
A Fast Multimodal Ectopic Beat Detection Method Applied for Blood Pressure Estimation Based on Pulse Wave Velocity Measurements in Wearable Sensors

Abstract
:1. Introduction
2. Previous Work
3. Materials and Methods
3.1. Pulse Wave Velocity Based on Electrocardiography and Photoplethysmography
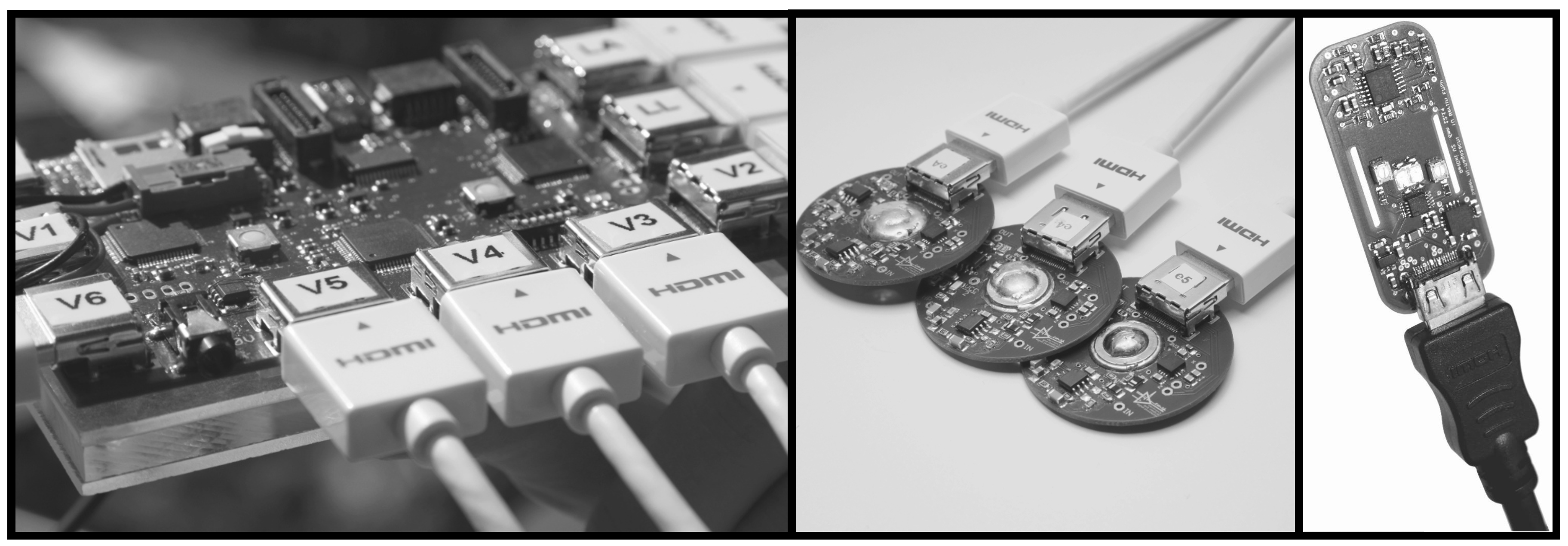
3.2. Wearable Hardware System
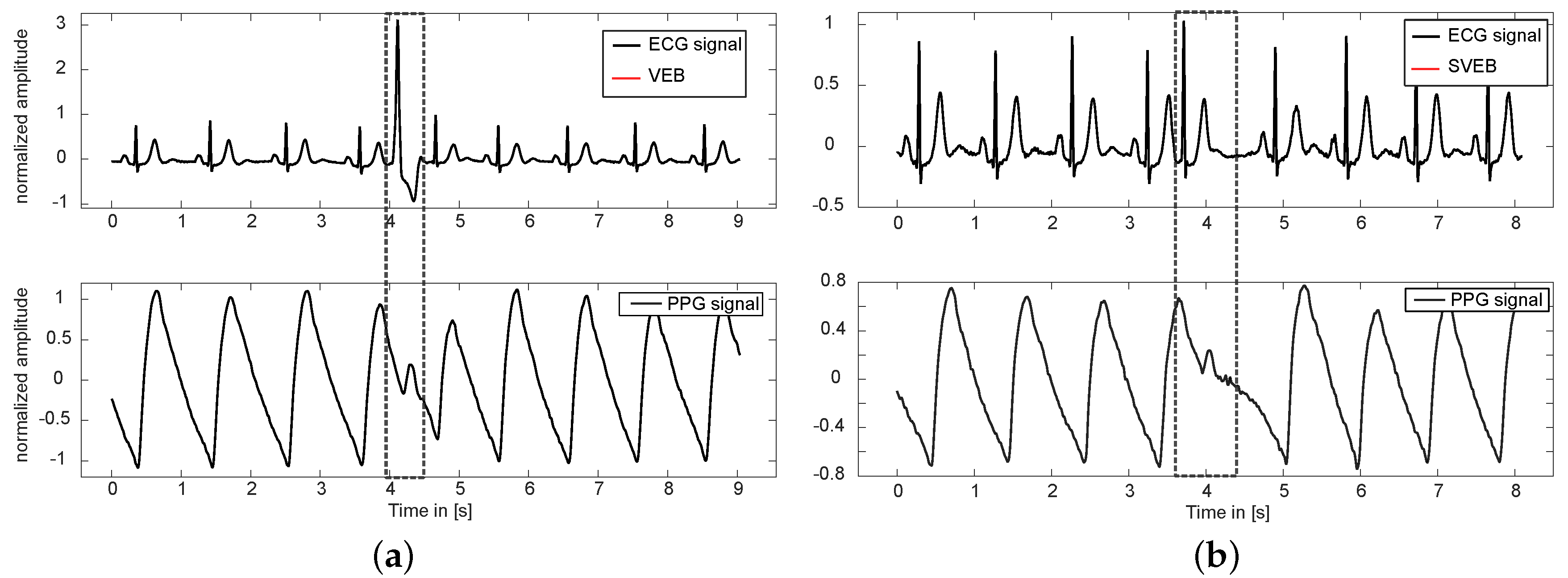
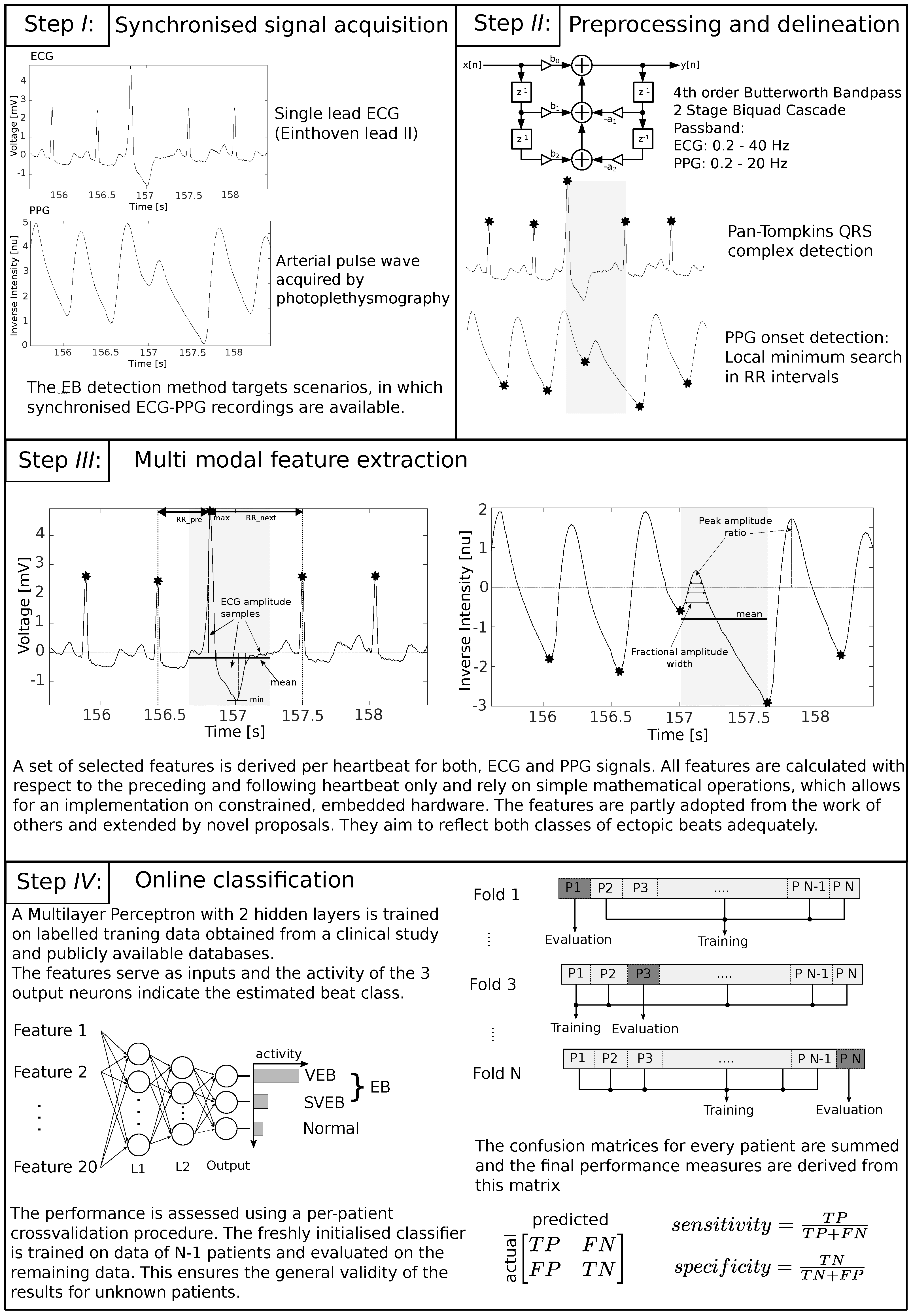
3.3. Multimodal Ectopic Beat Detection
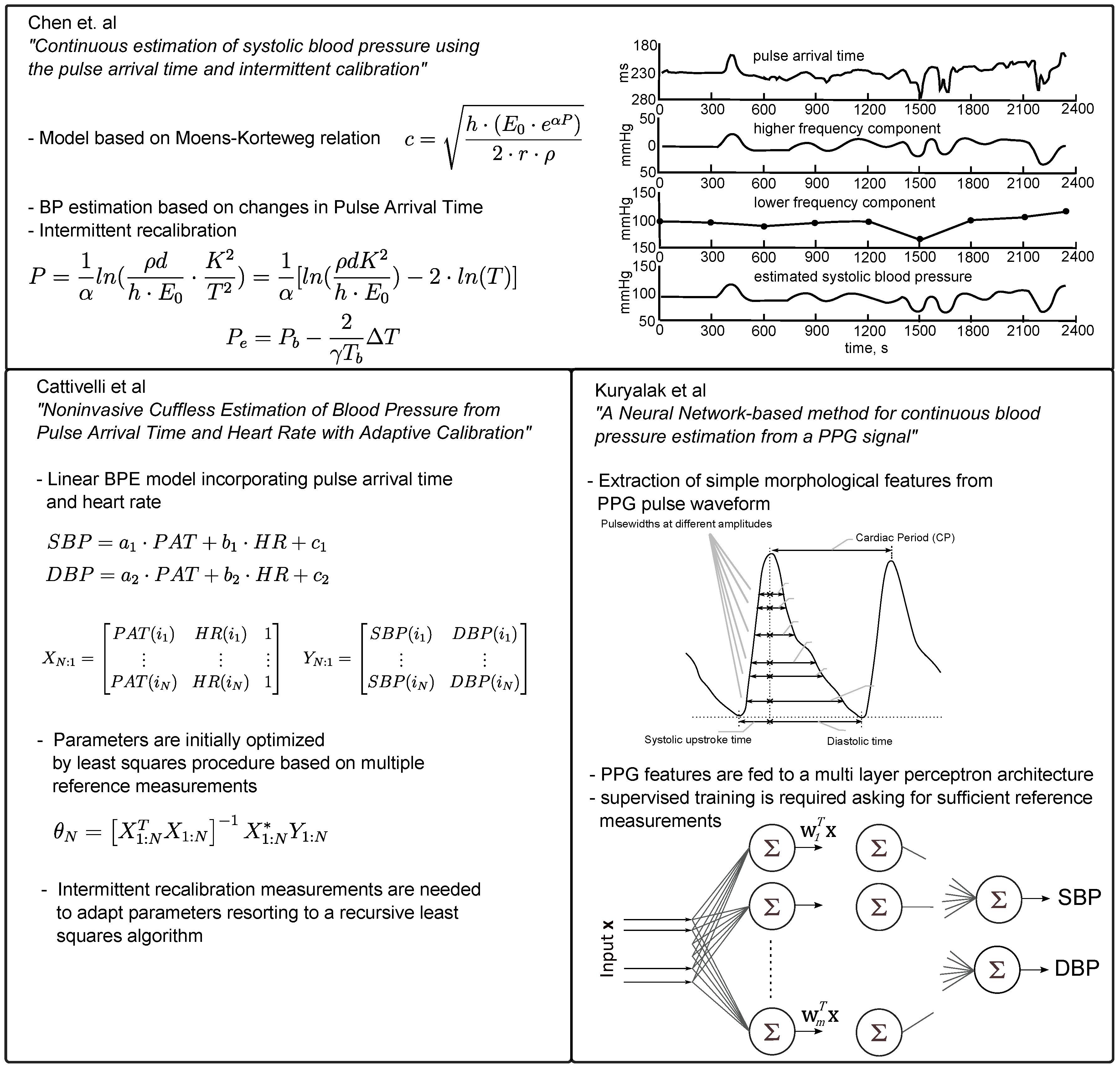
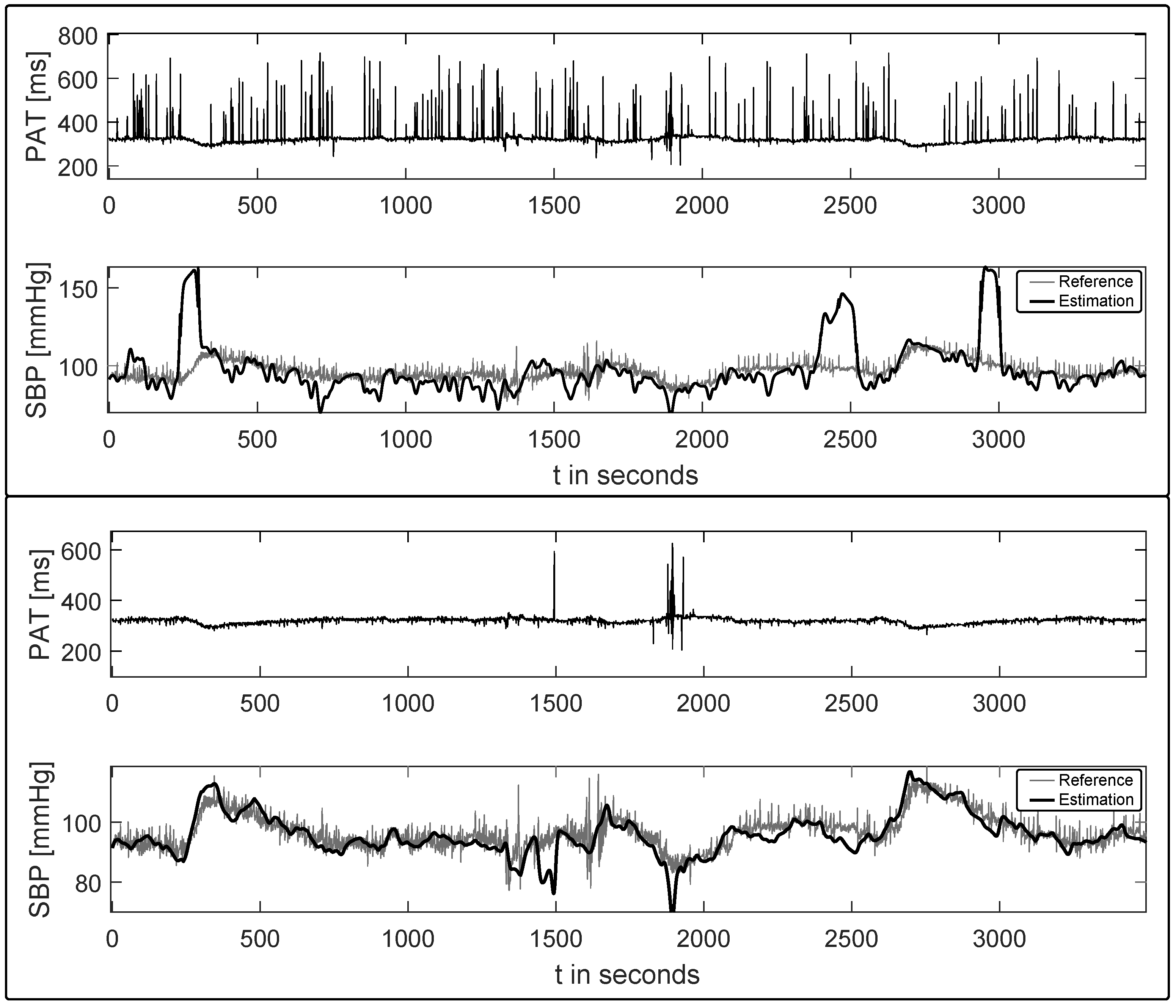
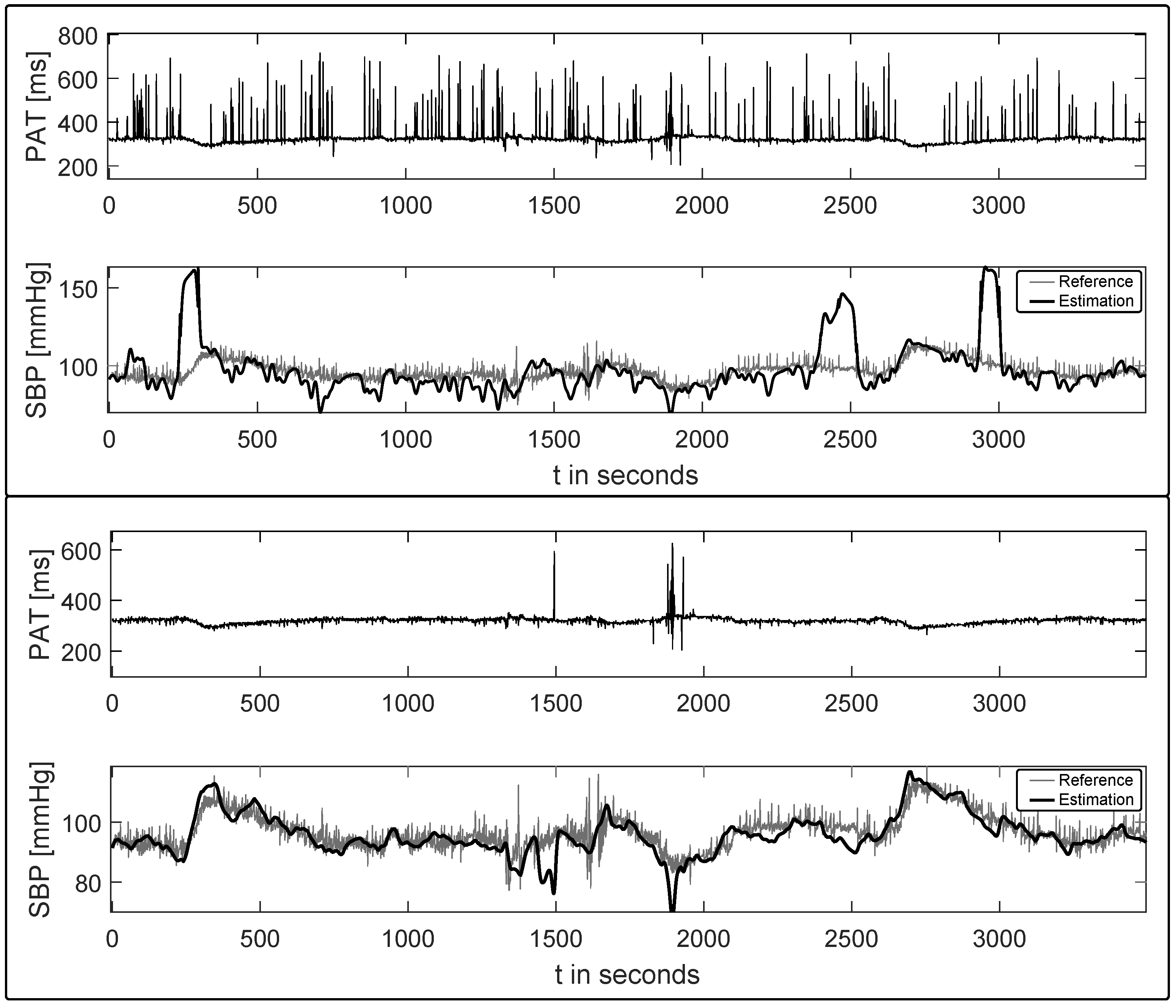
