
Identification of Genetic Variants for Risk Prediction and Early Diagnosis of Age-Related Macular Degeneration in the Taiwanese Population

 ,
,  , ,
, ,
Abstract
1. Introduction
2. Results
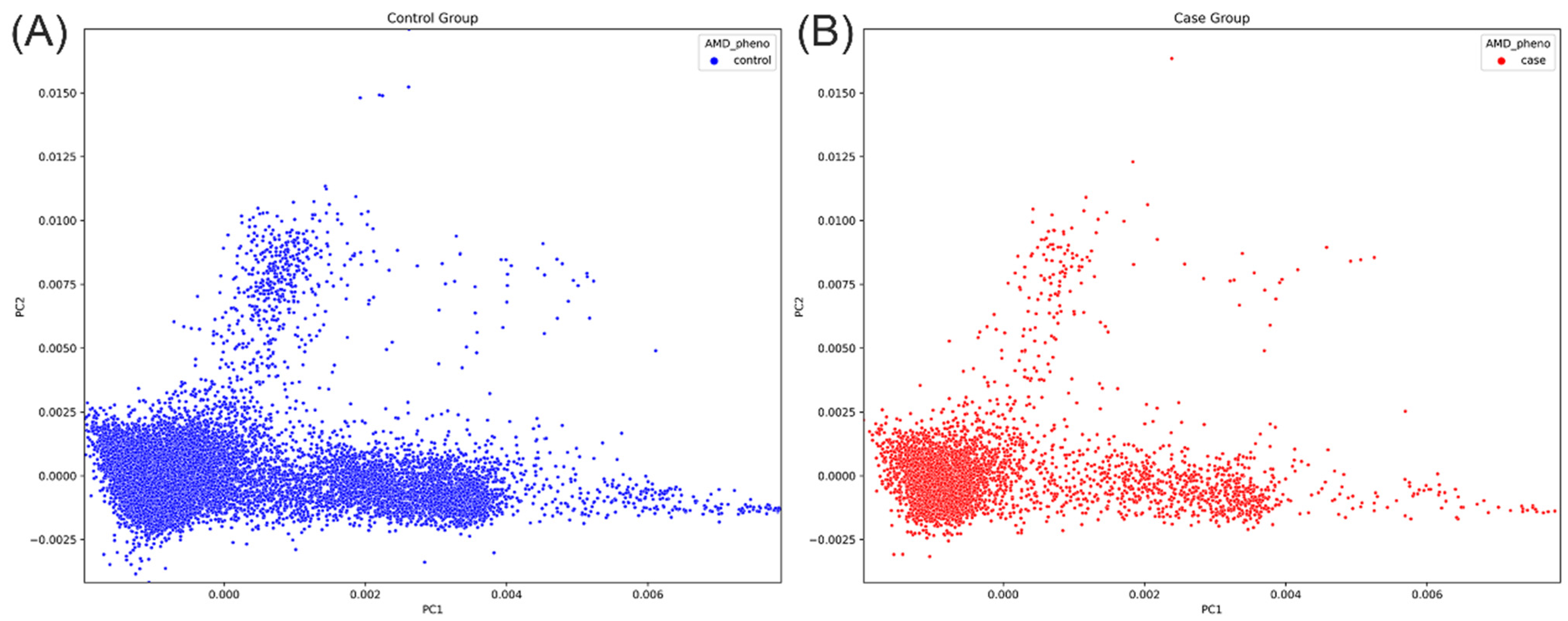
2.1. Characteristics of the Study Population
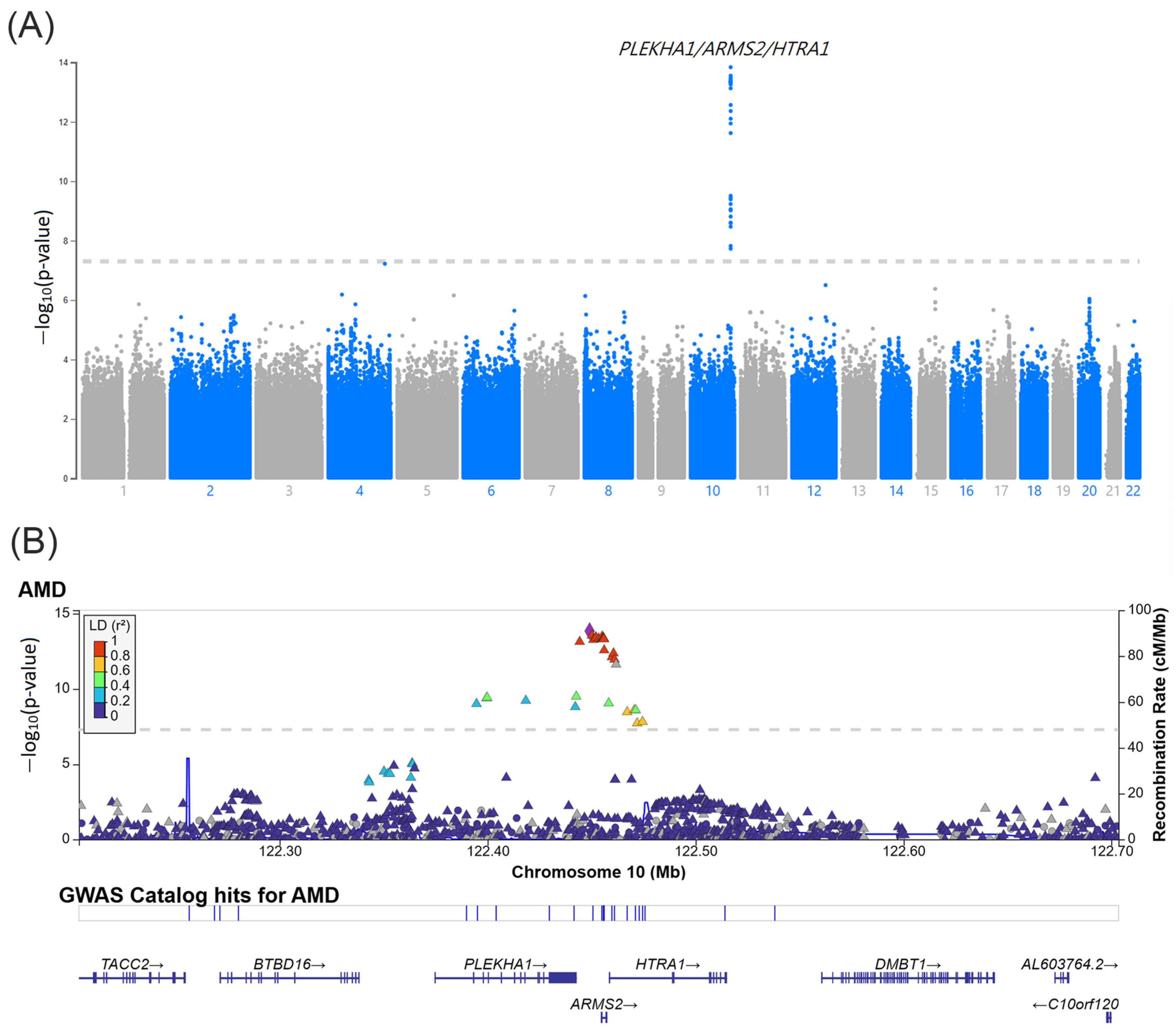
2.2. GWAS for Identifying AMD-Associated SNPs
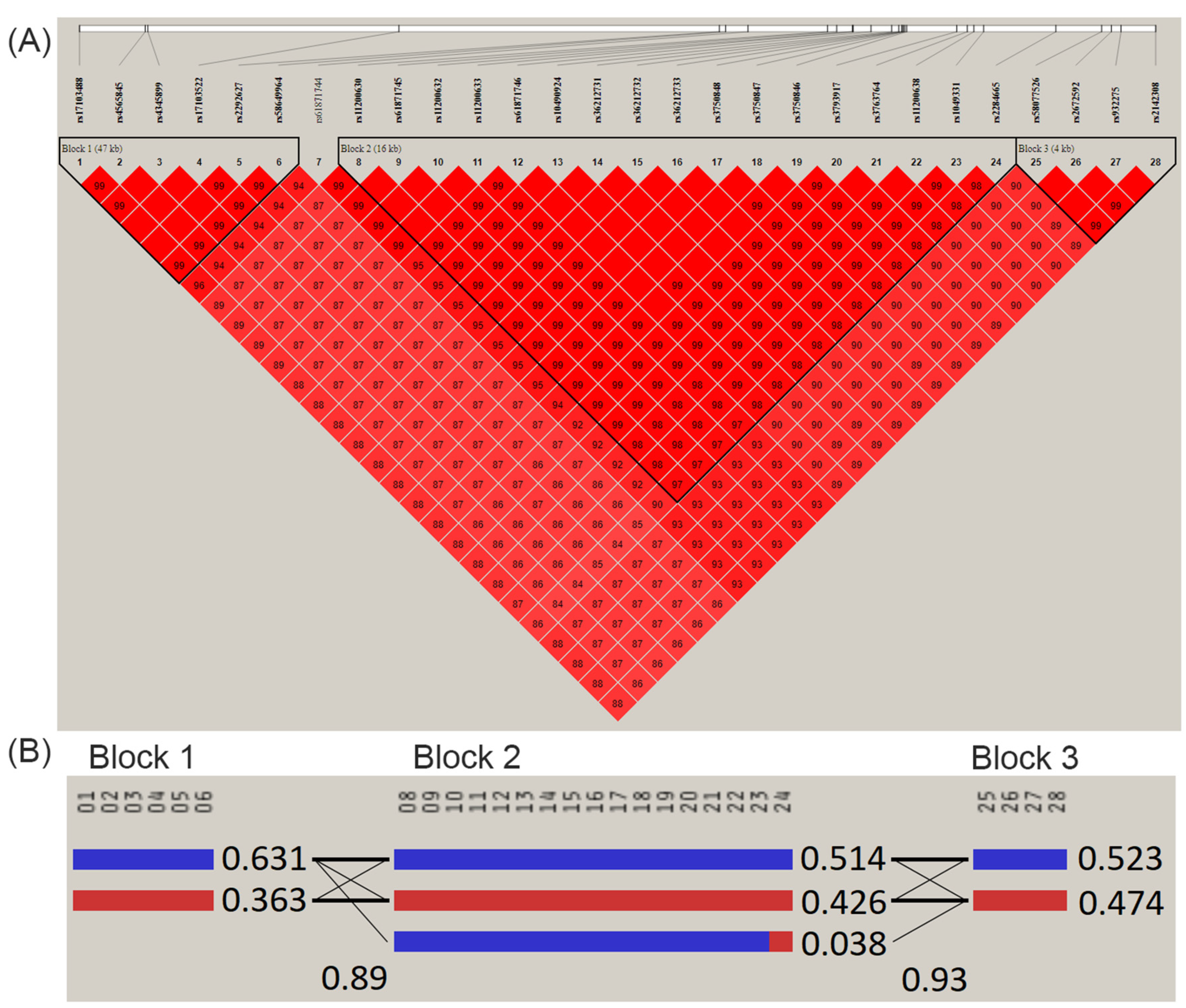
2.3. Linkage Disequilibrium and Haplotype Block Analyses
2.4. PRS for AMD Construction
2.5. Genetic Factors and PRS Predict the Risk of AMD Development
2.6. Performance of AMD Prediction Models
2.7. Association between PRS and Age at AMD Diagnosis
3. Discussion
4. Materials and Methods
4.1. Data Source
4.2. Study Population
4.3. Genotyping and Discovery GWAS
4.4. PRS Construction
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bourne, R.R.; Stevens, G.A.; White, R.A.; Smith, J.L.; Flaxman, S.R.; Price, H.; Jonas, J.B.; Keeffe, J.; Leasher, J.; Naidoo, K.; et al. Causes of vision loss worldwide, 1990–2010: A systematic analysis. Lancet Glob. Health 2013, 1, e339–e349. [Google Scholar] [CrossRef]
- Mitchell, P.; Liew, G.; Gopinath, B.; Wong, T.Y. Age-related macular degeneration. Lancet 2018, 392, 1147–1159. [Google Scholar] [CrossRef]
- Lim, L.S.; Mirza, R.G.; Gill, M.K. Age-related macular degeneration. Lancet 2012, 379, 1728–1738. [Google Scholar] [CrossRef]
- Rattner, A.; Nathans, J. Macular degeneration: Recent advances and therapeutic opportunities. Nat. Rev. Neurosci. 2006, 7, 860–872. [Google Scholar] [CrossRef]
- Jin, G.; Zou, M.; Chen, A.; Zhang, Y.; Young, C.A.; Wang, S.; Zheng, D. Prevalence of age-related macular degeneration in Chinese populations worldwide: A systematic review and meta-analysis. Clin. Exp. Ophthalmol. 2019, 47, 1019–1027. [Google Scholar] [CrossRef]
