
Predictive Value of Selected Plasma Biomarkers in the Assessment of the Occurrence and Severity of Coronary Artery Disease

 , , ,
, , ,
Abstract
1. Introduction
2. Results
2.1. Baseline Characteristics
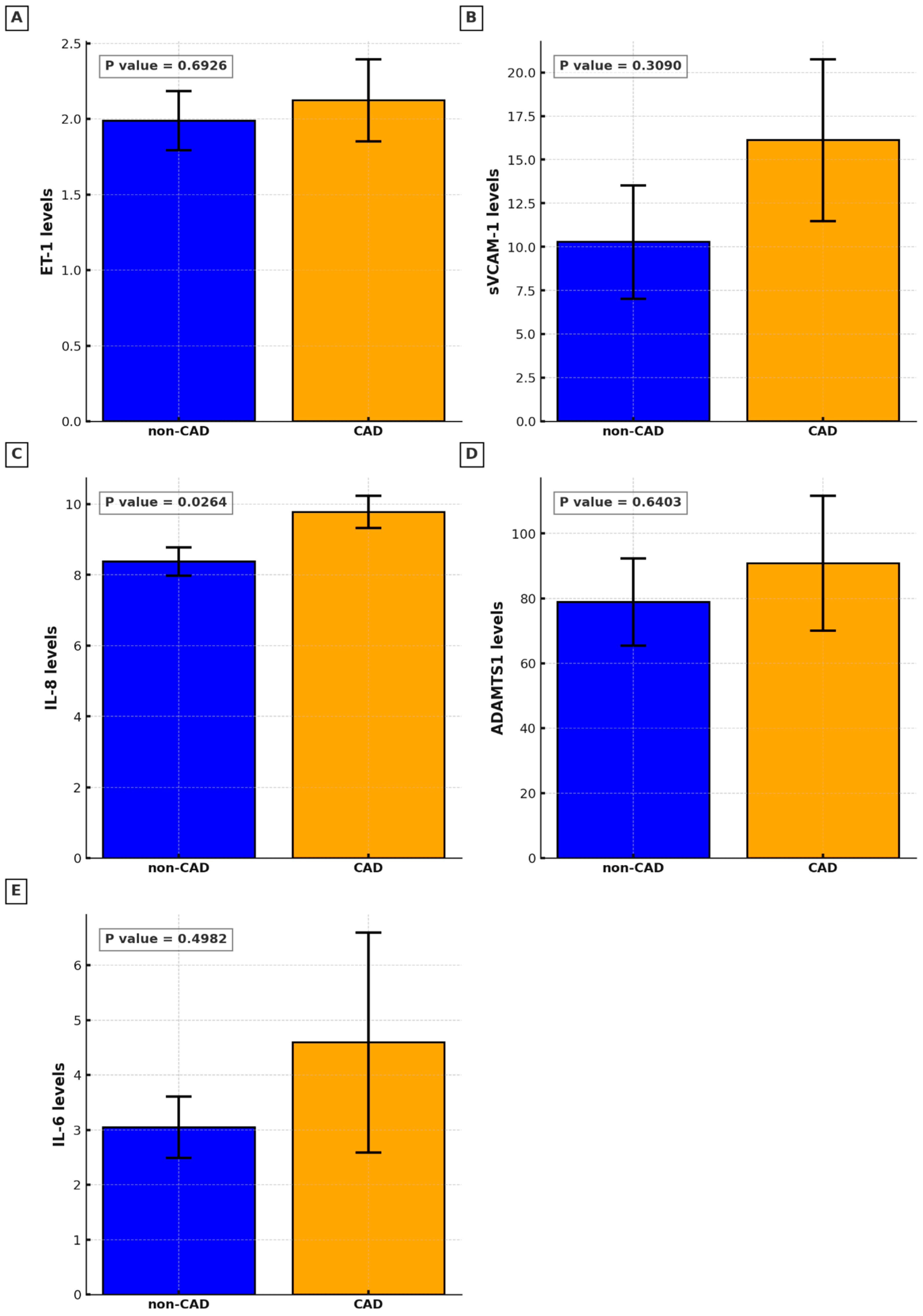
2.2. Circulatory Biomarkers
3. Discussion
Limitations of the Study
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kong, P.; Cui, Z.Y.; Huang, X.F.; Zhang, D.D.; Guo, R.J.; Han, M. Inflammation and atherosclerosis: Signaling pathways and therapeutic intervention. Signal Transduct. Target. Ther. 2022, 7, 131. [Google Scholar] [CrossRef] [PubMed]
- Ciprian Cacuci, A.; Krankenberg, H.; Ingwersen, M.; Gayed, M.; Stein, S.D.; Kretzschmar, D.; Schulze, P.C.; Thieme, M. Access Site Complications of Peripheral Endovascular Procedures: A Large, Prospective Registry on Predictors and Consequences. J. Endovasc. Ther. 2021, 28, 746–754. [Google Scholar] [CrossRef] [PubMed]
- Vrints, C.; Andreotti, F.; Koskinas, K.C.; Rossello, X.; Adamo, M.; Ainslie, J.; Banning, A.P.; Budaj, A.; Buechel, R.R.; Chiariello, G.A.; et al. 2024 ESC Guidelines for the management of chronic coronary syndromes. Eur. Heart J. 2024, 45, 3415–3537. [Google Scholar] [CrossRef]
- Medina-Leyte, D.J.; Zepeda-Garcia, O.; Dominguez-Perez, M.; González-Garrido, A.; Villarreal-Molina, T.; Jacobo-Albavera, L. Endothelial Dysfunction, Inflammation and Coronary Artery Disease: Potential Biomarkers and Promising Therapeutical Approaches. Int. J. Mol. Sci. 2021, 22, 3850. [Google Scholar] [CrossRef] [PubMed]
- Tousoulis, D.; Oikonomou, E.; Economou, E.K.; Crea, F.; Kaski, J.C. Inflammatory cytokines in atherosclerosis: Current therapeutic approaches. Eur. Heart J. 2016, 37, 1723–1732. [Google Scholar] [CrossRef] [PubMed]
- Mai, W.; Liao, Y. Targeting IL-1beta in the Treatment of Atherosclerosis. Front. Immunol. 2020, 11, 589654. [Google Scholar] [CrossRef]
- Romuk, E.; Skrzep-Poloczek, B.; Wojciechowska, C.; Tomasik, A.; Birkner, E.; Wodniecki, J.; Gabrylewicz, B.; Ochala, A.; Tendera, M. Selectin-P and interleukin-8 plasma levels in coronary heart disease patients. Eur. J. Clin. Investig. 2002, 32, 657–661. [Google Scholar] [CrossRef] [PubMed]
- Simonini, A.; Moscucci, M.; Muller, D.W.; Bates, E.R.; Pagani, F.D.; Burdick, M.D.; Strieter, R.M. IL-8 is an angiogenic factor in human coronary atherectomy tissue. Circulation 2000, 101, 1519–1526. [Google Scholar] [CrossRef] [PubMed]
- Inoue, T.; Komoda, H.; Nonaka, M.; Kameda, M.; Uchida, T.; Node, K. Interleukin-8 as an independent predictor of long-term clinical outcome in patients with coronary artery disease. Int. J. Cardiol. 2008, 124, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Wang, C.; Guo, J.; Yang, Y.; Huang, M.; Li, L.; Wang, Y.; Qin, Y.; Zhang, M. Serum Cytokines Predict the Severity of Coronary Artery Disease Without Acute Myocardial Infarction. Front. Cardiovasc. Med. 2022, 9, 896810. [Google Scholar] [CrossRef] [PubMed]
- Fatkhullina, A.R.; Peshkova, I.O.; Koltsova, E.K. The Role of Cytokines in the Development of Atherosclerosis. Biochemistry 2016, 81, 1358–1370. [Google Scholar] [CrossRef] [PubMed]
- Cesari, M.; Penninx, B.W.; Newman, A.B.; Kritchevsky, S.B.; Nicklas, B.J.; Sutton-Tyrrell, K.; Rubin, S.M.; Ding, J.; Simonsick, E.M.; Harris, T.B.; et al. Inflammatory markers and onset of cardiovascular events: Results from the Health ABC study. Circulation 2003, 108, 2317–2322. [Google Scholar] [CrossRef]
- Wolf, D.; Ley, K. Immunity and Inflammation in Atherosclerosis. Circ. Res. 2019, 124, 315–327. [Google Scholar] [CrossRef] [PubMed]
- Apostolakis, S.; Vogiatzi, K.; Amanatidou, V.; Spandidos, D.A. Interleukin 8 and cardiovascular disease. Cardiovasc. Res. 2009, 84, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Ridker, P.M.; Rane, M. Interleukin-6 Signaling and Anti-Interleukin-6 Therapeutics in Cardiovascular Disease. Circ. Res. 2021, 128, 1728–1746. [Google Scholar] [CrossRef] [PubMed]
