1. Introduction
TGF-β is a major contributor to pancreatic cancer [
1]. TGF-β plays a paradoxical role as both a tumor suppressor and a tumor promoter in pancreatic cancer [
1]. TGF-β signals primarily through transmembrane receptor kinases, activating downstream Smad proteins, allowing them to translocate to the nucleus and participate in the transcriptional control of TGF-β target genes. When intact, this pathway functions as a growth inhibitor for many cell types by inhibiting cell cycle progression, and loss of TGFβ responsiveness can lead to deregulated cell proliferation and ultimately tumor progression [
2]. Smad4/DPC4 gene inactivation is particularly frequent in pancreatic cancer, contributing to the highly invasive and metastatic characteristics [
3]. In those tumors retaining normal Smad4 function, TGF-β can exert potent antiproliferative effects by inducing cell cycle inhibitors such as p21(WAF1/CIP1) [
4]. Despite its tumor-suppressive function in early stages, TGF-β often adopts a tumor-promoting role in the late phase of tumor progression [
3]. TGF-β can stimulate fibrosis, facilitate immune evasion, and promote epithelial–mesenchymal transition (EMT) [
5,
6]. Chronic, high-level TGF-β exposure can drive aggressive tumor phenotype[s] and neoplastic transformation, in part through the downregulation of p21(WAF1/CIP1) [
4]. TGF-β may promote pancreatic cancer development by affecting stromal and hematopoietic cell function, fueling immunosuppression and rendering the tumor microenvironment more permissive to tumor growth [
6]. Multiple therapies have been investigated to target TGF-β signaling, including small-molecule inhibitors, neutralizing antibodies, and antisense approaches [
5,
7]. The inhibition of TGF-β2 synthesis via the antisense oligonucleotide trabedersen (AP 12009, OT-101) is a promising approach given that increased TGF-β2 levels in the serum or tumor tissue of patients with pancreatic cancer correlated with poor prognosis [
7]. The inhibition of TGF-βR to target components of the tumor microenvironment warrants consideration as a potential therapy for pancreatic cancer, particularly in patients who have already lost tumor-suppressive TGF-β signals in the epithelium [
6].
There are three main TGF-β isoforms—TGF-β1, TGF-β2, and TGF-β3. All three isoforms are overexpressed in pancreatic cancer compared to normal pancreatic tissue, but to varying degrees: pancreatic adenocarcinomas showed 11- (
p < 0.001), 7- (
p < 0.05), and 9-fold (
p < 0.001) increases in the messenger RNA (mRNA) levels encoding TGF-β1, TGF-β2, and TGF-β3, respectively [
8]. Immunohistochemical analyses revealed TGF-β1 presence in 47% of tumors, TGF-β2 in 42%, and TGF-β3 in 40% [
8]. Among the three isoforms, TGF-β2 was particularly associated with advanced tumor stage (
p < 0.05) and more prolonged postoperative survival [
8]. In chronic, cancer-associated obstructive pancreatitis (COP), TGF-β1 was prominent in macrophages and neutrophils, TGF-β2 was intensely positive in ductal cells, and TGF-β3 was broadly and less intensely distributed [
9]. These findings suggest that TGF-β1 may often be derived from inflammatory cells, while TGF-β2 and TGF-β3 may be more involved in paracrine signaling within ductal epithelial compartments. All three isoforms can promote pathological fibrosis and tumor progression in pancreatic cancer, in part by stimulating myofibroblasts. TGF-β1, however, shows particularly strong links to inflammatory cell infiltration [
9], whereas TGF-β2 has been specifically correlated with higher tumor stages [
8]. These distinctions highlight different cellular sources and slightly different roles in driving the fibroinflammatory and invasive phenotypes of pancreatic cancer. Because all three isoforms are frequently overexpressed, attempts at targeting TGF-β pathways (e.g., TGF-β ligands, receptors, or intracellular mediators) might need to account for overlapping yet somewhat distinct functional roles of TGF-β1, TGF-β2, and TGF-β3. Prognostically, the detection of TGF-β2 in particular may be relevant in advanced disease [
8], though further mechanistic studies are required to delineate each isoform’s precise contribution.
Methylation, a key epigenetic modification, plays a critical role in pancreatic ductal adenocarcinoma (PDAC) and other pancreatic neoplasms by regulating gene expression. Several studies have shown that aberrant methylation can lead to transcriptional silencing of tumor suppressor genes, the activation of oncogenic pathways, and changes in signaling cascades that drive pancreatic carcinogenesis. A large-scale analysis of 167 treatment-naïve, surgically resected PDACs and 29 adjacent non-tumorous pancreatic tissues revealed 11,634 CpG sites associated with 3522 genes that were differentially methylated in tumors [
10]. Hypermethylation was most pronounced in the 5′ regions of genes, which included promoters and 5′UTRs. Approximately 33% of differentially methylated genes showed significant inverse correlation with mRNA expression levels, highlighting the functional impact of this epigenetic change [
10]. Aberrantly methylated genes were enriched in pathways important to pancreatic cancer, including TGF-β, WNT, integrin signaling, cell adhesion, stellate cell activation, and axon guidance [
10]. Within that axon guidance pathway, the SLIT-ROBO genes (SLIT2, SLIT3, ROBO1, and ROBO3) were commonly methylated, as were ITGA2 and MET, which suggests epigenetic suppression of SLIT-ROBO signaling and upregulation of MET and ITGA2 expression [
10]. Notably, the hypomethylation of MET and ITGA2 correlated with higher expression and worse overall outcomes. Epigenetic inactivation of RUNX3 and the prognosis of loss of function of tumor suppressor genes via promoter hypermethylation has been described for RUNX3, an important mediator of the TGF-β signaling pathway. In one study of 32 pancreatic cancer samples, promoter hypermethylation was detected in 20 (62.5%) of these tumors and, in relation to clinicopathological data, was associated with significantly worse prognosis [
11].
A study analyzed three distinct datasets of pancreatic ductal adenocarcinoma (PDAC) in two age groups: early-onset PDAC (EOPC; ≤55 years) and average-age onset PDAC (AOPC; ≥70 years). A total of 293 samples were evaluated, comprising 90 EOPC and 203 AOPC [
12]. Among the known carcinogenesis-related genes, SMAD4 displayed higher mutation rates in younger patients [
12]. Transcriptomic analysis indicated that the TGFβ pathway increased activation in EOPC, with higher levels of phospho-GSK3 expression [
12]. These findings suggest that certain pathways, notably those involving SMAD4 and TGFβ, may distinguish younger-onset PDAC from older-onset disease. Despite evidence of distinct molecular alterations, survival outcomes revealed no differences between age groups [
12]. In other words, although there may be differences in underlying biology, these did not translate into an improved or worse OS solely based on younger vs. older age at diagnosis in the analyzed datasets.
