

Neuroactive Steroids as Novel Promising Drugs in Therapy of Postpartum Depression—Focus on Zuranolone


Abstract
1. Postpartum Depression
2. Current Therapeutic Approaches for PPD
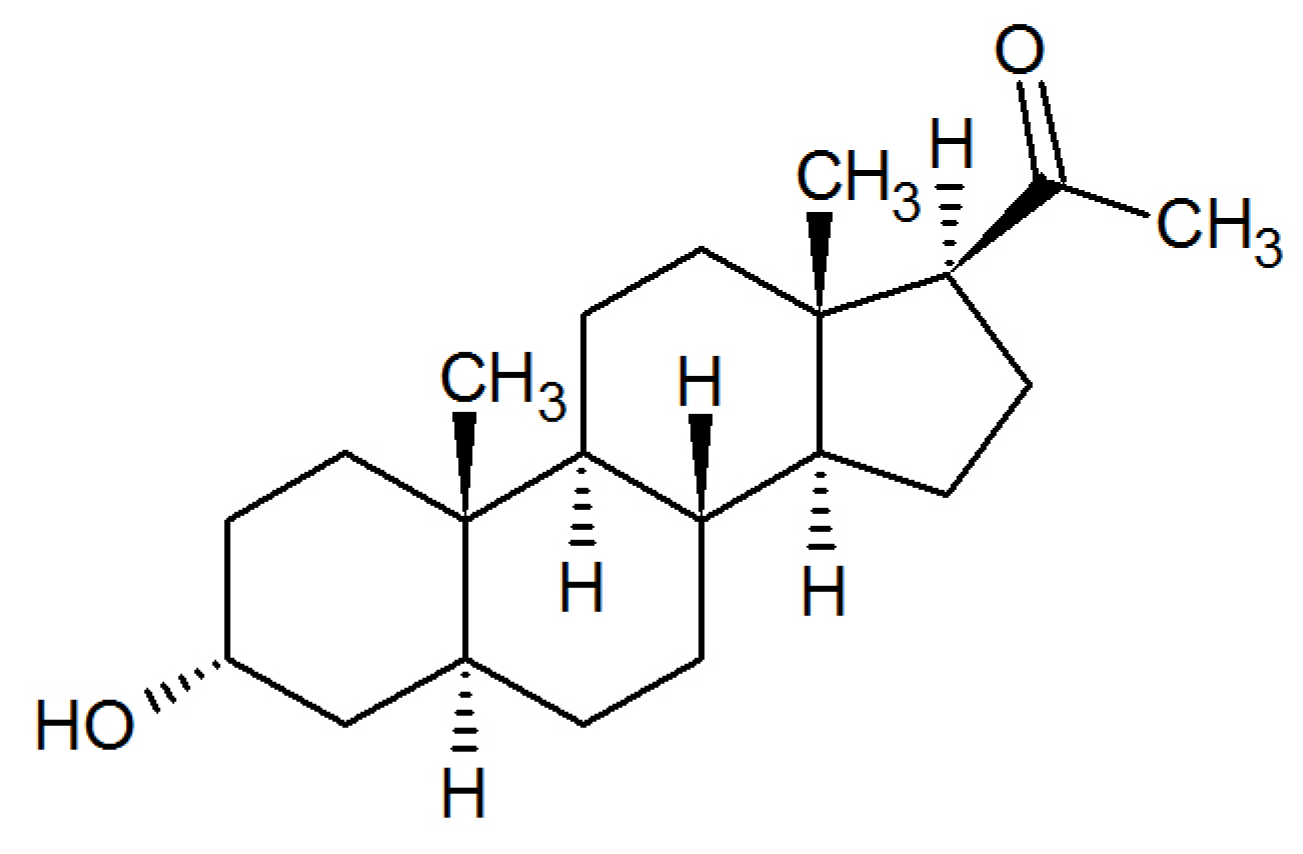
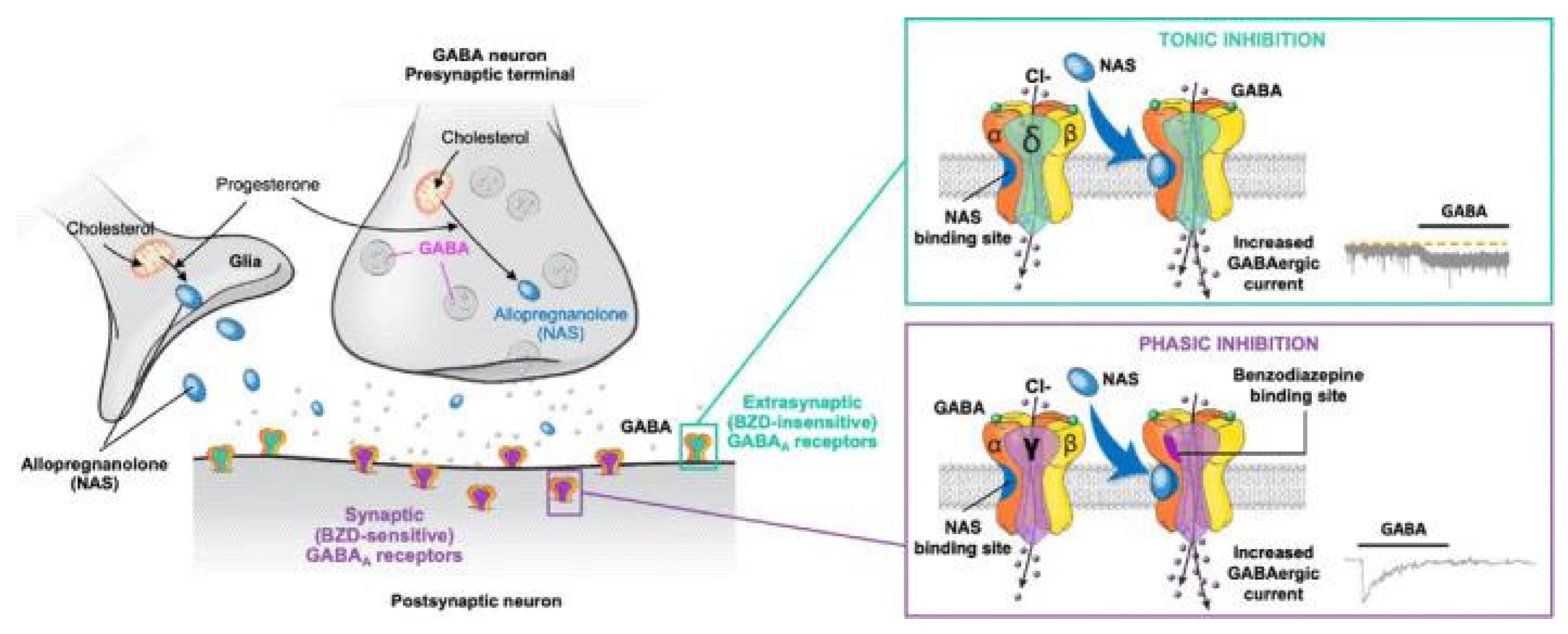
3. In Search of New Drugs for PPD—Neuroactive Steroids and GABAergic Signaling Hypothesis
4. Neuroactive Steroids as Novel Promising Drugs in Therapy of PPD
4.1. Brexanolone
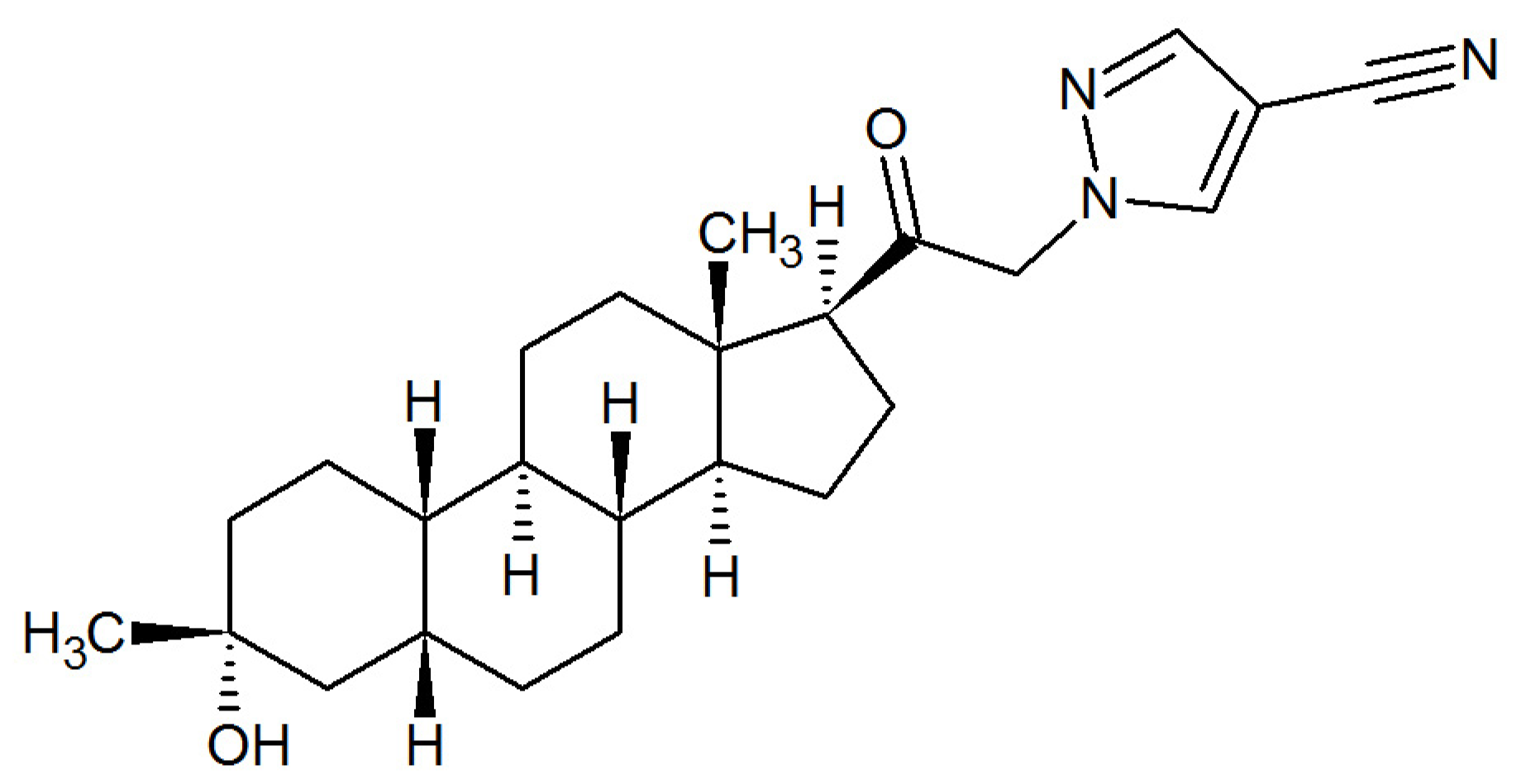
4.2. Zuranolone (ZURZUVAE™)—The First FDA-Approved Oral Neuroactive Steroid-Based Antidepressant for PPD
4.2.1. Zuranolone—Preclinical Studies
4.2.2. Zuranolone—Clinical Studies
Pharmacokinetic Parameters of Zuranolone in Humans
Therapeutical Effects and Safety of Zuranolone
5. Concluding Remarks
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AUC | Area under curve |
| CFB | Change from baseline |
| CGI-I | The Clinical Global Impression-Improvement |
| CL/F | Apparent clearance |
| Cmax | Maximum plasma concentration |
| DSM-5 | Diagnostic and Statistical Manual of Mental Disorders—Fifth Edition |
| Emax | Maximum efficacy |
| EPDS | Edinburgh Postnatal Depression Scale |
| FDA | Food and Drug Administration |
| GABA | Gamma aminobutyric acid |
| GABAARs | GABAA receptors |
| HAMD17 | 17-item Hamilton Rating Scale for Depression |
| HAMD | Hamilton Depression Rating Scale |
| IP | Intraperitoneally |
| MAD | Multiple ascending dose |
| MADRS | Montgomery–Åsberg Depression Rating Scale |
| MDD | Major depressive disorder |
| NAS | Neuroactive steroid |
| PAMs | Positive allosteric modulators |
| PO | Per os |
| PPD | Postpartum depression |
| RID | Relative infant dose |
| SAD | Single ascending dose |
| SDLP | Standard deviation of lateral position |
| SF-36 | 36-Item Short Form Health Survey |
| SNRIs | Serotonin and noradrenaline reuptake inhibitors |
| SSRIs | Selective serotonin reuptake inhibitors |
| t1/2 | Half-life time |
| TCAs | Tricyclic antidepressants |
| tmax | Time to reach maximum concentration |
References
- World Health Organization. Depressive Disorder (Depression); WHO: Geneva, Switzerland, 2023; Available online: https://www.who.int/news-room/fact-sheets/detail/depression (accessed on 14 February 2025).
- Balaram, K.; Marwaha, R. Postpartum Blues. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2022; Available online: https://psychiatryonline.org/doi/book/10.1176/appi.books.9780890425787 (accessed on 14 February 2025).
- ACOG Committee on Clinical Practice Guidelines–Obstetrics. Screening and diagnosis of mental health conditions during pregnancy and postpartum. Clinical Practice Guideline No. 4. American College of Obstetricians and Gynecologists. Obstet. Gynecol. 2023, 141, 1232–1261. [Google Scholar] [CrossRef] [PubMed]
