
Toward a Smartphone Application for Estimation of Pulse Transit Time



Abstract
:1. Introduction
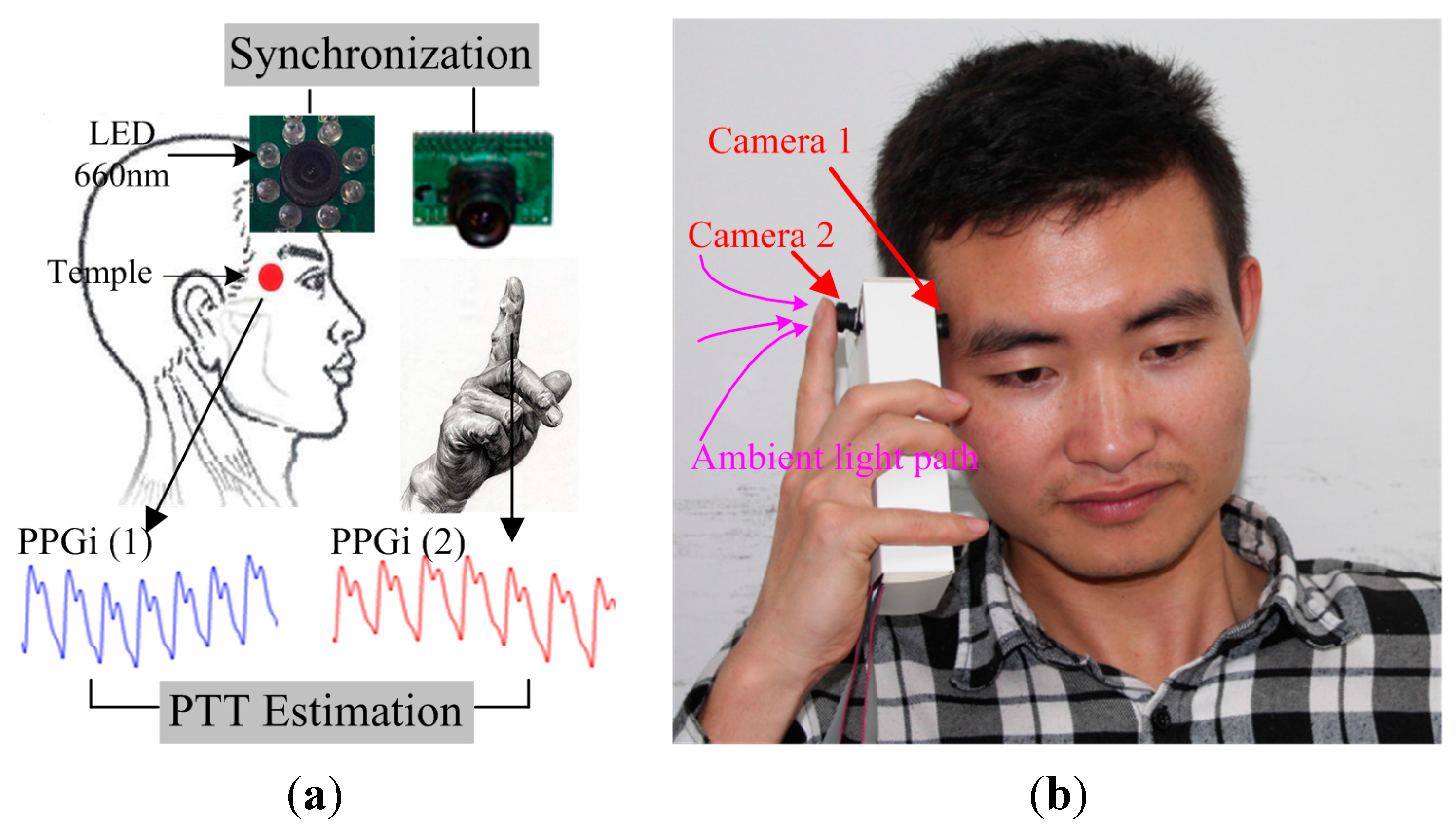
2. System Components and Configuration
2.1. Image Sensor Module
2.2. Configuration of Analytic System

2.3. Region of Interest (ROI)
2.4. Experimental Protocol
2.4.1. Experiment 1 Setup
2.4.2. Experiment 2 Setup
3. Algorithm
3.1. Image Acquisition and Processing
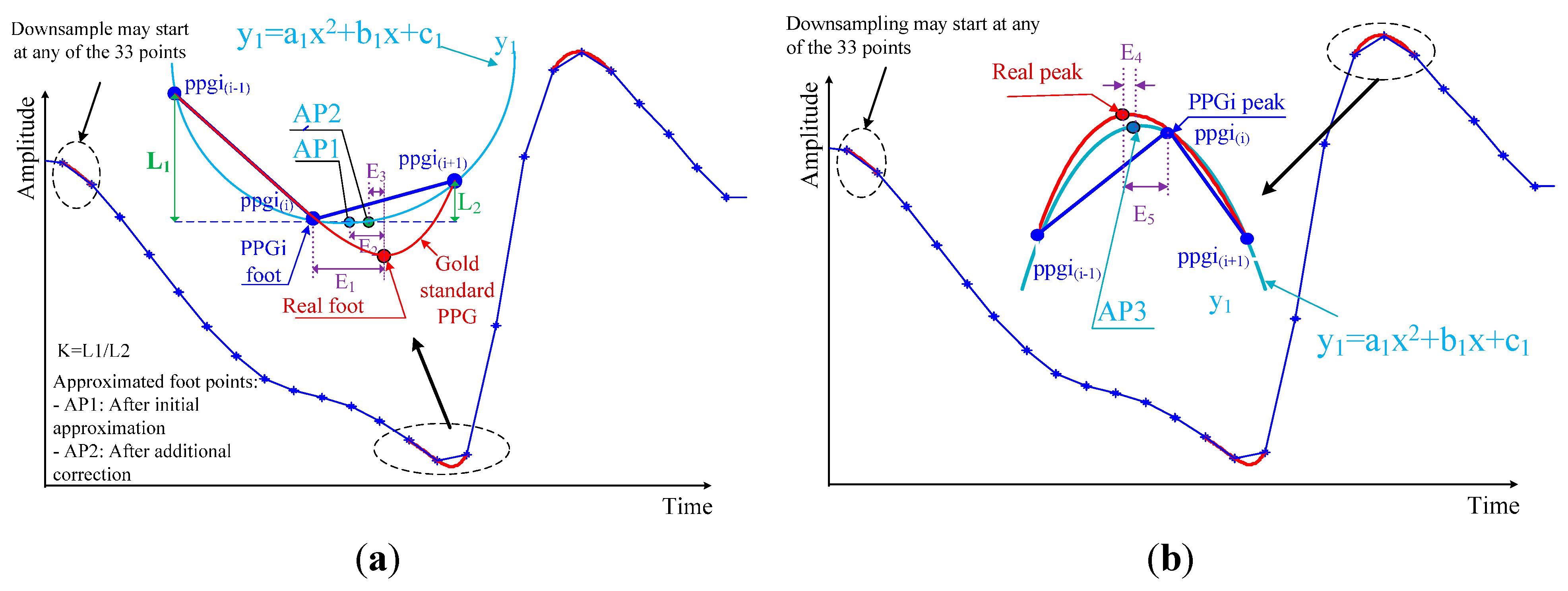
3.2. Detection of Maxima and Minima in PPGi Signals

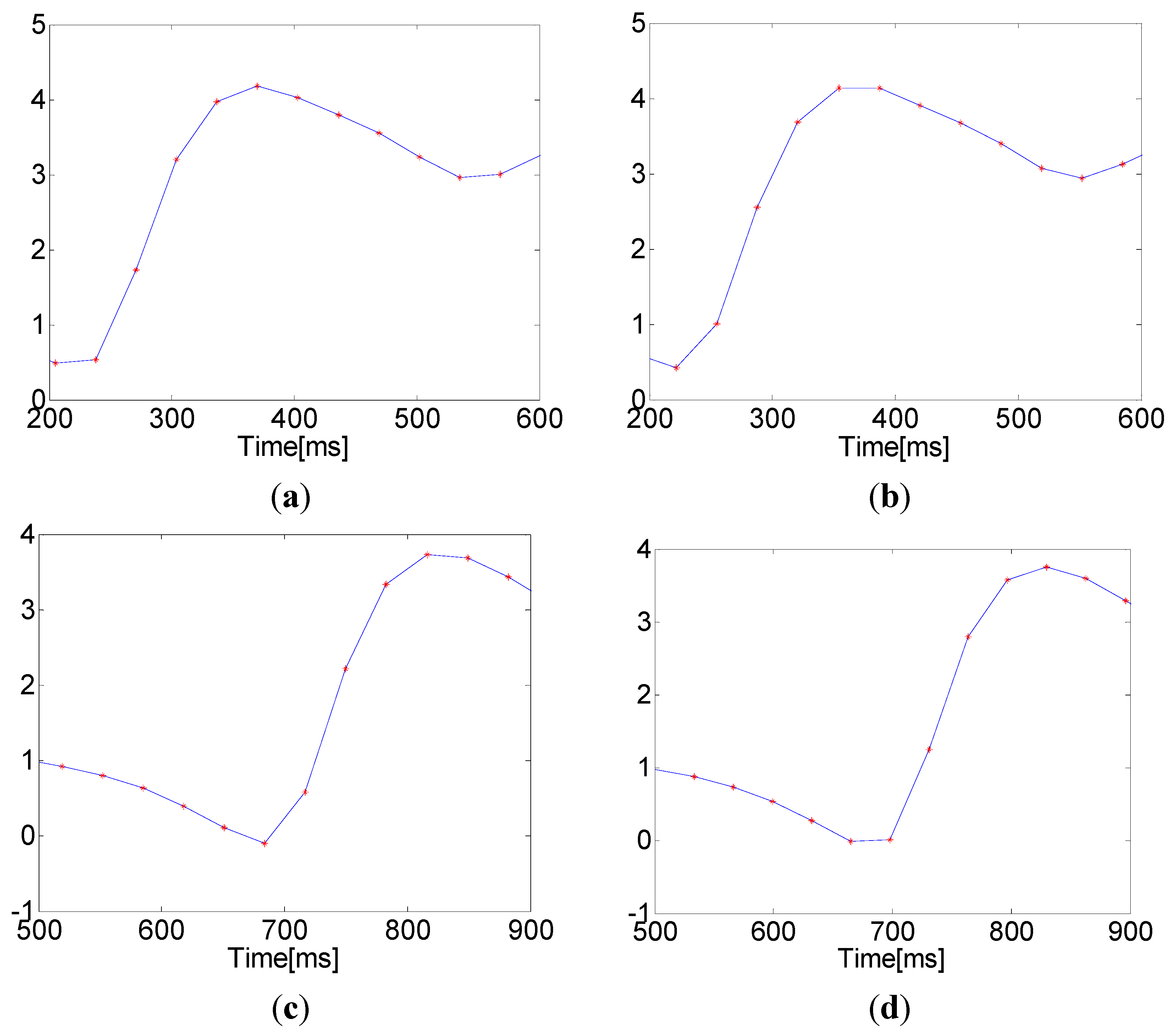
3.3. Improving the Detection Accuracy

3.4. PTT Estimation
3.5. Evaluation
4. Results
4.1. Performance in Detection of Maxima and Minima

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Illumination Light (Site) | Method | Maximum | Minimum | ||
|---|---|---|---|---|---|
| SE | PPV | SE | PPV | ||
| 660 nm (temple) | Shin’s method | 76.72% | 88.24% | 88.24% | 99.98% |
| The proposed method | 92.85% | 97.44% | 97.44% | 100% | |
| Ambient light (fingertip) | Shin’s method | 89.27% | 97.72% | 97.72% | 100% |
| The proposed method | 98.07% | 98.64% | 98.64% | 100% | |

4.2. Performance of Corrective Adjustments to Locations
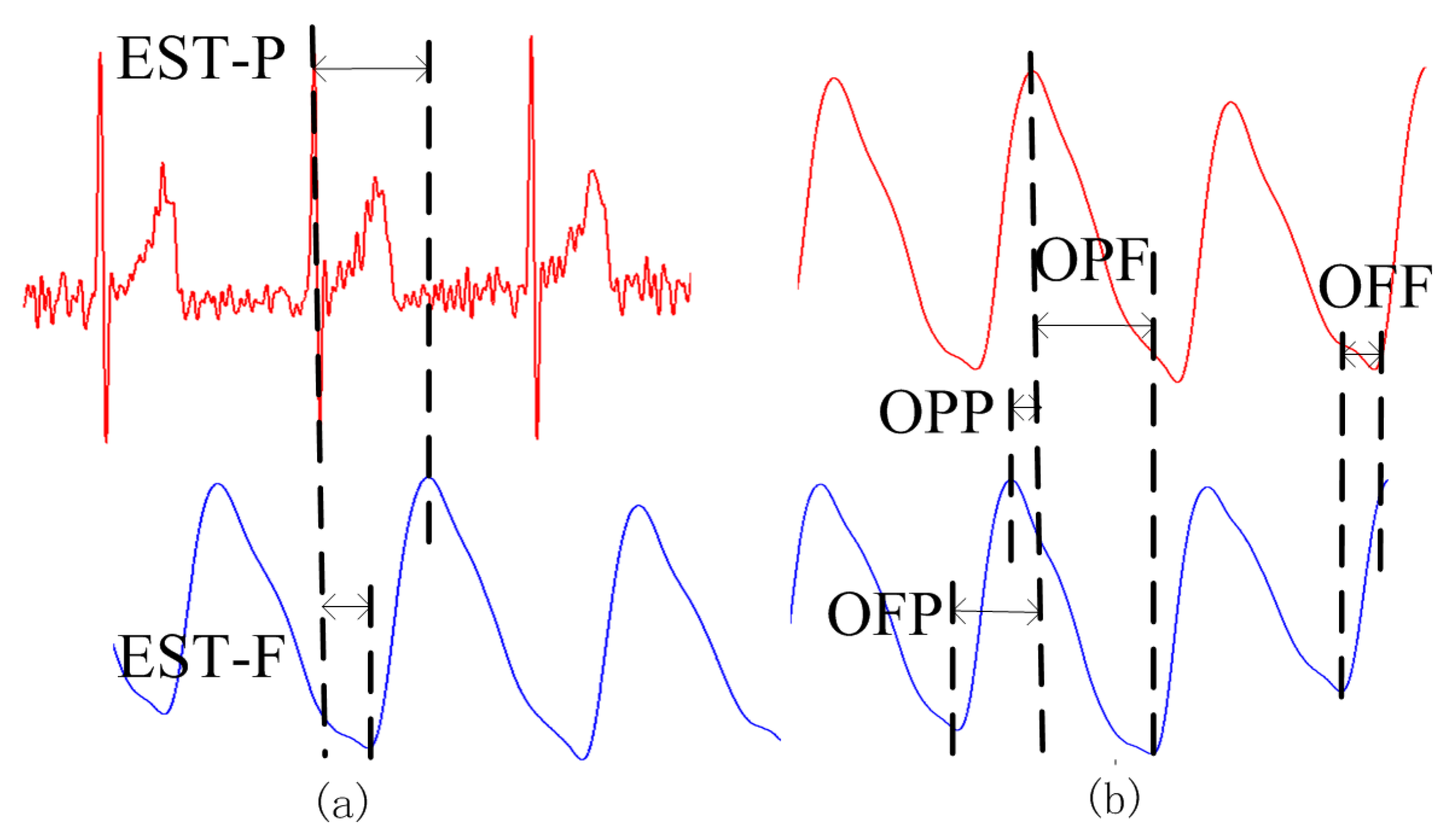
4.3. PTT Acquisition and Evaluation
4.3.1. Experiment 1
4.3.2. Experiment 2
| (mean ± SD) | Regression Slope | ||