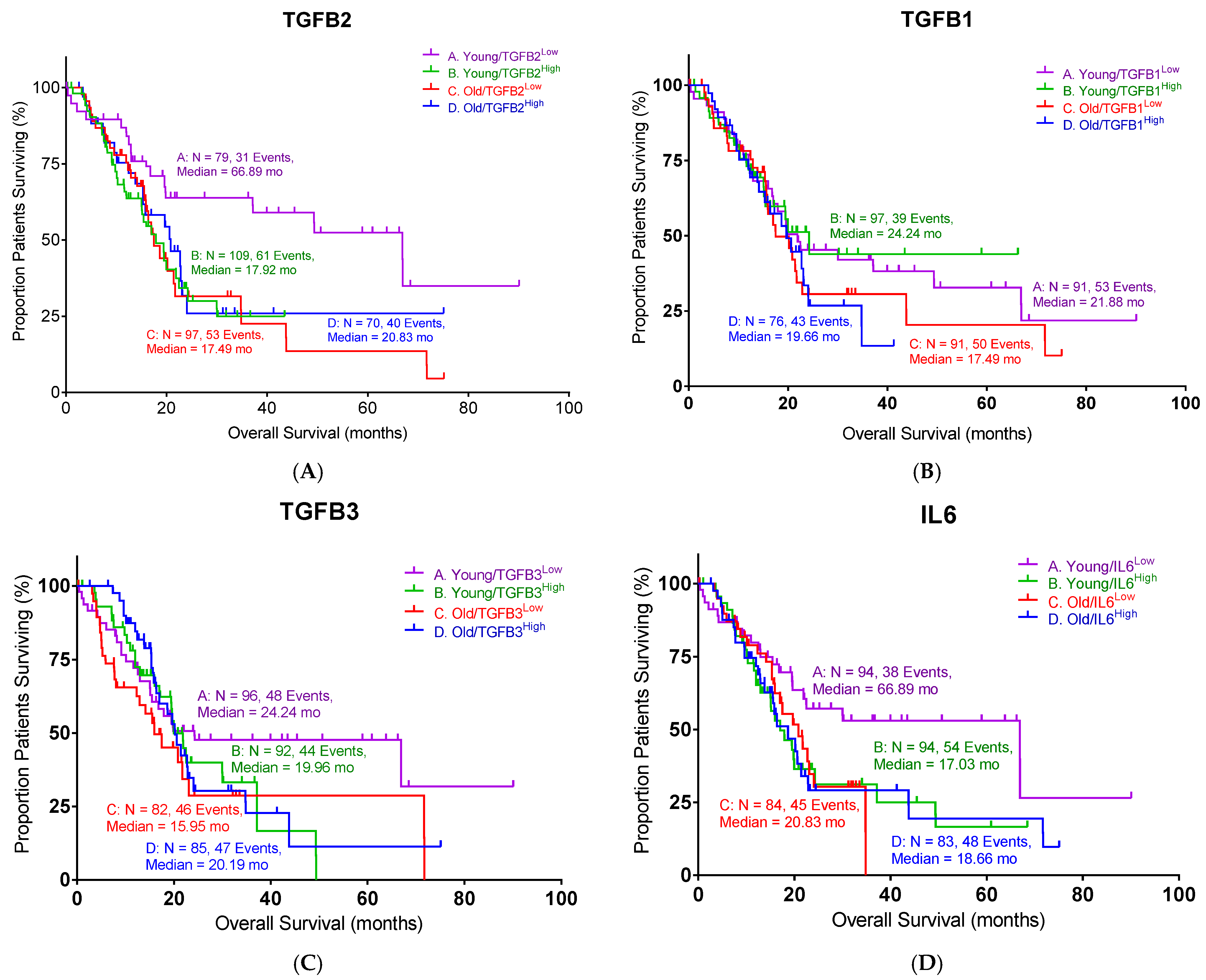
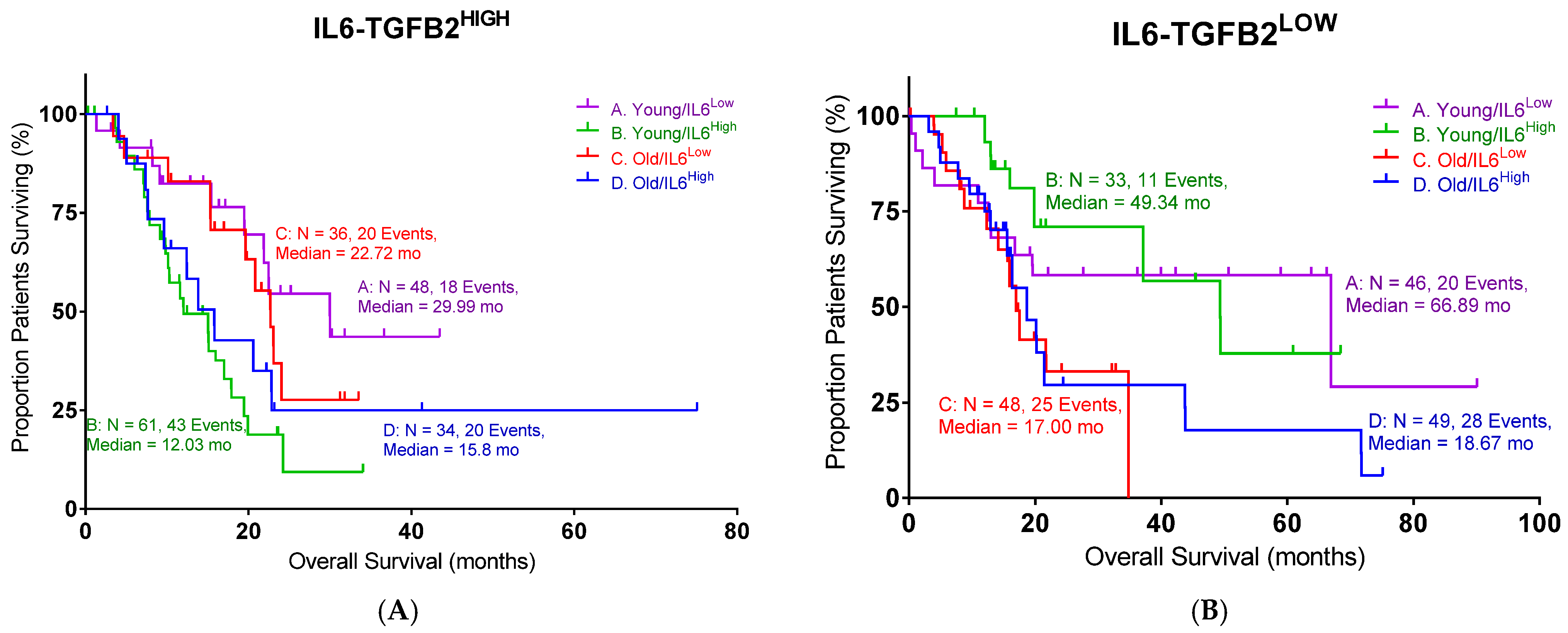
In this study, we examined the TGFB2 mRNA and TGFB2 gene methylation as predictors of OS in PDAC. The impact of age was also examined, and the bioinformatic data were confirmed with clinical data from our PDAC trial, where patients were treated with OT-101, an antisense against TGFB2. This study uniquely demonstrates that TGFB2 methylation and expression are prognostic factors in pancreatic ductal adenocarcinoma (PDAC) in an age-dependent manner and correlate with clinical responses to TGFB2-targeting antisense therapy. Specifically, high TGFB2 expression and low TGFB2 promoter methylation are associated with worse overall survival in PDAC patients under the age of 65, while the use of OT-101, an antisense oligonucleotide against TGFB2, improves survival outcomes in this younger patient population. These findings highlight the isoform- and age-specific role of TGFB2 as both a biomarker and therapeutic target in PDAC.
