


Exploring the Impact of Extraplatelet Content on Fibrin-Based Scaffold Performance for Regenerative Therapies

 and
and
Abstract

1. Introduction
2. Results
2.1. BPCP Shows a Two-Fold Increase of Both Platelet and Fibrinogen Levels
2.2. BPCP Fibrin Scaffold Fibers Have a Wider Diameter and Smaller Pore Size than sPRP Scaffold Fibers
2.3. Biomechanical Behavior
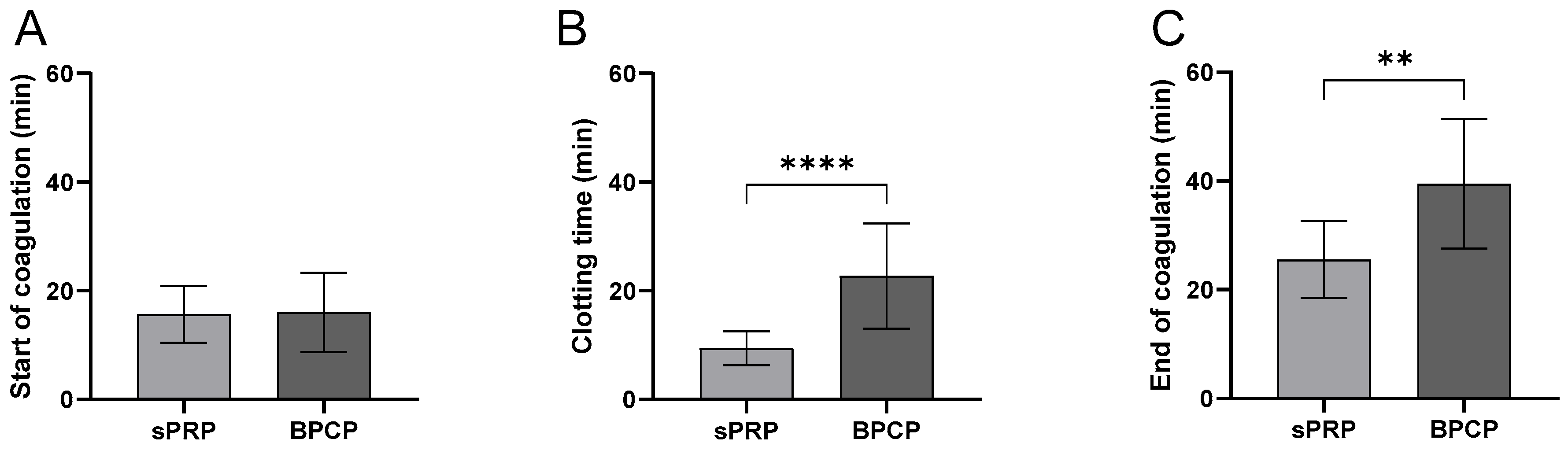
2.3.1. BPCP Shows a Deceleration of the Coagulation Process
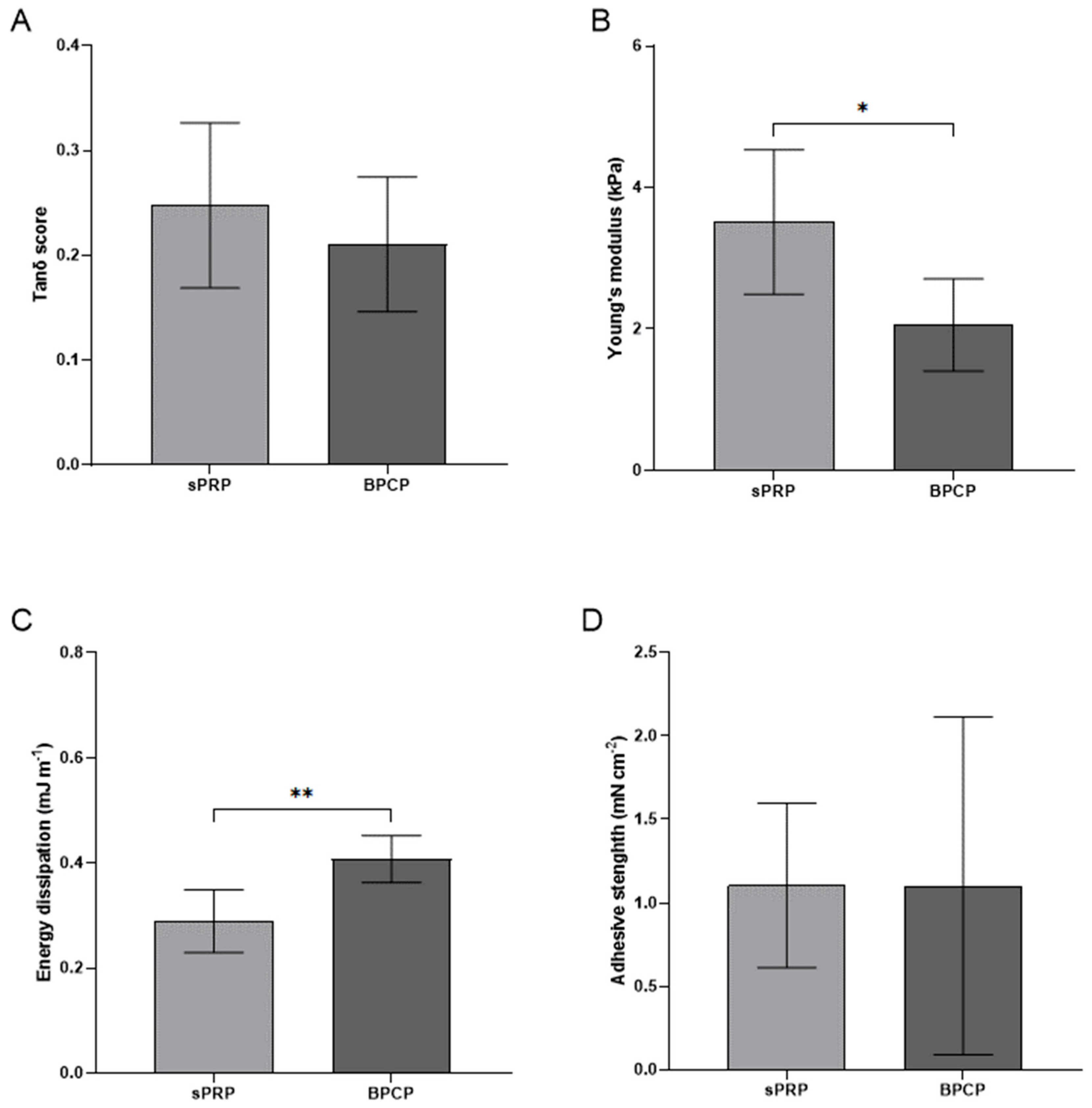
2.3.2. BPCP Exhibits a More Solid, Consistent and Stiffer Formulation
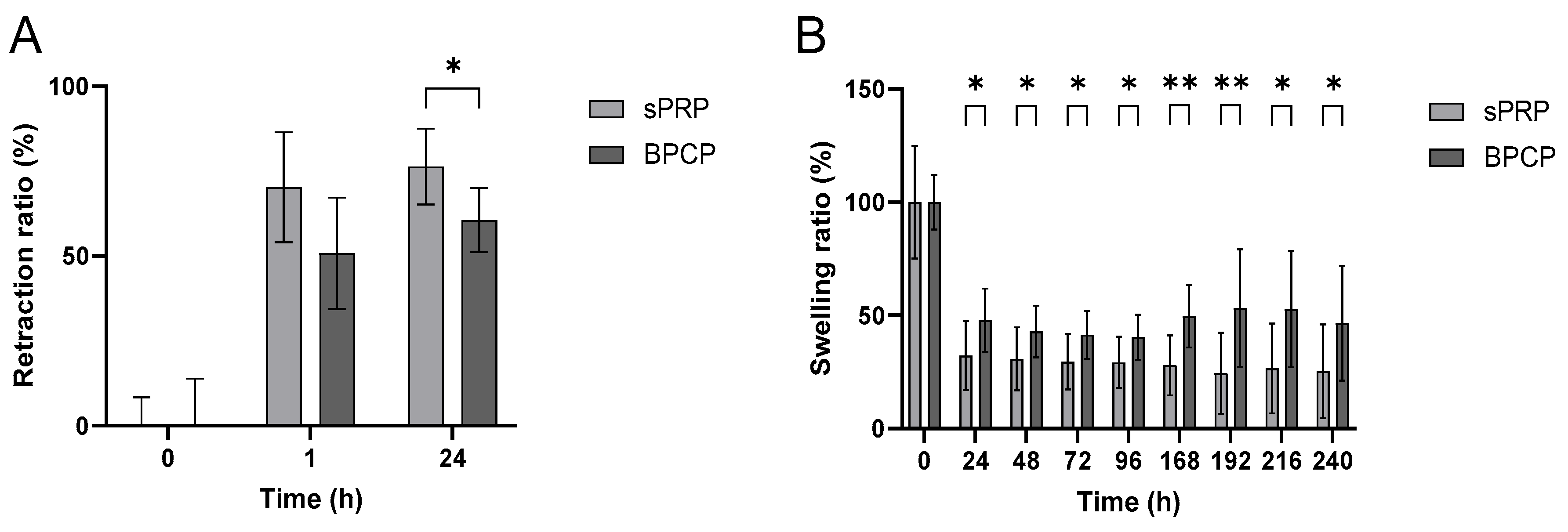
2.3.3. Retraction and Swelling Capacity
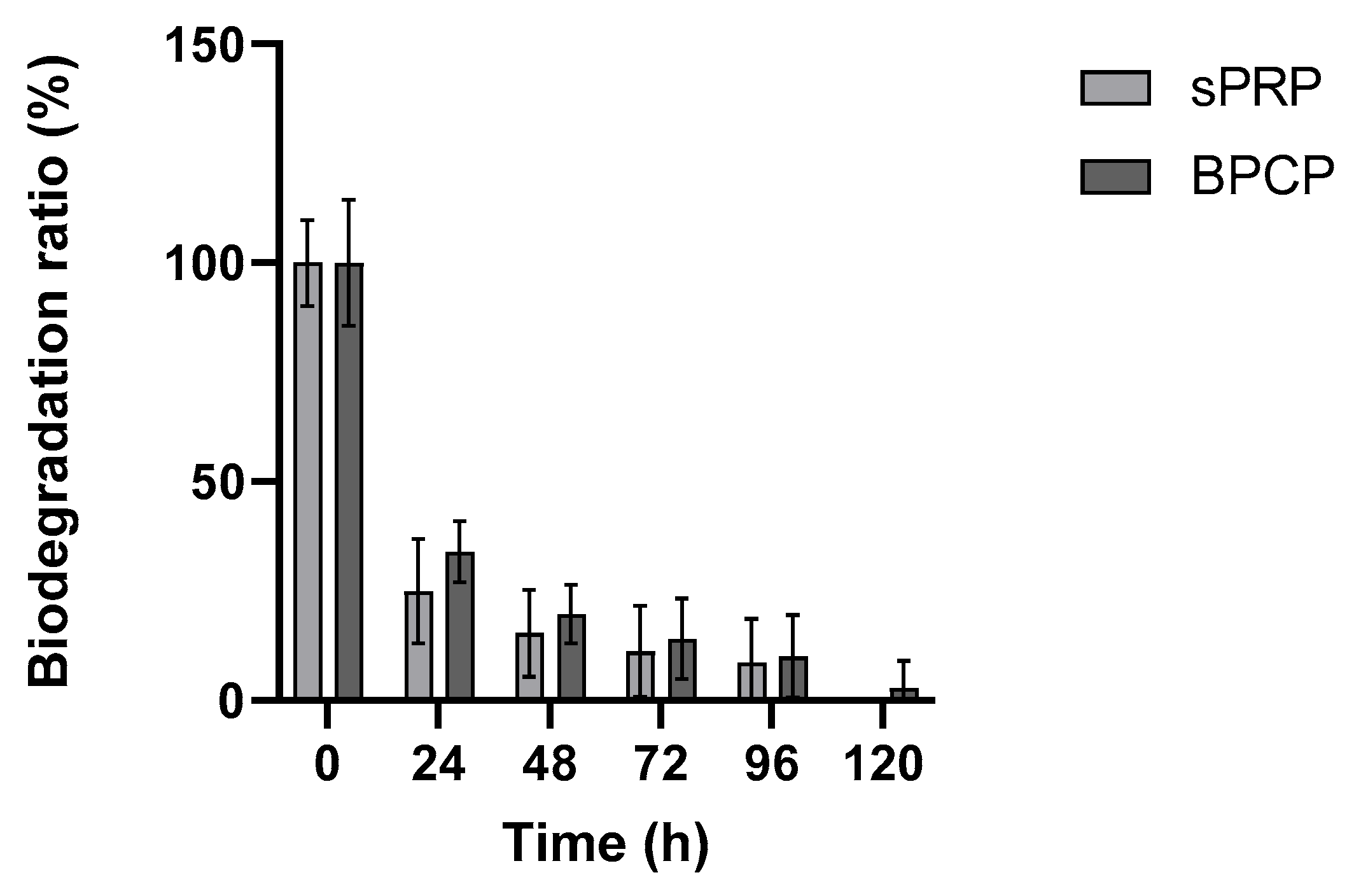
2.3.4. sPRP and BPCP Show a Similar Biodegradation Pattern
2.4. Release Kinetics
2.4.1. There Is a Higher Release of Growth Factors by BPCP, Especially on the First Day
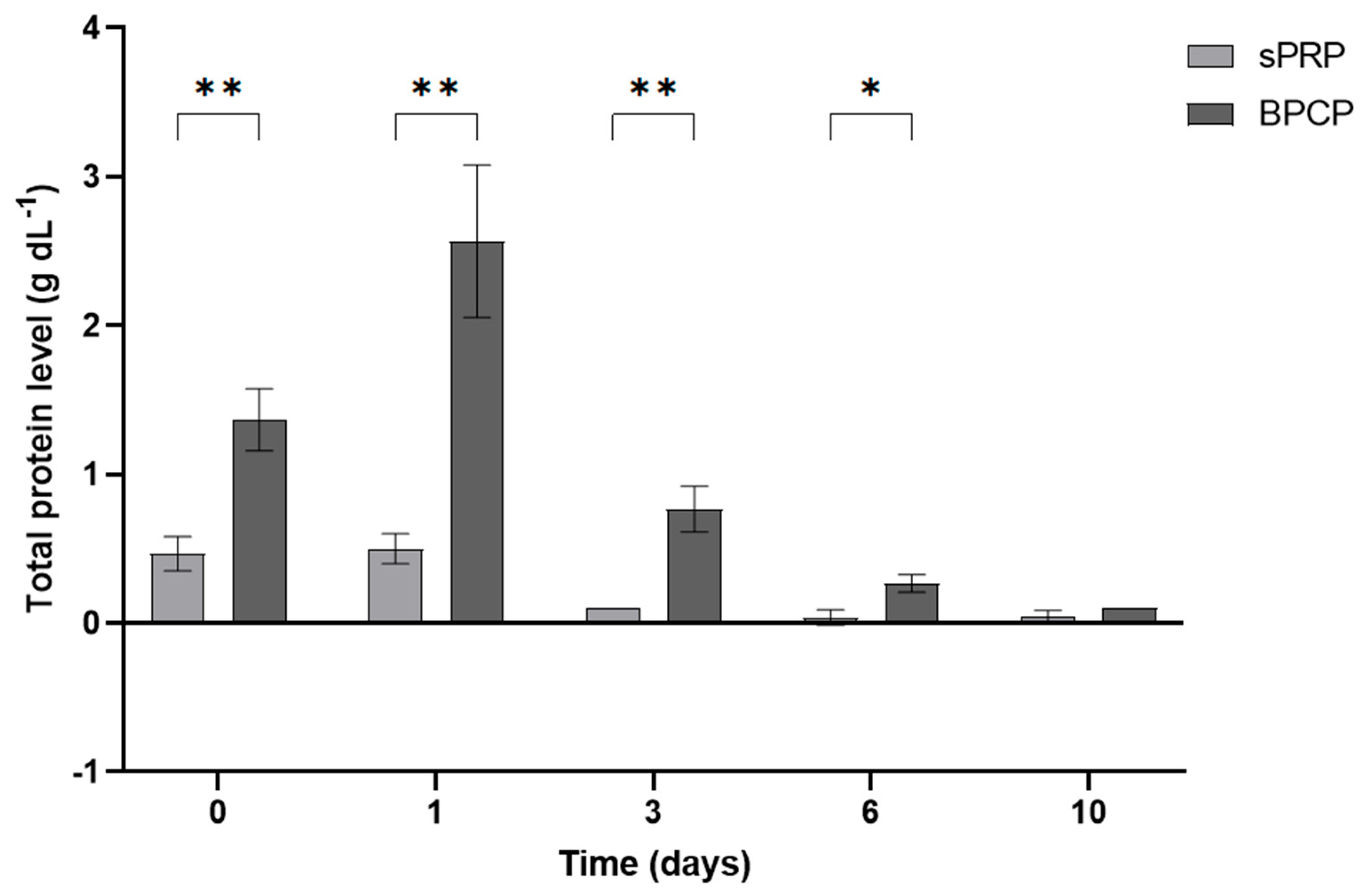
2.4.2. The Total Amount of Released Protein Is Higher in BPCP
3. Discussion
4. Materials and Methods
4.1. Sample Collection and Preparation
4.1.1. Donors
4.1.2. Standard Platelet-Rich Plasma Preparation
4.1.3. Balanced Protein-Concentrate Plasma Preparation
4.2. Platelet and Fibrinogen Level Measurement
4.3. Morphological Analysis
4.4. Biomechanical Behavior
4.4.1. Coagulation Kinetics
4.4.2. Mechanical Tests
4.4.3. Rheological Profile: Amplitude Sweep Oscillatory Test
4.4.4. Swelling and Retraction
4.4.5. Biodegradation
4.5. Release Kinetics
Platelet and Extraplatelet Growth Factor Concentration Measurements by Enzyme-like Immunosorbent Assay (ELISA) and Total Protein Release Analysis
4.6. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| A2M | Alpha-2-macroglobulin |
| BPCP | Balanced protein concentrate plasma |
| GF | Growth factor |
| HEAA | Hydroxyethyl acrylamide |
| HGF | Hepatocyte growth factor |
| IGF-1 | Insulin-like growth factor 1 |
| LVE | Linear viscoelasticity |
| OsO4 | Osmium tetroxide |
| PC | Plasma column |
| PDGF-AB | Platelet-derived growth factor AB |
| PRP | Platelet-rich plasma |
| RT | Room temperature |
| SEM | Scanning electron microscope |
| sPRP | Standard platelet-rich plasma |
| TGF-β1 | Transforming growth factor beta 1 |
| tPA | Tissue plasminogen activator |
| VEGF | Vascular endothelial growth factor |
References
- Everts, P.; Onishi, K.; Jayaram, P.; Lana, J.F.; Mautner, K. Platelet-Rich Plasma: New Performance Understandings and Therapeutic Considerations in 2020. Int. J. Mol. Sci. 2020, 21, 7794. [Google Scholar] [CrossRef] [PubMed]
- Lana, J.F.S.D.; Andrade Santana, M.H.; Dias Belangero, W.; Malheiros Luzo, A.C. (Eds.) Platelet-Rich Plasma: Regenerative Medicine: Sports Medicine, Orthopedic, and Recovery of Musculoskeletal Injuries; Lecture Notes in Bioengineering; Springer: Berlin/Heidelberg, Germany, 2014; ISBN 978-3-642-40117-6. [Google Scholar]
- Etulain, J. Platelets in wound healing and regenerative medicine. Platelets 2018, 29, 556–568. [Google Scholar] [CrossRef] [PubMed]