- Makris, S.; Venetsanou, K.; Spartalis, E.; Kontogiann, C.; Georgiopoulos, G.; Spartalis, M.; Tsilimigras, D.; Moris, D.; Kakisis, I.; Karaolanis, G.; et al. Changes in serum leptin levels as well as sICAM-1 and sVCAM-1 soluble adhesion molecules during carotid endarterectomy. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 2257–2262. [Google Scholar] [CrossRef]
- Helset, E.; Sildnes, T.; Seljelid, R.; Konopski, Z. Endothelin-1 stimulates human monocytes in vitro to release TNF-alpha, IL-1beta and IL-6. Mediat. Inflamm. 1993, 2, 417–422. [Google Scholar] [CrossRef] [PubMed]
- Cheng, M.; Li, Y.; Wu, J.; Nie, Y.; Li, L.; Liu, X.; Charoude, H.N.; Chen, H. IL-8 induces imbalances between nitric oxide and endothelin-1, and also between plasminogen activator inhibitor-1 and tissue-type plasminogen activator in cultured endothelial cells. Cytokine 2008, 41, 9–15. [Google Scholar] [CrossRef]
- Morawietz, H.; Duerrschmidt, N.; Niemann, B.; Galle, J.; Sawamura, T.; Holtz, J. Induction of the oxLDL receptor LOX-1 by endothelin-1 in human endothelial cells. Biochem. Biophys. Res. Commun. 2001, 284, 961–965. [Google Scholar] [CrossRef]
- Babaei, S.; Picard, P.; Ravandi, A.; Monge, J.C.; Lee, T.C.; Cernacek, P.; Stewart, D.J. Blockade of endothelin receptors markedly reduces atherosclerosis in LDL receptor deficient mice: Role of endothelin in macrophage foam cell formation. Cardiovasc. Res. 2000, 48, 158–167. [Google Scholar] [CrossRef] [PubMed]
- Jonsson-Rylander, A.C.; Nilsson, T.; Fritsche-Danielson, R.; Hammarstrom, A.; Behrendt, M.; Andersson, J.O.; Lindgren, K.; Andersson, A.K.; Wallbrandt, P.; Rosengren, B.; et al. Role of ADAMTS-1 in atherosclerosis: Remodeling of carotid artery, immunohistochemistry, and proteolysis of versican. Arterioscler. Thromb. Vasc. Biol. 2005, 25, 180–185. [Google Scholar] [CrossRef] [PubMed]
- Ashlin, T.G.; Kwan, A.P.; Ramji, D.P. Regulation of ADAMTS-1, -4 and -5 expression in human macrophages: Differential regulation by key cytokines implicated in atherosclerosis and novel synergism between TL1A and IL-17. Cytokine 2013, 64, 234–242. [Google Scholar] [CrossRef]
- Qu, Y.; Zhang, N. miR-365b-3p inhibits the cell proliferation and migration of human coronary artery smooth muscle cells by directly targeting ADAMTS1 in coronary atherosclerosis. Exp. Ther. Med. 2018, 16, 4239–4245. [Google Scholar] [CrossRef] [PubMed]
- Pelisek, J.; Deutsch, L.; Ansel, A.; Pongratz, J.; Stadlbauer, T.; Gebhard, H.; Matevossian, E.; Eckstein, H.-H. Expression of a metalloproteinase family of ADAMTS in human vulnerable carotid lesions. J. Cardiovasc. Med. 2017, 18, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Wagsater, D.; Bjork, H.; Zhu, C.; Björkegren, J.; Valen, G.; Hamsten, A.; Eriksson, P. ADAMTS-4 and -8 are inflammatory regulated enzymes expressed in macrophage-rich areas of human atherosclerotic plaques. Atherosclerosis 2008, 196, 514–522. [Google Scholar] [CrossRef] [PubMed]
- Salter, R.C.; Ashlin, T.G.; Kwan, A.P.; Ramji, D.P. ADAMTS proteases: Key roles in atherosclerosis? J. Mol. Med. 2010, 88, 1203–1211. [Google Scholar] [CrossRef]
- Ulucay, S.; Cam, F.S.; Batir, M.B.; Sutcu, R.; Bayturan, O.; Demircan, K. A novel association between TGFb1 and ADAMTS4 in coronary artery disease: A new potential mechanism in the progression of atherosclerosis and diabetes. Anatol. J. Cardiol. 2015, 15, 823–829. [Google Scholar] [CrossRef]
- Wei, M.; Pan, H.; Guo, K. Association Between Plasma ADAMTS-9 Levels and Severity of Coronary Artery Disease. Angiology 2021, 72, 371–380. [Google Scholar] [CrossRef]
- Wang, Z.; Ye, D.; Ye, J.; Wang, M.; Liu, J.; Jiang, H.; Xu, Y.; Zhang, J.; Chen, J.; Wan, J. ADAMTS-5 Decreases in Coronary Arteries and Plasma from Patients with Coronary Artery Disease. Dis. Markers 2019, 2019, 6129748. [Google Scholar] [CrossRef]
