
Bone Remodeling in Children with Acute Lymphoblastic Leukemia: A Two-Year Prospective Longitudinal Study

 , , , , ,
, , , , ,  and
and 
Abstract
1. Introduction
2. Results
2.1. Patient Population
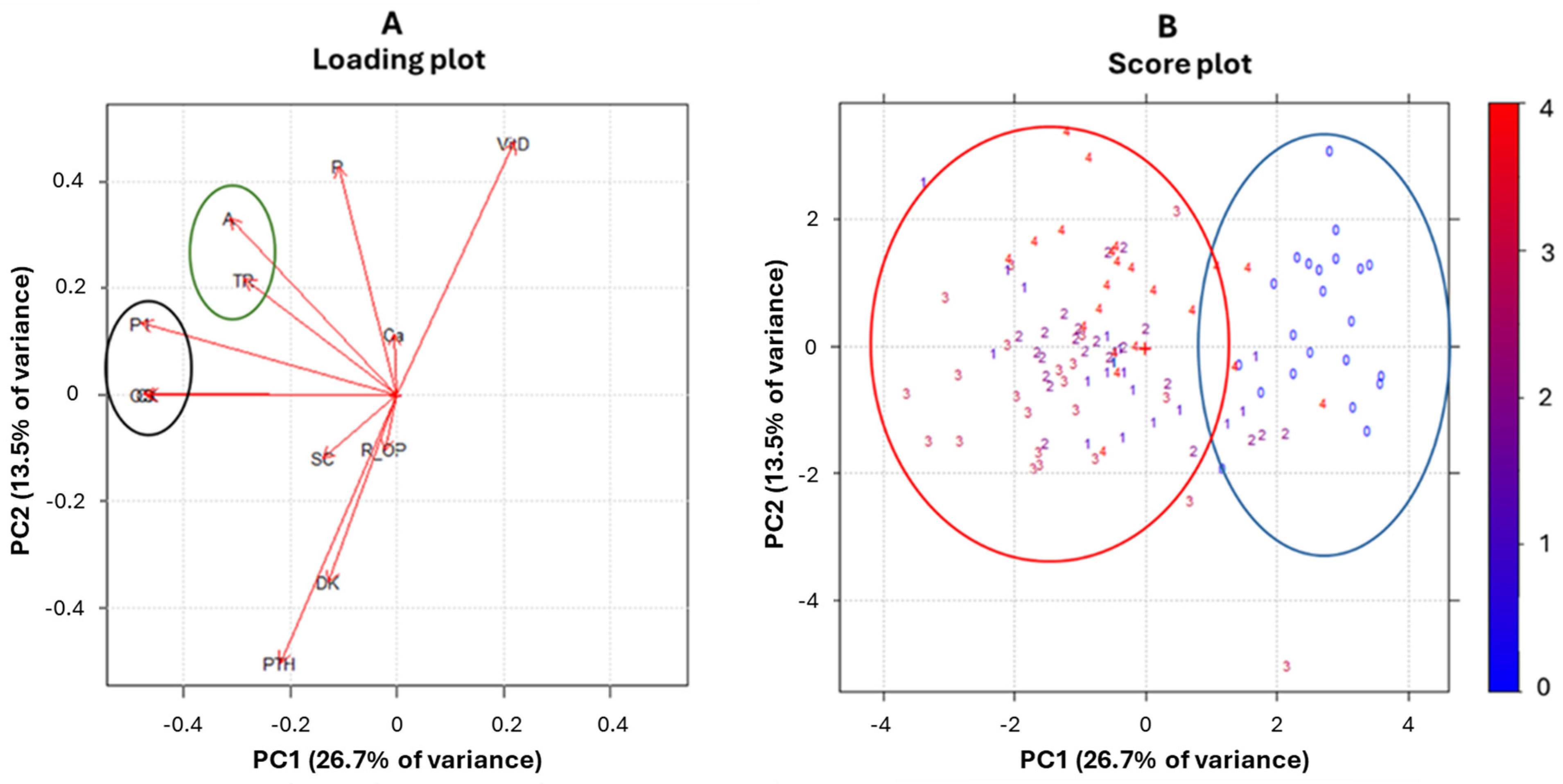
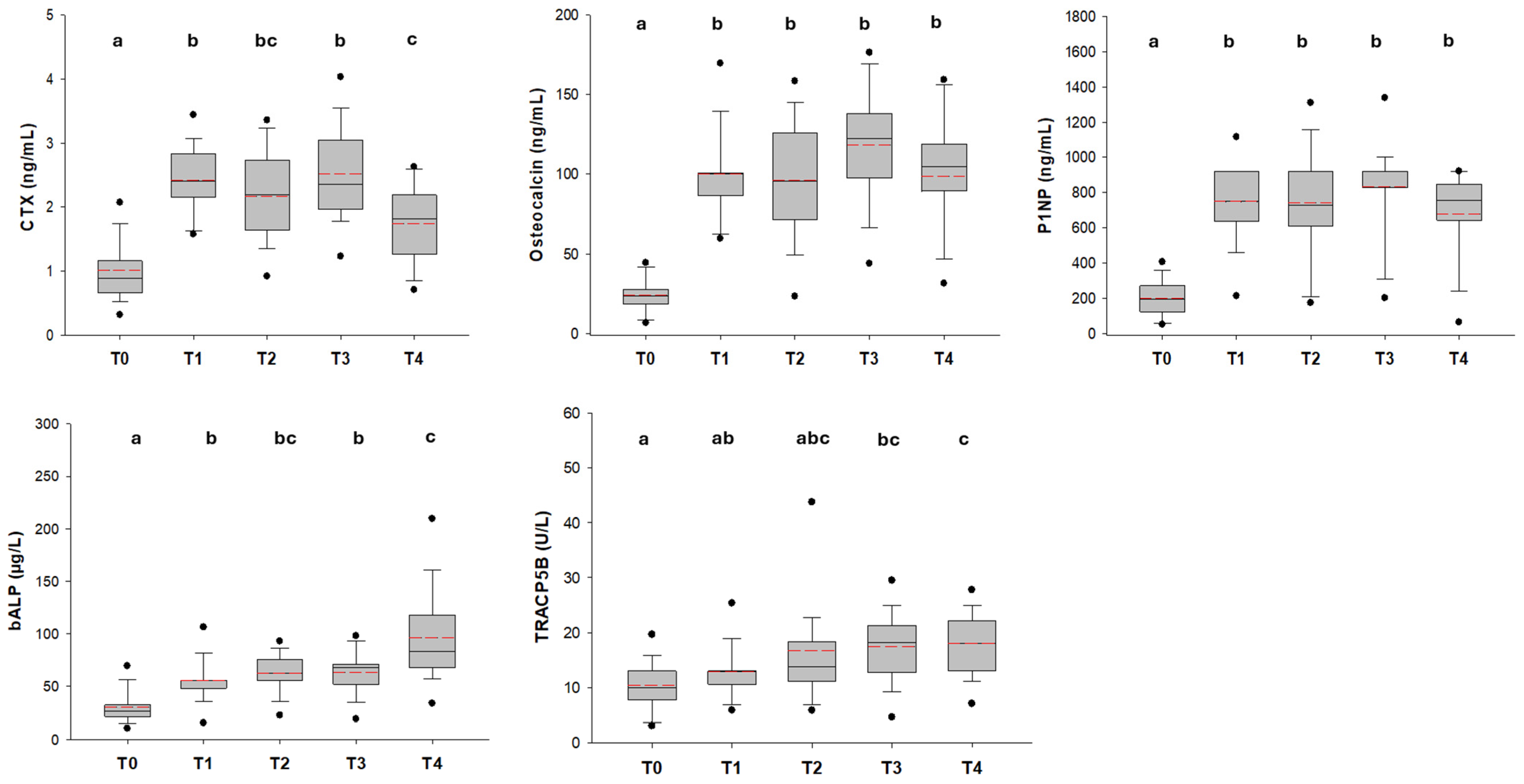
2.2. Bone Turnover and Bone-Remodeling Markers
3. Discussion
4. Materials and Methods
4.1. Subjects
4.2. Risk Stratification and Treatment
4.3. Clinical Data
4.4. Bone Turnover Markers
4.5. Bone Remodeling Cytokines Assessment
4.6. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ALL | acute lymphoblastic leukemia |
| GCs | glucocorticoids |
| RANKL | receptor activator of nuclear factor κB ligand |
| OPG | osteoprotegerin |
| DKK-1 | dickkopf-related protein 1 |
| bALP | bone alkaline phosphatase |
| OC | osteocalcin |
| P1NP | procollagen I N-propeptide |
| CTX | C-terminal telopeptide cross-links of type I collagen |
| TRAcP5b | tartrate-resistant acid phosphatase 5b |
| 25-OH vit D | 25 hydroxy vitamin D |
| PTH | parathormone |
| PCA | principal component analysis |
References
- Ward, E.; DeSantis, C.; Robbins, A.; Kohler, B.; Jemal, A. Childhood and adolescent cancer statistics, 2014. CA Cancer J. Clin. 2014, 64, 83–103. [Google Scholar] [CrossRef]
- Inaba, H.; Greaves, M.; Mullighan, C.G. Acute lymphoblastic leukaemia. Lancet 2013, 381, 1943–1955. [Google Scholar] [CrossRef]
- Saultier, P.; Michel, G. How I treat long-term survivors of childhood acute leukemia. Blood 2024, 143, 1795–1806. [Google Scholar] [CrossRef] [PubMed]
- Mody, R.; Li, S.; Dover, D.C.; Sallan, S.; Leisenring, W.; Oeffinger, K.C.; Yasui, Y.; Robison, L.L.; Neglia, J.P. Twenty-five-year follow-up among survivors of childhood acute lymphoblastic leukemia: A report from the Childhood Cancer Survivor Study. Blood 2008, 111, 5515–5523. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Delvecchio, M.; Muggeo, P.; Monteduro, M.; Lassandro, G.; Novielli, C.; Valente, F.; Salinaro, E.; Zito, A.; Ciccone, M.M.; Miniello, V.L.; et al. Non-alcoholic fatty liver disease is associated with early left ventricular dysfunction in childhood acute lymphoblastic leukaemia survivors. Eur. J. Endocrinol. 2017, 176, 111–121. [Google Scholar] [CrossRef]
