
Anti-ZSCAN1 Autoantibodies Are a Feasible Diagnostic Marker for ROHHAD Syndrome Not Associated with a Tumor


Abstract
1. Introduction
2. Results
2.1. Protein Array Results
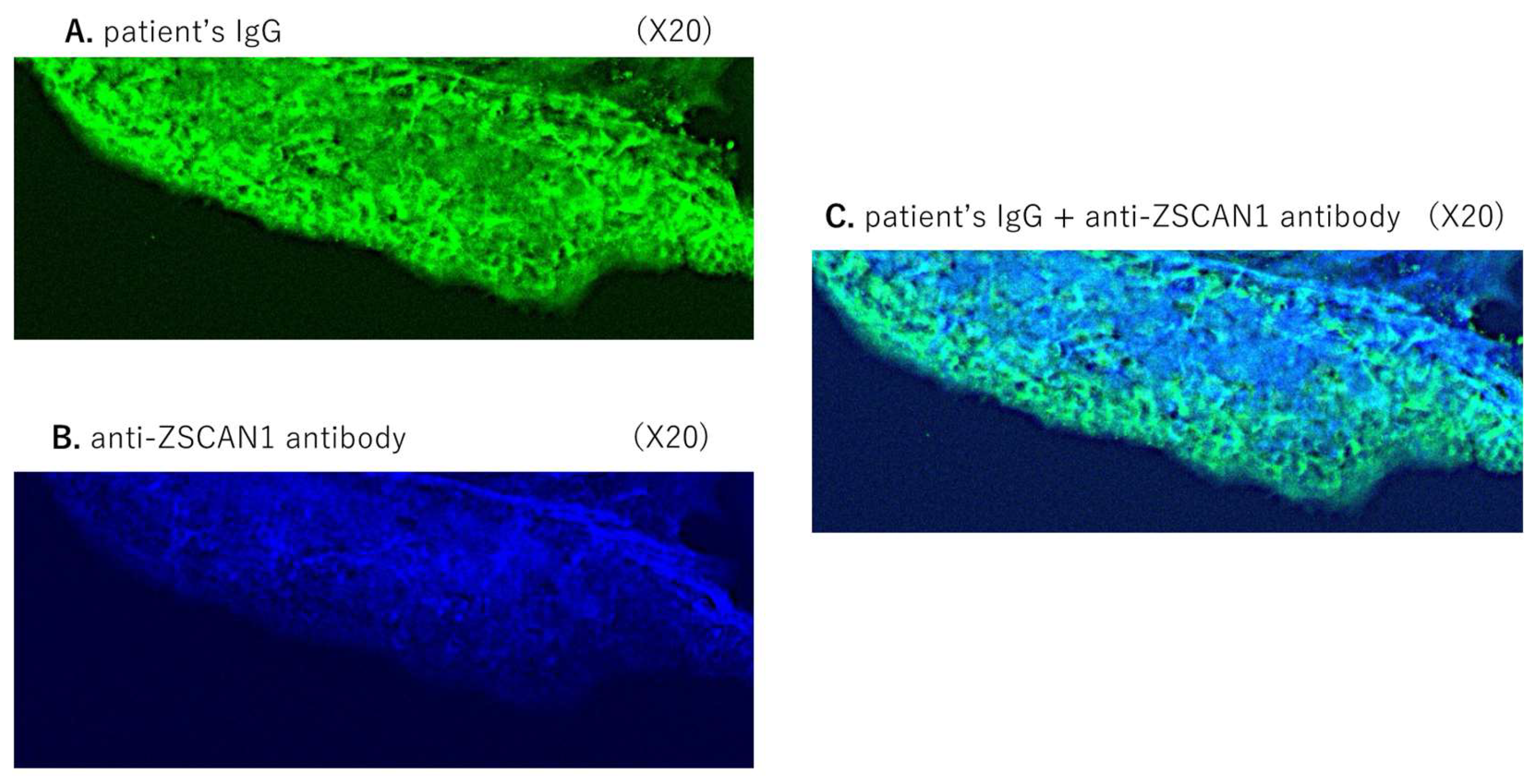
2.2. Immunostaining of the Mouse SFO
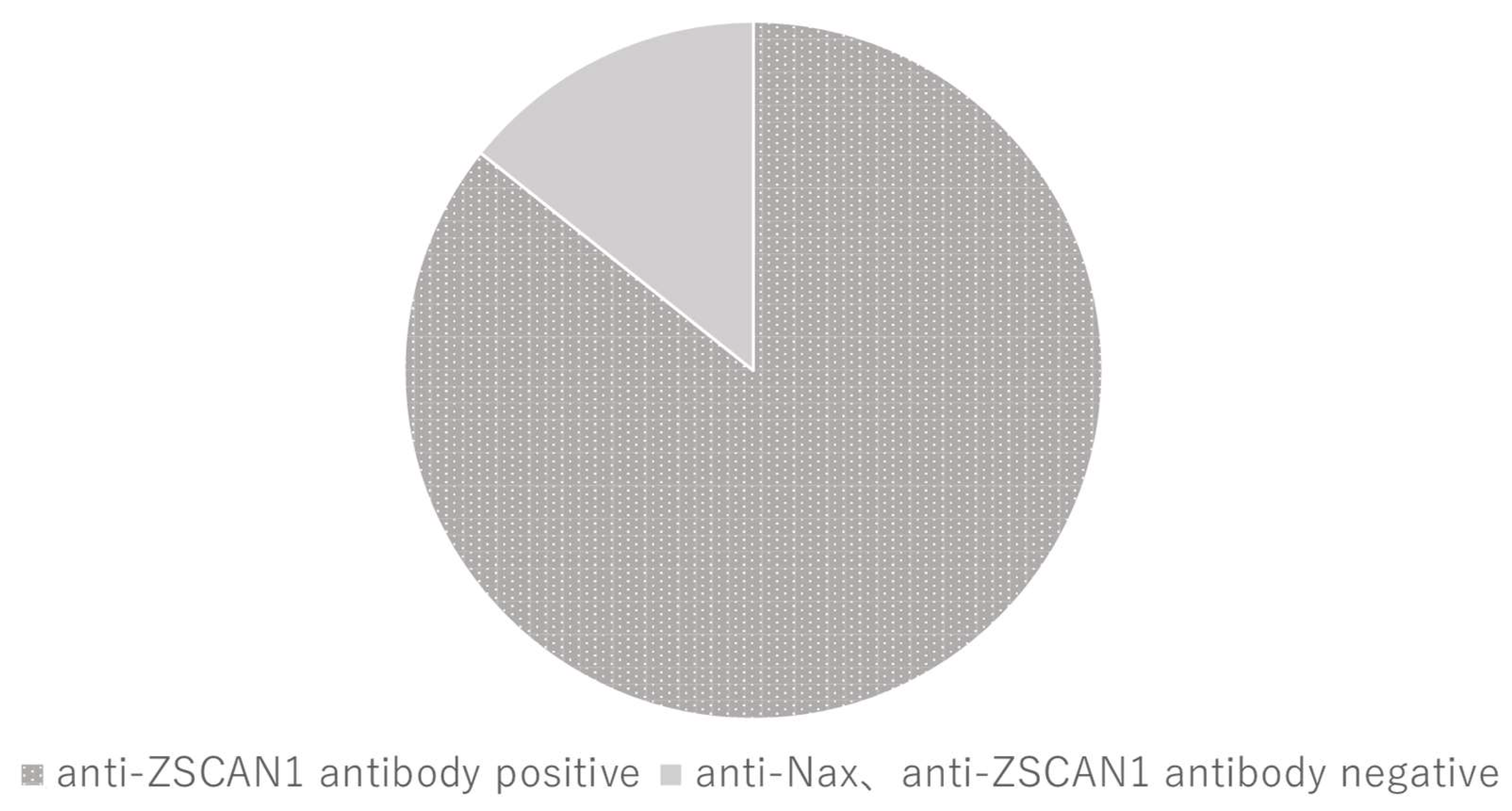
2.3. ELISA
3. Discussion
4. Materials and Methods
4.1. Subjects
4.2. Protein Arrays
4.3. Immunostaining of Mouse SFO
4.4. Detection of Anti-ZSCAN1 and Anti-Nax Autoantibodies by ELISA
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ize-Ludlow, D.; Gray, J.A.; Sperling, M.A.; Berry-Kravis, E.M.; Milunsky, J.M.; Farooqi, I.S.; Rand, C.M.; Weese-Mayer, D.E. Rapid-onset obesity with hypothalamic dysfunction, hypoventilation, and autonomic dysregulation presenting in childhood. Pediatrics 2007, 120, e179–e188. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.M.; Shin, J.; Kim, S.; Gee, H.Y.; Lee, J.S.; Cha, D.H.; Rim, J.H.; Park, S.J.; Kim, J.H.; Uçar, A.; et al. Rapid-Onset Obesity with Hypoventilation, Hypothalamic, Autonomic Dysregulation, and Neuroendocrine Tumors (ROHHADNET) Syndrome: A Systematic Review. Biomed. Res. Int. 2018, 21, 1250721. [Google Scholar] [CrossRef]
- Patwari, P.P.; Wolfe, L.F. Rapid-onset obesity with hypothalamic dysfunction, hypoventilation, and autonomic dysregulation: Review and update. Curr. Opin. Pediatr. 2014, 26, 487–492. [Google Scholar] [CrossRef]
- Harvengt, J.; Gernay, C.; Mastouri, M.; Farhat, N.; Lebrethon, M.C.; Seghaye, M.C.; Bours, V. ROHHAD(NET) Syndrome: Systematic Review of the Clinical Timeline and Recommendations for Diagnosis and Prognosis. J. Clin. Endocrinol. Metab. 2020, 105, dgaa247. [Google Scholar] [CrossRef]
