


Impact of Glucagon-Like Peptide 1 Receptor Agonists on Biochemical Markers of the Initiation of Atherosclerotic Process

Abstract
1. Introduction
2. Results
2.1. Study Group Characteristics
2.2. Metabolic Effect after 180 Days of Treatment
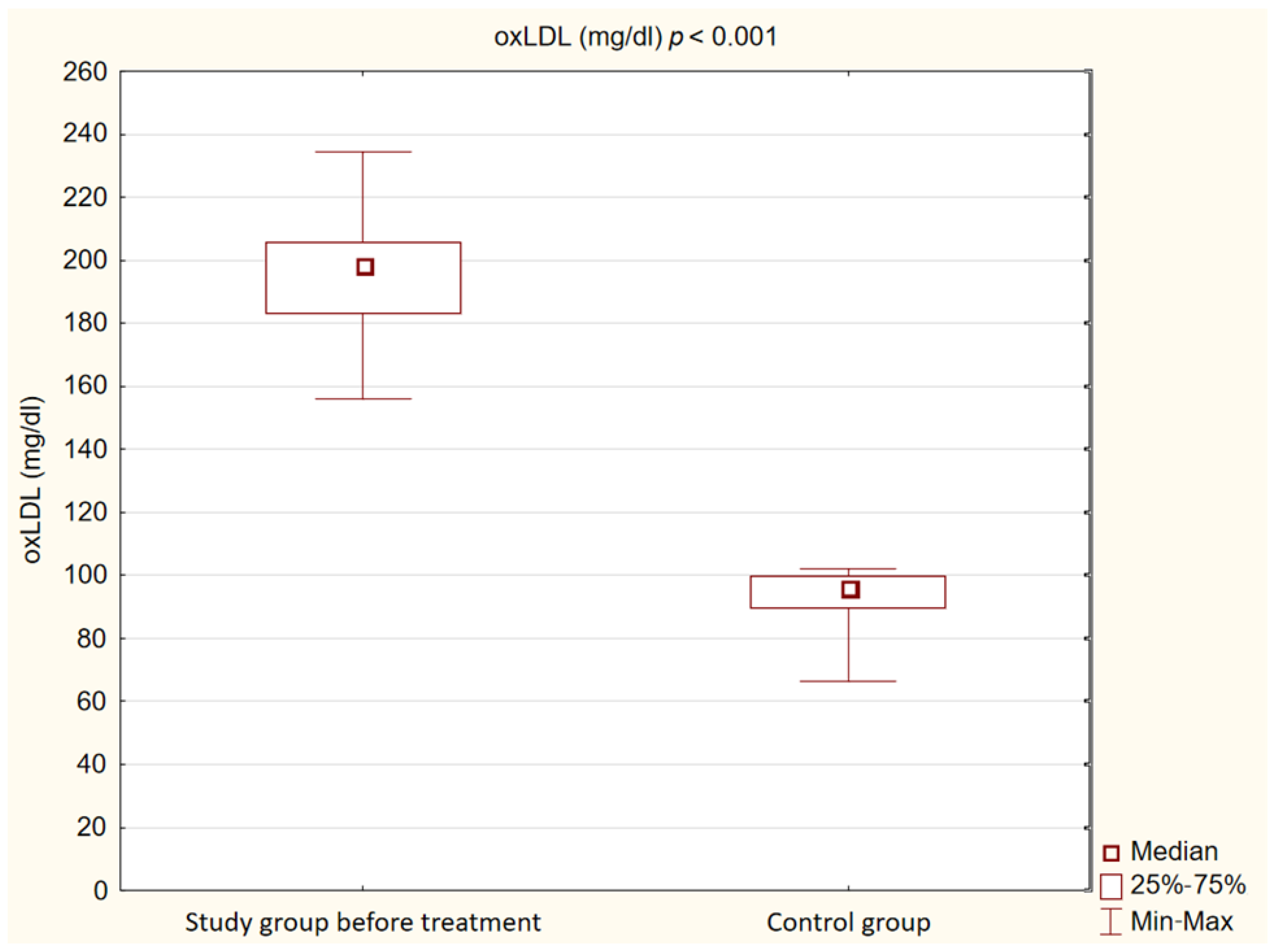
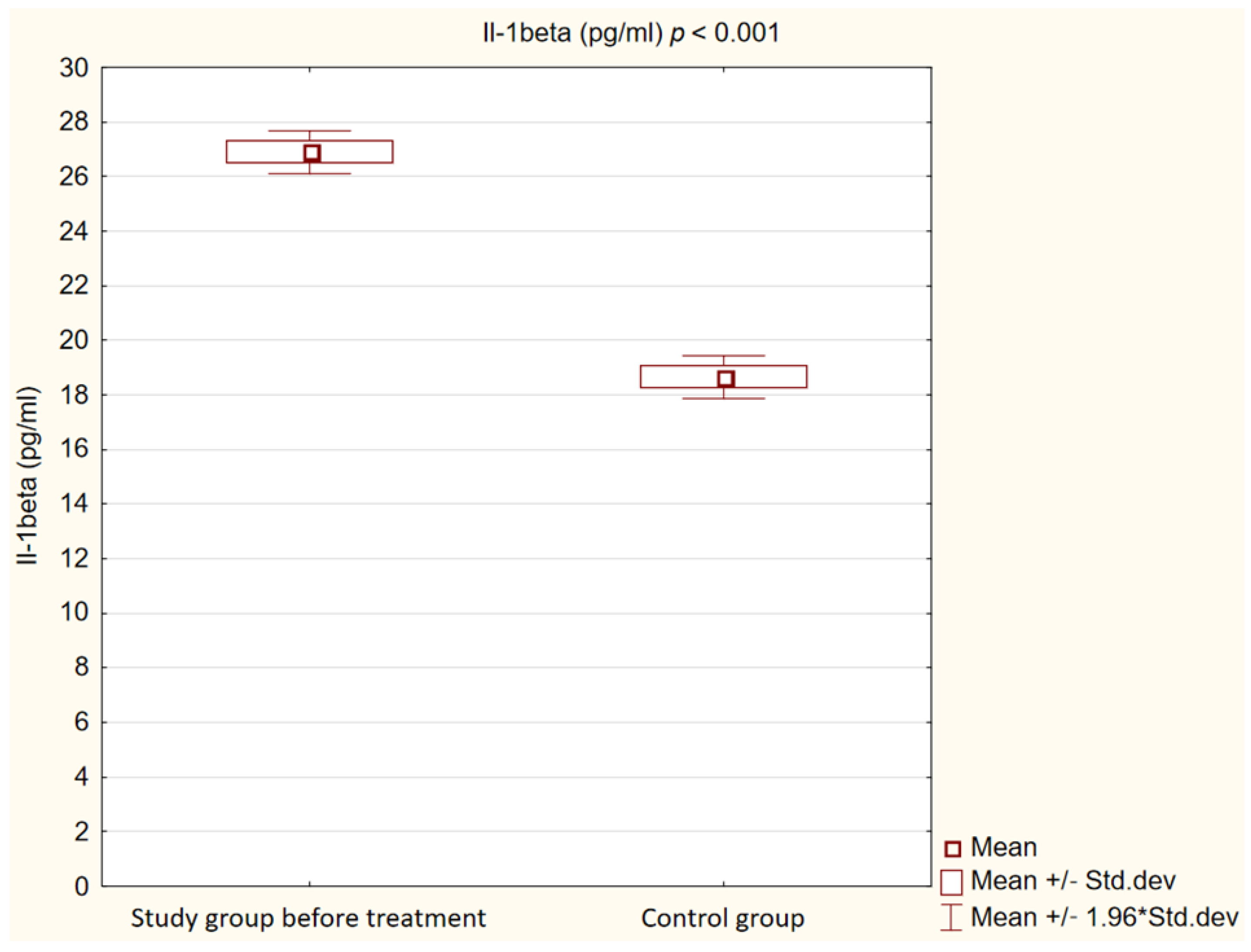
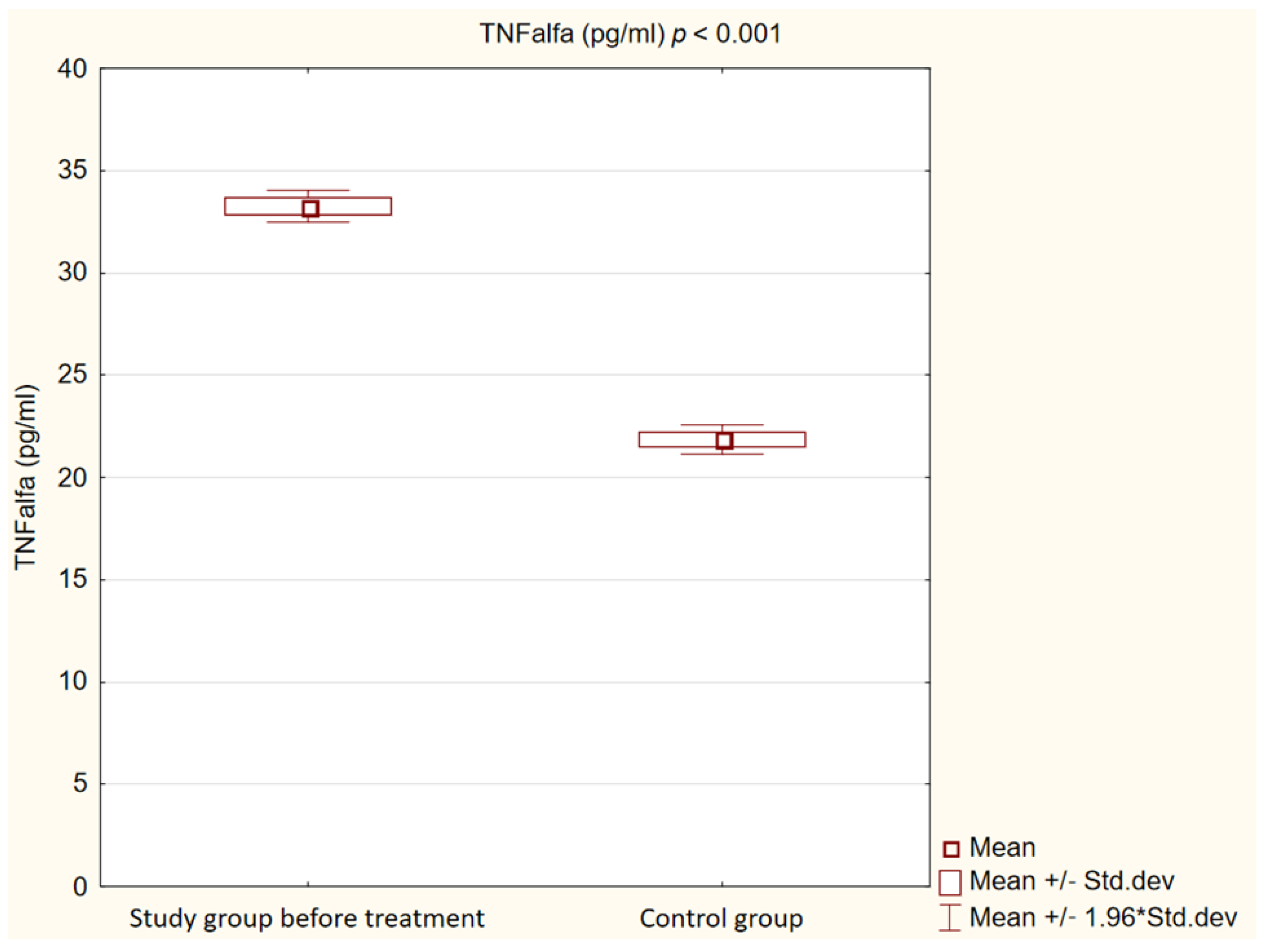
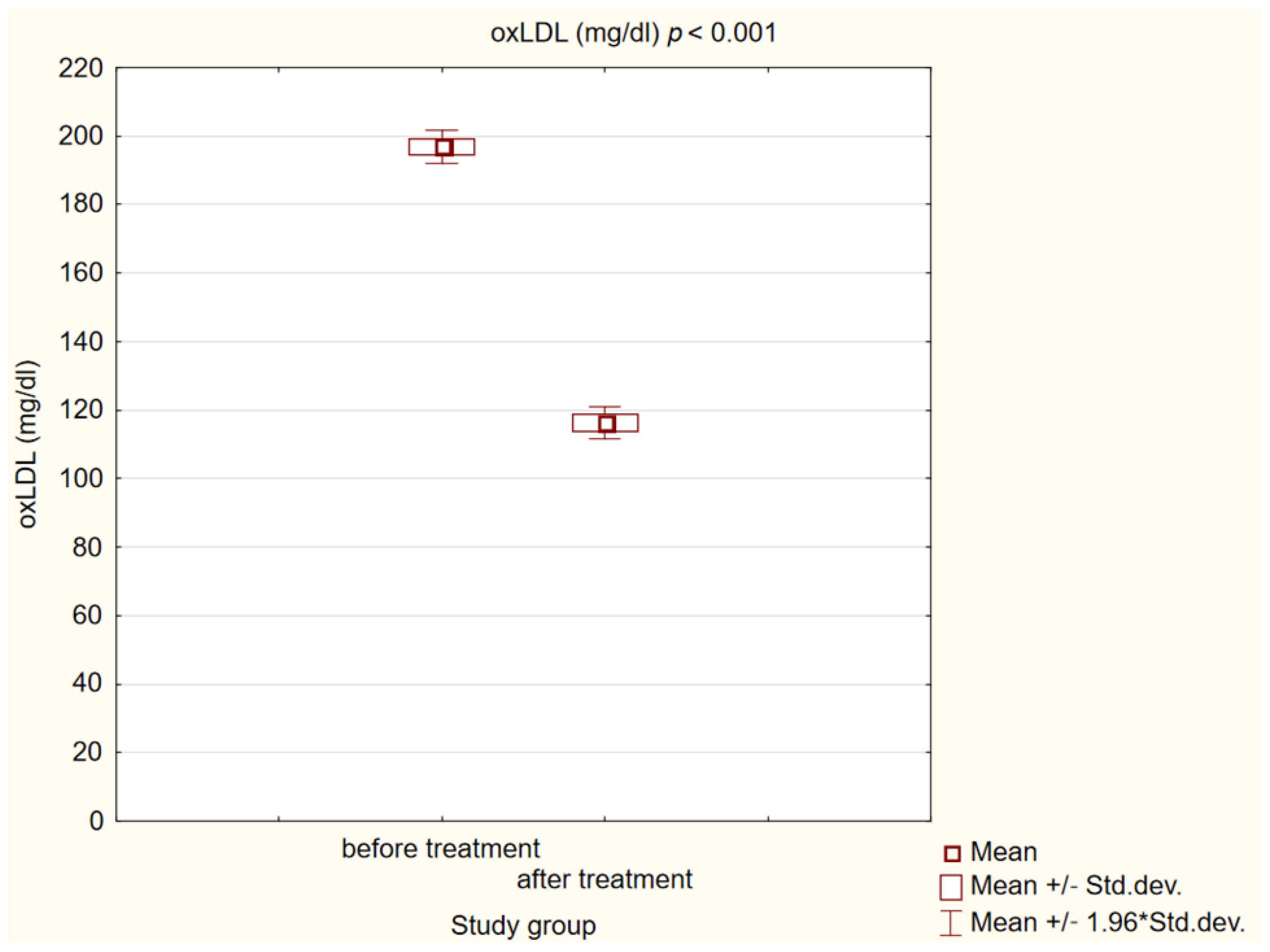
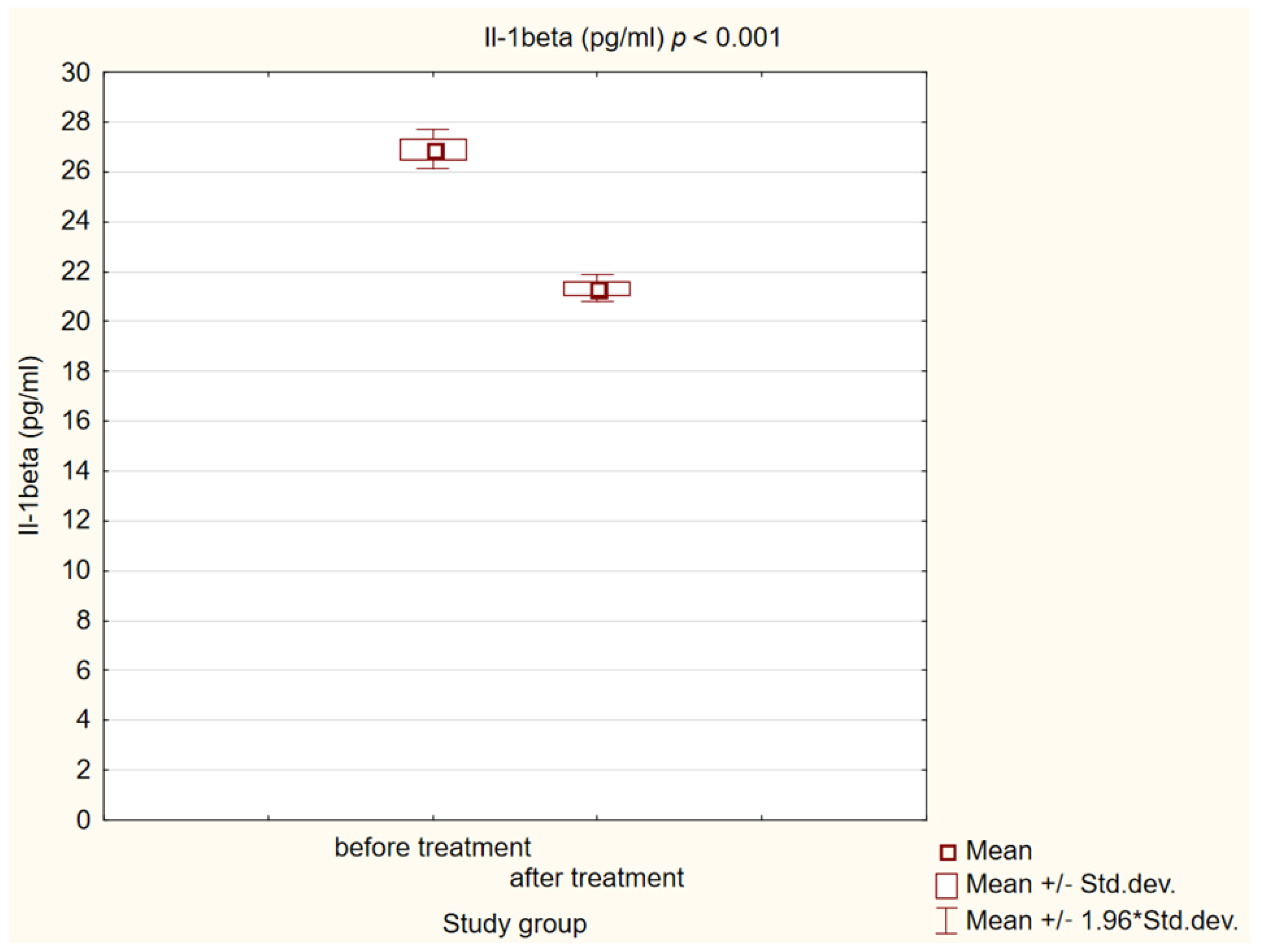
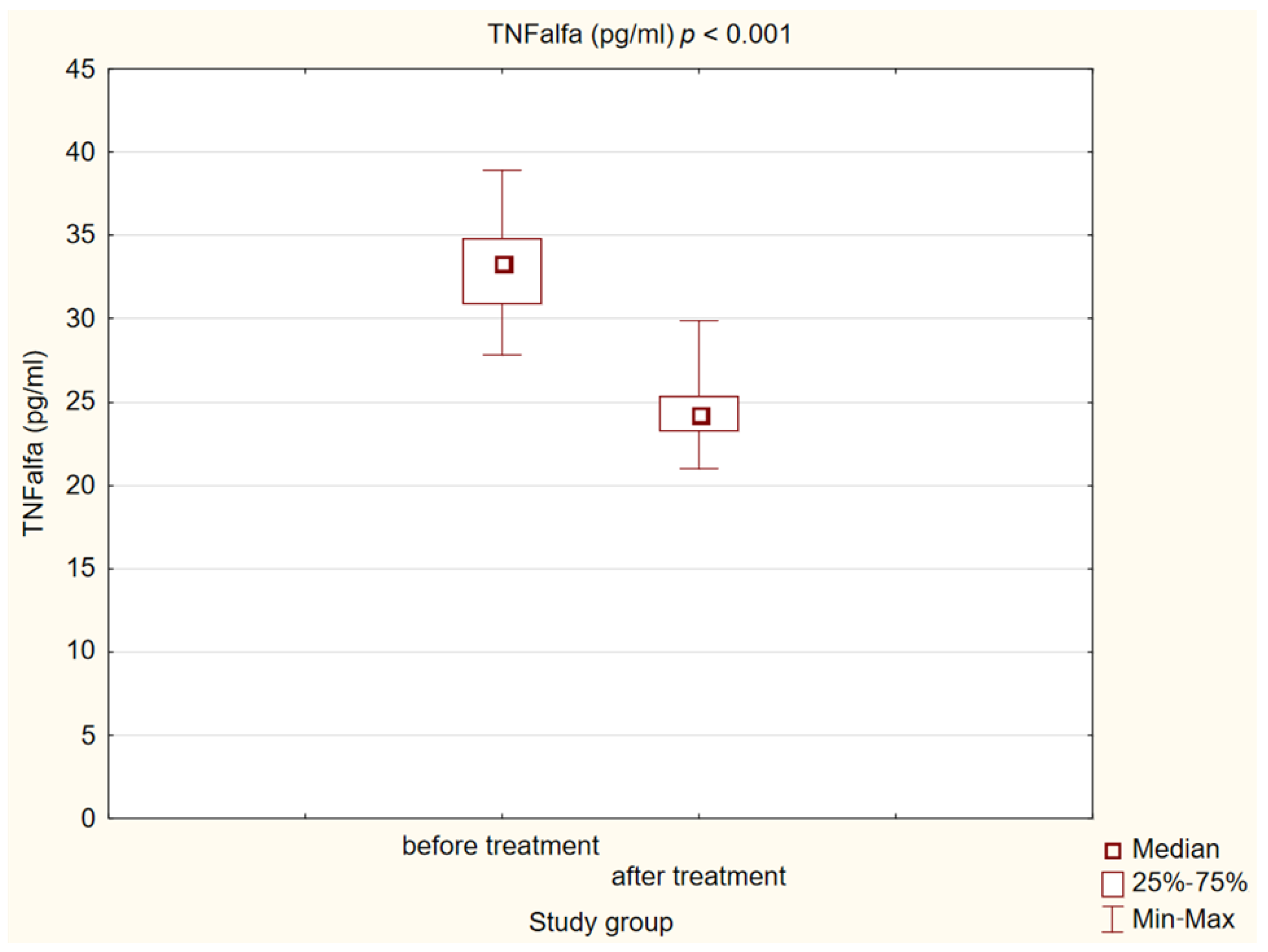
2.3. Effect on Biochemical Markers of Initiation of Atherosclerotic Process
2.4. Safety and Adverse Events
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. Inclusion and Exclusion Criteria
4.3. Laboratory and Anthropometric Measurements
4.4. Arteriosclerotic Plaque Examination
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rana, J.S.; Khan, S.S.; Lloyd-Jones, D.M.; Sidney, S. Changes in mortality in Top 10 causes of death from 2011 to 2018. J. Gen. Int. Med. 2021, 36, 2517–2518. [Google Scholar] [CrossRef] [PubMed]
- Hou, P.; Fang, J.; Liu, Z.; Shi, Y.; Agostini, M.; Bernassola, F.; Bove, P.; Candi, E.; Rovella, V.; Sica, G.; et al. Macrophage polarization and metabolism in atherosclerosis. Cell Death Dis. 2023, 14, 691. [Google Scholar] [CrossRef] [PubMed]
- Khatana, C.; Saini, N.K.; Chakrabarti, S.; Saini, V.; Sharma, A.; Saini, R.V.; Saini, A.K. Mechanistic Insights into the Oxidized Low-Density Lipoprotein-Induced Atherosclerosis. Oxid. Med. Cell Longev. 2020, 2020, 5245308. [Google Scholar] [CrossRef] [PubMed]
- Linton, M.F.; Babaev, V.R.; Huang, J.; Linton, E.F.; Tao, H.; Yancey, P.G. Macrophage apoptosis and efferocytosis in the pathogenesis of atherosclerosis. Circ. J. 2016, 80, 2259–2268. [Google Scholar] [CrossRef] [PubMed]
- Libby, P.; Hansson, G.K. From Focal Lipid Storage to Systemic Inflammation: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2019, 74, 1594–1607. [Google Scholar] [CrossRef] [PubMed]
