
Specific IgE and Basophil Activation Test by Microarray: A Promising Tool for Diagnosis of Platinum Compound Hypersensitivity Reactions


 , , ,
, , ,  and
and
Abstract
1. Introduction
2. Results
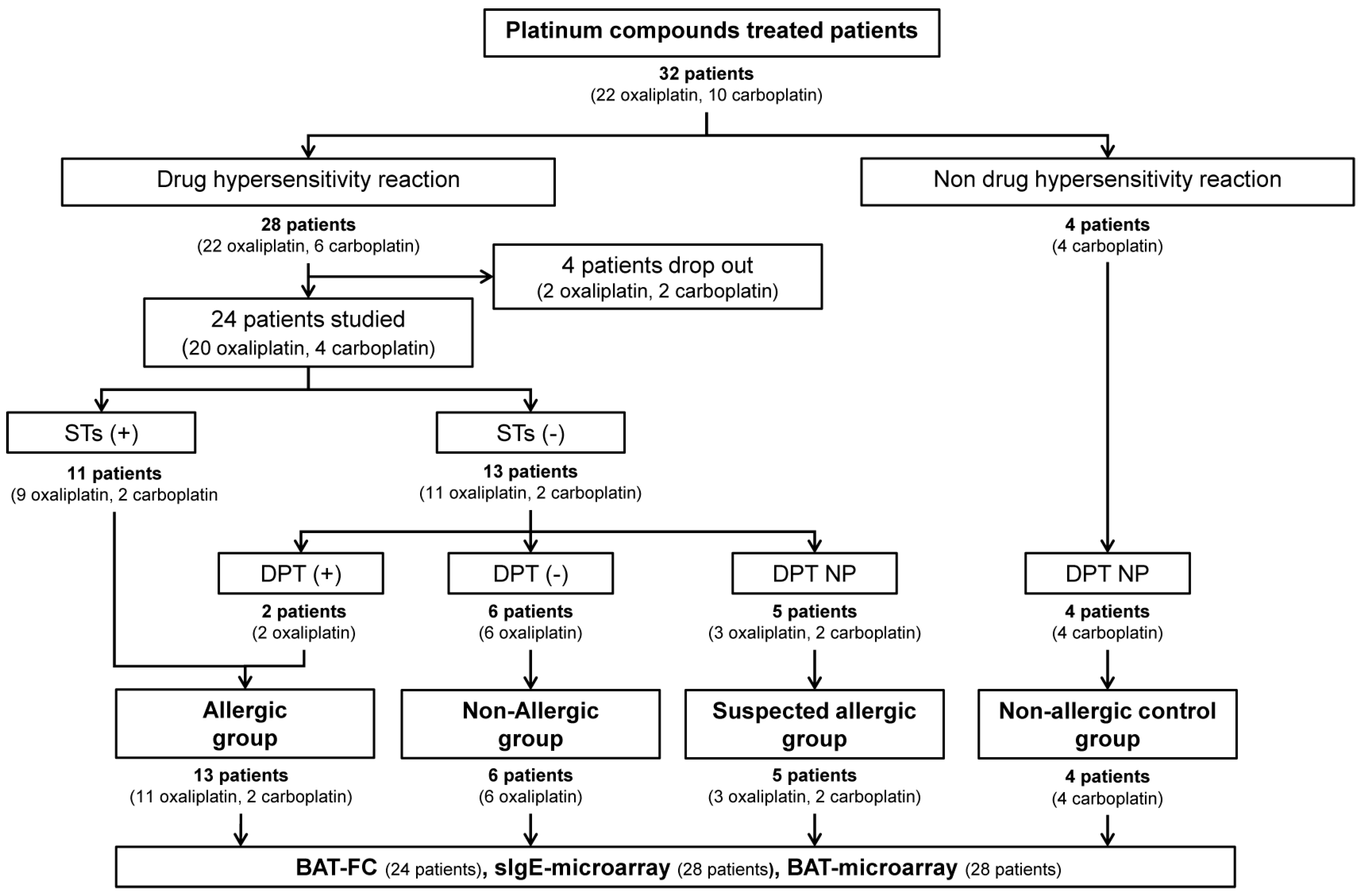
2.1. Characteristics of the Patients
2.2. Allergological Work-Up Outcomes
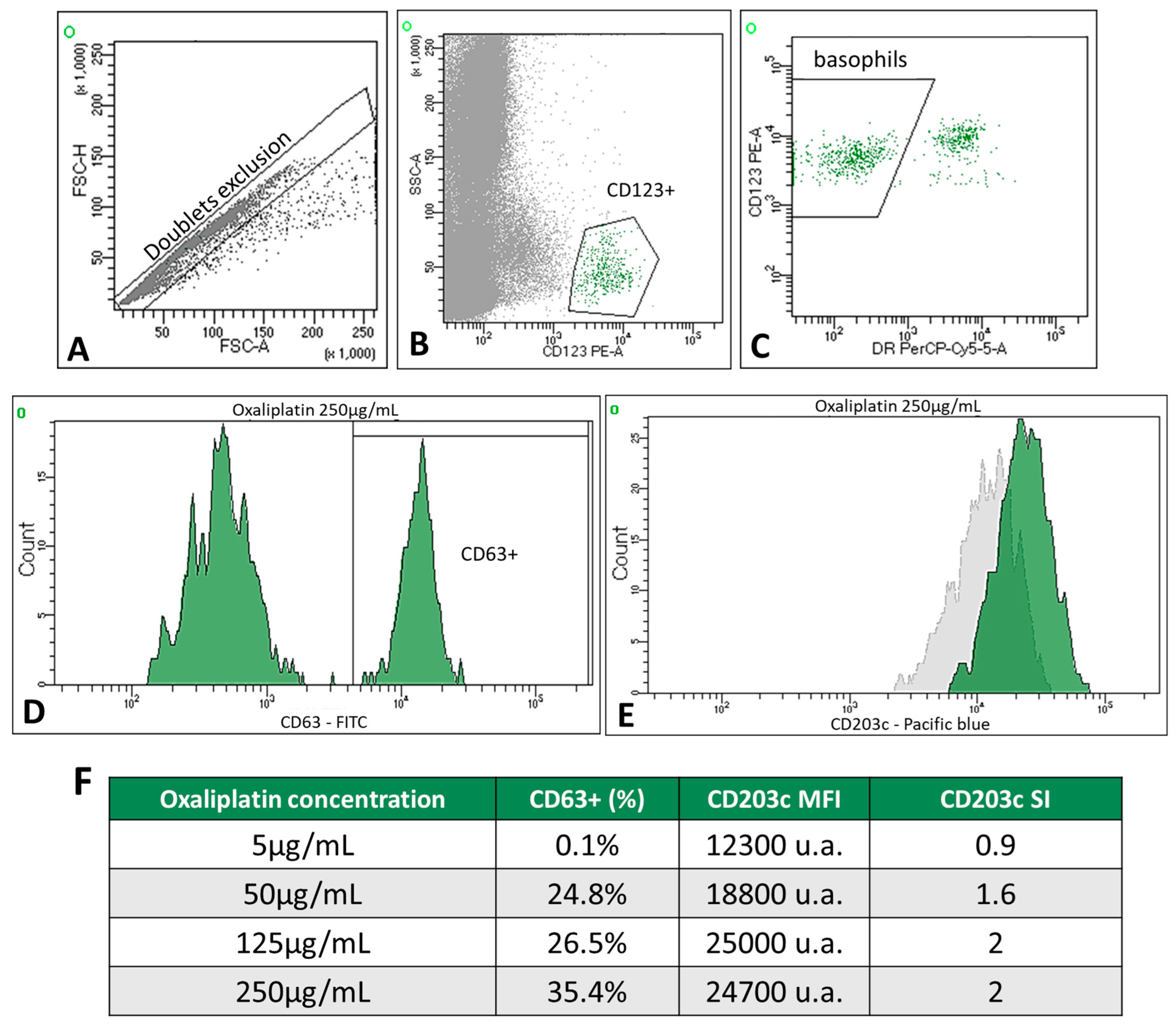
2.3. Basophil Activation Test by Flow Cytometry (BAT-FC)
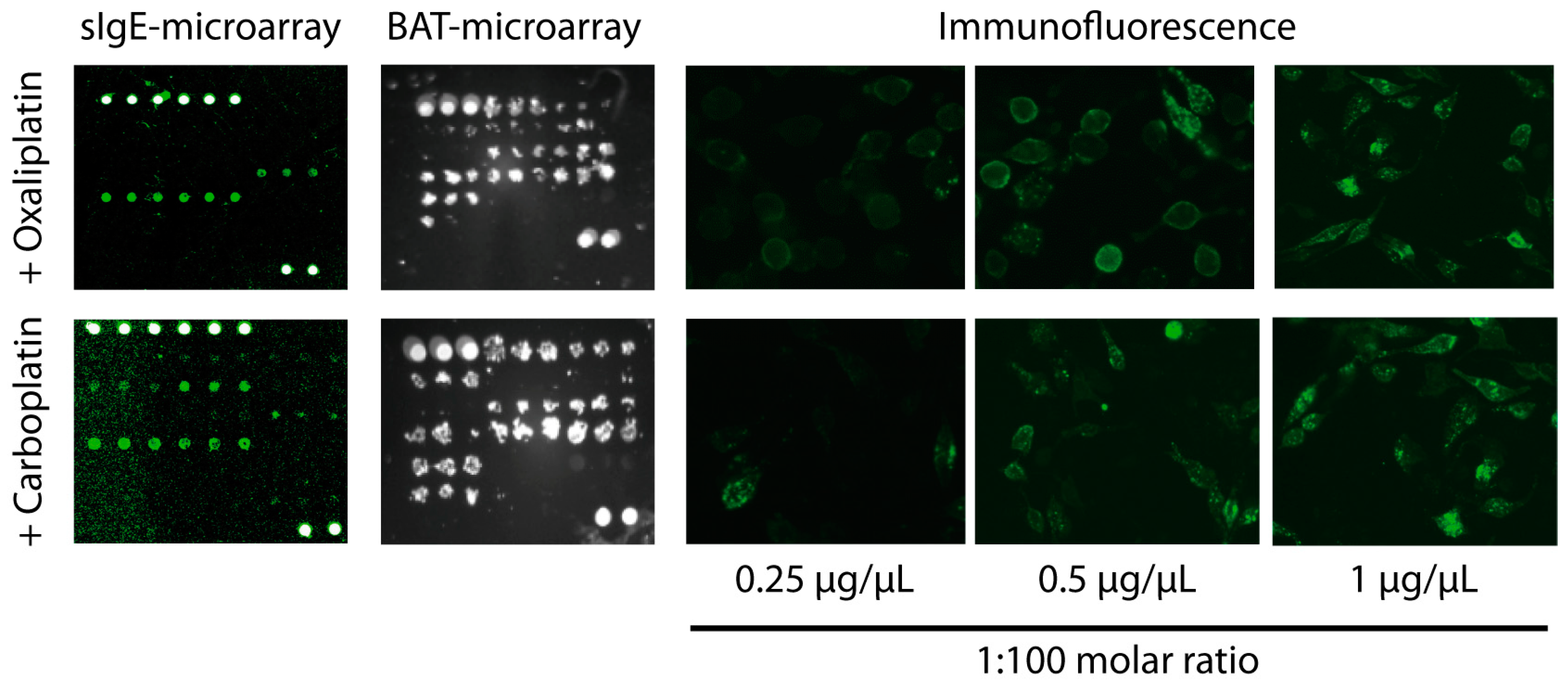
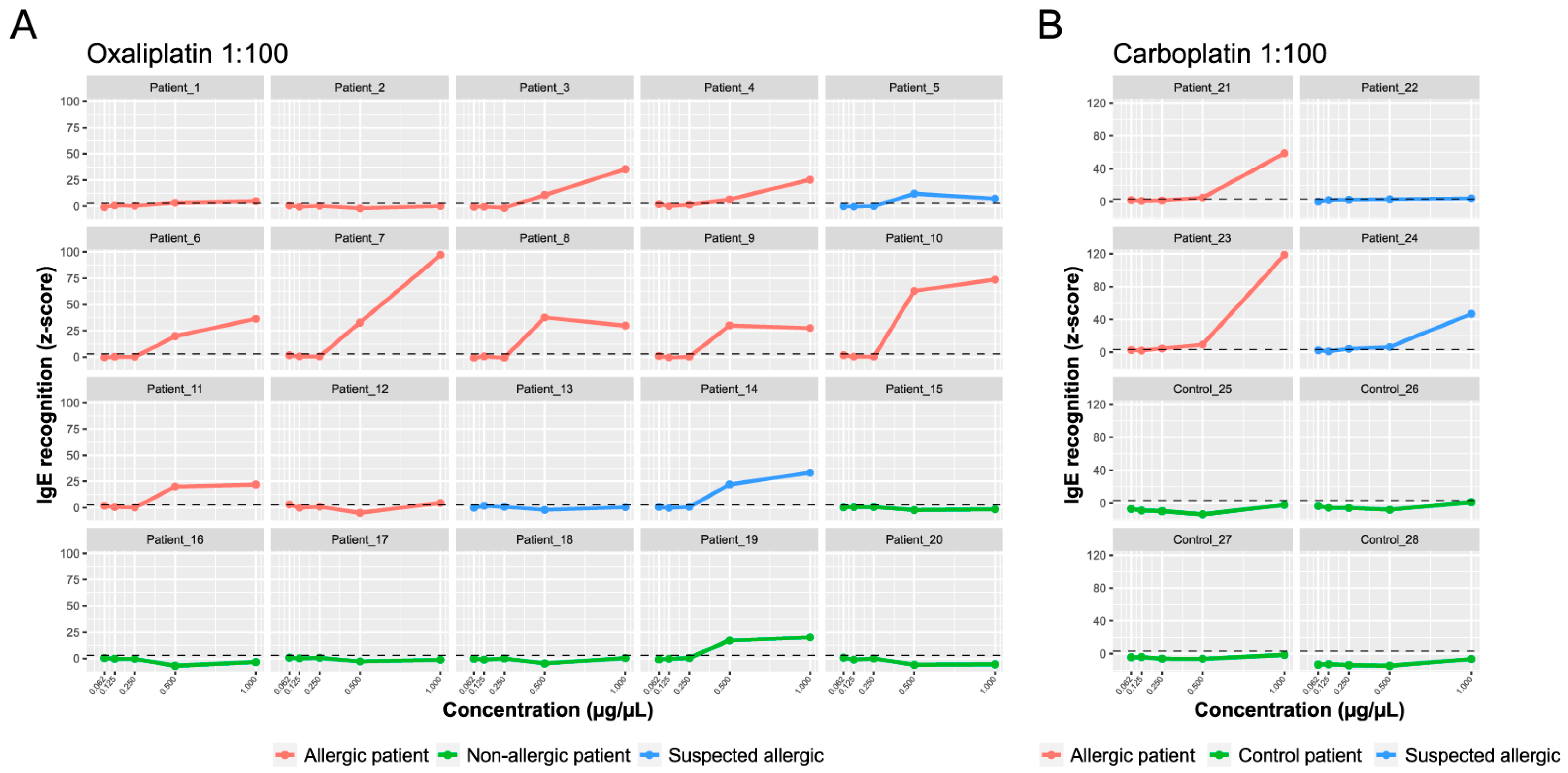
2.4. sIgE-Microarrays Immunoassay
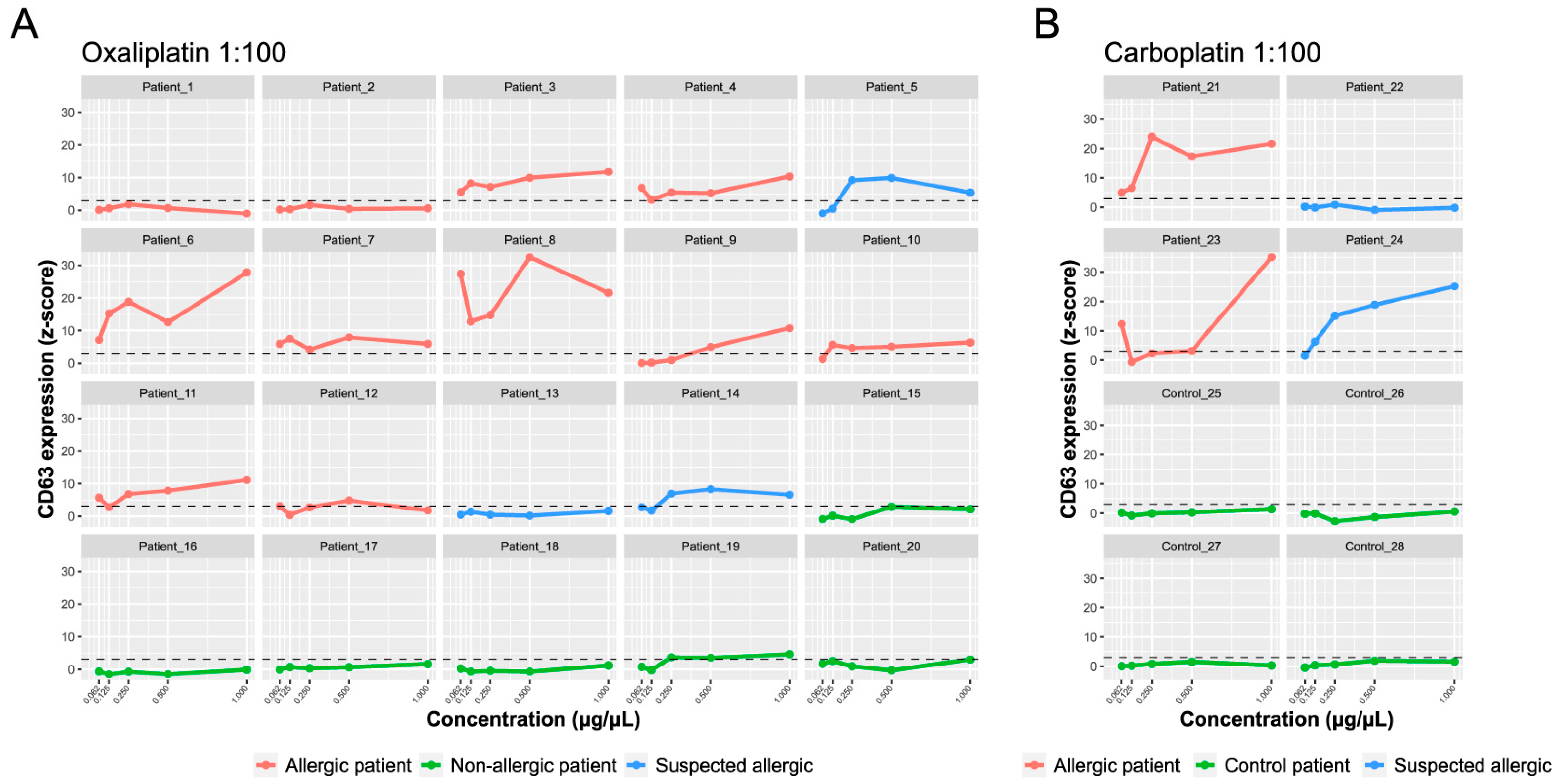
2.5. Basophil Activation Test on Microarray Support (BAT-Microarray)
3. Discussion
4. Materials and Methods
4.1. Patient Population and Study Design
4.2. Basophil Activation Test by Flow Cytometry (BAT-FC)
4.3. Microarray Printing
4.4. sIgE Microarray Immunoassay
4.5. Basophil Activation Test on Microarray Support (BAT-Microarray)
4.6. Data Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Silver, J.; Garcia-Neuer, M.; Lynch, D.M.; Pasaoglu, G.; Sloane, D.E.; Castells, M. Endophenotyping Oxaliplatin Hypersensitivity: Personalizing Desensitization to the Atypical Platin. J. Allergy Clin. Immunol. Pract. 2020, 8, 1668–1680.e2. [Google Scholar] [CrossRef] [PubMed]
- Pagani, M.; Bavbek, S.; Alvarez-Cuesta, E.; Berna Dursun, A.; Bonadonna, P.; Castells, M.; Cernadas, J.; Chiriac, A.; Sahar, H.; Madrigal-Burgaleta, R.; et al. Hypersensitivity reactions to chemotherapy: An EAACI Position Paper. Allergy 2022, 77, 388–403. [Google Scholar] [CrossRef] [PubMed]
- Madrigal-Burgaleta, R.; Bernal-Rubio, L.; Berges-Gimeno, M.P.; Carpio-Escalona, L.V.; Gehlhaar, P.; Alvarez-Cuesta, E. A Large Single-Hospital Experience Using Drug Provocation Testing and Rapid Drug Desensitization in Hypersensitivity to Antineoplastic and Biological Agents. J. Allergy Clin. Immunol. Pract. 2019, 7, 618–632. [Google Scholar] [CrossRef]
