
Dysregulation of Purinergic Signaling Sustains Chronic Inflammation and Oxidative Imbalance in Patients After PitNET Surgical Resection

 , , , , ,
, , , , ,  ,
,  and
and
Abstract
1. Introduction
2. Results
2.1. Sociodemographic Characteristics of Participants
2.2. Tumor Classification of Patients
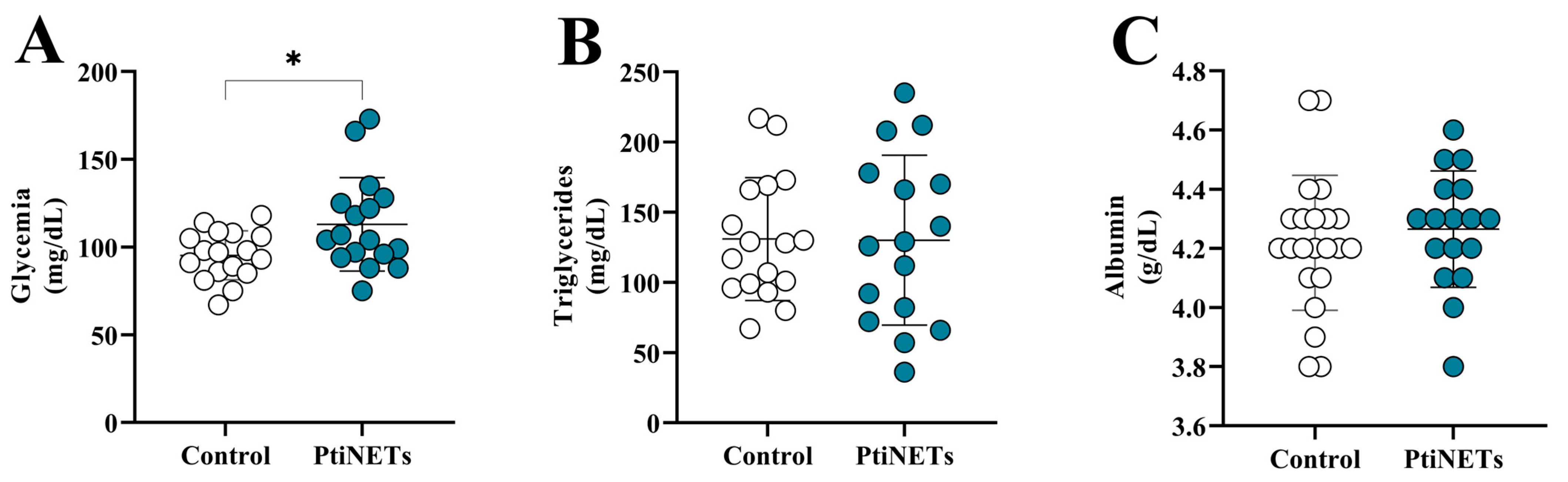
2.3. Levels of Biochemical Markers
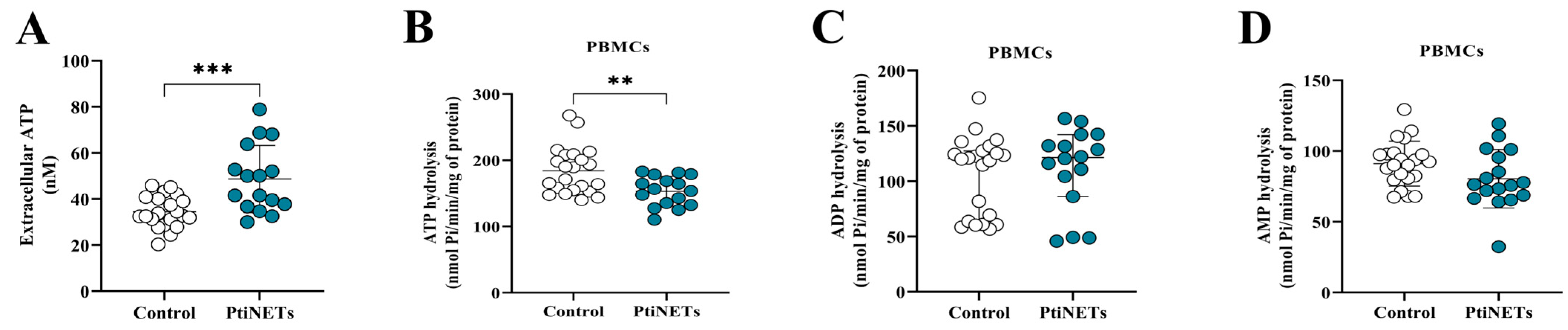
2.4. Patients Presented Purinergic Signaling Alterations
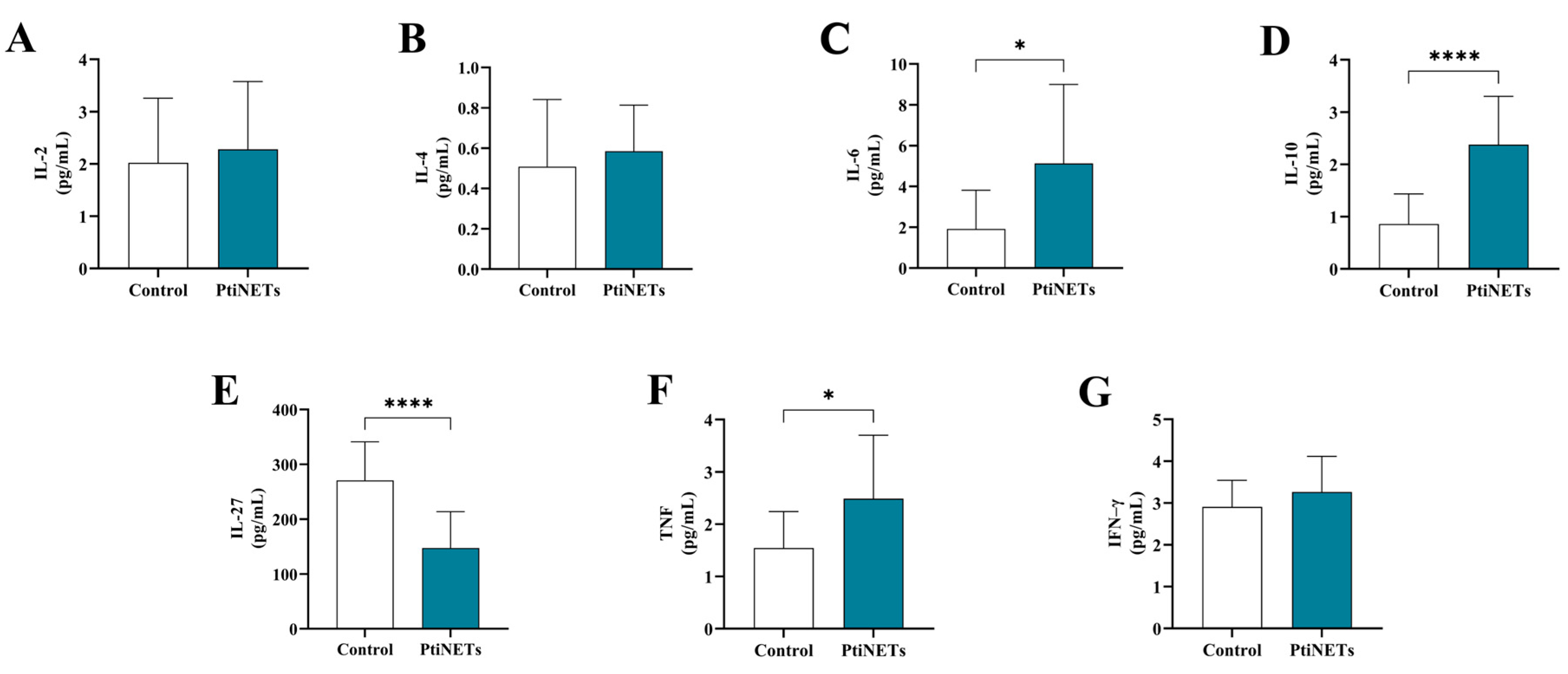
2.5. Patients Had Alterations in Cytokine Profiles
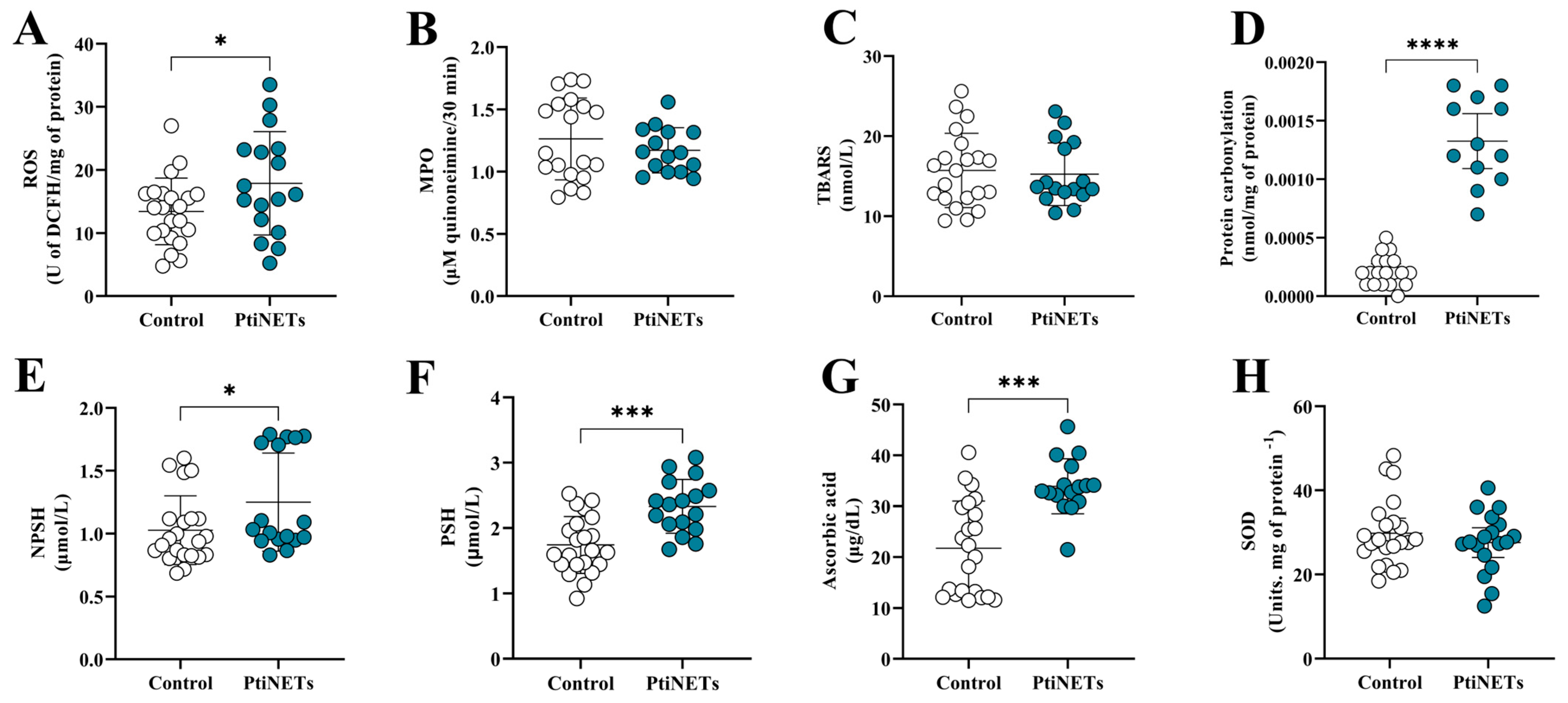
2.6. Patients Had an Imbalance in Their Redox Profiles
3. Discussions
4. Materials and Methods
4.1. Study Design and Participant Selection
4.2. Anthropometric Assessment
4.3. Collection of Biological Material
4.4. Processing of Biological Material and Separation of Peripheral Blood Mononuclear Cells (PBMCs)
4.5. Analysis of Peripheral Biochemical Markers
4.6. Analysis of Purinergic Signaling
4.6.1. Determination of Extracellular ATP (eATP) Levels
4.6.2. Assessment of Enzymatic Activity of Ectonucleotidases
4.7. Analysis of Immunological Profile
4.7.1. Cytokine Determination by Flow Cytometry
4.7.2. Determination of IL–27 Levels
4.8. Analysis of Redox Profile
4.8.1. Reactive Oxygen Species (ROS)
4.8.2. Thiobarbituric Acid Reactive Substances (TBARS) Assay
4.8.3. Myeloperoxidase (MPO) Enzymatic Activity
4.8.4. Protein Carbonylation
4.8.5. Ascorbic Acid (Vitamin C)
4.8.6. Total Thiol (PSH) and Non-Protein Thiol (NPSH)
4.8.7. Superoxide Dismutase (SOD) Enzymatic Activity
4.9. Protein Dosage of Samples
4.10. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability statement
Acknowledgments
Conflicts of Interest
References