- Dinarello, C.A. Overview of the IL-1 family in innate inflammation and acquired immunity. Immunol. Rev. 2018, 281, 8–27. [Google Scholar] [CrossRef]
- Grebe, A.; Latz, E. Cholesterol crystals and inflammation. Curr. Rheumatol. Rep. 2013, 15, 313. [Google Scholar] [CrossRef]
- Sharma, B.R.; Kanneganti, T.D. NLRP3 inflammasome in cancer and metabolic diseases. Nat. Immunol. 2021, 22, 550–559. [Google Scholar] [CrossRef]
- Pascual-Figal, D.A.; Bayes-Genis, A.; Asensio-Lopez, M.C.; Hernandez-Vicente, A.; Garrido-Bravo, I.; Pastor-Perez, F.; Diez, J.; Ibanez, B.; Lax, A. The Interleukin-1 Axis and Risk of Death in Patients with Acutely Decompensated Heart Failure. J. Am. Coll. Cardiol. 2019, 73, 1016–1025. [Google Scholar] [CrossRef]
- Silvain, J.; Kerneis, M.; Zeitouni, M.; Lattuca, B.; Galier, S.; Brugier, D.; Mertens, E.; Procopi, N.; Suc, G.; Salloum, T.; et al. Interleukin-1beta and Risk of Premature Death in Patients with Myocardial Infarction. J. Am. Coll. Cardiol. 2020, 76, 1763–1773. [Google Scholar] [CrossRef]
- Ridker, P.M.; Everett, B.M.; Thuren, T.; MacFadyen, J.G.; Chang, W.H.; Ballantyne, C.; Fonseca, F.; Nicolau, J.; Koenig, W.; Anker, S.D.; et al. Antiinflammatory Therapy with Canakinumab for Atherosclerotic Disease. N. Engl. J. Med. 2017, 377, 1119–1131. [Google Scholar] [CrossRef] [PubMed]
- Kattoor, A.J.; Pothineni, N.V.K.; Palagiri, D.; Mehta, J.L. Oxidative stress in atherosclerosis. Curr. Atheroscler. Rep. 2017, 19, 42. [Google Scholar] [CrossRef]
- Kleinbongard, P.; Heusch, G.; Schulz, R. TNFalpha in atherosclerosis, myocardial ischemia/reperfusion and heart failure. Pharmacol. Ther. 2010, 127, 295–314. [Google Scholar] [CrossRef] [PubMed]