3. Discussion
Our analysis underscores the critical role of TGFB2 in pancreatic ductal adenocarcinoma (PDAC) progression and prognosis, revealing significant age-dependent associations. Bioinformatic analyses from TCGA clearly demonstrated that high TGFB2 expression negatively impacted OS exclusively in younger PDAC patients (under 65 years old), significantly reducing median OS compared to patients with low expression. In contrast, TGFB1 and TGFB3 were not predictive factors. One likely explanation is that TGFB1 and TGFB3 have pleiotropic, context-dependent functions that dilute their single-agent prognostic power in PDAC. For example, TGFB1 has shown both tumor-suppressive and tumor-promoting effects depending on stage and context, leading to inconsistent correlations with patient outcomes [
17,
18]. In contrast, TGFB2 appears to have a more unidirectional or context-specific impact—its high expression negatively impacts overall survival, particularly in younger patients, perhaps by more directly shaping a fibrotic and immunosuppressive tumor microenvironment. Similarly, TGFB3’s expression may be elevated in PDAC [
8], but its role may not independently drive aggressive tumor biology to the extent that TGFB2 does. Thus, while all three isoforms are components of the TGFβ pathway, TGFB2 may serve as a more robust predictor because its signaling appears to consistently contribute to adverse outcomes (particularly in younger PDAC patients). Both TGFB2 and IL6 appear to serve as robust predictors in PDAC because they more directly drive and reinforce a tumor microenvironment that promotes aggressive disease. For instance, elevated levels of TGFB2 are associated with a fibrotic and immunosuppressive tumor microenvironment due to its ability to foster the expansion of cancer-associated fibroblasts (CAFs) and the infiltration of tumor-associated macrophages (TAMs) [
19]. In this setting, TGFB2 not only increases the deposition of extracellular matrix components (fueling fibrosis) but also helps shape an immune milieu that suppresses antitumor responses, thereby leading to worse overall survival, especially in younger patients. Similarly, IL6 is a well-known proinflammatory cytokine that can enhance tumor progression by driving persistent inflammation. IL6 can stimulate cancer cell proliferation and survival and promote the recruitment and activation of myeloid cells that further suppress antitumor immunity and facilitate tumor growth. The convergence of these pathways means that when both TGFB2 and IL6 are upregulated, their cooperative effects on the tumor stroma and the immune system are accentuated, rendering them particularly predictive of poor outcomes in PDAC.
TGF-β1 plays a pleiotropic role in cancer biology, functioning as a tumor suppressor in early carcinogenesis and a pro-tumorigenic cytokine in advanced disease through the induction of epithelial–mesenchymal transition (EMT), immune evasion, and fibrosis. In PDAC, elevated plasma TGF-β1 has been consistently linked to shortened overall survival, and dynamic changes in its levels correlate with therapeutic outcomes. In a Phase II study of galunisertib, patients experiencing on-treatment declines in TGF-β1 had improved survival, while rising levels predicted early death [
20,
