES), Kuala Lumpur, Malaysia, 8–10 December 2014; pp. 214–219. [Google Scholar]
- Rafiee, J.; Rafiee, M.; Prause, N.; Schoen, M. Wavelet basis functions in biomedical signal processing. Expert Syst. Appl. 2011, 38, 6190–6201. [Google Scholar] [CrossRef]
- Menshawy, M.E.; Benharref, A.; Serhani, M. An Automatic Mobile-Health based Approach for EEG Epileptic Seizures Detection. Expert Syst. Appl. 2015, 42, 7157–7174. [Google Scholar] [CrossRef]
- Teplan, M.; Krakovská, A.; Špajdel, M. Spectral EEG features of a Short Psycho-physiological Relaxation. Meas. Sci. Rev. 2014, 14, 237–242. [Google Scholar] [CrossRef]
- Welch, P. The use of fast Fourier transform for the estimation of power spectra: A method based on time averaging over short, modified periodograms. IEEE Trans. Audio Electroacoust. 1967, 15, 70–73. [Google Scholar] [CrossRef]
- Ko, K.-E.; Yang, H.-C.; Sim, K.-B. Emotion recognition using EEG signals with relative power values and Bayesian network. Int. J. Control Autom. Syst. 2009, 7, 865–870. [Google Scholar] [CrossRef]
- Moretti, D.; Fracassi, C.; Pievani, M.; Geroldi, C.; Binetti, G.; Zanetti, O.; Sosta, K.; Rossini, P.; Frisoni, G. Increase of theta/gamma ratio is associated with memory impairment. Clin. Neurophysiol. 2009, 120, 295–303. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic | Normal | Stroke-Related MCI | VaD |
|---|---|---|---|
| Number of subjects (Female/Male) | 15 (8/7) | 15 (10/5) | 5 (2/3) |
| Age | 60.06 ± 5.21 | 60.26 ± 7.77 | 64.6 ± 4.8 |
| MMSE | 29.6 ± 0.73 | 20.2 ± 5.63 | 14.8 ± 1.92 |
| MoCA | 29.06 ± 0.88 | 16.13 ± 5.97 | 13.2 ± 2.38 |
| Decomposition Levels | EEG Bands | Frequency Range (Hz) | Decomposed Signals |
|---|---|---|---|
| 1 | Noises | 64–128 | D1 |
| 2 | Gamma () | 32–64 | D2 |
| 3 | Beta () | 16–32 | D3 |
| 4 | Alpha () | 8–16 | D4 |
| 5 | Theta () | 4–8 | D5 |
| 5 | Delta () | 0–4 | A5 |
| Subjects | Kurtosis | Skewness | Sample Entropy |
|---|---|---|---|
| Control | 2.667 ± 1.759 | 5.133 ± 2.532 | 4.667 ± 1.633 |
| MCI | 2.867 ± 1.846 | 4.6 ± 2.098 | >3.867 ± 2.2 |
| VaD | 3.2 ± 1.6 | 5.4 ± 2.417 | 6 ± 1.673 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Qazzaz, N.K.; Hamid Bin Mohd Ali, S.; Ahmad, S.A.; Islam, M.S.; Escudero, J. Automatic Artifact Removal in EEG of Normal and Demented Individuals Using ICA–WT during Working Memory Tasks. Sensors 2017, 17, 1326. https://doi.org/10.3390/s17061326
Al-Qazzaz NK, Hamid Bin Mohd Ali S, Ahmad SA, Islam MS, Escudero J. Automatic Artifact Removal in EEG of Normal and Demented Individuals Using ICA–WT during Working Memory Tasks. Sensors. 2017; 17(6):1326. https://doi.org/10.3390/s17061326
Chicago/Turabian StyleAl-Qazzaz, Noor Kamal, Sawal Hamid Bin Mohd Ali, Siti Anom Ahmad, Mohd Shabiul Islam, and Javier Escudero. 2017. "Automatic Artifact Removal in EEG of Normal and Demented Individuals Using ICA–WT during Working Memory Tasks" Sensors 17, no. 6: 1326. https://doi.org/10.3390/s17061326
APA StyleAl-Qazzaz, N. K., Hamid Bin Mohd Ali, S., Ahmad, S. A., Islam, M. S., & Escudero, J. (2017). Automatic Artifact Removal in EEG of Normal and Demented Individuals Using ICA–WT during Working Memory Tasks. Sensors, 17(6), 1326. https://doi.org/10.3390/s17061326