
Evaluation of Torquetenovirus (TTV) Particle Integrity Utilizing PMAxx™

 , , , , , , , ,
, , , , , , , ,  and
and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Results
2.1. TTV DNA in Fresh and Frozen Samples with or Without PMAxx™ Treatment
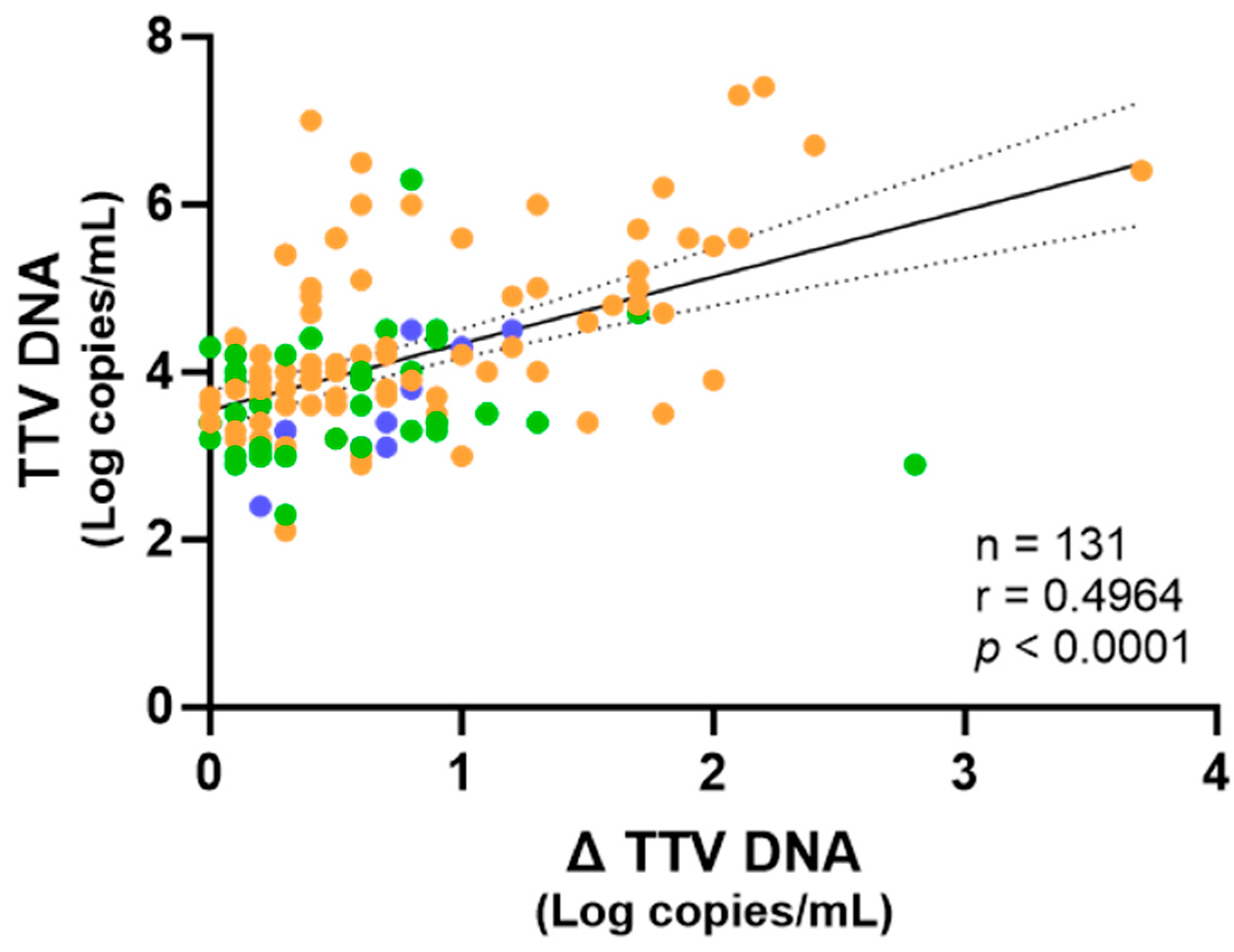
2.2. Correlation Between TTV DNA Levels After PMAxx™ Treatment and Immune Responses in PWH and LTR Patients
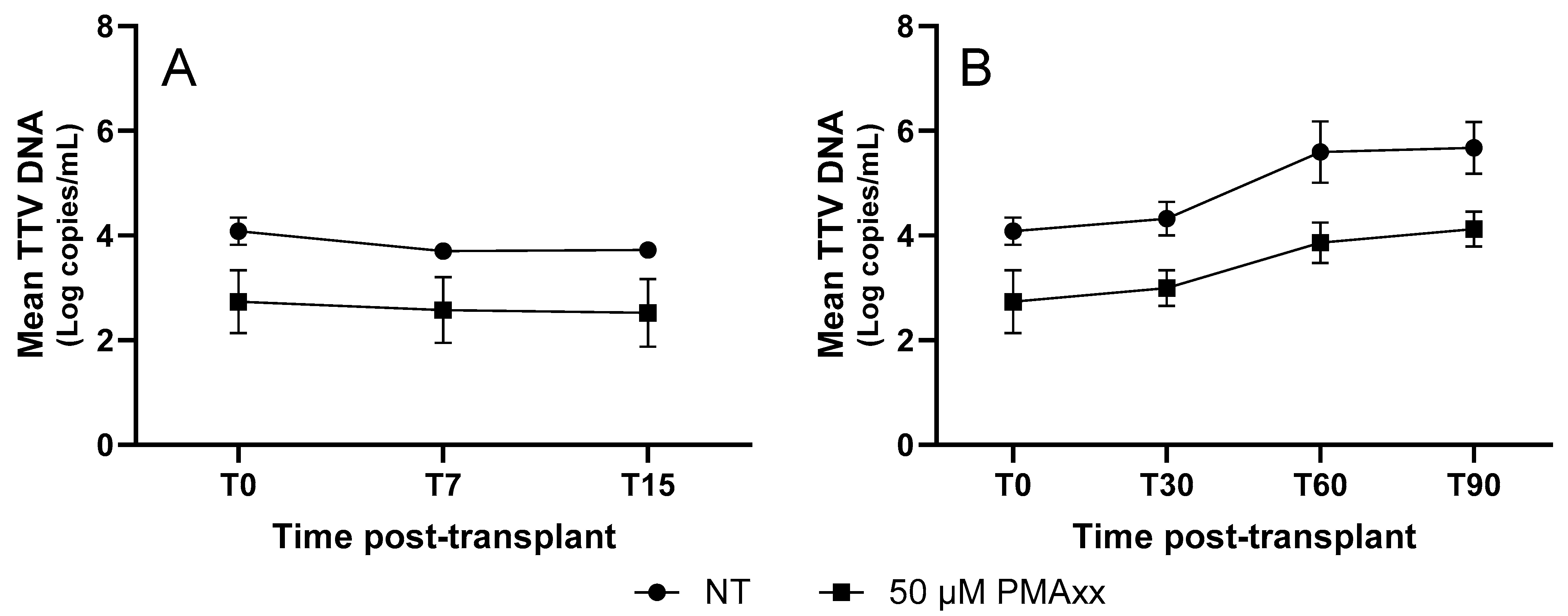
2.3. TTV DNA—PMAxx™ in LTRs over Time
3. Discussion
4. Materials and Methods
4.1. Specimens
4.2. PMAxx™ Treatment
4.3. TTV DNA Quantification
4.4. SARS-CoV-2 IgG Antibody Testing
4.5. SARS-CoV-2 Microneutralization Assay
4.6. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ddPCR | Digital droplet PCR |
| LTR | Liver transplant recipient |
| PMA | Propidium monoazide |
| PWH | People with HIV |
| TTV | Torquetenovirus |
References
- Okamoto, H. History of Discoveries and Pathogenicity of TT Viruses. In TT Viruses: The Still Elusive Human Pathogens; Current Topics in Microbiology and Immunology; Springer: Berlin/Heidelberg, Germany, 2009; Volume 331, pp. 1–20. [Google Scholar] [CrossRef]
- Brajão De Oliveira, K. Torque Teno Virus: A Ubiquitous Virus. Rev. Bras. De Hematol. E Hemoter. 2015, 37, 357–358. [Google Scholar] [CrossRef] [PubMed]
- Righi, F.; Arnaboldi, S.; Filipello, V.; Ianiro, G.; Di Bartolo, I.; Calò, S.; Bellini, S.; Trogu, T.; Lelli, D.; Bianchi, A.; et al. Torque Teno Sus Virus (TTSuV) Prevalence in Wild Fauna of Northern Italy. Microorganisms 2022, 10, 242. [Google Scholar] [CrossRef]
- Gallian, P.; Biagini, P.; Zhong, S.; Touinssi, M.; Yeo, W.; Cantaloube, J.F.; Attoui, H.; De Micco, P.; Johnson, P.J.; De Lamballerie, X. TT Virus: A Study of Molecular Epidemiology and Transmission of Genotypes 1, 2 and 3. J. Clin. Virol. 2000, 17, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Verschoor, E.J.; Langenhuijzen, S.; Heeney, J.L. TT Viruses (TTV) of Non-Human Primates and Their Relationship to the Human TTV Genotypes. J. Gen. Virol. 1999, 80, 2491–2499. [Google Scholar] [CrossRef]