- Caiado, J.; Picard, M. Diagnostic tools for hypersensitivity to platinum drugs and taxanes: Skin testing, specific IgE, and mast cell/basophil mediators. Curr. Allergy Asthma Rep. 2014, 14, 451. [Google Scholar] [CrossRef]
- Alpan, O.; Wasserman, R.L.; Kim, T.; Darter, A.; Shah, A.; Jones, D.; McNeil, D.; Li, H.; Ispas, L.; Rathkopf, M.; et al. Towards an FDA-cleared basophil activation test. Front. Allergy 2022, 3, 1009437. [Google Scholar] [CrossRef]
- Iwamoto, T.; Yuta, A.; Tabata, T.; Sugimoto, H.; Gabazza, E.C.; Hirai, H.; Kojima, S.; Okuda, M. Evaluation of basophil CD203c as a predictor of carboplatin-related hypersensitivity reaction in patients with gynecologic cancer. Biol. Pharm. Bull. 2012, 35, 1487–1495. [Google Scholar] [CrossRef] [PubMed]
- Giavina-Bianchi, P.; Galvao, V.R.; Picard, M.; Caiado, J.; Castells, M.C. Basophil Activation Test is a Relevant Biomarker of the Outcome of Rapid Desensitization in Platinum Compounds-Allergy. J. Allergy Clin. Immunol. Pract. 2017, 5, 728–736. [Google Scholar] [CrossRef]
- Ornelas, C.; Caiado, J.; Campos Melo, A.; Pereira Barbosa, M.; Castells, M.C.; Pereira Dos Santos, M.C. The Contribution of the Basophil Activation Test to the Diagnosis of Hypersensitivity Reactions to Oxaliplatin. Int. Arch. Allergy Immunol. 2018, 177, 274–280. [Google Scholar] [CrossRef]
- Caiado, J.; Venemalm, L.; Pereira-Santos, M.C.; Costa, L.; Barbosa, M.P.; Castells, M. Carboplatin-, oxaliplatin-, and cisplatin-specific IgE: Cross-reactivity and value in the diagnosis of carboplatin and oxaliplatin allergy. J. Allergy Clin. Immunol. Pract. 2013, 1, 494–500. [Google Scholar] [CrossRef]
- Huang, H.J.; Campana, R.; Akinfenwa, O.; Curin, M.; Sarzsinszky, E.; Karsonova, A.; Riabova, K.; Karaulov, A.; Niespodziana, K.; Elisyutina, O.; et al. Microarray-Based Allergy Diagnosis: Quo Vadis? Front. Immunol. 2020, 11, 594978. [Google Scholar] [CrossRef]
- Sanchez-Ruano, L.; de la Hoz, B.; Martinez-Botas, J. Clinical utility of microarray B-cell epitope mapping in food allergies: A systematic review. Pediatr. Allergy Immunol. 2020, 31, 175–185. [Google Scholar] [CrossRef] [PubMed]