- de Heredia, F.P.; Gómez-Martínez, S.; Marcos, A. Obesity, inflammation and the immune system. Proc. Nutr. Soc. 2012, 71, 332–338. [Google Scholar] [CrossRef] [PubMed]
- Alexandraki, K.; Piperi, C.; Kalofoutis, C.; Singh, J.; Alaveras, A.; Kalofoutis, A. Inflammatory process in type 2 diabetes: The role of cytokines. Ann. N. Y. Acad. Sci. 2006, 1084, 89–117. [Google Scholar] [CrossRef] [PubMed]
- Rakipovski, G.; Rolin, B.; Nøhr, J.; Klewe, I.; Frederiksen, K.S.; Augustin, R.; Hecksher-Sørensen, J.; Ingvorsen, C.; Polex-Wolf, J.; Knudsen, L.B. The GLP-1 Analogs Liraglutide and Semaglutide Reduce Atherosclerosis in ApoE-/- and LDLr-/- Mice by a Mechanism That Includes Inflammatory Pathways. JACC Basic Transl. Sci. 2018, 3, 844–857. [Google Scholar] [CrossRef]
- Marso, S.P.; Daniels, G.H.; Brown-Frandsen, K.; Kristensen, P.; Mann, J.F.; Nauck, M.A.; Nissen, S.E.; Pocock, S.; Poulter, N.R.; Ravn, L.S.; et al. Liraglutide and Cardiovascular Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2016, 375, 311–322. [Google Scholar] [CrossRef]
- Husain, M.; Birkenfeld, A.L.; Donsmark, M.; Dungan, K.; Eliaschewitz, F.G.; Franco, D.R.; Jeppesen, O.K.; Lingvay, I.; Mosenzon, O.; Pedersen, S.D.; et al. Oral Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N. Engl. J. Med. 2019, 381, 841–851. [Google Scholar] [CrossRef]
- Marso, S.P.; Bain, S.C.; Consoli, A.; Eliaschewitz, F.G.; Jódar, E.; Leiter, L.A.; Lingvay, I.; Rosenstock, J.; Seufert, J.; Warren, M.L.; et al. Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N. Engl. J. Med. 2016, 375, 1834–1844. [Google Scholar] [CrossRef]
- Gerstein, H.C.; Colhoun, H.M.; Dagenais, G.R.; Diaz, R.; Lakshmanan, M.; Pais, P.; Probstfield, J.; Riesmeyer, J.S.; Riddle, M.C.; Rydén, L.; et al. Dulaglutide and cardiovascular outcomes in type 2 diabetes (REWIND): A double-blind, randomised placebo-controlled trial. Lancet 2019, 394, 121–130. [Google Scholar] [CrossRef]