- Redondo, N.; Navarro, D.; Aguado, J.M.; Fernández-Ruiz, M. Viruses, Friends, and Foes: The Case of Torque Teno Virus and the Net State of Immunosuppression. Transpl. Infect. Dis. 2022, 24, e13778. [Google Scholar] [CrossRef] [PubMed]
- Minosse, C.; Matusali, G.; Meschi, S.; Grassi, G.; Francalancia, M.; D’Offizi, G.; Spezia, P.G.; Garbuglia, A.R.; Montalbano, M.; Focosi, D.; et al. Torquetenovirus Loads in Peripheral Blood Predict Both the Humoral and Cell-Mediated Responses to SARS-CoV-2 Elicited by the mRNA Vaccine in Liver Transplant Recipients. Vaccines 2023, 11, 1656. [Google Scholar] [CrossRef]
- Minosse, C.; Spezia, P.G.; Mazzotta, V.; Matusali, G.; Meschi, S.; Colavita, F.; Mariotti, D.; Notari, S.; Vergori, A.; Focosi, D.; et al. Assessing Torquetenovirus (TTV) as a Biomarker for Immune Responses to SARS-CoV-2 mRNA Vaccines in People Living with HIV and Healthy Individuals. Vaccines 2025, 13, 153. [Google Scholar] [CrossRef]
- Focosi, D.; Antonelli, G.; Pistello, M.; Maggi, F. Torquetenovirus: The Human Virome from Bench to Bedside. Clin. Microbiol. Infect. 2016, 22, 589–593. [Google Scholar] [CrossRef]
- Strassl, R.; Doberer, K.; Rasoul-Rockenschaub, S.; Herkner, H.; Görzer, I.; Kläger, J.P.; Schmidt, R.; Haslacher, H.; Schiemann, M.; Eskandary, F.A.; et al. Torque Teno Virus for Risk Stratification of Acute Biopsy-Proven Alloreactivity in Kidney Transplant Recipients. J. Infect. Dis. 2019, 219, 1934–1939. [Google Scholar] [CrossRef]
- Mouton, W.; Conrad, A.; Bal, A.; Boccard, M.; Malcus, C.; Ducastelle-Lepretre, S.; Balsat, M.; Barraco, F.; Larcher, M.-V.; Fossard, G.; et al. Torque Teno Virus Viral Load as a Marker of Immune Function in Allogeneic Haematopoietic Stem Cell Transplantation Recipients. Viruses 2020, 12, 1292. [Google Scholar] [CrossRef]
- Kuczaj, A.; Przybyłowski, P.; Hrapkowicz, T. Torque Teno Virus (TTV)-A Potential Marker of Immunocompetence in Solid Organ Recipients. Viruses 2023, 16, 17. [Google Scholar] [CrossRef] [PubMed]