- Falcone, F.H.; Alcocer, M.J.; Okamoto-Uchida, Y.; Nakamura, R. Use of humanized rat basophilic leukemia reporter cell lines as a diagnostic tool for detection of allergen-specific IgE in allergic patients: Time for a reappraisal? Curr. Allergy Asthma Rep. 2015, 15, 67. [Google Scholar] [CrossRef]
- Blanc, F.; Adel-Patient, K.; Drumare, M.F.; Paty, E.; Wal, J.M.; Bernard, H. Capacity of purified peanut allergens to induce degranulation in a functional in vitro assay: Ara h 2 and Ara h 6 are the most efficient elicitors. Clin. Exp. Allergy 2009, 39, 1277–1285. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.; Renault, N.; Haas, H.; Schramm, G.; Vieths, S.; Vogel, L.; Falcone, F.H.; Alcocer, M.J. A novel tool for the detection of allergic sensitization combining protein microarrays with human basophils. Clin. Exp. Allergy 2007, 37, 1854–1862. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Cato, P.; Lin, H.C.; Li, T.; Wan, D.; Alcocer, M.J.; Falcone, F.H. Optimisation and use of humanised RBL NF-AT-GFP and NF-AT-DsRed reporter cell lines suitable for high-throughput scale detection of allergic sensitisation in array format and identification of the ECM-integrin interaction as critical factor. Mol. Biotechnol. 2014, 56, 136–146. [Google Scholar] [CrossRef]
- Demoly, P.; Adkinson, N.F.; Brockow, K.; Castells, M.; Chiriac, A.M.; Greenberger, P.A.; Khan, D.A.; Lang, D.M.; Park, H.S.; Pichler, W.; et al. International Consensus on drug allergy. Allergy 2014, 69, 420–437. [Google Scholar] [CrossRef]
- Brown, S.G. Clinical features and severity grading of anaphylaxis. J. Allergy Clin. Immunol. 2004, 114, 371–376. [Google Scholar] [CrossRef]