- Santamaria, S.; de Groot, R. ADAMTS proteases in cardiovascular physiology and disease. Open Biol. 2020, 10, 200333. [Google Scholar] [CrossRef] [PubMed]
- Novak, R.; Hrkac, S.; Salai, G.; Bilandzic, J.; Mitar, L.; Grgurevic, L. The Role of ADAMTS-4 in Atherosclerosis and Vessel Wall Abnormalities. J. Vasc. Res. 2022, 59, 69–77. [Google Scholar] [CrossRef] [PubMed]
- An, Z.; Li, J.; Yu, J.; Wang, X.; Gao, H.; Zhang, W.; Wei, Z.; Zhang, J.; Zhang, Y.; Zhao, J.; et al. Neutrophil extracellular traps induced by IL-8 aggravate atherosclerosis via activation NF-kappaB signaling in macrophages. Cell Cycle 2019, 18, 2928–2938. [Google Scholar] [CrossRef]
- Li, X.; Guo, D.; Chen, Y.; Hu, Y.; Zhang, F. Effects of Altered Levels of Pro- and Anti-Inflammatory Mediators on Locations of In-Stent Reocclusions in Elderly Patients. Mediat. Inflamm. 2020, 2020, 1719279. [Google Scholar] [CrossRef]
- Kraaijenhof, J.M.; Nurmohamed, N.S.; Tzolos, E.; Meah, M.; Geers, J.; Kaiser, Y.; Kroon, J.; Hovingh, G.K.; Stroes, E.S.G.; Dweck, M.R. Interleukin 6 plasma levels are associated with progression of coronary plaques. Open Heart 2024, 11, e002773. [Google Scholar] [CrossRef] [PubMed]
- Li, K.; Wang, Z.W.; Hu, Z.; Ren, Z.; Hu, X.; Li, L.; Wu, Z.; Wu, H.; Li, B.; Huang, J.; et al. Assessing Serum Levels of ADAMTS1 and ADAMTS4 as New Biomarkers for Patients with Type A Acute Aortic Dissection. Med. Sci. Monit. 2017, 23, 3913–3922. [Google Scholar] [CrossRef] [PubMed]
- Zhou, M.; Dai, W.; Cui, Y.; Liu, H.; Li, Y. Associations between the IL-6-neutralizing sIL-6R-sgp130 buffer system and coronary artery disease in postmenopausal women. Ann. Transl. Med. 2020, 8, 379. [Google Scholar] [CrossRef] [PubMed]
- Kostov, K.; Blazhev, A. Circulating Levels of Endothelin-1 and Big Endothelin-1 in Patients with Essential Hypertension. Pathophysiology 2021, 28, 489–495. [Google Scholar] [CrossRef] [PubMed]
- Kowalska, I.; Straczkowski, M.; Szelachowska, M.; Kinalska, I.; Prokop, J.; Bach, H.; St, A. Circulating E-selectin, vascular cell adhesion molecule-1, and intercellular adhesion molecule-1 in men with coronary artery disease assessed by angiography and disturbances of carbohydrate metabolism. Metabolism 2002, 51, 733–736. [Google Scholar] [CrossRef] [PubMed]
- Ferri, C.; Bellini, C.; Desideri, G.; Baldoncini, R.; Properzi, G.; Santucci, A.; De Mattia, G. Circulating endothelin-1 levels in obese patients with the metabolic syndrome. Exp. Clin. Endocrinol. Diabetes 1997, 105 (Suppl. S2), 38–40. [Google Scholar] [CrossRef] [PubMed]
- Schneider, J.G.; Tilly, N.; Hierl, T.; Sommer, U.; Hamann, A.; Dugi, K.; Leidig-Bruckner, G.; Kasperk, C. Elevated plasma endothelin-1 levels in diabetes mellitus. Am. J. Hypertens. 2002, 15, 967–972. [Google Scholar] [CrossRef] [PubMed]
- Xu, N.; Zhu, P.; Yao, Y.; Jiang, L.; Jia, S.; Yuan, D.; Xu, J.; Wang, H.; Song, Y.; Gao, L.; et al. Big Endothelin-1 and long-term all-cause death in patients with coronary artery disease and prediabetes or diabetes after percutaneous coronary intervention. Nutr. Metab. Cardiovasc. Dis. 2022, 32, 2147–2156. [Google Scholar] [CrossRef] [PubMed]
- Inggriani, M.P.; Musthafa, A.; Puspitawati, I.; Fachiroh, J.; Dewi, F.S.T.; Hartopo, A.B. Increased endothelin-1 levels in coronary artery disease with diabetes mellitus in an Indonesian population. Can. J. Physiol. Pharmacol. 2022, 100, 1097–1105. [Google Scholar] [CrossRef]
- Ebrahimi, N.; Asadikaram, G.; Mohammadi, A.; Jahani, Y.; Moridi, M.; Masoumi, M. The association of endothelin-1 gene polymorphism and its plasma levels with hypertension and coronary atherosclerosis. Arch. Med. Sci. 2021, 17, 613–620. [Google Scholar] [CrossRef] [PubMed]