- Cemeroglu, A.P.; Eng, D.S.; Most, L.A.; Stalsonburg, C.M.; Kleis, L. Rapid-onset obesity with hypothalamic dysfunction, hypoventilation, and autonomic dysregulation syndrome and celiac disease in a 13-year-old girl: Further evidence for autoimmunity? J. Pediatr. Endocrinol. Metab. 2016, 29, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Gharial, J.; Ganesh, A.; Curtis, C.; Pauranik, A.; Chan, J.; Kurek, K.; Lafay-Cousin, L. Neuroimaging and Pathology Findings Associated With Rapid Onset Obesity, Hypothalamic Dysfunction, Hypoventilation, and Autonomic Dysregulation (ROHHAD) Syndrome. J. Pediatr. Hematol. Oncol. 2021, 43, e571–e576. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, L.A.; Rane, S.; McReynolds, L.J.; Steppan, D.A.; Chen, A.R.; Paz-Priel, I. Improved Behavior and Neuropsychological Function in Children With ROHHAD After High-Dose Cyclophosphamide. Pediatrics 2016, 138, e20151080. [Google Scholar] [CrossRef] [PubMed]
- Hawton, K.A.; Doffinger, R.; Ramanan, A.V.; Langton Hewer, S.C.; Evans, H.J.; Giri, D.; Hamilton Shield, J.P. Rituximab therapy in ROHHAD(NET) syndrome. J. Pediatr. Endocrinol. Metab. 2022, 35, 1102–1106. [Google Scholar] [CrossRef] [PubMed]
- Hiyama, T.Y.; Utsunomiya, A.N.; Matsumoto, M.; Fujikawa, A.; Lin, C.H.; Hara, K.; Kagawa, R.; Okada, S.; Kobayashi, M.; Ishikawa, M.; et al. Adipsic hypernatremia without hypothalamic lesions accompanied by autoantibodies to subfornical organ. Brain Pathol. 2016, 27, 323–331. [Google Scholar] [CrossRef]
- Mandel-Brehm, C.; Benson, L.A.; Tran, B.; Kung, A.F.; Mann, S.A.; Vazquez, S.E.; Retallack, H.; Sample, H.A.; Zorn, K.C.; Khan, L.M.; et al. ZSCAN1 Autoantibodies Are Associated with Pediatric Paraneoplastic, R.O.H.H.A.D. Ann. Neurol. 2022, 92, 279–291. [Google Scholar] [CrossRef] [PubMed]
- Hiyama, T.Y.; Matsuda, S.; Fujikawa, A.; Matsumoto, M.; Watanabe, E.; Kajiwara, H.; Niimura, F.; Noda, M. Autoimmunity to the sodium-level sensor in the brain causes essential hypernatremia. Neuron 2010, 66, 508–522. [Google Scholar] [CrossRef]
