
Intradermal Injection of Hybrid Complexes of High- and Low-Molecular-Weight Hyaluronan: Where Do We Stand and Where Are We Headed in Regenerative Medicine?

Abstract
1. Introduction: Pleiotropic Signalling of Hyaluronan in Cell Biology and Molecular Weight Specificity
2. NAHYCO® Hybrid Technology
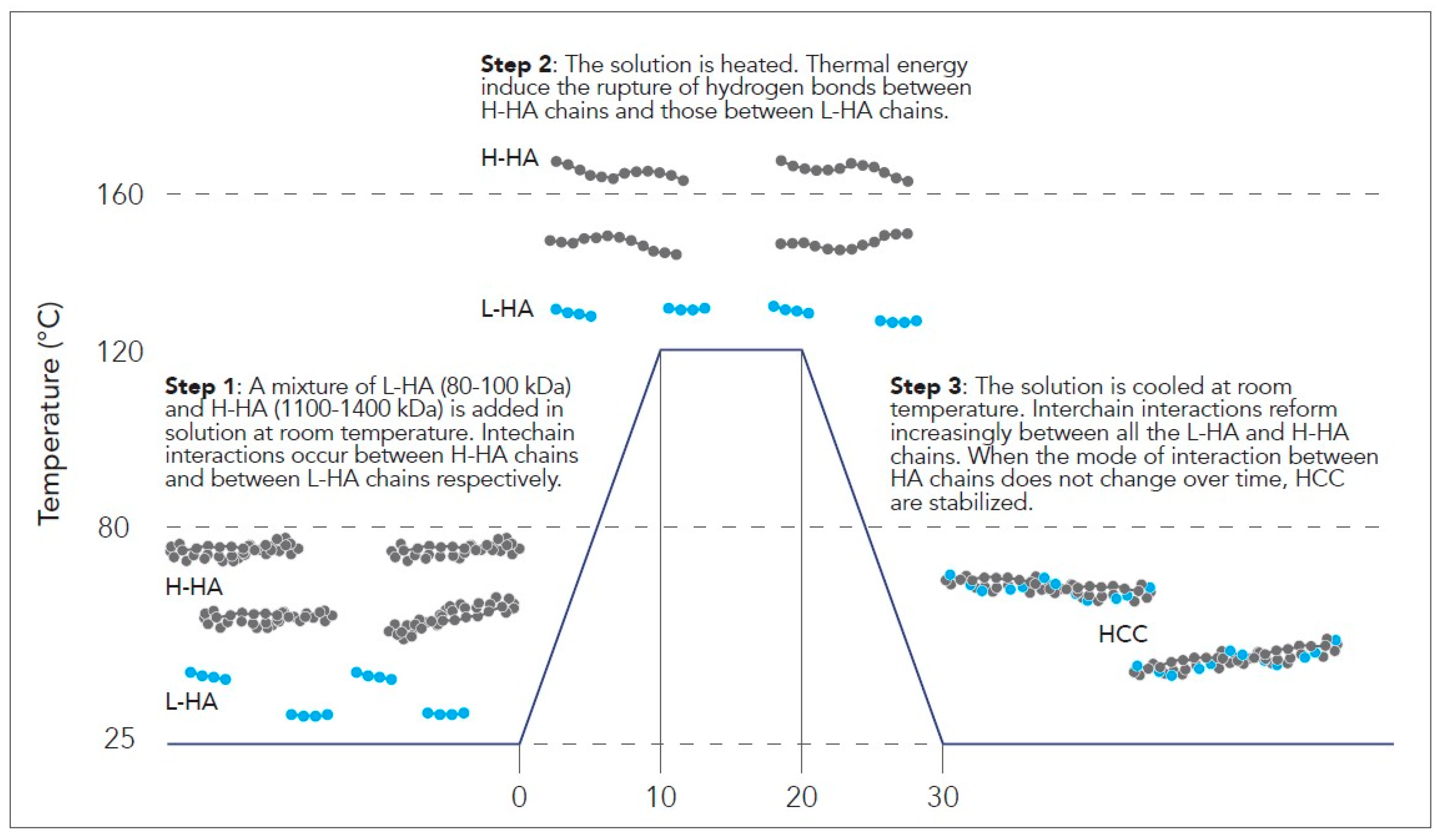
2.1. Creation of Hybrid Cooperative Hyaluronic Acid Complexes
2.2. Hydrolytic Degradation and Mechanical Stability
3. The Functional Impact of HCCs: In Vitro Studies
3.1. Epidermic and Dermic Layers
3.2. Subcutaneous Tissue
4. Medical Aesthetics Applications
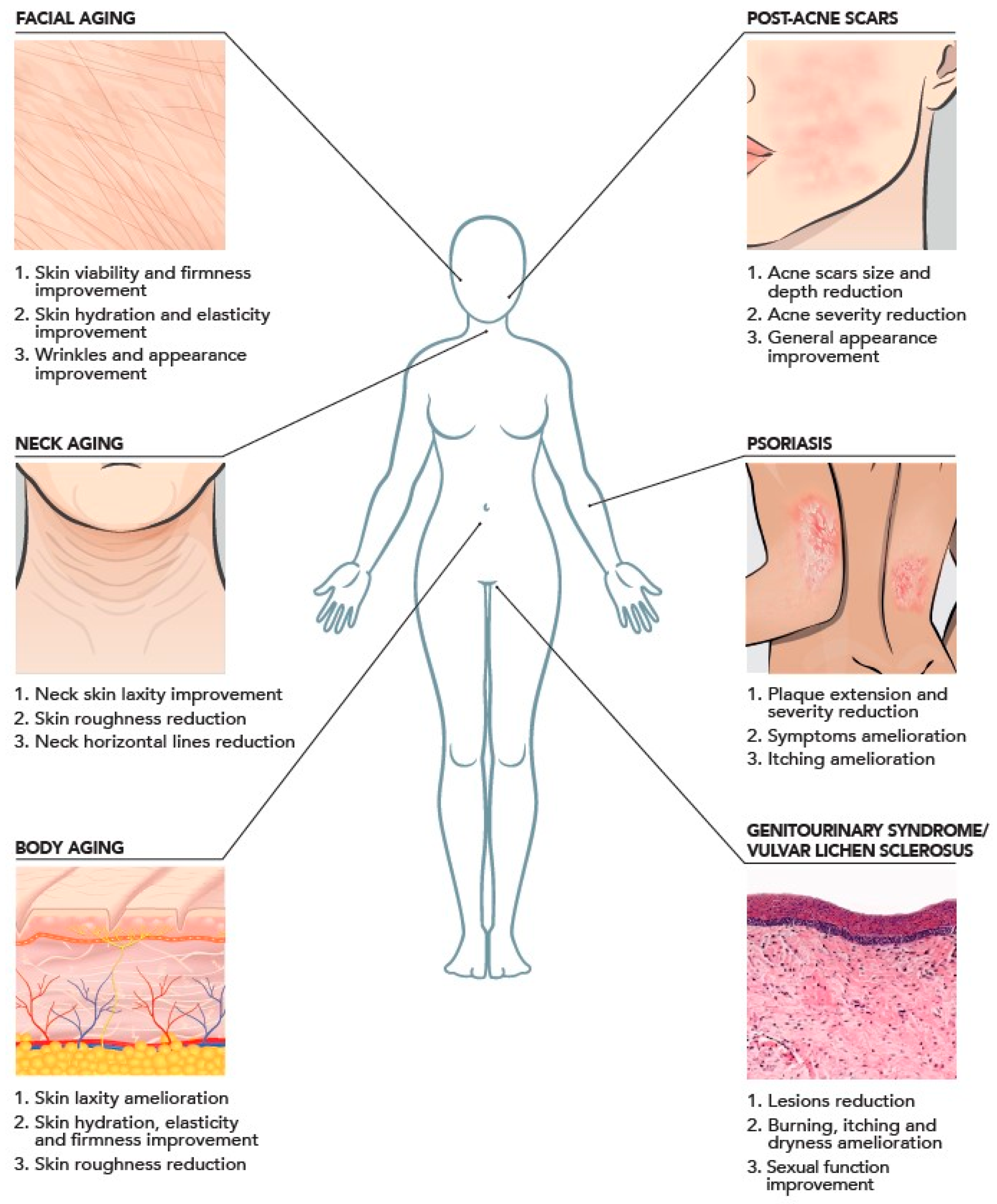
4.1. Face
4.2. Neck
4.3. Body
5. Role in Regenerative Medicine
5.1. Regenerative Medicine and Treatment Approaches
5.2. Future Perspectives of HCCs in Regenerative Medicine
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Abruzzese, F.; Basoli, F.; Constantini, M.; Giannitelli, S.; Gori, M.; Mozetic, P.; Rainer, A.; Trombetta, M. Hyaluronan: An Overview. J. Biol. Regul. Homeost. Agents 2017, 31 (4 Suppl. 2), 9–22. [Google Scholar]
- Maytin, E.V. Hyaluronan: More than Just a Wrinkle Filler. Glycobiology 2016, 26, 553–559. [Google Scholar] [CrossRef]
- Gilbert, E.; Hui, A.; Meehan, S.; Waldorf, H.A. The Basic Science of Dermal Fillers: Past and Present Part II: Adverse Effects. J. Drugs Dermatol. 2012, 11, 1069–1076. [Google Scholar]
- Stern, R. Hyaluronan Catabolism: A New Metabolic Pathway. Eur. J. Cell Biol. 2004, 83, 317–325. [Google Scholar] [CrossRef]
- Litwiniuk, M.; Krejner, A.; Grzela, T. Hyaluronic Acid in Inflammation and Tissue Regeneration|Wounds Research. Wounds 2016, 28, 78–88. [Google Scholar] [PubMed]
- Tavianatou, A.G.; Piperigkou, Z.; Barbera, C.; Beninatto, R.; Masola, V.; Caon, I.; Onisto, M.; Franchi, M.; Galesso, D.; Karamanos, N.K. Molecular Size-Dependent Specificity of Hyaluronan on Functional Properties, Morphology and Matrix Composition of Mammary Cancer Cells. Matrix Biol. Plus 2019, 3, 100008. [Google Scholar] [CrossRef] [PubMed]
- Tavianatou, A.G.; Caon, I.; Franchi, M.; Piperigkou, Z.; Galesso, D.; Karamanos, N.K. Hyaluronan: Molecular Size-Dependent Signaling and Biological Functions in Inflammation and Cancer. FEBS J. 2019, 286, 2883–2908. [Google Scholar] [CrossRef]
- Berdiaki, A.; Neagu, M.; Spyridaki, I.; Kuskov, A.; Perez, S.; Nikitovic, D. Hyaluronan and Reactive Oxygen Species Signaling—Novel Cues from the Matrix? Antioxidants 2023, 12, 824. [Google Scholar] [CrossRef] [PubMed]
- Abatangelo, G.; Vindigni, V.; Avruscio, G.; Pandis, L.; Brun, P. Hyaluronic Acid: Redefining Its Role. Cells 2020, 9, 1743. [Google Scholar] [CrossRef]
- Kobayashi, T.; Chanmee, T.; Itano, N. Hyaluronan: Metabolism and Function. Biomolecules 2020, 10, 1525. [Google Scholar] [CrossRef]
- Humzah, D.; Romagnoli, M.; Tateo, A.; Bellia, G. Hyaluronic Acid: A Strategic Molecule for Rejuvenating Procedures. Esperienze Dermatol. 2020, 22, 36–41. [Google Scholar] [CrossRef]