- Bai, Y.; Li, Q.; Cheng, K.K.; Caine, E.D.; Tong, Y.; Wu, X.; Gong, W. Prevalence of Postpartum Depression Based on Diagnostic Interviews: A Systematic Review and Meta-Analysis. Depress. Anxiety 2023, 2023, 8403222. [Google Scholar] [CrossRef] [PubMed]
- Radoš, S.N.; Akik, B.K.; Žutić, M.; Rodriguez-Muñoz, M.F.; Uriko, K.; Motrico, E.; Moreno-Peral, P.; Apter, G.; den Berg, M.L. Diagnosis of peripartum depression disorder: A state-of-the-art approach from the COST Action Riseup-PPD. Compr. Psychiatry 2024, 130, 152456. [Google Scholar] [CrossRef]
- Ko, J.Y.; Farr, S.L.; Dietz, P.M.; Robbins, C.L. Depression and treatment among U.S. pregnant and nonpregnant women of reproductive age, 2005–2009. J. Womens Health 2012, 21, 830–836. [Google Scholar] [CrossRef]
- Yim, I.S.; Tanner Stapleton, L.R.; Guardino, C.M.; Hahn-Holbrook, J.; Dunkel Schetter, C. Biological and psychosocial predictors of postpartum depression: Systematic review and call for integration. Annu. Rev. Clin. Psychol. 2015, 11, 99–137. [Google Scholar] [CrossRef]
- Matsumura, K.; Hamazaki, K.; Tsuchida, A.; Kasamatsu, H.; Inadera, H.; Japan Environment and Children’s Study (JECS) Group. Education level and risk of postpartum depression: Results from the Japan Environment and Children’s Study (JECS). BMC Psychiatry 2019, 19, 419. [Google Scholar] [CrossRef]
- Bauman, B.L.; Ko, J.Y.; Cox, S.; D’Angelo, D.V.; Warner, L.; Folger, S.; Tevendale, H.D.; Coy, K.C.; Harrison, L.; Barfield, W.D. Vital Signs: Postpartum Depressive Symptoms and Provider Discussions About Perinatal Depression—United States, 2018. MMWR Morb. Mortal. Wkly Rep. 2020, 69, 575–581. [Google Scholar] [CrossRef]
- Shi, X.; Ying, Y.; Yu, Z.; Xing, M.; Zhu, J.; Feng, W.; Xu, D.; Zhang, W.; Zhou, M.; Wang, J.; et al. Risk factors for postpartum depression in Chinese women: A cross-sectional study at 6 weeks postpartum. J. Psychosom. Res. 2021, 140, 110295. [Google Scholar] [CrossRef]
- Walker, A.L.; de Rooij, S.R.; Dimitrova, M.V.; Witteveen, A.B.; Verhoeven, C.J.; de Jonge, A.; Vrijkotte, T.G.; Henrichs, J. Psychosocial and peripartum determinants of postpartum depression: Findings from a prospective population-based cohort. The ABCD study. Compr. Psychiatry 2021, 108, 152239. [Google Scholar] [CrossRef]
- Liu, X.; Wang, S.; Wang, G. Prevalence and risk factors of postpartum depression in women: A systematic review and meta-analysis. J. Clin. Nurs. 2022, 31, 2665–2677. [Google Scholar] [CrossRef]
