
Personalized High-Resolution Genetic Diagnostics of Prostate Adenocarcinoma Guided by Multiparametric Magnetic Resonance Imaging: Results of a Pilot Study
 , ,
, ,
Abstract
1. Introduction
2. Results
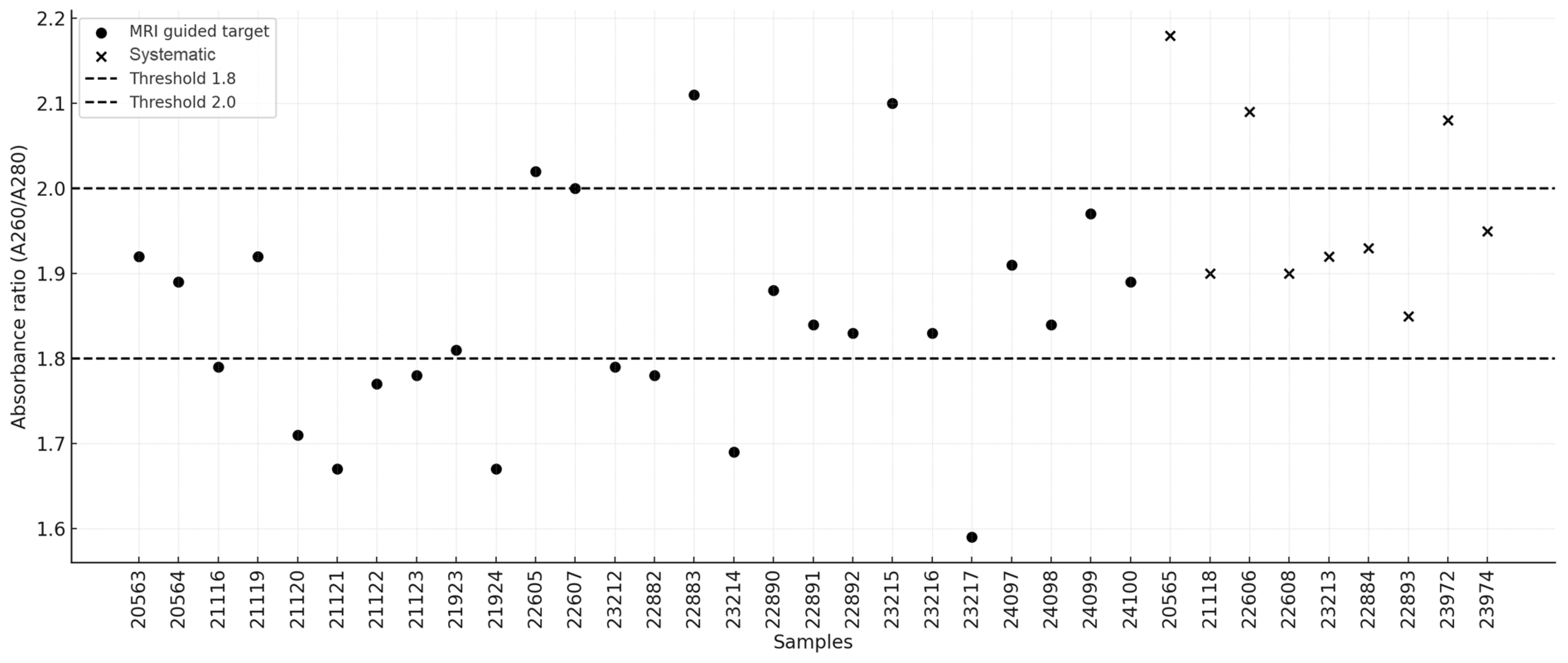
2.1. DNA Quality and Quantitative Metrics
2.2. Patient Clinical Characteristics
2.2.1. Patient 1
2.2.2. Patient 2
2.2.3. Patient 3
2.2.4. Patient 4
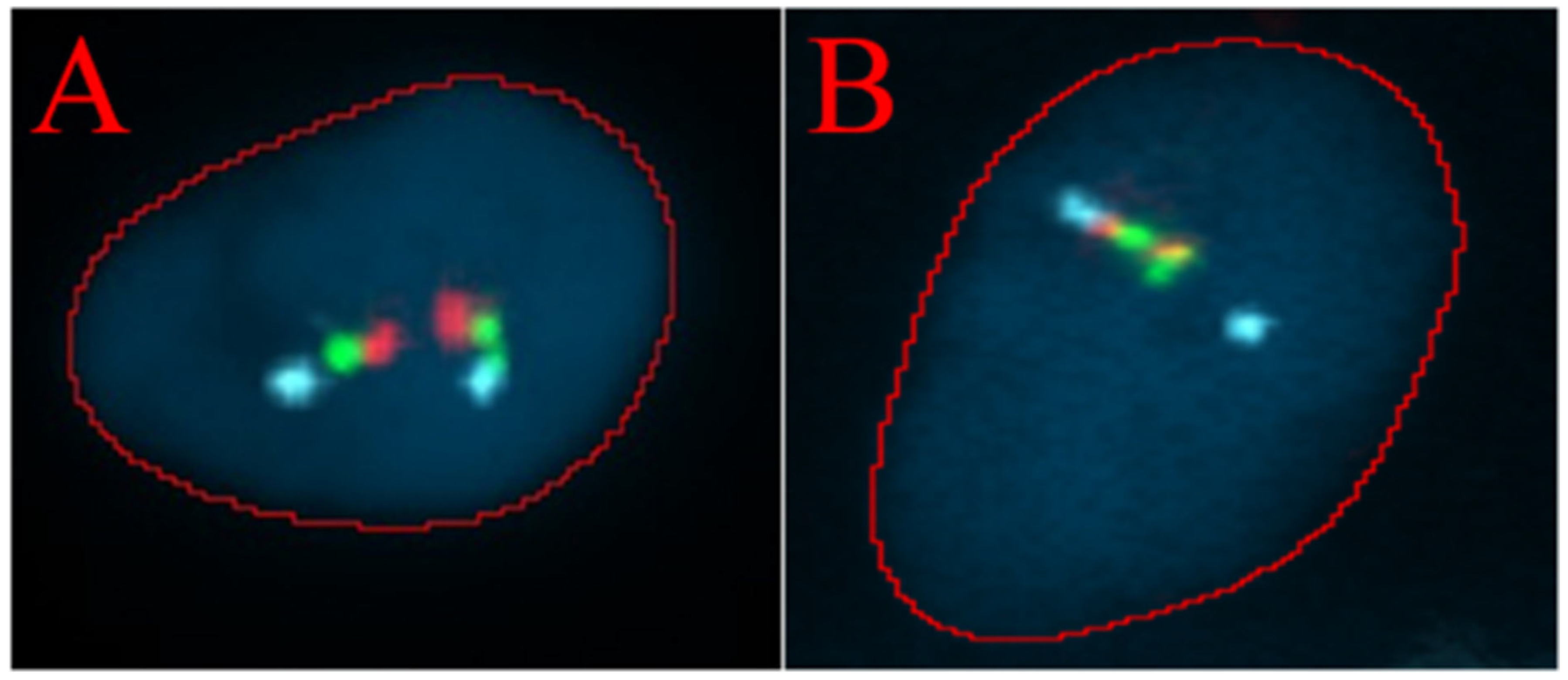
2.3. TMPRSS2/ERG Fusion Evaluation
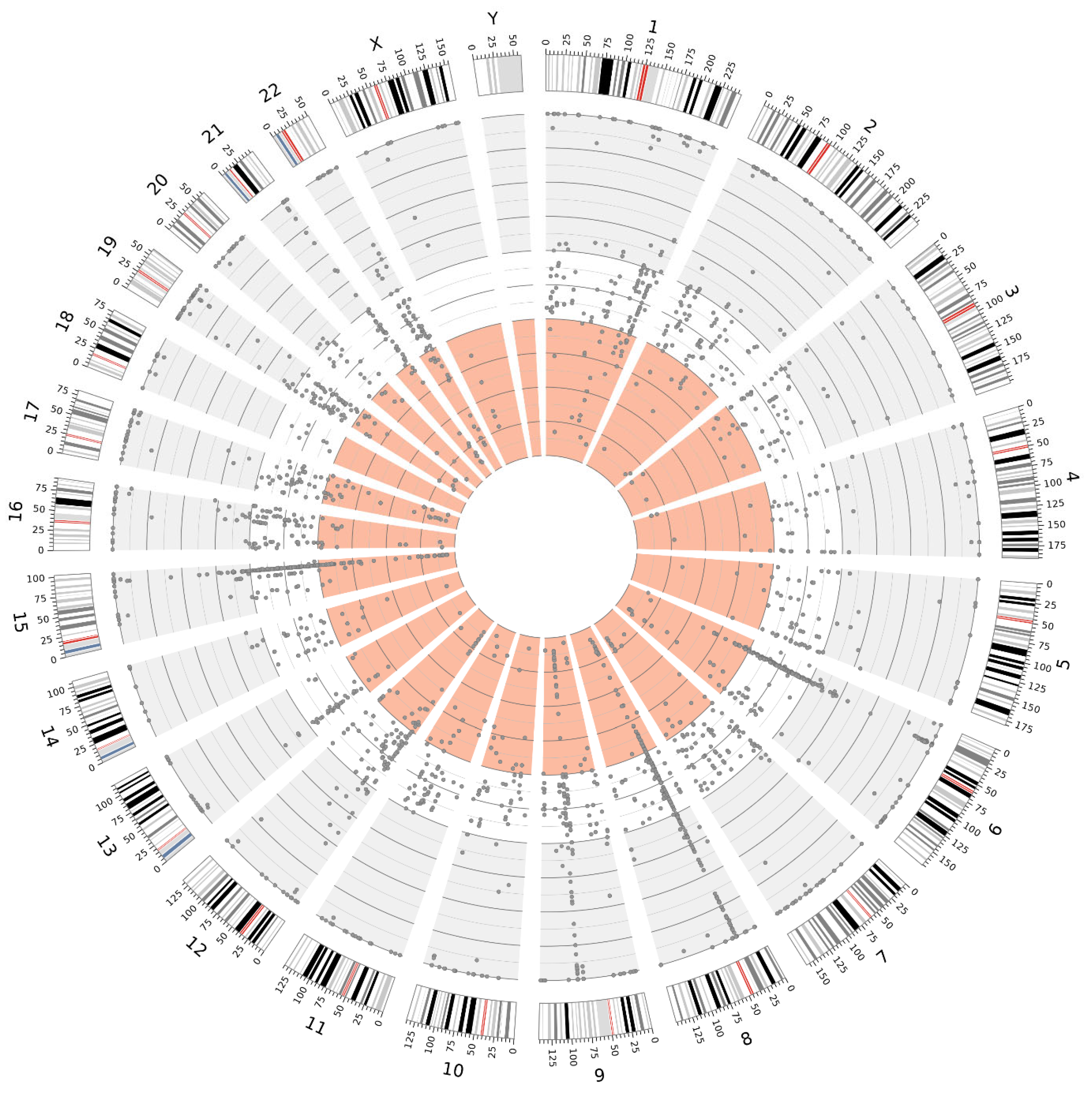
2.4. NGS Results
2.5. Clinical Follow-Up
3. Discussion
4. Materials and Methods
4.1. Material Acquisition
4.2. Fluorescence In Situ Hybridization
4.3. DNA Isolation
4.4. Next-Generation Sequencing
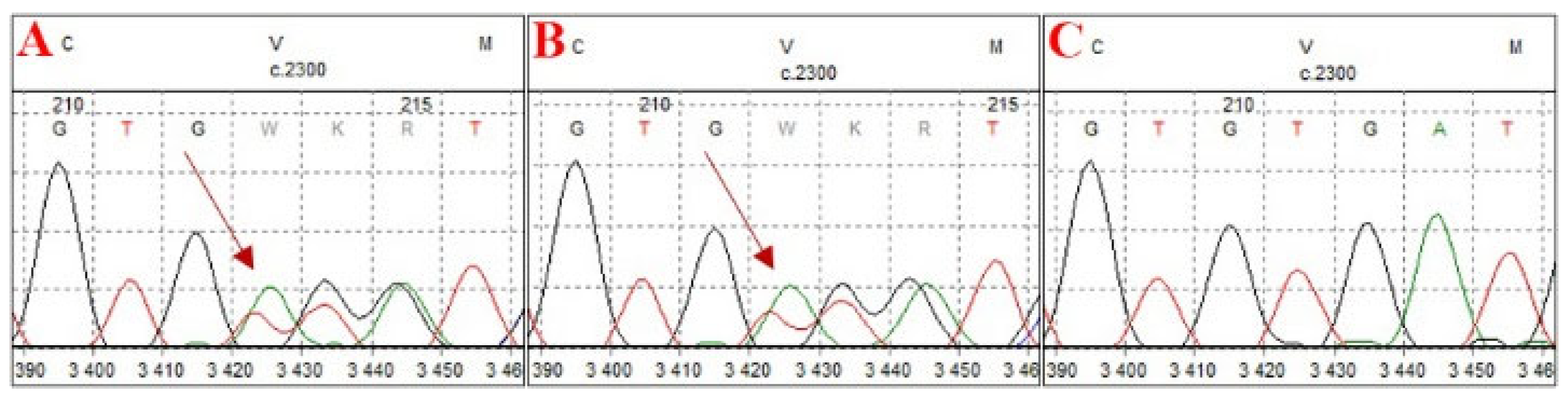
4.5. Sanger Sequencing
4.6. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
List of Abbreviations
| CGP | Comprehensive Genomic Profiling |
| CNV | Copy Number Variation |
| FISH | Fluorescence In Situ Hybridization |
| FFPE | Formalin-Fixed Paraffin-Embedded |
| HP | Histopathology |
| HRD | Homologous Recombination Deficiency |
| ICD-O | International Classification of Diseases for Oncology |
| IHC | Immunohistochemistry |
| LUTS | Lower Urinary Tract Symptoms |
| MRI | Magnetic Resonance Imaging |
| mCRPC | Metastatic Castration-Resistant Prostate Cancer |
| NGS | Next-Generation Sequencing |
| PARP | Poly(ADP-ribose) Polymerase |
| PC | Prostate Cancer |
| PI-RADS | Prostate Imaging Reporting and Data System |
| PSA | Prostate-Specific Antigen |
| PSAD | Prostate-Specific Antigen Density |
| SNV | Single Nucleotide Variant |
| SV | Structural Variant |
| TMB | Tumor Mutational Burden |
| TRUS | Transrectal Ultrasound |
| US | Ultrasound |
| VAF | Variant Allele Frequency |
References