- Haak, T.; Jungmann, E.; Raab, C.; Usadel, K.H. Elevated endothelin-1 levels after cigarette smoking. Metabolism 1994, 43, 267–269. [Google Scholar] [CrossRef] [PubMed]
- Derella, C.C.; Tingen, M.S.; Blanks, A.; Sojourner, S.J.; Tucker, M.A.; Thomas, J.; Harris, R.A. Smoking cessation reduces systemic inflammation and circulating endothelin-1. Sci. Rep. 2021, 11, 24122. [Google Scholar] [CrossRef] [PubMed]
- De Caterina, R.; Basta, G.; Lazzerini, G.; Dell’omo, G.; Petrucci, R.; Morale, M.; Carmassi, F.; Pedrinelli, R. Soluble vascular cell adhesion molecule-1 as a biohumoral correlate of atherosclerosis. Arterioscler. Thromb. Vasc. Biol. 1997, 17, 2646–2654. [Google Scholar] [CrossRef] [PubMed]
- Peter, K.; Weirich, U.; Nordt, T.K.; Ruef, J.; Bode, C. Soluble vascular cell adhesion molecule-1 (VCAM-1) as potential marker of atherosclerosis. Thromb. Haemost. 1999, 82 (Suppl. S1), 38–43. [Google Scholar] [PubMed]
- Lerman, A.; Holmes, D.R., Jr.; Bell, M.R.; Garratt, K.N.; Nishimura, R.A.; Burnett, J.C., Jr. Endothelin in coronary endothelial dysfunction and early atherosclerosis in humans. Circulation 1995, 92, 2426–2431. [Google Scholar] [CrossRef]
- Yang, C.; Deng, Z.; Li, J.; Ren, Z.; Liu, F. Meta-analysis of the relationship between interleukin-6 levels and the prognosis and severity of acute coronary syndrome. Clinics 2021, 76, e2690. [Google Scholar] [CrossRef]
- Shukor, M.F.A.; Musthafa, Q.A.; Mohd Yusof, Y.A.; Wan Ngah, W.Z.; Ismail, N.A.S. Biomarkers for Premature Coronary Artery Disease (PCAD): A Case Control Study. Diagnostics 2023, 13, 188. [Google Scholar] [CrossRef] [PubMed]
- Abulnaja, K.O.; Kannan, K.; Al-Manzlawi, A.M.K.; Kumosani, T.A.; Qari, M.; Moselhy, S.S. Sensitivity, specificity of biochemical markers for early prediction of endothelial dysfunction in atherosclerotic obese subjects. Afr. Health Sci. 2022, 22, 286–294. [Google Scholar] [CrossRef] [PubMed]
- Varona, J.F.; Ortiz-Regalon, R.; Sanchez-Vera, I.; López-Melgar, B.; García-Durango, C.; Vázquez, J.M.C.; Solís, J.; Fernández-Friera, L.; Vidal-Vanaclocha, F. Soluble ICAM 1 and VCAM 1 Blood Levels Alert on Subclinical Atherosclerosis in Non Smokers with Asymptomatic Metabolic Syndrome. Arch. Med. Res. 2019, 50, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Lin, R.; Junttila, J.; Piuhola, J.; Lepojärvi, E.S.; Magga, J.; Kiviniemi, A.M.; Perkiömäki, J.; Huikuri, H.; Ukkola, O.; Tulppo, M.; et al. Endothelin-1 is associated with mortality that can be attenuated with high intensity statin therapy in patients with stable coronary artery disease. Commun. Med. 2023, 3, 87. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Tian, T.; Wang, T.; Wang, J.; Guan, H.; Yuan, J.; Song, L.; Yang, W.; Qiao, S. Predictive Value of Plasma Big Endothelin-1 in Adverse Events of Patients with Coronary Artery Restenosis and Diabetes Mellitus: Beyond Traditional and Angiographic Risk Factors. Front. Cardiovasc. Med. 2022, 9, 854107. [Google Scholar] [CrossRef]
- Wang, F.; Li, T.; Cong, X.; Hou, Z.; Lu, B.; Zhou, Z.; Chen, X. Association between circulating big endothelin-1 and noncalcified or mixed coronary atherosclerotic plaques. Coron. Artery Dis. 2019, 30, 461–466. [Google Scholar] [CrossRef]
- Mayyas, F.; Ibrahim, K.; Ibdah, R.; Al-Kasasbeh, A.; Ababneh, M.J.; Ababneh, A.A.; Jarrah, M.I.; Rawashdeh, S. Association of plasma endothelin-1 levels with revascularization strategies and short-term clinical outcomes: Role of diabetes. Heliyon 2024, 10, e37777. [Google Scholar] [CrossRef] [PubMed]
- Kazemian, S.; Ahmadi, R.; Rafiei, A.; Azadegan-Dehkordi, F.; Khaledifar, A.; Abdollahpour-Alitappeh, M.; Bagheri, N. The Serum Levels of IL-36 in Patients with Coronary Artery Disease and Their Correlation with the Serum Levels of IL-32, IL-6, TNF-alpha, and Oxidative Stress. Int. Arch. Allergy Immunol. 2022, 183, 1137–1145. [Google Scholar] [CrossRef]
