
Titanium Surfaces with a Laser-Produced Microchannel Structure Enhance Pre-Osteoblast Proliferation, Maturation, and Extracellular Mineralization In Vitro


 and
and
Abstract
1. Introduction
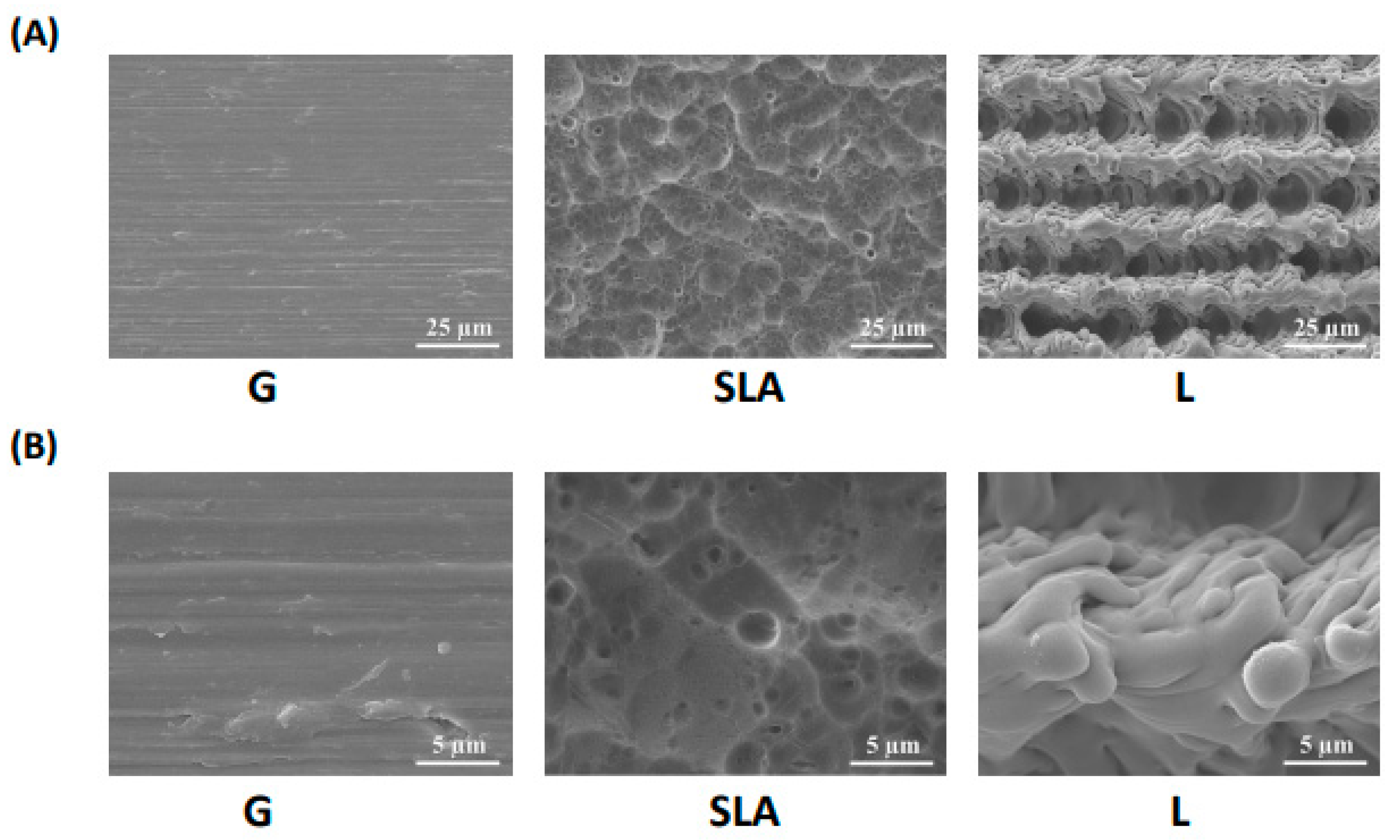
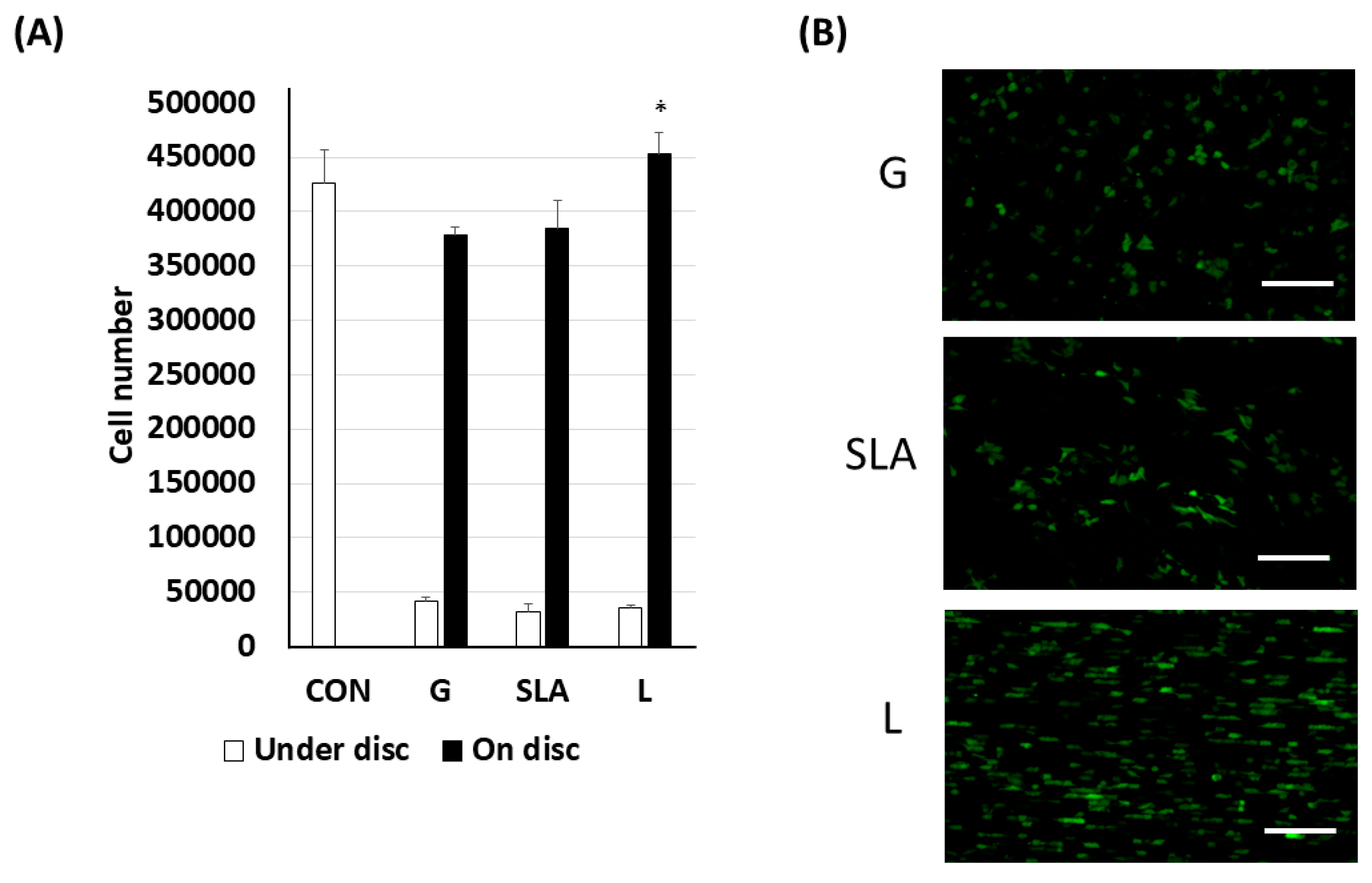
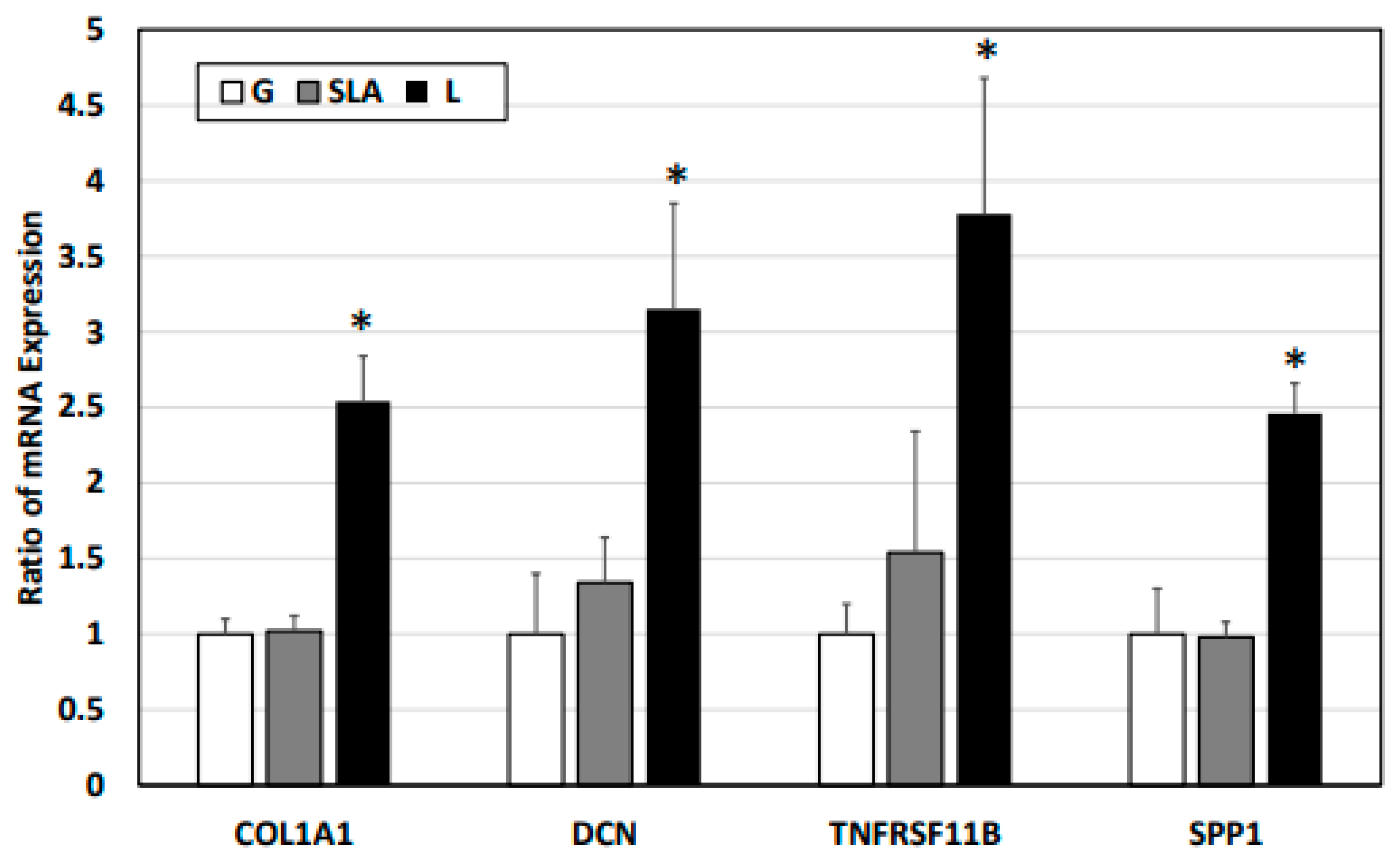
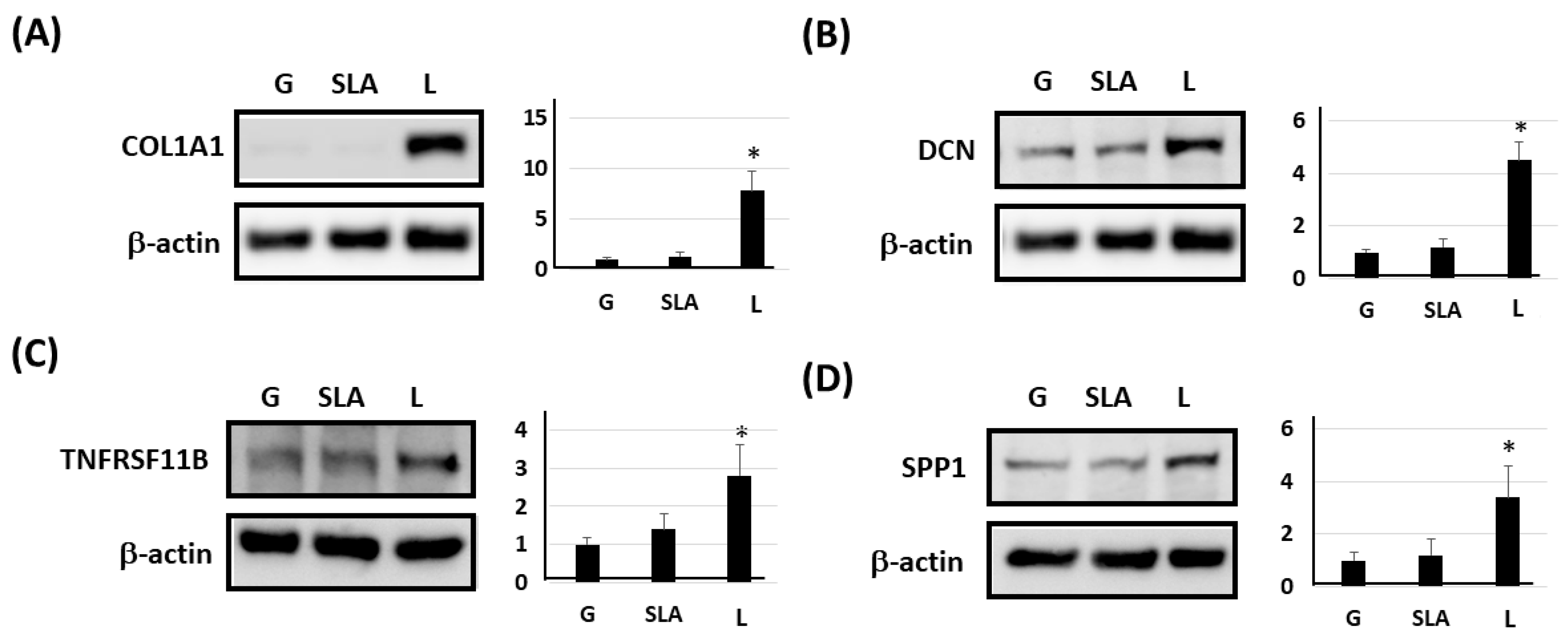
2. Results
3. Discussion
4. Materials and Methods
4.1. Cell Culture
4.2. Titanium Plate and Implant
4.3. Cell Number Determination
4.4. Cell Morphology
4.5. Reverse Transcription Quantitative Polymerase Chain Reaction
4.6. Protein Extraction and Western Blot Assay
4.7. Multiplex Assay
4.8. Extracellular Mineralization Assay
4.9. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Silva, R.C.S.; Agrelli, A.; Andrade, A.N.; Mendes-Marques, C.L.; Arruda, I.R.S.; Santos, L.R.L.; Vasconcelos, N.F.; Machado, G. Titanium Dental Implants: An Overview of Applied Nanobiotechnology to Improve Biocompatibility and Prevent Infections. Materials 2022, 15, 3150. [Google Scholar] [CrossRef]
- Hao, C.P.; Cao, N.J.; Zhu, Y.H.; Wang, W. The osseointegration and stability of dental implants with different surface treatments in animal models: A network meta-analysis. Sci. Rep. 2021, 11, 13849. [Google Scholar] [CrossRef]
- Insua, A.; Monje, A.; Wang, H.L.; Miron, R.J. Basis of bone metabolism around dental implants during osseointegration and peri-implant bone loss. J. Biomed. Mater. Res. A 2017, 105, 2075–2089. [Google Scholar] [CrossRef]
- Amarasekara, D.S.; Kim, S.; Rho, J. Regulation of Osteoblast Differentiation by Cytokine Networks. Int. J. Mol. Sci. 2021, 22, 2851. [Google Scholar] [CrossRef]
- Suzuki, S.; Kobayashi, H.; Ogawa, T. Implant stability change and osseointegration speed of immediately loaded photofunctionalized implants. Implant. Dent. 2013, 22, 481–490. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, Y.; Miron, R.J. Health, Maintenance, and Recovery of Soft Tissues around Implants. Clin. Implant. Dent. Relat. Res. 2016, 18, 618–634. [Google Scholar] [CrossRef]
- Stich, T.; Alagboso, F.; Křenek, T.; Kovářík, T.; Alt, V.; Docheva, D. Implant-bone-interface: Reviewing the impact of titanium surface modifications on osteogenic processes in vitro and in vivo. Bioeng. Transl. Med. 2021, 7, e10239. [Google Scholar] [CrossRef]