- Didkowska, J.; Barańska, K.; Miklewska, M.J.; Wojciechowska, U. Cancer Incidence and Mortality in Poland in 2023. Nowotw. J. Oncol. 2024, 74, 75–93. [Google Scholar] [CrossRef]
- Owczarek, A.J. Drzewa klasyfikacyjne w medycynie. Ann. Acad. Med. Siles. 2019, 68, 449–456. [Google Scholar]
- Garzotto, M.; Beer, T.M.; Hudson, R.G.; Peters, L.; Hsieh, Y.-C.; Barrera, E.; Klein, T.; Mori, M. Improved Detection of Prostate Cancer Using Classification and Regression Tree Analysis. J. Clin. Oncol. 2005, 23, 4322–4329. [Google Scholar] [CrossRef] [PubMed]
- Cornud, F.; Brolis, L.; Delongchamps, N.B.; Portalez, D.; Malavaud, B.; Renard-Penna, R.; Mozer, P. TRUS-MRI Image Registration: A Paradigm Shift in the Diagnosis of Significant Prostate Cancer. Abdom. Imaging 2013, 38, 1447–1463. [Google Scholar] [CrossRef]
- Logan, J.K.; Rais-Bahrami, S.; Turkbey, B.; Gomella, A.; Amalou, H.; Choyke, P.L.; Wood, B.J.; Pinto, P.A. Current Status of Magnetic Resonance Imaging (MRI) and Ultrasonography Fusion Software Platforms for Guidance of Prostate Biopsies. BJU Int. 2014, 114, 641–652. [Google Scholar] [CrossRef]
- Avolio, P.P.; Lughezzani, G.; Anidjar, M.; Hassan, T.; Rompré-Brodeur, A.; Buffi, N.M.; Lazzeri, M.; Sanchez-Salas, R. The Diagnostic Accuracy of Micro-Ultrasound for Prostate Cancer Diagnosis: A Review. World J. Urol. 2023, 41, 3267–3276. [Google Scholar] [CrossRef]
- Masarwa, I.; Bahouth, Z.; Shefler, A.; Bejar, J.; Shprits, S.; Avitan, O.; Halachmi, S.; Nativ, O. The Value of the SmartBxTM System in Improving the Detection of Prostate Cancer in Patients Undergoing Transrectal Ultrasound-Guided Biopsy. JMCM 2020, 3, 33–36. [Google Scholar] [CrossRef]
- Mandel, P.; Wenzel, M.; Hoeh, B.; Welte, M.N.; Preisser, F.; Inam, T.; Wittler, C.; Humke, C.; Köllermann, J.; Wild, P.; et al. Immunohistochemistry for Prostate Biopsy—Impact on Histological Prostate Cancer Diagnoses and Clinical Decision Making. Curr. Oncol. 2021, 28, 2123–2133. [Google Scholar] [CrossRef]