- Asa, S.L.; Mete, O.; Cusimano, M.D.; McCutcheon, I.E.; Perry, A.; Yamada, S.; Nishioka, H.; Casar-Borota, O.; Uccella, S.; La Rosa, S.; et al. Pituitary Neuroendocrine Tumors: A Model for Neuroendocrine Tumor Classification. Mod. Pathol. 2021, 34, 1634–1650. [Google Scholar] [CrossRef] [PubMed]
- Daly, A.F.; Beckers, A. The Epidemiology of Pituitary Adenomas. Endocrinol. Metab. Clin. North Am. 2020, 49, 347–355. [Google Scholar] [CrossRef] [PubMed]
- Ostrom, Q.T.; Cioffi, G.; Waite, K.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2014–2018. Neuro-Oncol. 2021, 23, iii1–iii105. [Google Scholar] [CrossRef] [PubMed]
- Tsukamoto, T.; Miki, Y. Imaging of Pituitary Tumors: An Update with the 5th WHO Classifications—Part 1. Pituitary Neuroendocrine Tumor (PitNET)/Pituitary Adenoma. Jpn. J. Radiol. 2023, 41, 789–806. [Google Scholar] [CrossRef] [PubMed]
- Raverot, G.; Ilie, M.D.; Lasolle, H.; Amodru, V.; Trouillas, J.; Castinetti, F.; Brue, T. Aggressive Pituitary Tumours and Pituitary Carcinomas. Nat. Rev. Endocrinol. 2021, 17, 671–684. [Google Scholar] [CrossRef] [PubMed]
- Feola, T.; Carbonara, F.; Verrico, M.; Di Crescenzo, R.M.; Gianno, F.; Colonnese, C.; Arcella, A.; De Alcubierre, D.; Tomao, S.; Esposito, V.; et al. Immunotherapy for Aggressive and Metastatic Pituitary Neuroendocrine Tumors (PitNETs): State-of-the Art. Cancers 2022, 14, 4093. [Google Scholar] [CrossRef] [PubMed]
- Ilie, M.D.; Lasolle, H.; Raverot, G. Emerging and Novel Treatments for Pituitary Tumors. J. Clin. Med. 2019, 8, 1107. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Thornton, L.M.; Shapiro, C.L.; Andersen, B.L. Surviving Recurrence: Psychological and Quality-of-life Recovery. Cancer 2008, 112, 1178–1187. [Google Scholar] [CrossRef] [PubMed]