- Walton, A.H.; Muenzer, J.T.; Rasche, D.; Boomer, J.S.; Sato, B.; Brownstein, B.H.; Pachot, A.; Brooks, T.L.; Deych, E.; Shannon, W.D.; et al. Reactivation of Multiple Viruses in Patients with Sepsis. PLoS ONE 2014, 9, e98819. [Google Scholar] [CrossRef]
- Kapps, S.; Haupenthal, F.; Bond, G. Torque Teno Virus-Guided Monitoring of Immunosuppressive Therapy. Nephrol. Dial. Transplant. 2024, 39, 1942–1944. [Google Scholar] [CrossRef]
- Pescarmona, R.; Mouton, W.; Walzer, T.; Dalle, S.; Eberhardt, A.; Brengel-Pesce, K.; Villard, M.; Lombard, C.; Trouillet-Assant, S.; Viel, S. Evaluation of TTV Replication as a Biomarker of Immune Checkpoint Inhibitors Efficacy in Melanoma Patients. PLoS ONE 2021, 16, e0255972. [Google Scholar] [CrossRef] [PubMed]
- Sabbaghian, M.; Gheitasi, H.; Shekarchi, A.A.; Tavakoli, A.; Poortahmasebi, V. The Mysterious Anelloviruses: Investigating Its Role in Human Diseases. BMC Microbiol. 2024, 24, 40. [Google Scholar] [CrossRef]
- Mulagapati, S.H.R.; Parupudi, A.; Witkos, T.; Bond, N.; Chen, X.; Linke, T.; Xi, G.; Schmelzer, A.E.; Xu, W. Size-Exclusion Chromatography as a Multi-Attribute Method for Process and Product Characterization of Adeno-Associated Virus. Mol. Ther. Methods Clin. Dev. 2024, 32, 101382. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Mulagapati, S.H.R.; Chen, Z.; Du, J.; Zhao, X.; Xi, G.; Chen, L.; Linke, T.; Gao, C.; Schmelzer, A.E.; et al. Developing an Anion Exchange Chromatography Assay for Determining Empty and Full Capsid Contents in AAV6.2. Mol. Ther. Methods Clin. Dev. 2019, 15, 257–263. [Google Scholar] [CrossRef]
- Sberna, G.; Mija, C.; Lalle, E.; Rozera, G.; Matusali, G.; Carletti, F.; Girardi, E.; Maggi, F. Rapid Determination of SARS-CoV-2 Integrity and Infectivity by Using Propidium Monoazide Coupled with Digital Droplet PCR. Int. J. Mol. Sci. 2024, 25, 6156. [Google Scholar] [CrossRef]
- Sberna, G.; Specchiarello, E.; Mija, C.; Carletti, F.; Belladonna, S.; Girardi, E.; Mazzotta, V.; Maggi, F. Measurement of the Infection and Integrity of Monkeypox Virus: A New Method Using PMAxx-ddPCR. Int. J. Mol. Sci. 2025, 26, 1195. [Google Scholar] [CrossRef]