- Kawasaki, R.; Yasuda, M.; Song, S.J.; Chen, S.-J.; Jonas, J.B.; Wang, J.J.; Mitchell, P.; Wong, T.Y. The prevalence of age-related macular degeneration in Asians: A systematic review and meta-analysis. Ophthalmology 2010, 117, 921–927. [Google Scholar] [CrossRef]
- Klein, R.; Klein, B.E.; Knudtson, M.D.; Wong, T.Y.; Cotch, M.F.; Liu, K.; Burke, G.; Saad, M.F.; Jacobs, D.R. Prevalence of age-related macular degeneration in 4 racial/ethnic groups in the multi-ethnic study of atherosclerosis. Ophthalmology 2006, 113, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Fleckenstein, M.; Keenan, T.D.; Guymer, R.H.; Chakravarthy, U.; Schmitz-Valckenberg, S.; Klaver, C.C.; Wong, W.T.; Chew, E.Y. Age-related macular degeneration. Nat. Rev. Dis. Primers 2021, 7, 1728–1738. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.-J.; Cheng, C.-Y.; Peng, K.-L.; Li, A.-F.; Hsu, W.-M.; Liu, J.-H.; Chou, P. Prevalence and associated risk factors of age-related macular degeneration in an elderly Chinese population in Taiwan: The Shihpai Eye Study. Investig. Opthalmol. Vis. Sci. 2008, 49, 3126–3133. [Google Scholar] [CrossRef] [PubMed]
- Seddon, J.M.; Cote, J.; Davis, N.; Rosner, B. Progression of age-related macular degeneration: Association with body mass index, waist circumference, and waist-hip ratio. Arch. Ophthalmol. 2003, 121, 785–792. [Google Scholar] [CrossRef] [PubMed]
- Velilla, S.; García-Medina, J.J.; García-Layana, A.; Dolz-Marco, R.; Pons-Vázquez, S.; Pinazo-Durán, M.D.; Gómez-Ulla, F.; Arévalo, J.F.; Díaz-Llopis, M.; Gallego-Pinazo, R. Smoking and Age-Related Macular Degeneration: Review and Update. J. Ophthalmol. 2013, 2013, 895147. [Google Scholar] [CrossRef]
- Seddon, J.M.; Willett, W.C.; Speizer, F.E.; Hankinson, S.E. A prospective study of cigarette smoking and age-related macular degeneration in women. JAMA 1996, 276, 1141–1146. [Google Scholar] [CrossRef]