- Brockow, K.; Romano, A.; Blanca, M.; Ring, J.; Pichler, W.; Demoly, P. General considerations for skin test procedures in the diagnosis of drug hypersensitivity. Allergy 2002, 57, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Vogel, L.; Luttkopf, D.; Hatahet, L.; Haustein, D.; Vieths, S. Development of a functional in vitro assay as a novel tool for the standardization of allergen extracts in the human system. Allergy 2005, 60, 1021–1028. [Google Scholar] [CrossRef]
- Lin, J.; Bardina, L.; Shreffler, W.G.; Andreae, D.A.; Ge, Y.; Wang, J.; Bruni, F.M.; Fu, Z.; Han, Y.; Sampson, H.A. Development of a novel peptide microarray for large-scale epitope mapping of food allergens. J. Allergy Clin. Immunol. 2009, 124, 315–322.E3. [Google Scholar] [CrossRef]
- Kolkhir, P.; Ali, H.; Babina, M.; Ebo, D.; Sabato, V.; Elst, J.; Frischbutter, S.; Pyatilova, P.; Maurer, M. MRGPRX2 in drug allergy: What we know and what we do not know. J. Allergy Clin. Immunol. 2023, 151, 410–412. [Google Scholar] [CrossRef]
- Hoffmann, H.J.; Santos, A.F.; Mayorga, C.; Nopp, A.; Eberlein, B.; Ferrer, M.; Rouzaire, P.; Ebo, D.G.; Sabato, V.; Sanz, M.L.; et al. The clinical utility of basophil activation testing in diagnosis and monitoring of allergic disease. Allergy 2015, 70, 1393–1405. [Google Scholar] [CrossRef] [PubMed]
- Depince-Berger, A.E.; Sidi-Yahya, K.; Jeraiby, M.; Lambert, C. Basophil activation test: Implementation and standardization between systems and between instruments. Cytom. Part A J. Int. Soc. Anal. Cytol. 2017, 91, 261–269. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Santos, A.F.; Alpan, O.; Hoffmann, H.J. Basophil activation test: Mechanisms and considerations for use in clinical trials and clinical practice. Allergy 2021, 76, 2420–2432. [Google Scholar] [CrossRef] [PubMed]
- Berges Gimeno, M.P.; Bernal Rubio, L.; Roldan, E.; Rita, C.G. Positive Basophil Activation Test Result in a Patient With Anaphylaxis to Cotrimoxazole. J. Investig. Allergol. Clin. Immunol. 2022, 32, 410–412. [Google Scholar] [CrossRef]