- Della Corte, L.; La Rosa, V.L.; Cassinese, E.; Ciebiera, M.; Zaręba, K.; De Rosa, N.; Verrazzo, P.; Improda, F.P.; Vitale, S.G.; Giampaolino, P.; et al. Prevalence and associated psychological risk factors of postpartum depression: A cross-sectional study. J. Obstet. Gynaecol. 2022, 42, 976–980. [Google Scholar] [CrossRef] [PubMed]
- Justesen, K.; Jourdaine, D. Peripartum Depression: Detection and Treatment. Am. Fam. Physician 2023, 108, 267–272. [Google Scholar] [PubMed]
- Sharma, V. Peripartum anxiety: Parsing heterogeneity in clinical settings. Braz. J. Psychiatry 2022, 441, 4–5. [Google Scholar] [CrossRef]
- Sit, D.; Luther, J.; Buysse, D.; Dills, J.L.; Eng, H.; Okun, M.; Wisniewski, S.; Wisner, K.L. Suicidal ideation in depressed postpartum women: Associations with childhood trauma, sleep disturbance and anxiety. J. Psychiatr. Res. 2015, 66–67, 95–104. [Google Scholar] [CrossRef]
- Orsolini, L.; Valchera, A.; Vecchiotti, R.; Tomasetti, C.; Iasevoli, F.; Fornaro, M.; De Berardis, D.; Perna, G.; Pompili, M.; Bellantuono, C. Suicide during Perinatal Period: Epidemiology, Risk Factors, and Clinical Correlates. Front. Psychiatry 2016, 7, 138. [Google Scholar] [CrossRef]
- Eastwood, J.G.; Jalaludin, B.B.; Kemp, L.A.; Phung, H.N.; Barnett, B.E. Relationship of postnatal depressive symptoms to infant temperament, maternal expectations, social support and other potential risk factors: Findings from a large Australian cross-sectional study. BMC Pregnancy Childbirth 2012, 12, 148. [Google Scholar] [CrossRef]
- Lilja, G.; Edhborg, M.; Nissen, E. Depressive mood in women at childbirth predicts their mood and relationship with infant and partner during the first year postpartum. Scand. J. Caring Sci. 2012, 26, 245–253. [Google Scholar] [CrossRef]
- Vismara, L.; Rollè, L.; Agostini, F.; Sechi, C.; Fenaroli, V.; Molgora, S.; Neri, E.; Prino, L.E.; Odorisio, F.; Trovato, A.; et al. Perinatal Parenting Stress, Anxiety, and Depression Outcomes in First-Time Mothers and Fathers: A 3- to 6-Months Postpartum Follow-Up Study. Front. Psychol. 2016, 7, 938. [Google Scholar] [CrossRef]
- Kerstis, B.; Aarts, C.; Tillman, C.; Persson, H.; Engström, G.; Edlund, B.; Öhrvik, J.; Sylvén, S.; Skalkidou, A. Association between parental depressive symptoms and impaired bonding with the infant. Arch. Womens Ment. Health 2016, 19, 87–94. [Google Scholar] [CrossRef]
- Saharoy, R.; Potdukhe, A.; Wanjari, M.; Taksande, A.B. Postpartum Depression and Maternal Care: Exploring the Complex Effects on Mothers and Infants. Cureus 2023, 15, e41381. [Google Scholar] [CrossRef]
- Pearson, R.M.; Evans, J.; Kounali, D.; Lewis, G.; Heron, J.; Ramchandani, P.G.; O’Connor, T.G.; Stein, A. Maternal depression during pregnancy and the postnatal period: Risks and possible mechanisms for offspring depression at age 18 years. JAMA Psychiatry 2013, 70, 1312–1319. [Google Scholar] [CrossRef] [PubMed]