- Seddon, J.M.; Cote, J.; Page, W.F.; Aggen, S.H.; Neale, M.C. The US twin study of age-related macular degeneration: Relative roles of genetic and environmental influences. Arch. Ophthalmol. 2005, 123, 321–327. [Google Scholar] [CrossRef]
- Grizzard, W.S.; Arnett, D.; Haag, S.L. Twin study of age-related macular degeneration. Ophthalmic Epidemiol. 2003, 10, 315–322. [Google Scholar] [CrossRef] [PubMed]
- Meyers, S.M. A twin study on age-related macular degeneration. Trans. Am. Ophthalmol. Soc. 1994, 92, 775–843. [Google Scholar] [CrossRef] [PubMed]
- Fritsche, L.G.; Igl, W.; Bailey, J.N.C.; Grassmann, F.; Sengupta, S.; Bragg-Gresham, J.L.; Burdon, K.P.; Hebbring, S.J.; Wen, C.; Gorski, M.; et al. A large genome-wide association study of age-related macular degeneration highlights contributions of rare and common variants. Nat. Genet. 2016, 48, 134–143. [Google Scholar] [CrossRef]
- Buitendijk, G.H.S.; Rochtchina, E.; Myers, C.; van Duijn, C.M.; Lee, K.E.; Klein, B.E.; Meuer, S.M.; de Jong, P.T.; Holliday, E.G.; Tan, A.G.; et al. Prediction of age-related macular degeneration in the general population: The Three Continent AMD Consortium. Ophthalmology 2013, 120, 2644–2655. [Google Scholar] [CrossRef] [PubMed]
- He, W.; Han, X.; Ong, J.-S.; Wu, Y.; Hewitt, A.W.; Mackey, D.A.; Gharahkhani, P.; MacGregor, S. Genome-Wide Meta-analysis Identifies Risk Loci and Improves Disease Prediction of Age-Related Macular Degeneration. Ophthalmology 2024, 131, 16–29. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.Y.; Yamashiro, K.; Jia Chen, L.; Ahn, J.; Huang, L.; Huang, L.; Cheung, C.M.G.; Miyake, M.; Cackett, P.D.; Yeo, I.Y.; et al. New loci and coding variants confer risk for age-related macular degeneration in East Asians. Nat. Commun. 2015, 6, 6063. [Google Scholar] [CrossRef] [PubMed]