- Nakamura-Utsunomiya, A.; Goda, S.; Hayakawa, S.; Sonoko, S.; Hoorn, E.J.; Blanchard, A.; Saito-Hakoda, A.; Kakimoto, H.; Hachiya, R.; Kamimura, M.; et al. Identification of clinical factors related to antibody-mediated immune response to the subfornical organ. Clin. Endocrinol. 2022, 97, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Nakamura-Utsunomiya, A.; Hiyama, T.Y.; Okada, S.; Noda, M.; Kobayashi, M. Characteristic clinical features of adipsic hypernatremia patients with subfornical organ-targeting antibody. Clin. Pediatr. Endocrinol. 2017, 26, 197–205. [Google Scholar] [CrossRef] [PubMed]
- Noda, M.; Hiyama, T.Y. Sodium sensing in the brain. Pflügers Arch. Eur. J. Physiol. 2015, 467, 465–474. [Google Scholar] [CrossRef] [PubMed]
- Artamonova, I.N.; Petrova, N.A.; Lyubimova, N.A.; Kolbina, N.Y.; Bryzzhin, A.V.; Borodin, A.V.; Levko, T.A.; Mamaeva, E.A.; Pervunina, T.M.; Vasichkina, E.S.; et al. Case Report: COVID-19-Associated ROHHAD-like Syndrome. Front Pediatr. 2022, 10, 854367. [Google Scholar] [CrossRef] [PubMed]
- Weese-Mayer, D.E.; Berry-Kravis, E.M.; Zhou, L.; Maher, B.S.; Silvestri, J.M.; Curran, M.E.; Marazita, M.L. Idiopathic congenital central hypoventilation syndrome: Analysis of genes pertinent to early autonomic nervous system embryologic development and identification of mutations in PHOX2b. Am. J. Med. Genet. A. 2003, 123A, 267–278. [Google Scholar] [CrossRef]
- Di Lascio, S.; Bachetti, T.; Saba, E.; Ceccherini, I.; Benfante, R.; Fornasari, D. Transcriptional dysregulation and impairment of PHOX2B auto-regulatory mechanism induced by polyalanine expansion mutations associated with congenital central hypoventilation syndrome. Neurobiol. Dis. 2013, 50, 187–200. [Google Scholar] [CrossRef] [PubMed]
- Barclay, S.F.; Rand, C.M.; Borch, L.A.; Nguyen, L.; Gray, P.A.; Gibson, W.T.; Wilson, R.J.; Gordon, P.M.; Aung, Z.; Berry-Kravis, E.M.; et al. Rapid-Onset Obesity with Hypothalamic Dysfunction, Hypoventilation, and Autonomic Dysregulation (ROHHAD): Exome sequencing of trios, monozygotic twins and tumours. Orphanet. J. Rare Dis. 2015, 10, 103. [Google Scholar] [CrossRef] [PubMed]