3.4. Blood Pressure Estimation
3.5. Data Acquisition/Databases
4. Results
4.1. Ectopic Beat Detection Performance
4.2. Blood Pressure Estimation Performance
5. Discussion
6. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| ABP | Arterial Blood Pressure |
| ANN | Artificial Neural Network |
| BPE | Blood Pressure Estimation |
| CC | Correlation Coefficient |
| DBP | Diastolic Blood Pressure |
| EB | Ectopic beat |
| ECG | Electrocardiography/Electrocardiogram |
| HR | Heart Rate |
| HRV | Heart Rate Variability |
| ICA | Independent Component Analysis |
| LDA | Linear Discrimination Analysis |
| PCA | Principal Component Analysis |
| PPG | Photoplethysmography/Photoplethysmogram |
| MGH/MF | Massachusetts General Hospital/Marquette Foundation |
| MIMIC | Multiparameter Intelligent Monitoring in Intensive Care |
| MIT-BIH | Massachusetts Institute of Technology - Beth Israel Hospital |
| MLP | Multi Layer Perceptron |
| MSE | Mean Squared Error |
| PAT | Pulse Arrival Time |
| PNN | Probabilistic Neural Networks |
| PTT | Pulse Transit Time |
| PWV | Pulse Wave Velocity |
| RMSE | Root Mean Square Error |
| RR | interval of two consecutive ECG R-Peaks |
| SBP | Systolic Blood Pressure |
| SD | Standard Deviation |