- Fittipaldi, M.; Nocker, A.; Codony, F. Progress in Understanding Preferential Detection of Live Cells Using Viability Dyes in Combination with DNA Amplification. J. Microbiol. Methods 2012, 91, 276–289. [Google Scholar] [CrossRef]
- Randazzo, W.; López-Gálvez, F.; Allende, A.; Aznar, R.; Sánchez, G. Evaluation of Viability PCR Performance for Assessing Norovirus Infectivity in Fresh-Cut Vegetables and Irrigation Water. Int. J. Food Microbiol. 2016, 229, 1–6. [Google Scholar] [CrossRef]
- Coudray-Meunier, C.; Fraisse, A.; Martin-Latil, S.; Guillier, L.; Perelle, S. Discrimination of Infectious Hepatitis A Virus and Rotavirus by Combining Dyes and Surfactants with RT-qPCR. BMC Microbiol. 2013, 13, 216. [Google Scholar] [CrossRef] [PubMed]
- Qi, W.; Qiu, Y.; Zhao, D.; Qiu, M.; Lin, H.; Cui, M.; Yang, S.; Zheng, W.; Zhu, J.; Chen, N. Propidium Monoazide Integrated With qPCR Enables Rapid and Universal Detection of Infectious Porcine Reproductive and Respiratory Syndrome Viruses. Transbound. Emerg. Dis. 2024, 2024, 6250851. [Google Scholar] [CrossRef]
- Li, Y.; Wang, Z.; Qing, J.; Hu, D.; Vo, H.T.; Thi, K.T.; Wang, X.; Li, X. Application of Propidium Monoazide Quantitative PCR to Discriminate of Infectious African Swine Fever Viruses. Front. Microbiol. 2023, 14, 1290302. [Google Scholar] [CrossRef] [PubMed]
- Kevill, J.L.; Farkas, K.; Ridding, N.; Woodhall, N.; Malham, S.K.; Jones, D.L. Use of Capsid Integrity-qPCR for Detecting Viral Capsid Integrity in Wastewater. Viruses 2023, 16, 40. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.; Piri, A.; Jung, J.; An, S.; Hwang, J. Determination of Airborne Influenza Virus and Coronavirus Infectivity Using Capsid Integrity Polymerase Chain Reaction. J. Hazard. Mater. 2024, 479, 135544. [Google Scholar] [CrossRef]
- Liang, C.; Wang, Z.; Fan, L.; Wang, Y.; Zhou, Y.; Yang, X.; Lin, J.; Ye, P.; Shi, W.; Huang, H.; et al. Rapidly Quantification of Intact Infectious H1N1 Virus Using ICA-qPCR and PMA-qPCR. Biosaf. Health 2024, 6, 327–336. [Google Scholar] [CrossRef]