- Marx, N.; Federici, M.; Schütt, K.; Müller-Wieland, D.; Ajjan, R.A.; Antunes, M.J.; Christodorescu, R.M.; Crawford, C.; Di Angelantonio, E.; Eliasson, B.; et al. 2023 ESC Guidelines for the management of cardiovascular disease in patients with diabetes. Eur. Heart J. 2023, 44, 4043–4140, Erratum in Eur. Heart J. 2023, ehad857. [Google Scholar] [CrossRef] [PubMed]
- Brili, S.; Tousoulis, D.; Antonopoulos, A.S.; Antoniades, C.; Hatzis, G.; Bakogiannis, C.; Papageorgiou, N.; Stefanadis, C. Effects of atorvastatin on endothelial function and the expression of proinflammatory cytokines and adhesion molecules in young subjects with successfully repaired coarctation of aorta. Heart 2012, 98, 325–329. [Google Scholar] [CrossRef] [PubMed]
- Abbasifard, M.; Kandelouei, T.; Aslani, S.; Razi, B.; Imani, D.; Fasihi, M.; Cicero, F.G.; Sahebkar, A. Effect of statins on the plasma/serum levels of inflammatory markers in patients with cardiovascular disease; a systematic review and meta-analysis of randomized clinical trials. Inflammopharmacology 2022, 30, 369–383. [Google Scholar] [CrossRef]
- Jamialahmadi, T.; Baratzadeh, F.; Reiner, Ž.; Mannarino, M.R.; Cardenia, V.; Simental-Mendía, L.E.; Pirro, M.; Watts, G.F.; Sahebkar, A. The Effects of Statin Therapy on Oxidized LDL and Its Antibodies: A Systematic Review and Meta-Analysis. Oxid. Med. Cell. Longev. 2022, 2022, 7850659. [Google Scholar] [CrossRef]
- Saud, A.; Ali, N.; Gali, F.; Qassam, H.; Hadi, N.R. The effect of evolocumab alone and in combination with atorvastatin on atherosclerosis progression and TLRs expression. J. Med. Life 2023, 16, 759–765. [Google Scholar] [CrossRef] [PubMed]
- Basiak, M.; Kosowski, M.; Hachula, M.; Okopien, B. Impact of PCSK9 Inhibition on Proinflammatory Cytokines and Matrix Metalloproteinases Release in Patients with Mixed Hyperlipidemia and Vulnerable Atherosclerotic Plaque. Pharmaceuticals 2022, 15, 802. [Google Scholar] [CrossRef]