- Giordano, P.; Muggeo, P.; Delvecchio, M.; Carbonara, S.; Romano, A.; Altomare, M.; Ricci, G.; Valente, F.; Zito, A.; Scicchitano, P.; et al. Endothelial dysfunction and cardiovascular risk factors in childhood acute lymphoblastic leukemia survivors. Int. J. Cardiol. 2017, 228, 621–627. [Google Scholar] [CrossRef] [PubMed]
- Muggeo, P.; Muggeo, V.M.R.; Giordano, P.; Delvecchio, M.; Altomare, M.; Novielli, C.; Ciccone, M.M.; D’Amato, G.; Faienza, M.F.; Santoro, N. Cardiovascular dysfunction and vitamin D status in childhood acute lymphoblastic leukemia survivors. World J. Pediatr. 2019, 15, 465–470. [Google Scholar] [CrossRef]
- Inaba, H.; Cao, X.; Han, A.Q.; Panetta, J.C.; Ness, K.K.; Metzger, M.L.; Rubnitz, J.E.; Ribeiro, R.C.; Sandlund, J.T.; Jeha, S.; et al. Bone mineral density in children with acute lymphoblastic leukemia. Cancer 2018, 124, 1025–1035. [Google Scholar] [CrossRef] [PubMed]
- Nadeau, G.; Samoilenko, M.; Fiscaletti, M.; Veilleux, L.N.; Curnier, D.; Laverdière, C.; Sinnett, D.; Krajinovic, M.; Lefebvre, G.; Alos, N. Predictors of low and very low bone mineral density in long-term childhood acute lymphoblastic leukemia survivors: Toward personalized risk prediction. Pediatr. Blood Cancer 2024, 71, e31047. [Google Scholar] [CrossRef] [PubMed]
- van Atteveld, J.E.; Mulder, R.L.; van den Heuvel-Eibrink, M.M.; Hudson, M.M.; Kremer, L.C.M.; Skinner, R.; Wallace, W.H.; Constine, L.S.; Higham, C.E.; Kaste, S.C.; et al. Bone mineral density surveillance for childhood, adolescent, and young adult cancer survivors: Evidence-based recommendations from the International Late Effects of Childhood Cancer Guideline Harmonization Group. Lancet Diabetes Endocrinol. 2021, 9, 622–637. [Google Scholar] [CrossRef]
- Frenkel, B.; White, W.; Tuckermann, J. Glucocorticoid-Induced Osteoporosis. Adv. Exp. Med. Biol. 2015, 872, 179–215. [Google Scholar] [PubMed]
- Faienza, M.F.; Luce, V.; Lonero, A.; Ventura, A.; Colaianni, G.; Colucci, S.; Cavallo, L.; Grano, M.; Brunetti, G. Treatment of osteoporosis in children with glucocorticoid-treated diseases. Expert. Rev. Endocrinol. Metab. 2014, 9, 525–534. [Google Scholar] [CrossRef] [PubMed]
- Urquiaga, M.; Saag, K.G. Risk for osteoporosis and fracture with glucocorticoids. Best. Pract. Res. Clin. Rheumatol. 2022, 36, 101793. [Google Scholar] [CrossRef] [PubMed]