- Murciano-Goroff, Y.R.; Drilon, A.; Stadler, Z.K. The NCI-MATCH: A National, Collaborative Precision Oncology Trial for Diverse Tumor Histologies. Cancer Cell 2021, 39, 22–24. [Google Scholar] [CrossRef]
- Meric-Bernstam, F.; Ford, J.M.; O’Dwyer, P.J.; Shapiro, G.I.; McShane, L.M.; Freidlin, B.; O’Cearbhaill, R.E.; George, S.; Glade-Bender, J.; Lyman, G.H.; et al. National Cancer Institute Combination Therapy Platform Trial with Molecular Analysis for Therapy Choice (ComboMATCH). Clin. Cancer Res. 2023, 29, 1412–1422. [Google Scholar] [CrossRef]
- Coombs, N.J.; Gough, A.C.; Primrose, J.N. Optimisation of DNA and RNA Extraction from Archival Formalin-Fixed Tissue. Nucleic Acids Res. 1999, 27, e12. [Google Scholar] [CrossRef]
- Schäfer, S.C.; Pfnür, M.; Yerly, S.; Fandel, T.M.; Jichlinski, P.; Lehr, H.-A. Cryopreservation of Prostate Cancer Tissue during Routine Processing of Fresh Unfixed Prostatectomy Specimen: Demonstration and Validation of a New Technique. Prostate 2009, 69, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Hedegaard, J.; Thorsen, K.; Lund, M.K.; Hein, A.-M.K.; Hamilton-Dutoit, S.J.; Vang, S.; Nordentoft, I.; Birkenkamp-Demtröder, K.; Kruhøffer, M.; Hager, H.; et al. Next-Generation Sequencing of RNA and DNA Isolated from Paired Fresh-Frozen and Formalin-Fixed Paraffin-Embedded Samples of Human Cancer and Normal Tissue. PLoS ONE 2014, 9, e98187. [Google Scholar] [CrossRef]
- Schweiger, M.R.; Kerick, M.; Timmermann, B.; Albrecht, M.W.; Borodina, T.; Parkhomchuk, D.; Zatloukal, K.; Lehrach, H. Genome-Wide Massively Parallel Sequencing of Formaldehyde Fixed-Paraffin Embedded (FFPE) Tumor Tissues for Copy-Number- and Mutation-Analysis. PLoS ONE 2009, 4, e5548. [Google Scholar] [CrossRef]