- Meyer, L.J.M.; Stern, R. Age-Dependent Changes of Hyaluronan in Human Skin. J. Investig. Dermatol. 1994, 102, 385–389. [Google Scholar] [CrossRef]
- Papakonstantinou, E.; Roth, M.; Karakiulakis, G. Hyaluronic Acid: A Key Molecule in Skin Aging. Dermatoendocrinology 2012, 4, 253–258. [Google Scholar] [CrossRef]
- Tzellos, T.G.; Klagas, I.; Vahtsevanos, K.; Triaridis, S.; Printza, A.; Kyrgidis, A.; Karakiulakis, G.; Zouboulis, C.C.; Papakonstantinou, E. Extrinsic Ageing in the Human Skin Is Associated with Alterations in the Expression of Hyaluronic Acid and Its Metabolizing Enzymes. Exp. Dermatol. 2009, 18, 1028–1035. [Google Scholar] [CrossRef]
- Cassuto, D.; Bellia, G.; Schiraldi, C. An Overview of Soft Tissue Fillers for Cosmetic Dermatology: From Filling to Regenerative Medicine. Clin. Cosmet. Investig. Dermatol. 2021, 14, 1857–1866. [Google Scholar] [CrossRef]
- Giubertoni, G.; Koenderink, G.H.; Bakker, H.J. Direct Observation of Intrachain Hydrogen Bonds in Aqueous Hyaluronan. J. Phys. Chem. A 2019, 123, 8220–8225. [Google Scholar] [CrossRef]
- Dong, Q.; Guo, X.; Li, L.; Yu, C.; Nie, L.; Tian, W.; Zhang, H.; Huang, S.; Zang, H. Understanding hyaluronic acid induced variation of water structure by near-infrared spectroscopy. Sci. Rep. 2020, 10, 1387. [Google Scholar] [CrossRef]
- Snetkov, P.; Zakharova, K.; Morozkina, S.; Olekhnovich, R.; Uspenskaya, M. Hyaluronic Acid: The Influence of Molecular Weight on Structural, Physical, Physico-Chemical, and Degradable Properties of Biopolymer. Polymers 2020, 12, 1800. [Google Scholar] [CrossRef] [PubMed]
- Stellavato, A.; Corsuto, L.; D’Agostino, A.; La Gatta, A.; Diana, P.; Bernini, P.; De Rosa, M.; Schiraldi, C. Hyaluronan Hybrid Cooperative Complexes as a Novel Frontier for Cellular Bioprocesses Re-Activation. PLoS ONE 2016, 11, e0163510. [Google Scholar] [CrossRef] [PubMed]
- Scrima, M.; Merola, F.; Vito, N.; Pacchioni, D.; Vecchi, G.; Melito, C.; Iorio, A.; Giori, A.M.; Ferravante, A. Elucidations on the Performance and Reversibility of Treatment with Hyaluronic Acid Based Dermal Fillers: In Vivo and in Vitro Approaches. Clin. Cosmet. Investig. Dermatol. 2022, 15, 2629. [Google Scholar] [CrossRef] [PubMed]
- Vassallo, V.; Di Meo, C.; Alessio, N.; La Gatta, A.; Ferraro, G.A.; Nicoletti, G.F.; Schiraldi, C. Highly Concentrated Stabilized Hybrid Complexes of Hyaluronic Acid: Rheological and Biological Assessment of Compatibility with Adipose Tissue and Derived Stromal Cells towards Regenerative Medicine. Int. J. Mol. Sci. 2024, 25, 2019. [Google Scholar] [CrossRef]
- D’Agostino, A.; Stellavato, A.; Busico, T.; Papa, A.; Tirino, V.; Papaccio, G.; La Gatta, A.; De Rosa, M.; Schiraldi, C. In Vitro Analysis of the Effects on Wound Healing of High- and Low-Molecular Weight Chains of Hyaluronan and Their Hybrid H-HA/L-HA Complexes. BMC Cell Biol. 2015, 16, 19. [Google Scholar] [CrossRef]
- Stellavato, A.; La Noce, M.; Corsuto, L.; Pirozzi, A.V.A.; De Rosa, M.; Papaccio, G.; Schiraldi, C.; Tirino, V. Hybrid Complexes of High and Low Molecular Weight Hyaluronans Highly Enhance Hascs Differentiation: Implication for Facial Bioremodeling. Cell. Physiol. Biochem. 2017, 44, 1078–1092. [Google Scholar] [CrossRef] [PubMed]