| SVEB | Supraventricular Ectopic Beat |
| SVM | Support Vector Machine |
| VEB | Ventricular Ectopic Beat |
References
- Bayes de Luna, A. Clinical Electrocardiography: A Textbook; Wiley-Blackwell: West Sussex, UK, 2012. [Google Scholar]
- Laplante, L.; Benzaquen, B.S. A Review of the Potential Pathogenicity and Management of Frequent Premature Ventricular Contractions. Pac. Clin. Electrophysiol. 2016, 39, 723–730. [Google Scholar] [CrossRef] [PubMed]
- Marino, P.L.; Sutin, K.M. The ICU Book; Williams & Wilkins Baltimore: Philadelphia, PA, USA, 1998. [Google Scholar]
- Augusto, J.F.; Teboul, J.L.; Radermacher, P.; Asfar, P. Interpretation of blood pressure signal: Physiological bases, clinical relevance, and objectives during shock states. Intensive Care Med. 2011, 37, 411–419. [Google Scholar] [CrossRef] [PubMed]
- Buxi, D.; Redoute, J.; Yuce, M. A survey on signals and systems in ambulatory blood pressure monitoring using pulse transit time. Physiol. Meas. 2015, 36, R1–R26. [Google Scholar] [CrossRef] [PubMed]
- Chow, H.S.; Moody, G.B.; Mark, R.G. Detection of ventricular ectopic beats using neural networks. In Proceedings of the Computers in Cardiology, Durham, NC, USA, 11–14 October 1992; pp. 659–662.
