
Investigating the Role of Skin Autofluorescence in Gestational Diabetes Mellitus: A Systematic Review

 ,
,  , , and
, , and
Abstract
1. Introduction
2. Results
3. Discussion
3.1. AGEs and Their Relevance to Pregnancy
3.2. Heterogenous Diagnosis of GDM
3.3. Interpopulation Variability
3.4. GDM-Complicated Pregnancy Outcome and SAF
3.5. OS and Brain Implications
3.6. Future Perspectives
3.7. Strengths and Limitations
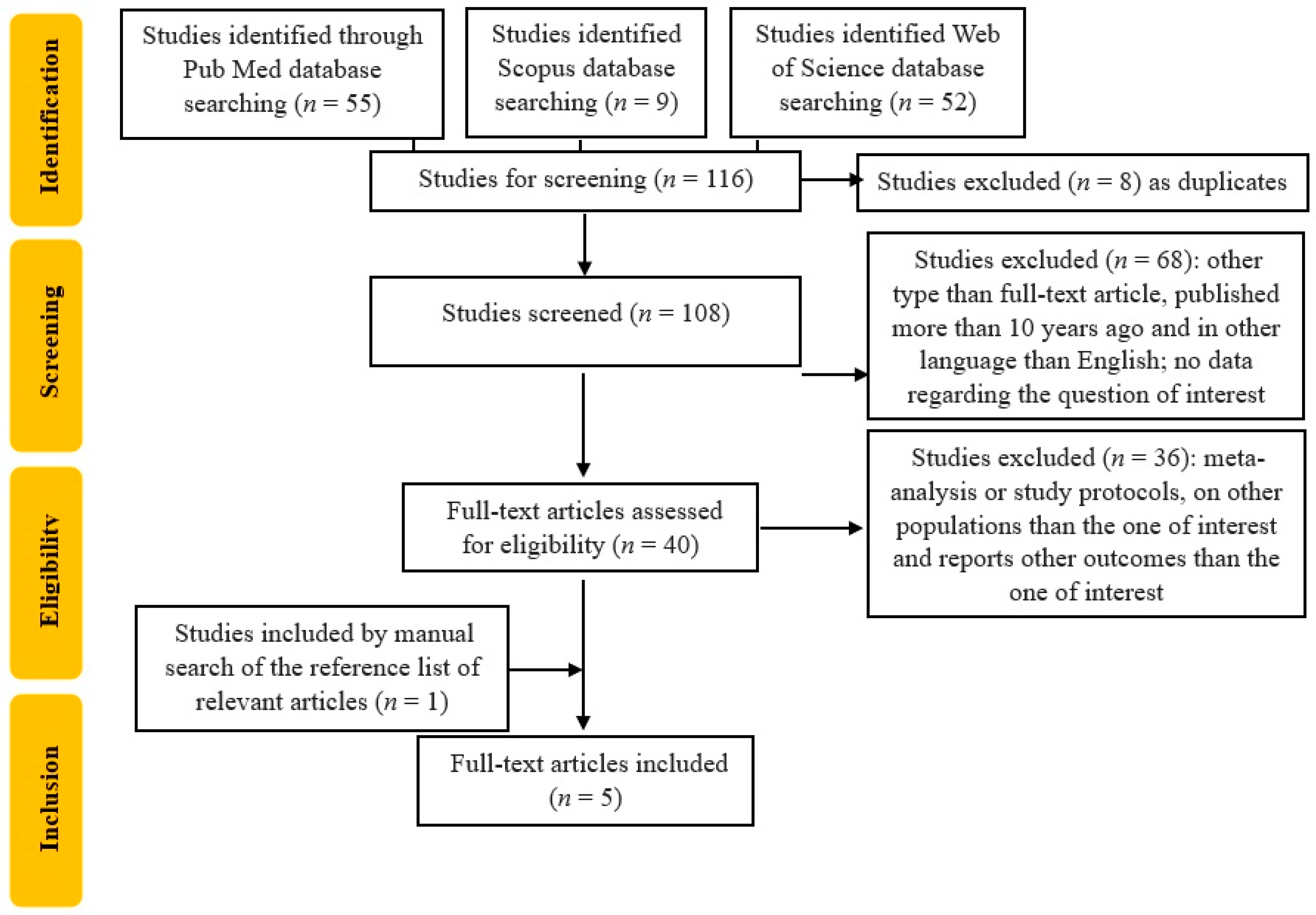
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ADA | American Diabetes Association |
| AGEs | Advanced Glycation End Products |
| AU | Arbitrary Unit |
| CGMS | Continuous Glucose Monitoring systems |
| CI | Confidence Interval |
| CV | Cardiovascular |
| CVD | Cardiovascular Disease |
| DM | Diabetes Mellitus |
| GDM | Gestational Diabetes Mellitus |
| GW | Gestational Weeks |
| IR | Insulin Resistance |
| OGTT | Oral Glucose Tolerance Test |
| OR | Odds Ratio |
| OS | Oxidative Stress |
| PDM | Pregestational Diabetes Mellitus |
| RAGE | Receptor for AGEs |
| ROS | Reactive Oxygen Species |
| SAF | Skin Autofluorescence |
| T1DM | Type 1 Diabetes Mellitus |
| T2DM | Type 2 Diabetes Mellitus |
References
- American Diabetes Association Professional Practice Committee. 2. Diagnosis and Classification of Diabetes: Standards of Care in Diabetes-2024. Diabetes Care 2024, 47 (Suppl. S1), S20–S42. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bilous, R.W.; Jacklin, P.B.; Maresh, M.J.; Sacks, D.A. Resolving the Gestational Diabetes Diagnosis Conundrum: The Need for a Randomized Controlled Trial of Treatment. Diabetes Care 2021, 44, 858–864. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Feig, D.S.; Hwee, J.; Shah, B.R.; Booth, G.L.; Bierman, A.S.; Lipscombe, L.L. Trends in incidence of diabetes in pregnancy and serious perinatal outcomes: A large, population-based study in Ontario, Canada, 1996–2010. Diabetes Care 2014, 37, 1590–1596. [Google Scholar] [CrossRef] [PubMed]
- Committee on Practice Bulletins—Obstetrics. ACOG Practice Bulletin No. 190: Gestational Diabetes Mellitus. Obstet. Gynecol. 2018, 131, e49–e64. [Google Scholar] [CrossRef] [PubMed]
- Hedderson, M.M.; Gunderson, E.P.; Ferrara, A. Gestational weight gain and risk of gestational diabetes mellitus. Obstet. Gynecol. 2010, 115, 597–604, Erratum in Obstet. Gynecol. 2010, 115, 1092. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kim, C.; Liu, T.; Valdez, R.; Beckles, G.L. Does frank diabetes in first-degree relatives of a pregnant woman affect the likelihood of her developing gestational diabetes mellitus or nongestational diabetes? Am. J. Obstet. Gynecol. 2009, 201, 576.e1–576.e6. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hedderson, M.M.; Williams, M.A.; Holt, V.L.; Weiss, N.S.; Ferrara, A. Body mass index and weight gain prior to pregnancy and risk of gestational diabetes mellitus. Am. J. Obstet. Gynecol. 2008, 198, 409.e1–409.e7. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Huerta-Chagoya, A.; Vázquez-Cárdenas, P.; Moreno-Macías, H.; Tapia-Maruri, L.; Rodríguez-Guillén, R.; López-Vite, E.; García-Escalante, G.; Escobedo-Aguirre, F.; Parra-Covarrubias, A.; Cordero-Brieño, R.; et al. Genetic determinants for gestational diabetes mellitus and related metabolic traits in Mexican women. PLoS ONE 2015, 10, e0126408. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Papadopoulou, A.; Lynch, K.F.; Shaat, N.; Håkansson, R.; Ivarsson, S.A.; Berntorp, K.; Agardh, C.D.; Lernmark, Å.; DiPiS Study Group. Gestational diabetes mellitus is associated with TCF7L2 gene polymorphisms independent of HLA-DQB1*0602 genotypes and islet cell autoantibodies. Diabet. Med. 2011, 28, 1018–1027. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Firneisz, G.; Rosta, K.; Al-Aissa, Z.; Hadarits, O.; Harreiter, J.; Nádasdi, Á.; Bancher-Todesca, D.; Németh, L.; Igaz, P.; Rigó, J., Jr.; et al. The MTNR1B rs10830963 Variant in Interaction with Pre-Pregnancy BMI is a Pharmacogenetic Marker for the Initiation of Antenatal Insulin Therapy in Gestational Diabetes Mellitus. Int. J. Mol. Sci. 2018, 19, 3734. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Li, Y.; Hadden, C.; Singh, P.; Mercado, C.P.; Murphy, P.; Dajani, N.K.; Lowery, C.L.; Roberts, D.J.; Maroteaux, L.; Kilic, F. GDM-associated insulin deficiency hinders the dissociation of SERT from ERp44 and down-regulates placental 5-HT uptake. Proc. Natl. Acad. Sci. USA 2014, 111, E5697–E5705. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Red-Horse, K.; Zhou, Y.; Genbacev, O.; Prakobphol, A.; Foulk, R.; McMaster, M.; Fisher, S.J. Trophoblast differentiation during embryo implantation and formation of the maternal-fetal interface. J. Clin. Investig. 2004, 114, 744–754. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Venkatesh, K.K.; Lynch, C.D.; Powe, C.E.; Costantine, M.M.; Thung, S.F.; Gabbe, S.G.; Grobman, W.A.; Landon, M.B. Risk of Adverse Pregnancy Outcomes Among Pregnant Individuals with Gestational Diabetes by Race and Ethnicity in the United States, 2014–2020. JAMA 2022, 327, 1356–1367. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pilliod, R.A.; Page, J.M.; Burwick, R.M.; Kaimal, A.J.; Cheng, Y.W.; Caughey, A.B. The risk of fetal death in nonanomalous pregnancies affected by polyhydramnios. Am. J. Obstet. Gynecol. 2015, 213, 410.e1–410.e6. [Google Scholar] [CrossRef] [PubMed]
- Usami, T.; Yokoyama, M.; Ueno, M.; Iwama, N.; Sagawa, N.; Kawano, R.; Waguri, M.; Sameshima, H.; Hiramatsu, Y.; Sugiyama, T.; et al. Comparison of pregnancy outcomes between women with early-onset and late-onset gestational diabetes in a retrospective multi-institutional study in Japan. J. Diabetes Investig. 2020, 11, 216–222. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Page, J.M.; Allshouse, A.A.; Cassimatis, I.; Smid, M.C.; Arslan, E.; Thorsten, V.; Parker, C.; Varner, M.W.; Dudley, D.J.; Saade, G.R.; et al. Characteristics of Stillbirths Associated with Diabetes in a Diverse U.S. Cohort. Obstet. Gynecol. 2020, 136, 1095–1102. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Dudley, D.J. Diabetic-associated stillbirth: Incidence, pathophysiology, and prevention. Obstet. Gynecol. Clin. North Am. 2007, 34, 293–307. [Google Scholar] [CrossRef] [PubMed]
- Vääräsmäki, M.; Pouta, A.; Elliot, P.; Tapanainen, P.; Sovio, U.; Ruokonen, A.; Hartikainen, A.L.; McCarthy, M.; Järvelin, M.R. Adolescent manifestations of metabolic syndrome among children born to women with gestational diabetes in a general-population birth cohort. Am. J. Epidemiol. 2009, 169, 1209–1215. [Google Scholar] [CrossRef] [PubMed]
- Bjornstad, P.; Chao, L.C.; Cree-Green, M.; Dart, A.B.; King, M.; Looker, H.C.; Magliano, D.J.; Nadeau, K.J.; Pinhas-Hamiel, O.; Shah, A.S.; et al. Youth-onset type 2 diabetes mellitus: An urgent challenge. Nat. Rev. Nephrol. 2023, 19, 168–184. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Vounzoulaki, E.; Khunti, K.; Abner, S.C.; Tan, B.K.; Davies, M.J.; Gillies, C.L. Progression to type 2 diabetes in women with a known history of gestational diabetes: Systematic review and meta-analysis. BMJ 2020, 369, m1361. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Varner, M.W.; Rice, M.M.; Landon, M.B.; Casey, B.M.; Reddy, U.M.; Wapner, R.J.; Rouse, D.J.; Tita, A.T.N.; Thorp, J.M.; Chien, E.K.; et al. Pregnancies After the Diagnosis of Mild Gestational Diabetes Mellitus and Risk of Cardiometabolic Disorders. Obstet. Gynecol. 2017, 129, 273–280. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Iordachescu, A.C.; Cirstoiu, M.M.; Zugravu, C.A.; Teodor, O.M.; Turcan, N.; Ducu, I.; Bohiltea, R.E. Dietary behavior during pregnancy. Exp. Ther. Med. 2020, 20, 2460–2464. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kramer, C.K.; Campbell, S.; Retnakaran, R. Gestational diabetes and the risk of cardiovascular disease in women: A systematic review and meta-analysis. Diabetologia 2019, 62, 905–914. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.X.; Mitsunami, M.; Manson, J.E.; Gaskins, A.J.; Rich-Edwards, J.W.; Wang, L.; Zhang, C.; Chavarro, J.E. Association of Gestational Diabetes with Subsequent Long-Term Risk of Mortality. JAMA Intern. Med. 2023, 183, 1204–1213. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Weisz, B.; Shrim, A.; Homko, C.J.; Schiff, E.; Epstein, G.S.; Sivan, E. One hour versus two hours postprandial glucose measurement in gestational diabetes: A prospective study. J. Perinatol. 2005, 25, 241–244. [Google Scholar] [CrossRef] [PubMed]