- Woolhouse, H.; Gartland, D.; Mensah, F.; Giallo, R.; Brown, S. Maternal depression from pregnancy to 4 years postpartum and emotional/behavioural difficulties in children: Results from a prospective pregnancy cohort study. Arch. Womens Ment. Health 2016, 19, 141–151. [Google Scholar] [CrossRef] [PubMed]
- Netsi, E.; Pearson, R.M.; Murray, L.; Cooper, P.; Craske, M.G.; Stein, A. Association of Persistent and Severe Postnatal Depression with Child Outcomes. JAMA Psychiatry 2018, 75, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Slomian, J.; Honvo, G.; Emonts, P.; Reginster, J.Y.; Bruyère, O. Consequences of maternal postpartum depression: A systematic review of maternal and infant outcomes. Womens Health 2019, 15, 1745506519844044. [Google Scholar] [CrossRef]
- Rogers, A.; Obst, S.; Teague, S.J.; Rossen, L.; Spry, E.A.; Macdonald, J.A.; Sunderland, M.; Olsson, C.A.; Youssef, G.; Hutchinson, D. Association Between Maternal Perinatal Depression and Anxiety and Child and Adolescent Development: A Meta-analysis. JAMA Pediatr. 2020, 174, 1082–1092. [Google Scholar] [CrossRef]
- Schwarze, C.E.; Lerche, V.; Wallwiener, S.; Pauen, S. Partnership quality and maternal depressive symptoms in the transition to parenthood: A prospective cohort study. BMC Pregnancy Childbirth. 2024, 4, 664. [Google Scholar] [CrossRef]
- Torres, A.; Gelabert, E.; Roca, A.; Navarro, P.; Plaza, A.; Subirà, S.; Martin-Santos, R.; Ascaso, C.; Garcia-Esteve, L. Course of a major postpartum depressive episode: A prospective 2 years naturalistic follow-up study. J. Affect. Disord. 2019, 245, 965–970. [Google Scholar] [CrossRef]
- Vliegen, N.; Casalin, S.; Luyten, P. The course of postpartum depression: A review of longitudinal studies. Harv. Rev. Psychiatry 2014, 22, 1–22. [Google Scholar] [CrossRef]
- Zhang, K.; He, L.; Li, Z.; Ding, R.; Han, X.; Chen, B.; Cao, G.; Ye, J.H.; Li, T.; Fu, R. Bridging Neurobiological Insights and Clinical Biomarkers in Postpartum Depression: A Narrative Review. Int. J. Mol. Sci. 2024, 25, 8835. [Google Scholar] [CrossRef]
- Dennis, C.L.; Dowswell, T. Psychosocial and psychological interventions for preventing postpartum depression. Cochrane Database Syst. Rev. 2013, 2, Cd001134. [Google Scholar] [CrossRef]
- Zlotnick, C.; Tzilos, G.; Miller, I.; Seifer, R.; Stout, R. Randomized controlled trial to prevent postpartum depression in mothers on public assistance. J. Affect. Disord. 2016, 189, 263–268. [Google Scholar] [CrossRef] [PubMed]