- Osann, K.; Wenzel, L.; McKinney, C.; Wagner, L.; Cella, D.; Fulci, G.; Scroggins, M.J.; Lankes, H.A.; Wang, V.; Nephew, K.P.; et al. Fear of Recurrence, Emotional Well-Being and Quality of Life among Long-Term Advanced Ovarian Cancer Survivors. Gynecol. Oncol. 2023, 171, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Jimenez-Canizales, C.E.; Rojas, W.; Alonso, D.; Romero, I.; Tabares, S.; Veronesi Zuluaga, L.A.; Modica, R.; Colao, A. Clinical Presentation and Recurrence of Pituitary Neuroendocrine Tumors: Results from a Single Referral Center in Colombia. J. Endocrinol. Investig. 2023, 46, 2275–2286. [Google Scholar] [CrossRef] [PubMed]
- De Marchi, E.; Orioli, E.; Pegoraro, A.; Sangaletti, S.; Portararo, P.; Curti, A.; Colombo, M.P.; Di Virgilio, F.; Adinolfi, E. The P2X7 Receptor Modulates Immune Cells Infiltration, Ectonucleotidases Expression and Extracellular ATP Levels in the Tumor Microenvironment. Oncogene 2019, 38, 3636–3650. [Google Scholar] [CrossRef] [PubMed]
- Kawano, A.; Hayakawa, A.; Kojima, S.; Tsukimoto, M.; Sakamoto, H. Purinergic Signaling Mediates Oxidative Stress in UVA-Exposed THP-1 Cells. Toxicol. Rep. 2015, 2, 391–400. [Google Scholar] [CrossRef] [PubMed]
- Kepp, O.; Bezu, L.; Yamazaki, T.; Di Virgilio, F.; Smyth, M.J.; Kroemer, G.; Galluzzi, L. ATP and Cancer Immunosurveillance. EMBO J. 2021, 40, e108130. [Google Scholar] [CrossRef] [PubMed]
- Haas, C.B.; Lovászi, M.; Braganhol, E.; Pacher, P.; Haskó, G. Ectonucleotidases in Inflammation, Immunity, and Cancer. J. Immunol. 2021, 206, 1983–1990. [Google Scholar] [CrossRef] [PubMed]
- Manica, A.; Da Silva, A.M.; Cardoso, A.M.; Moreno, M.; Leal, D.B.; Dutra Da Silva, A.; Schetinger, M.R.C.; Morsch, V.M.M.; Bagatini, M.D. High Levels of Extracellular ATP Lead to Chronic Inflammatory Response in Melanoma Patients. J. Cell. Biochem. 2018, 119, 3980–3988. [Google Scholar] [CrossRef] [PubMed]