- Tsai, M.H.; Haung, C.F.; Shyu, S.S.; Chou, Y.R.; Lin, M.H.; Peng, P.W.; Ou, K.L.; Yu, C.H. Surface modification induced phase transformation and structure variation on the rapidly solidified recast layer of titanium. Mater. Charact. 2015, 106, 463–469. [Google Scholar] [CrossRef]
- Huang, M.S.; Chen, L.K.; Ou, K.L.; Cheng, H.Y.; Wang, C.S. Rapid Osseointegration of titanium implant with innovative nanoporous surface modification: Animal model and clinical trial. Implant. Dent. 2015, 24, 441–447. [Google Scholar] [CrossRef] [PubMed]
- Chiang, H.J.; Hsu, H.J.; Peng, P.W.; Wu, C.Z.; Ou, K.L.; Cheng, H.Y.; Walinski, C.J.; Sugiatno, E. Early bone response to machined, sandblasting acid etching (SLA) and novel surface-functionalization (SLAffinity) titanium implants: Characterization, biomechanical analysis and histological evaluation in pigs. J. Biomed. Mater. Res. A 2016, 104, 397–405. [Google Scholar] [CrossRef] [PubMed]
- Dzogbewu, T.C.; du Preez, W.B. Additive manufacturing of Ti-based intermetallic alloys: A review and conceptualization of a next-generation machine. Materials 2021, 14, 4317. [Google Scholar] [CrossRef]
- Davis, R.; Singh, A.; Jackson, M.J.; Coelho, R.T.; Prakash, D.; Charalambous, C.P.; Ahmed, W.; da Silva, L.R.R.; Lawrence, A.A. A comprehensive review on metallic implant biomaterials and their subtractive manufacturing. Int. J. Adv. Manuf. Technol. 2022, 120, 1473–1530. [Google Scholar] [CrossRef]
- Kligman, S.; Ren, Z.; Chung, C.H.; Perillo, M.A.; Chang, Y.C.; Koo, H.; Zheng, Z.; Li, C. The impact of dental implant surface modifications on osseointegration and biofilm formation. J. Clin. Med. 2021, 10, 1641. [Google Scholar] [CrossRef]
- Hasegawa, M.; Saruta, J.; Hirota, M.; Taniyama, T.; Sugita, Y.; Kubo, K.; Ishijima, M.; Ikeda, T.; Maeda, H.; Ogawa, T. A newly created meso-, micro-, and nano-scale rough titanium surface promotes bone-implant integration. Int. J. Mol. Sci. 2020, 21, 783. [Google Scholar] [CrossRef]