- Ferencik, M.; Mayrhofer, T.; Lu, M.T.; Bittner, D.O.; Emami, H.; Puchner, S.B.; Meyersohn, N.M.; Ivanov, A.V.; Adami, E.C.; Voora, D.; et al. Coronary Atherosclerosis, Cardiac Troponin, and Interleukin-6 in Patients with Chest Pain: The PROMISE Trial Results. JACC Cardiovasc. Imaging 2022, 15, 1427–1438. [Google Scholar] [CrossRef] [PubMed]
- Gilani, S.T.A.; Khan, D.A.; Rauf, A.; Haroon, Z.H.; Khan, K.A.; Hassan, F.U. Early Diagnosis of Coronary Artery Disease by Inflammatory Biomarkers of Atherosclerosis in Patients with Angina. J. Interferon Cytokine Res. 2022, 42, 493–500. [Google Scholar] [CrossRef]
- Liu, S.; Ni, S.; Wang, C.; Yang, K.; Yang, Y.; Li, L.; Liu, J.; Wang, Y.; Qin, Y.; Zhang, M. Association of serum cytokines with coronary chronic total occlusion and their role in predicting procedural outcomes. Hellenic J. Cardiol. 2024, 78, 25–35. [Google Scholar] [CrossRef] [PubMed]
- Netto, J.; Teren, A.; Burkhardt, R.; Willenberg, A.; Beutner, F.; Henger, S.; Schuler, G.; Thiele, H.; Isermann, B.; Thiery, J.; et al. Biomarkers for Non-Invasive Stratification of Coronary Artery Disease and Prognostic Impact on Long-Term Survival in Patients with Stable Coronary Heart Disease. Nutrients 2022, 14, 3433. [Google Scholar] [CrossRef]
- Tsirebolos, G.; Tsoporis, J.N.; Drosatos, I.A.; Izhar, S.; Gkavogiannakis, N.; Sakadakis, E.; Triantafyllis, A.S.; Parker, T.G.; Rallidis, L.S.; Rizos, I. Emerging markers of inflammation and oxidative stress as potential predictors of coronary artery disease. Int. J. Cardiol. 2023, 376, 127–133. [Google Scholar] [CrossRef]
- Newman, J.D.; Anthopolos, R.; Ruggles, K.V.; Cornwell, M.; Reynolds, H.R.; Bangalore, S.; Mavromatis, K.; Held, C.; Wallentin, L.; Kullo, I.J.; et al. Biomarkers and cardiovascular events in patients with stable coronary disease in the ISCHEMIA Trials. Am. Heart J. 2023, 266, 61–73. [Google Scholar] [CrossRef] [PubMed]
- Fadaei, R.; Moradi, N.; Kazemi, T.; Chamani, E.; Azdaki, N.; Moezibady, S.A.; Shahmohamadnejad, S.; Fallah, S. Decreased serum levels of CTRP12/adipolin in patients with coronary artery disease in relation to inflammatory cytokines and insulin resistance. Cytokine 2019, 113, 326–331. [Google Scholar] [CrossRef]
- Moradi, N.; Fouani, F.Z.; Vatannejad, A.; Arani, A.B.; Shahrzad, S.; Fadaei, R. Serum levels of Asprosin in patients diagnosed with coronary artery disease (CAD): A case-control study. Lipids Health Dis. 2021, 20, 88. [Google Scholar] [CrossRef] [PubMed]
- Shokoohi Nahrkhalaji, A.; Ahmadi, R.; Fadaei, R.; Panahi, G.; Razzaghi, M.; Fallah, S. Higher serum level of CTRP15 in patients with coronary artery disease is associated with disease severity, body mass index and insulin resistance. Arch. Physiol. Biochem. 2022, 128, 276–280. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Ye, J.; Wang, M.; Liu, J.; Wang, Z.; Jiang, H.; Ye, D.; Zhang, J.; Wan, J. The expression of interleukin-25 increases in human coronary artery disease and is associated with the severity of coronary stenosis. Anatol. J. Cardiol. 2020, 23, 151–159. [Google Scholar] [CrossRef]
- Kazemi Fard, T.; Tavakoli, S.; Ahmadi, R.; Moradi, N.; Fadaei, R.; Mohammadi, A.; Fallah, S. Evaluation of IP10 and miRNA 296-a Expression Levels in Peripheral Blood Mononuclear Cell of Coronary Artery Disease Patients and Controls. DNA Cell Biol. 2020, 39, 1678–1684. [Google Scholar] [CrossRef] [PubMed]
- Babaee, M.; Chamani, E.; Ahmadi, R.; Bahreini, E.; Balouchnejadmojarad, T.; Nahrkhalaji, A.S.; Fallah, S. The expression levels of miRNAs-27a and 23a in the peripheral blood mononuclear cells (PBMCs) and their correlation with FOXO1 and some inflammatory and anti-inflammatory cytokines in the patients with coronary artery disease (CAD). Life Sci. 2020, 256, 117898. [Google Scholar] [CrossRef]