- Yang, J.; Ma, X.; Niu, D.; Sun, Y.; Chai, X.; Deng, Y.; Wang, J.; Dong, J. PCSK9 inhibitors suppress oxidative stress and inflammation in atherosclerotic development by promoting macrophage autophagy. Am. J. Transl. Res. 2023, 15, 5129–5144. [Google Scholar]
- Que, Q.; Guo, X.; Zhan, L.; Chen, S.; Zhang, Z.; Ni, X.; Ye, B.; Wan, S. The GLP-1 agonist, liraglutide, ameliorates inflammation through the activation of the PKA/CREB pathway in a rat model of knee osteoarthritis. J Inflamm (Lond.) 2019, 16, 13. [Google Scholar] [CrossRef]
- Tao, Y.; Ge, G.; Wang, Q.; Wang, W.; Zhang, W.; Bai, J.; Lin, J.; Shen, J.; Guo, X.; Xu, Y.; et al. Exenatide ameliorates inflammatory response in human rheumatoid arthritis fibroblast-like synoviocytes. IUBMB Life 2019, 71, 969–977. [Google Scholar] [CrossRef]
- Ferdaoussi, M.; Abdelli, S.; Yang, J.Y.; Cornu, M.; Niederhauser, G.; Favre, D.; Widmann, C.; Regazzi, R.; Thorens, B.; Waeber, G.; et al. Exendin-4 protects beta-cells from interleukin-1 beta-induced apoptosis by interfering with the c-Jun NH2-terminal kinase pathway. Diabetes 2008, 57, 1205–1215. [Google Scholar] [CrossRef]
- Wang, Y.; Parlevliet, E.T.; Geerling, J.J.; van der Tuin, S.J.; Zhang, H.; Bieghs, V.; Jawad, A.H.; Shiri-Sverdlov, R.; Bot, I.; de Jager, S.C.; et al. Exendin-4 decreases liver inflammation and atherosclerosis development simultaneously by reducing macrophage infiltration. Br. J. Pharmacol. 2014, 171, 723–734. [Google Scholar] [CrossRef]