- Kunstreich, M.; Kummer, S.; Laws, H.J.; Borkhardt, A.; Kuhlen, M. Osteonecrosis in children with acute lymphoblastic leukemia. Haematologica 2016, 101, 1295–1305. [Google Scholar] [CrossRef] [PubMed]
- Girard, P.; Auquier, P.; Barlogis, V.; Contet, A.; Poiree, M.; Demeocq, F.; Berbis, J.; Herrmann, I.; Villes, V.; Sirvent, N.; et al. Symptomatic osteonecrosis in childhood leukemia survivors: Prevalence, risk factors and impact on quality of life in adulthood. Haematologica 2013, 98, 1089–1097. [Google Scholar] [CrossRef]
- McAvoy, S.; Baker, K.S.; Mulrooney, D.; Blaes, A.; Arora, M.; Burns, L.J.; Majhail, N.S. Corticosteroid dose as a risk factor for avascular necrosis of the bone after hematopoietic cell transplantation. Biol. Blood Marrow Transplant. 2010, 16, 1231–1236. [Google Scholar] [CrossRef]
- van den Heuvel-Eibrink, M.M.; Pieters, R. Steroids and risk of osteonecrosis in ALL: Take a break. Lancet Oncol. 2012, 13, 855–857. [Google Scholar] [CrossRef]
- Larsen, E.C.; Devidas, M.; Chen, S.; Salzer, W.L.; Raetz, E.A.; Loh, M.L.; Mattano, L.A., Jr.; Cole, C.; Eicher, A.; Haugan, M.; et al. Dexamethasone and High-Dose Methotrexate Improve Outcome for Children and Young Adults with High-Risk B-Acute Lymphoblastic Leukemia: A Report from Children’s Oncology Group Study AALL0232. J. Clin. Oncol. 2016, 34, 2380–2388. [Google Scholar] [CrossRef]
- Maggioli, C.; Stagi, S. Bone modeling, remodeling, and skeletal health in children and adolescents: Mineral accrual, assessment and treatment. Ann. Pediatr. Endocrinol. Metab. 2017, 22, 1–5. [Google Scholar] [CrossRef]
- Orgel, E.; Mueske, N.M.; Wren, T.A.; Gilsanz, V.; Butturini, A.M.; Freyer, D.R.; Mittelman, S.D. Early injury to cortical and cancellous bone from induction chemotherapy for adolescents and young adults treated for acute lymphoblastic leukemia. Bone 2016, 85, 131–137. [Google Scholar] [CrossRef]
- Van Atteveld, J.E.; Pluijm, S.M.F.; Ness, K.K.; Hudson, M.M.; Chemaitilly, W.; Kaste, S.C.; Robison, L.L.; Neggers, S.J.C.M.M.; Yasui, Y.; van den Heuvel-Eibrink, M.M.; et al. Prediction of Low and Very Low Bone Mineral Density Among Adult Survivors of Childhood Cancer. J. Clin. Oncol. 2019, 37, 2217–2225. [Google Scholar] [CrossRef] [PubMed]