21]. Similar associations have been observed in other malignancies. In oral and prostate cancers, high intratumoral TGF-β1 expression is associated with nodal metastasis, high Gleason score, and reduced survival [
22,
23]. In hepatocellular carcinoma (HCC), both plasma TGF-β1 and circulating TGF-β1-responsive regulatory T cells are independently prognostic factors for worse outcomes [
24,
25]. These observations underscore the clinical importance of TGF-β1 as a non-invasive biomarker of tumor progression and immune suppression in multiple cancers, including PDAC. TGF-β3 is known to substitute for TGF-β1 in T cell polarization, capable of promoting both regulatory and proinflammatory responses depending on cytokine context [
26,
27]. In infectious diseases such as malaria, higher levels of latent TGF-β3 correlate with milder disease, suggesting an immunomodulatory, possibly protective, role [
28]. IL-6 is a key proinflammatory cytokine implicated in cancer cachexia, immune suppression, and resistance to therapy. In PDAC, elevated baseline IL-6 levels are associated with reduced survival, and in patients with concurrent high IL-10, outcomes are particularly poor [
21,
25]. Similar prognostic significance has been demonstrated in head and neck squamous cell carcinoma (HNSCC) and breast cancer [
29,
30]. IL-6 genotypes such as 174GG and 634GG correlate with increased cytokine production and have been associated with cardiovascular disease and cancer predisposition [
31,
32]. In inflammatory diseases, IL-6 levels also serve as independent predictors of mortality, as seen in community-acquired pneumonia [
33]. While TGFB2 emerged as the most robust prognostic marker in this study, the differential behaviors of TGFB1, TGFB3, and IL6, as related to methylation, warrant further discussion.
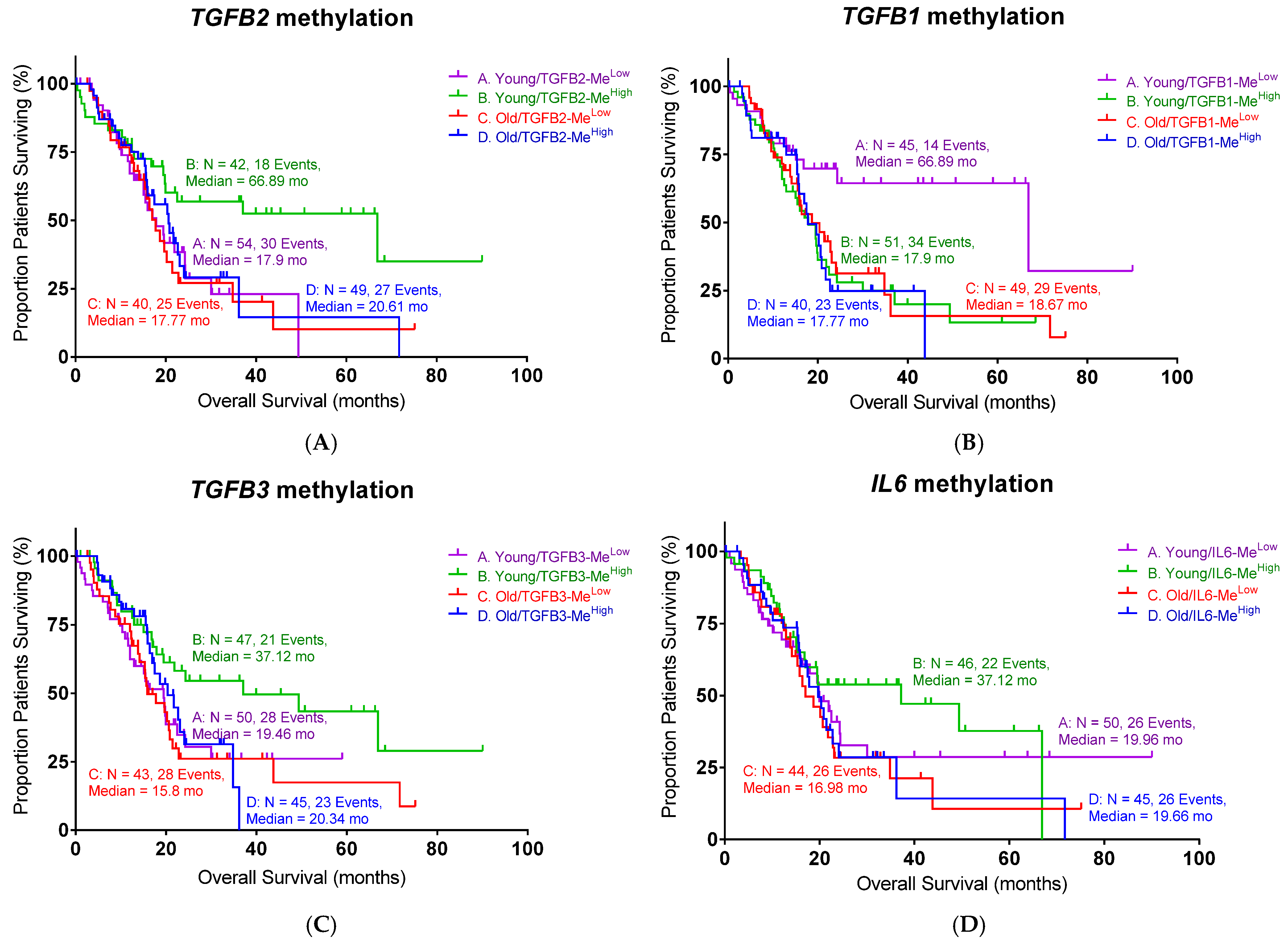
TGFB1 promoter methylation was paradoxically associated with worse survival in younger patients, in contrast to the effect observed for TGFB2. This discrepancy may stem from TGFB1’s pleiotropic and context-dependent functions—it can act as a tumor suppressor in early PDAC stages by enforcing growth arrest, yet also promote late-stage progression via fibrosis and immune evasion. Moreover, TGFB1 expression may be governed by epigenetic mechanisms beyond promoter methylation, such as histone modifications or enhancer activity, weakening the predictive utility of methylation status alone. In contrast, TGFB3 showed no consistent association with overall survival despite demonstrating a strong inverse correlation between methylation and expression. This suggests that while TGFB3 is epigenetically regulated, its downstream effects may be redundant or compensated for by TGFB1/2 activity in PDAC. It is also possible that TGFB3’s role is more prominent in developmental or wound-healing contexts and does not independently drive aggressive tumor behavior in pancreatic cancer. Finally, IL6 expression correlated with poor outcomes only in younger patients, likely reflecting the greater impact of IL6-driven inflammation and immunosuppression in a competent immune microenvironment. In older patients, immunosenescence and baseline inflammation may obscure IL6’s effects, diminishing its prognostic value in this group.