- Dai, Y.; Dai, D.; Wang, X.; Ding, Z.; Li, C.; Mehta, J.L. GLP-1 agonists inhibit ox-LDL uptake in macrophages by activating protein kinase A. J. Cardiovasc. Pharmacol. 2014, 64, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, M.; Matsuo, Y.; Yamakage, H.; Masuda, S.; Terada, Y.; Muranaka, K.; Wada, H.; Hasegawa, K.; Shimatsu, A.; Satoh-Asahara, N. Differential effects of GLP-1 receptor agonist on foam cell formation in monocytes between non-obese and obese subjects. Metabolism 2016, 65, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Ma, G.F.; Chen, S.; Yin, L.; Gao, X.D.; Yao, W.B. Exendin-4 ameliorates oxidized-LDL-induced inhibition of macrophage migration in vitro via the NF-κB pathway. Acta Pharmacol. Sin. 2014, 35, 195–202. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Zobel, E.H.; Ripa, R.S.; von Scholten, B.J.; Curovic, V.R.; Diaz, L.J.; Hansen, T.W.; Rossing, P.; Kjaer, A. Effect of Liraglutide on Vascular Inflammation Evaluated by [64Cu]DOTATATE. Diagnostics 2021, 11, 1431. [Google Scholar] [CrossRef] [PubMed]
- Luna-Marco, C.; de Marañon, A.M.; Hermo-Argibay, A.; Rodriguez-Hernandez, Y.; Hermenejildo, J.; Fernandez-Reyes, M.; Apostolova, N.; Vila, J.; Sola, E.; Morillas, C.; et al. Effects of GLP-1 receptor agonists on mitochondrial function, inflammatory markers and leukocyte-endothelium interactions in type 2 diabetes. Redox Biol. 2023, 66, 102849. [Google Scholar] [CrossRef] [PubMed]
- Hogan, A.E.; Gaoatswe, G.; Lynch, L.; Corrigan, M.A.; Woods, C.; O’Connell, J.; O’Shea, D. Glucagon-like peptide 1 analogue therapy directly modulates innate immune-mediated inflammation in in-dividuals with type 2 diabetes mellitus. Diabetologia 2014, 57, 781–784. [Google Scholar] [CrossRef]
- Belančić, A.; Kresović, A.; Troskot Dijan, M. Glucagon-like peptide-1 receptor agonists in the era of COVID-19: Friend or foe? Clin. Obes. 2021, 11, e12439. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Group | Control Group | p | |
|---|---|---|---|
| Number of patients | 50 | 26 | |
| Age, years | 60.76 ± 9.52 | 33.08 ± 5.45 | <0.001 |
| Women, % | 54 | 50 | 0.74 |