- Clifford, G.; Tarassenko, L.; Townsend, N. Fusing conventional ECG QRS detection algorithms with an auto-associative neural network for the detection of ectopic beats. In Proceedings of the International Conference on Signal Processing Proceedings, Beijing, China, 21–25 August 2000; pp. 1623–1628.
- Clifford, G.; Tarassenko, L.; Townsend, N. One-pass training of optimal architecture auto-associative neural network for detecting ectopic beats. Electron. Lett. 2011, 37, 1126–1127. [Google Scholar] [CrossRef]
- Martis, R.J.; Acharya, U.R.; Lim, C.M. ECG beat classification using PCA, LDA, ICA and Discrete Wavelet Transform. Biomed. Signal Process. Control 2013, 8, 437–448. [Google Scholar] [CrossRef]
- De Chazal, P.; O’Dwyer, M.; Reilly, R.B. Automatic classification of heartbeats using ECG morphology and heartbeat interval features. IEEE Trans. Biomed. Eng. 2004, 51, 1196–1206. [Google Scholar] [CrossRef] [PubMed]
- Sadiq, I.; Khan, S.A. Heart Beat Classification of ECGs Using Morphology and Beat Intervals. In Proceedings of the 5th International Conference on Bioinformatics and Biomedical Engineering, Wuhan, China, 10–12 May 2011; pp. 1–5.
- Solosenko, A.; Marozas, V. Automatic Premature Ventricular Contraction detection in photoplethysmographic signals. In Proceedings of the Biomedical Circuits and Systems Conference, Lousanne, Switzerland, 22–24 October 2014; pp. 49–52.
- Solosenko, A.; Petrenas, A.; Marozas, V. Photoplethysmography-Based Method for Automatic Detection of Premature Ventricular Contractions. IEEE Trans. Biomed. Circ. Syst. 2015, 9, 662–669. [Google Scholar] [CrossRef] [PubMed]
- Solosenko, A.; Marozas, V. Automatic Extrasystole Detection Using Photoplethysmographic Signals. In Proceedings of the Mediterranean Conference on Medical and Biological Engineering and Computing, Seville, Spain, 25–28 September 2013; pp. 985–988.
- Drijkoningen, L.; Lenaerts, F.; Van der Auwera, J.; Leysen, K.; Nuyens, D.; Vandervoort, P.; Grieten, L. Validation of a smartphone based photoplethysmographic beat detection algorithm for normal and ectopic complexes. In Proceedings of the Computing in Cardiology Conference, Cambridge, MA, USA, 7–10 September 2014; pp. 845–848.
- Palaniappan, R.; Navin Gupta, C.; Chan, K.L.; Krishnan, S.M. Multi-parameter detection of ectopic heart beats. In Proceedings of the IEEE International Workshop on Biomedical Circuits and Systems, Singapore, 1–3 December 2004.
- Palaniappan, R.; Krishnan, S.M. Detection of ectopic heart beats using ECG and blood pressure signals. In Proceedings of the International Conference on Signal Processing and Communications, Bangalore, India, 11–14 December 2004; pp. 573–576.
- Clifford, G.; Azuaje, F.; McSharry, P. Advanced Methods and Tools for ECG Data Analysis; Artech House Inc.: Norwood, MA, USA, 2006. [Google Scholar]
- Gacek, A.; Pedrycz, W. ECG Signal Processing, Classification and Interpretation: A Comprehensive Framework of Computational Intelligence; Springer Science & Business Media: London, UK, 2011. [Google Scholar]
- Webster, J.G. Design of Pulse Oximeters; CRC Press: Boca Raton, FL, USA, 1997. [Google Scholar]
- Allen, J. Photoplethysmography and its application in clinical physiological measurement. Physiol. Meas. 2007, 28, R1–R39. [Google Scholar] [CrossRef] [PubMed]
- Zong, W.; Heldt, T.; Moody, G.B.; Mark, R.G. An open-source algorithm to detect onset of arterial blood pressure pulses. In Proceedings of the Computers in Cardiology, Thessaloniki, Greece, 21–24 September 2003; pp. 259–262.