- Veugen, J.M.J.; Schoenmakers, T.; van Loo, I.H.M.; Haagmans, B.L.; Leers, M.P.G.; Lamers, M.M.; Lucchesi, M.; van Bussel, B.C.T.; van Mook, W.N.K.A.; Nuijts, R.M.M.A.; et al. Advancing COVID-19 Diagnostics: Rapid Detection of Intact SARS-CoV-2 Using Viability RT-PCR Assay. Microbiol. Spectr. 2024, 12, e0016024. [Google Scholar] [CrossRef]
- Lauzier, A.-M.; Douette, É.; Labrie, A.; Jubinville, É.; Goulet-Beaulieu, V.; Hamon, F.; Jean, J. Comparison of Sample Pretreatments Used to Distinguish between Infectious and Non-Infectious Foodborne Viruses by RT-qPCR. J. Virol. Methods 2025, 335, 115130. [Google Scholar] [CrossRef]
- Haupenthal, F.; Rahn, J.; Maggi, F.; Gelas, F.; Bourgeois, P.; Hugo, C.; Jilma, B.; Böhmig, G.A.; Herkner, H.; Wolzt, M.; et al. A Multicentre, Patient- and Assessor-Blinded, Non-Inferiority, Randomised and Controlled Phase II Trial to Compare Standard and Torque Teno Virus-Guided Immunosuppression in Kidney Transplant Recipients in the First Year after Transplantation: TTVguideIT. Trials 2023, 24, 213. [Google Scholar] [CrossRef]
- Querido, S.; Martins, C.; Gomes, P.; Pessanha, M.A.; Arroz, M.J.; Adragão, T.; Casqueiro, A.; Oliveira, R.; Costa, I.; Azinheira, J.; et al. Kinetics of Torque Teno Virus Viral Load Is Associated with Infection and De Novo Donor Specific Antibodies in the First Year after Kidney Transplantation: A Prospective Cohort Study. Viruses 2023, 15, 1464. [Google Scholar] [CrossRef] [PubMed]
- Albert, E.; Giménez, E.; Hernani, R.; Piñana, J.L.; Solano, C.; Navarro, D. Torque Teno Virus DNA Load in Blood as an Immune Status Biomarker in Adult Hematological Patients: The State of the Art and Future Prospects. Viruses 2024, 16, 459. [Google Scholar] [CrossRef] [PubMed]
- Jaksch, P.; Görzer, I.; Puchhammer-Stöckl, E.; Bond, G. Integrated Immunologic Monitoring in Solid Organ Transplantation: The Road Toward Torque Teno Virus-Guided Immunosuppression. Transplantation 2022, 106, 1940–1951. [Google Scholar] [CrossRef] [PubMed]
- Biotium. PMAxx. Available online: https://biotium.com/product/pmaxx-20-mm-in-h2o/ (accessed on 26 June 2025).
- Qiagen. QIAamp DNA Mini Kit. Available online: https://www.qiagen.com/us (accessed on 26 June 2025).