- Mandapathil, M.; Boduc, M.; Roessler, M.; Güldner, C.; Walliczek-Dworschak, U.; Mandic, R. Ectonucleotidase CD39 Expression in Regional Metastases in Head and Neck Cancer. Acta Otolaryngol. (Stockh.) 2018, 138, 428–432. [Google Scholar] [CrossRef] [PubMed]
- Di Virgilio, F.; Vuerich, M. Purinergic Signaling in the Immune System. Auton. Neurosci. 2015, 191, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Burnstock, G.; Boeynaems, J.-M. Purinergic Signalling and Immune Cells. Purinergic Signal. 2014, 10, 529–564. [Google Scholar] [CrossRef] [PubMed]
- Zelentsova, A.S.; Deykin, A.V.; Soldatov, V.O.; Ulezko, A.A.; Borisova, A.Y.; Belyaeva, V.S.; Skorkina, M.Y.; Angelova, P.R. P2X7 Receptor and Purinergic Signaling: Orchestrating Mitochondrial Dysfunction in Neurodegenerative Diseases. eneuro 2022, 9, ENEURO.0092-22.2022. [Google Scholar] [CrossRef] [PubMed]
- Jelic, M.D.; Mandic, A.D.; Maricic, S.M.; Srdjenovic, B.U. Oxidative Stress and Its Role in Cancer. J. Cancer Res. Ther. 2021, 17, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.; Zhou, L.; Duan, J.; Qin, S.; Jiang, J.; Chen, H.; Wang, K.; Liu, R.; Yuan, M.; Tang, X.; et al. Oxidative Stress Promotes Liver Cancer Metastasis via RNF25-Mediated E-Cadherin Protein Degradation. Adv. Sci. 2024, 11, 2306929. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, A.; Patel, A.B.; Kioutchoukova, I.P.; Diaz, M.J.; Lucke-Wold, B. Mechanisms of Mitochondrial Oxidative Stress in Brain Injury: From Pathophysiology to Therapeutics. Oxygen 2023, 3, 163–178. [Google Scholar] [CrossRef]
- Zhou, Y.; Zhang, A.; Fang, C.; Yuan, L.; Shao, A.; Xu, Y.; Zhou, D. Oxidative Stress in Pituitary Neuroendocrine Tumors: Affecting the Tumor Microenvironment and Becoming a New Target for Pituitary Neuroendocrine Tumor Therapy. CNS Neurosci. Ther. 2023, 29, 2744–2759. [Google Scholar] [CrossRef] [PubMed]