- Patwari, P.P.; Rand, C.M.; Berry-Kravis, E.M.; Ize-Ludlow, D.; Weese-Mayer, D.E. Monozygotic twins discordant for ROHHAD phenotype. Pediatrics 2011, 128, e711–e715. [Google Scholar] [CrossRef] [PubMed]
- Grossi, A.; Rusmini, M.; Cusano, R.; Massidda, M.; Santamaria, G.; Napoli, F.; Angelelli, A.; Fava, D.; Uva, P.; Ceccherini, I.; et al. Whole genome sequencing in ROHHAD trios proved inconclusive: What’s beyond? Front Genet. 2023, 14, 1031074. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Case 1 | Case 2 | Case 3 | Case 4 | Case 5 | |
|---|---|---|---|---|---|
| Age/sex | 12/F | 14/F | 4/F | 4/F | 5y/M |
| Serum Na (mEq/L) (normal range:138–145) | 153 | 146 | 156 | 149 | 152 |
| Tumor | - | - | - | + | - |
| Obesity | + | + | + | + | - |
| Growth Hormone deficiency | + | + | - | + | - |
| Anti-SFO autoantibody response | + | + | + | + | + |
| Anti-Nax autoantibody response | - | - | - | - | - |
| No. | Gene Symbol | Clone ID | ① | ② | ③ | ④ | ⑤ |
|---|---|---|---|---|---|---|---|
| 1 | GPRC5A | FLJ10899AAAF | 0.9 | 18.7 | 0.2 | 0.2 | 0.1 |
| 2 | HDGFL1 | FLJ32262AAAF | 3.2 | 0 | −0.5 | −0.5 | −0.6 |
| 3 | TRIM34 | FLJ14970AAAF | 0.3 | 0.2 | −0.2 | 0 | −0.2 |
| 4 | FICD | FLJ20007AAF | 17.4 | 0.4 | 0 | 0 | −0.2 |
| 5 | SMOC2 | FLJ32138AAAF | 1 | 0.7 | 0.1 | 10.2 | 0 |
| 6 | ZSCAN1 | FLJ33779AAAF | 11.6 | 72.1 | 96.2 | 6.6 | 189.6 |
| 7 | ZNF329 | FLJ39223AAAF | 1.3 | 3.4 | 1.7 | 0.6 | 47.6 |
| 8 | REM2 | FLJ38964AAAF | 0.8 | 0.4 | 4 | 0.2 | 0.6 |
| 9 | SREBF1 | FLJ33812AAAF | 0.8 | 9.9 | 0.7 | 0.9 | 0 |
| 10 | GATAD2A | FLJ43986AAAF | 3.7 | 27.4 | 1.3 | 1.3 | 1.3 |
| 11 | ATG16L1 | FLJ4948AAAF | 1.3 | 0.7 | 0.1 | 7.9 | 0.6 |
| 12 | ZNF641 | FLJ31295AAAF | 0.7 | 0.5 | −0.1 | 34 | 0.2 |
| 13 | ZNF133 | FLJ16801AAAF | 0.6 | 0.4 | 1.2 | 54.6 | 0.2 |
| 14 | CCDC136 | FLJ42456AAAF | 1.1 | 0.2 | −0.1 | 16.5 | −0.2 |
| 15 | ZNF414 | FLJ23611AAAF | 0.6 | 9.6 | 0.4 | 0.2 | 0.3 |
| 16 | EMCN | FLJ94060AAAF | 0 | 0.7 | 16.7 | 0 | −0.2 |