| Men, % | 46 | 50 | 0.74 |
| WHO guidelines on physical activity, % | 40 | 54 | <0.05 |
| Smokers, % | 18 | 4 | <0.01 |
| Alcohol abuse, % | 0 | 0 | 1 |
| Study Group before Treatment | Control Group | ||||||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | p | |||
| BMI (kg/m2) | 35.02 | 7.10 | 22.46 | 2.54 | <0.001 | ||
| WHR | 0.97 | 0.06 | 0.83 | 0.09 | <0.001 | ||
| DBP (mmHg) | 82.36 | 8.56 | 77.96 | 8.19 | <0.001 | ||
| Median | Q1 | Q3 | Median | Q1 | Q3 | ||
| SBP | 135 | 125 | 145 | 122 | 120 | 132 | <0.001 |
| Glucose (mg/dL) | 160.50 | 133.10 | 203.30 | 89 | 84.80 | 95 | <0.001 |
| TC (mg/dL) | 166.55 | 150.30 | 199 | 173.80 | 156.10 | 196.60 | 0.72 |
| LDL (mg/dL) | 83 | 67 | 105 | 90.50 | 74 | 110 | 0.46 |
| HDL (mg/dL) | 48.95 | 43.70 | 56.80 | 64.30 | 58.80 | 71.10 | <0.001 |
| non-HDL (mg/dl) | 113.70 | 100 | 155.60 | 109 | 86 | 129 | 0.15 |
| TG (mg/dL) | 167.95 | 110.50 | 207.10 | 86.50 | 62.30 | 108 | <0.001 |
| Creatinine (mg/dL) | 1.06 | 0.98 | 1.15 | 0.93 | 0.79 | 1.03 | <0.001 |
| GFR (ml/min/1.73 m2) | 67.50 | 58 | 81 | 96.50 | 86 | 113 | <0.001 |
| HbA1C (%) | 8.75 | 7.60 | 9.60 | 5.50 | 5.20 | 5.70 | <0.001 |
| FIB-4 | 1.50 | 1.18 | 1.90 | 0.66 | 0.54 | 0.88 | <0.001 |
|
Study Group before Treatment |
Study Group after Treatment | ||||||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | p | |||
| BMI (kg/m2) | 35.02 | 7.10 | 33.21 | 6.94 | <0.001 | ||
| SBP (mmHg) | 135.36 | 13.72 | 129.62 | 10.24 | <0.001 | ||
| DBP (mmHg) | 82.36 | 8.56 | 78.76 | 5.62 | <0.001 | ||
| HbA1C (%) | 8.68 | 1.52 | 7.56 | 1.04 | <0.001 | ||
| GFR (ml/min/1.73 m2) | 69.76 | 14.51 | 73.10 | 18.21 | 0.11 | ||
| Median | Q1 | Q3 | Median | Q1 | Q3 | ||
| WHR | 0.96 | 0.92 | 1.02 | 0.96 | 0.92 | 1.01 | 0.13 |
| Glucose (mg/dL) | 160.50 | 133.10 | 203.30 | 138.30 | 117.40 | 164.10 | <0.001 |