|---|---|---|---|
| EST_P~OPP | 0.65 ± 0.14 | Negative | 8 |
| EST_F~OPP | 0.05 ± 0.18 | N/A a | 0 |
| EST_P~OPF | 0.68 ± 0.07 | Negative | 11 |
| EST_F~OPF | 0.23 ± 0.11 | Positive | 0 |
| EST_P~OFP | 0.86 ± 0.06 | Positive | 12 |
| EST_F~OFP | 0.60 ± 0.09 | Positive | 5 |
| EST_P~OFF | 0.57 ± 0.15 | Positive | 4 |
| EST_F~OFF | 0.76 ± 0.12 | Positive | 11 |

5. Discussion
5.1. PTT Detection
5.2. Shortcomings and Improvements
6. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Campo, A.; Segers, P.; Heuten, H.; Goovaerts, I.; Ennekens, G.; Vrints, C.; Baets, R.; Dirckx, J. Non-invasive technique for assessment of vascular wall stiffness using laser doppler vibrometry. Meas. Sci. Technol. 2014, 25, 065701–065711. [Google Scholar] [CrossRef]
- Salvi, P.; Palombo, C.; Salvi, G.M.; labat, C.; Parati, G.; Benetos, A. Left ventricular ejection time, not heart rate, is an independent correlate of aortic pulse wave velocity. J. Appl. Physiol. 2013, 115, 1610–1617. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Yan, B.P.; Yu, C.M.; Zhang, Y.T.; Poon, C.Y. Attenuation of Systolic Blood Pressure and Pulse Transit Time Hysteresis During Exercise and Recovery in Cardiovascular Patients. IEEE. Trans. Biomed. Eng. 2014, 61, 346–352. [Google Scholar] [PubMed]
