
Bacterial Volatile Organic Compounds as Potential Caries and Periodontitis Disease Biomarkers

 ,
,  , and
, and
Abstract
1. Introduction
2. Results
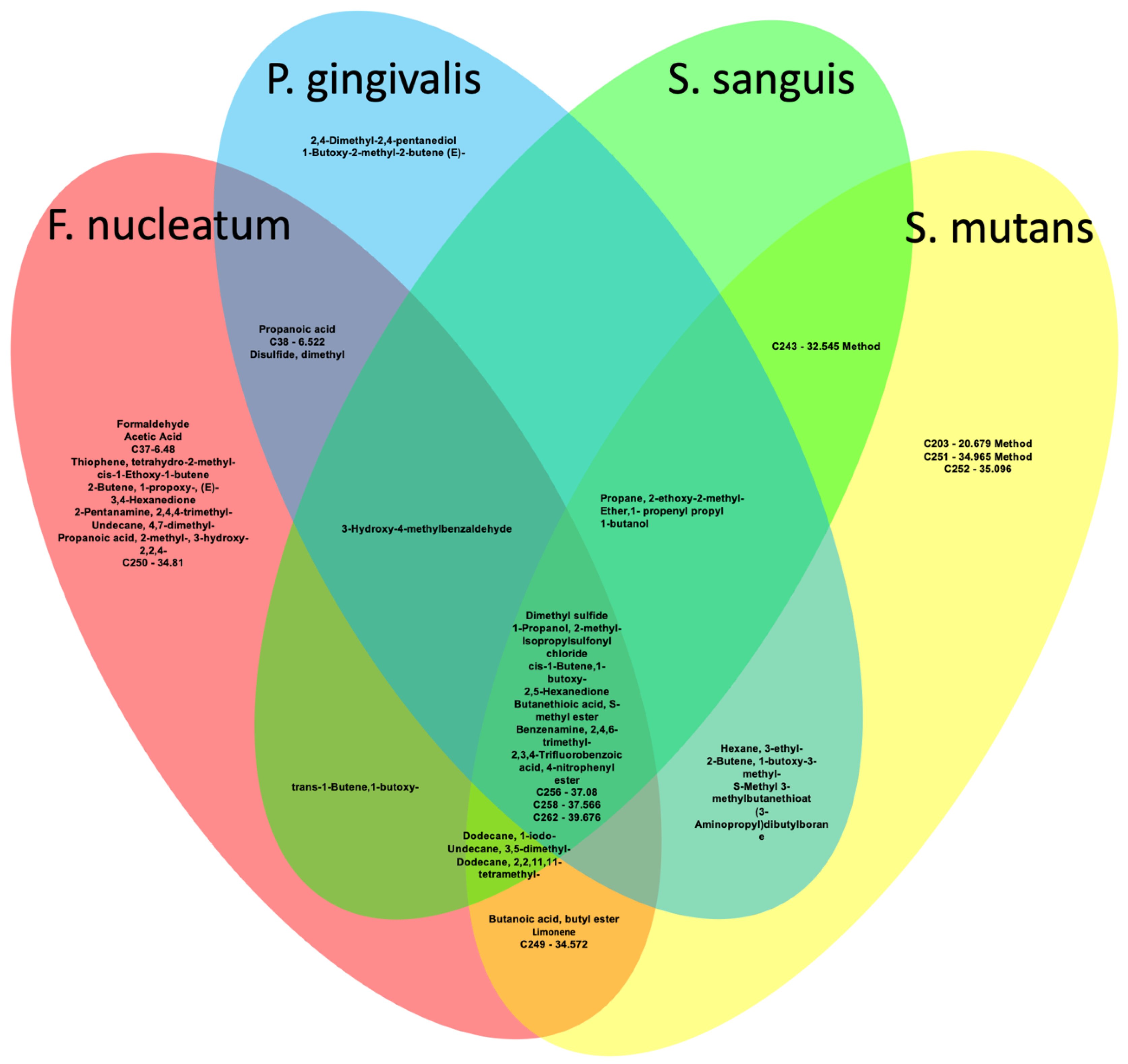
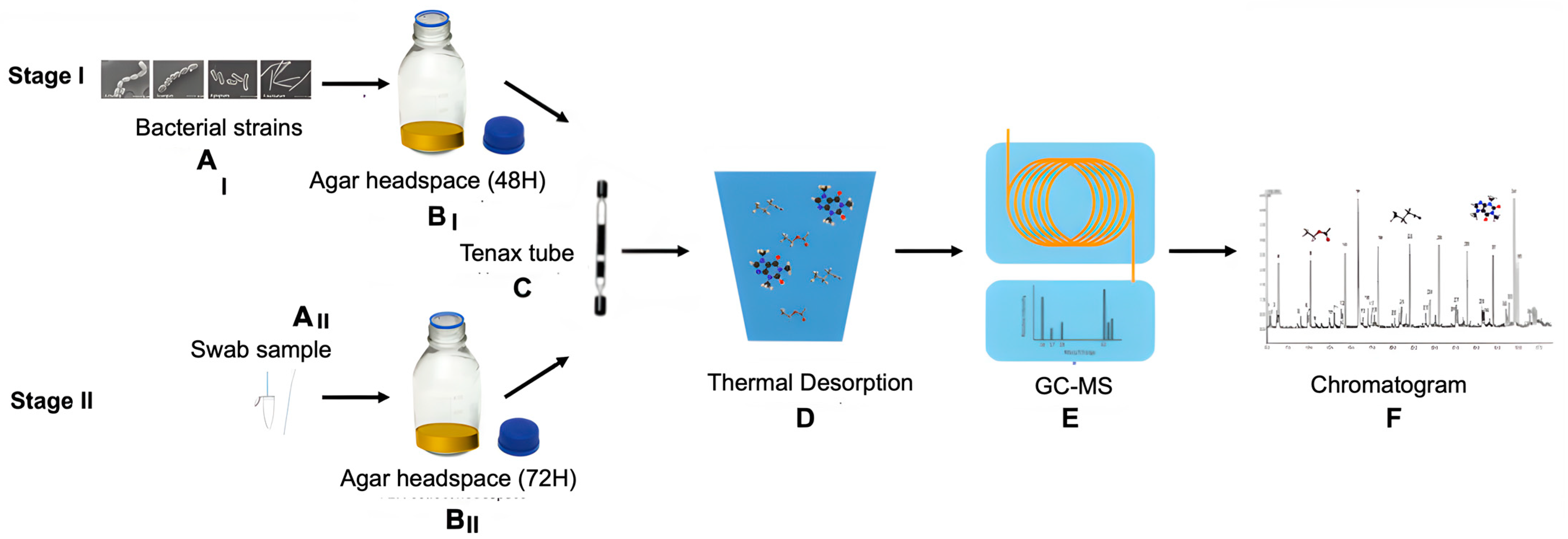
2.1. Stage I
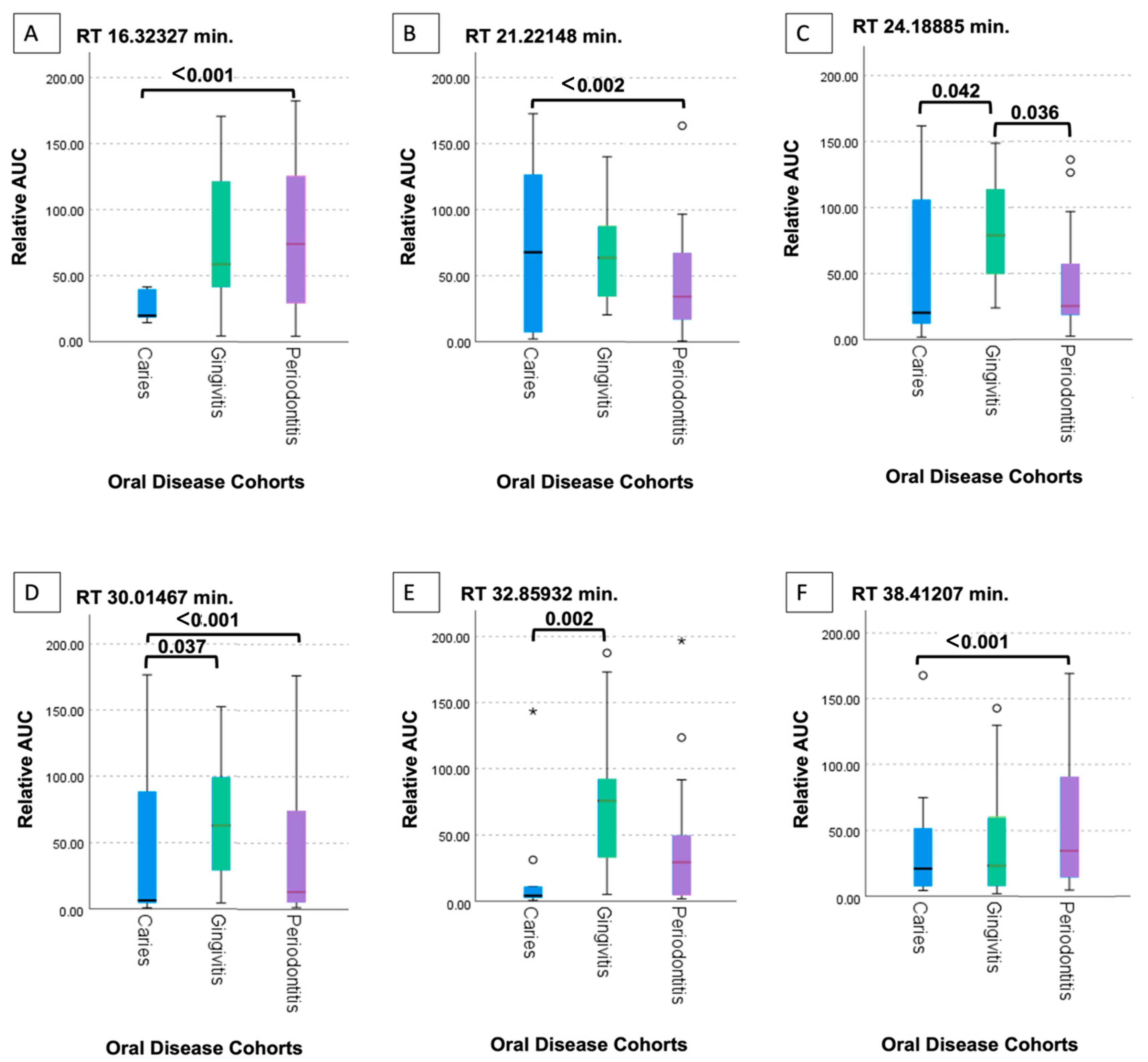
2.2. Stage II
3. Discussion
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ANOVA | Analysis of Variance |
| ATCC | American Type Culture Collection |
| BHI | Brain Heart Infusion |
| CEET | Collaboration for Environmental Evidence Tool |
| CF | Cystic Fibrosis |
| COPD | Chronic Obstructive Pulmonary Disease |
| DMDS | Dimethyl Disulfide |
| FadA | Fusobacterium adhesionA |