- Everts, P.A.; Lana, J.F.; Alexander, R.W.; Dallo, I.; Kon, E.; Ambach, M.A.; van Zundert, A.; Podesta, L. Profound Properties of Protein-Rich, Platelet-Rich Plasma Matrices as Novel, Multi-Purpose Biological Platforms in Tissue Repair, Regeneration, and Wound Healing. Int. J. Mol. Sci. 2024, 25, 7914. [Google Scholar] [CrossRef] [PubMed]
- van der Meijden, P.E.J.; Heemskerk, J.W.M. Platelet biology and functions: New concepts and clinical perspectives. Nat. Rev. Cardiol. 2019, 16, 166–179. [Google Scholar] [CrossRef]
- Pineda-Cortel, M.R.; Suarez, C.; Cabrera, J.-T.; Daya, M.; Bonifacio, R.B.L.; Vergara, R.C.; Dacanay, A.T.L.; Villavieja, A. Complexity of Platelet-Rich Plasma: Mechanism of Action, Growth Factor Utilization and Variation in Preparation. Plasmatology 2024, 18, 26348535241277625. [Google Scholar] [CrossRef]
- Knezevic, N.N.; Candido, K.D.; Desai, R.; Kaye, A.D. Is Platelet-Rich Plasma a Future Therapy in Pain Management? Med. Clin. N. Am. 2016, 100, 199–217. [Google Scholar] [CrossRef]
- Jasmine, S.; Thangavelu, A.; Krishnamoorthy, R.; Alshatwi, A.A. Platelet Concentrates as Biomaterials in Tissue Engineering: A Review. Regen. Eng. Transl. Med. 2021, 7, 419–431. [Google Scholar] [CrossRef]
- Şeker, Ş.; Elçin, A.E.; Elçin, Y.M. Current trends in the design and fabrication of PRP-based scaffolds for tissue engineering and regenerative medicine. Biomed. Mater. 2025, 20, 022001. [Google Scholar] [CrossRef]
- Barbon, S.; Stocco, E.; Macchi, V.; Contran, M.; Grandi, F.; Borean, A.; Parnigotto, P.P.; Porzionato, A.; De Caro, R. Platelet-Rich Fibrin Scaffolds for Cartilage and Tendon Regenerative Medicine: From Bench to Bedside. Int. J. Mol. Sci. 2019, 20, 1701. [Google Scholar] [CrossRef]
- Anitua, E.; Sánchez, M.; Orive, G. Potential of endogenous regenerative technology for in situ regenerative medicine. Adv. Drug Deliv. Rev. 2010, 62, 741–752. [Google Scholar] [CrossRef]
- Ahmed, T.A.E.; Dare, E.V.; Hincke, M. Fibrin: A versatile scaffold for tissue engineering applications. Tissue Eng. Part B Rev. 2008, 14, 199–215. [Google Scholar] [CrossRef] [PubMed]
- Anitua, E.; Zalduendo, M.; Troya, M.; Tierno, R.; Alkhraisat, M.H. Cellular composition modifies the biological properties and stability of platelet rich plasma membranes for tissue engineering. J. Biomed. Mater. Res. A 2023, 111, 1710–1721. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi-Ataabadi, M.; Mostafavi-pour, Z.; Vojdani, Z.; Sani, M.; Latifi, M.; Talaei-Khozani, T. Fabrication and characterization of platelet-rich plasma scaffolds for tissue engineering applications. Mater. Sci. Eng. C 2017, 71, 372–380. [Google Scholar] [CrossRef]
- Brown, A.C.; Barker, T.H. Fibrin-based biomaterials: Modulation of macroscopic properties through rational design at the molecular level. Acta Biomater. 2014, 10, 1502–1514. [Google Scholar] [CrossRef]
- Sanz-Horta, R.; Matesanz, A.; Gallardo, A.; Reinecke, H.; Jorcano, J.L.; Acedo, P.; Velasco, D.; Elvira, C. Technological advances in fibrin for tissue engineering. J. Tissue Eng. 2023, 14, 20417314231190288. [Google Scholar] [CrossRef]
- Anitua, E.; Pino, A.; Troya, M.; Jaén, P.; Orive, G. A novel personalized 3D injectable protein scaffold for regenerative medicine. J. Mater. Sci. Mater. Med. 2017, 29, 7. [Google Scholar] [CrossRef] [PubMed]