- Sandu, C.; Bica, C.; Salmen, T.; Stoica, R.; Bohiltea, R.; Gherghiceanu, F.; Pacu, I.; Stefan, S.; Serafinceanu, C.; Stoian, A.P. Gestational diabetes—Modern management and therapeutic approach (Review). Exp. Ther. Med. 2021, 21, 81. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Galindo, R.J.; Umpierrez, G.E.; Rushakoff, R.J.; Basu, A.; Lohnes, S.; Nichols, J.H.; Spanakis, E.K.; Espinoza, J.; Palermo, N.E.; Awadjie, D.G.; et al. Continuous Glucose Monitors and Automated Insulin Dosing Systems in the Hospital Consensus Guideline. J. Diabetes Sci. Technol. 2020, 14, 1035–1064. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Feig, D.S.; Donovan, L.E.; Corcoy, R.; Murphy, K.E.; Amiel, S.A.; Hunt, K.F.; Asztalos, E.; Barrett, J.F.R.; Sanchez, J.J.; de Leiva, A.; et al. Continuous glucose monitoring in pregnant women with type 1 diabetes (CONCEPTT): A multicentre international randomised controlled trial. Lancet 2017, 390, 2347–2359, Erratum in Lancet 2017, 390, 2346. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Stirban, A. Noninvasive Skin Fluorescence Spectroscopy for Diabetes Screening. J. Diabetes Sci. Technol. 2013, 7, 1001–1004. [Google Scholar] [CrossRef]
- Boersma, H.E.; van der Klauw, M.M.; Smit, A.J.; Wolffenbuttel, B.H.R. A non-invasive risk score including skin autofluorescence predicts diabetes risk in the general population. Sci. Rep. 2022, 12, 21794. [Google Scholar] [CrossRef]
- Tanin, Ö.Ş.; Kara, M.; Engin-Üstün, Y.; Göçmen, A.Y.; Yalvaç, E.S. Comparison of glucose degradation product and receptor levels in diabetic and normal pregnancy. J. Turk. Ger. Gynecol. Assoc. 2021, 22, 127–131. [Google Scholar] [CrossRef] [PubMed]
- Cosson, E.; Gary, F.; Nguyen, M.T.; Bianchi, L.; Sandre-Banon, D.; Biri, L.; Jaber, Y.; Cussac-Pillegand, C.; Banu, I.; Chiheb, S.; et al. Gradual increase in advanced glycation end-products from no diabetes to early and regular gestational diabetes: A case-control study. Diabetes Metab. 2019, 45, 586–589. [Google Scholar] [CrossRef] [PubMed]
- Foussard, N.; Cougnard-Grégoire, A.; Rajaobelina, K.; Delcourt, C.; Helmer, C.; Lamireau, T.; Gonzalez, C.; Grouthier, V.; Haissaguerre, M.; Blanco, L.; et al. Skin Autofluorescence of Pregnant Women with Diabetes Predicts the Macrosomia of Their Children. Diabetes 2019, 68, 1663–1669. [Google Scholar] [CrossRef] [PubMed]
- de Ranitz-Greven, W.L.; Kaasenbrood, L.; Poucki, W.K.; Hamerling, J.; Bos, D.C.; Visser, G.H.; Biesma, D.H.; Beulens, J.W.; de Valk, H.W. Advanced glycation end products, measured as skin autofluorescence, during normal pregnancy and pregnancy complicated by diabetes mellitus. Diabetes Technol. Ther. 2012, 14, 1134–1139. [Google Scholar] [CrossRef] [PubMed]
- de Ranitz-Greven, W.L.; Bos, D.C.; Poucki, W.K.; Visser, G.H.; Beulens, J.W.; Biesma, D.H.; de Valk, H.W. Advanced glycation end products, measured as skin autofluorescence, at diagnosis in gestational diabetes mellitus compared with normal pregnancy. Diabetes Technol. Ther. 2012, 14, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Maury, E.; Savel, J.; Grouthier, V.; Rajaobelina, K.; Corvo, L.; Lorrain, S.; Gonzalez, C.; Gin, H.; Barberger-Gateau, P.; Rigalleau, V. Is skin autofluorescence a marker of metabolic memory in pregnant women with diabetes? Diabet. Med. 2015, 32, 1575–1579. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.H.; Lin, X.; Bu, C.; Zhang, X. Role of advanced glycation end products in mobility and considerations in possible dietary and nutritional intervention strategies. Nutr. Metab. 2018, 15, 72. [Google Scholar] [CrossRef]
- Rajaraman, B.; Ramadas, N.; Krishnasamy, S.; Ravi, V.; Pathak, A.; Devasena, C.S.; Swaminathan, K.; Ganeshprasad, A.; Kuppuswamy, A.A.; Vedantham, S. Correction to: Hyperglycemia cause vascular inflammation through advanced glycation end products/early growth response-1 axis in gestational diabetes mellitus. Mol. Cell. Biochem. 2022, 477, 977–978. [Google Scholar] [CrossRef]