- Alessio, N.; Stellavato, A.; Squillaro, T.; Del Gaudio, S.; Di Bernardo, G.; Peluso, G.; De Rosa, M.; Schiraldi, C.; Galderisi, U. Hybrid Complexes of High and Low Molecular Weight Hyaluronan Delay in Vitro Replicative Senescence of Mesenchymal Stromal Cells: A Pilot Study for Future Therapeutic Application. Aging 2018, 10, 1575–1585. [Google Scholar] [CrossRef] [PubMed]
- Stellavato, A.; Abate, L.; Vassallo, V.; Donniacuo, M.; Rinaldi, B.; Schiraldi, C. An in Vitro Study to Assess the Effect of Hyaluronan-Based Gels on Muscle-Derived Cells: Highlighting a New Perspective in Regenerative Medicine. PLoS ONE 2020, 15, e0236164. [Google Scholar] [CrossRef] [PubMed]
- La Noce, M.; Stellavato, A.; Vassallo, V.; Cammarota, M.; Laino, L.; Desiderio, V.; Del Vecchio, V.; Nicoletti, G.F.; Tirino, V.; Papaccio, G.; et al. Hyaluronan-Based Gel Promotes Human Dental Pulp Stem Cells Bone Differentiation by Activating YAP/TAZ Pathway. Cells 2021, 10, 2899. [Google Scholar] [CrossRef]
- Bravo, B.; Correia, P.; Gonçalves Junior, J.E.; Sant’Anna, B.; Kerob, D. Benefits of topical hyaluronic acid for skin quality and signs of skin aging: From literature review to clinical evidence. Dermatol. Ther. 2022, 35, e15903. [Google Scholar] [CrossRef]
- Pieretti, G.; Rafaniello, C.; Fraenza, F.; Donniacuo, M.; Cuomo, R.; Lanzano, G.; Ciccarelli, F.; Capuano, A.; Nicoletti, G. Hyaluronic acid-based fillers in patients with autoimmune inflammatory diseases. J. Cosmet. Dermatol. 2023, 22, 2420–2423. [Google Scholar] [CrossRef]
- Agolli, E.; Diffidenti, B.; Di Zitti, N.; Massidda, E.; Patella, F.; Santerini, C.; Beatini, A.; Bianchini, M.; Bizzarri, S.; Camilleri, V.; et al. Hybrid Cooperative Complexes of High and Low Molecular Weight Hyaluronans (Profhilo®): Review of the Literature and Presentation of the VisionHA Project. Esperienze Dermatol. 2021, 20, 5–14. [Google Scholar] [CrossRef]
- Cassuto, D.; Delledonne, M.; Zaccaria, G.; Illiano, I.; Giori, A.M.; Bellia, G. Safety Assessment of High- and Low-Molecular-Weight Hyaluronans (Profhilo®) as Derived from Worldwide Postmarketing Data. Biomed. Res. Int. 2020, 2020, 8159047. [Google Scholar] [CrossRef]
- Laurino, C.; Palmieri, B.; Coacci, A. Efficacy, Safety, and Tolerance of a New Injection Technique for High- and Low-Molecular-Weight Hyaluronic Acid Hybrid Complexes. Eplasty 2015, 15, e46. [Google Scholar]
- Sparavigna, A.; Tenconi, B. Efficacy and Tolerance of an Injectable Medical Device Containing Stable Hybrid Cooperative Complexes of High- and Low-Molecular-Weight Hyaluronic Acid: A Monocentric 16 Weeks Open-Label Evaluation. Clin. Cosmet. Investig. Dermatol. 2016, 9, 297–305. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez Abascal, M.; Saldana Fernandez, M. Bio-Remodelación Facial Mediante Inyección Intradérmica de Un Complejo Híbrido Estabilizado de Ácido Hialurónico de Alto y Bajo Peso Molecular: Estudio Prospectivo En 30 Pacientes. Eur. Aesthetic Plast. Surg. J. 2015, 5, 123–131. [Google Scholar]