- Cha, C.; Kim, S.Y.; Cao, L.; Kong, H. Decoupled control of stiffness and permeability with a cell-encapsulating poly(ethylene glycol) dimethacrylate hydrogel. Biomaterials 2010, 31, 4864–4871. [Google Scholar] [CrossRef]
- Jansen, E.E.; Hartmann, M. Clot Retraction: Cellular Mechanisms and Inhibitors, Measuring Methods, and Clinical Implications. Biomedicines 2021, 9, 1064. [Google Scholar] [CrossRef]
- Nurden, A.T. Molecular basis of clot retraction and its role in wound healing. Thromb. Res. 2022, 231, 159–169. [Google Scholar] [CrossRef]
- Lei, Y.; Bortolin, L.; Benesch-Lee, F.; Oguntolu, T.; Dong, Z.; Bondah, N.; Billiar, K. Hyaluronic acid regulates heart valve interstitial cell contraction in fibrin-based scaffolds. Acta Biomater. 2021, 136, 124–136. [Google Scholar] [CrossRef]
- Rojas-Murillo, J.A.; Simental-Mendía, M.A.; Moncada-Saucedo, N.K.; Delgado-Gonzalez, P.; Islas, J.F.; Roacho-Pérez, J.A.; Garza-Treviño, E.N. Physical, Mechanical, and Biological Properties of Fibrin Scaffolds for Cartilage Repair. Int. J. Mol. Sci. 2022, 23, 9879. [Google Scholar] [CrossRef] [PubMed]
- Beitia, M.; Delgado, D.; Mercader, J.; Sánchez, P.; López de Dicastillo, L.; Sánchez, M. Action of Platelet-Rich Plasma on In Vitro Cellular Bioactivity: More than Platelets. Int. J. Mol. Sci. 2023, 24, 5367. [Google Scholar] [CrossRef] [PubMed]
- Passaretti, F.; Tia, M.; D’Esposito, V.; De Pascale, M.; Del Corso, M.; Sepulveres, R.; Liguoro, D.; Valentino, R.; Beguinot, F.; Formisano, P.; et al. Growth-promoting action and growth factor release by different platelet derivatives. Platelets 2014, 25, 252–256. [Google Scholar] [CrossRef]
- Caruana, A.; Savina, D.; Macedo, J.P.; Soares, S.C. From Platelet-Rich Plasma to Advanced Platelet-Rich Fibrin: Biological Achievements and Clinical Advances in Modern Surgery. Eur. J. Dent. 2019, 13, 280–286. [Google Scholar] [CrossRef]
- Sánchez, M.; Mercader Ruiz, J.; Marijuán Pinel, D.; Sánchez, P.; Fiz, N.; Guadilla, J.; Azofra, J.; Beitia, M.; Delgado, D. Increasing the concentration of plasma molecules improves the biological activity of platelet-rich plasma for tissue regeneration. Sci. Rep. 2025, 15, 4523. [Google Scholar] [CrossRef]
- Kon, E.; Di Matteo, B.; Delgado, D.; Cole, B.J.; Dorotei, A.; Dragoo, J.L.; Filardo, G.; Fortier, L.A.; Giuffrida, A.; Jo, C.H.; et al. Platelet-rich plasma for the treatment of knee osteoarthritis: An expert opinion and proposal for a novel classification and coding system. Expert Opin. Biol. Ther. 2020, 20, 1447–1460. [Google Scholar] [CrossRef]
- Santos, R.G.D.; Santos, G.S.; Alkass, N.; Chiesa, T.L.; Azzini, G.O.; da Fonseca, L.F.; Santos, A.F.D.; Rodrigues, B.L.; Mosaner, T.; Lana, J.F. The regenerative mechanisms of platelet-rich plasma: A review. Cytokine 2021, 144, 155560. [Google Scholar] [CrossRef] [PubMed]
- Masuki, H.; Okudera, T.; Watanebe, T.; Suzuki, M.; Nishiyama, K.; Okudera, H.; Nakata, K.; Uematsu, K.; Su, C.-Y.; Kawase, T. Growth factor and pro-inflammatory cytokine contents in platelet-rich plasma (PRP), plasma rich in growth factors (PRGF), advanced platelet-rich fibrin (A-PRF), and concentrated growth factors (CGF). Int. J. Implant. Dent. 2016, 2, 19. [Google Scholar] [CrossRef]