- Laude, A.; Cackett, P.D.; Vithana, E.N.; Yeo, I.Y.; Wong, D.; Koh, A.H.; Wong, T.Y.; Aung, T. Polypoidal choroidal vasculopathy and neovascular age-related macular degeneration: Same or different disease? Prog. Retin. Eye Res. 2010, 29, 19–29. [Google Scholar] [CrossRef] [PubMed]
- Shih, C.-H.; Chuang, H.-K.; Hsiao, T.-H.; Yang, Y.-P.; Gao, C.-E.; Chiou, S.-H.; Hsu, C.-C.; Hwang, D.-K. Genome-wide association study and identification of systemic comorbidities in development of age-related macular degeneration in a hospital-based cohort of Han Chinese. Front. Genet. 2023, 14, 1064659. [Google Scholar] [CrossRef] [PubMed]
- Kondo, N.; Bessho, H.; Honda, S.; Negi, A. Complement factor H Y402H variant and risk of age-related macular degeneration in Asians: A systematic review and meta-analysis. Ophthalmology 2011, 118, 339–344. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.-M.; Wan, L.; Tsai, Y.-Y.; Lin, H.-J.; Tsai, Y.; Lee, C.-C.; Tsai, C.-H.; Tsai, F.-J.; Tseng, S.-H. HTRA1 polymorphism in dry and wet age-related macular degeneration. Retina 2008, 28, 309–313. [Google Scholar] [CrossRef] [PubMed]
- Williams, B.L.; Seager, N.A.; Gardiner, J.D.; Pappas, C.M.; Cronin, M.C.; Filippo, C.A.d.S.; Anstadt, R.A.; Liu, J.; Toso, M.A.; Nichols, L.; et al. Chromosome 10q26–driven age-related macular degeneration is associated with reduced levels of HTRA1 in human retinal pigment epithelium. Proc. Natl. Acad. Sci. USA 2021, 118, e2103617118. [Google Scholar] [CrossRef] [PubMed]
- Hageman, G.S.; Anderson, D.H.; Johnson, L.V.; Hancox, L.S.; Taiber, A.J.; Hardisty, L.I.; Hageman, J.L.; Stockman, H.A.; Borchardt, J.D.; Gehrs, K.M.; et al. A common haplotype in the complement regulatory gene factor H (HF1/CFH) predisposes individuals to age-related macular degeneration. Proc. Natl. Acad. Sci. USA 2005, 102, 7227–7232. [Google Scholar] [CrossRef] [PubMed]