- Genovez, M.; Vanderkruik, R.; Lemon, E.; Dimidjian, S. Psychotherapeutic treatments for depression during pregnancy. Clin. Obstet. Gynecol. 2018, 61, 562–572. [Google Scholar] [CrossRef] [PubMed]
- Motrico, E.; Moreno-Peral, P.; Uriko, K.; Hancheva, C.; Brekalo, M.; Ajaz, E.; Apter, G.; Bramante, A.; Conejo-Cerón, S.; Christoforou, A.; et al. Clinical practice guidelines with recommendations for peripartum depression: A European systematic review. Acta Psychiatr. Scand. 2022, 146, 325–339. [Google Scholar] [CrossRef]
- Sushmitha, G.; Eashwar, V.M.A.; Pandian, S.; Albert Sekhar, M.; Pricilla, S.E. Non-pharmacological Radical Methods for Treating Postpartum Depression Around the Globe: A Narrative Review. Cureus 2024, 16, e76052. [Google Scholar] [CrossRef]
- Hamon, M.; Blier, P. Monoamine neurocircuitry in depression and strategies for new treatments. Prog. Neuropsychopharmacol. Biol. Psychiatry 2013, 45, 54–63. [Google Scholar] [CrossRef]
- McEvoy, K.; Payne, J.L.; Osborne, L.M. Neuroactive steroids and perinatal depression: A review of recent literature. Curr. Psychiatry Rep. 2018, 20, 78. [Google Scholar] [CrossRef]
- Meltzer-Brody, S.; Kanes, S.J. Allopregnanolone in postpartum depression: Role in pathophysiology and treatment. Neurobiol. Stress 2020, 12, 100212. [Google Scholar] [CrossRef]
- Brown, J.V.E.; Wilson, C.A.; Ayre, K.; Robertson, L.; South, E.; Molyneaux, E.; Trevillion, K.; Howard, L.M.; Khalifeh, H. Antidepressant treatment for postnatal depression. Cochrane Database Syst. Rev. 2021, 2, CD013560. [Google Scholar] [CrossRef]
- Giannopoulos, A.; Singh, J.; Deligiannidis, K.M. Clinical Utility of Zuranolone for Postpartum Depression: A Narrative Review. Neuropsychiatr. Dis. Treat. 2025, 21, 93–105. [Google Scholar] [CrossRef]
- Patterson, R.; Balan, I.; Morrow, A.L.; Meltzer-Brody, S. Novel neurosteroid therapeutics for post-partum depression: Perspectives on clinical trials, program development, active research, and future directions. Neuropsychopharmacology 2024, 49, 67–72. [Google Scholar] [CrossRef]
- Powell, J.G.; Garland, S.; Preston, K.; Piszczatoski, C. Brexanolone (Zulresso): Finally, an FDA-approved treatment for postpartum depression. Ann. Pharmacother. 2020, 54, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Heo, Y.A. Zuranolone: First approval. Drugs 2023, 83, 1559–1567. [Google Scholar] [CrossRef] [PubMed]
- Chu, A.; Wadhwa, R. Selective Serotonin Reuptake Inhibitors. In StatPearls [Internet]; [Updated 1 May 2023]; StatPearls Publishing: Treasure Island, FL, USA, 2025. [Google Scholar]
- SNRIs (Serotonin and Norepinephrine Reuptake Inhibitors). Available online: https://my.clevelandclinic.org/health/treatments/24797-snri (accessed on 26 June 2025).