- Winkel, M.L.; Pieters, R.; Hop, W.C.; Roos, J.C.; Bokkerink, J.P.; Leeuw, J.A.; Bruin, M.C.; Kollen, W.J.; Veerman, A.J.; de Groot-Kruseman, H.A.; et al. Bone mineral density at diagnosis determines fracture rate in children with acute lymphoblastic leukemia treated according to the DCOG-ALL9 protocol. Bone 2014, 59, 223–228. [Google Scholar] [CrossRef]
- Cummings, E.A.; Ma, J.; Fernandez, C.V.; Halton, J.; Alos, N.; Miettunen, P.M.; Jaremko, J.L.; Ho, J.; Shenouda, N.; Matzinger, M.A.; et al. Incident vertebral fractures in children with leukemia during the four years following diagnosis. J. Clin. Endocrinol. Metab. 2015, 100, 3408–3417. [Google Scholar] [CrossRef]
- Rajakumar, S.A.; Papp, E.; Lee, K.K.; Grandal, I.; Merico, D.; Liu, C.C.; Allo, B.; Zhang, L.; Grynpas, M.D.; Minden, M.D.; et al. B cell acute lymphoblastic leukemia cells mediate RANK-RANKL-dependent bone destruction. Sci. Transl. Med. 2020, 12, eaba5942. [Google Scholar] [CrossRef] [PubMed]
- Cheung, L.C.; Tickner, J.; Hughes, A.M.; Skut, P.; Howlett, M.; Foley, B.; Oommen, J.; Wells, J.E.; He, B.; Singh, S.; et al. New therapeutic opportunities from dissecting the pre-B leukemia bone marrow microenvironment. Leukemia 2018, 32, 2326–2338. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Eriksen, E.F. Cellular mechanisms of bone remodeling. Rev. Endocr. Metab. Disord. 2010, 11, 219–227. [Google Scholar] [CrossRef]
- Theill, L.E.; Boyle, W.J.; Penninger, J.M. RANK-L and RANK: T cells, bone loss, and mammalian evolution. Annu. Rev. Immunol. 2002, 20, 795–823. [Google Scholar] [CrossRef]
- Krishnan, V.; Bryant, H.U.; Mac Dougald, O.A. Regulation of bone mass by Wnt signaling. J. Clin. Investig. 2006, 116, 1202–1209. [Google Scholar] [CrossRef]
- Brunetti, G.; D’Amato, G.; Chiarito, M.; Tullo, A.; Colaianni, G.; Colucci, S.; Grano, M.; Faienza, M.F. An update on the role of RANKL-RANK/osteoprotegerin and WNT-ß-catenin signaling pathways in pediatric diseases. World J. Pediatr. 2019, 15, 4–11. [Google Scholar] [CrossRef]
- D’Amato, G.; Brescia, V.; Fontana, A.; Natale, M.P.; Lovero, R.; Varraso, L.; Di Serio, F.; Simonetti, S.; Muggeo, P.; Faienza, M.F. Biomarkers and Biochemical Indicators to Evaluate Bone Metabolism in Preterm Neonates. Biomedicines 2024, 12, 1271. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Brescia, V.; Lovero, R.; Fontana, A.; Zerlotin, R.; Colucci, S.C.; Grano, M.; Cazzolla, A.P.; Di Serio, F.; Crincoli, V.; Faienza, M.F. Reference Intervals (RIs) of the Bone Turnover Markers (BTMs) in Children and Adolescents: A Proposal for Effective Use. Biomedicines 2024, 13, 34. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gupta, V.; Dash, S.; Aggarwal, P.; Singh, S.K. Alterations in Bone Turnover during Chemotherapy in Children with Acute Lymphoblastic Leukemia. S. Asian J. Cancer 2021, 10, 183–186. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Boot, A.M.; van den Heuvel-Eibrink, M.M.; Hählen, K.; Krenning, E.P.; de Muinck Keizer-Schrama, S.M. Bone mineral density in children with acute lymphoblastic leukaemia. Eur. J. Cancer 1999, 35, 1693–1697. [Google Scholar] [CrossRef] [PubMed]
- Muggeo, P.; Grassi, M.; D’Ascanio, V.; Brescia, V.; Fontana, A.; Piacente, L.; Di Serio, F.; Giordano, P.; Faienza, M.F.; Santoro, N. Bone Remodeling Markers in Children with Acute Lymphoblastic Leukemia after Intensive Chemotherapy: The Screenshot of a Biochemical Signature. Cancers 2023, 15, 2554. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chiarito, M.; Brunetti, G.; D’Amato, G.; Faienza, M.F. Monitoring and maintaining bone health in patients with Turner syndrome. Expert. Rev. Endocrinol. Metab. 2020, 15, 431–438. [Google Scholar] [CrossRef] [PubMed]
- Atilano-Miguel, S.; Barbosa-Cortés, L.; Ortiz-Muñiz, R.; Maldonado-Hernández, J.; Martin-Trejo, J.A.; Rodríguez-Cruz, M.; Balcázar-Hernández, L.; Solís-Labastida, K.A.; Bautista-Martínez, B.A.; Juárez-Moya, A.; et al. Changes in RANKL, OPG, and 25(OH)D Levels in Children with Leukemia from Diagnosis to Remission. Cancers 2024, 16, 2811. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ward, L.M. Glucocorticoid-Induced Osteoporosis: Why Kids Are Different. Front. Endocrinol. 2020, 11, 576. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ma, J.; Siminoski, K.; Jaremko, J.L.; Koujok, K.; Matzinger, M.A.; Shenouda, N.; Wilson, N.; Cheng, M.; Alos, N.; Atkinson, S.; et al. Vertebral Body Reshaping after Fractures: An Important Index of Recovery in Glucocorticoid-Treated Children. J. Clin. Endocrinol. Metab. 2024, 109, e1225–e1237. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Todor, S.B.; Ichim, C. Microbiome Modulation in Pediatric Leukemia: Impact on Graft-Versus-Host Disease and Treatment Outcomes: A Narrative Review. Children 2025, 12, 166. [Google Scholar] [CrossRef]