| 17 | ZNRD1 | FLJ81067AAAF | 0.2 | 0.4 | 1.2 | 0.2 | 0.3 |
| 18 | HDAC3 | FLJ80944AAAF | 0.4 | 0.4 | 0.2 | 0 | −0.4 |
| 19 | ADAD2 | FLJ96146AAAF | 1 | 16.4 | 2.7 | 0.6 | 0.5 |
| 20 | APBB1 | FLJ54642AAAF | 9 | 0.2 | 4.5 | 0.1 | −0.2 |
| 21 | MOK | FLJ93194AAAF | 0.7 | 0.5 | 0.5 | 30.6 | 0.2 |
| 22 | SHKBP1 | FLJ93157AAAF | 0.4 | 0.2 | 0.2 | 0.2 | 0.1 |
| 23 | PTK2 | FLJ57218AAAF | 41.2 | 0.3 | −0.4 | 0.3 | −0.4 |
| 24 | IRX2 | FLJ93157AAAF | 0.2 | 0.5 | 0 | 53.7 | −0.1 |
| 25 | COL26A1 | FLJ57218AAAF | 21.2 | 0.2 | 0 | 0 | −0.2 |
| 26 | PPARGC1A | FLJ82376AAAF | 0.1 | 1 | 1.9 | 0.3 | 0 |
| 27 | IFT74 | FLJ13645AAAN | 0.7 | 0.1 | 4.8 | 0.1 | 0.3 |
| 28 | ATF7IP | FLJ21497AAAN | 1.8 | 0.1 | −0.2 | −0.2 | −0.2 |
| 29 | TNKS1BP1 | FLJ42913AAAN | 0.4 | 0.3 | 6.2 | −0.2 | 5.5 |
| 30 | HES1 | FLJ20408AAAN | 8 | 0.5 | 0.1 | 0.1 | 0 |
| 31 | ZC3H18 | FLJ84571AAAN | 0 | 22.7 | −0.2 | 0 | −0.5 |
| 32 | AKAP4 | N0751-C01-7_FOD_00129 | 9.8 | 0.3 | 0.4 | 0 | −0.2 |
| 33 | LIPE | N0831-D05-1_FOD_21144 | 0.2 | 13.3 | −0.1 | 0 | 0.1 |
| ROHHAD Case | Age/Sex | Serum Na (mEq/L) | Obesity | GHD | Central Apnea | Anti-Nax Antibody | Prognosis | Anti-ZSCAN1 Titer |
|---|---|---|---|---|---|---|---|---|
| 1 | 3/F | 153 | + | + | - | - | Alive | 54 |
| 2 | 4/F | 157 | + | - | - | - | Alive | 70 |
| 3 | 3/M | 157 | + | + | - | - | Alive | 70 |
| 4 | 13/M | 173 | - | - | - | N/A | Alive | 59 |
| 5 | 9/M | 164 | + | + | + | + | Alive | 62 |
| 6 | 2/F | 147 | + | - | + | - | Alive | 160 |
| 7 | 17/F | 194 | + | + | + | - | Death | 244 |
| 8 | 10/M | 150 | + | + | - | - | Alive | 0 |
| 9 | 11/M | 155 | + | + | - | - | Alive | 62 |
| 10 | 2/F | 143 | + | N/A | + | - | Alive | 49 |
| 11 | 7/F | 150 | + | + | - | - | Alive | 317 |
| 12 | 12/M | 151 | + | - | + | - | Alive | 105 |
| 13 | 8/M | 145 | + | - | - | - | Alive | 0 |
| 14 | 2/F | 167 | + | - | + | - | Alive | 128 |
| Control case | Age/sex | Serum Na (mEq/L) | Obesity | GHD | Central apnea | Anti-Nax Antibody | Diagnosis | Anti-ZSCAN1 titer |