- Liu, L.; Luo, F. Alterations in the fecal microbiota and serum metabolome in unstable angina pectoris patients. Front. Biosci. (Landmark Ed.) 2022, 27, 100. [Google Scholar] [CrossRef]
- Bouzidi, N.; Gamra, H. Relationship between serum interleukin-6 levels and severity of coronary artery disease undergoing percutaneous coronary intervention. BMC Cardiovasc. Disord. 2023, 23, 586. [Google Scholar] [CrossRef]
- Wainstein, M.V.; Mossmann, M.; Araujo, G.N.; Gonçalves, S.C.; Gravina, G.L.; Sangalli, M.; Veadrigo, F.; Matte, R.; Reich, R.; Costa, F.G.; et al. Elevated serum interleukin-6 is predictive of coronary artery disease in intermediate risk overweight patients referred for coronary angiography. Diabetol. Metab. Syndr. 2017, 9, 67. [Google Scholar] [CrossRef]
- Momot, K.; Zarębiński, M.; Flis, K.; Czarzasta, K.; Puchalska, L.; Wojciechowska, M. Biochemical and clinical evaluation of endothelial injury after distal or traditional transr dial access in percutaneous interventions. Kardiol. Pol. 2022, 80, 651–656. [Google Scholar] [CrossRef]
- Casolo, G.; Gabrielli, D.; Colivicchi, F.; Murrone, A.; Grosseto, D.; Gulizia, M.M.; Di Fusco, S.; Domenicucci, S.; di Uccio, F.S.; Di Tano, G.; et al. ANMCO POSITION PAPER: Prognostic and therapeutic relevance of non-obstructive coronary atherosclerosis. Eur. Heart J. 2021, 23 (Suppl. C), C164–C175. [Google Scholar] [CrossRef] [PubMed]
- Rampidis, G.P.; Benetos, G.; Benz, D.C.; Giannopoulos, A.; Buechel, R. A guide for Gensini Score calculation. Atherosclerosis 2019, 287, 181–183. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Characteristic | CAD (n = 20) | Non-CAD (n = 20) | p Value |
|---|---|---|---|
| Male, n (%) | 15 (75%) | 12 (60%) | ns |
| Age, years (SD) | 69 ± 1.75 | 67 ± 2.11 | ns |
| Obesity, n (%) | 7 (35%) | 8 (40%) | ns |
| BMI, mean (SD) | 28.72 ± 5.32 | 29.73 ± 5.76 | ns |
| Diabetes mellitus, n (%) | 5 (25%) | 9 (45%) | ns |
| Kidney disease, n (%) | 2 (10%) | 0 | ns |
| Hypertension, n (%) | 11 (55) | 13 (65%) | ns |
| Smoking, n (%) | 5 (25%) | 12 (60%) | 0.03 |
| Atrial fibrillation, n (%) | 2 (10%) | 5 (25%) | ns |
| Statin treatment, n (%) | 5 (25%) | 11 (55%) | ns |
| Total Gensini Score, median (IQR) | 21 (7.5–42) | 0 (0–0.25) | <0.0001 |
| Marker | Results |
|---|---|
| IL-8 | IL-8 levels were higher in patients with stable CAD in comparison with healthy subjects. Additionally IL-8 appeared to be a useful clinical predictor of unstable CAD [7] |
| None of the 10 cytokine levels, namely IL-1β, IL-2, IL-4, IL-5, IL-6, IL-8, IL-10, tumor necrosis factor (TNF)-α, granulocyte-macrophage colony stimulating factor (GM-CSF) and interferon-γ (IFN-γ), were correlated with the severity of CAD; however, IL-8 was the only cytokine that predicted long-term cardiovascular outcomes independently of the other cytokines and hs-CRP [9] | |
| IL-6, IL-8, hypercholesterolemia, diabetes mellitus, and hs-CRP independently predict restenosis risk in CAD patients who underwent percutaneous coronary intervention with drug-eluting stents [33] | |
| Patients with atherosclerosis exhibited higher serum levels of IL-8 than healthy controls [32] | |
| IL-8 serum level did not change significantly between severe and non-severe CAD patients. IL-12p70 and IL-17, HDL-C, gender and diabetes were the independent predictors of severe CAD [10] | |
| The lack of association between IL-8 plasma levels and plaque progression in CCTA over a 12-month period in stable CAD patients [34] | |
| sVCAM-1 | Premature CAD (PCAD) patients had significantly higher circulating values of sVCAM-1 that healthy controls; also, older CAD patients showed higher levels of sVCAM-1, CRP, and IL-2 when compared to their age-matched controls. However, after adjusting for multiple parameters, only CRP remained significant for PCAD and IL-2 remained significant for CAD [50] |