- Prasad, A.; Bekker, P.; Tsimikas, S. Advanced Glycation End Products and Diabetic Cardiovascular Disease. Cardiol. Rev. 2012, 20, 177–183. [Google Scholar] [CrossRef]
- Du, T.; Brandl, B.; Hauner, H.; Skurk, T. Skin Autofluorescence Mirrors Surrogate Parameters of Vascular Aging: An Enable Study. Nutrients 2023, 15, 1597. [Google Scholar] [CrossRef]
- van Waateringe, R.P.; Fokkens, B.T.; Slagter, S.N.; van der Klauw, M.M.; van Vliet-Ostaptchouk, J.V.; Graaff, R.; Paterson, A.D.; Smit, A.J.; Lutgers, H.L.; Wolffenbuttel, B.H.R. Skin autofluorescence predicts incident type 2 diabetes, cardiovascular disease and mortality in the general population. Diabetologia 2019, 62, 269–280. [Google Scholar] [CrossRef] [PubMed]
- Reurean-Pintilei, D.; Pantea Stoian, A.; Salmen, T.; Stoica, R.-A.; Mititelu-Tartau, L.; Lazăr, S.; Timar, B. Associations between Skin Autofluorescence Levels with Cardiovascular Risk and Diabetes Complications in Patients with Type 2 Diabetes. Biomedicines 2024, 12, 890. [Google Scholar] [CrossRef] [PubMed]
- Mao, Y.; Hu, W.; Xia, B.; Liu, L.; Han, X.; Liu, Q. Association Between Gestational Diabetes Mellitus and the Risks of Type-Specific Cardiovascular Diseases. Front. Public Health 2022, 10, 940335. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chen, A.; Tan, B.; Du, R.; Chong, Y.S.; Zhang, C.; Koh, A.S.; Li, L.J. Gestational diabetes mellitus and development of intergenerational overall and subtypes of cardiovascular diseases: A systematic review and meta-analysis. Cardiovasc. Diabetol. 2024, 23, 320. [Google Scholar] [CrossRef]
- Jinno, M.; Takeuchi, M.; Watanabe, A.; Teruya, K.; Hirohama, J.; Eguchi, N.; Miyazaki, A. Advanced glycation end-products accumulation compromises embryonic development and achievement of pregnancy by assisted reproductive technology. Hum. Reprod. 2011, 26, 604–610. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.; Barden, A.; Mori, T.; Beilin, L. Advanced glycation end-products: A review. Diabetologia 2001, 44, 129–146. [Google Scholar] [CrossRef]
- Goto, M.; Yamagishi, S.I.; Matsui, T.; Koide, K.; Takita, H.; Tokunaka, M.; Sekizawa, A. Predictive ability of serum advanced glycation end products at 11 to 13 weeks of gestation for early-onset preeclampsia. AJOG Glob. Rep. 2022, 2, 100052. [Google Scholar] [CrossRef]
- Shi, Y.; Qian, J.; Zhang, Q.; Hu, Y.; Sun, D.; Jiang, L. Advanced glycation end products increased placental vascular permeability of human BeWo cells via RAGE/NF-kB signaling pathway. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 250, 93–100. [Google Scholar] [CrossRef]
- McElwain, C.J.; Tuboly, E.; McCarthy, F.P.; McCarthy, C.M. Mechanisms of Endothelial Dysfunction in Pre-eclampsia and Gestational Diabetes Mellitus: Windows into Future Cardiometabolic Health? Front. Endocrinol. 2020, 11, 655. [Google Scholar] [CrossRef]
- Gurbuz, O.; Yorgancı, A.; Ozgu-Erdinc, A.S.; Tasci, Y. First trimester screening of serum advanced glycation end products levels of pregnant women who have risk factors for gestational diabetes and their obstetric outcomes: A preliminary case-control study. J. Obstet. Gynaecol. J. Inst. Obstet. Gynaecol. 2022, 42, 3048–3054. [Google Scholar] [CrossRef]
- Li, H.; Dong, A.; Lv, X. Advanced glycation end products and adipocytokines and oxidative stress in placental tissues of pregnant women with gestational diabetes mellitus. Exp. Ther. Med. 2019, 18, 685–691. [Google Scholar] [CrossRef]
- Saucedo, R.; Ortega-Camarillo, C.; Ferreira-Hermosillo, A.; Díaz-Velázquez, M.F.; Meixueiro-Calderón, C.; Valencia-Ortega, J. Role of Oxidative Stress and Inflammation in Gestational Diabetes Mellitus. Antioxidants 2023, 12, 1812. [Google Scholar] [CrossRef]
- Berceanu, C.; Cîrstoiu, M.; Mehedințu, C.; Brătilă, P.; Berceanu, S.; Vlădăreanu, S.; Bohîlțea, R.; Brătilă, E. Hormone deficiency and its impact on the lower urinary tract. In Proceedings of the 13th National Congress of Urogynecology, Brașov, Romania, 29 September–1 October 2016; Filodiritto Editore: Bologna, Italy, 2016; pp. 29–38, ISBN 978-88-95922-78-2. [Google Scholar]