We also identified epigenetic regulation as a key modulatory mechanism, demonstrating that increased
TGFB2 promoter methylation correlates with improved OS specifically in younger patients, presumably due to the gene silencing effects reducing TGFβ2 expression. Interestingly, an opposite methylation effect was observed for
TGFB1, suggesting distinct epigenetic regulatory mechanisms among TGF-β isoforms and highlighting the complex interplay of methylation patterns with gene expression and clinical outcomes. A possible explanation hinges on the idea that
TGFB2 and
TGFB1 are subject to distinct epigenetic regulatory controls that lead to different functional outcomes. In the case of
TGFB2, increased promoter methylation appears to induce gene silencing, thereby reducing its expression. This silencing likely diminishes the pro-tumorigenic effects that
TGFB2 normally exerts—such as promoting a fibrotic and immunosuppressive tumor microenvironment—which in turn correlates with improved OS in younger patients. In contrast, the opposite methylation effect observed for
TGFB1 suggests that its promoter methylation does not similarly repress gene expression. The regulation that is specific to isoforms emphasizes the intricate relationship between methylation patterns, gene expression, and clinical outcomes [
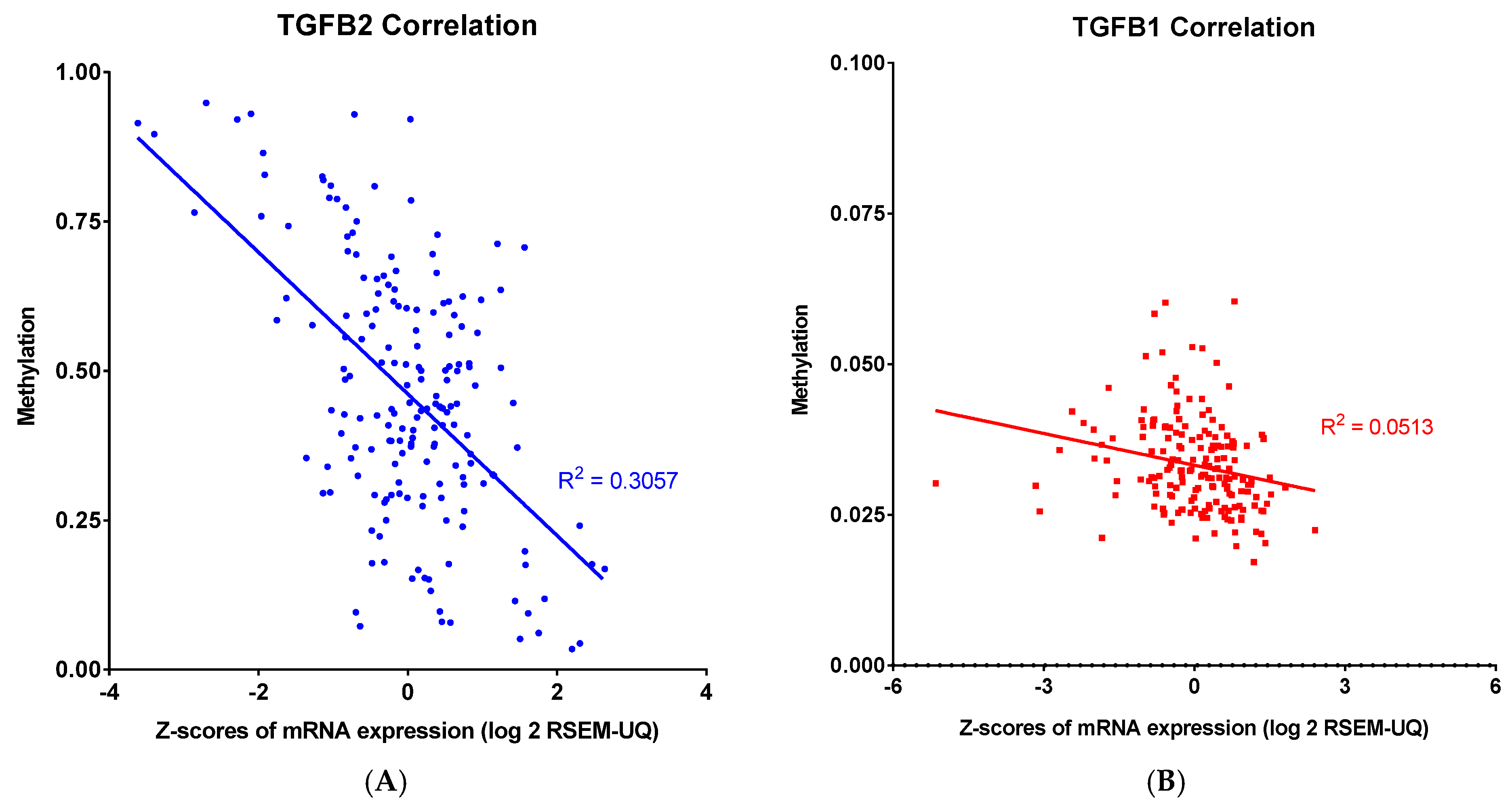
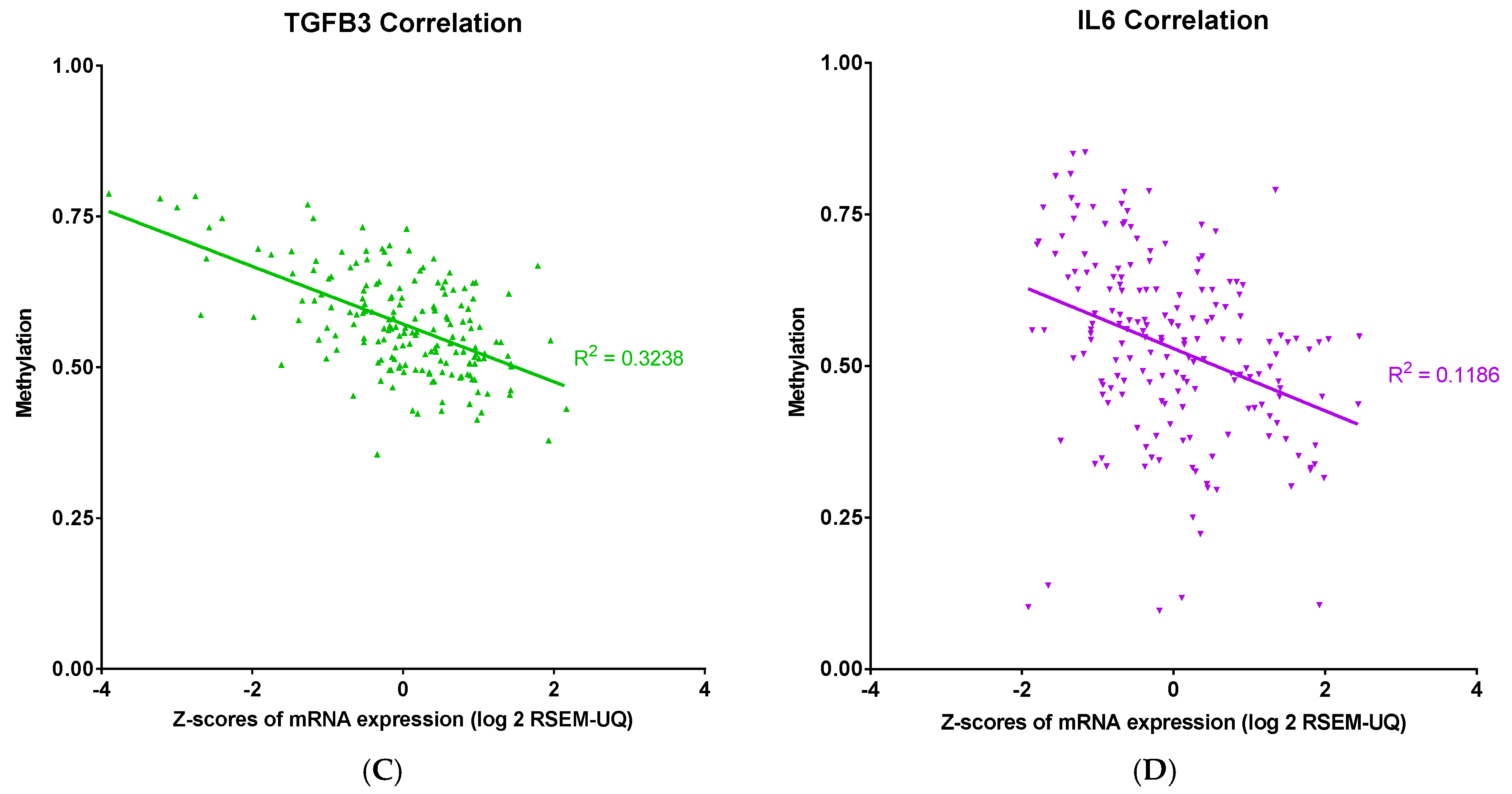
34]. The observed inverse correlation between promoter methylation and mRNA expression for TGFB2 and TGFB3 suggests that these isoforms harbor DNA elements—such as well-defined CpG islands—that are particularly vulnerable to methylation-induced silencing. When methylation occurs in key regions, it may hinder the binding of transcription factors or attract methyl-binding repressor proteins, such as MeCP2, leading to the silencing of gene expression. Specific methylation patterns, such as those found between positions -666 and -426 relative to the transcription start site in the IL6 promoter, can serve as binding sites for these repressive proteins [
35]. Although this study directly addressed
IL6, a similar mechanism may be at play in
TGFB2 and
TGFB3, contributing to their robust inverse correlations between methylation and expression. In sharp contrast,
TGFB1 and
IL6 showed weaker or absent correlations with promoter methylation. This suggests that these genes are likely governed by additional or alternate regulatory pathways that diminish the sole impact of DNA methylation. Although IL6’s promoter methylation is critical in gene silencing—as evidenced by its binding to MeCP2 and H3meK9 in non-expressing cell lines [
35]—its overall expression might be modulated by potent cytokine inducers like TNF-α, which can override methylation-mediated repression under certain conditions. Thus, the strong inverse correlations for
TGFB2 and
TGFB3 suggest that their genomic regions contain methylation-sensitive elements that directly impact transcription, whereas
TGFB1 and
IL6 are under the influence of layered regulatory inputs. These insights underline the importance of considering gene-specific promoter contexts and the complexity of epigenetic regulation. By selectively modulating these distinct regulatory axes, this could open new avenues for targeted therapeutic interventions.