- Phillips-Angles, E.; Gonzalez-Munoz, M.; Dominguez-Ortega, J.; Cabanas, R.; Quirce, S. Usefulness of basophil activation test in diagnosis of hypersensitivity to etoricoxib. J. Allergy Clin. Immunol. Pract. 2016, 4, 350–351. [Google Scholar] [CrossRef]
- Puan, K.J.; Andiappan, A.K.; Lee, B.; Kumar, D.; Lai, T.S.; Yeo, G.; Bercin, D.; Starke, M.; Haase, D.; Lum, J.; et al. Systematic characterization of basophil anergy. Allergy 2017, 72, 373–384. [Google Scholar] [CrossRef]
- Falcone, F.H.; Gibbs, B.F. Purification of Basophils from Peripheral Human Blood. Methods Mol. Biol. 2020, 2163, 35–48. [Google Scholar]
- Ladics, G.S.; van Bilsen, J.H.; Brouwer, H.M.; Vogel, L.; Vieths, S.; Knippels, L.M. Assessment of three human FcepsilonRI-transfected RBL cell-lines for identifying IgE induced degranulation utilizing peanut-allergic patient sera and peanut protein extract. Regul. Toxicol. Pharmacol. RTP 2008, 51, 288–294. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Type of Tumor | Sex | Age (Years) | Drug | Grade of Initial Reaction Brown/HRYC | Lifetime Exposure (Previous Cycles) | Time to Index Reaction (min) | Symptoms | History of Atopic Disease/HR |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Colorectal | F | 68 | Oxaliplatin | 1.1 | 7 | 60 | Urticaria, erythema, pruritus | No/No |
| 2 | Colorectal | M | 69 | Oxaliplatin | 2.2 | 20 | 5 | Urticaria, erythema, pruritus, nausea | No/No |
| 3 | Colon | M | 76 | Oxaliplatin | 1.1 | 4 | 30 | Erythema, pruritus, warm sensation | No/No |
| 4 | Sigmoid | F | 63 | Oxaliplatin | 2.1–2 | 9 | 60 | Warm, diaphoresis, chills | No/No |
| 5 | Colon | M | 71 | Oxaliplatin | 3.3 | 10 | 120 | Erythema, flushing, pruritus, desaturation | No/No |
| 6 | Gastric | F | 53 | Oxaliplatin | 2.3 | 6 | 45 | Erythema, flushing, pruritus, chest tightness | No/No |
| 7 | Rectal | F | 64 | Oxaliplatin | 1.1 | 3 | 60 | Erythema, flushing | No/No |
| 8 | Sigmoid and rectal | M | 63 | Oxaliplatin | 3.3 | 9 | 70 | Pruritus, maculopapular rash, desaturation | Yes/Yes |
| 9 | Colon | M | 68 | Oxaliplatin | 3.3 | 3 | 60 | Cough, desaturation, throat tightness | No/No |