- Sisay, M.; Edessa, D.; Ali, T.; Mekuria, A.N.; Gebrie, A. The relationship between advanced glycation end products and gestational diabetes: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0240382. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2020. Diabetes Care 2020, 43 (Suppl. S1), S14–S31. [Google Scholar] [CrossRef] [PubMed]
- Lowe, W.L., Jr.; Scholtens, D.M.; Kuang, A.; Linder, B.; Lawrence, J.M.; Lebenthal, Y.; McCance, D.; Hamilton, J.; Nodzenski, M.; Talbot, O.; et al. HAPO Follow-up Study Cooperative Research Group Hyperglycemia and Adverse Pregnancy Outcome Follow-up Study (HAPO FUS): Maternal Gestational Diabetes Mellitus and Childhood Glucose Metabolism. Diabetes Care 2019, 42, 372–380. [Google Scholar] [CrossRef] [PubMed]
- Scholtens, D.M.; Kuang, A.; Lowe, L.P.; Hamilton, J.; Lawrence, J.M.; Lebenthal, Y.; Brickman, W.J.; Clayton, P.; Ma, R.C.; McCance, D.; et al. HAPO Follow-up Study Cooperative Research Group, & HAPO Follow-Up Study Cooperative Research Group Hyperglycemia and Adverse Pregnancy Outcome Follow-up Study (HAPO FUS): Maternal Glycemia and Childhood Glucose Metabolism. Diabetes Care 2019, 42, 381–392. [Google Scholar] [CrossRef]
- Josefson, J.L.; Scholtens, D.M.; Kuang, A.; Catalano, P.M.; Lowe, L.P.; Dyer, A.R.; Petito, L.C.; Lowe, W.L., Jr.; Metzger, B.E. HAPO Follow-up Study Cooperative Research Group Newborn Adiposity and Cord Blood C-Peptide as Mediators of the Maternal Metabolic Environment and Childhood Adiposity. Diabetes Care 2021, 44, 1194–1202. [Google Scholar] [CrossRef]
- Landon, M.B.; Rice, M.M.; Varner, M.W.; Casey, B.M.; Reddy, U.M.; Wapner, R.J.; Rouse, D.J.; Biggio, J.R., Jr.; Thorp, J.M.; Chien, E.K.; et al. Eunice Kennedy Shriver National Institute of Child Health and Human Development Maternal-Fetal Medicine Units (MFMU) Network Mild gestational diabetes mellitus and long-term child health. Diabetes Care 2015, 38, 445–452. [Google Scholar] [CrossRef]
- Tam, W.H.; Ma, R.C.W.; Ozaki, R.; Li, A.M.; Chan, M.H.M.; Yuen, L.Y.; Lao, T.T.H.; Yang, X.; Ho, C.S.; Tutino, G.E.; et al. In Utero Exposure to Maternal Hyperglycemia Increases Childhood Cardiometabolic Risk in Offspring. Diabetes Care 2017, 40, 679–686. [Google Scholar] [CrossRef]
- Saccone, G.; Khalifeh, A.; Al-Kouatly, H.B.; Sendek, K.; Berghella, V. Screening for gestational diabetes mellitus: One step versus two step approach. A meta-analysis of randomized trials. J. Matern. -Fetal Neonatal Med. 2020, 33, 1616–1624. [Google Scholar] [CrossRef]
- Bartakova, V.; Kollarova, R.; Kuricova, K.; Sebekova, K.; Belobradkova, J.; Kankova, K. Serum carboxymethyl-lysine, a dominant advanced glycation end product, is increased in women with gestational diabetes mellitus. Biomed. Pap. Med. Fac. Univ. Palacky Olomouc. Czech. Repub. 2016, 160, 70–75. [Google Scholar] [CrossRef] [PubMed]
- Júnior, J.P.L.; Brescansin, C.P.; Santos-Weiss, I.C.R.; Welter, M.; de Souza, E.M.; Rego, F.G.d.M.; Picheth, G.; Alberton, D. Serum Fluorescent Advanced Glycation End (F-AGE) products in gestational diabetes patients. Arch Endocrinol. Metab. 2017, 61, 233–237. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ahmad, M.S.; Kimhofer, T.; Ahmad, S.; AlAma, M.N.; Mosli, H.H.; Hindawi, S.I.; Mook-Kanamori, D.O.; Šebeková, K.; Damanhouri, Z.A.; Holmes, E. Ethnicity and skin autofluorescence-based risk-engines for cardiovascular disease and diabetes mellitus. PLoS ONE 2017, 12, e0185175. [Google Scholar] [CrossRef]
- Smit, A.J.; van de Zande, S.C.; Mulder, D.J. Skin autofluorescence as tool for cardiovascular and diabetes risk prediction. Curr. Opin. Nephrol. Hypertens. 2022, 31, 522–526. [Google Scholar] [CrossRef] [PubMed]
- Mooldijk, S.S.; Lu, T.; Waqas, K.; Chen, J.; Vernooij, M.W.; Ikram, M.K.; Zillikens, M.C.; Ikram, M.A. Skin autofluorescence, reflecting accumulation of advanced glycation end products, and the risk of dementia in a population-based cohort. Sci. Rep. 2024, 14, 1256. [Google Scholar] [CrossRef] [PubMed]
- Cavero-Redondo, I.; Soriano-Cano, A.; Álvarez-Bueno, C.; Cunha, P.G.; Martínez-Hortelano, J.A.; Garrido-Miguel, M.; Berlanga-Macías, C.; Martínez-Vizcaíno, V. Skin Autofluorescence-Indicated Advanced Glycation End Products as Predictors of Cardiovascular and All-Cause Mortality in High-Risk Subjects: A Systematic Review and Meta-analysis. J. Am. Heart Assoc. 2018, 7, e009833. [Google Scholar] [CrossRef]