- Jakobsdottir, J.; Conley, Y.P.; Weeks, D.E.; Mah, T.S.; Ferrell, R.E.; Gorin, M.B. Susceptibility genes for age-related maculopathy on chromosome 10q26. Am. J. Hum. Genet. 2005, 77, 389–407. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.-M.; Tsai, Y.-Y.; Wan, L.; Lin, H.-J.; Tsai, Y.; Lee, C.-C.; Tsai, C.-H.; Tsai, F.-J.; Tseng, S.-H. Complement factor H variant increases the risk for early age-related macular degeneration. Retina 2008, 28, 1416–1420. [Google Scholar] [CrossRef]
- Magnusson, K.P.; Duan, S.; Sigurdsson, H.; Petursson, H.; Yang, Z.; Zhao, Y.; Bernstein, P.S.; Ge, J.; Jonasson, F.; Stefansson, E.; et al. CFH Y402H confers similar risk of soft drusen and both forms of advanced AMD. PLoS Med. 2006, 3, e5. [Google Scholar] [CrossRef]
- Kim, J.E.; Tomkins-Netzer, O.; Elman, M.J.; Lally, D.R.; Goldstein, M.; Goldenberg, D.; Shulman, S.; Benyamini, G.; Loewenstein, A. Evaluation of a self-imaging SD-OCT system designed for remote home monitoring. BMC Ophthalmol. 2022, 22, 261. [Google Scholar] [CrossRef]
- Liu, T.-Y.; Lin, C.-F.; Wu, H.-T.; Wu, Y.-L.; Chen, Y.-C.; Liao, C.-C.; Chou, Y.-P.; Chao, D.; Lu, H.-F.; Chang, Y.-S.; et al. Comparison of multiple imputation algorithms and verification using whole-genome sequencing in the CMUH genetic biobank. Biomedicine 2021, 11, 57–65. [Google Scholar] [CrossRef]
- Chen, C.-H.; Yang, J.-H.; Chiang, C.W.K.; Hsiung, C.-N.; Wu, P.-E.; Chang, L.-C.; Chu, H.-W.; Chang, J.; Song, I.W.; Yang, S.-L.; et al. Population structure of Han Chinese in the modern Taiwanese population based on 10,000 participants in the Taiwan Biobank project. Hum. Mol. Genet. 2016, 25, 5321–5331. [Google Scholar] [CrossRef]
- Liao, W.-L.; Liu, T.-Y.; Cheng, C.-F.; Chou, Y.-P.; Wang, T.-Y.; Chang, Y.-W.; Chen, S.-Y.; Tsai, F.-J. Analysis of HLA Variants and Graves’ Disease and Its Comorbidities Using a High Resolution Imputation System to Examine Electronic Medical Health Records. Front. Endocrinol. 2022, 13, 842673. [Google Scholar] [CrossRef]