- Bio-Rad. Droplet Digital PCR (ddPCR). Available online: https://www.bio-rad.com/it-it/life-science/droplet-digital-pcr (accessed on 26 June 2025).
- Berg, R.; Clemmensen, T.S.; Petersen, M.S.; Mogensen, L.J.H.; Christiansen, M.; Rolid, K.; Nytrøen, K.; Møller, B.K.; Gullestad, L.; Eiskjær, H.; et al. Kinetics of Torque Teno Virus in Heart Transplant Patients. Hum. Immunol. 2023, 84, 110720. [Google Scholar] [CrossRef]
- Doberer, K.; Schiemann, M.; Strassl, R.; Haupenthal, F.; Dermuth, F.; Görzer, I.; Eskandary, F.; Reindl-Schwaighofer, R.; Kikić, Ž.; Puchhammer-Stöckl, E.; et al. Torque Teno Virus for Risk Stratification of Graft Rejection and Infection in Kidney Transplant Recipients-A Prospective Observational Trial. Am. J. Transplant. 2020, 20, 2081–2090. [Google Scholar] [CrossRef]
- Abbott. Dosaggi Immunologici per SARS-CoV-2. Available online: https://www.corelaboratory.abbott/int/it/offerings/segments/infectious-disease/sars-cov-2.html (accessed on 26 June 2025).
- World Health Organization. Establishment of the WHO International Standard and Reference Panel for Anti-SARS-CoV-2 Antibody. Available online: https://www.who.int/publications/m/item/WHO-BS-2020.2403 (accessed on 26 June 2025).
- National Institute for Biological Standards and Control (NIBSC). First WHO International Standard Anti-SARS-CoV-2 Immunoglobulin (Human). Available online: https://www.nibsc.org/products/brm_product_catalogue/detail_page.aspx?catid=20/136 (accessed on 26 June 2025).
- Matusali, G.; Sberna, G.; Meschi, S.; Gramigna, G.; Colavita, F.; Lapa, D.; Francalancia, M.; Bettini, A.; Capobianchi, M.R.; Puro, V.; et al. Differential Dynamics of SARS-CoV-2 Binding and Functional Antibodies upon BNT162b2 Vaccine: A 6-Month Follow-Up. Viruses 2022, 14, 312. [Google Scholar] [CrossRef]
- GraphPad. GraphPad Prism. Available online: https://www.graphpad.com/features (accessed on 26 June 2025).



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sberna, G.; Minosse, C.; Mija, C.; Specchiarello, E.; Spezia, P.G.; Belladonna, S.; Berno, G.; Fabeni, L.; Matusali, G.; Meschi, S.; et al. Evaluation of Torquetenovirus (TTV) Particle Integrity Utilizing PMAxx™. Int. J. Mol. Sci. 2025, 26, 6542. https://doi.org/10.3390/ijms26136542
Sberna G, Minosse C, Mija C, Specchiarello E, Spezia PG, Belladonna S, Berno G, Fabeni L, Matusali G, Meschi S, et al. Evaluation of Torquetenovirus (TTV) Particle Integrity Utilizing PMAxx™. International Journal of Molecular Sciences. 2025; 26(13):6542. https://doi.org/10.3390/ijms26136542
Chicago/Turabian StyleSberna, Giuseppe, Claudia Minosse, Cosmina Mija, Eliana Specchiarello, Pietro Giorgio Spezia, Sara Belladonna, Giulia Berno, Lavinia Fabeni, Giulia Matusali, Silvia Meschi, and et al. 2025. "Evaluation of Torquetenovirus (TTV) Particle Integrity Utilizing PMAxx™" International Journal of Molecular Sciences 26, no. 13: 6542. https://doi.org/10.3390/ijms26136542
APA StyleSberna, G., Minosse, C., Mija, C., Specchiarello, E., Spezia, P. G., Belladonna, S., Berno, G., Fabeni, L., Matusali, G., Meschi, S., Focosi, D., & Maggi, F. (2025). Evaluation of Torquetenovirus (TTV) Particle Integrity Utilizing PMAxx™. International Journal of Molecular Sciences, 26(13), 6542. https://doi.org/10.3390/ijms26136542