- Dhaliwal, J.S.; Abd Rahman, N.A.; Ming, L.C.; Dhaliwal, S.K.S.; Knights, J.; Albuquerque, R.F., Jr. Microbial biofilm decontamination on dental implant surfaces: A mini review. Front. Cell Infect. Microbiol. 2021, 11, 736186. [Google Scholar] [CrossRef]
- Lee, H.T.; Lin, C.C. Enhanced cell proliferation on biomedical titanium surfaces by laser ablation-induced micro- and nanoscale hybrid structures. Mater. Trans. 2019, 60, 1799–1860. [Google Scholar] [CrossRef]
- Bressel, T.A.B.; de Queiroz, J.D.F.; Gomes Moreira, S.M.; da Fonseca, J.T.; Filho, E.A.; Guastaldi, A.C.; Batistuzzo de Medeiros, S.R. Laser-modified titanium surfaces enhance the osteogenic differentiation of human mesenchymal stem cells. Stem Cell Res. Ther. 2017, 8, 269. [Google Scholar] [CrossRef]
- Lee, K.K.; Sirichai, K.; Verasak, P.; Nisanat, L.; Natthamet, W.; Dutmanee, S. The affinity of human fetal osteoblast to laser-modified titanium implant fixtures. Open Dent. J. 2020, 14, 52. [Google Scholar] [CrossRef]
- Galli, C.; Macaluso, G.M.; Elezi, E.; Ravanetti, F.; Cacchioli, A.; Gualini, G.; Passeri, G. The effects of Er:YAG laser treatment on titanium surface profile and osteoblastic cell activity: An in vitro study. J. Periodontol. 2011, 82, 1169–1177. [Google Scholar] [CrossRef]
- Wehner, C.; Laky, M.; Shokoohi-Tabrizi, H.A.; Behm, C.; Moritz, A.; Rausch-Fan, X.; Andrukhov, O. Effects of Er:YAG laser irradiation of different titanium surfaces on osteoblast response. J. Mater. Sci. Mater. Med. 2021, 32, 22. [Google Scholar] [CrossRef]
- Facer, S.R.; Zaharias, R.S.; Andracki, M.E.; Lafoon, J.; Hunter, S.K.; Schneider, G.B. Rotary culture enhances pre-osteoblast aggregation and mineralization. J. Dent. Res. 2005, 84, 542–547. [Google Scholar]
- Hou, H.H.; Lee, B.S.; Liu, Y.C.; Wang, Y.P.; Kuo, W.T.; Chen, I.H.; He, A.C.; Lai, C.H.; Tung, K.L.; Chen, Y.W. Vapor-induced pore-forming atmospheric-plasma-sprayed zinc-, strontium-, and magnesium-doped hydroxyapatite coatings on titanium implants enhance new bone formation-an in vivo and in vitro investigation. Int. J. Mol. Sci. 2023, 24, 4933. [Google Scholar] [CrossRef]
- Setzer, B.; Bächle, M.; Metzger, M.C.; Kohal, R.J. The gene-expression and phenotypic response of hFOB 1.19 osteoblasts to surface-modified titanium and zirconia. Biomaterials 2009, 30, 979–990. [Google Scholar] [CrossRef]