- Foo, J.Y.; Lim, C.S.; Wang, P. Evaluation of blood pressure changes using vascular transit time. Physiol. Meas. 2006, 27, 685–694. [Google Scholar] [CrossRef] [PubMed]
- Katz, E.S.; Lutz, J.; Black, C.; Marcus, C.L. Pulse transit time as measure of arousal and respiratory effort in children with sleep-disordered breathing. Pediatr. Res. 2003, 53, 580–588. [Google Scholar] [CrossRef] [PubMed]
- Pepin, J.L.; Delavie, N.; Pin, I.; Deschaux, C.; Argod, J.; Bost, M.; Levy, P. Pulse transit time improves detection of sleep respiratory events and microarousals in children. Chest. J. 2005, 127, 722–730. [Google Scholar] [CrossRef] [PubMed]
- Poyares, D.; Guilleminault, C.; Rosa, A.; Ohayon, M.; koester, U. Arousal, EEG spectral power and pulse transit time UARS and mild OSAS subjects. Clin. Neurophysiol. 2002, 113, 1598–1606. [Google Scholar]
- Argod, J.; Pepin, J.; Smith, R.P.; Lew, P. Comparison of esophageal pressure with pulse transit time as a measure of respiratory effort for scoring obstructive nonapneic respiratory events. Am. J. Respir. Crit. Care. Med. 2000, 162, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.P.; Argod, J.; Pepi, J.L.; Levy, P.A. Pulse transit time: An appraisal of potential clinical applications. Thorax 1999, 54, 452–457. [Google Scholar] [CrossRef] [PubMed]