| A significant elevation of serum levels of sVCAM-1 along with sICAM-1, E-selectin, ox-LDL and 8-iso-PGF2α in obese with atherosclerosis compared with obese without atherosclerosis or control groups [51] | |
| Compared with controls, metabolic syndrome (MetS) patients had higher prevalence of carotid plaques, which was associated with a remarkable increase in circulating sICAM-1, sVCAM-1 and PAI-1. The increase in sICAM-1, sVCAM-1 and PAI-1, together with decreases in omentin-1, pointed to the presence of subclinical atherosclerosis and improved CVD risk stratification in non-smoking patients at early stage MetS beyond the traditional scores [52] | |
| The lack of association between VCAM-1 plasma levels and plaque progression in CCTA over a 12-month period in stable CAD patients [34] | |
| ET-1 | An association of circulating ET-1 levels with higher risk for all-cause mortality, cardiovascular death, non-cardiovascular death and sudden cardiac death in patients with stable CAD (prognostic value) [53] |
| Baseline high ET-1 levels were independently associated with long-term all-cause death in prediabetes and diabetes patients with CAD undergoing PCI, suggesting that ET-1 may be a valuable marker in patients with impaired glucose metabolism [41] | |
| ET-1 level was significantly higher in CAD patients than in controls. Increased ET-1 level was significantly associated with diabetes mellitus and dyslipidemia in patients with CAD [42] | |
| Increased plasma ET-1 was independently associated with a higher risk of adverse cardiovascular prognosis in patients with in-stent restenosis and diabetes (a predictive biomarker). However, high ET-1 was not significantly associated with the risk of major adverse cardiovascular events in patients without diabetes [54] | |
| ET-1 plasma level was significantly higher in the group of hypertensive patients with atherosclerosis in comparison with the other groups, especially hypertensive patients without atherosclerosis [43] | |
| ET-1 could be an independent predictor for the presence of noncalcified and mixed plaques, which are considered as the high-risk coronary plaques [55] | |
| Plasma ET-1 levels correlated with the severity and progression of CAD and associated with the need for revascularization in DM patients [56] | |
| IL-6 | Higher levels of IL-32, IL-36, TNF-α and IL-6 in the CAD group compared to control [57] |
| Concentrations of hs-cTn and IL-6 were associated with CAD characteristics and MACEs. | |
| hs-cTn was associated with high-risk plaque and IL-6 with significant stenosis. In participants with nonobstructive CAD (stenosis 1–69%), the presence of both hs-cTn and IL-6 above median was strongly associated with MACEs [58] | |
| No association between IL-6 and the severity of CAD [10] | |
| There was a significant positive correlation between IL-6 and the severity of CAD assessed by Gensini score [59] | |
| IL-4, IL-6, and HDL-C levels were strongly associated with chronic total occlusion, and IL-6 was also linked to procedural outcomes of CTO [60] | |
| IL-6 levels positively correlated with the advancement of coronary artery disease and long-term survival [61] | |
| Circulating levels of IL-6 along with sICAM-1, sVCAM-1, E-selectin, ox-LDL and 8-iso-PGF2α are sensitive markers for early prediction of atherosclerosis in obese subjects [50] | |
| CAD patients, especially those with diabetes, have higher levels of IL-6 as compared with controls [62] | |
| After adjusting for age, sex, LVEF, ischemia severity and confirmed multivessel CAD with ≥70% stenosis, each IQR increase in IL-6, hsTnT, GDF-15, NT-proBNP, or sCD40L was individually associated with the primary and secondary outcome [63] | |