- Blair, H.C.; Larrouture, Q.C.; Li, Y.; Lin, H.; Beer-Stoltz, D.; Liu, L.; Tuan, R.S.; Robinson, L.J.; Schlesinger, P.H.; Nelson, D.J. Osteoblast differentiation and bone matrix formation in vivo and in vitro. Tissue Eng. Part. B Rev. 2017, 23, 268–280. [Google Scholar] [CrossRef]
- Li, F.; Yang, Y.; Zhu, P.; Chen, W.; Qi, D.; Shi, X.; Zhang, C.; Yang, Z.; Li, P. Echinacoside promotes bone regeneration by increasing OPG/RANKL ratio in MC3T3-E1 cells. Fitoterapia 2012, 83, 1443–1450. [Google Scholar] [CrossRef]
- Gallo, J.; Goodman, S.B.; Konttinen, Y.T.; Raska, M. Particle disease: Biologic mechanisms of periprosthetic osteolysis in total hip arthroplasty. Innate Immun. 2013, 19, 213–224. [Google Scholar] [CrossRef]
- Goiato, M.C.; Dos Santos, D.M.; Santiago, J.F., Jr.; Moreno, A.; Pellizzer, E.P. Longevity of dental implants in type IV bone: A systematic review. Int. J. Oral. Maxillofac. Surg. 2014, 43, 1108–1116. [Google Scholar] [CrossRef]
- Esposito, M.; Hirsch, J.M.; Lekholm, U.; Thomsen, P. Biological factors contributing to failures of osseointegrated oral implants. (I). Success. criteria and epidemiology. Eur. J. Oral. Sci. 1998, 106, 527–551. [Google Scholar]
- Esposito, M.; Thomsen, P.; Ericson, L.E.; Lekholm, U. Histopathologic observations on early oral implant failures. Int. J. Oral. Maxillofac. Implant. 1999, 14, 798–810. [Google Scholar]
- Huynh-Ba, G.; Friedberg, J.R.; Vogiatzi, D.; Ioannidou, E. Implant failure predictors in the posterior maxilla: A retrospective study of 273 consecutive implants. J. Periodontol. 2008, 79, 2256–2261. [Google Scholar] [CrossRef]
- Sverzut, A.T.; Stabile, G.A.; de Moraes, M.; Mazzonetto, R.; Moreira, R.W. The influence of tobacco on early dental implant failure. J. Oral. Maxillofac. Surg. 2008, 66, 1004–1009. [Google Scholar] [CrossRef]
- Urban, T.; Kostopoulos, L.; Wenzel, A. Immediate implant placement in molar regions: Risk factors for early failure. Clin. Oral. Implants Res. 2012, 23, 220–227. [Google Scholar] [CrossRef]