- Stirban, A.; Heinemann, L. Skin Autofluorescence—A Non-invasive Measurement for Assessing Cardiovascular Risk and Risk of Diabetes. Eur Endocrinol. 2014, 10, 106–110. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- McIntyre, N.J. Trend and Monitoring of Skin Autofluorescence in Patients Receiving Hemodialysis. Kidney Int. Rep. 2024, 9, 2335–2336. [Google Scholar] [CrossRef]
- Martínez-García, I.; Cavero-Redondo, I.; Pascual-Morena, C.; Otero-Luis, I.; Fenoll-Morate, M.; Lever-Megina, C.G.; Rodríguez-Gutiérrez, E.; Saz-Lara, A. Reference Values of Skin Autofluorescence by Age Groups in Healthy Spanish Adults: Results from the EVasCu Study, a Systematic Review, and a Meta-Analysis. J. Clin. Med. 2025, 14, 474. [Google Scholar] [CrossRef]
- Sánchez, E.; Sánchez, M.; López-Cano, C.; Bermúdez-López, M.; Valdivielso, J.M.; Farràs-Sallés, C.; Pamplona, R.; Torres, G.; Mauricio, D.; Castro, E.; et al. Is There a Link between Obesity Indices and Skin Autofluorescence? A Response from the ILERVAS Project. Nutrients 2022, 15, 203. [Google Scholar] [CrossRef]
- Reurean-Pintilei, D.; Pantea Stoian, A.; Potcovaru, C.-G.; Salmen, T.; Cinteză, D.; Stoica, R.-A.; Lazăr, S.; Timar, B. Skin Autofluorescence as a Potential Adjunctive Marker for Cardiovascular Risk Assessment in Type 2 Diabetes: A Systematic Review. Int. J. Mol. Sci. 2024, 25, 3889. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Waqas, K.; Tan, R.C.; Voortman, T.; Ikram, M.A.; Nijsten, T.E.C.; de Groot, L.C.; Uitterlinden, A.G.; Zillikens, M.C. The association between dietary and skin advanced glycation end products: The Rotterdam Study. Am. J. Clin. Nutr. 2020, 112, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Atzeni, I.M.; Boersema, J.; Pas, H.H.; Diercks, G.F.H.; Scheijen, J.L.J.M.; Schalkwijk, C.G.; Mulder, D.J.; van der Zee, P.; Smit, A.J. Is skin autofluorescence (SAF) representative of dermal advanced glycation endproducts (AGEs) in dark skin? A pilot study. Heliyon 2020, 6, e05364. [Google Scholar] [CrossRef]
- Noordzij, M.J.; Lefrandt, J.D.; Graaff, R.; Smit, A.J. Dermal Factors Influencing Measurement of Skin Autofluorescence. Diabetes Technol. Ther. 2011, 13, 165–170. [Google Scholar] [CrossRef]
- Lutgers, H.L.; Graaff, R.; Links, T.P.; Ubink-Veltmaat, L.J.; Bilo, H.J.; Gans, R.O.; Smit, A.J. Skin autofluoresce as a noninvasive marker of vascular damage in patients with type 2 diabetes. Diabetes Care 2006, 29, 2654–2659. [Google Scholar] [CrossRef]
- Simon Klenovics, K.; Kollárová, R.; Hodosy, J.; Celec, P.; Sebeková, K. Reference values of skin autofluorescence as an estimation of tissue accumulation of advanced glycation end products in a general Slovak population. Diabet. Med. A J. Br. Diabet. Assoc. 2014, 31, 581–585. [Google Scholar] [CrossRef] [PubMed]
- Alkhami, F.; Borderie, G.; Foussard, N.; Larroumet, A.; Blanco, L.; Barbet-Massin, M.A.; Ferriere, A.; Ducos, C.; Mohammedi, K.; Fawaz, S.; et al. The skin autofluorescence may help to select patients with Type 2 diabetes candidates for screening to revascularization procedures. Cardiovasc. Diabetol. 2024, 23, 32. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chen, J.; Arshi, B.; Waqas, K.; Lu, T.; Bos, D.; Ikram, M.A.; Uitterlinden, A.G.; Kavousi, M.; Zillikens, M.C. Advanced glycation end products measured by skin autofluorescence and subclinical cardiovascular disease: The Rotterdam Study. Cardiovasc. Diabetol. 2023, 22, 326. [Google Scholar] [CrossRef]
- Boersma, H.E.; van Waateringe, R.P.; van der Klauw, M.M.; Graaff, R.; Paterson, A.D.; Smit, A.J.; Wolffenbuttel, B.H.R. Skin autofluorescence predicts new cardiovascular disease and mortality in people with type 2 diabetes. BMC Endocr. Disord. 2021, 21, 14. [Google Scholar] [CrossRef]
- Hebert, J.F.; Myatt, L. Placental mitochondrial dysfunction with metabolic diseases: Therapeutic approaches. Biochim. Biophys. Acta-Mol. Basis Dis. 2021, 1867, 165967. [Google Scholar] [CrossRef]
- Di Fabrizio, C.; Giorgione, V.; Khalil, A.; Murdoch, C.E. Antioxidants in Pregnancy: Do We Really Need More Trials? Antioxidants 2022, 11, 812. [Google Scholar] [CrossRef] [PubMed]