- Foo, J.Y.; Wilson, S.J.; Bradle, A.P.; Williams, G.R.; Harris, M.A.; Cooper, D.M. Use of pulse transit time to distinguish respiratory events from tidal breathing in sleeping children. Chest. J. 2005, 128, 3013–3019. [Google Scholar] [CrossRef] [PubMed]
- Loukogeorgakis, S.; Dawson, R.; Phillips, N.; Martyn, C.N.; Greenwald, S.E. Validation of a device to measure arterial pulse wave velocity by a photoplethysmographic method. Physiol. Meas. 2002, 23, 581–596. [Google Scholar] [CrossRef] [PubMed]
- Hahn, J.; Reisner, A.T.; Asada, H.H. Estimation of pulse transit time using two diametric blood pressure waveform measurements. Med. Eng. Phys. 2010, 32, 753–759. [Google Scholar] [CrossRef] [PubMed]
- Xu, D.; Ryan, K.L.; Rickards, C.A.; Zhang, G.Q.; Convertino, V.A.; Mukkamala, R. Improved pulse transit time estimation by system identification analysis of proximal and distal arterial waveforms. Am. J. Primatol. 2011, 301, 1389–1395. [Google Scholar] [CrossRef] [PubMed]
- Rashedi, M.; Fazeli, N.; Chappell, A.; Wang, S.; MacArthur, R.; McMurtry, M.S.; Finegan, B.A.; Hahn, J. Comparative Study on Tube-Load Modeling of Arterial Hemodynamics in Humans. J. Biomech. Eng. 2013, 135. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Wang, Y.D.; Wang, L. A review of non-contact, low-cost physiological information measurement based on photoplethysmographic imaging. In Proceedings of the 2012 Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), San Diego, CA, USA, 28 August–1 September 2012; pp. 2088–2091.