- Nastri, L.; Moretti, A.; Migliaccio, S.; Paoletta, M.; Annunziata, M.; Liguori, S.; Toro, G.; Bianco, M.; Cecoro, G.; Guida, L.; et al. Do Dietary Supplements and Nutraceuticals Have Effects on Dental Implant Osseointegration? A Scoping Review. Nutrients 2020, 12, 268. [Google Scholar] [CrossRef]
- Grande, F.; Pozzan, M.C.; Marconato, R.; Mollica, F.; Catapano, S. Evaluation of Load Distribution in a Mandibular Model with Four Implants Depending on the Number of Prosthetic Screws Used for OT-Bridge System: A Finite Element Analysis (FEA). Materials 2022, 15, 7963. [Google Scholar] [CrossRef]
- Hoque, M.E.; Showva, N.N.; Ahmed, M.; Rashid, A.B.; Sadique, S.E.; El-Bialy, T.; Xu, H. Titanium and titanium alloys in dentistry: Current trends, recent developments, and future prospects. Heliyon 2022, 8, e11300. [Google Scholar] [CrossRef]
- Han, X.; Ma, J.; Tian, A.; Wang, Y.; Li, Y.; Dong, B.; Tong, X.; Ma, X. Surface modification techniques of titanium and titanium alloys for biomedical orthopaedics applications: A review. Colloids Surf. B Biointerfaces 2023, 227, 113339. [Google Scholar] [CrossRef]
- Li, J.; Zheng, Y.; Yu, Z.; Kankala, R.K.; Lin, Q.; Shi, J.; Chen, C.; Luo, K.; Chen, A.; Zhong, Q. Surface-modified titanium and titanium-based alloys for improved osteogenesis: A critical review. Heliyon 2023, 10, e23779. [Google Scholar] [CrossRef]
- Schneider, G.B.; Zaharias, R.; Seabold, D.; Keller, J.; Stanford, C. Differentiation of preosteoblasts is affected by implant surface microtopographies. J. Biomed. Mater. Res. A 2004, 69, 462–468. [Google Scholar] [CrossRef]
- Gaggl, A.; Schultes, G.; Müller, W.D.; Kärcher, H. Scanning electron microscopical analysis of laser-treated titanium implant surfaces—A comparative study. Biomaterials 2000, 21, 1067–1073. [Google Scholar] [CrossRef]
- Kreisler, M.; Kohnen, W.; Christoffers, A.B.; Götz, H.; Jansen, B.; Duschner, H.; d’Hoedt, B. In vitro evaluation of the biocompatibility of contaminated implant surfaces treated with an Er:YAG laser and an air powder system. Clin. Oral. Implants Res. 2005, 16, 36–43. [Google Scholar] [CrossRef]
- Allegrini, S., Jr.; Yoshimoto, M.; Salles, M.B.; de Almeida Bressiani, A.H. Biologic response to titanium implants with laser-treated surfaces. Int. J. Oral. Maxillofac. Implants 2014, 29, 63–70. [Google Scholar] [CrossRef]