- Spencer, D.H.; Sehn, J.K.; Abel, H.J.; Watson, M.A.; Pfeifer, J.D.; Duncavage, E.J. Comparison of Clinical Targeted Next-Generation Sequence Data from Formalin-Fixed and Fresh-Frozen Tissue Specimens. J. Mol. Diagn. 2013, 15, 623–633. [Google Scholar] [CrossRef]
- Adiconis, X.; Borges-Rivera, D.; Satija, R.; DeLuca, D.S.; Busby, M.A.; Berlin, A.M.; Sivachenko, A.; Thompson, D.A.; Wysoker, A.; Fennell, T.; et al. Comparative Analysis of RNA Sequencing Methods for Degraded or Low-Input Samples. Nat. Methods 2013, 10, 623–629. [Google Scholar] [CrossRef]
- Morlan, J.D.; Qu, K.; Sinicropi, D.V. Selective Depletion of rRNA Enables Whole Transcriptome Profiling of Archival Fixed Tissue. PLoS ONE 2012, 7, e42882. [Google Scholar] [CrossRef]
- Norton, N.; Sun, Z.; Asmann, Y.W.; Serie, D.J.; Necela, B.M.; Bhagwate, A.; Jen, J.; Eckloff, B.W.; Kalari, K.R.; Thompson, K.J.; et al. Gene Expression, Single Nucleotide Variant and Fusion Transcript Discovery in Archival Material from Breast Tumors. PLoS ONE 2013, 8, e81925. [Google Scholar] [CrossRef]
- Högnäs, G.; Kivinummi, K.; Kallio, H.M.L.; Hieta, R.; Ruusuvuori, P.; Koskenalho, A.; Kesseli, J.; Tammela, T.L.J.; Riikonen, J.; Ilvesaro, J.; et al. Feasibility of Prostate PAXgene Fixation for Molecular Research and Diagnostic Surgical Pathology: Comparison of Matched Fresh Frozen, FFPE, and PFPE Tissues. Am. J. Surg. Pathol. 2018, 42, 103–115. [Google Scholar] [CrossRef]
- Menon, R.; Deng, M.; Boehm, D.; Braun, M.; Fend, F.; Boehm, D.; Biskup, S.; Perner, S. Exome Enrichment and SOLiD Sequencing of Formalin Fixed Paraffin Embedded (FFPE) Prostate Cancer Tissue. Int. J. Mol. Sci. 2012, 13, 8933–8942. [Google Scholar] [CrossRef]