- Scully, C.G.; Lee, J.; Meyer, J.; Gorbach, A.M.; Granquist-Fraser, D.; Mendelson, Y.; Chon, K.H. Physiological Parameter Monitoring from Optical Recordings With a Mobile Phone. IEEE. Trans. Biomed. Eng. 2012, 59, 303–306. [Google Scholar] [CrossRef] [PubMed]
- Chandrasekaran, V.; Dantu, R.; Jonnada, S.; Thiyagaraja, S.; Subbu, K.P. Cuffless Differential Blood Pressure Estimation Using Smart Phones. IEEE. Trans. Biomed. Eng. 2013, 60, 1080–1089. [Google Scholar] [CrossRef] [PubMed]
- Nitzan, M.; Khanokh, B.; Slovik, Y. The difference in pulse transit time to the toe and finger measured by photoplethysmography. Physiol. Meas. 2002, 23, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Ivanov, K.; Wang, Y.D.; Wang, L. An novel method based on two cameras for accurate estimation of arterial oxygen saturation. Biomed. Eng. Online 2015, 14. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Wang, Y.D.; Wang, L. FPGA-Based Remote Pulse Rate Detection Using Photoplethys-Mographic Imaging. In Proceedings of the 2013 IEEE International Conference on Body Sensor Networks (BSN), Cambridge, MA, USA, 6–9 May 2009; pp. 1–5.