- De Tullio, I.; Berardini, M.; Di Iorio, D.; Perfetti, F.; Perfetti, G. Comparative evaluation among laser-treated, machined, and sandblasted/acid-etched implant surfaces: An in vivo histologic analysis on sheep. Int. J. Implant. Dent. 2020, 6, 7. [Google Scholar] [CrossRef]
- Kang, S.H.; Cho, S.A. Comparison of removal torques for laser-treated titanium implants with anodized implants. J. Craniofac Surg. 2011, 22, 1491–1495. [Google Scholar] [CrossRef]
- Mongardini, C.; Zeza, B.; Pelagalli, P.; Blasone, R.; Scilla, M.; Berardini, M. Radiographic bone level around particular laser-treated dental implants: 1 to 6 years multicenter retrospective study. Int. J. Implant. Dent. 2020, 6, 29. [Google Scholar] [CrossRef]
- Rong, M.; Lu, H.; Wan, L.; Zhang, X.; Lin, X.; Li, S.; Zhou, L.; Lv, Y.; Su, Y. Comparison of early osseointegration between laser-treated/acid-etched and sandblasted/acid-etched titanium implant surfaces. J. Mater. Sci. Mater. Med. 2018, 29, 43. [Google Scholar] [CrossRef]
- Baltriukienė, D.; Sabaliauskas, V.; Balčiūnas, E.; Melninkaitis, A.; Liutkevičius, E.; Bukelskienė, V.; Rutkūnas, V. The effect of laser-treated titanium surface on human gingival fibroblast behavior. J. Biomed. Mater. Res. A 2014, 102, 713–720. [Google Scholar] [CrossRef]
- Prodanov, L.; Lamers, E.; Wolke, J.; Huiberts, R.; Jansen, J.A.; Walboomers, X.F. In vivo comparison between laser-treated and grit blasted/acid etched titanium. Clin. Oral. Implants Res. 2014, 25, 234–239. [Google Scholar] [CrossRef]
- Ionescu, A.C.; Brambilla, E.; Azzola, F.; Ottobelli, M.; Pellegrini, G.; Francetti, L.A. Laser microtextured titanium implant surfaces reduce in vitro and in situ oral biofilm formation. PLoS ONE 2018, 13, e0202262. [Google Scholar] [CrossRef]
- Sun, Y.; Sun, J.; Wu, X.W.; Li, Y.; Li, X.Y.; Li, R.X.; Wang, T.; Bi, W.; Cui, W.G.; Yu, Y.C. Mechanism of zirconia microgroove surface structure for osseointegration. Mater. Today Adv. 2021, 12, 100159. [Google Scholar] [CrossRef]
- Chu, S.F.; Huang, M.T.; Ou, K.L.; Sugiatno, E.; Cheng, H.Y.; Huang, Y.H.; Chiu, W.T.; Liou, T.H. Enhanced biocompatible and hemocompatible nano/micro porous surface as a biological scaffold for functionalizational and biointegrated implants. J. Alloys Compd. 2016, 684, 726–732. [Google Scholar] [CrossRef]