| GC-MS | Gas Chromatography-Mass Spectrometry |
| HbA1c | Hemoglobin A1c |
| HNSCC | Head and Neck Squamous Cell Carcinoma |
| ICDAS | International Caries Detection and Assessment System |
| ICMJE | International Committee of Medical Journal Editors |
| IRB | Institutional Review Board |
| LNBD | Laboratory for Nanomaterial-Based Devices |
| LSD | Least Significant Difference |
| m/z | Mass-to-Charge Ratio |
| NIST | National Institute of Standards and Technology |
| PBS | Phosphate-Buffered Saline |
| ppb | Parts per Billion |
| ppt | Parts per Trillion |
| PTR-TOF-MS | Proton Transfer Reaction-Time of Flight-Mass Spectrometry |
| SAS | Statistical Analysis System |
| SCFA | Short-Chain Fatty Acid |
| SPSS | Statistical Package for the Social Sciences |
| TD | Thermal Desorption |
| VOC | Volatile Organic Compound |
References
- Peres, M.A.; Macpherson, L.M.D.; Weyant, R.J.; Daly, B.; Venturelli, R.; Mathur, M.R.; Listl, S.; Celeste, R.K.; Guarnizo-Herreño, C.C.; Kearns, C.; et al. Oral diseases: A global public health challenge. Lancet 2019, 394, 249–260. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Oral Health Status Report: Towards Universal Health Coverage for Oral Health by 2030; World Health Organization: Geneva, Switzerland, 2022. Available online: https://www.who.int/publications/i/item/9789240061484 (accessed on 12 May 2023).