- Jafari, E.; Ahmadzadehfar, H.; Bagheri, D.; Amini, A.; Assadi, M. Assessment of Early Oxidative Stress Following the Use of Radiotheranostics Agents 177Lu-PSMA for Prostate Cancer and 177Lu-DOTATATE for Neuroendocrine Tumors; Radioprotective Effect of Vitamin C. Nucl. Med. Commun. 2021, 42, 325–331. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. A Healthy Lifestyle—WHO Recommendations; World Health Organization: Geneva, Switzerland, 2010.
- Trivellin, G.; Hernández-Ramírez, L.C.; Swan, J.; Stratakis, C.A. An Orphan G-Protein-Coupled Receptor Causes Human Gigantism and/or Acromegaly: Molecular Biology and Clinical Correlations. Best Pract. Res. Clin. Endocrinol. Metab. 2018, 32, 125–140. [Google Scholar] [CrossRef] [PubMed]
- Carbonara, F.; Feola, T.; Gianno, F.; Polidoro, M.A.; Di Crescenzo, R.M.; Arcella, A.; De Angelis, M.; Morace, R.; De Alcubierre, D.; Esposito, V.; et al. Clinical and Molecular Characteristics of Gonadotroph Pituitary Tumors According to the WHO Classification. Endocr. Pathol. 2024, 35, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Iyengar, N.M.; Gucalp, A.; Dannenberg, A.J.; Hudis, C.A. Obesity and Cancer Mechanisms: Tumor Microenvironment and Inflammation. J. Clin. Oncol. 2016, 34, 4270–4276. [Google Scholar] [CrossRef] [PubMed]
- Avgerinos, K.I.; Spyrou, N.; Mantzoros, C.S.; Dalamaga, M. Obesity and Cancer Risk: Emerging Biological Mechanisms and Perspectives. Metabolism 2019, 92, 121–135. [Google Scholar] [CrossRef] [PubMed]
- Lochner, R.H.; Delfin, L.; Nezami, B.G.; Cohen, M.L.; Asa, S.L.; Burguera, B.; Couce, M.E. Severe Obesity Associated With Pituitary Corticotroph Hyperplasia and Neoplasia. Endocr. Pract. 2023, 29, 471–477. [Google Scholar] [CrossRef] [PubMed]
- WHO Obesity and Overweight 2024. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 13 July 2025).