- Sparavigna, A. Long Term Efficacy and Tolerance Of High-And Low-Molecular-Weight Hyaluronans (Profhilo®) Intradermal Injections. J. Plast. Pathol. Dermatol. 2022, 18, 185–191. [Google Scholar]
- Goltsova, E.; Shemonaeva, O. Hybrid Cooperative Complexes of H-HA and L-HA (Profhilo®) and the BAP Technique for Facial Skin Bioremodeling: A Clinical Experience at the NEO-Clinic (Tyumen, Russia). Esperienze Dermatol. 2019, 21, 47–53. [Google Scholar] [CrossRef]
- Satardinova, E. Hybrid Cooperative Complexes of High and Low Molecular Weight Hyaluronans for Facial Skin Rejuvenation in the Oriental Mongoloid Face: A Case Series. Aesthetic Med. 2019, 5, 14–19. [Google Scholar]
- Sparavigna, A.; Lualdi, R.; Cicerone, M.; Giori, A.M.; Bellia, G. A Pilot Study Testing Efficacy and Tolerability of Hybrid Cooperative Complexes of Hyaluronic Acid Intradermal Injections in Chinese Women. Aesthetic Med. Plast. Surg. 2023, 1, 5–12. [Google Scholar]
- Sparavigna, A.; Cigni, C.; Grimolizzi, F.; Bellia, G. Neck and face rejuvenation outcomes with Profhilo®: A comparative analysis between Chinese and Caucasian cohorts. Gazz. Med. Ital.-Arch. Sci. Med. 2023, 182, 628–633. [Google Scholar] [CrossRef]
- Tateo, A.; Sofo, G. Optimization of the Lipofilling Procedure with Hybrid Cooperative Complexes of High and Low Molecular Weight Hyaluronic Acid: Preliminary Experiments. Esperienze Dermatol. 2019, 21, 22–28. [Google Scholar] [CrossRef]
- Sparavigna, A.; Grimolizzi, F.; Cigni, C.; Lualdi, R.; Bellia, G. Efficacy and tolerability of Profhilo® Structura intended to restore lateral cheek fat compartment: An observational pilot study. Health Sci. Rep. 2024, 7, e1743. [Google Scholar] [CrossRef]
- Cassuto, D.; Cigni, C.; Bellia, G.; Schiraldi, C. Restoring Adipose Tissue Homeostasis in Response to Aging: Initial Clinical Experience with Profhilo Structura®. Gels 2023, 9, 614. [Google Scholar] [CrossRef]
- Paganelli, A.; Mandel, V.D.; Pellacani, G.; Rossi, E. Synergic Effect of Plasma Exeresis and Non-Cross-Linked Low and High Molecular Weight Hyaluronic Acid to Improve Neck Skin Laxities. J. Cosmet. Dermatol. 2020, 19, 55–60. [Google Scholar] [CrossRef]
- Sparavigna, A.; Bombelli, L.; Giori, A.M.; Bellia, G. Efficacy and Tolerability of Hybrid Complexes of High- and Low-Molecular-Weight Hyaluronan Intradermal Injections for the Treatment of Skin Roughness and Laxity of the Neck. Sci. World J. 2022, 2022, 4497176. [Google Scholar] [CrossRef] [PubMed]
- Sparavigna, A.; Musella, D.; Cicerone, M.; Giori, A.M.; Bellia, G. Hybrid cooperative complexes of high and low molecular weight hyaluronans (96 mg/3 mL) for the treatment of skin laxity of the inner arm and abdomen. Gazz. Med. Ital. Arch. Sci. Med. 2022, 181, 487–495. [Google Scholar] [CrossRef]
- Sparavigna, A.; Grimolizzi, F.; Cigni, C.; Lualdi, R.; Bellia, G. Profhilo Body® for Tackling Skin Roughness and Laxity of Inner Arm, Abdomen and Knees. J. Plast. Pathol. Dermatol. 2023, 19, 31–38. [Google Scholar]