| IL-6 levels were higher in CAD patients than in the control group. Moreover, IL-6 levels were positively related to Gensini scores [36] | |
| Serum levels of IL-6 showed higher levels in the CAD group (8.67 ± 3.66 pg/mL) compared to the control group (5.39 ± 1.82 pg/mL; p < 0.001) [64] | |
| Serum TNF-α, and IL-6 levels significantly elevated in CAD group compared to the control group [65] | |
| The blood levels of IL-6 did not differ between patients with atherosclerosis and healthy controls [32] | |
| Serum IL-6 was found to be higher in the CAD group than in the control group [66] | |
| The concentrations of serum IL-25, IL-6 and TNF-α positively correlated with the Gensini Score [67] | |
| IP10, IL-6, and TNF-α levels in CAD patients were significantly higher than those in controls. Concerning positive relationship between miRNA 296-a gene expression level and serum concentrations of IL-6 and TNF-α in CAD patients, it is proposed that IL-6 and TNF-α inhibitor could be the main targets of miRNA 296a and, thereby, the IL-6 and TNF-α levels were increased; however, further study is needed [68] | |
| Serum concentration of IL-6 and TNF-a are significantly increased in the patients with CAD than the healthy controls [69] | |
| Unstable angina pectoris patients had lower serum IGF-1, IGFBP-4, and STC2 and higher serum inflammatory cytokine (hs-CRP, TNF-α, and IL-6) levels than the healthy controls [70] | |
| IL-6 levels were associated with the severity of CAD assessed by the GS. Moreover, based on the highest levels of IL-6 measured in patients with STEMI, the study strongly suggests that IL-6 could be a powerful marker in evaluating myocardial necrosis [71] | |
| In intermediate risk patients referred for coronary angiography, a serum IL-6 level above 1 pg/mL is predictive of significant CAD. IL-6 determination may be useful to reclassify CAD intermediate risk patients into higher risk categories [72] | |
| Plasma IL-6 levels are significantly associated with increased total and noncalcified short-term plaque progression in patients with stable coronary artery disease [34] | |
| None of the 10 cytokine levels, namely: IL-1β, IL-2, IL-4, IL-5, IL-6, IL-8, IL-10, TNF-α, granulocyte-macrophage colony stimulating factor (GM-CSF) and interferon-γ (IFN-γ), were correlated with the severity of CAD [9]. | |
| IL-6 serum level did not change significantly between severe and non-severe CAD patients. IL-12p70 and IL-17, HDL-C, gender and diabetes were the independent predictors of severe CAD [10] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wojciechowska, M.; Nizio, M.; Wróbel, K.; Momot, K.; Czarzasta, K.; Flis, K.; Zarębiński, M. Predictive Value of Selected Plasma Biomarkers in the Assessment of the Occurrence and Severity of Coronary Artery Disease. Int. J. Mol. Sci. 2025, 26, 537. https://doi.org/10.3390/ijms26020537
Wojciechowska M, Nizio M, Wróbel K, Momot K, Czarzasta K, Flis K, Zarębiński M. Predictive Value of Selected Plasma Biomarkers in the Assessment of the Occurrence and Severity of Coronary Artery Disease. International Journal of Molecular Sciences. 2025; 26(2):537. https://doi.org/10.3390/ijms26020537
Chicago/Turabian StyleWojciechowska, Małgorzata, Michał Nizio, Katarzyna Wróbel, Karol Momot, Katarzyna Czarzasta, Krzysztof Flis, and Maciej Zarębiński. 2025. "Predictive Value of Selected Plasma Biomarkers in the Assessment of the Occurrence and Severity of Coronary Artery Disease" International Journal of Molecular Sciences 26, no. 2: 537. https://doi.org/10.3390/ijms26020537
APA StyleWojciechowska, M., Nizio, M., Wróbel, K., Momot, K., Czarzasta, K., Flis, K., & Zarębiński, M. (2025). Predictive Value of Selected Plasma Biomarkers in the Assessment of the Occurrence and Severity of Coronary Artery Disease. International Journal of Molecular Sciences, 26(2), 537. https://doi.org/10.3390/ijms26020537