- Pflugradt, M.; Steffen, M.; Tigges, T.; Goernig, M.; Orglmeister, R. Multi-modal signal acquisition using a synchronized wireless body sensor network in geriatric patients. Biomed. Eng. 2016, 61, 57–68. [Google Scholar] [CrossRef] [PubMed]
- Pan, J.; Tompkins, W.J. A Real-Time QRS Detection Algorithm. IEEE Trans. Biomed. Eng. 1985, BME-32, 230–236. [Google Scholar] [CrossRef] [PubMed]
- Teng, X.F.; Zhang, Y.T. Continuous and noninvasive estimation of arterial blood pressure using a photoplethysmographic approach. In Proceedings of the 25th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Cancun, Mexico, 17–21 September 2003; Volume 4, pp. 3153–3156.
- Gribbin, B.; Steptoe, A.; Sleight, P. Pulse wave velocity as a measure of blood pressure change. Psychophysiology 1976, 1, 86–90. [Google Scholar] [CrossRef]
- Hughes, D.J.; Babbs, C.F.; Geddes, L.A.; Bouland, J.D. Measurements of Young’s modulus of elasticity of the canine aorta with ultrasound. Ultrason. Imag. 1979, 1, 356–367. [Google Scholar] [CrossRef]
- Baruch, M.; Warburton, D.; Bredin, S.; Cote, A.; Gerdt, D.; Adkins, C. Pulse Decomposition Analysis of the digital arterial pulse during hemorrhage simulation. Nonlinear Biomed. Phys. 2011, 1, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Kobayashi, T.; Ichikawa, S.; Takeuchi, Y.; Togawa, T. Continuous estimation of systolic blood pressure using the pulse arrival time and intermittent calibration. Med. Biol. Engi. Comput. 2000, 38, 569–574. [Google Scholar] [CrossRef]
- Cattivelli, F.S.; Garudadri, H. Noninvasive Cuffless Estimation of Blood Pressure from Pulse Arrival Time and Heart Rate with Adaptive Calibration. In Proceedings of the Sixth International Workshop on Wearable and Implantable Body Sensor Networks, Berkeley, CA, USA, 3–5 June 2009; pp. 114–119.
- Kurylyak, Y.; Lamonaca, F.; Grimaldi, D. A Neural Network-based method for continuous blood pressure estimation from a PPG signal. In Proceedings of the IEEE International Instrumentation and Measurement Technology Conference (I2MTC), Minneapolis, MN, USA, 6–9 May 2013; pp. 280–283.
- Linder, S.; Wendelken, S.; Wei, E.; McGrath, S. Using the morphology of photoplethsymogram peaks to detect changes in posture. J. Clin. Monit. Comput. 2006, 20, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Clifford, G.D.; Silva, I.; Moody, B.; Li, Q.; Kella, D.; Shahin, A.; Kooistra, T.; Perry, D.; Mark, R.G. Physiobank, physiotoolkit, and physionet components of a new research resource for complex physiologic signals. Comput. Cardiol. 2015, 42, 273–276. [Google Scholar]
- Goldberger, A.L.; Amaral, L.A.N.; Glass, L.; Hausdorff, J.M.; Plamen, C.H.; Roger, R.; Mietus, J.; Moody, G.B.; George, B.; Peng, C.K.; et al. Physiobank, physiotoolkit, and physionet components of a new research resource for complex physiologic signals. Circulation 1996, 23, 215–220. [Google Scholar] [CrossRef]
- Moody, G.B.; Mark, R.G. A database to support development and evaluation of intelligent intensive care monitoring. Comput. Cardiol. 1996, 23, 657–660. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number | Description | References |
|---|---|---|
| 1 | leading/trailing interval of consecutive R-Peaks (RR) | [10] |
| 2 | ECG heartbeat power | |
| 3 | ECG hearbeat mean | |
| 4 | ECG heartbeat max/min | |
| 5–14 | samples around R peak | [10] |
| 15–17 | PPG fractional amplitude | [25] |
| 18 | PPG pulse wave power | |
| 19 | PPG pulse wave mean | |
| 20 | current/next PPG pulse peak amplitude |
| Mean Error | RMSE | CC | Prob. 0% | Prob. 10% | Prob. 16% |
|---|---|---|---|---|---|
| mmHg | mmHg |
| Mean Error | Standard Deviation of Error | MSE |