- Delaneau, O.; Zagury, J.-F.; Marchini, J. Improved whole-chromosome phasing for disease and population genetic studies. Nat. Methods 2013, 10, 5–6. [Google Scholar] [CrossRef]
- Howie, B.; Fuchsberger, C.; Stephens, M.; Marchini, J.; Abecasis, G.R. Fast and accurate genotype imputation in genome-wide association studies through pre-phasing. Nat. Genet. 2012, 44, 955–959. [Google Scholar] [CrossRef] [PubMed]
- Sudmant, P.H.; Rausch, T.; Gardner, E.J.; Handsaker, R.E.; Abyzov, A.; Huddleston, J.; Zhang, Y.; Ye, K.; Jun, G.; Fritz, M.H.-Y.; et al. An integrated map of structural variation in 2504 human genomes. Nature 2015, 526, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.W.; O’Reilly, P.F. PRSice-2: Polygenic Risk Score software for biobank-scale data. GigaScience 2019, 8, giz082. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.C.; Chow, C.C.; Tellier, L.C.; Vattikuti, S.; Purcell, S.M.; Lee, J.J. Second-generation PLINK: Rising to the challenge of larger and richer datasets. GigaScience 2015, 4, s13742-015. [Google Scholar] [CrossRef]
- Barrett, J.C.; Fry, B.; Maller, J.; Daly, M.J. Haploview: Analysis and visualization of LD and haplotype maps. Bioinformatics 2005, 21, 263–265. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Discovery Cohort (n = 14,343) | Replication Cohort (n = 6146) | |||
|---|---|---|---|---|
| Control Participants | AMD Patients | Control Participants | AMD Patients | |
| Sample size | 2827 | 1212 | ||
| Dry type (%) Wet type (%) | 11,514 | 1980 (70.0) 847 (30.0) | 4934 | 865 (71.4) 347 (28.6) |
| Age (yrs, mean ± SD) | 74.3 ± 7.3 | 74.7 ± 10.1 69.8 ± 9.7 1 | 74.3 ± 7.3 | 74.9 ± 10.4 69.6 ± 10.0 1 |
| Sex | ||||