- Marsh, P.D. Microbial ecology of dental plaque and its significance in health and disease. Adv. Dent. Res. 1994, 8, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Marsh, P.D. Are dental diseases examples of ecological catastrophes? Microbiology 2003, 149, 279–294. [Google Scholar] [CrossRef]
- Kleinberg, I. A mixed-bacteria ecological approach to understanding the role of the oral bacteria in dental caries causation: An alternative to Streptococcus mutans and the specific-plaque hypothesis. Crit. Rev. Oral Biol. Med. 2002, 13, 108–125. [Google Scholar] [CrossRef]
- Takahashi, N.; Nyvad, B. Caries ecology revisited: Microbial dynamics and the caries process. Caries Res. 2008, 42, 409–418. [Google Scholar] [CrossRef]
- Nyvad, B.; Kilian, M. Microbiology of the early colonization of human enamel and root surfaces in vivo. Scand. J. Dent. Res. 1987, 95, 369–380. [Google Scholar] [CrossRef] [PubMed]
- Hamada, S.; Slade, H.D. Biology, immunology, and cariogenicity of Streptococcus mutans. Microbiol. Rev. 1980, 44, 331–384. [Google Scholar] [CrossRef]
- Loesche, W.J. Role of Streptococcus mutans in human dental decay. Microbiol. Rev. 1986, 50, 353–380. [Google Scholar] [CrossRef]
- Balakrishnan, M.; Simmonds, R.S.; Tagg, J.R. Dental caries is a preventable infectious disease. Aust. Dent. J. 2000, 45, 235–245. [Google Scholar] [CrossRef]
- Patini, R.; Staderini, E.; Lajolo, C.; Lopetuso, L.; Mohammed, H.; Rimondini, L.; Rocchetti, V.; Franceschi, F.; Cordaro, M.; Gallenzi, P. Relationship between oral microbiota and periodontal disease: A systematic review. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 5775–5788. [Google Scholar] [CrossRef]
- de Andrade, K.Q.; Almeida-da-Silva, C.L.C.; Coutinho-Silva, R. Immunological pathways triggered by Porphyromonas gingivalis and Fusobacterium nucleatum: Therapeutic possibilities? Mediat. Inflamm. 2019, 2019, 7241312. [Google Scholar] [CrossRef] [PubMed]
- Holt, S.C.; Ebersole, J.L. Porphyromonas gingivalis, Treponema denticola, and Tannerella forsythia: The “red complex”, a prototype polybacterial pathogenic consortium in periodontitis. Periodontol. 2000 2005, 38, 72–122. [Google Scholar] [CrossRef] [PubMed]
- Armitage, G.C. Periodontal diagnoses and classification of periodontal diseases. Periodontol. 2000 2004, 34, 9–21. [Google Scholar] [CrossRef]
- Baker, J.L.; Edlund, A. Exploiting the oral microbiome to prevent tooth decay: Has evolution already provided the best tools? Front. Microbiol. 2019, 9, 3323. [Google Scholar] [CrossRef] [PubMed]
- Sedghi, L.M.; Bacino, M.; Kapila, Y.L. Periodontal disease: The good, the bad, and the unknown. Front. Cell. Infect. Microbiol. 2021, 11, 766944. [Google Scholar] [CrossRef]
- Thorn, R.M.; Greenman, J. Microbial volatile compounds in health and disease conditions. J. Breath Res. 2012, 6, 024001. [Google Scholar] [CrossRef]
- Broza, Y.Y.; Zhou, X.; Yuan, M.; Qu, D.; Zheng, Y.; Vishinkin, R.; Khatib, M.; Wu, W.; Haick, H. Disease detection with molecular biomarkers: From chemistry of body fluids to nature-inspired chemical sensors. Chem. Rev. 2019, 119, 11761–11817. [Google Scholar] [CrossRef]
- Nakhleh, M.K.; Amal, H.; Jeries, R.; Broza, Y.Y.; Aboud, M.; Gharra, A.; Ivgi, H.; Khatib, S.; Badarneh, S.; Har-Shai, L.; et al. Diagnosis and classification of 17 diseases from 1404 subjects via pattern analysis of exhaled molecules. ACS Nano 2017, 11, 112–125. [Google Scholar] [CrossRef]