- Asa, S.L.; Mete, O.; Perry, A.; Osamura, R.Y. Overview of the 2022 WHO Classification of Pituitary Tumors. Endocr. Pathol. 2022, 33, 6–26. [Google Scholar] [CrossRef] [PubMed]
- Armeni, E.; Grossman, A. The Spectrum of Familial Pituitary Neuroendocrine Tumors. Endocr. Pathol. 2023, 34, 57–78. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, G.B.; Manica, D.; Dallagnol, P.; Narzetti, R.A.; Marafon, F.; Da Silva, A.P.; Matias, L.d.S.; Cassol, J.V.; Moreno, M.; Kempka, A.P.; et al. Rosmarinic Acid Modulates Purinergic Signaling and Induces Apoptosis in Melanoma Cells. Purinergic Signal. 2024, 21, 353–363. [Google Scholar] [CrossRef] [PubMed]
- Zanini, D.; Schmatz, R.; Pimentel, V.C.; Gutierres, J.M.; Maldonado, P.A.; Thomé, G.R.; Cardoso, A.M.; Stefanello, N.; Oliveira, L.; Chiesa, J.; et al. Lung Cancer Alters the Hydrolysis of Nucleotides and Nucleosides in Platelets. Biomed. Pharmacother. 2012, 66, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Dong, C.-R.; Hu, D.-X.; Liu, S.-C.; Luo, H.-L.; Zhang, W.-J. AKT/GSK-3beta/VEGF Signaling Is Involved in P2RY2 Activation-Induced the Proliferation and Metastasis of Gastric Cancer. Carcinogenesis 2023, 44, 65–79. [Google Scholar] [CrossRef] [PubMed]
- Burnstock, G.; Di Virgilio, F. Purinergic Signalling and Cancer. Purinergic Signal. 2013, 9, 491–540. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Chen, E.; Wang, X.; Song, J.; Zhang, H.; Chen, X. An Emerging Master Inducer and Regulator for Epithelial-Mesenchymal Transition and Tumor Metastasis: Extracellular and Intracellular ATP and Its Molecular Functions and Therapeutic Potential. Cancer Cell Int. 2023, 23, 20. [Google Scholar] [CrossRef] [PubMed]
- Di Virgilio, F.; Vultaggio-Poma, V.; Falzoni, S.; Giuliani, A.L. Extracellular ATP: A Powerful Inflammatory Mediator in the Central Nervous System. Neuropharmacology 2023, 224, 109333. [Google Scholar] [CrossRef] [PubMed]
- Di Virgilio, F.; Dal Ben, D.; Sarti, A.C.; Giuliani, A.L.; Falzoni, S. The P2X7 Receptor in Infection and Inflammation. Immunity 2017, 47, 15–31. [Google Scholar] [CrossRef] [PubMed]
- Carlini, V.; Noonan, D.M.; Abdalalem, E.; Goletti, D.; Sansone, C.; Calabrone, L.; Albini, A. The Multifaceted Nature of IL-10: Regulation, Role in Immunological Homeostasis and Its Relevance to Cancer, COVID-19 and Post-COVID Conditions. Front. Immunol. 2023, 14, 1161067. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Yang, H.; Lee, W.S.; Cheon, J.; Sang, Y.B.; Kang, B.; Chon, H.J.; Kim, C. High Levels of Baseline Serum IL-10 Are Associated with Reduced Clinical Benefit from First-Line Immune Checkpoint Inhibitor Therapy in Advanced Renal Cell Carcinoma. J. Cancer 2023, 14, 935–942. [Google Scholar] [CrossRef] [PubMed]
- Czajka-Francuz, P.; Francuz, T.; Cisoń-Jurek, S.; Czajka, A.; Fajkis, M.; Szymczak, B.; Kozaczka, M.; Malinowski, K.P.; Zasada, W.; Wojnar, J.; et al. Serum Cytokine Profile as a Potential Prognostic Tool in Colorectal Cancer Patients–One Center Study. Rep. Pract. Oncol. Radiother. 2020, 25, 867–875. [Google Scholar] [CrossRef] [PubMed]
- Hunter, C.A. New IL-12-Family Members: IL-23 and IL-27, Cytokines with Divergent Functions. Nat. Rev. Immunol. 2005, 5, 521–531. [Google Scholar] [CrossRef] [PubMed]
- Imamichi, T.; Bai, X.-F.; Robinson, C.; Gee, K. Editorial: IL-27 in Health and Disease. Front. Immunol. 2023, 14, 1191228. [Google Scholar] [CrossRef] [PubMed]
- Kountz, T.S.; Jairaman, A.; Kountz, C.D.; Stauderman, K.A.; Schleimer, R.P.; Prakriya, M. Differential Regulation of ATP- and UTP-Evoked Prostaglandin E2 and IL-6 Production from Human Airway Epithelial Cells. J. Immunol. 2021, 207, 1275–1287. [Google Scholar] [CrossRef] [PubMed]
- Nortey, A.; Garces, K.; Hackam, A. Exploring the Role of Interleukin-27 as a Regulator of Neuronal Survival in Central Nervous System Diseases. Neural Regen. Res. 2022, 17, 2149. [Google Scholar] [CrossRef] [PubMed]