- de Schaetzen van Brienen, L.; Larmuseau, M.; Van der Eecken, K.; De Ryck, F.; Robbe, P.; Schuh, A.; Fostier, J.; Ost, P.; Marchal, K. Comparative Analysis of Somatic Variant Calling on Matched FF and FFPE WGS Samples. BMC Med. Genom. 2020, 13, 94. [Google Scholar] [CrossRef] [PubMed]
- Jennings, L.J.; Arcila, M.E.; Corless, C.; Kamel-Reid, S.; Lubin, I.M.; Pfeifer, J.; Temple-Smolkin, R.L.; Voelkerding, K.V.; Nikiforova, M.N. Guidelines for Validation of Next-Generation Sequencing-Based Oncology Panels: A Joint Consensus Recommendation of the Association for Molecular Pathology and College of American Pathologists. J. Mol. Diagn. 2017, 19, 341–365. [Google Scholar] [CrossRef]
- Yao, Y.; Wang, H.; Li, B.; Tang, Y. Evaluation of the TMPRSS2:ERG Fusion for the Detection of Prostate Cancer: A Systematic Review and Meta-Analysis. Tumour Biol. 2014, 35, 2157–2166. [Google Scholar] [CrossRef] [PubMed]
- Sanguedolce, F.; Cormio, A.; Brunelli, M.; D’Amuri, A.; Carrieri, G.; Bufo, P.; Cormio, L. Urine TMPRSS2: ERG Fusion Transcript as a Biomarker for Prostate Cancer: Literature Review. Clin. Genitourin. Cancer 2016, 14, 117–121. [Google Scholar] [CrossRef] [PubMed]
- Delongchamps, N.B.; Peltier, A.; Potiron, E.; Bladou, F.; Anract, J.; Diamand, R.; Robert, G.; Messas, A.; Van Velthoven, R. Targeted Microwave Ablation of Localised Prostate Cancer: Initial Results of VIOLETTE Trial. BJUI Compass 2024, 5, 1307–1313. [Google Scholar] [CrossRef]
- Sondka, Z.; Bamford, S.; Cole, C.G.; Ward, S.A.; Dunham, I.; Forbes, S.A. The COSMIC Cancer Gene Census: Describing Genetic Dysfunction across All Human Cancers. Nat. Rev. Cancer 2018, 18, 696–705. [Google Scholar] [CrossRef]
- Jiang, H.; Lei, R.; Ding, S.-W.; Zhu, S. Skewer: A Fast and Accurate Adapter Trimmer for next-Generation Sequencing Paired-End Reads. BMC Bioinform. 2014, 15, 182. [Google Scholar] [CrossRef]