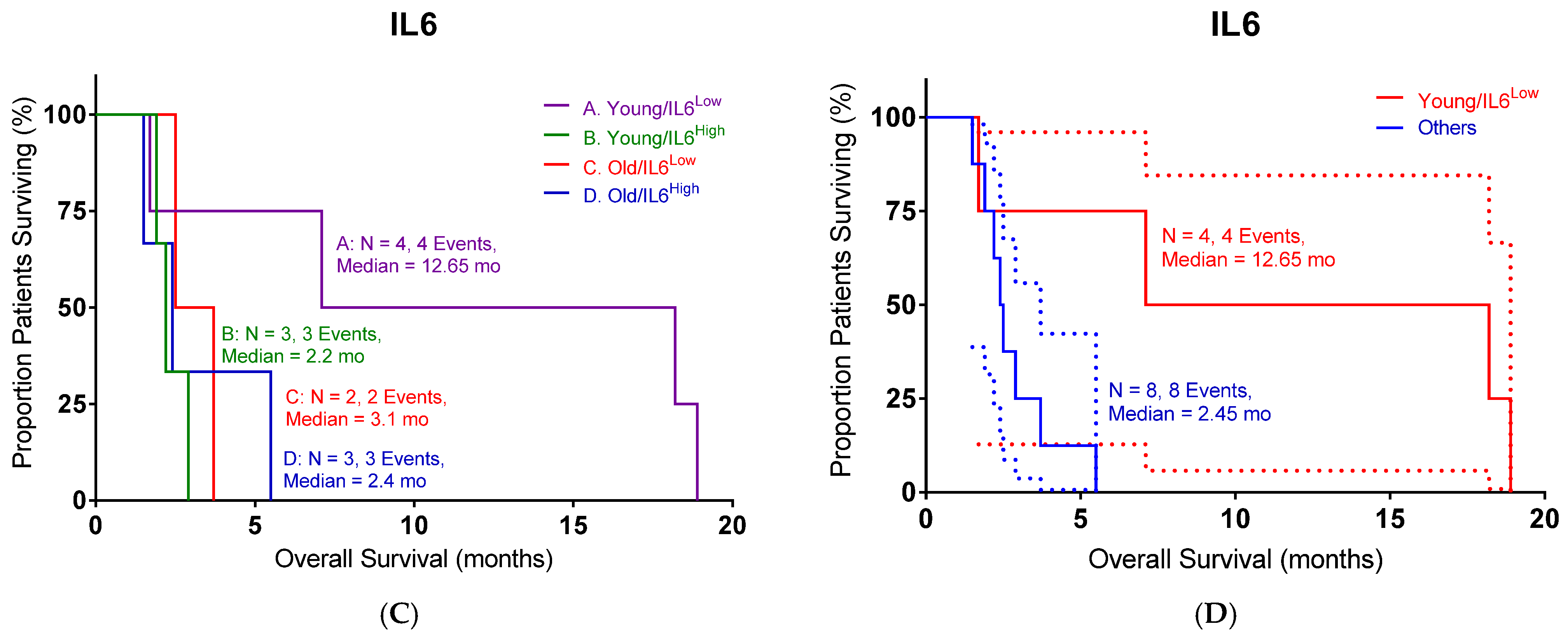
Clinically, our findings were validated by data from the OT-101 Phase I/II clinical trial, where the antisense oligodeoxynucleotide specifically targeting TGFB2 significantly improved OS in younger PDAC patients relative to older patients. TGFB isoforms, particularly TGFB2, play pivotal roles in PDAC progression by modulating key mechanisms such as immunosuppression, angiogenesis, metastasis, and the tumor microenvironment. Elevated levels of TGF-β2 are associated with the aggressive advancement of pancreatic cancer [
36,
37]. Clinical observations underscore that the dual role of TGFβ signaling—in particular, its context-dependent function as both a tumor suppressor and promoter—has complicated the efforts to target this pathway therapeutically. Trabedersen (OT-101) is an antisense oligodeoxynucleotide specifically designed to inhibit TGFB2 mRNA. Preclinical investigations have demonstrated that inhibiting TGFB2 can reduce cell proliferation and migration and reverse TGFB2-mediated immunosuppression. One study found that trabedersen diminished the secretion of TGF-β2 in human pancreatic cell lines and effectively inhibited the migration of pancreatic ductal adenocarcinoma (PDAC) cells [
16]. This mode of action attenuates the fibrotic and immunosuppressive tumor microenvironment and provides a strong rationale for its use as a therapeutic agent in PDAC. Clinical findings indicate that targeting specific isoforms, particularly TGFβ2, might be more beneficial than broad TGFβ inhibition, as our results indicate that elevated levels of TGFβ2 expression adversely affected OS primarily in younger patients with PDAC. Moreover, our studies suggest that
TGFB2 and
TGFB3 may contain DNA elements particularly vulnerable to methylation-induced silencing, resulting in significant inverse correlations between promoter methylation and mRNA expression. This suggests that the biological roles of TGFB2 and TGFB3 may exhibit a more linear or unidirectional impact on disease progression. In contrast, TGFB1 and IL6 are influenced by additional regulatory factors, which may complicate the potential benefits of targeting these pathways. This isoform-specific vulnerability may contribute to the observed improved outcomes when TGFβ2 is precisely targeted. TGFB2 not only facilitates fibrosis but also fosters an immunosuppressive setting. Thus, inhibiting TGFB2 could potentially enhance T cell-mediated cytotoxicity, as evidenced by recent studies showing increased infiltration of CD8+ T cells and a reduction in regulatory T cells [
38]. Conversely, in tumors where TGFβ signaling redundancy or compensatory pathways exist, the blockade of one pathway component might not be sufficient to reverse immunosuppression or tumor progression. Data from the OT-101 Phase I/II clinical trial support the targeting of TGFB2 for therapeutic purposes. The findings indicate that an antisense oligodeoxynucleotide specifically aimed at TGFB2 notably enhanced overall survival in younger patients with pancreatic ductal adenocarcinoma when compared to older patients. This suggests that certain patient subgroups, potentially characterized by unique epigenetic or microenvironmental factors, may experience greater benefits from TGFB2 inhibition. Coupled with encouraging preclinical results—such as the inhibition of cell proliferation, migration, and the reversal of immunosuppression—alongside positive clinical outcomes in younger individuals, OT-101 shows promise as a component of combination treatment strategies for PDAC. However, the necessity to further elucidate which patients are most likely to respond based on molecular and epigenetic tumor profiles remains, thereby optimizing the use of OT-101 in a precision medicine approach.
The age-related differences in TGFB2 expression and methylation may reflect a shift in the tumor microenvironment and immune response, particularly in the context of T cell engagement and mesenchymal–epithelial transition. The hypermethylation of
TGFB2 is associated with lower TGFB2 expression and improved patient survival. Importantly, multivariate analysis shows that this phenomenon is independent of SMAD4 and canonical TGFβ signaling, suggesting a non-SMAD, immune-related role for TGFB2 methylation [
39]. Additionally,
TGFB2 methylation correlates inversely with numerous T cell receptor (TCR) signaling components—HLA-D molecules, CD3D, CD28, and LCK—all of which are upregulated in the tumor when
TGFB2 is weakly methylated [
39]. This suggests that low methylation (high TGFB2 expression) may suppress T cell engagement and undermine a robust adaptive immune response, while high methylation (low TGFB2) may allow greater T cell infiltration and activity. Finally, the expression of TGFB2 is associated with the genes involved in mesenchymal–epithelial transition [
40]. Tumors with low
TGFB2 methylation may be more prone to a mesenchymal phenotype, which typically correlates with an immunosuppressive microenvironment and reduced T cell infiltration. Age-related epigenomic alterations might influence this process by adding methyl groups to
TGFB2, thereby dampening its expression and shifting the tumor toward a more “epithelial-like” and less immunosuppressive state [
41]. Clinically, higher
TGFB2 methylation corresponds to a more robust T cell-mediated immune response and a less mesenchymal, less aggressive tumor, contributing to improved patient survival. Furthermore, this profile may help identify patients who might respond to immunotherapy (such as T cell receptor therapies or checkpoint inhibitors) and MET-targeted therapies (like trametinib or CAR-M-c-MET) [
42,
43]. Aging leads to significant changes in the immune system, a phenomenon referred to as immunosenescence. This process is characterized by several key features, including the involution of the thymus, which restricts the production of new naïve T cells, an imbalance between naïve and memory T cells, altered metabolic processes, and extensive epigenetic changes. The disruption of T cell populations, along with persistent antigen stimulation, contributes to the early senescence of immune cells. As these senescent immune cells age, they develop a proinflammatory secretory phenotype that intensifies the phenomenon known as inflammaging [
44]. This overall decline results in a reduced capacity to mount antitumor immune responses, which is why older patients often experience a diminished benefit from therapies that rely on a robust immune system. Several studies provide evidence for these age-related alterations. The chronic inflammatory state or inflammaging observed in older individuals further blunts the immune rescue mechanisms that might otherwise compensate for the tumor’s escape signals. Given the documented decline in immune competence with age, it becomes critical to tailor immunotherapeutic strategies for older patients. The idea behind age-specific dosing and immuno-priming is that reversing or lessening immune senescence could improve the effectiveness of cancer treatments. Younger patients, who retain a more effective pool of cytotoxic T and NK cells, can capitalize on the uncloaked tumor environment following TGFB2 blockade. In contrast, older patients—with their age-related immune deficits—may gain incremental benefit from a dual strategy where TGFB2 inhibition is paired with immuno-priming to overcome the blunted immune response. This dual approach aims to excise key immunosuppressive nodes while simultaneously boosting the residual immune function in older hosts. The successful implementation of age-specific dosing or immuno-priming requires well-designed, biomarker-guided clinical studies. For example, evaluating dynamic pharmacodynamic readouts such as IL-6 or phospho-STAT3 levels will help determine the optimal timing and dosing of these interventions in conjunction with TGFB2 blockade. The identification of age-related epigenetic profiles may further allow for the rational combination of agents (e.g., DNMT inhibitors for hypermethylation of TGFB2 loci) with immuno-priming therapies to enhance treatment durability.