- Conter, V.; Bartram, C.R.; Valsecchi, M.G.; Schrauder, A.; Panzer-Grümayer, R.; Möricke, A.; Aricò, M.; Zimmermann, M.; Mann, G.; De Rossi, G.; et al. Molecular response to treatment redefines all prognostic factors in children and adolescents with B-cell precursor acute lymphoblastic leukemia: Results in 3184 patients of the AIEOP-BFM ALL 2000 study. Blood 2010, 115, 3206–3214. [Google Scholar] [CrossRef]
- Cacciari, E.; Milani, S.; Balsamo, A.; Spada, E.; Bona, G.; Cavallo, L.; Cerutti, F.; Gargantini, L.; Greggio, N.; Tonini, G.; et al. Italian cross-sectional growth charts for height, weight and BMI (2 to 20 yr). J. Endocrinol. Investig. 2006, 29, 581–593. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Patients (n = 22) | |
|---|---|
| Gender (male/female) | 12/10 |
| Age at diagnosis—years | 5.5 ± 3.6 |
| Height (SDS) | −0.75 ± 1.26 |
| Weight (SDS) | −0.14 ± 1.18 |
| BMI (SDS) | 0.49 ± 0.91 |
| Acute Lymphoblastic Leukemia phenotype: | |
| B-lineage | 19 |
| T-lineage | 2 |
| B-lineage t (9; 22) | 1 |
| Risk group: | |
| Standard risk | 8 |
| Intermediate risk | 13 |
| High risk | 1 |
| Bone pain yes/no | 5/22 |
| Marker | T0 | T1 | T2 | T3 | T4 | p-Value |
|---|---|---|---|---|---|---|
| CTX-I (ng/mL) | 1.0 ± 0.5 a | 2.4 ± 0.6 b | 2.2 ± 0.7 bc | 2.5 ± 0.9 b | 1.7 ± 0.6 c | 1 <0.001 |
| OC (ng/mL) | 23.6 (17.1 ÷ 28.2) a | 100.0 (84.6 ÷ 103.0) b | 95.9 (71.4 ÷ 127.9) b | 122.5 (97.4 ÷ 143.0) b | 104.7 (79.8 ÷ 121.4) b | 2 <0.001 |
| P1NP (ng/mL) | 193.0 (117.7 ÷ 273.0) a | 749.0 (634.0 ÷ 920.0) b | 728.4 (606.3 ÷ 920.0) b | 920.0 (812.2 ÷ 1050.2) b | 753.9 (640.0 ÷ 860.7) b | 2 <0.001 |
| bALP (µg/L) | 26.7 (21.4 ÷ 32.3) a | 55.7 (48.0 ÷ 56.0) b | 62.2 (55.2 ÷ 76.4) bc | 67.6 (51.9 ÷ 71.3) b | 83.5 (67.8 ÷ 119.7) c | 2 <0.001 |
| TRAcP5b (U/L) | 10.0 (7.6 ÷ 13.0) a | 12.9 (10.5 ÷ 13.0) ab | 13.9 (11.0 ÷ 18.7) abc | 18.2 (12.6 ÷ 21.5) bc | 18.0 (13.0 ÷ 22.2) c | 2 <0.001 |
| 25-OH-Vit D | 25.5 (19.0 ÷ 35.3) a | 15.0 (11.5 ÷ 19.3) b | 15.0 (10.0 ÷ 21.0) b | 12.0 (7.0 ÷ 16.3) b | 27.0 (20.8 ÷ 32.3) a | 2 <0.001 |
| RANKL(pmol/L) | 4302 (1312 ÷ 20,336) a | 5859 (1315 ÷ 8383) a | 3264 (562 ÷ 13,859) a | 1601 (843 ÷ 13,014) a | 2010 (86 ÷ 24600) a | 2 0.220 |
| OPG (pmol/L) | 4.4 (2.9 ÷ 7.5) ab | 3.8 (3.5 ÷ 4.1) b | 3.1 (2.7 ÷ 3.9) c | 3.4 (2.8 ÷ 4.2) bc | 5.1 (4.0 ÷ 6.3) a | 2 <0.001 |