- Mwenifumbo, S.; Li, M.; Chen, J.; Beye, A.; Soboyejo, W. Cell/surface interactions on laser micro-textured titanium-coated silicon surfaces. J. Mater. Sci. Mater. Med. 2007, 18, 9–23. [Google Scholar] [CrossRef]
- Chen, X.; Macica, C.M.; Ng, K.W.; Broadus, A.E. Stretch-induced PTH-related protein gene expression in osteoblasts. J. Bone Miner. Res. 2005, 20, 1454–1461. [Google Scholar] [CrossRef]
- Berardi, D.; Colagiovanni, M.; Scoccia, A.; Raffaelli, L.; Manicone, P.F.; Perfetti, G. Evaluation of a new laser surface implant: Scanning electron microscopy/energy dispersive X-ray and X-ray photoelectron spectroscopy analyses. J. Biol. Regul. Homeost. Agents 2008, 22, 161–167. [Google Scholar]
- Wang, R.; Ni, S.; Ma, L.; Li, M. Porous construction and surface modification of titanium-based materials for osteogenesis: A review. Front. Bioeng. Biotechnol. 2022, 10, 973297. [Google Scholar] [CrossRef]
- Mochida, Y.; Parisuthiman, D.; Pornprasertsuk-Damrongsri, S.; Atsawasuwan, P.; Sricholpech, M.; Boskey, A.L.; Yamauchi, M. Decorin modulates collagen matrix assembly and mineralization. Matrix Biol. 2009, 28, 44–52. [Google Scholar] [CrossRef]
- Zhang, W.; Ge, Y.; Cheng, Q.; Zhang, Q.; Fang, L.; Zheng, J. Decorin is a pivotal effector in the extracellular matrix and tumour microenvironment. Oncotarget 2018, 9, 5480–5491. [Google Scholar] [CrossRef]
- Cawley, K.M.; Bustamante-Gomez, N.C.; Guha, A.G.; MacLeod, R.S.; Xiong, J.; Gubrij, I.; Liu, Y.; Mulkey, R.; Palmieri, M.; Thostenson, J.D.; et al. Local production of osteoprotegerin by osteoblasts suppresses bone resorption. Cell Rep. 2020, 32, 108052. [Google Scholar] [CrossRef]
- Tang, L.L.; Xian, C.Y.; Wang, Y.L. The MGF expression of osteoblasts in response to mechanical overload. Arch. Oral. Biol. 2006, 51, 1080–1085. [Google Scholar] [CrossRef]
- Dalagiorgou, G.; Piperi, C.; Adamopoulos, C.; Georgopoulou, U.; Gargalionis, A.N.; Spyropoulou, A.; Zoi, I.; Nokhbehsaim, M.; Damanaki, A.; Deschner, J.; et al. Mechanosensor polycystin-1 potentiates differentiation of human osteoblastic cells by upregulating Runx2 expression via induction of JAK2/STAT3 signaling axis. Cell Mol. Life Sci. 2017, 74, 921–936. [Google Scholar] [CrossRef]