| Male (%) Female (%) | 5121 (44.5) 6393 (55.5) | 1376 (48.7) ** 1451 (51.3) | 2183 (44.2) 2751 (55.8) | 603 (49.8) * 609 (50.2) |
| BMI (kg/m2) 2 | ||||
| ≤25 (%) >25 (%) | 5719 (55.6) 4573 (44.4) | 1446 (56.3) 1124 (43.7) | 2390 (53.8) 2054 (46.2) | 617 (56.6) 473 (43.3) |
| Smoking status 2 | ||||
| Smoking (%) Non-smoking (%) | 894 (9.2) 8815 (90.8) | 246 (10.1) 2193 (89.9) | 392 (9.3) 3813 (90.7) | 102 (9.9) 928 (90.1) |
| Haplotype Block Pattern | Haplotype Frequency | p Value | |
|---|---|---|---|
| AMD Cases | Non-AMD Controls | ||
| Block 1 1 | |||
| TACTTT | 0.590 | 0.641 | 2.26 × 10−16 |
| CCTCGA | 0.404 | 0.353 | 2.23 × 10−16 |
| Block 2 2 | |||
| TGACTGGATTCTCAGCG | 0.473 | 0.524 | 1.42 × 10−16 |
| CAGTCTTGCGTCGGATT | 0.475 | 0.415 | 4.60 × 10−22 |
| TGACTGGATTCTCAGCT | 0.033 | 0.039 | 0.009 |
| Block 3 3 | |||
| AGGG | 0.482 | 0.533 | 3.87 × 10−15 |
| CTAC | 0.515 | 0.463 | 1.75 × 10−15 |
| Adjusted Odds Ratio (95% CI), p Value 1 | |||
|---|---|---|---|
| Overall AMD | Dry AMD | Wet AMD | |
| Model 1 rs11200630 (per risk allele C) | 1.31 (1.20–1.43) p < 0.001 | 1.22 (1.10–1.35) p < 0.001 | 1.55 (1.33–1.81) p < 0.001 |
| Model 2 PRS_1412 SNP (The top 5% vs. the bottom quartile) | 1.40 (1.04–1.89) p = 0.025 | 1.46 (1.04–2.04) p = 0.028 | 1.28 (0.76–2.13) p = 0.353 |
| AUC (95% CI), p-Value | |||
|---|---|---|---|
| Overall AMD | Dry AMD | Wet AMD | |
| Covariates 1 | 0.646 (0.625–0.668), p <0.001) | 0.646 (0.621–0.670), p < 0.001 | 0.656 (0.617–0.695), p < 0.001 |
| Model 1 (rs11200630) | |||
| SNP only | 0.549 (0.531–0.568), p <0.001) | 0.537 (0.516–0.558), p = 0.001 | 0.580 (0.547–0.613), p < 0.001 |
| SNP + covariates | 0.662 (0.641–0.683), p <0.001) | 0.654 (0.629–0.679), p < 0.001 | 0.692 (0.656–0.728), p < 0.001 |
| Model 2 (PRS_1412 SNP) | |||
| PRS only | 0.511 (0.493–0.529), p = 0.225) | 0.507 (0.486–0.528), p = 0.499 | 0.521 (0.490–0.552), p = 0.183 |