| RANKL/OPG ratio | 920 (311 ÷ 2839) a | 1469 (263 ÷ 2212) a | 882 (161 ÷ 3873) a | 620 (178 ÷ 4089) a | 365 (15 ÷ 3756) a | 2 0.567 |
| PTH (pg/mL) | 18.0 (8.0 ÷ 29.3) a | 40.0 (32.8 ÷ 42.5) ab | 46.0 (36.5 ÷ 52.5) b | 55.0 (39.0 ÷ 70.5) b | 32.5 (21.0 ÷ 35.5) a | 2 <0.001 |
| DKK-1 (pg/mL) | 2266 (1362 ÷ 4902) a | 4724 (3416 ÷ 5752) ab | 4016 (2752 ÷ 4814) a | 6180 (4564 ÷ 8405) b | 3346 (2765 ÷ 4191) a | 2 <0.001 |
| Sclerostin (pmol/L) | 14.9 (13.9 ÷ 18.3) a | 17.6 (15.7 ÷ 19.9) a | 16.7 (15.3 ÷ 22.3) a | 19.0 (13.9 ÷ 23.2) a | 18.5 (16.6 ÷ 20.6) a | 2 0.162 |
| Calcium (mg/dL) | 9.1 (8.6 ÷ 9.4) a | 9.4 (8.8 ÷ 9.5) ab | 9.1 (8.8 ÷ 9.7) ab | 9.3 (8.8 ÷ 9.4) a | 9.8 (9.4 ÷ 10.1)b | 2 0.021 |
| Phosphorus (mg/dL) | 5.2 (4.4 ÷ 5.6) a | 5.0 (4.7 ÷ 5.1) a | 5.0 (4.8 ÷ 5.2) a | 5.0 (4.5 ÷ 5.3) a | 4.9 (4.1 ÷ 5.1) a | 2 0.517 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muggeo, P.; Grassi, M.; D’Ascanio, V.; Forte, J.; Brescia, V.; Di Serio, F.; Piacente, L.; Giordano, P.; Santoro, N.; Faienza, M.F. Bone Remodeling in Children with Acute Lymphoblastic Leukemia: A Two-Year Prospective Longitudinal Study. Int. J. Mol. Sci. 2025, 26, 4307. https://doi.org/10.3390/ijms26094307
Muggeo P, Grassi M, D’Ascanio V, Forte J, Brescia V, Di Serio F, Piacente L, Giordano P, Santoro N, Faienza MF. Bone Remodeling in Children with Acute Lymphoblastic Leukemia: A Two-Year Prospective Longitudinal Study. International Journal of Molecular Sciences. 2025; 26(9):4307. https://doi.org/10.3390/ijms26094307
Chicago/Turabian StyleMuggeo, Paola, Massimo Grassi, Vito D’Ascanio, Jessica Forte, Vincenzo Brescia, Francesca Di Serio, Laura Piacente, Paola Giordano, Nicola Santoro, and Maria Felicia Faienza. 2025. "Bone Remodeling in Children with Acute Lymphoblastic Leukemia: A Two-Year Prospective Longitudinal Study" International Journal of Molecular Sciences 26, no. 9: 4307. https://doi.org/10.3390/ijms26094307
APA StyleMuggeo, P., Grassi, M., D’Ascanio, V., Forte, J., Brescia, V., Di Serio, F., Piacente, L., Giordano, P., Santoro, N., & Faienza, M. F. (2025). Bone Remodeling in Children with Acute Lymphoblastic Leukemia: A Two-Year Prospective Longitudinal Study. International Journal of Molecular Sciences, 26(9), 4307. https://doi.org/10.3390/ijms26094307