- Hagen, J.M.; Cornelissen, A.; Veeneman, R.R.; van der Heijden, H.S.; Sutterland, A.L.; Vermeulen, J.M.; Tan, H.L.; de Haan, L. Skin advanced glycation end products, indicating cumulative oxidative stress, associated with schizophrenia but not with psychosis-like experiences. Schizophr. Res. 2025, 276, 237–242. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Zhang, Y.; Yue, C.; Ye, Y.; Chen, P.; Peng, W.; Wang, Y. Accumulation of Advanced Glycation End Products Involved in Inflammation and Contributing to Severe Preeclampsia, in Maternal Blood, Umbilical Blood and Placental Tissues. Gynecol. Obstet. Investig. 2017, 82, 388–397. [Google Scholar] [CrossRef]
- Wierzchowska-Opoka, M.; Grunwald, A.; Rekowska, A.K.; Łomża, A.; Mekler, J.; Santiago, M.; Kabała, Z.; Kimber-Trojnar, Ż.; Leszczyńska-Gorzelak, B. Impact of Obesity and Diabetes in Pregnant Women on Their Immunity and Vaccination. Vaccines 2023, 11, 1247. [Google Scholar] [CrossRef]
- Nelson, B.N.; Friedman, J.E. Developmental Programming of the Fetal Immune System by Maternal Western-Style Diet: Mechanisms and Implications for Disease Pathways in the Offspring. Int. J. Mol. Sci. 2024, 25, 5951. [Google Scholar] [CrossRef]
- Eleftheriades, A.; Koulouraki, S.; Belegrinos, A.; Eleftheriades, M.; Pervanidou, P. Maternal Obesity and Neurodevelopment of the Offspring. Nutrients 2025, 17, 891. [Google Scholar] [CrossRef]
- Marschallinger, J.; Iram, T.; Zardeneta, M.; Lee, S.E.; Lehallier, B.; Haney, M.S.; Pluvinage, J.V.; Mathur, V.; Hahn, O.; Morgens, D.W.; et al. Lipid-droplet-accumulating microglia represent a dysfunctional and proinflammatory state in the aging brain. Nat. Neurosci. 2020, 23, 194–208. [Google Scholar] [CrossRef]
- Jankowska, M.; Szadkowska, A.; Pietrzak, I.; Chrzanowski, J.; Sołek, J.; Fendler, W.; Mianowska, B. Assessment of Skin Autofluorescence and Its Association with Glycated Hemoglobin, Cardiovascular Risk Markers, and Concomitant Chronic Diseases in Children with Type 1 Diabetes. Nutrients 2024, 16, 1940. [Google Scholar] [CrossRef] [PubMed]
- Zavorins, A.; Silova, A.; Voicehovska, J.; Kisis, J. Rubeosis faciei diabeticorum is not associated with oxidative stress and skin autofluorescence. An. Bras. Dermatol. 2019, 94, 561–566. [Google Scholar] [CrossRef]
- Mustață, M.-L.; Neagoe, C.-D.; Rădulescu, V.-M.; Dragne, I.-G.; Cîmpeanu, R.-C.; Radu, L.; Ahrițculesei, R.-V.; Forțofoiu, D.; Predoi, M.-C.; Ianoși, S.-L. Association Between Systemic Inflammation, Metabolic Syndrome and Quality of Life in Psoriasis Patients. Life 2025, 15, 212. [Google Scholar] [CrossRef]
- Metcalfe, A.; Sabr, Y.; Hutcheon, J.A.; Donovan, L.; Lyons, J.; Burrows, J.; Joseph, K.S. Trends in Obstetric Intervention and Pregnancy Outcomes of Canadian Women with Diabetes in Pregnancy from 2004 to 2015. J. Endocr. Soc. 2017, 1, 1540–1549. [Google Scholar] [CrossRef] [PubMed]
- Rajaobelina, K.; Farges, B.; Nov, S.; Maury, E.; Cephise-Velayoudom, F.L.; Gin, H.; Helmer, C.; Rigalleau, V. Skin autofluorescence and peripheral neuropathy four years later in type 1 diabetes. Diabetes/Metab. Res. Rev. 2017, 33, e2832. [Google Scholar] [CrossRef] [PubMed]
- Mustață, M.-L.; Ionescu, M.; Radu, L.; Neagoe, C.-D.; Ahrițculesei, R.-V.; Cîmpeanu, R.-C.; Matei, D.; Amzolini, A.-M.; Predoi, M.-C.; Ianoși, S.-L. The Role of Metabolic Syndrome in Psoriasis Treatment Response: A One-Year Comparative Analysis of PASI Progression. Diagnostics 2024, 14, 2887. [Google Scholar] [CrossRef] [PubMed]
- Edmonds, L.K.; Kandasamy, Y.; Lamont, A.; O’Connor, S. Perinatal arterial ischemic stroke in northern Queensland. Am. J. Perinatol. 2012, 29, 483–488. [Google Scholar] [CrossRef]
- Said, A.S.; Manji, K.P. Risk factors and outcomes of fetal macrosomia in a tertiary centre in Tanzania: A case-control study. BMC Pregnancy Childbirth 2016, 16, 243. [Google Scholar] [CrossRef]
- Nielsen, L.R.; Ekbom, P.; Damm, P.; Glümer, C.; Frandsen, M.M.; Jensen, D.M.; Mathiesen, E.R. HbA1c levels are significantly lower in early and late pregnancy. Diabetes Care 2004, 27, 1200–1201. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| First Author, Publication Year | Country | Study Period | Sample Size: Groups | GW Measurement | DM Type | SAF Model | Baseline SAF Level (AU) | Adverse Pregnancy Outcome Parameter | Outcome | p Value |