- Moraczewski, J.; Awosika, A.O.; Aedma, K.K. Tricyclic Antidepressants. In StatPearls [Internet]; [Updated 17 August 2023]; StatPearls Publishing: Treasure Island, FL, USA, 2025. [Google Scholar]
- Mohamad, F.H.; Mohamad Jamali, M.A.; Che Has, A.T. Structure-function Studies of GABA (A) Receptors and Related computer-aided Studies. J. Mol. Neurosci. 2023, 73, 804–817. [Google Scholar] [CrossRef]
- Ghit, A.; Assal, D.; Al-Shami, A.S.; Hussein, D.E.E. GABAA receptors: Structure, function, pharmacology, and related disorders. J. Genet. Eng. Biotechnol. 2021, 19, 123. [Google Scholar] [CrossRef]
- Pinna, G.; Almeida, F.B.; Davis, M. Allopregnanolone in Postpartum Depression. Front. Glob. Womens Health 2022, 3, 823616. [Google Scholar] [CrossRef]
- Grötsch, M.K.; Ehlert, U. Allopregnanolone in the peripartum: Correlates, concentrations, and challenges—A systematic review. Psychoneuroendocrinolgy 2024, 166, 107081. [Google Scholar] [CrossRef]
- Deligiannidis, K.M.; Kroll-Desrosiers, A.R.; Mo, S.; Nguyen, H.; Svenson, A.; Jaitly, N.; Hall, J.E.; Barton, B.A.; Rothschild, A.J.; Shaffer, S.A. Peripartum neuroactive steroid and γ-aminobutyric acid profiles in women at-risk for postpartum depression. Psychoneuroendocrinology 2016, 70, 98–107. [Google Scholar] [CrossRef]
- Purdy, R.H.; Morrow, A.L.; Moore, P.H., Jr.; Paul, S.M. Stress-induced elevations of gamma-aminobutyric acid type A receptor-active steroids in the rat brain. Proc. Natl. Acad. Sci. USA 1991, 88, 4553–4557. [Google Scholar] [CrossRef]
- Walton, N.L.; Antonoudiou, P.; Barros, L.; Dargan, T.; DiLeo, A.; Evans-Strong, A.; Gabby, J.; Howard, S.; Paracha, R.; Sánchez, E.J.; et al. Impaired Endogenous Neurosteroid Signaling Contributes to Behavioral Deficits Associated with Chronic Stress. Biol. Psychiatry 2023, 94, 249–261. [Google Scholar] [CrossRef]
- Porcu, P.; Barron, A.M.; Frye, C.A.; Walf, A.A.; Yang, S.Y.; He, X.Y.; Morrow, A.L.; Panzica, G.C.; Melcangi, R.C. Neurosteroidogenesis Today: Novel Targets for Neuroactive Steroid Synthesis and Action and Their Relevance for Translational Research. J. Neuroendocrinol. 2016, 28, 12351. [Google Scholar] [CrossRef]
- Paul, S.M.; Purdy, R.H. Neuroactive steroids. FASEB J. 1992, 6, 2311–2322. [Google Scholar] [CrossRef] [PubMed]
- Zorumski, C.F.; Covey, D.F.; Izumi, Y.; Evers, A.S.; Maguire, J.L.; Mennerick, S.J. New directions in neurosteroid therapeutics in neuropsychiatry. Neurosci. Biobehav. Rev. 2025, 172, 106119. [Google Scholar] [CrossRef] [PubMed]
- Sarkar, J.; Wakefield, S.; MacKenzie, G.; Moss, S.J.; Maguire, J. Neurosteroidogenesis is required for the physiological response to stress: Role of neurosteroid-sensitive GABAA receptors. J. Neurosci. 2011, 31, 18198–18210. [Google Scholar] [CrossRef] [PubMed]
- Crowley, S.K.; Girdler, S.S. Neurosteroid, GABAergic and hypothalamic pituitary adrenal (HPA) axis regulation: What is the current state of knowledge in humans? Psychopharmacology 2014, 231, 3619–3634. [Google Scholar] [CrossRef]
- Diotel, N.; Charlierm, T.D.; Lefebvre d’Hellencourt, C.; Couret, D.; Trudeau, V.L.; Nicolau, J.C.; Meilhac, O.; Kah, O.; Pellegrini, E. Steroid transport, local synthesis, and signaling within the brain: Roles in neurogenesis, neuroprotection, and sexual behaviors. Front. Neurosci. 2018, 12, 84. [Google Scholar] [CrossRef]
- Murugan, S.; Jakka, P.; Namani, S.; Mujumdar, V.; Radhakrishnan, G. The neurosteroid pregnenolone promotes degradation of key proteins in the innate immune signaling to suppress inflammation. J. Biol. Chem. 2019, 294, 4596–4607. [Google Scholar] [CrossRef]
- Balan, I.; Beattie, M.C.; O’Buckley, T.K.; Aurelian, L.; Morrow, A.L. Endogenous neurosteroid (3⍺,5⍺)3-hydroxypregnan-20-one inhibits toll-like-4 receptor activation and pro-inflammatory signaling in macrophages and brain. Sci. Rep. 2019, 9, 1220. [Google Scholar] [CrossRef]
- Lambert, J.J.; Cooper, M.A.; Simmons, R.D.; Weir, C.J.; Belelli, D. Neurosteroids: Endogenous allosteric modulators of GABA(A) receptors. Psychoneuroendocrinology 2009, 34 (Suppl. S1), S48–S58. [Google Scholar] [CrossRef]
- Carver, C.M.; Reddy, D.S. Neurosteroid interactions with synaptic and extrasynaptic GABA(A) receptors: Regulation of subunit plasticity, phasic and tonic inhibition, and neuronal excitability. Psychopharmacology 2013, 230, 151–188. [Google Scholar] [CrossRef]