- Hasan, J.; Bright, R.; Hayles, A.; Palms, D.; Zilm, P.; Barker, D.; Vasilev, K. Preventing Peri-implantitis: The Quest for a Next Generation of Titanium Dental Implants. ACS Biomater. Sci. Eng. 2022, 8, 4697–4737. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gene Name | Forward | Reverse |
|---|---|---|
| COL1A1 | GATTCCCTGGACCTAAAGGTGC | AGCCTCTCCATCTTTGCCAGCA |
| DCN | AGCTGAAGGAATTGCCAGAA | CTCTGCTGATTTTGTTGCCA |
| TNFRSF11B | GAACCCCAGAGCGAAATAC | CGCTGTTTTCACAGAGGTC |
| SPP1 | CGAGGTGATAGTGTGGTTTATGG | GCACCATTCAACTCCTCGCTTTC |
| GAPDH | GTCTCCTCTGACTTCAACAGCG | ACCACCCTGTTGCTGTAGCCAA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.-W.; Chiang, T.; Chen, I.-H.; Yuh, D.-Y.; Tseng, H.-Y.; Wang, C.-W.; Hou, H.-H. Titanium Surfaces with a Laser-Produced Microchannel Structure Enhance Pre-Osteoblast Proliferation, Maturation, and Extracellular Mineralization In Vitro. Int. J. Mol. Sci. 2024, 25, 3388. https://doi.org/10.3390/ijms25063388
Chen Y-W, Chiang T, Chen I-H, Yuh D-Y, Tseng H-Y, Wang C-W, Hou H-H. Titanium Surfaces with a Laser-Produced Microchannel Structure Enhance Pre-Osteoblast Proliferation, Maturation, and Extracellular Mineralization In Vitro. International Journal of Molecular Sciences. 2024; 25(6):3388. https://doi.org/10.3390/ijms25063388
Chicago/Turabian StyleChen, Yi-Wen, Tao Chiang, I-Hui Chen, Da-Yo Yuh, Hsiu-Yang Tseng, Chuang-Wei Wang, and Hsin-Han Hou. 2024. "Titanium Surfaces with a Laser-Produced Microchannel Structure Enhance Pre-Osteoblast Proliferation, Maturation, and Extracellular Mineralization In Vitro" International Journal of Molecular Sciences 25, no. 6: 3388. https://doi.org/10.3390/ijms25063388
APA StyleChen, Y.-W., Chiang, T., Chen, I.-H., Yuh, D.-Y., Tseng, H.-Y., Wang, C.-W., & Hou, H.-H. (2024). Titanium Surfaces with a Laser-Produced Microchannel Structure Enhance Pre-Osteoblast Proliferation, Maturation, and Extracellular Mineralization In Vitro. International Journal of Molecular Sciences, 25(6), 3388. https://doi.org/10.3390/ijms25063388