- Sparavigna, A.; Grimolizzi, F.; Cigni, C.; Lualdi, R.; Bellia, G. Use of intradermic injection of hybrid cooperative complexes of hyaluronic acid to counteract Skin Roughness and Laxity on the Back of the Hands. J. Plast. Pathol. Dermatol. 2023, 19, 7–13. [Google Scholar]
- Margara, A.; Haykal, D.; Musella, D.; Bellia, G.; Boriani, F. Hyaluronan Hybrid Cooperative Complexes Injection as a Biostimulation for Postobese Skin Laxity in the Arm: A Histopathologic Study. Aesthetic Surg. J. Open Forum 2024, 6, ojad110. [Google Scholar] [CrossRef]
- Ntege, E.H.; Sunami, H.; Shimizu, Y. Advances in regenerative therapy: A review of the literature and future directions. Regen. Ther. 2020, 14, 136–153. [Google Scholar] [CrossRef]
- Zarbafian, M.; Fabi, S.G.; Dayan, S.; Goldie, K. The Emerging Field of Regenerative Aesthetics—Where We Are Now. Dermatol. Surg. 2022, 48, 101–108. [Google Scholar] [CrossRef]
- Petrosyan, A.; Martins, P.N.; Solez, K.; Uygun, B.E.; Gorantla, V.S.; Orlando, G. Regenerative medicine applications: An overview of clinical trials. Front. Bioeng. Biotechnol. 2022, 10, 942750. [Google Scholar] [CrossRef]
- McKinley, K.L.; Longaker, M.T.; Naik, S. Emerging frontiers in regenerative medicine. Science 2023, 380, 796–798. [Google Scholar] [CrossRef]
- Mao, A.S.; Mooney, D.J. Regenerative medicine: Current therapies and future directions. Proc. Natl. Acad. Sci. USA 2015, 112, 14452–14459. [Google Scholar] [CrossRef]
- Iismaa, S.E.; Kaidonis, X.; Nicks, A.M.; Bogush, N.; Kikuchi, K.; Naqvi, N.; Harvey, R.P.; Husain, H.; Graham, R.M. Comparative regenerative mechanisms across different mammalian tissues. npj Regen. Med. 2018, 3, 6. [Google Scholar] [CrossRef]
- Tatullo, M.; Zavanx, B.; Piattelli, A. Critical Overview on Regenerative Medicine: New Insights into the Role of Stem Cells and Innovative Biomaterials. Int. J. Mol. Sci. 2023, 24, 7936. [Google Scholar] [CrossRef] [PubMed]
- Jin, Y.; Li, S.; Yu, Q.; Chen, T.; Liu, D. Application of stem cells in regeneration medicine. MedComm. 2023, 4, e291. [Google Scholar] [CrossRef]
- Mahheidari, N.; Kamalabadi-Farahani, M.; Nourani, M.R. Biological study of skin wound treated with Alginate/Carboxymethyl cellulose/chorion membrane, diopside nanoparticles, and Botox A. npj Regen. Med. 2024, 9, 9. [Google Scholar] [CrossRef]
- Nii, T.; Katayama, Y. Biomaterial-Assisted Regenerative Medicine. Int. J. Mol. Sci. 2021, 22, 8657. [Google Scholar] [CrossRef]
- Wang, Y.; Cheng, L.; Zhao, H.; Li, Z.; Chen, J.; Cen, Y.; Zhang, Z. The Therapeutic Role of ADSC-EVs in Skin Regeneration. Front. Med. 2022, 9, 858824. [Google Scholar] [CrossRef]
- Shimizu, Y.; Ntege, E.H.; Sunami, H. Current regenerative medicine-based approaches for skin regeneration: A review of literature and a report on clinical applications in Japan. Regen. Ther. 2022, 21, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Goldie, K. The evolving field of regenerative aesthetics. J. Cosmet. Dermatol. 2023, 22 (Suppl. 1), 1–7. [Google Scholar] [CrossRef] [PubMed]