This study has some notable limitations and therefore primarily generates a hypothesis that should be confirmed with additional studies to be performed in the future, primarily due to the use of bioinformatics analyses of the TCGA dataset. Additional laboratory confirmation of TGFB1, TGFB2, TGFB3, and IL6 gene methylation and gene expression would be needed for further validation. The validation of the mRNA markers will require techniques such as quantitative RT-PCR and immunohistochemistry. It is possible that these differences are reflective of age-dependent changes in immunity; therefore, we are actively looking at identifying immune cells involved in the tumor microenvironment responsible for these observations. We attempted to validate the TCGA analyses using data from our Phase I/II PDAC trial for OT-101, a suppressor of TGFB2. A number of limitations should be pointed out for our clinical study, including its heterogeneous nature, single-arm design, and small size for the patient population. It will be important to further evaluate the clinical potential of OT101 in a larger and more homogenous patient population in our current Phase III PDAC trial, OT-01-P201 (NCT06079346). OT-01-P201 is designed as a randomized, open-label, active-controlled, multicenter Phase IIB/III study designed to compare the efficacy and safety of OT-101 in combination with modified FOLFIRINOX (folinic acid, 5-FU, irinotecan, and oxaliplatin) to modified FOLFIRINOX alone in patients with advanced and unresectable or metastatic pancreatic cancer.
4. Materials and Methods
4.1. Domain-Specific Identification of PubMed Articles Augmented by Artificial Intelligence
After searching PubMed using appropriate keywords (aging, cancer, il6, tgfbeta, methylation, and pancreatic cancer), the resulting 19,510 abstracts were downloaded as text documents for processing using the Chatbot-enabled tools developed at Oncotelic Therapeutics (Agoura Hills, CA, USA). Each abstract was then (aided using puppeteer 19.11.1) embedded and transformed (langchain-openai 0.2.3, openai 1.52.0) into a vector of numbers capturing semantic similarity between text elements (tokens) and then stored in our Qdrant vector database (
https://qdrant.tech/). Semantically similar abstracts were transformed into the same vector “embedding” space, as the embedding model was trained to minimize the distance between pairs of abstracts in this space. Using an agglomerative clustering algorithm (hdbscan 0.8.39) to group the vectors, we automatically labeled these clusters using the question-answering model to identify any similarity between the abstracts corresponding to each cluster’s vectors. During the question-answering process, the user’s query was converted into an embedding vector. A similarity metric, such as cosine similarity, was then utilized to find the embedded abstract vectors nearest to the vector representing the query. The abstracts that corresponded to the nearest vectors were subsequently provided to the question-answering model as context, alongside the original query, to produce a response to the user’s question.
The React framework served as the backbone of the user interface, providing an open source and flexible solution for developing powerful front-end user interfaces (
https://react.dev/, accessed on 25 March 2024). In addition, we used the @mui/material (
https://mui.com/, accessed on 25 March 2024) libraries for the interface’s design aspects and aimed to follow the material design guidelines closely. Serving the front end was Node.Js (
https://nodejs.org/en, accessed on 25 March 2024). The Node.js libraries included in the project were @adobe/pdfservices-node-sdk 3.4.2@aws-sdk/client-s3 3.412.0, @langchain/community 0.2.5, @material-ui/core 4.12.4, @mui/base 5.0.0-beta.18, @mui/icons-material 5.11.16, @mui/material 5.15.20, @mui/styled-engine-sc 5.12.0, @mui/x-date-pickers 6.15.0, @qdrant/js-client-rest 1.4.0, carrot2 0.0.1, pdf2img 0.5.0, pdfjs-dist 4.5.136, puppeteer 19.11.1, react 18.2.0, sequelize 6.31.1, and zod 3.22.4.
The integration of our Chatbot technology applied to PubMed abstracts facilitated the rapid discovery of key primary publications used in the writing of this manuscript.
4.2. TCGA and TNM Data
Clinical and transcriptomic data of pancreatic ductal adenocarcinoma (PDAC) patients were obtained from The Cancer Genome Atlas (TCGA) database via the cBioPortal web analysis portal (
https://www.cbioportal.org/study/summary?id=paad_icgc%2Cpaad_qcmg_uq_2016%2Cpaad_tcga%2Cpaad_tcga_pan_can_atlas_2018%2Cpaad_utsw_2015%2Cpaad_cptac_2021, accessed on 13 April 2025). The dataset used in this study corresponds to the TCGA-PAAD (Pancreatic Adenocarcinoma) project to determine the prognostic impact of TGFB1, TGFB2, TGFB3, and IL6 median expression cut-off values for high versus low patient sub-groupings on OS for all PDAC patients (
n = 355) and PDAC patient with different methylation levels (
n = 185). Data were downloaded in accordance with TCGA guidelines and usage policies. The data portal offers the option to view gene expression as Z-scores for transcripts per million (TPM), calculated using RNA-Seq with the expectation-maximization (RSEM) algorithm [
45]. Briefly, RSEM normalizes TPM through a three-step process. It first aligns RNA-Seq reads to a reference transcriptome using a probabilistic expectation-maximization (EM) algorithm to estimate the origins of multi-mapping reads. Next, it calculates the expected number of fragments per transcript, considering transcript length and sequencing depth. Finally, RSEM computes reads per kilobase (RPK) for each transcript and scales these values to achieve a total of one million, yielding TPM = (RPK/sum RPKs) × 10
6. The TPM values are then log2-transformed.
The mRNA expression levels of target genes and correlation analysis in pancreatic ductal adenocarcinoma (PDAC) tumor and normal tissues were analyzed using the TNMplot public database (
https://tnmplot.com/analysis/, accessed on 13 April 2025).
The gene expression data normalization method for RNA-Seq data in TNMplot involves a two-step process. In the first step, DESeq2 algorithm employs the median-of-ratios method to normalize raw aligned HTSeq-counts by estimating size factors; it computes the geometric mean of counts for each gene across all samples, calculates the ratio of each gene’s count to this geometric mean for each sample, and determines the size factor as the median of these ratios. Raw counts are then divided by their respective size factors, thus correcting for variations in sequencing depth and RNA composition. The second step typically involves an additional scaling normalization to further harmonize the data, especially when merging datasets across multiple sources, such as cancers for TCGA and normal tissue counts from GTEx [
46].