- Mascanfroni, I.D.; Yeste, A.; Vieira, S.M.; Burns, E.J.; Patel, B.; Sloma, I.; Wu, Y.; Mayo, L.; Ben-Hamo, R.; Efroni, S.; et al. IL-27 Acts on DCs to Suppress the T Cell Response and Autoimmunity by Inducing Expression of the Immunoregulatory Molecule CD39. Nat. Immunol. 2013, 14, 1054–1063. [Google Scholar] [CrossRef] [PubMed]
- Doseděl, M.; Jirkovský, E.; Macáková, K.; Krčmová, L.; Javorská, L.; Pourová, J.; Mercolini, L.; Remião, F.; Nováková, L.; Mladěnka, P.; et al. Vitamin C—Sources, Physiological Role, Kinetics, Deficiency, Use, Toxicity, and Determination. Nutrients 2021, 13, 615. [Google Scholar] [CrossRef] [PubMed]
- Tossounian, M.-A.; Zhao, Y.; Yu, B.Y.K.; Markey, S.A.; Malanchuk, O.; Zhu, Y.; Cain, A.; Gout, I. Low-Molecular-Weight Thiol Transferases in Redox Regulation and Antioxidant Defence. Redox Biol. 2024, 71, 103094. [Google Scholar] [CrossRef] [PubMed]
- Salbitani, G.; Maresca, V.; Cianciullo, P.; Bossa, R.; Carfagna, S.; Basile, A. Non-Protein Thiol Compounds and Antioxidant Responses Involved in Bryophyte Heavy-Metal Tolerance. Int. J. Mol. Sci. 2023, 24, 5302. [Google Scholar] [CrossRef] [PubMed]
- Manica, D.; Sandri, G.; Da Silva, G.B.; Manica, A.; Da Silva Rosa Bonadiman, B.; Dos Santos, D.; Flores, É.M.M.; Bolzan, R.C.; Barcelos, R.C.S.; Tomazoni, F.; et al. Evaluation of the Effects of Metformin on Antioxidant Biomarkers and Mineral Levels in Patients with Type II Diabetes Mellitus: A Cross-Sectional Study. J. Diabetes Complications 2023, 37, 108497. [Google Scholar] [CrossRef] [PubMed]
- Böyum, A. Isolation of Mononuclear Cells and Granulocytes from Human Blood. Isolation of Monuclear Cells by One Centrifugation, and of Granulocytes by Combining Centrifugation and Sedimentation at 1 g. Scand. J. Clin. Lab. Investig. Suppl. 1968, 97, 77–89. [Google Scholar]
- Lunkes, G.I.; Lunkes, D.; Stefanello, F.; Morsch, A.; Morsch, V.M.; Mazzanti, C.M.; Schetinger, M.R.C. Enzymes That Hydrolyze Adenine Nucleotides in Diabetes and Associated Pathologies. Thromb. Res. 2003, 109, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Pilla, C.; Emanuelli, T.; Frassetto, S.S.; Battastini, A.M.O.; Dias, R.D.; Sarkis, J.J.F. ATP Diphosphohydrolase Activity (Apyrase, EC 3.6.1.5) in Human Blood Platelets. Platelets 1996, 7, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Ali, S.F.; LeBel, C.P.; Bondy, S.C. Reactive Oxygen Species Formation as a Biomarker of Methylmercury and Trimethyltin Neurotoxicity. Neurotoxicology 1992, 13, 637–648. [Google Scholar] [PubMed]
- Jentzsch, A.M.; Bachmann, H.; Fürst, P.; Biesalski, H.K. Improved Analysis of Malondialdehyde in Human Body Fluids. Free Radic. Biol. Med. 1996, 20, 251–256. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, K.; Ota, H.; Sasagawa, S.; Sakatani, T.; Fujikura, T. Assay Method for Myeloperoxidase in Human Polymorphonuclear Leukocytes. Anal. Biochem. 1983, 132, 345–352. [Google Scholar] [CrossRef] [PubMed]
- Wehr, N.B.; Levine, R.L. Quantification of Protein Carbonylation. In Cell Senescence; Galluzzi, L., Vitale, I., Kepp, O., Kroemer, G., Eds.; Methods in Molecular Biology; Humana Press: Totowa, NJ, USA, 2013; ISBN 978-1-62703-238-4. [Google Scholar]
- Jacques-Silva, M.C.; Nogueira, C.W.; Broch, L.C.; Flores, É.M.M.; Rocha, J.B.T. Diphenyl Diselenide and Ascorbic Acid Changes Deposition of Selenium and Ascorbic Acid in Liver and Brain of Mice: DEPOSITION OF SELENIUM AND ASCORBIC ACID IN LIVER AND BRAIN OF MICE. Pharmacol. Toxicol. 2001, 88, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Ellman, G.L. Tissue Sulfhydryl Groups. Arch. Biochem. Biophys. 1959, 82, 70–77. [Google Scholar] [CrossRef] [PubMed]