| 10 | Colorectal | F | 58 | Oxaliplatin | 3.4 | 3 | 60 | Erythema, flushing, dyspnea, desaturation, syncope, confusion, dizziness | No/Yes |
| 11 | Colon | M | 70 | Oxaliplatin | 3.3 | 5 | 20 | Erythema, flushing, pruritus, desaturation | Yes/No |
| 12 | Sigmoid | F | 71 | Oxaliplatin | 1.1 | 9 | 5 | Localized urticaria, pruritus | No/No |
| 13 | Sigmoid | M | 60 | Oxaliplatin | 2.2 | 1 | 120 | Dysesthesias, dyspnea, dysphonia, uvula edema | Yes/Yes |
| 14 | Sigmoid | F | 70 | Oxaliplatin | 1.1 | 3 | 60 | Localized urticaria, pruritus | No/No |
| 15 | Colon | M | 49 | Oxaliplatin | 1.1 | 8 | 70 | Erythema, Dysesthesias | Yes/No |
| 16 | Sigmoid | F | 68 | Oxaliplatin | 2.2 | 1 | 60 | Dyspnea, dysphonia, tachycardia | No/No |
| 17 | Sigmoid | F | 75 | Oxaliplatin | 2.3 | 1 | 120 | Dyspnea, wheeze | Yes/No |
| 18 | Rectal | M | 82 | Oxaliplatin | 1.1 | 22 | 480 | Flushing | Yes/No |
| 19 | Colon | F | 57 | Oxaliplatin | 2.3 | 1 | 60 | Dysesthesias, dyspnea, throat tightness | No/No |
| 20 | Colorectal | F | 58 | Oxaliplatin | 1.1 | 3 | 48 | Pruritus, dysesthesia | No/No |
| 21 | Endometrial | F | 57 | Carboplatin | 3.3 | 6 | 15 | Dyspnea, desaturation, hypertension, chest pain | No/Yes |
| 22 | Ovarian | F | 48 | Carboplatin | 2.2 | 15 | Not Known | Localized urticaria, dyspnea | No/Yes |
| 23 | Lung | M | 75 | Carboplatin | 3.3 | 7 | 60 | Pruritus, dyspnea, desaturation | No/No |
| 24 | Ovarian | F | 69 | Carboplatin | 1.1 | 9 | 15 | Urticaria, hands and foot pruritus | No/No |
| 25 | Lung | M | 73 | Carboplatin | NR ‡ | 1 | NA † | NA † | No/No |
| 26 | Vulvar | F | 53 | Carboplatin | NR ‡ | 2 | NA † | NA † | Yes/Yes |
| 27 | Ovarian | F | 43 | Carboplatin | NR ‡ | 1 | NA † | NA † | No/Yes |
| 28 | Breast | F | 34 | Carboplatin | NR ‡ | 4 | NA † | NA † | No/Yes |