- Khunger, N. Regenerative medicine in aesthetic surgery: Hope or hype? J Cutan Aesthet Surg. 2014, 7, 187–188. [Google Scholar] [CrossRef] [PubMed]
- Ray, S.; Ta, H.T. Investigating the Effect of Biomaterials Such as Poly-(l-Lactic Acid) Particles on Collagen Synthesis In Vitro: Method Is Matter. J. Funct. Biomater. 2020, 11, 51. [Google Scholar] [CrossRef] [PubMed]
- Ali, M.; Khan, N.R.; Basit, H.M.; Mahmood, S. Physico-chemical based mechanistic insight into surfactant modulated sodium carboxymethylcellulose film for skin tissue regeneration applications. J. Polym. Res. 2019, 27, 20. [Google Scholar] [CrossRef]
- Vleggaar, D.; Fitzgerald, R.; Lorenc, Z.P. Composition and mechanism of action of poly-L-lactic acid in soft tissue augmentation. J. Drugs Dermatol. 2014, 13 (Suppl. 4), S29–S31. [Google Scholar]
- Nowag, B.; Schäfer, D.; Hengl, T.; Corduff, N.; Goldie, K. Biostimulating fillers and induction of inflammatory pathways: A preclinical investigation of macrophage response to calcium hydroxylapatite and poly-L lactic acid. J. Cosmet. Dermatol. 2024, 23, 99–106. [Google Scholar] [CrossRef]
- Aguilera, S.B.; McCarthy, A.; Khalifian, S.; Lorenc, Z.P.; Goldie, K.; Chernoff, W.G. The Role of Calcium Hydroxylapatite (Radiesse) as a Regenerative Aesthetic Treatment: A Narrative Review. Aesthet. Surg. J. 2023, 43, 1063–1090. [Google Scholar] [CrossRef]
- Funt, D.K. Treatment of Delayed-onset Inflammatory Reactions to Hyaluronic Acid Filler: An Algorithmic Approach. Plast. Reconstr. Surg. Glob. Open 2022, 10, e4362. [Google Scholar] [CrossRef]
- Gonzaga da Cunha, M.; Engracia, M.; Gasques de Souza, L.; D’Apparecida Machado Filho, C. Biostimulators and their mechanisms of action. Surg. Cosm. Derm. 2020, 12, 109–117. [Google Scholar] [CrossRef]
- Muthu, S.; Bapat, A.; Jain, R.; Jeyaraman, N.; Jeyaraman, M. Exosomal therapy-a new frontier in regenerative medicine. Stem Cell Investig. 2021, 8, 7. [Google Scholar] [CrossRef] [PubMed]
- Thakur, A.; Shah, D.; Rai, D.; Parra, D.C.; Pathikonda, S.; Kurilova, S.; Cili, A. Therapeutic Values of Exosomes in Cosmetics, Skin Care, Tissue Regeneration, and Dermatological Diseases. Cosmetics 2023, 10, 65. [Google Scholar] [CrossRef]
- Olumesi, K.R.; Goldberg, D.J. A review of exosomes and their application in cutaneous medical aesthetics. J. Cosmet. Dermatol. 2023, 22, 2628–2634. [Google Scholar] [CrossRef]
- Li, X.; Corbett, A.L.; Taatizadeh, E.; Tasnim, N.; Little, J.P.; Garnis, C.; Daugaard, M.; Guns, E.; Hoorfar, M.; Li, I.T.S. Challenges and opportunities in exosome research-Perspectives from biology, engineering, and cancer therapy. APL Bioeng. 2019, 3, 011503. [Google Scholar] [CrossRef]
- Shir-az, O.; Berl, A.; Mann, D.; Bilal, B.S.; Levy, Y.; Shalom, A. Treatment of Scleroderma-Related Microstomia Using Hyaluronic Acid: An Interventional Study. Life 2023, 13, 2176. [Google Scholar] [CrossRef]