- Schulz, S.; Dickschat, J.S. Bacterial volatiles: The smell of small organisms. Nat. Prod. Rep. 2007, 24, 814–842. [Google Scholar] [CrossRef]
- Broza, Y.Y.; Haick, H. Nanomaterial-based sensors for detection of disease by volatile organic compounds. Nanomedicine 2013, 8, 785–806. [Google Scholar] [CrossRef]
- Netzker, T.; Shepherdson, E.M.F.; Zambri, M.P.; Elliot, M.A. Bacterial Volatile Compounds: Functions in Communication, Cooperation, and Competition. Annu. Rev. Microbiol. 2020, 74, 409–430. [Google Scholar] [CrossRef]
- Hu, W.; Wu, W.; Jian, Y.; Haick, H.; Zhang, G.; Qian, Y.; Yuan, M.; Yao, M. Volatolomics in healthcare and its advanced detection technology. Nano Res. 2022, 15, 8185–8213. [Google Scholar] [CrossRef] [PubMed]
- Serasanambati, M.; Broza, Y.Y.; Haick, H. Volatile Compounds Are Involved in Cellular Crosstalk and Upregulation. Adv. Biosyst. 2019, 3, e1900131. [Google Scholar] [CrossRef]
- Yaegaki, K.; Sanada, K. Volatile sulfur compounds in mouth air from clinically healthy subjects and patients with periodontal disease. J. Periodontal Res. 1992, 27, 233–238. [Google Scholar] [CrossRef] [PubMed]
- Phillips, M.; Herrera, J.; Krishnan, S.; Zain, M.; Greenberg, J.; Cataneo, R.N. Variation in volatile organic compounds in the breath of normal humans. J. Chromatogr. B Biomed. Sci. Appl. 1999, 729, 75–88. [Google Scholar] [CrossRef] [PubMed]
- Phillips, M.; Cataneo, R.N.; Greenberg, J.; Munawar, M.; Nachnani, S.; Samtani, S. Pilot study of a breath test for volatile organic compounds associated with oral malodor: Evidence for the role of oxidative stress. Oral Diseases 2005, 11 (Suppl. 1), 32–34. [Google Scholar] [CrossRef]
- van den Velde, S.; Quirynen, M.; van Hee, P.; van Steenberghe, D. Halitosis-associated volatiles in breath of healthy subjects. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2007, 853, 54–61. [Google Scholar] [CrossRef]
- Haraszthy, V.I.; Zambon, J.J.; Sreenivasan, P.K.; Zambon, M.M.; Gerber, D.; Rego, R.; Parker, C. Identification of oral bacterial species associated with halitosis. J. Am. Dent. Assoc. 2007, 138, 1113–1120. [Google Scholar] [CrossRef]
- Van den Velde, S.; van Steenberghe, D.; Van Hee, P.; Quirynen, M. Detection of odorous compounds in breath. J. Dent. Res. 2009, 88, 285–289. [Google Scholar] [CrossRef]
- Tangerman, A.; Winkel, E.G. Volatile Sulfur Compounds as the Cause of Bad Breath: A Review. Phosphorus Sulfur Silicon Relat. Elem. 2013, 188, 396–402. [Google Scholar] [CrossRef]
- Khalid, T.Y.; Saad, S.; Greenman, J.; de Lacy Costello, B.; Probert, C.S.; Ratcliffe, N.M. Volatiles from oral anaerobes confounding breath biomarker discovery. J. Breath Res. 2013, 7, 017114. [Google Scholar] [CrossRef] [PubMed]
- Nakhleh, M.K.; Quatredeniers, M.; Haick, H. Detection of halitosis in breath: Between the past, present, and future. Oral Dis. 2018, 24, 685–695. [Google Scholar] [CrossRef] [PubMed]
- Roslund, K.; Uosukainen, M.; Järvik, K.; Hartonen, K.; Lehto, M.; Pussinen, P.; Groop, P.H.; Metsälä, M. Antibiotic treatment and supplemental hemin availability affect the volatile organic compounds produced by P. gingivalis in vitro. Sci. Rep. 2022, 12, 22534. [Google Scholar] [CrossRef]
- Hertel, M.; Preissner, R.; Gillissen, B.; Schmidt-Westhausen, A.M.; Paris, S.; Preissner, S. Detection of signature volatiles for cariogenic microorganisms. Eur. J. Clin. Microbiol. Infect. Dis. 2016, 35, 235–244. [Google Scholar] [CrossRef] [PubMed]