| Patient | Drug | Skin Tests | DPT | Tryptase (Basal) | Tryptase (Reaction) | Total IgE | BAT-FC CD63 | BAT-FC CD203c | sIgE-Microarray | BAT-Microarray |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Oxaliplatin | +(IDT 0.5 mg/mL) | NP † | 6.67 | NP † | 354 | - | NP † | 4.96 | ND ‡ |
| 2 | Oxaliplatin | +(IDT 0.5 mg/ml | NP † | 7.57 | NP † | 71 | - | - | 0.02 | 0.55 |
| 3 | Oxaliplatin | - | + | <1 | NP † | 4 | - | - | 35.39 | 11.75 |
| 4 | Oxaliplatin | - | + | 13.8 | 13.70 | 6 | - | - | 25.40 | 10.33 |
| 5 | Oxaliplatin | - | NP † | <1 | NP † | 157 | - | - | 7.37 | 5.39 |
| 6 | Oxaliplatin | +(IDT 5 mg/mL) | NP † | 1.03 | NP † | 43 | + | + | 36.37 | 27.76 |
| 7 | Oxaliplatin | +(IDT 0.5 mg/mL) | NP † | 7.34 | NP † | 608 | - | - | 97.20 | 5.96 |
| 8 | Oxaliplatin | +(SPT 0.5–5 mg/mL) | NP † | 6.69 | NP † | 798 | - | - | 29.79 | 21.57 |
| 9 | Oxaliplatin | +(IDT 5 mg/mL) | NP † | 5.09 | NP † | 240 | - | - | 27.45 | 10.75 |
| 10 | Oxaliplatin | +(IDT 0.005 mg/mL) | NP † | 7.49 | NP † | 23 | - | - | 73.75 | 6.38 |
| 11 | Oxaliplatin | +(IDT 0.5 mg/mL) | NP † | 6.56 | NP † | 17 | - | - | 21.99 | 11.12 |
| 12 | Oxaliplatin | +(IDT 0.5 mg/mL) | NP † | 6.06 | NP † | 29 | - | - | 4.57 | 4.84 * |
| 13 | Oxaliplatin | - | NP † | 5.08 | NP † | 90 | - | - | 0.38 | 1.61 |
| 14 | Oxaliplatin | - | NP † | 5.81 | NP † | 71 | NP † | NP † | 33.45 | 6.60 |
| 15 | Oxaliplatin | - | - | 6.32 | NP † | 38 | - | - | ND ‡ | 2.11 |
| 16 | Oxaliplatin | - | - | 3.6 | NP † | 32 | - | - | 0.32 | ND ‡ |
| 17 | Oxaliplatin | - | - | 4.37 | NP † | 9 | NV § | - | ND | 1.57 |
| 18 | Oxaliplatin | - | - | 3.02 | NP † | 633 | - | - | 0.36 | 1.16 |
| 19 | Oxaliplatin | - | - | 3.41 | NP † | 463 | NV § | NP † | 19.91 | 4.60 |
| 20 | Oxaliplatin | - | - | 7.32 | NP † | 41 | - | NP † | ND ‡ | 2.90 |
| 21 | Carboplatin | +(IDT 1 mg/mL) | NP † | 2.14 | NP † | 743 | + | - | 58.76 | 21.62 |
| 22 | Carboplatin | - | NP † | 4.48 | NP † | 54 | - | - | 3.92 | ND ‡ |
| 23 | Carboplatin | +(IDT 1 mg/mL) | NP † | 7.41 | NP † | 49 | - | - | 118.72 | 35.11 |
| 24 | Carboplatin | - | NP † | 3.67 | NP † | 5 | - | - | 46.76 | 25.21 |