- Allen, J.; Murray, A. Similarity in bilateral photoplethysmographic peripheral pulse wave characteristics at the ears, thumbs and toes. Physiol. Meas. 2000, 21, 369–377. [Google Scholar] [CrossRef] [PubMed]
- Tur, E.; Tur, M.; Maibach, H.I.; Guy, R.H. Basal perfusion of the cutaneous microcirculation: Measurements as a function of anatomic position. J. Invest. Dermatol. 1983, 81, 442–446. [Google Scholar] [CrossRef] [PubMed]
- Asmar, R.; Benetos, A.; Topouchian, J.; Laurent, P.; Pannier, B.; Brisac, A.M.; Target, R.; Levy, B.I. Assessment of arterial distensibility by automatic pulse wave velocity measurement. Validation and clinical application studies. Hypertension 1995, 26, 485–490. [Google Scholar] [CrossRef] [PubMed]
- Talke, P.; Snapir, A.; Huiku, M. The effects of sympathectomy on finger photoplethysmography and temperature measurements in healthy subjects. Anesth. Analg. 2011, 113, 78–83. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Xu, G.; Wang, Y.D.; Wang, L. The Effect of Light Conditions on Photoplethysmographic Image Acquisition Using a Commercial Camera. IEEE J. Transl. Eng. Health Med. 2014, 2. [Google Scholar] [CrossRef]
- Poh, M.Z.; McDuff, D.J.; Picard, R.W. Non-contact, automated cardiac pulse measurements using video imaging and blind source separation. Opt. Express. 2010, 18, 10762–10774. [Google Scholar] [CrossRef] [PubMed]
- Verkruysse, W.; Svaasand, L.O.; Nelson, J.S. Remote plethysmographic imaging using ambient light. Opt. Express. 2008, 16, 21434–21445. [Google Scholar] [CrossRef] [PubMed]
- Matsumura, K.; Rolfe, P.; Lee, J.; Yamakoshi, T. Iphone 4s Photoplethymography: Which Light Color Yields the Most Accurate Heart Rate and Normalized Pulse Volume Using the iPhysioMeter Application in the Presence of Motion Artifact? PLoS ONE 2014, 9. [Google Scholar] [CrossRef] [PubMed]
- Shin, H.S.; Lee, C.; Lee, M. Adaptive threshold method for the peak detection of photoplethys-mographic waveform. Comput. Biol. Med. 2009, 39, 1145–1152. [Google Scholar] [CrossRef] [PubMed]
- Nichols, W.; O’Rourke, M.; Vlachopoulos, C. McDonald’s Blood Flow in Arteries, Sixth Edition: Theoretical, Experimental and Clinical Principles; CRC Press: Boca Raton, FL, USA, 2011. [Google Scholar]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 327, 307–310. [Google Scholar] [CrossRef]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, H.; Ivanov, K.; Wang, Y.; Wang, L. Toward a Smartphone Application for Estimation of Pulse Transit Time. Sensors 2015, 15, 27303-27321. https://doi.org/10.3390/s151027303
Liu H, Ivanov K, Wang Y, Wang L. Toward a Smartphone Application for Estimation of Pulse Transit Time. Sensors. 2015; 15(10):27303-27321. https://doi.org/10.3390/s151027303
Chicago/Turabian StyleLiu, He, Kamen Ivanov, Yadong Wang, and Lei Wang. 2015. "Toward a Smartphone Application for Estimation of Pulse Transit Time" Sensors 15, no. 10: 27303-27321. https://doi.org/10.3390/s151027303
APA StyleLiu, H., Ivanov, K., Wang, Y., & Wang, L. (2015). Toward a Smartphone Application for Estimation of Pulse Transit Time. Sensors, 15(10), 27303-27321. https://doi.org/10.3390/s151027303