|---|---|---|---|---|---|---|---|---|---|---|
| de Ranitz-Greven et al. [34], 2012 | The Netherlands | April 2010–December 2011 | 155: 79 GDM 21 PDM (13 T1DM, 8 T2DM) 55 without DM | weeks 26–29, 30–33, 34–37, and >38 GW; during the first postpartum visit (8 weeks postpartum). | GDM, T1DM, T2DM | AGE Reader (DiagnOptics Technologies BV, Groningen, The Netherlands) | PDM 1.93 Controls 1.75 | Any Complication | OR 1.6 (0.56–4.7) | NS |
| LGA | OR 1.3 (0.31–1.7) | |||||||||
| CS | OR 1.5 (0.55–4.3) | |||||||||
| de Ranitz-Greven et al. [35], 2012 | The Netherlands | April–December 2010 | 124: 60 GDM 44 without DM 20 with an abnormal value at OGTT | During 100 g-OGTT (24–28 GWs) or within the first 3 weeks after OGTT | GDM | AGE Reader (DiagnOptics Technologies BV, Groningen, The Netherlands | GDM 1.74 Controls 1.76 | Increased maternal age | With every year, SAF increases with 0.02 AU | p < 0.001 |
| Ethnicity (lower SAF values in white Europeans with GDM) | 1.6 AU vs. 1.9 AU | p < 0.001 | ||||||||
| Maury et al. [36], 2015 | France | November 2011–November 2012 | 252: 200 GDM 30 PDM (21 T1DM, 9 T2DM) 22 control group (nonpregnant and without DM) | 24–30 GWs | GDM, T1DM, T2DM | AGE ReaderTM; DiagnOptics BV, Groningen, the Netherlands | GDM 1.77 PDM 1.97 Control group 1.6 | SAF higher in patients with 2 or 3 criteria for hyperglycemia * | β = 0.154; β = 0.011 after adjusting for age | p = 0.02; p = 0.009 |
| Increasing age | β = 0.013 | p = 0.0019 | ||||||||
| Fasting plasma glucose | β = 0.073 | p = 0.03 | ||||||||
| 1-h OGTT value | β = 0.032 | p = 0.02 | ||||||||
| SAF was higher in GDM patients with history of hyperglycemia | 0.10 AU higher | p = 0.04 | ||||||||
| SAF was higher in pregnant women vs. controls | 1.80 ± 0.35 AU vs. 1.6 ± 0.32 AU | p = 0.009 | ||||||||
| SAF was higher in PDM than GDM | 0.20 AU higher | p = 0.003 | ||||||||
| Foussard et al. [33], 2019 | France | 2011–2015 | 343: 39 PDM 95 early GDM 209 late GDM | PDM: 21.9 ± 8.2 Early GDM: 22.7 ± 7.2 Late GDM: 29.0 ± 3.4 | GDM, PDM | AGEs-reader (DiagnOptics BV, Groningen, the Netherlands) | Not specified | Macrosomia (whole population) vs. no macrosomia | 2.03 ± 0.30 vs. 1.80 ± 0.34 | p < 0.0001 |
| Macrosomia (GDM) | OR: 3.80; 95% CI: 1.20–12.00 | p = 0.02 | ||||||||
| Cosson et al. [32], 2018 | France | August 2015–July 2016 | 188: 62 early GDM 48 GDM 8 DIP 70 controls | Not specified | GDM, DIP | AGE Reader (DiagnOptics BV, Groningen, The Netherlands | GDM: 1.99 ± 0.47 Early GDM: 2.11 ± 0.48 DIP: 2.42 ± 0.34 | No GDM | 1.79 ± 0.32 AU | NS |
| GDM | 1.99 ± 0.47 AU | NS | ||||||||
| Early GDM | 2.11 ± 0.48 AU | NS | ||||||||
| DIP | 2.42 ± 0.34 AU | p = 0.015; p = 0.021 after adjusting for age; p = 0.021 after adjusting for age and ethnicity |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salmen, B.-M.; Reurean-Pintilei, D.; Trofin, D.; Durdu, C.-E.; Neagu, A.-C.; Bohiltea, R.-E. Investigating the Role of Skin Autofluorescence in Gestational Diabetes Mellitus: A Systematic Review. Int. J. Mol. Sci. 2025, 26, 3022. https://doi.org/10.3390/ijms26073022
Salmen B-M, Reurean-Pintilei D, Trofin D, Durdu C-E, Neagu A-C, Bohiltea R-E. Investigating the Role of Skin Autofluorescence in Gestational Diabetes Mellitus: A Systematic Review. International Journal of Molecular Sciences. 2025; 26(7):3022. https://doi.org/10.3390/ijms26073022
Chicago/Turabian StyleSalmen, Bianca-Margareta, Delia Reurean-Pintilei, Dan Trofin, Cristiana-Elena Durdu, Alexandra-Cristina Neagu, and Roxana-Elena Bohiltea. 2025. "Investigating the Role of Skin Autofluorescence in Gestational Diabetes Mellitus: A Systematic Review" International Journal of Molecular Sciences 26, no. 7: 3022. https://doi.org/10.3390/ijms26073022
APA StyleSalmen, B.-M., Reurean-Pintilei, D., Trofin, D., Durdu, C.-E., Neagu, A.-C., & Bohiltea, R.-E. (2025). Investigating the Role of Skin Autofluorescence in Gestational Diabetes Mellitus: A Systematic Review. International Journal of Molecular Sciences, 26(7), 3022. https://doi.org/10.3390/ijms26073022