- McCord, J.M.; Fridovich, I. Superoxide Dismutase. An Enzymic Function for Erythrocuprein (Hemocuprein). J. Biol. Chem. 1969, 244, 6049–6055. [Google Scholar] [CrossRef] [PubMed]
- Bradford, M.M. A Rapid and Sensitive Method for the Quantitation of Microgram Quantities of Protein Utilizing the Principle of Protein-Dye Binding. Anal. Biochem. 1976, 72, 248–254. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject Groups | ||
|---|---|---|
| Characteristics | PitNETs n = 17 | Controls n = 22 |
| Age (years old) | 57.78 ± 13.52 | 51.88 ± 13.62 |
| Gender (%) | ||
| Male | 35.30 (n = 6) | 50.00 (n = 11) |
| Female | 64.70 (n = 11) | 50.00 (n = 11) |
| BMI(kg/m2) * | 30.70 ± 7.61 | 28.79 ± 3.50 |
| Eutrophic | 17.64 (n = 3) | 27.28 (n = 6) |
| Overweight | 52.95 (n = 9) | 31.82 (n = 7) |
| Obesity | 29.41 (n = 5) | 40.90 (n = 9) |
| Baseline chronic diseases (%) | ||
| Arterial hypertension | 23.53 (n = 4) | - |
| Diabetes (type 2) | 5.88 (n = 1) | - |
| Hypothyroidism | 5.88 (n = 1) | - |
| Dyslipidemia | 5.88 (n = 1) | - |
| Arterial hypertension + diabetes (type 2) | 11.76 (n = 2) | - |
| Arterial hypertension + dyslipidemia | 11.76 (n = 2) | - |
| Hypothyroidism + depression | 5.88 (n = 1) | - |
| Arterial hypertension + diabetes (type 2) + dyslipidemia + depression | 5.88 (n = 1) | |
| No disease | 23.53 (n = 4) | - |
| Bad habits (%) | ||
| Smoking | 11.76 (n = 2) | - |
| Alcoholism | 5.88 (n = 1) | - |
| No bad habits | 82.35 (n = 14) | - |
| Tumor Classification | |
|---|---|
| By size | |
| Microadenoma | 5.88% (n = 1) |
| Macroadenoma | 94.11% (n = 16) |
| By histological subtype | |
| Densely granulated somatotroph | 5.88% (n = 1) |
| Somatotroph | 17.64% (n = 3) |
| Sparsely granulated lactotroph | 5.88% (n = 1) |
| Densely granulated lactotroph | 5.88% (n = 1) |
| Densely granulated corticotroph | 11.76% (n = 2) |
| Gonadotroph | 23.52% (n = 4) |
| Multihormonal | 17.64% (n = 3) |
| Null cell | 11.76% (n = 2) |
| By cell lineage | |
| PIT-1 | 35.30% (n = 6) |
| T-PIT | 11.76% (n = 2) |
| SF-1 | 23.52% (n = 4) |
| No distinct cell lineage | 29.41% (n = 5) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fistarol, G.; de Oliveira, L.A.; da Silva, G.B.; Manica, D.; Hanauer, M.C.; Dallagnol, P.; Narzetti, R.A.; Bergamini, M.L.; de Melo, V.C.; Vidal, T.; et al. Dysregulation of Purinergic Signaling Sustains Chronic Inflammation and Oxidative Imbalance in Patients After PitNET Surgical Resection. Int. J. Mol. Sci. 2025, 26, 6890. https://doi.org/10.3390/ijms26146890
Fistarol G, de Oliveira LA, da Silva GB, Manica D, Hanauer MC, Dallagnol P, Narzetti RA, Bergamini ML, de Melo VC, Vidal T, et al. Dysregulation of Purinergic Signaling Sustains Chronic Inflammation and Oxidative Imbalance in Patients After PitNET Surgical Resection. International Journal of Molecular Sciences. 2025; 26(14):6890. https://doi.org/10.3390/ijms26146890
Chicago/Turabian StyleFistarol, Geile, Luiz A. de Oliveira, Gilnei B. da Silva, Daiane Manica, Marceli C. Hanauer, Paula Dallagnol, Rafael A. Narzetti, Maria L. Bergamini, Vitória C. de Melo, Tais Vidal, and et al. 2025. "Dysregulation of Purinergic Signaling Sustains Chronic Inflammation and Oxidative Imbalance in Patients After PitNET Surgical Resection" International Journal of Molecular Sciences 26, no. 14: 6890. https://doi.org/10.3390/ijms26146890
APA StyleFistarol, G., de Oliveira, L. A., da Silva, G. B., Manica, D., Hanauer, M. C., Dallagnol, P., Narzetti, R. A., Bergamini, M. L., de Melo, V. C., Vidal, T., Pillat, M. M., de Lima, J., da Cunha, M. L. V., Makiyama, M. L., Marafon, F., Kempka, A. P., Zamoner, A., & Bagatini, M. D. (2025). Dysregulation of Purinergic Signaling Sustains Chronic Inflammation and Oxidative Imbalance in Patients After PitNET Surgical Resection. International Journal of Molecular Sciences, 26(14), 6890. https://doi.org/10.3390/ijms26146890