- Li, S.; Dan, X.; Chen, H.; Li, T.; Liu, B.; Ju, Y.; Li, Y.; Lei, L.; Fan, X. Developing fibrin-based biomaterials/scaffolds in tissue engineering. Bioact. Mater. 2024, 40, 597–623. [Google Scholar] [CrossRef]
- Mercader Ruiz, J.; Beitia, M.; Delgado, D.; Sánchez, P.; Arnaiz, M.J.; López de Dicastillo, L.; Benito-Lopez, F.; Basabe-Desmonts, L.; Sánchez, M. New Formulation of Platelet-Rich Plasma Enriched in Platelet and Extraplatelet Biomolecules Using Hydrogels. Int. J. Mol. Sci. 2023, 24, 13811. [Google Scholar] [CrossRef]
- Dempfle, C.-E.; Kälsch, T.; Elmas, E.; Suvajac, N.; Lücke, T.; Münch, E.; Borggrefe, M. Impact of fibrinogen concentration in severely ill patients on mechanical properties of whole blood clots. Blood Coagul. Fibrinolysis 2008, 19, 765–770. [Google Scholar] [CrossRef]
- Delgado, D.; Beitia, M.; Mercader Ruiz, J.; Sánchez, P.; Montoya-Alzola, M.; Fiz, N.; Sánchez, M. A Novel Fibrin Matrix Derived from Platelet-Rich Plasma: Protocol and Characterization. Int. J. Mol. Sci. 2024, 25, 4069. [Google Scholar] [CrossRef] [PubMed]
- Swieringa, F.; Spronk, H.M.H.; Heemskerk, J.W.M.; van der Meijden, P.E.J. Integrating platelet and coagulation activation in fibrin clot formation. Res. Pract. Thromb. Haemost. 2018, 2, 450–460. [Google Scholar] [CrossRef]
- Chapin, J.C.; Hajjar, K.A. Fibrinolysis and the control of blood coagulation. Blood Rev. 2015, 29, 17–24. [Google Scholar] [CrossRef]
- Hoover-Plow, J. Does plasmin have anticoagulant activity? Vasc. Health Risk Manag. 2010, 6, 199–205. [Google Scholar] [CrossRef]
- Windberger, U.; Dibiasi, C.; Lotz, E.M.; Scharbert, G.; Reinbacher-Koestinger, A.; Ivanov, I.; Ploszczanski, L.; Antonova, N.; Lichtenegger, H. The effect of hematocrit, fibrinogen concentration and temperature on the kinetics of clot formation of whole blood. Clin. Hemorheol. Microcirc. 2020, 75, 431–445. [Google Scholar] [CrossRef] [PubMed]
- Youngwon, N.; Kim, J.-E.; Lim, H.S.; Han, K.-S.; Kim, H.K. Coagulation Proteins Influencing Global Coagulation Assays in Cirrhosis: Hypercoagulability in Cirrhosis Assessed by Thrombomodulin-Induced Thrombin Generation Assay. Biomed. Res. Int. 2013, 2013, 856754. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Bidarian, S.J.; Sim, M.; Song, X.; Wood, J.P. Protein S Coordinates the Inhibition of Prothrombinase By Tfpiα and Activated Protein C. Blood 2019, 134, 2386. [Google Scholar] [CrossRef]
- Dahlbäck, B. Protein S and C4b-binding protein: Components involved in the regulation of the protein C anticoagulant system. Thromb. Haemost. 1991, 66, 49–61. [Google Scholar] [CrossRef]
- Esmon, C.T. The roles of protein C and thrombomodulin in the regulation of blood coagulation. J. Biol. Chem. 1989, 264, 4743–4746. [Google Scholar] [CrossRef]
- Amiral, J.; Seghatchian, J. Revisiting the activated protein C-protein S-thrombomodulin ternary pathway: Impact of new understanding on its laboratory investigation. Transfus. Apher. Sci. 2019, 58, 538–544. [Google Scholar] [CrossRef]