| 1 | 12/F | 138 | - | - | - | - | healthy | 0.1 |
| 2 | 3/M | 140 | - | - | - | - | healthy | 2.6 |
| 3 | 1/F | 143 | - | - | - | - | healthy | 1.1 |
| 4 | 2/F | 137 | - | - | - | - | West syndrome | 3.3 |
| 5 | 9/M | 139 | - | - | - | - | healthy | 2.3 |
| 6 | 14/F | 140 | - | - | - | - | Basedow’s disease | 7.8 |
| 7 | 1/M | 137 | - | - | - | - | healthy | 4.3 |
| 8 | 2/M | 140 | - | - | - | - | healthy | 4.8 |
| 9 | 8/M | 139 | + | - | - | - | Congenital hypothyroidism | 4.2 |
| 10 | 13/M | 140 | - | - | - | - | healthy | 0.7 |
| 11 | 15/M | 139 | - | - | - | - | IDDM | 3.2 |
| 12 | 14/F | 138 | - | - | - | - | Myasthenia gravis | 1.2 |
| 13 | 1/M | 140 | - | - | - | - | healthy | 2.5 |
| 14 | 12/F | 139 | - | - | - | - | Basedow’s disease | 7.4 |
| 15 | 13/M | 140 | - | - | - | - | healthy | 2.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakamura-Utsunomiya, A.; Yamaguchi, K.; Goshima, N. Anti-ZSCAN1 Autoantibodies Are a Feasible Diagnostic Marker for ROHHAD Syndrome Not Associated with a Tumor. Int. J. Mol. Sci. 2024, 25, 1794. https://doi.org/10.3390/ijms25031794
Nakamura-Utsunomiya A, Yamaguchi K, Goshima N. Anti-ZSCAN1 Autoantibodies Are a Feasible Diagnostic Marker for ROHHAD Syndrome Not Associated with a Tumor. International Journal of Molecular Sciences. 2024; 25(3):1794. https://doi.org/10.3390/ijms25031794
Chicago/Turabian StyleNakamura-Utsunomiya, Akari, Kei Yamaguchi, and Naoki Goshima. 2024. "Anti-ZSCAN1 Autoantibodies Are a Feasible Diagnostic Marker for ROHHAD Syndrome Not Associated with a Tumor" International Journal of Molecular Sciences 25, no. 3: 1794. https://doi.org/10.3390/ijms25031794
APA StyleNakamura-Utsunomiya, A., Yamaguchi, K., & Goshima, N. (2024). Anti-ZSCAN1 Autoantibodies Are a Feasible Diagnostic Marker for ROHHAD Syndrome Not Associated with a Tumor. International Journal of Molecular Sciences, 25(3), 1794. https://doi.org/10.3390/ijms25031794