- Siquier-Dameto, G.; Solalinde, L. Positive Effect of Hybrid Stable Cooperative Complexes of High- and Low-Molecular-Weight Hyaluronic Acid in Psoriasis: A Clinical Series. Esperienze Dermatol. 2021, 22, 53–55. [Google Scholar] [CrossRef]
- Cassuto, D.; Yuri, V. Treatment of Scar Contracture with Intralesional Jet-Assisted Injection of Hyaluronic Acid. J. Dermatol. Res. Ther. 2020, 6, 94–98. [Google Scholar]
- Artzi, O.; Cohen, S.; Koren, A.; Niv, R.; Friedman, O. Dual-Plane Hyaluronic Acid Treatment for Atrophic Acne Scars. J. Cosmet. Dermatol. 2020, 19, 69–74. [Google Scholar] [CrossRef]
- Dastgheib, M.; Heidari, S.; Azizipour, A.; Kavyani, M.; Lajevardi, V.; Ehsani, A.H.; Teimourpour, A.; Daneshpazhooh, M.; Kashani, M.N.; Balighi, K. Investigating the impact of added Profhilo mesogel to subcision versus subcision monotherapy in treating acne scars; a single-blinded, split-face randomized trial. J. Cosmet. Dermatol. 2024. [Google Scholar] [CrossRef] [PubMed]
- Akerman, L.; Mimouni, D.; Nosrati, A.; Hilewitz, D.; Solomon-Cohen, E. A Combination of Non-Ablative Laser and Hyaluronic Acid Injectable for Postacne Scars: A Novel Treatment Protocol. J. Clin. Aesthet. Dermatol. 2022, 15, 53. [Google Scholar]
- Mohammed, G.F.; Al-Dhubaibi, M.S. Triple Steps Acne Scar Revision Technique: A New Combination Therapeutic Modality for Atrophic Acne Scars. J. Cosmet. Dermatol. 2022, 21, 4659–4668. [Google Scholar] [CrossRef]
- Tedesco, M.; Garelli, V.; Elia, F.; Sperati, F.; Biondi, F.; Mosiello, L.; Morrone, A.; Migliano, E. Efficacy of Injecting Hybrid Cooperative Complexes of Hyaluronic Acid for the Treatment of Vulvar Lichen Sclerosus: A Preliminary Study. J. Cosmet. Dermatol. 2023, 22, 449–457. [Google Scholar] [CrossRef] [PubMed]
- Tedesco, M.; Alei, L.; Bonadies, A.; Pallara, T.; Parisi, P.; Latini, A.; Bellei, B.; Sperati, F.; Migliano, E. Hybrid cooperative complexes to decrease VAS score and enhance sexual function in women with vulvar lichen sclerosus. Eur. Rev. Med. Pharmacol. Sci. 2024, 28, 814–821. [Google Scholar] [PubMed]
- Garavaglia, E.; Sala, C.; Busato, M.; Bellia, G.; Tamburlin, N.; Massirone, A. First Use of Thermal Stabilized Hyaluronic Acid Injection in One-Year Follow-Up Patients with Genitourinary Syndrome. Med. Devices 2020, 13, 399–410. [Google Scholar] [CrossRef] [PubMed]
- D’Agostino, A.; La Gatta, A.; Stellavato, A.; Cimini, D.; Corsuto, L.; Cammarota, M.; D’Agostino, M.; Schiraldi, C. Potential of Biofermentative Unsulfated Chondroitin and Hyaluronic Acid in Dermal Repair. Int. J. Mol. Sci. 2022, 23, 1686. [Google Scholar] [CrossRef]
- Li, X.; Li, C.; Zhang, W.; Wang, Y.; Qian, P.; Huang, H. Inflammation and aging: Signaling pathways and intervention therapies. Sig Transduct. Target. Ther. 2023, 8, 239. [Google Scholar] [CrossRef] [PubMed]
- Vassallo, V.; Di Meo, C.; Toro, G.; Alfano, A.; Iolascon, G.; Schiraldi, C. Hyaluronic Acid-Based Injective Medical Devices: In Vitro Characterization of Novel Formulations Containing Biofermentative Unsulfated Chondroitin or Extractive Sulfated One with Cyclodextrins. Pharmaceuticals 2023, 16, 1429. [Google Scholar] [CrossRef]