- Krzywinski, M.; Schein, J.; Birol, I.; Connors, J.; Gascoyne, R.; Horsman, D.; Jones, S.J.; Marra, M.A. Circos: An Information Aesthetic for Comparative Genomics. Genome Res. 2009, 19, 1639–1645. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n | Sample | Site | Concentration (ng/μL) | Absorbance Ratio (A260/A280) |
|---|---|---|---|---|
| 1 | 20563 | MRI-guided target | 25.9 | 1.92 |
| 2 | 20564 | MRI-guided target | 25.4 | 1.89 |
| 3 | 20565 | systematic | 12.9 | 2.18 |
| 4 | 21116 | MRI-guided target | 33.3 | 1.79 |
| 5 | 21118 | systematic | 49.6 | 1.9 |
| 6 | 21119 | MRI-guided target | 46.1 | 1.92 |
| 7 | 21120 | MRI-guided target | 31.2 | 1.71 |
| 8 | 21121 | MRI-guided target | 28.5 | 1.67 |
| 9 | 21122 | MRI-guided target | 43.8 | 1.77 |
| 10 | 21123 | MRI-guided target | 26.1 | 1.78 |
| 11 | 21923 | MRI-guided target | 10.5 | 1.81 |
| 12 | 21924 | MRI-guided target | 8.1 | 1.67 |
| 13 | 22605 | MRI-guided target | 26.4 | 2.02 |
| 14 | 22606 | systematic | 18.5 | 2.09 |
| 15 | 22607 | MRI-guided target | 26.4 | 2 |
| 16 | 22608 | systematic | 44.5 | 1.9 |
| 17 | 23212 | MRI-guided target | 22.5 | 1.79 |
| 18 | 22882 | MRI-guided target | 6.2 | 1.78 |
| 19 | 22883 | MRI-guided target | 25.4 | 2.11 |
| 20 | 23213 | systematic | 10.4 | 1.92 |
| 21 | 22884 | systematic | 10.4 | 1.93 |
| 22 | 23214 | MRI-guided target | 16.1 | 1.69 |
| 23 | 22890 | MRI-guided target | 29.1 | 1.88 |
| 24 | 22891 | MRI-guided target | 34.1 | 1.84 |
| 25 | 22892 | MRI-guided target | 44.2 | 1.83 |
| 26 | 22893 | systematic | 57.2 | 1.85 |
| 27 | 23215 | MRI-guided target | 19.2 | 2.1 |
| 28 | 23216 | MRI-guided target | 12.3 | 1.83 |
| 29 | 23217 | MRI-guided target | 5.8 | 1.59 |
| 30 | 24097 | MRI-guided target | 18.19 | 1.91 |