| 25 | Carboplatin | NP † | NP † | NP † | NP † | NP † | - | - | ND ‡ | 1.33 |
| 26 | Carboplatin | NP † | NP † | NP † | NP † | NP † | - | - | 1.03 | 0.56 |
| 27 | Carboplatin | NP † | NP † | NP † | NP † | NP † | NP † | NP † | ND ‡ | 0.26 |
| 28 | Carboplatin | NP † | NP † | NP † | NP † | NP † | NP † | NP † | ND ‡ | 1.59 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-Lozano, C.; Rita, C.G.; Barra-Castro, A.; de la Hoz Caballer, B.; Roldán, E.; Pueyo López, C.; Martinez-Botas, J.; Berges-Gimeno, M.P. Specific IgE and Basophil Activation Test by Microarray: A Promising Tool for Diagnosis of Platinum Compound Hypersensitivity Reactions. Int. J. Mol. Sci. 2024, 25, 3890. https://doi.org/10.3390/ijms25073890
Fernández-Lozano C, Rita CG, Barra-Castro A, de la Hoz Caballer B, Roldán E, Pueyo López C, Martinez-Botas J, Berges-Gimeno MP. Specific IgE and Basophil Activation Test by Microarray: A Promising Tool for Diagnosis of Platinum Compound Hypersensitivity Reactions. International Journal of Molecular Sciences. 2024; 25(7):3890. https://doi.org/10.3390/ijms25073890
Chicago/Turabian StyleFernández-Lozano, Carlos, Claudia Geraldine Rita, Alicia Barra-Castro, Belén de la Hoz Caballer, Ernesto Roldán, Cristina Pueyo López, Javier Martinez-Botas, and María Pilar Berges-Gimeno. 2024. "Specific IgE and Basophil Activation Test by Microarray: A Promising Tool for Diagnosis of Platinum Compound Hypersensitivity Reactions" International Journal of Molecular Sciences 25, no. 7: 3890. https://doi.org/10.3390/ijms25073890
APA StyleFernández-Lozano, C., Rita, C. G., Barra-Castro, A., de la Hoz Caballer, B., Roldán, E., Pueyo López, C., Martinez-Botas, J., & Berges-Gimeno, M. P. (2024). Specific IgE and Basophil Activation Test by Microarray: A Promising Tool for Diagnosis of Platinum Compound Hypersensitivity Reactions. International Journal of Molecular Sciences, 25(7), 3890. https://doi.org/10.3390/ijms25073890