| TC (mg/dL) | 166.55 | 150.30 | 199 | 169.10 | 146 | 198 | 0.62 |
| LDL (mg/dL) | 83 | 67 | 105 | 80.50 | 60 | 117 | 0.53 |
| HDL (mg/dL) | 48.95 | 43.70 | 56.80 | 50.65 | 46.30 | 60.50 | 0.18 |
| non-HDL (mg/dL) | 113.70 | 100 | 155.60 | 107.80 | 93.40 | 148.20 | 0.19 |
| TG (mg/dL) | 167.95 | 110.50 | 207.10 | 146.50 | 104 | 189 | 0.28 |
| Creatinine (mg/dL) | 1.06 | 0.98 | 1.15 | 1.04 | 0.92 | 1.14 | 0.45 |
| FIB-4 | 1.50 | 1.18 | 1.90 | 1.30 | 1.03 | 1.60 | <0.001 |
| ΔHbA1C | ΔWeight | |
|---|---|---|
| ΔIl-1β | R = 0.012, p > 0.05 | R = 0.015, p > 0.05 |
| ΔTNFα | R = 0.039, p > 0.05 | R = 0.001, p > 0.05 |
| ΔoxLDL | R = 0.15, p > 0.01 | R = 0.089, p > 0.05 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hachuła, M.; Kosowski, M.; Ryl, S.; Basiak, M.; Okopień, B. Impact of Glucagon-Like Peptide 1 Receptor Agonists on Biochemical Markers of the Initiation of Atherosclerotic Process. Int. J. Mol. Sci. 2024, 25, 1854. https://doi.org/10.3390/ijms25031854
Hachuła M, Kosowski M, Ryl S, Basiak M, Okopień B. Impact of Glucagon-Like Peptide 1 Receptor Agonists on Biochemical Markers of the Initiation of Atherosclerotic Process. International Journal of Molecular Sciences. 2024; 25(3):1854. https://doi.org/10.3390/ijms25031854
Chicago/Turabian StyleHachuła, Marcin, Michał Kosowski, Sabina Ryl, Marcin Basiak, and Bogusław Okopień. 2024. "Impact of Glucagon-Like Peptide 1 Receptor Agonists on Biochemical Markers of the Initiation of Atherosclerotic Process" International Journal of Molecular Sciences 25, no. 3: 1854. https://doi.org/10.3390/ijms25031854
APA StyleHachuła, M., Kosowski, M., Ryl, S., Basiak, M., & Okopień, B. (2024). Impact of Glucagon-Like Peptide 1 Receptor Agonists on Biochemical Markers of the Initiation of Atherosclerotic Process. International Journal of Molecular Sciences, 25(3), 1854. https://doi.org/10.3390/ijms25031854