- Hertel, M.; Schuette, E.; Kastner, I.; Hartwig, S.; Schmidt-Westhausen, A.M.; Preissner, R.; Paris, S.; Preissner, S. Volatile organic compounds in the breath of oral candidiasis patients: A pilot study. Clin. Oral Investig. 2018, 22, 721–731. [Google Scholar] [CrossRef]
- Roslund, K.; Lehto, M.; Pussinen, P.; Groop, P.H.; Halonen, L.; Metsälä, M. On-line profiling of volatile compounds produced in vitro by pathogenic oral bacteria. J. Breath Res. 2019, 14, 016010. [Google Scholar] [CrossRef]
- Mäkitie, A.A.; Almangush, A.; Youssef, O.; Metsälä, M.; Silén, S.; Nixon, I.J.; Haigentz, M., Jr.; Rodrigo, J.P.; Saba, N.F.; Vander Poorten, V.; et al. Exhaled breath analysis in the diagnosis of head and neck cancer. Head Neck 2020, 42, 787–793. [Google Scholar] [CrossRef]
- Mentel, S.; Gallo, K.; Wagendorf, O.; Preissner, R.; Nahles, S.; Heiland, M.; Preissner, S. Prediction of oral squamous cell carcinoma based on machine learning of breath samples: A prospective controlled study. BMC Oral Health 2021, 21, 500. [Google Scholar] [CrossRef]
- Roslund, K.; Lehto, M.; Pussinen, P.; Hartonen, K.; Groop, P.H.; Halonen, L.; Metsälä, M. Identifying volatile in vitro biomarkers for oral bacteria with proton-transfer-reaction mass spectrometry and gas chromatography-mass spectrometry. Sci. Rep. 2021, 11, 16897. [Google Scholar] [CrossRef]
- Hefti, A.F.; Preshaw, P.M. Examiner alignment and assessment in clinical periodontal research. Periodontol. 2000 2012, 59, 41–60. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Sanz, M. Implementation of the new classification of periodontal diseases: Decision-making algorithms for clinical practice and education. J. Clin. Periodontol. 2019, 46, 398–405. [Google Scholar] [CrossRef] [PubMed]
- National Center for Biotechnology Information. PubChem Compound Summary for CID 6433417, 2-Methyl-2-buten-1-OL. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/2-Methyl-2-buten-1-OL (accessed on 19 December 2023).
- Magrin, G.L.; Strauss, F.J.; Benfatti, C.A.M.; Maia, L.C.; Gruber, R. Effects of short-chain fatty acids on human oral epithelial cells and the potential impact on periodontal disease: A systematic review of in vitro studies. Int. J. Mol. Sci. 2020, 21, 4895. [Google Scholar] [CrossRef] [PubMed]
- National Center for Biotechnology Information. PubChem Compound Summary for CID 141153, 2,4-Dimethyl-2,4-pentanediol. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/141153 (accessed on 19 December 2023).
- Dharmawardana, N.; Goddard, T.; Woods, C.; Watson, D.I.; Ooi, E.H.; Yazbeck, R. Development of a non-invasive exhaled breath test for the diagnosis of head and neck cancer. Br. J. Cancer 2020, 123, 1775–1781. [Google Scholar] [CrossRef]
- Wehinger, A.; Schmid, A.; Mechtcheriakov, S.; Ledochowski, M.; Grabmer, C.; Gastl, G.A.; Amann, A. Lung cancer detection by proton transfer reaction mass-spectrometric analysis of human breath gas. Int. J. Mass Spectrom. 2007, 265, 49–59. [Google Scholar] [CrossRef]
- Anesti, V.; McDonald, I.R.; Ramaswamy, M.; Wade, W.G.; Kelly, D.P.; Wood, A.P. Isolation and molecular detection of methylotrophic bacteria occurring in the human mouth. Environ. Microbiol. 2005, 7, 1227–1238. [Google Scholar] [CrossRef]
- Pitts, N. “ICDAS”—An international system for caries detection and assessment being developed to facilitate caries epidemiology, research, and appropriate clinical management. Community Dent. Health 2004, 21, 193–198. [Google Scholar]