- Saravanakumar, K.; Park, S.J.; Santosh, S.S.; Ganeshalingam, A.; Thiripuranathar, G.; Sathiyaseelan, A.; Vijayasarathy, S.; Swaminathan, A.; Priya, V.V.; Wang, M.H. Application of Hyaluronic Acid in Tissue Engineering, Regenerative Medicine, and Nanomedicine: A Review. Int. J. Biol. Macromol. 2022, 222 Pt B, 2744–2760. [Google Scholar] [CrossRef]
- Liu, T.; Zhang, L.; Joo, D.; Sun, S.C. NF-κB signaling in inflammation. Signal Transduct. Target. Ther. 2017, 2, 17023. [Google Scholar] [CrossRef]
- Valachová, K.; Šoltés, L. Hyaluronan as a Prominent Biomolecule with Numerous Applications in Medicine. Int. J. Mol. Sci. 2021, 22, 7077. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Tissue/Cell Type | HCCs’ Effect | Citation |
|---|---|---|
| Keratinocytes, fibroblasts |
| [19,22] |
| Adipocytes |
| [21,23] |
| Mesenchymal stromal cells |
| [24,25,26] |
| Treatment | Target Area/Layer | Injection Technique | Main Clinical Outcomes | Ref. |
|---|---|---|---|---|
| Profhilo® | Face/dermis | BAP technique (five injection points of 0.2 mL on each hemiface with 29G needle) |
| [30,31,32,33,34,35,38] |
| Neck/dermis | BAP technique (10 injection points of 0.2 mL with 29G needle) |
| [36,38,43] | |
| Profhilo® Structura | Face/adipose tissue | A total of 1 mL in preauricular area of each hemiface with 25G cannula |
| [40,41] |
| Profhilo® Body | Inner arms, abdomen, knees/dermis | BAP technique (10 injection points of 0.3 mL with 29G needle) |
| [44,45] |
| Hands/dermis | A total of 1.5 mL in each hand with 22G cannula (0.3 mL per passage) |
| [46] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Humzah, D.; Molina, B.; Salti, G.; Cigni, C.; Bellia, G.; Grimolizzi, F. Intradermal Injection of Hybrid Complexes of High- and Low-Molecular-Weight Hyaluronan: Where Do We Stand and Where Are We Headed in Regenerative Medicine? Int. J. Mol. Sci. 2024, 25, 3216. https://doi.org/10.3390/ijms25063216
Humzah D, Molina B, Salti G, Cigni C, Bellia G, Grimolizzi F. Intradermal Injection of Hybrid Complexes of High- and Low-Molecular-Weight Hyaluronan: Where Do We Stand and Where Are We Headed in Regenerative Medicine? International Journal of Molecular Sciences. 2024; 25(6):3216. https://doi.org/10.3390/ijms25063216
Chicago/Turabian StyleHumzah, Dalvi, Beatriz Molina, Giovanni Salti, Clara Cigni, Gilberto Bellia, and Franco Grimolizzi. 2024. "Intradermal Injection of Hybrid Complexes of High- and Low-Molecular-Weight Hyaluronan: Where Do We Stand and Where Are We Headed in Regenerative Medicine?" International Journal of Molecular Sciences 25, no. 6: 3216. https://doi.org/10.3390/ijms25063216
APA StyleHumzah, D., Molina, B., Salti, G., Cigni, C., Bellia, G., & Grimolizzi, F. (2024). Intradermal Injection of Hybrid Complexes of High- and Low-Molecular-Weight Hyaluronan: Where Do We Stand and Where Are We Headed in Regenerative Medicine? International Journal of Molecular Sciences, 25(6), 3216. https://doi.org/10.3390/ijms25063216