- Chiu, C.L.; Hecht, V.; Duong, H.; Wu, B.; Tawil, B. Permeability of Three-Dimensional Fibrin Constructs Corresponds to Fibrinogen and Thrombin Concentrations. BioRes. Open Access 2012, 1, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Risman, R.A.; Belcher, H.A.; Ramanujam, R.K.; Weisel, J.W.; Hudson, N.E.; Tutwiler, V. Comprehensive Analysis of the Role of Fibrinogen and Thrombin in Clot Formation and Structure for Plasma and Purified Fibrinogen. Biomolecules 2024, 14, 230. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Zhong, W.; Li, J.; Luo, J. Mechanical Properties and Cushioning Effectiveness of FPUF-EPS Combination Materials. Materials 2023, 16, 6886. [Google Scholar] [CrossRef] [PubMed]
- Bayer, I.S. Advances in Fibrin-Based Materials in Wound Repair: A Review. Molecules 2022, 27, 4504. [Google Scholar] [CrossRef]
- Nandi, S.; Sommerville, L.; Nellenbach, K.; Mihalko, E.; Erb, M.; Freytes, D.O.; Hoffman, M.; Monroe, D.; Brown, A.C. Platelet-like particles improve fibrin network properties in a hemophilic model of provisional matrix structural defects. J. Colloid. Interface Sci. 2020, 577, 406–418. [Google Scholar] [CrossRef]
- Huang, J.; Li, X.; Shi, X.; Zhu, M.; Wang, J.; Huang, S.; Huang, X.; Wang, H.; Li, L.; Deng, H.; et al. Platelet integrin αIIbβ3: Signal transduction, regulation, and its therapeutic targeting. J. Hematol. Oncol. 2019, 12, 26. [Google Scholar] [CrossRef]
- Osdoit, S.; Rosa, J.-P. Fibrin Clot Retraction by Human Platelets Correlates with αIIbβ3Integrin-dependent Protein Tyrosine Dephosphorylation. J. Biol. Chem. 2001, 276, 6703–6710. [Google Scholar] [CrossRef]
- Montero, A.; Quílez, C.; Valencia, L.; Girón, P.; Jorcano, J.L.; Velasco, D. Effect of Fibrin Concentration on the In Vitro Production of Dermo-Epidermal Equivalents. Int. J. Mol. Sci. 2021, 22, 6746. [Google Scholar] [CrossRef]
- Dietrich, F.; Duré, G.L.; Klein, C.P.; Bampi, V.F.; Padoin, A.V.; Silva, V.D.; Braga-Silva, J. Platelet-Rich Fibrin Promotes an Accelerated Healing of Achilles Tendon When Compared to Platelet-Rich Plasma in Rat. World J. Plast. Surg. 2015, 4, 101–109. [Google Scholar]
- Narayanaswamy, R.; Patro, B.P.; Jeyaraman, N.; Gangadaran, P.; Rajendran, R.L.; Nallakumarasamy, A.; Jeyaraman, M.; Ramani, P.; Ahn, B.-C. Evolution and Clinical Advances of Platelet-Rich Fibrin in Musculoskeletal Regeneration. Bioengineering 2023, 10, 58. [Google Scholar] [CrossRef] [PubMed]
- Pereira, V.B.S.; Lago, C.A.P.; Almeida, R.d.A.C.; Barbirato, D.d.S.; Vasconcelos, B.C.d.E. Biological and Cellular Properties of Advanced Platelet-Rich Fibrin (A-PRF) Compared to Other Platelet Concentrates: Systematic Review and Meta-Analysis. Int. J. Mol. Sci. 2023, 25, 482. [Google Scholar] [CrossRef]
- Martino, M.M.; Briquez, P.S.; Ranga, A.; Lutolf, M.P.; Hubbell, J.A. Heparin-binding domain of fibrin(ogen) binds growth factors and promotes tissue repair when incorporated within a synthetic matrix. Proc. Natl. Acad. Sci. USA 2013, 110, 4563–4568. [Google Scholar] [CrossRef]