- Burgos-Barragan, G.; Wit, N.; Meiser, J.; Dingler, F.A.; Pietzke, M.; Mulderrig, L.; Pontel, L.B.; Rosado, I.V.; Brewer, T.F.; Cordell, R.L.; et al. Mammals divert endogenous genotoxic formaldehyde into one-carbon metabolism. Nature 2017, 548, 549–554. [Google Scholar] [CrossRef]
- Pietzke, M.; Meiser, J.; Vazquez, A. Formate metabolism in health and disease. Mol. Metab. 2019, 33, 23–27. [Google Scholar] [CrossRef]
- Ratcliff, P.A.; Johnson, P.W. The relationship between oral malodor, gingivitis, and periodontitis: A review. J. Periodontol. 1999, 70, 485–489. [Google Scholar] [CrossRef]
- Takahashi, N.; Saito, K.; Schachtele, C.F.; Yamada, T. Acid tolerance and acid-neutralizing activity of Porphyromonas gingivalis, Prevotella intermedia and Fusobacterium nucleatum. Oral Microbiol. Immunol. 1997, 12, 323–328. [Google Scholar] [CrossRef] [PubMed]
- Attene-Ramos, M.S.; Wagner, E.D.; Plewa, M.J.; Gaskins, H.R. Evidence that hydrogen sulfide is a genotoxic agent. Mol. Cancer Res. 2006, 4, 9–14. [Google Scholar] [CrossRef]
- Karpiński, T.M. Role of Oral Microbiota in Cancer Development. Microorganisms 2019, 7, 20. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Shahir, A.M.; Sha, J.; Feng, Z.; Eapen, B.; Nithianantham, S.; Das, B.; Karn, J.; Weinberg, A.; Bissada, N.F.; et al. Short-chain fatty acids from periodontal pathogens suppress histone deacetylases, EZH2, and SUV39H1 to promote Kaposi’s sarcoma-associated herpesvirus replication. J. Virol. 2014, 88, 4466–4479. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Zhu, Y.; Li, X.; Sun, B. Dynamic balancing of intestinal short-chain fatty acids: The crucial role of bacterial metabolism. Trends Food Sci. Technol. 2020, 100, 118–130. [Google Scholar] [CrossRef]
- Leonov, G.E.; Varaeva, Y.R.; Livantsova, E.N.; Starodubova, A.V. The complicated relationship of short-chain fatty acids and oral microbiome: A narrative review. Biomedicines 2023, 11, 2749. [Google Scholar] [CrossRef]
- Po, H.N.; Senozan, N.M. The Henderson-Hasselbalch equation: Its history and limitations. J. Chem. Educ. 2001, 78, 1499. [Google Scholar] [CrossRef]
- Woolfenden, E. Monitoring VOCs in Air Using Sorbent Tubes Followed by Thermal Desorption-Capillary GC Analysis: Summary of Data and Practical Guidelines. J. Air Waste Manag. Assoc. 1997, 47, 20–36. [Google Scholar] [CrossRef]
- Blom, D.; Fabbri, C.; Connor, E.C.; Schiestl, F.P.; Klauser, D.R.; Boller, T.; Eberl, L.; Weisskopf, L. Production of plant growth modulating volatiles is widespread among rhizosphere bacteria and strongly depends on culture conditions. Environ. Microbiol. 2011, 13, 3047–3058. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Chemical Class | Compound | F. nucleatum (34 Molecules) | P. gingivalis (24 Molecules) | S. mutans (28 Molecules) | S. sanguis (21 Molecules) |
|---|---|---|---|---|---|
| Aldehyde | Formaldehyde | 1 | |||
| Carboxylic Acid | Propanoic acid | 1 | 1 | ||
| Sulfur Compound | Dimethyl sulfide | 1 | 1 | 1 | 1 |
| Ether | Propane, 2-ethoxy-2-methyl- | 1 | 1 | 1 | |
| Carboxylic Acid | Acetic Acid | 1 | |||
| C37—6.48 | 1 | ||||
| C38—6.522 | 1 | 1 | |||
| Alcohol | 1-Propanol, 2-methyl- | 1 | 1 | 1 | 1 |
| Sulfur Compound | Thiophene, tetrahydro-2-methyl- | 1 | |||
| Ether | Ether,1-propenyl propyl | 1 | 1 | 1 | |
| Ether | cis-1-Ethoxy-1-butene | 1 | |||
| Sulfonyl Chloride | Isopropylsulfonyl chloride | 1 | 1 | 1 | 1 |
| Alcohol | 1-butanol | 1 | 1 | 1 | |
| Diol | 2,4-Dimethyl-2,4-pentanediol | 1 | |||
| Hydrocarbon | 2-Butene, 1-propoxy-, (E)- | 1 | |||