|---|---|---|
| mmHg | mmHg | 5 mmHg |
| Absolute Error | Relative Error |
|---|---|
| mmHg |
| Database | Record | # N | # Ventricular Ectopic Beats | # Supraventricular Ectopic Beats |
|---|---|---|---|---|
| rBSN | au_03 | 1381 | 4 | 27 |
| rBSN | dd_02 | 645 | 0 | 70 |
| rBSN | dd_03 | 141 | 6 | 7 |
| rBSN | dd_06 | 688 | 4 | 3 |
| PC15 | a624s | 302 | 1 | 2 |
| PC15 | a746s | 406 | 5 | 0 |
| PC15 | b340s | 254 | 0 | 22 |
| PC15 | b341l | 260 | 0 | 23 |
| PC15 | b515l | 211 | 2 | 4 |
| PC15 | b517l | 227 | 0 | 6 |
| PC15 | b560s | 139 | 10 | 17 |
| PC15 | b562s | 123 | 29 | 11 |
| PC15 | b838s | 242 | 20 | 28 |
| PC15 | f642s | 457 | 0 | 8 |
| PC15 | t416s | 240 | 1 | 40 |
| PC15 | t662s | 567 | 6 | 0 |
| PC15 | t680s | 348 | 15 | 3 |
| PC15 | t752s | 383 | 0 | 5 |
| PC15 | t762s | 313 | 5 | 38 |
| PC15 | v132s | 227 | 15 | 0 |
| PC15 | v158s | 77 | 6 | 1 |
| PC15 | v205l | 87 | 10 | 9 |
| PC15 | v253l | 535 | 77 | 0 |
| PC15 | v254s | 441 | 35 | 3 |
| PC15 | v255l | 445 | 47 | 0 |
| PC15 | v368s | 329 | 6 | 0 |
| PC15 | v427l | 175 | 0 | 17 |
| PC15 | v557l | 264 | 4 | 0 |
| PC15 | v559l | 354 | 23 | 9 |
| PC15 | v573l | 335 | 0 | 2 |
| PC15 | v648s | 340 | 2 | 1 |
| PC15 | v696s | 237 | 0 | 46 |
| PC15 | v769l | 357 | 25 | 1 |
| PC15 | v831l | 319 | 15 | 0 |
| PC15 | v833l | 217 | 13 | 3 |
| TOTAL | 12066 | 386 | 406 |
| Set of Features | Sensitivity | Sensitivity SVEB | Sensitivity VEB | Specificity |
|---|---|---|---|---|
| PPG | 77.7 | 68.2 | 87.6 | 95.5 |
| ECG | 91.12 | 87.2 | 95.3 | 98.9 |
| All | 95.7 | 96.1 | 95.3 | 99.0 |
| Clock Cycles | RAM Usage (Byte) | ||||
|---|---|---|---|---|---|
| Step | per | ECG | PPG | ECG | PPG |
| Filter | 64 samples | 2414 | 2414 | 68 | 68 |
| Delineation | sample | 418 | 75 | 388 | 44 |
| Feature Extraction | heartbeat | 8822 | 8445 | 4000 | 4000 |
| Classification | heartbeat | 980 | 1200 | ||
| Total | heartbeat | 283,239 | 4456 | ||
| Method | Mean Error | SD Error | CC | MSE | RMS | ||
|---|---|---|---|---|---|---|---|
| (a) BPE performance measures on datasets with no ectopic beats | |||||||
| Chen | |||||||
| Cattiveli | |||||||
| Kuryalak | |||||||
| (b) BPE performance measures on datasets with ectopic beat presence | |||||||
| Chen | |||||||
| Cattiveli | |||||||
| Kuryalak | 7112 | ||||||
| (c) BPE performance measures on datasets with ectopic beat presence, after prior EB clearance | |||||||
| Chen | |||||||
| Cattiveli | |||||||
| Kuryalak | |||||||
© 2017 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pflugradt, M.; Geissdoerfer, K.; Goernig, M.; Orglmeister, R. A Fast Multimodal Ectopic Beat Detection Method Applied for Blood Pressure Estimation Based on Pulse Wave Velocity Measurements in Wearable Sensors. Sensors 2017, 17, 158. https://doi.org/10.3390/s17010158
Pflugradt M, Geissdoerfer K, Goernig M, Orglmeister R. A Fast Multimodal Ectopic Beat Detection Method Applied for Blood Pressure Estimation Based on Pulse Wave Velocity Measurements in Wearable Sensors. Sensors. 2017; 17(1):158. https://doi.org/10.3390/s17010158
Chicago/Turabian StylePflugradt, Maik, Kai Geissdoerfer, Matthias Goernig, and Reinhold Orglmeister. 2017. "A Fast Multimodal Ectopic Beat Detection Method Applied for Blood Pressure Estimation Based on Pulse Wave Velocity Measurements in Wearable Sensors" Sensors 17, no. 1: 158. https://doi.org/10.3390/s17010158
APA StylePflugradt, M., Geissdoerfer, K., Goernig, M., & Orglmeister, R. (2017). A Fast Multimodal Ectopic Beat Detection Method Applied for Blood Pressure Estimation Based on Pulse Wave Velocity Measurements in Wearable Sensors. Sensors, 17(1), 158. https://doi.org/10.3390/s17010158