| 31 | 24098 | MRI-guided target | 25.24 | 1.84 |
| 32 | 23972 | systematic | 16.76 | 2.08 |
| 33 | 24099 | MRI-guided target | 14.93 | 1.97 |
| 34 | 24100 | MRI-guided target | 21.24 | 1.89 |
| 35 | 23974 | systematic | 46.88 | 1.95 |
| n | Sample | PI-RADS v2 | Concentration (ng/μL) | Absorbance Ratio (A260/A280) |
|---|---|---|---|---|
| 1 | 25484 | 4 | 12.8 | 1.55 |
| 2 | 25485 | 4 | 21.7 | 1.65 |
| 3 | 25486 | 3 | 17.2 | 1.67 |
| 4 | 25487 | 4 | 35.7 | 1.67 |
| Case | PI-RADS v2 | FISH Result | % of Cells with Fusion | HP |
|---|---|---|---|---|
| 1 | 4 | nuc ish (TMPRSS2,TMPRSS2,ERG)x2[50] | - | benign prostatic hyperplasia, focal glandular atrophy, and chronic inflammation |
| 2 | 4 | nuc ish (TMPRSS2,TMPRSS2,ERG)x2[50] | - | mild glandular atrophy, focal chronic inflammatory infiltration, and hyperplastic changes |
| 3 | 3 | nuc ish (TMPRSS2,ERG)x2(TMPRSS2/TMPRSS2 sep ERG)x1[32/50] | 64% | prostatic acinar adenocarcinoma |
| 4 | 4 | nuc ish (TMPRSS2,ERG)x2(TMPRSS2/TMPRSS2 sep ERG)x1[42/50] | 84% | prostatic acinar adenocarcinoma |
| n | Sample | Aligned Reads (on Target) | Proportion of Aligned Reads (in %) | Duplicate Rate (in %) | Average Coverage | Number of Small Variants |
|---|---|---|---|---|---|---|
| 1 | 22890 | 34.245 | 36.12 | 16.81 | 845.58 | 2636 |
| 2 | 23215 | 36.773 | 38.62 | 16.8 | 909.18 | 2609 |
| 3 | 24097 | 33.628 | 34.77 | 15.24 | 832.98 | 2577 |
| 4 | 24098 | 34.148 | 35.33 | 15.18 | 846.9 | 2585 |
| 5 | 24099 | 32.563 | 33.81 | 15.58 | 806.42 | 2546 |
| 6 | 24100 | 32.599 | 34.84 | 17.78 | 810.53 | 2535 |
| n | Sample | Aligned Reads (on Target) | Proportion of Aligned Reads (in %) | Duplicate Rate (in %) | Average Coverage | Number of Small Variants |
|---|---|---|---|---|---|---|
| 1 | 25486 | 2.723 | 6.08 | 49.63 | 60.68 | 2939 |