| Ketone | 3,4-Hexanedione | 1 | |||
| Sulfur Compound | Disulfide, dimethyl | 1 | 1 | ||
| Amine | 2-Pentanamine, 2,4,4-trimethyl- | 1 | |||
| Hydrocarbon | Hexane, 3-ethyl- | 1 | 1 | ||
| Hydrocarbon | trans-1-Butene,1-butoxy- | 1 | 1 | ||
| Hydrocarbon | cis-1-Butene,1-butoxy- | 1 | 1 | 1 | 1 |
| Ketones | 2,5-Hexanedione | 1 | 1 | 1 | 1 |
| Sulfur Compound | Butanethioic acid, S-methyl ester | 1 | 1 | 1 | 1 |
| Ether | trans-1-Butene,1-butoxy- | 1 | 1 | ||
| Hydrocarbon | 2-Butene, 1-butoxy-3-methyl- | 1 | 1 | ||
| Thioester | S-Methyl 3-methylbutanethioat | 1 | 1 | ||
| Boran Derivative | (3-Aminopropyl)dibutylborane | 1 | 1 | ||
| Hydrocarbon | 1-Butoxy-2-methyl-2-butene (E)- | 1 | |||
| Ester | Butanoic acid, butyl ester | 1 | 1 | ||
| Terpene | Limonene | 1 | 1 | ||
| Aldehyde | 3-Hydroxy-4-methylbenzaldehyde | 1 | 1 | 1 | |
| Amine | Benzenamine, 2,4,6-trimethyl- | 1 | 1 | 1 | 1 |
| Hydrocarbon | Undecane, 4,7-dimethyl- | 1 | |||
| Hydrocarbon | Dodecane, 1-iodo- | 1 | 1 | 1 | |
| Hydrocarbon | Undecane, 3,5-dimethyl- | 1 | 1 | 1 | |
| Hydrocarbon | Dodecane, 2,2,11,11-tetramethyl- | 1 | 1 | 1 | |
| Carboxylic Acid | Propanoic acid, 2-methyl-, 3-hydroxy-2,2,4- | 1 | |||
| C203—20.679 Method | 1 | ||||
| Carboxylic Acid | 2,3,4-Trifluorobenzoic acid, 4-nitrophenyl ester | 1 | 1 | 1 | 1 |
| C243—32.545 Method | 1 | 1 | |||
| C249—34.572 | 1 | 1 | |||
| C250—34.81 | 1 | ||||
| C251—34.965 Method | 1 | ||||
| C252—35.096 | 1 | ||||
| C256—37.08 | 1 | 1 | 1 | 1 | |
| C258—37.566 | 1 | 1 | 1 | 1 | |
| C262—39.676 | 1 | 1 | 1 | 1 |
| RT | Caries Median [N] | Gingivitis Median [N] | Periodontitis Median [N] | KW Statistics Median [N] | KW p | MW p Caries-Periodontitis | MW p Caries-Gingivitis | MW p Periodontitis-Gingivitis |
|---|---|---|---|---|---|---|---|---|
| 16.32 | 19.64 [6] | 58.60 [17] | 74.12 [16] | 24.82 | <0.001 | <0.001 | 0.065 | 0.958 |
| 21.22 | 67.72 [11] | 63.60 [14] | 34.25 [17] | 29.28 | <0.001 | 0.002 | 0.371 | 0.193 |
| 24.18 | 20.27 [12] | 78.95 [16] | 25.33 [17] | 22.24 | <0.001 | 0.922 | 0.042 | 0.036 |
| 30.01 | 6.36 [17] | 62.89 [16] | 13.06 [20] | 21.89 | <0.001 | <0.001 | 0.037 | 0.093 |
| 32.85 | 4.11 [9] | 75.61 [15] | 29.40 [18] | 30.99 | <0.001 | 0.102 | 0.002 | 0.082 |
| 38.41 | 20.92 [10] | 23.09 [16] | 34.76 [17] | 13.56 | 0.009 | <0.001 | 0.912 | 0.271 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haiek, M.; Dvoyris, V.; Broza, Y.Y.; Haick, H.; Weiss, E.; Houri-Haddad, Y. Bacterial Volatile Organic Compounds as Potential Caries and Periodontitis Disease Biomarkers. Int. J. Mol. Sci. 2025, 26, 3591. https://doi.org/10.3390/ijms26083591
Haiek M, Dvoyris V, Broza YY, Haick H, Weiss E, Houri-Haddad Y. Bacterial Volatile Organic Compounds as Potential Caries and Periodontitis Disease Biomarkers. International Journal of Molecular Sciences. 2025; 26(8):3591. https://doi.org/10.3390/ijms26083591
Chicago/Turabian StyleHaiek, Maisa, Vladislav Dvoyris, Yoav Y. Broza, Hossam Haick, Ervin Weiss, and Yael Houri-Haddad. 2025. "Bacterial Volatile Organic Compounds as Potential Caries and Periodontitis Disease Biomarkers" International Journal of Molecular Sciences 26, no. 8: 3591. https://doi.org/10.3390/ijms26083591
APA StyleHaiek, M., Dvoyris, V., Broza, Y. Y., Haick, H., Weiss, E., & Houri-Haddad, Y. (2025). Bacterial Volatile Organic Compounds as Potential Caries and Periodontitis Disease Biomarkers. International Journal of Molecular Sciences, 26(8), 3591. https://doi.org/10.3390/ijms26083591