- Gunduz-Bruce, H.; Takahashi, K.; Huang, M.Y. Development of neuroactive steroids for the treatment of postpartum depression. J. Neuroendocrinol. 2022, 34, e13019. [Google Scholar] [CrossRef]
- Chen, Z.W.; Bracamontes, J.R.; Budelier, M.M.; Germann, A.L.; Shin, D.J.; Kathiresan, K.; Qian, M.X.; Manion, B.; Cheng, W.W.L.; Reichert, D.E.; et al. Multiple functional neurosteroid binding sites on GABAA receptors. PLoS Biol. 2019, 17, e3000157. [Google Scholar] [CrossRef] [PubMed]
- Goldschen-Ohm, M.P. Benzodiazepine Modulation of GABAA Receptors: A Mechanistic Perspective. Biomolecules 2022, 12, 1784. [Google Scholar] [CrossRef] [PubMed]
- Takasu, K.; Yawata, Y.; Tashima, R.; Aritomi, H.; Shimada, S.; Onodera, T.; Taishi, T.; Ogawa, K. Distinct mechanisms of allopregnanolone and diazepam underlie neuronal oscillations and differential antidepressant effect. Front. Cell. Neurosci. 2024, 17, 1274459. [Google Scholar] [CrossRef] [PubMed]
- Antonoudiou, P.; Colmers, P.L.W.; Walton, N.L.; Weiss, G.L.; Smith, A.C.; Nguyen, D.P.; Lewis, M.; Quirk, M.C.; Barros, L.; Melon, L.C.; et al. Allopregnanolone Mediates Affective Switching Through Modulation of Oscillatory States in the Basolateral Amygdala. Biol. Psychiatry 2022, 91, 283–293. [Google Scholar] [CrossRef]
- Lüscher, B.; Möhler, H. Brexanolone, a neurosteroid antidepressant, vindicates the GABAergic deficit hypothesis of depression and may foster resilience. F1000Res. 2019, 8, F1000, Faculty Rev-751. [Google Scholar] [CrossRef]
- Kanes, S.; Colquhoun, H.; Gunduz-Bruce, H.; Raines, S.; Arnold, R.; Schacterle, A.; Doherty, J.; Epperson, C.N.; Deligiannidis, K.M.; Riesenberg, R.; et al. Brexanolone (SAGE-547 injection) in post-partum depression: A randomised controlled trial. Lancet 2017, 390, 480–489. [Google Scholar] [CrossRef]
- Epperson, C.N.; Rubinow, D.R.; Meltzer-Brody, S.; Deligiannidis, K.M.; Riesenberg, R.; Krystal, A.D.; Bankole, K.; Huang, M.Y.; Li, H.; Brown, C.; et al. Effect of brexanolone on depressive symptoms, anxiety, and insomnia in women with postpartum depression: Pooled analyses from 3 double-blind, randomized, placebo-controlled clinical trials in the HUMMINGBIRD clinical program. J. Affect. Disord. 2023, 320, 353–359. [Google Scholar] [CrossRef]
- Meltzer-Brody, S.; Colquhoun, H.; Riesenberg, R.; Epperson, C.N.; Deligiannidis, K.M.; Rubinow, D.R.; Li, H.; Sankoh, A.J.; Clemso, C.; Schacterle, A.; et al. Brexanolone injection in post-partum depression: Two multicentre, double-blind, randomised, placebo-controlled, phase 3 trials. Lancet 2018, 392, 1058–1070. [Google Scholar] [CrossRef]
- Reddy, D.S.; Mbilinyi, R.H.; Estes, E. Preclinical and clinical pharmacology of brexanolone (allopregnanolone) for postpartum depression: A landmark journey from concept to clinic in neurosteroid replacement therapy. Psychopharmacology 2023, 240, 1841–1863. [Google Scholar] [CrossRef]
- Martinez, B.G.; Salituro, F.G.; Harrison, B.L.; Beresis, R.T.; Bai, Z.; Blanco, M.J.; Belfort, G.M.; Dai, J.; Loya, C.M.; Ackle, M.A.; et al. Neuroactive Steroids. 2. 3α-Hydroxy-3β-methyl-21-(4-cyano-1H-pyrazol-1’-yl)-19-nor-5β-pregnan-20-one (SAGE-217): A Clinical Next Generation Neuroactive Steroid Positive Allosteric Modulator of the (γ-Aminobutyric Acid)A Receptor. J. Med. Chem. 2017, 60, 7810–7819. [Google Scholar] [CrossRef]
- National Center for Biotechnology Information. (2025) PubChem Compound Summary for CID 86294073, Zuranolone. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/Zuranolone (accessed on 10 April 2025).
- Althaus, A.L.; Ackley, M.A.; Belfort, G.M.; Gee, S.M.; Dai, J.; Nguyen, D.P.; Kazdoba, T.M.; Modgil, A.; Davies, P.A.; Moss, S.J.; et al. Preclinical characterization of zuranolone (SAGE-217), a selective neuroactive steroid GABAA receptor positive allosteric modulator. Neuropharmacology 2020, 181, 108333. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, E.; Nomikos, G.G.; Kaul, I.; Raines, S.; Wald, J.; Bullock, A.; Sankoh, A.J.; Doherty, J.; Kanes, S.J.; Colquhoun, H. SAGE-217, A Novel GABAA Receptor Positive Allosteric Modulator: Clinical Pharmacology and Tolerability in Randomized Phase I Dose-Finding Studies. Clin. Pharmacokinet. 2020, 59, 111–120. [Google Scholar] [CrossRef] [PubMed]
- Biogen Inc. Zurzuvae (Zuranolone) [Package Insert]. FDA. Revised March 2019. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/217369s000lbl.pdf (accessed on 25 March 2025).