- Anitua, E.; Zalduendo, M.M.; Prado, R.; Alkhraisat, M.H.; Orive, G. Morphogen and proinflammatory cytokine release kinetics from PRGF-Endoret fibrin scaffolds: Evaluation of the effect of leukocyte inclusion. J. Biomed. Mater. Res. A 2015, 103, 1011–1020. [Google Scholar] [CrossRef]
- Shao, Z.; Lyu, C.; Teng, L.; Xie, X.; Sun, J.; Zou, D.; Lu, J. An Injectable Fibrin Scaffold Rich in Growth Factors for Skin Repair. Biomed. Res. Int. 2021, 2021, 8094932. [Google Scholar] [CrossRef] [PubMed]
- Willerth, S.M.; Rader, A.; Sakiyama-Elbert, S.E. The Effect of Controlled Growth Factor Delivery on Embryonic Stem Cell Differentiation Inside of Fibrin Scaffolds. Stem Cell Res. 2008, 1, 205–218. [Google Scholar] [CrossRef] [PubMed]
- Sakiyama-Elbert, S.E.; Hubbell, J.A. Development of fibrin derivatives for controlled release of heparin-binding growth factors. J. Control. Release 2000, 65, 389–402. [Google Scholar] [CrossRef]
- Fujioka-Kobayashi, M.; Miron, R.J.; Hernandez, M.; Kandalam, U.; Zhang, Y.; Choukroun, J. Optimized Platelet-Rich Fibrin With the Low-Speed Concept: Growth Factor Release, Biocompatibility, and Cellular Response. J. Periodontol. 2017, 88, 112–121. [Google Scholar] [CrossRef] [PubMed]
- Mittermayr, R.; Slezak, P.; Haffner, N.; Smolen, D.; Hartinger, J.; Hofmann, A.; Schense, J.; Spazierer, D.; Gampfer, J.; Goppelt, A.; et al. Controlled release of fibrin matrix-conjugated platelet derived growth factor improves ischemic tissue regeneration by functional angiogenesis. Acta Biomater. 2016, 29, 11–20. [Google Scholar] [CrossRef]
- El Bagdadi, K.; Kubesch, A.; Yu, X.; Al-Maawi, S.; Orlowska, A.; Dias, A.; Booms, P.; Dohle, E.; Sader, R.; Kirkpatrick, C.J.; et al. Reduction of relative centrifugal forces increases growth factor release within solid platelet-rich-fibrin (PRF)-based matrices: A proof of concept of LSCC (low speed centrifugation concept). Eur. J. Trauma Emerg. Surg. 2019, 45, 467–479. [Google Scholar] [CrossRef]
- Jimi, S.; Jaguparov, A.; Nurkesh, A.; Sultankulov, B.; Saparov, A. Sequential Delivery of Cryogel Released Growth Factors and Cytokines Accelerates Wound Healing and Improves Tissue Regeneration. Front. Bioeng. Biotechnol. 2020, 8, 345. [Google Scholar] [CrossRef] [PubMed]
- Hong, M.-H.; Hong, H.J.; Pang, H.; Lee, H.-J.; Yi, S.; Koh, W.-G. Controlled Release of Growth Factors from Multilayered Fibrous Scaffold for Functional Recoveries in Crushed Sciatic Nerve. ACS Biomater. Sci. Eng. 2018, 4, 576–586. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Guo, X.; Xiu, W.; Liu, Y.; Ren, L.; Xiao, H.; Yang, F.; Gao, Y.; Xu, C.; Wang, L. Accelerating thrombolysis using a precision and clot-penetrating drug delivery strategy by nanoparticle-shelled microbubbles. Sci. Adv. 2020, 6, eaaz8204. [Google Scholar] [CrossRef]
- Hotaling, N.A.; Bharti, K.; Kriel, H.; Simon, C.G. DiameterJ: A validated open source nanofiber diameter measurement tool. Biomaterials 2015, 61, 327–338. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| sPRP | BPCP | |
|---|---|---|
| 1. PRP Preparation | ||
| Initial blood volume | 9 mL per tube | 9 mL per tube |
| Anticoagulant | Sodium citrate 3.8% (wt V−1) | Sodium citrate 3.8% (wt V−1) |