In cBioPortal, methylation levels are represented as beta-values, which range from 0 (indicating unmethylated) to 1 (indicating fully methylated), related to the proportion of methylated signal intensity relative to the total signal (methylated and unmethylated). To account for the presence of multiple probes associated with a single gene, cBioPortal selects a representative probe, typically the one most anti-correlated with gene expression.
Survival analyses and linear correlation analyses were performed using GraphPad Prism version 6.7 for Windows (Boston, MA, USA).
4.3. OS Outcomes and IL6 Levels for PDAC Patients Treated with OT-101
Our clinical trial (NCT00844064) was approved by the Ethics Committee of the Charité Berlin Campus VirchowKlinikum (Berlin, Germany). Written informed consent was obtained from all study subjects, and all participating centers provided ethical committee approval.
The Phase I/II trial of trabedersen (AP 12009/OT-101) for pancreatic ductal adenocarcinoma (PDAC) was designed as an open-label, multi-center dose-escalation study to assess the safety and tolerability of OT-101 in adult patients with TGF-β2 overproducing advanced solid tumors. Age at diagnosis was used, thus avoiding confounding factors such as prior chemotherapy, radiotherapy, or surgical interventions. The study incorporated a cohort-based dose-escalation strategy, enrolling 3 to 6 patients per cohort at increasing dose levels until the maximum tolerated dose (MTD) was determined. Upon reaching the MTD, additional patients were treated at the recommended Phase II dose. The trial featured both initial (7-day continuous infusion every 2 weeks) and modified (4-day continuous infusion every 2 weeks) schedules, with dose levels up to 480 mg/m2/day and 590 mg/m2/day, respectively. The study consisted of a core period involving two full cycles of therapy, with the option for patients showing clinical benefit or stable disease to receive up to eight additional extension cycles, totaling ten cycles. Follow-up visits were scheduled every 8 weeks post-infusion, regardless of the number of cycles completed. Inclusion criteria required patients to be between 18 and 75 years old, with histologically confirmed Stage IVA or IVB pancreatic cancer, a Karnofsky performance status of at least 80%, and adequate organ function. Exclusion criteria included inability to comply with protocol; active infections such as HIV, HBV, or HCV; significant cardiovascular issues; brain metastases; and recent antitumor therapies. The primary endpoint was the determination of the MTD, while secondary endpoints involved safety assessments, cardiac monitoring, tumor response, overall survival, TGF-β2 plasma concentrations, and pharmacokinetic profiling of AP 12009. Comprehensive safety assessments were maintained throughout the study, including vital signs, physical exams, ECGs, laboratory tests, and adverse event monitoring. Tumor assessments were conducted via CT scans every 8 weeks to evaluate response categories such as complete response, partial response, stable disease, and progressive disease. Biomarker analyses included evaluating AP 12009 pharmacokinetics and TGF-β2 levels, as well as tumor markers CA 19-9 and CEA, which are crucial indicators in advanced PDAC.
Safety assessments in this study encompassed adverse events (AEs), laboratory analyses (hematology, biochemistry, and urinalysis), electrocardiograms (ECGs), cardiac monitoring, physical examinations, vital signs, and performance status measurements. All adverse events (AEs) were listed using coding for System Organ Class (SOC) and Preferred Term (PT) (using the MedDRA version 9.0 or later). Treatment-emergent AEs (TEAEs) were defined as any AEs occurring or worsening after the start (date and time) of the first infusion and before 28 days after the last treatment (stop day of last infusion, including extension cycles). Moreover, AEs occurring or worsening later than 4 weeks after the last treatment were also defined as treatment-emergent if these were considered to be related to the study drug. Dose-limiting toxicities (DLTs) and unacceptable toxicities were captured during the core study period (two cycles) and, if applicable, during extension cycles. These events were exhaustively tracked to guide dose-escalation decisions and ensure patient safety. DLTs or unacceptable toxicities were summarized by cycle and by schedule, cohort, and indication, for final- and recommended-dose cohorts. Investigators also recorded action taken with respect to the investigational product and other interventions as needed. Each AE was classified by system organ class (SOC) and preferred term (PT), with additional analysis by severity (graded using NCI-CTC grades or 4-point-severity scale if NCI-CTC grades were not available), relationship to trial medication, action taken (e.g., dose interrupted, dose reduced, study drug withdrawn), outcome, and seriousness. Laboratory data included hematology, biochemistry, and urinalysis. Investigators flagged out-of-range values as clinically relevant (clin. rel.) or non-clinically relevant (non-clin. rel.). Laboratory values were converted to SI units, and reference ranges were standardized to facilitate comparability across sites. For hematology and serum chemistry, NCI-CTC grades are reported for those hematology and biochemistry parameters where NCI-CTC grading is available using NCI-CTC Lab criteria (NCI-CTC v2.0).
Efficacy was primarily assessed via imaging-based tumor response (RECIST criteria) with computed tomography (CT) scans performed every 8 weeks, as well as through time-related endpoints such as time to progression (TTP), progression-free survival (PFS), and overall survival (OS). The results of tumor assessments were analyzed in the evaluable efficacy population. Tumor markers (e.g., CA 19-9 and/or CEA) were also measured in patients with pancreatic or colorectal cancer.
The study used RECIST-based categories of complete response (CR), partial response (PR), stable disease (SD), and progressive disease (PD). An additional category of unknown (UK) was applied if no definitive assessment could be made. For each 8-week interval, investigators evaluated the overall best response; rates of CR, PR, SD, and PD were summarized. The “best overall tumor response” referred to the best response the patient achieved at any of the scheduled assessments. Response-related endpoints included the complete response rate (CRR), the partial response rate (PRR), the overall response rate (CR + PR), and the tumor growth control rate (CR + PR + SD). Time to progression and PFS were analyzed using Kaplan–Meier methods, with summaries including median estimates in days, weeks, months, and 95% confidence intervals. Overall survival was similarly evaluated by Kaplan–Meier analysis. Non-deceased or lost-to-follow-up patients were censored at the last date known to be alive.
The following 31 analytes were measured: EGF, eotaxin, FGF-basic, G-CSF, granulocyte–monocyte colony-stimulating factor, HGF, IFN-α, IFN-γ, IL-1RA, IL-1β, IL-2, IL-2R, IL-4, IL-5, IL-6, IL-7, IL-8, IL-10, IL-12 (p40/p70), IL-13, IL-15, IL-17, IP-10, MCP-1, MIG, MIP-1α, MIP-1β, RANTES, TNF-α, VEGF, and MICA. Cyto-/chemokine concentration in pg/mL for each plasma sample was measured in duplicate. In cases where the concentration was too low to be determined, the values of the detection limit were used for further calculations. Detection limits were provided by the manufacturer of the assay (Lophius Biosciences). In cases where the concentration was too high to be determined, the 1.5-fold value of the highest standard for the applicable cyto-/chemokine that was measured on the plate was used for further calculations. Plasma levels of IL6 were tracked over three cycles of OT-101 therapy (140 mg/m2/day) in 12 PDAC patients. Samples were acquired before the onset of OT-101 therapy and at eight selected time points during therapy.


 ,
, 



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}