| 2 | 25487 | 3.175 | 5.88 | 49.11 | 72.6 | 2933 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wilkosz, J.; Sobieraj, D.W.; Kałużewski, T.; Kaczmarek, J.; Szwalski, J.; Bednarek, M.; Morel, A.; Kasprzyk, Ż.; Kępczyński, Ł.; Sałamunia, J.; et al. Personalized High-Resolution Genetic Diagnostics of Prostate Adenocarcinoma Guided by Multiparametric Magnetic Resonance Imaging: Results of a Pilot Study. Int. J. Mol. Sci. 2025, 26, 5648. https://doi.org/10.3390/ijms26125648
Wilkosz J, Sobieraj DW, Kałużewski T, Kaczmarek J, Szwalski J, Bednarek M, Morel A, Kasprzyk Ż, Kępczyński Ł, Sałamunia J, et al. Personalized High-Resolution Genetic Diagnostics of Prostate Adenocarcinoma Guided by Multiparametric Magnetic Resonance Imaging: Results of a Pilot Study. International Journal of Molecular Sciences. 2025; 26(12):5648. https://doi.org/10.3390/ijms26125648
Chicago/Turabian StyleWilkosz, Jacek, Dariusz Wojciech Sobieraj, Tadeusz Kałużewski, Jakub Kaczmarek, Jarosław Szwalski, Michał Bednarek, Agnieszka Morel, Żaneta Kasprzyk, Łukasz Kępczyński, Jordan Sałamunia, and et al. 2025. "Personalized High-Resolution Genetic Diagnostics of Prostate Adenocarcinoma Guided by Multiparametric Magnetic Resonance Imaging: Results of a Pilot Study" International Journal of Molecular Sciences 26, no. 12: 5648. https://doi.org/10.3390/ijms26125648
APA StyleWilkosz, J., Sobieraj, D. W., Kałużewski, T., Kaczmarek, J., Szwalski, J., Bednarek, M., Morel, A., Kasprzyk, Ż., Kępczyński, Ł., Sałamunia, J., Gach, A., & Kałużewski, B. (2025). Personalized High-Resolution Genetic Diagnostics of Prostate Adenocarcinoma Guided by Multiparametric Magnetic Resonance Imaging: Results of a Pilot Study. International Journal of Molecular Sciences, 26(12), 5648. https://doi.org/10.3390/ijms26125648