| System | Closed | Open |
| Centrifugation | Yes | Yes |
| Number | 1 | 1 |
| Speed | 580× g—8 min | 1200× g—8 min |
| Water absorption | No | Yes |
| Method | --- | HEAA hydrogel |
| Hydrogel concentration | --- | 0.125 g mL−1 |
| Contact time | --- | 5 min |
| Final PRP volume | 2 mL per tube | 2 mL per subject |
| 2. PRP Characteristics | ||
| PRP Type | 13-00-11 [27] | 13-00-11 [27] |
| Platelets | 335.76 × 103 µL−1 ± 111.32 | 342.94 × 103 µL−1 ± 117 |
| Fibrinogen | 364.57 mg dL−1 ± 32.56 | 718.71 mg dL−1 ± 55.95 |
| Red Blood Cells | <0.01 × 106 µL−1 | <0.01 × 106 µL−1 |
| White Blood Cells | <0.05 × 106 µL−1 | <0.05 × 106 µL−1 |
| Neutrophils | --- | --- |
| Lymphocytes | --- | --- |
| Monocytes | --- | --- |
| Eosinophils | --- | --- |
| Basophils | --- | --- |
| Activation | CaCl2 (10% wt vol−1) | CaCl2 (10% wt vol−1) |
| 3. Application Characteristics | ||
| Dose | 10% | 10% |
| Direct/Indirect | Direct | Direct |
| 4. Other remarkable PRP and study features | ||
| The product used for the study was the fibrin clot obtained following the activation of PRP with calcium chloride (10%). | ||
| sPRP | BPCP | p Value | ||
|---|---|---|---|---|
| Rheological properties | Elastic modulus (G′) (kPa) | 422.41 ± 280.05 | 588.89 ± 383.9 | 0.3722 |
| Viscous modulus (G″) (kPa) | 99.31 ± 69.07 | 131.76 ± 95.32 | 0.4797 | |
| Tanδ | 0.25 ± 0.08 | 0.21 ± 0.06 | 0.5350 |
| P1 | P2 | P3 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| sPRP | BPCP | p Value | sPRP | BPCP | p Value | sPRP | BPCP | p Value | |
| T0 | |||||||||
| TGF-β1 | 1357 ± 47.68 | 2048 ± 75.64 | 0.008 ** | 1543 ± 26.61 | 3302 ± 33.17 | 0.0003 *** | 3724 ± 20.71 | 4060 ± 8.98 | 0.002 ** |
| PDGF-AB | 371 ± 3.99 | 592 ± 12.25 | 0.002 ** | 438 ± 2.24 | 964 ± 28.66 | 0.0015 ** | 1139 ± 52.52 | 1132 ± 27.61 | 0.88 |
| VEGF | 6.5 ± 0.21 | 15 ± 1.57 | 0.016 * | 16 ± 0.87 | 38 ± 1.78 | 0.004 ** | 18 ± 1.30 | 21 ± 0.00 | 0.11 |
| IGF-1 | 5 ± 0.10 | 16 ± 0.41 | 0.0007 *** | 6 ± 0.10 | 28 ± 0.01 | <0.0001 **** | 8 ± 0.08 | 17 ± 0.05 | <0.0001 **** |
| HGF | 12.5 ± 0.00 | 52 ± 6.24 | 0.12 | 10 ± 1.89 | 55 ± 0.12 | 0.0009 *** | 32 ± 3.06 | 86.5 ± 4.07 | 0.004 ** |
| T1 (24 h) | |||||||||
| TGF-β1 | 2480 ± 68.84 | 3902 ± 39.76 | 0.0015 ** | 2877 ± 52.15 | 5645 ± 166.10 | 0.002 ** | 4057 ± 33.96 | 4973 ± 55.49 | 0.003 ** |
| PDGF-AB | 620 ± 22.04 | 1189 ± 2.80 | 0.0008 *** | 669 ± 0.73 | 1874 ± 24.59 | 0.0002 *** | 1347 ± 6.89 | 2313 ± 71.58 | 0.003 ** |
| VEGF | 17 ± 0.33 | 37 ± 0.29 | 0.0002 *** | 37 ± 0.24 | 81 ± 3.19 | 0.003 ** | 50 ± 0.43 | 60 ± 1.00 | 0.006 ** |
| IGF-1 | 7 ± 0.14 | 26 ± 0.02 | <0.0001 **** | 6.5 ± 0.24 | 45 ± 1.16 | 0.0005 *** | 7 ± 0.46 | 23 ± 0.15 | 0.0004 *** |
| HGF | 21 ± 2.48 | 105 ± 11.98 | 0.0104 * | 7 ± 0.48 | 101 ± 15.17 | 0.013 * | 39 ± 3.33 | 252 ± 14.94 | 0.003 ** |
| T3 (72 h) | |||||||||
| TGF-β1 | 593 ± 23.13 | 2157 ± 87.37 | 0.002 ** | 773 ± 30.58 | 1890 ± 16.69 | 0.0005 *** | 1761 ± 0.36 | 3306 ± 137.54 | 0.004 ** |
| PDGF-AB | 149 ± 0.15 | 515 ± 46.15 | 0.009 ** | 189 ± 12.83 | 516 ± 9.56 | 0.0012 ** | 439 ± 6.76 | 872 ± 13.92 | 0.0006 *** |