- Deligiannidis, K.M.; Citrome, L.; Huang, M.Y.; Acaster, S.; Fridman, M.; Bonthapally, V.; Lasser, R.; Kanes, S.J. Effect of Zuranolone on Concurrent Anxiety and Insomnia Symptoms in Women with Postpartum Depression. J. Clin. Psychiatry 2023, 84(1), 22m14475. [Google Scholar] [CrossRef]
- Deligiannidis, K.M.; Meltzer-Brody, S.; Gunduz-Bruce, H.; Doherty, J.; Jonas, J.; Li, S.; Sankoh, A.J.; Silber, C.; Campbell, A.D.; Werneburg, B.; et al. Effect of Zuranolone vs. Placebo in Postpartum Depression: A Randomized Clinical Trial. JAMA Psychiatry 2021, 78, 951–959. [Google Scholar] [CrossRef]
- Deligiannidis, K.M.; Meltzer-Brody, S.; Maximos, B.; Peeper, E.Q.; Freeman, M.; Lasser, R.; Bullock, A.; Kotecha, M.; Li, S.; Forrestal, F.; et al. Zuranolone for the Treatment of Postpartum Depression. Am. J. Psychiatry 2023, 180, 668–675. [Google Scholar] [CrossRef]
- Clayton, A.H.; Suthoff, E.; Jain, R.; Kosinski, M.; Fridman, M.; Deligiannidis, K.M.; Meltzer-Brody, S.; Chen, S.Y.; Gervitz, L.; Huang, M.Y.; et al. The magnitude and sustainability of treatment benefit of zuranolone on function and well-being as assessed by the SF-36 in adult patients with MDD and PPD: An integrated analysis of 4 randomized clinical trials. J. Affect. Disord. 2024, 351, 904–914. [Google Scholar] [CrossRef]
- Raja, A.; Ahmed, S.; Basit Ali Siddiqui, M.; Lamiya Mir, S.; Kumar, R.; Ahmed, M.; Raja, S.; Bin Amin, S.; Alim Ur Rahman, H.; Deepak, F.; et al. Evaluating the safety and efficacy of zuranolone in the management of major depressive disorder and postpartum depression, with or without concurrent insomnia: A rigorous systematic review and meta-analysis. Front. Psychiatry 2024, 15, 1425295. [Google Scholar] [CrossRef]
- Meltzer-Brody, S.; Gerbasi, M.E.; Mak, C.; Toubouti, Y.; Smith, S.; Roskell, N.; Tan, R.; Chen, S.S.; Deligiannidis, K.M. Indirect comparisons of relative efficacy estimates of zuranolone and selective serotonin reuptake inhibitors for postpartum depression. J. Med. Econ. 2024, 27, 582–595. [Google Scholar] [CrossRef]
- Dunbar, J.; Morelli, G.; Jain, R.; Vaudreuil, C.; Nandy, I.; Ona, V.; Moseley, M.K.; Levin, S.; Kay, G. Effects of zuranolone on next-day simulated driving in healthy adults. Psychopharmacology 2025, 242, 389–400. [Google Scholar] [CrossRef]
- Deligiannidis, K.M.; Bullock, A.; Nandy, I.; Dunbar, J.; Lasser, R.; Witte, M.; Leclair, B.; Wald, J. Zuranolone Concentrations in the Breast Milk of Healthy, Lactating Individuals: Results from a Phase 1 Open-Label Study. J. Clin. Psychopharmacol. 2024, 44, 337–344. [Google Scholar] [CrossRef]
- Swieczkowski, D.; Kwaśny, A.; Pruc, M.; Szarpak, L.; Cubała, W.J. Racial and ethnic diversity in zuranolone and brexanolone clinical trials for postpartum depression: A cross-sectional analysis of ClinicalTrials.gov. Eur. Neuropsychopharmacol. 2025, 96, 5–6. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Drug | FDA Approval for PPD Treatment/Year of Approval | Other Indications Approved by FDA |
|---|---|---|
| Neuroactive steroids | None [44,45] | |
| -Brexanolone [44] | YES/2019 | |
| -Zuranolone [45] | YES/2023 | |
| SSRIs [46] | NO | Major depressive disorder, generalized anxiety disorder, obsessive-compulsive disorder, panic disorder, post-traumatic stress disorder, social anxiety disorder, premenstrual dysphoric disorder, bulimia nervosa |
| SNRIs [47] | NO | Major depressive disorder, generalized anxiety disorder, social anxiety disorder, panic disorder, diabetic peripheral neuropathic pain, fibromyalgia, chronic musculoskeletal pain |
| TCAs [48] | NO | Major depressive disorder, obsessive-compulsive disorder (clomipramine) |
| Reference | Treatment | Participants, No. | Ethnicity, No. (%) | Race, No. (%) | Change from Baseline in HAM-D Score | Treatment-Emergent Adverse Events No. (%) | |||
|---|---|---|---|---|---|---|---|---|---|
| Hispanic or Latino | Not Hispanic or Latino | African American | White | Other a | |||||
| [83] | zuranolone 30 mg | 76 | 16 (21) | 60 (79) | 31 (41) | 44 (58) | 1 (1) | −17.8 points | 47 (60) |
| placebo | 74 | 18 (24) | 56 (76) | 31 (42) | 40 (54) | 3 (4) | −13.6 points | 38 (52) | |
| [84] | zuranolone 50 mg | 98 | 33 (33.7) | 65 (66.3) | 25 (25.5) | 68 (69.4) | 5 (5.1) | −15.6 points | 65 (66.3) |
| placebo | 98 | 42 (42.9) | 56 (57.1) | 18 (18.4) | 69 (70.4) | 11 (11.2) | −11.6 points | 52 (53.1) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zawilska, J.B.; Zwierzyńska, E. Neuroactive Steroids as Novel Promising Drugs in Therapy of Postpartum Depression—Focus on Zuranolone. Int. J. Mol. Sci. 2025, 26, 6545. https://doi.org/10.3390/ijms26136545
Zawilska JB, Zwierzyńska E. Neuroactive Steroids as Novel Promising Drugs in Therapy of Postpartum Depression—Focus on Zuranolone. International Journal of Molecular Sciences. 2025; 26(13):6545. https://doi.org/10.3390/ijms26136545
Chicago/Turabian StyleZawilska, Jolanta B., and Ewa Zwierzyńska. 2025. "Neuroactive Steroids as Novel Promising Drugs in Therapy of Postpartum Depression—Focus on Zuranolone" International Journal of Molecular Sciences 26, no. 13: 6545. https://doi.org/10.3390/ijms26136545
APA StyleZawilska, J. B., & Zwierzyńska, E. (2025). Neuroactive Steroids as Novel Promising Drugs in Therapy of Postpartum Depression—Focus on Zuranolone. International Journal of Molecular Sciences, 26(13), 6545. https://doi.org/10.3390/ijms26136545