| PRS + covariates | 0.648 (0.627–0.670), p < 0.001 | 0.648 (0.627–0.670), p < 0.001 | 0.659 (0.620–0.698), p < 0.001 |
| Multivariable Analysis | Beta (95% CI) 1 | p Value 1 |
|---|---|---|
| Variable | ||
| PRS quartile | −0.62 (−1.15, −0.09) | 0.023 |
| Smoking status Smoking vs. non-smoking | −6.95 (−13.6, −0.34) | 0.039 |
| Sex Male vs. female | 0.24 (−1.01, 1.48) | 0.706 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, Y.-C.; Liao, W.-L.; Lin, H.-J.; Huang, Y.-T.; Chang, Y.-W.; Liu, T.-Y.; Chen, Y.-C.; Weng, A.L.; Tsai, F.-J. Identification of Genetic Variants for Risk Prediction and Early Diagnosis of Age-Related Macular Degeneration in the Taiwanese Population. Int. J. Mol. Sci. 2024, 25, 3230. https://doi.org/10.3390/ijms25063230
Huang Y-C, Liao W-L, Lin H-J, Huang Y-T, Chang Y-W, Liu T-Y, Chen Y-C, Weng AL, Tsai F-J. Identification of Genetic Variants for Risk Prediction and Early Diagnosis of Age-Related Macular Degeneration in the Taiwanese Population. International Journal of Molecular Sciences. 2024; 25(6):3230. https://doi.org/10.3390/ijms25063230
Chicago/Turabian StyleHuang, Yu-Chuen, Wen-Ling Liao, Hui-Ju Lin, Yu-Te Huang, Ya-Wen Chang, Ting-Yuan Liu, Yu-Chia Chen, Angel L. Weng, and Fuu-Jen Tsai. 2024. "Identification of Genetic Variants for Risk Prediction and Early Diagnosis of Age-Related Macular Degeneration in the Taiwanese Population" International Journal of Molecular Sciences 25, no. 6: 3230. https://doi.org/10.3390/ijms25063230
APA StyleHuang, Y.-C., Liao, W.-L., Lin, H.-J., Huang, Y.-T., Chang, Y.-W., Liu, T.-Y., Chen, Y.-C., Weng, A. L., & Tsai, F.-J. (2024). Identification of Genetic Variants for Risk Prediction and Early Diagnosis of Age-Related Macular Degeneration in the Taiwanese Population. International Journal of Molecular Sciences, 25(6), 3230. https://doi.org/10.3390/ijms25063230