| VEGF | 0.5 ± 0.32 | 14 ± 0.16 | 0.0003 *** | 10 ± 0.19 | 19 ± 0.24 | 0.0005 *** | 19 ± 0.52 | 15 ± 1.48 | 0.051 |
| IGF-1 | 0.8 ± 0.00 | 10.5 ± 0.42 | 0.0009 *** | 1 ± 0.04 | 10 ± 0.00 | <0.0001 **** | 1 ± 0.01 | 9 ± 0.11 | 0.0001 *** |
| HGF | 9 ± 12.27 | 34 ± 0.80 | 0.102 * | 4 ± 0.00 | 15 ± 4.45 | 0.31 | 6 ± 8.30 | 48 ± 2.34 | 0.02 * |
| T6 (144 h) | |||||||||
| TGF-β1 | 333 ± 8.33 | 902 ± 40.19 | 0.003 ** | 705 ± 15.10 | 1232 ± 37.91 | 0.003 ** | 943 ± 9.84 | 2748 ± 123.57 | 0.002 ** |
| PDGF-AB | 66 ± 1.47 | 208 ± 1.59 | 0.00012 *** | 119 ± 1.60 | 256 ± 10.13 | 0.003 ** | 247 ± 5.03 | 639 ± 7.34 | 0.0002 *** |
| VEGF | 0 ± 0.00 | 1 ± 0.40 | 0.037 * | 3 ± 0.16 | 6 ± 0.00 | 0.001 ** | 8 ± 4.38 | 7 ± 0.38 | 0.78 |
| IGF-1 | 0.5 ± 0.00 | 2 ± 0.04 | 0.0004 *** | 0.5 ± 0.00 | 3 ± 0.02 | <0.0001 **** | 0.6 ± 0.03 | 3 ± 0.02 | 0.00012 *** |
| HGF | 0.2± 0.12 | 8.5 ± 2.04 | 0.029 | 2 ± 1.01 | 5 ± 0.73 | 0.12 | 0 ± 0.00 | 18.5 ± 6.34 | 0.053 |
| T10 (240 h) | |||||||||
| TGF-β1 | 586 ± 5.70 | 820 ± 10.72 | 0.0013 ** | 462 ± 23.21 | 1654 ± 26.53 | 0.0004 *** | 724 ± 1.49 | 1900 ± 16.31 | <0.0001 **** |
| PDGF-AB | 48 ± 1.35 | 103 ± 4.04 | 0.003 ** | 82 ± 4.61 | 163 ± 2.88 | 0.002 ** | 106 ± 0.63 | 345 ± 3.22 | <0.0001 **** |
| VEGF | 0.3 ± 0.31 | 0 ± 0.00 | 0.26 | 0 ± 0.00 | 4 ± 0.30 | 0.003 ** | 1 ± 0.62 | 4 ± 0.81 | 0.09 |
| IGF-1 | 0.5 ± 0.00 | 0.5 ± 0.01 | 0.063 | 0.5 ± 0.01 | 0.3 ± 0.02 | 0.005 ** | 0.6 ± 0.02 | 0.7 ± 0.04 | 0.24 |
| HGF | 2 ± 0.97 | 4 ± 0.00 | 0.29 | 1 ± 0.37 | 0 ± 0.00 | 0.11 | 7 ± 5.00 | 10 ± 0.00 | 0.42 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marijuán-Pinel, D.; Mercader-Ruiz, J.; Beitia, M.; Sánchez, P.; López de Dicastillo, L.; Gonzalez, S.; Espregueira-Mendes, J.; Aizpurua, B.; Oraá, J.; Delgado, D.; et al. Exploring the Impact of Extraplatelet Content on Fibrin-Based Scaffold Performance for Regenerative Therapies. Int. J. Mol. Sci. 2025, 26, 5967. https://doi.org/10.3390/ijms26135967
Marijuán-Pinel D, Mercader-Ruiz J, Beitia M, Sánchez P, López de Dicastillo L, Gonzalez S, Espregueira-Mendes J, Aizpurua B, Oraá J, Delgado D, et al. Exploring the Impact of Extraplatelet Content on Fibrin-Based Scaffold Performance for Regenerative Therapies. International Journal of Molecular Sciences. 2025; 26(13):5967. https://doi.org/10.3390/ijms26135967
Chicago/Turabian StyleMarijuán-Pinel, Daniel, Jon Mercader-Ruiz, Maider Beitia, Pello Sánchez, Leonor López de Dicastillo, Sergio Gonzalez, João Espregueira-Mendes, Beatriz Aizpurua, Jaime Oraá, Diego Delgado, and et al. 2025. "Exploring the Impact of Extraplatelet Content on Fibrin-Based Scaffold Performance for Regenerative Therapies" International Journal of Molecular Sciences 26, no. 13: 5967. https://doi.org/10.3390/ijms26135967
APA StyleMarijuán-Pinel, D., Mercader-Ruiz, J., Beitia, M., Sánchez, P., López de Dicastillo, L., Gonzalez, S., Espregueira-Mendes, J., Aizpurua, B., Oraá, J., Delgado, D., & Sánchez, M. (2025). Exploring the Impact of Extraplatelet Content on Fibrin-Based Scaffold Performance for Regenerative Therapies. International Journal of Molecular Sciences, 26(13), 5967. https://doi.org/10.3390/ijms26135967